100 Random Orthopedic MCQs for Board Prep (2026 Update)
14 Apr 2026
138 min read
136 Views

Key Takeaway
This topic focuses on ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW4, The anterior band of the anterior bundle of the elbow medial ulnar collateral ligament (UCL) exhibits an isometric strain pattern throughout elbow range of motion (ROM). This anatomical detail is crucial for understanding elbow kinematics and is frequently covered in elbow orthopedic mcqs, emphasizing the anterior bundle's primary role as a restraint to valgus instability of the elbow.
100 Random Orthopedic MCQs for Board Prep (20...
00:00
Start Quiz
Question 1High Yield
Which of the following fascial structures does not contribute to the formation of the spiral cord:
Explanation
The pretendinous band, spiral band, lateral digital sheet, and Grayson's ligament are all parts of the normal fascia that contribute to the formation of the spiral cord. C leland's ligament is not involved at all in the disease process.
Question 2High Yield
The main blood supply to the capital femoral epiphysis in a 10-year-old child is supplied from the ](http://www.orthobullets.com/anatomy/10123/hip-blood-supply)
Explanation
No detailed explanation available.
Question 3High Yield
A 78-year-old woman underwent total hip arthroplasty 15 years ago. She reports a recent history of increasing thigh pain prior to a fall and is now unable to ambulate. Radiographs are shown in Figures 87a and 87b. What is the best treatment for this condition?


Explanation
DISCUSSION: Severe periprosthetic fractures after total hip arthroplasty with a loose implant and progressive bone loss are difficult problems for orthopaedic surgeons, with a high complication rate. Recent literature favors the use of long fluted tapered stems that have a long distal taper that may optimally engage the remaining femoral shaft isthmus. Plating options are problematic because the ability to use screws with the plate is limited by the intramedullary stem. Although not the only solution to this problem (such as allograft-prosthetic composites, impaction grafting, tumor prostheses), long distally fixed stems circumvent this problem by enhancing fracture healing and create a long-term prosthetic solution in these most difficult cases.
DISCUSSION: Severe periprosthetic fractures after total hip arthroplasty with a loose implant and progressive bone loss are difficult problems for orthopaedic surgeons, with a high complication rate. Recent literature favors the use of long fluted tapered stems that have a long distal taper that may optimally engage the remaining femoral shaft isthmus. Plating options are problematic because the ability to use screws with the plate is limited by the intramedullary stem. Although not the only solution to this problem (such as allograft-prosthetic composites, impaction grafting, tumor prostheses), long distally fixed stems circumvent this problem by enhancing fracture healing and create a long-term prosthetic solution in these most difficult cases.
Scientific References
- : Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475503.
Kwong LM, Miller AJ, Lubinus P: A modular distal fixation option for proximal bone loss in revision total hip
arthroplasty: A 2- to 6-year follow-up study. J Arthroplasty 2003;18:94-97.
Figure 88a Figure 88b
Question 4High Yield
A 20-year-old man who sustains closed femoral and tibial shaft fractures has
2. mild distention of the abdomen, a systolic blood pressure of 75 mm Hg, and a
3. pulse rate of 135/min. His neurovascular examination is normal. Lateral
4. cervical spine, chest, and AP pelvis radiographs are normal. After
5. administration of 2 L of crystalloid, he has a systolic blood pressure of 95 mm
6. Hg and a pulse rate of 120/min. Management should now include
7. 1- diagnostic peritoneal lavage.
8. 2- immediate femoral nailing and splinting of the tibia.
9. 3- immediate stabilization of both the femur and the tibia.
10. 4- splinting the tibia and placing the femur in skeletal traction.
11. 5- simultaneous retrograde femoral nailing and an exploratory laparotomy.
2. mild distention of the abdomen, a systolic blood pressure of 75 mm Hg, and a
3. pulse rate of 135/min. His neurovascular examination is normal. Lateral
4. cervical spine, chest, and AP pelvis radiographs are normal. After
5. administration of 2 L of crystalloid, he has a systolic blood pressure of 95 mm
6. Hg and a pulse rate of 120/min. Management should now include
7. 1- diagnostic peritoneal lavage.
8. 2- immediate femoral nailing and splinting of the tibia.
9. 3- immediate stabilization of both the femur and the tibia.
10. 4- splinting the tibia and placing the femur in skeletal traction.
11. 5- simultaneous retrograde femoral nailing and an exploratory laparotomy.
Explanation
1.
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Ostrum RF, Verghese GB, Santner TJ: The lack of association between femoral shaft fractures and hypotensive shock. J Orthop Trauma 1993;7:338-342. Shock, in Alexander RH, Proctor HJ (eds): Advanced Trauma Life Support: Program for Physicians, ed 5. Chicago, IL, American College of Physicians, 1993, pp 75-110.
#
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Ostrum RF, Verghese GB, Santner TJ: The lack of association between femoral shaft fractures and hypotensive shock. J Orthop Trauma 1993;7:338-342. Shock, in Alexander RH, Proctor HJ (eds): Advanced Trauma Life Support: Program for Physicians, ed 5. Chicago, IL, American College of Physicians, 1993, pp 75-110.
#
Question 5High Yield
A mutation in which of the following genes causes a disturbance in normal limb outgrowth patterning:
Explanation
P63 is an important factor in normal limb outgrowth patterning. The other factors are involved with common disorders:
C BFA1: C leidocranial dysplasia
C OMP: Multiple epiphyseal dysplasia
C OL1A1: Osteogenesis imperfecta (easy to remember type I collagen) VDR3: Osteoporosis (easy to remember vitamin D receptor)
C orrect Answer: P63
C BFA1: C leidocranial dysplasia
C OMP: Multiple epiphyseal dysplasia
C OL1A1: Osteogenesis imperfecta (easy to remember type I collagen) VDR3: Osteoporosis (easy to remember vitamin D receptor)
C orrect Answer: P63
Question 6High Yield
The best treatment is
Explanation
- chemotherapy and wide surgical resection._
Question 7High Yield
The best index to measure acetabular deficiency in the coronal plane is:
Explanation
Literature from Europe and North America suggests that a patient with acetabular dysplasia whose anteroposterior radiograph shows a center edge angle of Wiberg less than 15° is a good candidate for periacetabular osteotomy
Question 8High Yield
When performing an index finger ray amputation, the orthopaedic surgeon should move the
Explanation
Ray amputation often is performed to improve function and decrease pain by removing the digit through the metacarpal. Hyperesthesia and painful light touch are the most disabling complications. The digital nerves should be placed proximal to the wound to prevent a symptomatic neuroma. The radial and ulnar digital nerves can be sutured together, transposed to the interosseous muscle, or resected proximally, although no technique is superior. Excessive mobilization is discouraged, and care is taken to protect the radial digital nerve to the long finger at the time of index ray amputation. Transfer of the first dorsal interosseous, EIP and FDS to the long finger are procedures that have fallen out of favor because of lack of benefit and resulting stiffness.
RECOMMENDED READINGS
57. Blazar PE, Garon MT. Ray Resections of the Fingers: Indications, Techniques, and Outcomes. J Am Acad Orthop Surg. 2015 Aug;23(8):476-84. doi: 10.5435/JAAOS-D-14-00056. Review. PubMed PMID: 26209144.
58. Murray JF, Carman W, MacKenzie JK. Transmetacarpal amputation of the index finger: a clinical assessment of hand strength and complications. J Hand Surg Am. 1977 Nov;2(6):471-
81/. PubMed PMID: 925334.
CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 55
A 60-year-old man has a symptomatic contracture of his dominant-hand ring finger. Treatment options are discussed, and he elects to proceed with palmar fasciectomy.
RECOMMENDED READINGS
57. Blazar PE, Garon MT. Ray Resections of the Fingers: Indications, Techniques, and Outcomes. J Am Acad Orthop Surg. 2015 Aug;23(8):476-84. doi: 10.5435/JAAOS-D-14-00056. Review. PubMed PMID: 26209144.
58. Murray JF, Carman W, MacKenzie JK. Transmetacarpal amputation of the index finger: a clinical assessment of hand strength and complications. J Hand Surg Am. 1977 Nov;2(6):471-
81/. PubMed PMID: 925334.
CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 55
A 60-year-old man has a symptomatic contracture of his dominant-hand ring finger. Treatment options are discussed, and he elects to proceed with palmar fasciectomy.
Question 9High Yield
An 85-year-old woman falls and injures her elbow in her non dominant arm. Radiographs are shown in Figure A and
Explanation
4/. Total elbow arthroplasty
5/. Casting for 4 weeks then ROM
Total elbow arthroplasty (TEA) is ideal for treating comminuted osteoporotic fractures of the distal humerus in low demand elderly patients. Outcomes are good to excellent with quick return of stability and functional motion but with carrying weight restriction of 5 lbs. ORIF would be the best choice for younger individuals with better bone quality.
Cobb described the outcomes of 21 total elbow arthroplasties in elderly patients all of which had good or excellent results without evidence of component loosening. The mean motion was 25 to 130 degrees. Complications included fracture of the ulnar component in one patient after another fall, ulnar neurapraxia in three, and reflex sympathetic dystrophy in one.
McKee et al. performed a randomized controlled study of TEA versus fixation and found that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF. They also found that although elderly patients with this injury have an increased baseline DASH score, they appear to accommodate to objective limitations in function with time.
Frankle et al. retrospectively compared TEA to plate fixation for distal humerus fractures in the elderly and found a significant improvement in outcomes and revision rates with TEA as compared to plate fixation. The differences were seen most in women with associated comorbidities, such as rheumatoid arthritis, osteoporosis, and conditions requiring the use of systemic steroids.
5/. Casting for 4 weeks then ROM
Total elbow arthroplasty (TEA) is ideal for treating comminuted osteoporotic fractures of the distal humerus in low demand elderly patients. Outcomes are good to excellent with quick return of stability and functional motion but with carrying weight restriction of 5 lbs. ORIF would be the best choice for younger individuals with better bone quality.
Cobb described the outcomes of 21 total elbow arthroplasties in elderly patients all of which had good or excellent results without evidence of component loosening. The mean motion was 25 to 130 degrees. Complications included fracture of the ulnar component in one patient after another fall, ulnar neurapraxia in three, and reflex sympathetic dystrophy in one.
McKee et al. performed a randomized controlled study of TEA versus fixation and found that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF. They also found that although elderly patients with this injury have an increased baseline DASH score, they appear to accommodate to objective limitations in function with time.
Frankle et al. retrospectively compared TEA to plate fixation for distal humerus fractures in the elderly and found a significant improvement in outcomes and revision rates with TEA as compared to plate fixation. The differences were seen most in women with associated comorbidities, such as rheumatoid arthritis, osteoporosis, and conditions requiring the use of systemic steroids.
Question 10High Yield
-
A 30-year-old man underwent replantation of his dominant thumb at the metacarpophalangeal joint level 2 days ago. Since replantation, the temperature of the thumb has been between 87.8 F (31 C) and 93.2 F (34 C). The temperature is now 82.4 F (28 C), and there is brisk capillary refill and venous engorgement. Management at this time should include
A 30-year-old man underwent replantation of his dominant thumb at the metacarpophalangeal joint level 2 days ago. Since replantation, the temperature of the thumb has been between 87.8 F (31 C) and 93.2 F (34 C). The temperature is now 82.4 F (28 C), and there is brisk capillary refill and venous engorgement. Management at this time should include
Explanation
The patient is experiencing impending failure of the replanted thumb. In a study by Moneim and Chacon, they found that vascular thrombosis in the postoperative period is the major factor in failure after replantation. When it occurs, it has to be aggressively dealt with by surgical exploration and revision of the vascular repair. The best results are obtained within 11 hours of the repair and nonsurgical management uniformly led to failure.
Question 11High Yield
The most common extraskeletal manifestation of this disease is
Explanation
- café au lait macules._
Question 12High Yield
A 24-year-old man has a deep knife wound across the dorsal aspect of his wrist, transecting all of his wrist and finger extensor tendons. How does the surgeon determine which of the proximal tendon stumps in the fourth dorsal compartment is the extensor indicis proprius? ](http://www.orthobullets.com/anatomy/10040/extensor-indicis)Review Topic
Explanation
No detailed explanation available.
Question 13High Yield
Figures 32a through 32d are the radiographs and MR images of a 13-year-old girl with new posterolateral knee pain following a fall. What is the best next step?


Explanation
This patient has an incidentally noted benign-appearing fibro-osseous lesion of her proximal tibia. The lesion does not correspond to her area of pain, and there is no indication she experienced pain from the lesion prior to the fall. Radiographs and MR imaging findings are consistent with a fibrous cortical defect or nonossifying fibroma. There is no surrounding edema in the bone or soft tissue and no soft-tissue mass, and the lesion has a sclerotic rim around it. These are common lesions in children, and there is no need for a biopsy, curettage, or referral to a tumor specialist. This patient should not be at high risk for pathologic fracture from this lesion. Observation with follow-up radiographs in 3 to 6 months is the treatment of choice.
RECOMMENDED READINGS
11. [Gebhardt MC, Ready JE, Mankin HJ. Tumors about the knee in children. Clin Orthop Relat Res. 1990 Jun;(255):86-110. Review. PubMed PMID: 2189635.](http://www.ncbi.nlm.nih.gov/pubmed/2189635)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2189635)
12. [Aboulafia AJ, Kennon RE, Jelinek JS. Benign bone tumors of childhood. J Am Acad Orthop Surg. 1999 Nov-Dec;7(6):377-88. Review. PubMed PMID: 11505926. ](http://www.ncbi.nlm.nih.gov/pubmed/11505926)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11505926)
RECOMMENDED READINGS
11. [Gebhardt MC, Ready JE, Mankin HJ. Tumors about the knee in children. Clin Orthop Relat Res. 1990 Jun;(255):86-110. Review. PubMed PMID: 2189635.](http://www.ncbi.nlm.nih.gov/pubmed/2189635)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2189635)
12. [Aboulafia AJ, Kennon RE, Jelinek JS. Benign bone tumors of childhood. J Am Acad Orthop Surg. 1999 Nov-Dec;7(6):377-88. Review. PubMed PMID: 11505926. ](http://www.ncbi.nlm.nih.gov/pubmed/11505926)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11505926)
Question 14High Yield
A relative contraindication for anteromedial tibial tubercle transfer for patellar instability is arthrosis in what portion of the patella?
Explanation
Anteromedial displacement of the tibial tubercle unloads the distal and lateral facets of the patella and shifts the forces to the proximal and medial facets. Therefore, if findings indicate arthrosis predominately in the medial and proximal areas of the patella, this is considered a relative contraindication because it may accentuate arthritic symptoms.
REFERENCES: Fulkerson JP: Anteromedialization of the tibial tuberosity for patellofemoral malalignment. Clin Orthop 1983;177:176-181.
Bellemans J, Cauwenberghs F, Witvrouw E, et al: Anteromedial tibial tubercle transfer in patients with chronic anterior knee pain and a subluxation-type patellar malalignment. Am J Sports Med 1997;25:375-381.
Kuroda R, Kambic H, Valdevit A, et al: Articular cartilage contact pressure after tibial tuberosity transfer: A cadaveric study. Am J Sports Med 2001;29:403-409.
REFERENCES: Fulkerson JP: Anteromedialization of the tibial tuberosity for patellofemoral malalignment. Clin Orthop 1983;177:176-181.
Bellemans J, Cauwenberghs F, Witvrouw E, et al: Anteromedial tibial tubercle transfer in patients with chronic anterior knee pain and a subluxation-type patellar malalignment. Am J Sports Med 1997;25:375-381.
Kuroda R, Kambic H, Valdevit A, et al: Articular cartilage contact pressure after tibial tuberosity transfer: A cadaveric study. Am J Sports Med 2001;29:403-409.
Question 15High Yield
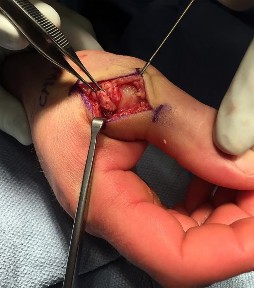
A 32-year-old man sustained an injury to the right thumb metacarpophalangeal (MP) joint ulnar collateral ligament (UCL) and is undergoing surgical repair (Figure 1). What structure in the clinical photograph is blocking reduction of the ulnar collateral ligament?
Explanation
When the thumb MP UCL is torn from the proximal phalanx, the distal stump can be displaced superficial to the adductor aponeurosis, known as a Stener lesion. The adductor aponeurosis effectively blocks reduction of the ligament to the normal attachment site. The EPB and EPL tendons are dorsal to the UCL, and the ulnar sesamoid bone/volar plate are in a volar position in relation to the UCL. The dorsal capsule would also not block reduction of the UCL due to it's anatomic location. The other responses do not block _the UCL with this type of injury._
Question 16High Yield
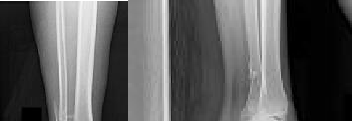
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for
Explanation
DISCUSSION: In patients with an osteomyelitic infection, radiographic findings at 1 to 5 days usually show soft-tissue swelling only. Seven to 14 days after symptoms begin, radiographs will most likely show the classic signs of acute osteomyelitis. Reactive bone formation would be expected by 6 months.
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Song KM, Sloboda JF: Acute hematogenous osteomyelitis in children. J Am Acad Orthop Surg 2001;9:166-175.
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Song KM, Sloboda JF: Acute hematogenous osteomyelitis in children. J Am Acad Orthop Surg 2001;9:166-175.
Question 17High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Anatomic reduction and stabilization of the posterior malleolus fracture component
---
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Anatomic reduction and stabilization of the posterior malleolus fracture component
---

Explanation
The radiographs reveal a trimalleolar ankle fracture dislocation with an
associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior
malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
17. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
18. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
19. Maximizes the surface area for ankle joint loading
20. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior
malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
17. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
18. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
19. Maximizes the surface area for ankle joint loading
20. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
Question 18High Yield
The clinical photograph of the hand of a 72-year-old woman who sustained a
2. laceration of the flexor pollicis longus in her thumb is shown in Figure 45. She
3. cannot actively flex the interphalangeal joint. Which pulley, in addition to the
4. oblique pulley, has been lacerated?
5. 1- A-1
6. 2- A-2
7. 3- A-3
8. 4- A-4
9. 5- A-5
2. laceration of the flexor pollicis longus in her thumb is shown in Figure 45. She
3. cannot actively flex the interphalangeal joint. Which pulley, in addition to the
4. oblique pulley, has been lacerated?
5. 1- A-1
6. 2- A-2
7. 3- A-3
8. 4- A-4
9. 5- A-5
Explanation
1.
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Doyle JR, Blythe WF: Anatomy of the flexor tendon sheath and pulleys of the thumb. J Hand Surg 1977;2:149-151.
#
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Doyle JR, Blythe WF: Anatomy of the flexor tendon sheath and pulleys of the thumb. J Hand Surg 1977;2:149-151.
#
Question 19High Yield
An otherwise healthy 25-year-old man underwent a right anterior cruciate ligament reconstruction with a bone-patellar tendon-bone allograft. Routine preimplantation cultures of the allograft taken by the surgeon were positive for coagulase-negative Staphylococcus 5 days postoperatively. The patient has exhibited no evidence of clinical infection and his postoperative course has been uncomplicated during this time. What is the ideal management of this patient?


Explanation
DISCUSSION: The incidence of preimplantation positive cultures of musculoskeletal allografts used for anterior cruciate ligament reconstruction has varied between 4.8% and 13.3%. Interestingly, in none of the studies evaluating this issue did any of the patients implanted with a “contaminated” graft develop a clinical infection. The results of the current literature suggest that the treatment of low- virulence organisms is unnecessary if no evidence of clinical infection exists. Preimplantation cultures do not appear to correlate with clinical infection. Therefore, the routine culture of allograft tissue is not recommended.
REFERENCES: Diaz-de-Rada P, Barriga A, Barroso JL, et al: Positive culture in allograft ACL- reconstruction: What to do? Knee Surg Sports Traumatol Arthrosc 2003; 11:219-222.
Guelich DR, Lowe WR, Wilson B: The routine culture of allograft tissue in anterior cruciate ligament reconstruction. Am J Sports Med 2007;35:1495-1499.
Centeno JM, Woolf S, Reid JB III, et al: Do anterior cruciate ligament allograft culture results correlate with clinical infections? Arthroscopy 2007;23:1100-1103.
72 • American Academy of Orthopaedic Surgeons
Figure 87a Figure 87b
REFERENCES: Diaz-de-Rada P, Barriga A, Barroso JL, et al: Positive culture in allograft ACL- reconstruction: What to do? Knee Surg Sports Traumatol Arthrosc 2003; 11:219-222.
Guelich DR, Lowe WR, Wilson B: The routine culture of allograft tissue in anterior cruciate ligament reconstruction. Am J Sports Med 2007;35:1495-1499.
Centeno JM, Woolf S, Reid JB III, et al: Do anterior cruciate ligament allograft culture results correlate with clinical infections? Arthroscopy 2007;23:1100-1103.
72 • American Academy of Orthopaedic Surgeons
Figure 87a Figure 87b
Question 20High Yield
Slide 1 Slide 2
A 42-year-old male patient presents with a history of repeated giving way of his ankle. He notes that this has been present for 1 year. He does not experience any pain, even with the episodic bouts of the ankle buckling. On examination, the ankle range of motion is normal, no pain is elicited, and there is no crepitus. A stress radiograph (Slide 1) and a lateral weight-bearing radiograph (Slide 2) are presented. The patient does not want to undergo surgery, but he needs to know the possibility of problems with his ankle in the future. The patient should be advised that:
A 42-year-old male patient presents with a history of repeated giving way of his ankle. He notes that this has been present for 1 year. He does not experience any pain, even with the episodic bouts of the ankle buckling. On examination, the ankle range of motion is normal, no pain is elicited, and there is no crepitus. A stress radiograph (Slide 1) and a lateral weight-bearing radiograph (Slide 2) are presented. The patient does not want to undergo surgery, but he needs to know the possibility of problems with his ankle in the future. The patient should be advised that:
Explanation
Ankle arthritis is rarely idiopathic. In the United States, the most common source of ankle arthritis is following trauma, usually of a major nature. Repetitive ankle injury, particularly when associated with recurrent instability and a varus or cavus foot, will likely lead to the development of ankle arthritis. Patients should be counseled that recurrent instability of the ankle, particularly when osteophytes are already present, frequently leads to arthritis.
Question 21High Yield
A concussion diagnosis is made when there is







Explanation
Neurocognitive testing is a helpful tool in the management of concussions, but testing does not independently determine if an athlete has experienced a concussion or when he or she can return to play. Neuroimaging findings typically are normal in concussive injury. Loss of consciousness occurs in fewer than 10% of patients with concussions. A concussion diagnosis is difficult to determine because of the lack of objective clinical and/or imaging findings. In general, a concussion is a disturbance in brain function caused by a direct or indirect force to the head.
Figure 26
Figure 27a
Figure 27b
Figure 28
Figure 29
Figure 30
Figure 31a
Figure 31b
RESPONSES FOR QUESTIONS 26 THROUGH 31
1. Plain radiographs
2. CT scan
3. MRI
4. Arthrogram
Which imaging method listed above is most appropriate for definitive diagnosis and management of each clinical scenario described below?
Figure 26
Figure 27a
Figure 27b
Figure 28
Figure 29
Figure 30
Figure 31a
Figure 31b
RESPONSES FOR QUESTIONS 26 THROUGH 31
1. Plain radiographs
2. CT scan
3. MRI
4. Arthrogram
Which imaging method listed above is most appropriate for definitive diagnosis and management of each clinical scenario described below?
Question 22High Yield
Figure 11a is the radiograph of a 45-year-old woman with a moderate bunion deformity. A Chevron osteotomy was performed and after 6 weeks the patient was doing reasonably well. Six months later she reports increasing pain and stiffness in her toe. Clinically the toe is reasonably straight, but she has significant calluses and overload under the second and third metatarsals. A follow-up radiograph is shown in Figure 11b. The patient wants to be free of pain. What is the most appropriate treatment?

Explanation
The patient developed osteonecrosis of the metatarsal head with shortening of the first metatarsal and subsequent overload of the lesser metatarsals. The most reliable option is to perform a metatarsophalangeal joint fusion with an autologous bone block to restore length. A revision bunion repair will not address the arthritic
changes. A Keller’s excision arthroplasty will further aggravate the lesser metatarsal overload. An allograft replacement of the metatarsal head has a very low predictability rating and is highly experimental.
---
changes. A Keller’s excision arthroplasty will further aggravate the lesser metatarsal overload. An allograft replacement of the metatarsal head has a very low predictability rating and is highly experimental.
---
Question 23High Yield
Varus malunion following talar neck fracture is best corrected by:
Explanation
The best way to address varus malunion in talar neck fractures and maintain motion is by talar neck osteotomy. However, there is a further possible risk of talar avascular necrosis with this procedure. The other acceptable treatment is a triple arthrodesis, although this eliminates all hindfoot motion.
Question 24High Yield
A tailorâs bunion is an abnormal prominence of the lateral aspect of the 5th metatarsal head. Similar to hallux valgus deformities, tailorâs bunions can be due to a widened intermetatarsal angle between the 4th and 5th metatarsal shafts. The normal 4-5 intermetatarsal angle is:
Explanation
4-5 intermetarsal angle in normal feet averages 6.2 degrees. Different authors believe an abnormally wide 4-5 intermetatarsal angle to be anything greater than 8°-9°.
Question 25High Yield
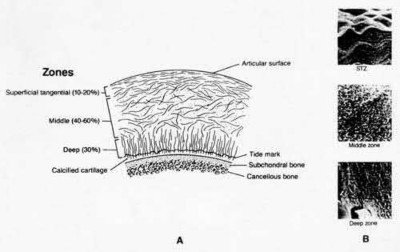
Which of the following resist articular cartilage compression and fluid flow:
Explanation
Type II collagen fibers resist tensile and shear deformation forces in the articular cartilage.
In contrast, the glycosaminoglycan aggregates resist articular cartilage compression and fluid flow.
In contrast, the glycosaminoglycan aggregates resist articular cartilage compression and fluid flow.
Question 26High Yield
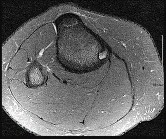
Figures 1 and 2 are the MR images of a 5-year-old who has had progressive right knee pain and swelling, fevers to 38.4°C, and refusal to bear weight for the past several days. Laboratory evaluation reveals hematocrit 29.9, WBC count 17.5 with 92% neutrophil on differential count, ESR 48, and CRP level of 8.2. What is the most appropriate course of action?

Explanation
■
The patient presents with acute hematogenous osteomyelitis. Leukocytosis with left shift, fevers, elevated acute phase reactant and large circumferential ring-enhancing subperiosteal and intraosseous abscess on MRI are diagnostic. Empiric antibiotics with close surveillance of clinical and laboratory response is appropriate if diagnosis is early in disease course when no drainable abscess is identified. However, the abscesses in this case must be surgically irrigated and debrided to decrease local infectious burden and enable effective antibiotic therapy. Arthroscopic lavage is not indicated, as there is no knee effusion on MRI. Febrile presentation, elevated infectious and inflammatory labs, and lack of soft-tissue mass on MRI rule against neoplasm / sarcoma thus staging biopsy, and hematology/oncology consultation are not warranted.
■
The patient presents with acute hematogenous osteomyelitis. Leukocytosis with left shift, fevers, elevated acute phase reactant and large circumferential ring-enhancing subperiosteal and intraosseous abscess on MRI are diagnostic. Empiric antibiotics with close surveillance of clinical and laboratory response is appropriate if diagnosis is early in disease course when no drainable abscess is identified. However, the abscesses in this case must be surgically irrigated and debrided to decrease local infectious burden and enable effective antibiotic therapy. Arthroscopic lavage is not indicated, as there is no knee effusion on MRI. Febrile presentation, elevated infectious and inflammatory labs, and lack of soft-tissue mass on MRI rule against neoplasm / sarcoma thus staging biopsy, and hematology/oncology consultation are not warranted.
Question 27High Yield
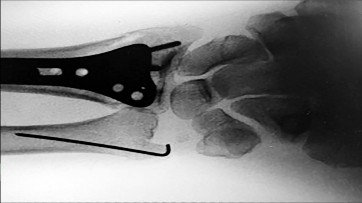
Figures 25a through 25c are the radiographs of a 65-year-old man who sustained a fracture from a fall. The patient elects open reduction and internal fixation of the distal radius. After plating the distal radius, the distal radioulnar joint (DRUJ) is examined and found to be unstable in both pronation and supination. What is the best next step?



Explanation
Figure 25
The initial radiographs show a comminuted displaced distal radius fracture, along with a displaced fracture of the base of the ulnar styloid. The displacement is best seen on the oblique view. After reduction and fixation of the radius, DRUJ stability should be assessed. The majority of scenarios that involve this injury pattern will not be unstable because of the oblique band of the interosseous ligament. When DRUJ instability is present after fixation of the radius, reduction and fixation of the ulnar styloid fracture is the best option to provide stability of the distal radioulnar joint (DRUJ) (Figure 25d). A study by Lawton and associates revealed that all distal radius fractures complicated by DRUJ instability were accompanied by an ulnar styloid fracture. A fracture at the ulnar styloid’s base and substantial displacement of an ulnar styloid fracture were found to increase risk for DRUJ instability. An ulnar styloid base fracture involves the insertion of the radioulnar ligaments and can cause DRUJ instability if displaced. If persistent instability is present after fixation of the ulnar styloid, DRUJ pinning is a reasonable option. Early ROM with splinting would not allow reduction or healing of the ulnar styloid and would result in persistent instability. Short-arm casting also would not allow stability of the DRUJ and would be a less reliable method with which to achieve healing of the ulnar styloid.
RECOMMENDED READINGS
33. May MM, Lawton JN, Blazar PE. Ulnar styloid fractures associated with distal radius fractures: incidence and implications for distal radioulnar joint instability. J Hand Surg Am. 2002 Nov;27(6):965-
[71/. PubMed PMID: 12457345.](http://www.ncbi.nlm.nih.gov/pubmed/12457345)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12457345)
34. [Sammer DM, Shah HM, Shauver MJ, Chung KC. The effect of ulnar styloid fractures on patient-rated outcomes after volar locking plating of distal radius fractures. J Hand Surg Am. 2009 Nov;34(9):1595-602. doi: 10.1016/j.jhsa.2009.05.017. PubMed PMID: 19896004. ](http://www.ncbi.nlm.nih.gov/pubmed/19896004)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19896004)
35. [Wysocki RW, Ruch DS. Ulnar styloid fracture with distal radius fracture. J Hand Surg Am. 2012 Mar;37(3):568-9. doi: 10.1016/j.jhsa.2011.08.035. Epub 2011 Oct 22. Review. PubMed PMID: 22018474. ](http://www.ncbi.nlm.nih.gov/pubmed/22018474)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22018474)
The initial radiographs show a comminuted displaced distal radius fracture, along with a displaced fracture of the base of the ulnar styloid. The displacement is best seen on the oblique view. After reduction and fixation of the radius, DRUJ stability should be assessed. The majority of scenarios that involve this injury pattern will not be unstable because of the oblique band of the interosseous ligament. When DRUJ instability is present after fixation of the radius, reduction and fixation of the ulnar styloid fracture is the best option to provide stability of the distal radioulnar joint (DRUJ) (Figure 25d). A study by Lawton and associates revealed that all distal radius fractures complicated by DRUJ instability were accompanied by an ulnar styloid fracture. A fracture at the ulnar styloid’s base and substantial displacement of an ulnar styloid fracture were found to increase risk for DRUJ instability. An ulnar styloid base fracture involves the insertion of the radioulnar ligaments and can cause DRUJ instability if displaced. If persistent instability is present after fixation of the ulnar styloid, DRUJ pinning is a reasonable option. Early ROM with splinting would not allow reduction or healing of the ulnar styloid and would result in persistent instability. Short-arm casting also would not allow stability of the DRUJ and would be a less reliable method with which to achieve healing of the ulnar styloid.
RECOMMENDED READINGS
33. May MM, Lawton JN, Blazar PE. Ulnar styloid fractures associated with distal radius fractures: incidence and implications for distal radioulnar joint instability. J Hand Surg Am. 2002 Nov;27(6):965-
[71/. PubMed PMID: 12457345.](http://www.ncbi.nlm.nih.gov/pubmed/12457345)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12457345)
34. [Sammer DM, Shah HM, Shauver MJ, Chung KC. The effect of ulnar styloid fractures on patient-rated outcomes after volar locking plating of distal radius fractures. J Hand Surg Am. 2009 Nov;34(9):1595-602. doi: 10.1016/j.jhsa.2009.05.017. PubMed PMID: 19896004. ](http://www.ncbi.nlm.nih.gov/pubmed/19896004)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19896004)
35. [Wysocki RW, Ruch DS. Ulnar styloid fracture with distal radius fracture. J Hand Surg Am. 2012 Mar;37(3):568-9. doi: 10.1016/j.jhsa.2011.08.035. Epub 2011 Oct 22. Review. PubMed PMID: 22018474. ](http://www.ncbi.nlm.nih.gov/pubmed/22018474)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22018474)
Question 28High Yield
A 3-year old child from an isolated mountain area is evaluated for multiple medical problems, including vomiting, loss of appetite, polyuria, and failure to thrive. History reveals the child was normal at birth. The parents, who appear healthy, are second cousins and have two other children who are normal. The parents state that they know of another family member who died at age 6 years after a similar medical history. Radiographs of the lower extremities show bowing of the long bones with cupping and widening of the physes. What is the most likely diagnosis?
Explanation
Hypophosphatemia-The patients who were symptomatic had obtundation,
hemolytic anemia, rhabdomyolysis, and hepatocellular injury that began during refeeding and resolved with treatment. The signs and symptoms, pathophysiology, and treatment of refeeding hypophosphatemia are reviewed.
Renal Osteodystrophy-Musculoskeletal complications in patients with chronic renal failure are common and may be related to the disease itself or to treatment. The altered metabolism in patients with chronic renal failure leads to renal osteodystrophy, which consists of osteomalacia and secondary hyperparathyroidism [1]. Erosive changes attributable to secondary hyperparathyroidism may be easily confused with rheumatoid arthritis, seronegative spondyloarthropathies, infection, or even malignancy.
Primary Hyperparathyroidism-Preferential involvement of cortical bone with apparent preservation of cancellous bone in primary hyperparathyroidism was confirmed by percutaneous bone biopsy. Over 80% of patients had a mean cortical width below the expected mean, whereas cancellous bone volume in over 80% of patients was above the expected mean.
Skeletal disease in primary hyperparathyroidism J Bone Miner Res 1989 Jun; 4(3):283-91
Nutritional vitamin D deficiency-Rickets, osteomalacia, and renal osteodystrophy are disorders of the mineralization of bone that result from a lack of available calcium, phosphorus, or both. The diseases that result from numerous mechanisms present with a symptom-sign-radiographic complex with such a high degree of stereotypy that laboratory investigation is often required to distinguish one form from another. The disorders in children, known as rickets, produce bowing and other deformities of the long bones and dwarfism. These disorders are principally related to the profound effect of the deficiency states on the epiphyseal plate; whereas the same disorders in adults produce an often severe osteopenia and pathologic fractures. Because of newer developments in our understanding of the factors affecting calcium-phosphorus
hemostasis and vitamin D metabolism, many of the children and Rickets, osteomalacia, and renal osteodystrophy.
hemolytic anemia, rhabdomyolysis, and hepatocellular injury that began during refeeding and resolved with treatment. The signs and symptoms, pathophysiology, and treatment of refeeding hypophosphatemia are reviewed.
Renal Osteodystrophy-Musculoskeletal complications in patients with chronic renal failure are common and may be related to the disease itself or to treatment. The altered metabolism in patients with chronic renal failure leads to renal osteodystrophy, which consists of osteomalacia and secondary hyperparathyroidism [1]. Erosive changes attributable to secondary hyperparathyroidism may be easily confused with rheumatoid arthritis, seronegative spondyloarthropathies, infection, or even malignancy.
Primary Hyperparathyroidism-Preferential involvement of cortical bone with apparent preservation of cancellous bone in primary hyperparathyroidism was confirmed by percutaneous bone biopsy. Over 80% of patients had a mean cortical width below the expected mean, whereas cancellous bone volume in over 80% of patients was above the expected mean.
Skeletal disease in primary hyperparathyroidism J Bone Miner Res 1989 Jun; 4(3):283-91
Nutritional vitamin D deficiency-Rickets, osteomalacia, and renal osteodystrophy are disorders of the mineralization of bone that result from a lack of available calcium, phosphorus, or both. The diseases that result from numerous mechanisms present with a symptom-sign-radiographic complex with such a high degree of stereotypy that laboratory investigation is often required to distinguish one form from another. The disorders in children, known as rickets, produce bowing and other deformities of the long bones and dwarfism. These disorders are principally related to the profound effect of the deficiency states on the epiphyseal plate; whereas the same disorders in adults produce an often severe osteopenia and pathologic fractures. Because of newer developments in our understanding of the factors affecting calcium-phosphorus
hemostasis and vitamin D metabolism, many of the children and Rickets, osteomalacia, and renal osteodystrophy.
Question 29High Yield
During fracture repair systemiCas well as local factors come into play. Which of the following is considered a systemiCfactor in fracture healing:
Explanation
The degree of vascular injury is considered a local factor in fracture healing. Other such factors include degree of local trauma, type of bone affected, degree of bone loss, degree of immoblization, infection and local pathologiCconditions. SystemiCfactors include age of the patient, hormone function, functional activity, nerve function and nutritional state
Question 30High Yield
Which of the following factors is associated with a decrease in the accuracy of measurement of congenital scoliosis:
Explanation
Measurement of congenital scoliosis has an intraobserver variation of 8°. Measurement accuracy decreases with decreased level of training, increased curve size, and decreased clarity of the endpoints. A coned and centered film would give better detail.
Question 31High Yield
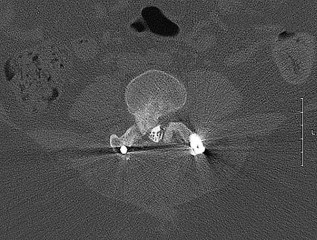
The above surgery was performed with recombinant human bone morphogenetic protein-2 (rhBMP-2). She reports immediate relief of her leg pain and is discharged home on postoperative day 2. The patient reports new-onset radicular pain and weakness in her leg 1 year later. Figures 22a and 22b are her postoperative CT myelogram images. What is the most likely cause of her pain?
22A B
22A B

Explanation
Transient thigh pain after lateral, transpsoas interbody fusion is common and generally lasts for less than 3 months. Transpsoas interbody fusion with slip reduction can result in indirect spinal decompression and often obviates the need for a laminectomy for most patients. Complications with this approach are comparable to those experienced with open surgery, but the hospital stay is generally shorter.
Use of BMP in interbody devices has also become common. The images above show heterotopic bone growth into the spinal canal causing nerve compression. This complication is more commonly encountered after posterior lumbar interbody fusions.
RECOMMENDED READINGS
Oliveira L, Marchi L, Coutinho E, Pimenta L. A radiographic assessment of the ability of the extreme lateral interbody fusion procedure to indirectly decompress the neural elements.
[Spine (Phila Pa 1976). 2010 Dec 15;35(26 Suppl):S331-7. doi: 10.1097/BRS.0b013e3182022db0. PubMed PMID: 21160397. ](http://www.ncbi.nlm.nih.gov/pubmed/21160397)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21160397) Cummock MD, Vanni S, Levi AD, Yu Y, Wang MY. An analysis of postoperative thigh symptoms after minimally invasive transpsoas lumbar interbody fusion. J Neurosurg Spine. 2011 Jul;15(1):11-8. doi: 10.3171/2011.2.SPINE10374. Epub 2011 Apr 8. PubMed PMID:
[21476801.](http://www.ncbi.nlm.nih.gov/pubmed/21476801)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21476801)
[Rodgers WB, Gerber EJ, Patterson J. Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Spine (Phila Pa 1976). 2011 Jan 1;36(1):26-32. doi: 10.1097/BRS.0b013e3181e1040a. PubMed PMID: 21192221. ](http://www.ncbi.nlm.nih.gov/pubmed/21192221)[View](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
[Wong DA, Kumar A, Jatana S, Ghiselli G, Wong K. Neurologic impairment from ectopic bone in the lumbar canal: a potential complication of off-label PLIF/TLIF use of bone morphogenetic protein-2 (BMP-2). Spine J. 2008 Nov-Dec;8(6):1011-8. Epub 2007 Nov 26. PubMed PMID: 18037352.](http://www.ncbi.nlm.nih.gov/pubmed/18037352)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18037352)
[Chen NF, Smith ZA, Stiner E, Armin S, Sheikh H, Khoo LT. Symptomatic ectopic bone formation after off-label use of recombinant human bone morphogenetic protein-2 in transforaminal lumbar interbody fusion. J Neurosurg Spine. 2010 Jan;12(1):40-6. doi: 10.3171/2009.4.SPINE0876. PubMed PMID: 20043763.](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)[View ](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)
Rouben D, Casnellie M, Ferguson M. Long-term durability of minimal invasive posterior transforaminal lumbar interbody fusion: a clinical and radiographic follow-up. J Spinal Disord Tech. 2011 Jul;24(5):288-96. doi:10.1097/BSD.0b013e3181f9a60a. PubMed PMID:
[20975594.](http://www.ncbi.nlm.nih.gov/pubmed/20975594)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20975594)
Use of BMP in interbody devices has also become common. The images above show heterotopic bone growth into the spinal canal causing nerve compression. This complication is more commonly encountered after posterior lumbar interbody fusions.
RECOMMENDED READINGS
Oliveira L, Marchi L, Coutinho E, Pimenta L. A radiographic assessment of the ability of the extreme lateral interbody fusion procedure to indirectly decompress the neural elements.
[Spine (Phila Pa 1976). 2010 Dec 15;35(26 Suppl):S331-7. doi: 10.1097/BRS.0b013e3182022db0. PubMed PMID: 21160397. ](http://www.ncbi.nlm.nih.gov/pubmed/21160397)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21160397) Cummock MD, Vanni S, Levi AD, Yu Y, Wang MY. An analysis of postoperative thigh symptoms after minimally invasive transpsoas lumbar interbody fusion. J Neurosurg Spine. 2011 Jul;15(1):11-8. doi: 10.3171/2011.2.SPINE10374. Epub 2011 Apr 8. PubMed PMID:
[21476801.](http://www.ncbi.nlm.nih.gov/pubmed/21476801)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21476801)
[Rodgers WB, Gerber EJ, Patterson J. Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Spine (Phila Pa 1976). 2011 Jan 1;36(1):26-32. doi: 10.1097/BRS.0b013e3181e1040a. PubMed PMID: 21192221. ](http://www.ncbi.nlm.nih.gov/pubmed/21192221)[View](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
[Wong DA, Kumar A, Jatana S, Ghiselli G, Wong K. Neurologic impairment from ectopic bone in the lumbar canal: a potential complication of off-label PLIF/TLIF use of bone morphogenetic protein-2 (BMP-2). Spine J. 2008 Nov-Dec;8(6):1011-8. Epub 2007 Nov 26. PubMed PMID: 18037352.](http://www.ncbi.nlm.nih.gov/pubmed/18037352)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18037352)
[Chen NF, Smith ZA, Stiner E, Armin S, Sheikh H, Khoo LT. Symptomatic ectopic bone formation after off-label use of recombinant human bone morphogenetic protein-2 in transforaminal lumbar interbody fusion. J Neurosurg Spine. 2010 Jan;12(1):40-6. doi: 10.3171/2009.4.SPINE0876. PubMed PMID: 20043763.](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)[View ](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)
Rouben D, Casnellie M, Ferguson M. Long-term durability of minimal invasive posterior transforaminal lumbar interbody fusion: a clinical and radiographic follow-up. J Spinal Disord Tech. 2011 Jul;24(5):288-96. doi:10.1097/BSD.0b013e3181f9a60a. PubMed PMID:
[20975594.](http://www.ncbi.nlm.nih.gov/pubmed/20975594)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20975594)
Question 32High Yield
An active 38-year-old male carpenter reports activity-related medial knee pain. Arthroscopy performed 3 years ago revealed a torn medial meniscus that was debrided and mild condylar changes of the medial femoral condyle and medial tibial plateau. Current standing radiographs reveal Ahlback stage II changes with mild medial femoral joint space narrowing and a 5-degree varus deformity. What is the best treatment option?
Explanation
The choice of high tibial osteotomy is appropriate to correct a deformity that has a very high risk of leading to progressive arthritis. It should be more important than either the arthroscopic method or the osteoarticular transplantation, though one may also consider these options. Prosthetic choices are limited for a young active male in favor of less “end stage” options.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and
function decline in knee osteoarthritis. JAMA 2001;286:188-195.
Wright JM, Crockett HC, Slawski DP, et al: High tibial osteotomy. J Am Acad Orthop Surg 2005-13 279289.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and
function decline in knee osteoarthritis. JAMA 2001;286:188-195.
Wright JM, Crockett HC, Slawski DP, et al: High tibial osteotomy. J Am Acad Orthop Surg 2005-13 279289.
Question 33High Yield
Time to soft-tissue coverage was not shown to have a statistically significant difference on the rate of infection in the level II study by Pollak et. al
A 38-year-old male suffers the injury shown in Figure A. During operative fixation, free osteoarticular fragments are encountered and reconstruction of these pieces is attempted. Postoperatively, which of the following will have the most beneficial effect on the healing potential of the surviving chondrocytes within these reconstructed articular segments?
A 38-year-old male suffers the injury shown in Figure A. During operative fixation, free osteoarticular fragments are encountered and reconstruction of these pieces is attempted. Postoperatively, which of the following will have the most beneficial effect on the healing potential of the surviving chondrocytes within these reconstructed articular segments?








































Explanation
Joint stability is critical for successful nonoperative management of posterior wall acetabular fractures. Recent evidence has established that dynamic fluoroscopic stress examination is the best method to determine joint stability in the setting of a posterior wall fracture. The obturator oblique view allows for the best evaluation of hip joint stability during examination for posterior wall fractures.
Grimshaw and Moed retrospectively reviewed the results of patients with posterior wall acetabular fractures managed nonoperatively after evaluation with dynamic fluoroscopic stress tests. At two year follow up, all had good to excellent Merle d’Aubigne clinical scores for hip function and no evidence of post-traumatic hip arthritis on AP pelvis radiographs.
Tornetta retrospectively reviewed his results managing patients with dynamic fluoroscopic stress examination for acetabular fractures which met radiographic nonoperative criteria. Good-to-excellent clinical results were seen in 91% of patients managed nonoperatively.
Tornetta reviewed management of acetabular fractures and Tornetta and Mostafavi separately reviewed management of hip dislocations. In both
articles, emphasis is placed on dynamic examination of posterior wall fractures as instability has been seen with fractures comprising as little as 15% of the posterior wall.
Illustration A demonstrates two fluoroscopic images from a dynamic stress exam of a patient with a posterior wall fracture. The image obtained in the obturator oblique view clearly demonstrates that the femoral head loses congruency with the acetabular dome.
Incorrect Answers:
Answers 1 & 2: Posterior wall fragment size less than 40% was historically used as an indirect measure of stability, however measurements of fragment size may be unreliable and instability has been seen with fractures much smaller than 40%
: A history of hip dislocation was thought to indicate a more unstable fracture. In the level IV study by Grimshaw and Moed, patients with an associated hip dislocation who were stable under stress exam had no significant difference in outcome with nonoperative management.
Answer 5: The iliac oblique view is used to evaluate the anterior wall and posterior column. Displacement or instability of the posterior wall would not be seen with this view
A 64-year-old woman is thrown off a horse, sustaining the injury shown in Figures A and B. She undergoes surgical fixation as seen in Figures C through E. What is the most commonly reported complication of this procedure?
1) Axillary nerve injury
2) Valgus migration of the fracture
3) Nonunion
4) Hardware failure
5) Screw penetration
The patient in the scenario has a 2-part proximal humerus fracture treated with a locking plate as seen in Figures A-E. The most common complication with the use of this implant is screw penetration. The terms screw cut out and penetration are often used interchangeably in the literature with cut out appearing more frequently in reports regarding intertrochanteric fractures.
Owsley et al retrospectively reviewed 53 proximal humerus fractures treated with locking plates and the same post-operative protocol. The most common complication was screw cut out or penetration, followed by varus displacement. They concluded that 3 and 4-part fractures in patients over 60 years have a higher incidence of failure.
Agudelo et al retrospectively reviewed 153 patients at a level-one trauma center treated with proximal humerus locking plates, investigating modes of failure for the implant. They determined that varus malreduction (head-shaft angle
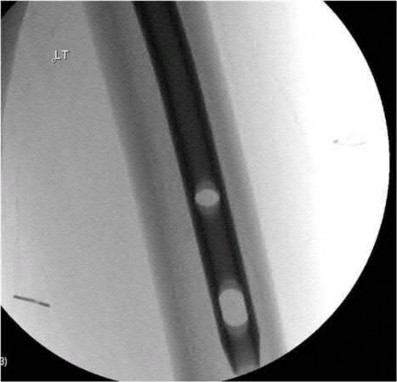
A 25-year-old male sustained a closed midshaft femur fracture following a motor vehicle collision. He is taken to the operating room for supine intramedullary nail fixation of the fracture. Figure A is a lateral fluoroscopic view of the distal femur taken just prior to distal interlocking screw placement. What change in position (with the Carm stationary) would be expected to produce a perfect lateral view of the interlocking hole?
1) Raising the leg
2) Lowering the leg
3) Internal (or external) rotation of the leg
4) Abduction (or adduction) of the leg
5) Fluoroscopic magnification
Interlocking of intramedullary nails using fluoroscopy requires attention to detail. A true lateral of the intramedullary nail is present when "perfect circle" views of interlocking holes are present. Once perfect circles are obtained, the drill can be advanced parallel to the fluoroscopic beam.
Knowledge of the implications of the appearance of the interlocking holes when "perfect circles" are not present can be helpful in minimizing the number of manipulations and fluoroscopic exposure. Widening of the interlocking hole in the proximal-distal direction (as is seen in this case) signifies the need for an adjustment in the abduction/adduction plane. Similarly, widening of the interlocking hole in the anterior-posterior plane signifies the need for an adjustment in the internal/external rotation plane (Answer 3).
Raising or lowering the leg (Answer A and B) should not have major effects of the appearance of the interlocking hole. Similarly, magnification of the C-arm (Answer D) will not affect the appearance. Internal/external rotation will result in widening in the anterior-posterior plane (as this dimension is currently adequate). Abduction or adduction will result in creating "perfect circles" (Answer 4). The position of the leg may hint to which of these is correct. If further widening occurs in the proximal-distal direction, the opposite maneuver will correct to the proper position.
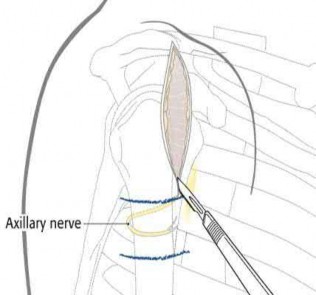
A 46-year-old male is involved in a motor vehicle accident and suffers a proximal humerus fracture. Operative treatment is recommended, and plate fixation is performed through an extended anterolateral acromial approach. Which of the following structures is at increased risk of injury using this surgical exposure compared to the deltopectoral approach?
1) Musculocutaneous nerve
2) Posterior humeral circumflex artery
3) Axillary nerve
4) Cephalic vein
5) Anterior humeral circumflex artery
The anterolateral acromial approach was developed to allow less invasive treatment of proximal humerus fractures. The plane of the avascular anterior
deltoid raphe is utilized, and the axillary nerve is at particular risk of injury and must be identified and protected. With this approach, anterior dissection near the critical blood supply is avoided, substantial muscle retraction is minimized, and the lateral plating zone is directly accessed.
Gardner et al evaluated 23 patients who had acute displaced fractures of the proximal humerus treated with the anterolateral acromial approach and either a locking plate or an intramedullary nail. At one year post-op, there were no axillary nerve deficits, and they found that the approach allowed direct access to the lateral fracture planes for fracture reduction and plate placement or safe nail and interlocking screw placement.
Gardner et al, in another study, performed cadveric dissection using the extended anterolateral acromial approach and measured multiple parameters regarding the axillary nerve. The nerve was predictably found approximately 35 mm from the prominence of the greater tuberosity.
Morgan et al performed a cadaveric study to describe the anatomic insertion point of the deltoid onto the proximal humerus. They found that the deltoid insertion is long and broad, and that placement of 4.5-mm plate would result in detaching 13.5 mm of its insertional footprint. This would leave half of the insertion still attached to the humerus.
Illustration A shows the position of the axillary nerve in relation to the approach.
Which of the following statements is true regarding brake travel time after surgical treatment of complex lower extremity trauma?
1) Brake travel time is significantly increased until 6 weeks after patient begins weight bearing
2) Return of normal brake travel time takes longer after long bone fracture compared to articular fractures
3) Normal brake travel time correlates with improved short musculoskeletal
functional assessment scores
4) Brake travel time is significantly reduced until 8 weeks after patient begins weight bearing
5) Brake travel time returns to normal when weight bearing begins
Brake travel time (BTT) has been shown to be significantly increased until 6 weeks after initiation of weight bearing in both long bone and articular fractures of the right lower extremity.
Egol et al used a computerized driving simulator to compare BTT in three groups of patients; 1)control group, 2)long bone lower extremity fracture group, 3)lower extremity articular fracture group. They concluded that BTT was significantly increased until 6 weeks after initiation of weight bearing in both long bone and articular fractures of the right lower extremity, and that short musculoskeletal functional assessment scores improved with respect to function and other indexes, but did not correlate with improvement in BTT.
An earlier study by Egol et al looked at total brake time as it related to distance traveled by the automobile before braking at 6, 9, and 12 weeks after operative fixation of a right ankle fracture. When compared with controls, braking time was shown to return to normal by 9 weeks post-operatively, and no significant association was found between the functional scores and this normalization.
Giddins et al provide a review of the literature, the law and the views of the major motor insurers related to driving after injury or operations.
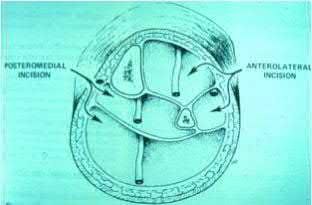
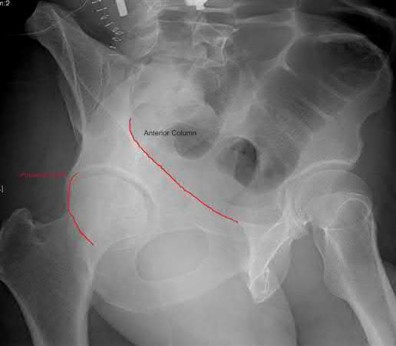
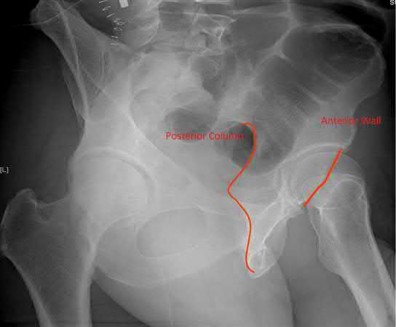
What acetabular component is best appreciated on an obturator oblique radiograph of the pelvis as seen in Figure A?
1) Ilioischial line
2) Posterior column
3) Posterior wall
4) Anterior wall
5) Sacroiliac joint
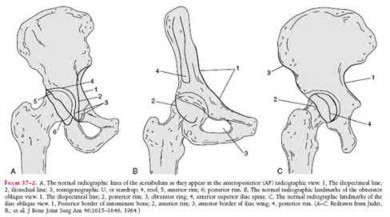
Letournel and Judet developed a schematic representation of the acetabulum as being contained within asymmetric long anterior and short posterior arms of an inverted “Y”.
On the bony pelvis, the ilioischial component becomes that posterior column and the iliopectineal line becomes the anterior column. The Judet-Letournel classification system is based on this scheme. By careful evaluation of landmarks on a standard AP pelvis radiograph, as well as on 45-degree oblique obturator and iliac views, the extent of injury can be determined accurately.
The AP view usually demonstrates the six fundamental landmarks relatively well as seen in illustration A. The obturator oblique view reveals additional information about the anterior column and posterior wall(see illustration A(B),
B). In an obturator oblique view the x-ray beam is centered on and almost perpendicular to the obturator foramen. The iliac oblique view visualizes the posterior column and anterior wall (illustration A(C), C). This view also shows the best detail of the iliac wing as the radiographic beam is roughly perpendicular to the iliac wing. Inclusion of the opposite hip is essential for evaluation of symmetrical contours that may have slight individual variations
and to evaluate the width of the normal articular cartilage in each view in a pelvic series (AP, Judet's) .
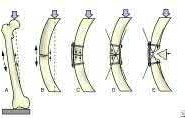
Which of the following fractures seen in Figures A through E would be amenable to fixation with a construct using tension band principles?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
In order for a fracture to be successfully treated with tension band principles the bone must be eccentrically loaded, the construct must be applied on the tensile side, and the opposite cortex must be able to withstand compressive
forces. Of the fractures seen in Figures A-E, the subtrochanteric fracture seen in Figure A best meets the criteria for stabilization according to tension band principles.
Kinast et al retrospectively compared their results with 95 degree blade plate fixation of subtrochanteric fractures utilizing the blade plate as a dynamic tension band. They performed either wide exposure of the fracture site with autogenous bone grafting according to AO technique at the time (group 1), or indirect reduction techniques without bone grafting the medial side as advocated by Mast et al (group 2). The authors found 100% union rates at six months with indirect reduction techniques without bone grafting (group 2), and emphasize the key concepts of preservation of the medial soft tissues and intraoperative pretensioning of the plate.
Illustration A demonstrates the principles of tension band fixation specifically applied to the femur. Within Illustration A, Figure C shows the correct application of a plate along the lateral cortex to resist tensile forces, along with incorrect application of the plate along the medial cortex (Figure D) or in a fracture pattern with an absent opposite cortex (Figure E). Illustration B shows an example of blade plate fixation of a subtrochanteric fracture.
Incorrect Answers:
Answer 2. Figure B demonstrates a comminuted proximal tibia fracture. Although the tibia is eccentrically loaded and an implant applied to anterior cortex could function as a tension band, the posterior comminution would lead to collapse.
Answer 3. Figure C demonstrates a comminuted distal humeral shaft fracture. Again,the comminution prevents application of a tension band construct Answer 4: Figure D shows a valgus impacted proximal humerus fracture.
Eccentric loading is absent for this type of fracture
Answer 5: Figure E demonstrates a comminuted olecranon fracture with extension distal to the coronoid process. Although tension band constructs are commonly used for olecranon fractures, the comminution and distal extension of this fracture would prevent application of a tension band.
Which of the following is an advantage of computer-assisted navigation used to place medullary nail interlocking screws compared to a freehand techinque?
1) Reduced fluoroscopy time
2) More reliable placement of interlocking screws through the nail
3) Reduced procedure time
4) Increased quality of fluoroscopic images
5) Improved accuracy of screw length
Computer-assisted navigation has been shown to reduce radiation exposure for surgeons when performing interlocking of medullary nails compared to freehand technique.
Ricci et al compared two fluoroscopic navigation tracking technologies, optical and electromagnetic versus standard freehand fluoroscopic targeting, in a standardized foam block model for placement of interlocking screws. They found that fluoroscopy time (seconds) and number of fluoroscopy images were significantly less when using the computer-guided systems than for freehand-unguided insertion. Average distance of pin placement from the target in the foam blocks was significantly greater for controls than for each of the navigated systems.
Suhm et al performed a prospective controlled clinical study to compare fluoroscopic guidance with fluoroscopy-based surgical navigation for distal locking of intramedullary implants. The surgical navigation group showed increased procedure time, but equivalent precision with reduced radiation exposure. There was no significant difference in the technical reliability
between both groups.
An 82-year-old nursing home resident falls onto his elbow while rising from a seated position. He has pain and swelling at the elbow without evidence of instability. His radiographs show a comminuted displaced olecranon fracture involving 25% of the articular surface with global osteopenia. Which of the following treatment options has a low risk of complications and a high likelihood of a functional elbow outcome?
1) Cast immobilization in 45 degrees of flexion for 8 weeks
2) Closed reduction and percutaneous pinning
3) ORIF with a tension band construct
4) ORIF with a locking plate
5) Cast immobilization in 90 degrees flexion
The patient in the scenario is a low-demand, elderly patient with a comminuted olecranon fracture. Recent studies have demonstrated good outcomes with
non-operative treatment of olecranon fractures in this patient population.
Hak (jaos'00) reviewed the treatment of olecranon fractures, recommending ORIF for displaced intra-articular fractures, either via tension band wiring or plate osteosynthesis based on fracture pattern and associated ligamentous disruption. For elderly, low-demand, osteoporotic patients, triceps advancement and fragment excision is an option in the case of severely comminuted, osteoporotic patients with a fracture involving
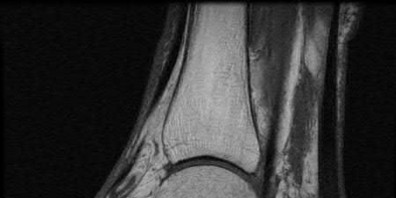
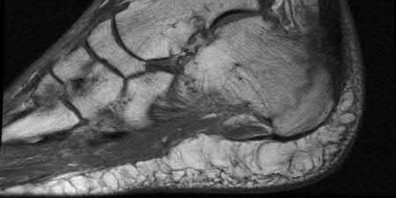
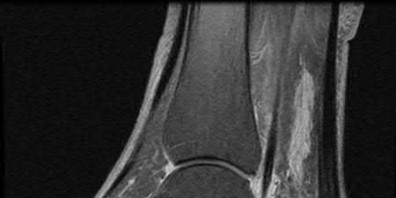
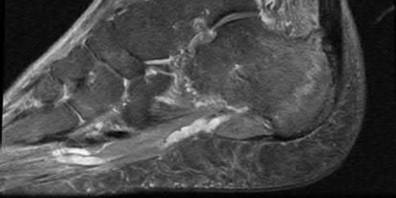
A 47-year-old male presents with a one month history of heel pain after starting marathon training. The heel is tender when squeezed. A foot radiograph is shown in Figure A, and an MRI is obtained which is shown in Figures B and C. What is the most likely diagnosis?
1) Osteomyelitis
2) Acute fracture
3) Subtalar arthritis
4) Achilles tendinitis
5) Stress fracture
The patients history, physical exam, and MRI findings are most consistent with the diagnosis of a stress fracture. Low signal on T1 and increased signal on T2-weighted images is the classic appearance of a stress fracture on magnetic resonance images. Usually the fracture appears as a linear signal band that arises from the cortex of the bone and extends perpendicular to the surface of the bone. Figures A and B show a linear area of enhancement in the posterior aspect of the calcaneus signifying a likely stress reaction from recent overtraining.
Boden et al review the pathogenesis and treatment of stress fractures. With regard to diagnosis, they state that it is primarily clinical, but imaging modalities such as plain radiography, scintigraphy, computed tomography, and magnetic resonance imaging may provide confirmation.
Gehrmann et al review stress fractures of the foot, and state that with regards to calcaneal stress injuries, MRI studies should be obtained for definitive diagnosis when radiographs are negative, and pain persists. With regards to
treatment, they state that these injuries usually heal with activity restrictions, heel-pad inserts, and protected weightbearing for a short period of time.
A 35-year-old right hand dominant man falls from a ladder and sustains the injury seen in Figure A. When discussing the risks and benefits of operative versus nonoperative treatment for his fracture, which of the following is true?
1) No difference in shoulder function
2) Higher risk of nonunion with operative management
3) Higher risk of symptomatic malunion or nonunion with nonoperative management
4) Earlier return to sport with nonoperative management
5) No difference in union rates
Historically, displaced midshaft clavicle fractures, as seen in Figure A, were managed nonoperatively. Recent literature has demonsrated improved outcomes with operative management of these fractures.
Khan et al review current concepts in the management of clavicle fractures. For displaced midshaft clavice fractures, operative treatment seems to result in improved patient and surgeon-based outcomes, decreased rates of malunion and nonunion, and shorter time to union.
Kim and McKee review recent evidence regarding the management of clavicle fractures. For midshaft clavicle fractures, the incidence of nonunion and symptomatic malunion with nonoperative management is higher than
previously believed. They state that risk factors include 100% displacement, comminution, increasing age and female gender.
Incorrect Answers
Answer 1. Recent randomized prospective trials have shown improved short term shoulder function with operative management of displaced midshaft clavicle fractures.
Answer 2. Nonunion rates of 7-15% have been shown with nonoperative management versus 2% with operative fixation
Answer 4. Earlier return to activities has been reported with operative management
Answer 5. As with answer 2, there is a significantly higher rate of nonunion with nonoperative management
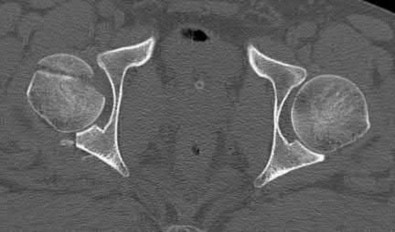
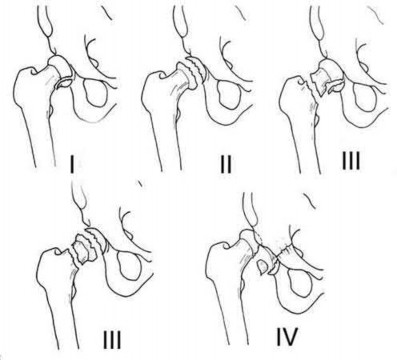
Assuming the images represent isolated injuries, which of the following Figures demonstrates a Pipkin II femoral head fracture?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Figure D represents a Pipkin II femoral head fracture, which is defined as a fracture which is superior to the fovea. Differentiation between Pipkin I and Pipkin II fractures can be important, as suprafoveal injuries often require surgical fixation. Illustration A demonstrates the Pipkin fracture types.
Droll et al review femoral head fracture evaluation and treatment. They discuss non-operative indications (typically reserved for Pipkin I injuries) which include an anatomic or near anatomic reduction (
A 20-year-old female presents following a motor vehicle collision with the injuries seen in Figures A and B. She was initially hypotensive and tachycardic however she now has stable vital signs following a 2 liter bolus of saline and 2 units of packed red blood cells. Which of the following would indicate that this patient has occult end-organ hypoperfusion and should be further resuscitated prior to definitive fixation?
1) Heart rate of 80 beats per minute
2) Systolic blood pressure of 120 mmHg
3) Base deficit of -1.8 mEq/L
4) Serum lactate of 5 mmol/Liter
5) Urine output of 40ml/hour
Figure A demonstrates an unstable pelvic fracture and subtrochanteric femur fracture and Figure B shows a scapular body and mutliple rib fractures. These high-energy fractures, along with the patient's initial hypotension and tacchycardia indicate a multiply injured patient in shock. Serum markers such as lactate (normal
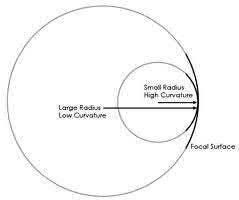
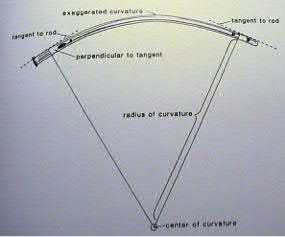
An 80-year-old female falls and sustains the fracture seen in Figure A. She is treated with an antegrade cephalomedullary nail. Which of the following led to the complication seen in Figure B?
1) Nail with a lesser radius of curvature
2) Nail with a greater radius of curvature
3) Piriformis entry portal
4) Trochanteric entry portal
5) Lateral decubitus patient position
The image in Figure A shows an unstable intertrochanteric fracture and the image in Figure B shows perforation of the anterior cortex of the femur by the intramedullary implant. This complication is due to a mismatch of the curvature of the nail with the anterior bow of the femur, and was likely caused by a nail of a greater radius of curvature (eg, straighter than the femur).
Egol et al measured the radius of curvature for 474 matched cadaveric femurs and found the average anterior radius of curvature to be 120cm (+/- 36cm). In contrast, the radii of curvature for the measured intramedullary nails ranged from 186cm to 300cm, demonstrating that the nails were straighter than the femurs. The authors advocate for a decreased radius of curvature (more curve) for intramedullary nails, especially larger diameter implants designed for fractures about the hip
Ostrum and Levy present a case series of 3 patients with subtrochanteric
fractures who had anterior penetration of the femoral cortex. They state that the mismatch in femoral bow between the bone and the implant is a contributing factor to distal femoral anterior cortex penetration in intramedullary nailing of subtrochanteric fractures.
Simonian et al present 4 iatrogenic femoral neck fractures that occured during a series of 315 femoral nails. The authors attempted to reproduce the iatrogenic fractures with cadaveric femurs and felt that the iatrogenic fractures may be due to a combination of a valgus femoral neck and impingement from the AO insertion jig used at the time.
Harper and Carson examined 14 cadaveric femurs and intramedullary implants at the time. Similar to Egol et al, they found a mismatch between the radius of curvature of the femurs and the intramedullary nails.
Illustration A shows the difference between a lesser and greater radius of curvature. Illustration B demonstrates how to calculate radius of curvature based on an implant with an exaggerated bow. Illustration C shows the anterior bow of a synthetic femoral model compared with several intramedullary implants.
Bridge plating of the olecranon is MOST appropriate in which of the following clinical scenarios?
1) Fixation of an olecranon osteotomy used for distal humerus surgery in a 24-year-old male
2) Simple transverse olecranon fracture in 33-year-old female
3) Comminuted olecranon fracture in 45-year-old male
4) Severely comminuted proximal olecranon fracture in an osteoporotic 91-year-old female
5) Aphophyseal elbow fracture in 6-year-old male
Bridge plating is most appropriately used for fixation of comminuted fractures which are not able to be fixed anatomically. Of the choices listed above, this would be most appropriate in a comminuted fracture in a 45-year-old male. In contrast, literature shows that severely comminuted, osteoporotic low-demand elderly are best treated with olecranon fracture excision and triceps advancement when possible.
Bailey et al looked at the outcome of plate fixation of olecranon fractures. They concluded that plate fixation is effective for displaced olecranon fractures and leads to good functional outcome. There were low incidence of complications, although 20% did have removal of hardware due to irritation.
Hak et al reviewed the fixation options for olecranon fractures. In their review, they state that comminuted olecranon fractures can be treated by limited-contact dynamic-compression plates. They also supported the use of supplemental bone graft to support comminuted depressed articular fragments. Fragment excision and triceps advancement is appropriate in selected cases in which open reduction seems unlikely to be successful, such as in osteoporotic elderly patients with severely comminuted fractures.
A 75-year-old ambulatory male who lives independently presents with the fracture shown in Figure A. Which of the following is true regarding timing of surgical fixation and post-operative mortality?
1) 30 day mortality is decreased if surgery is delayed 4-7 days
2) 1 year mortality is increased if surgery is delayed greater than 4 days
3) Delay of surgery due to treatment of acute medical comorbidities has no effect on post-operative mortality rates
4) 90 day mortality rate is decreased if surgery is delayed greater than 7 days
5) Timing of surgical fixation has no statistically significant affect on postoperative mortality
Figure A shows a displaced femoral neck fracture.
Moran et al studied 2660 elderly patients who underwent surgical treatment of a hip fracture to determine whether a delay in surgery affects postoperative mortality. The 30-day mortality for patients for whom the surgery had been delayed for more than 4 days was 10.7%, compared to 7.3% in those delayed 1-4 days. The group delayed >4 days also had significantly increased mortality at 90 days and 1 year. Patients who had been admitted with an acute medical comorbidity that required treatment prior to the surgery had a 30-day mortality of 17%, which was nearly 2.5 times greater than that for patients without and acute comorbidity. The study concluded that patients with medical comorbidities that delayed surgery had 2.5 times the risk of death within 30 days after the surgery compared with patients without comorbidities. Mortality was not increased when the surgery was delayed up to four days for patients who were otherwise fit for hip fracture surgery, however, a delay of more than four days significantly increased mortality.
Healy et al examined 120 patients who underwent surgical treatment of 186 displaced femoral neck fractures with either internal fixation, hemiarthroplasty, or total hip arthroplasty. Arthroplasty was associated with more independent living, and was more cost-effective than internal fixation. There was no difference in rates of reoperation or mortality, but arthroplasty produced a longer interval to reoperation or death. They concluded that total hip arthroplasty was the best treatment for displaced fractures of the femoral neck in their series.
Illustration A shows a scoring system developed by Rogmark et al to aid in decision making.
A 35-year-old male suffers an anterior column acetabular fracture during a motor vehicle collision, and subsequently undergoes percutaneous acetabular fixation. Intraoperatively, fluoroscopy is positioned to obtain an obturator oblique-inlet view while placing a supraacetabular screw. Which of the following screw relationships is best evaluated with this view?
1) Intraarticular penetration of the screw
2) Position of the screw cephalad to the sciatic notch
3) Screw starting point at the anterior inferior iliac spine
4) Screw starting point at the gluteal pillar
5) Screw position between the inner and outer tables of the ilium
The obturator oblique-inlet view, as seen in Illustration A, best demonstrates the position of a supra-acetabular screw or pin relative to the tables of the ilium.
Starr et al review their initial results and technique of closed or limited open reduction and percutaneous fixation of acetabular fractures. They defined two groups of patients who may benefit from this technique; elderly patients with multiple comorbidities to facilitate early mobilization and restore hip morphology, and young patients with elementary fracture patterns and multiple associated injuries.
Starr et al describe their operative technique and outcomes for a case series of 3 patients using percutaneous acetabular fixation to augment open reduction of acetabular fractures. The authors state that, for placement of an anterior colum ramus screw, an iliac oblique-inlet (not obturator oblique-inlet) will ensure that the screw is within the medullary canal of the ramus and does not exit anterior or posterior.
Gardner and Nork describe a technique for placement of a large femoral distractor in the supra-acetabular region to compress displaced posterior pelvic ring injuries. They note that the obturator oblique-inlet view is necessary to view the entire length of the pin as well as to ensure that pin remains in bone.
Incorrect answers:
Answer 1: Relationshiop of the screw to the acetabulum is best evaluated with the obturator oblique-outlet view as well as the iliac oblique view
Answer 2: The iliac oblique view is used to ensure the trajectory of the screw is superior to the sciatic notch
Answer 3: The Obturator oblique-outlet view, otherwise known as the "teepee" or "tear drop" view, is used to identify the start for supra-acetabular implant placement
Answer 4: The gluteal pillar is not utilized as a start point when placing supraacetabular fixation, and the obturator oblique-inlet view would not be ideal to visualize this region of the pelvis
A 74-year-old man falls, sustaining the injury shown in Figures A through C. In surgical planning, what is the best surgical approach to treat this injury?
1) Kocher-Langenbeck
2) Watson-Jones
3) Extended iliofemoral
4) Ilioinguinal
5) Hardinge
Figures A through C depict and AP pelvis and Judet views of a T-type fracture of the right acetabulum. The ilioinguinal approach provides access to the anterior wall and anterior column for fracture fixation, in addition to allowing fixation of the nondisplaced posterior transverse fracture line. The lateral femoral cutaneous nerve (LFCN) is at risk in the superficial part of the dissection. Another option for the approach would be the modified Stoppa, which would also allow excellent access to the anterior column as well as the internal aspect of the iliac wing and quadrilateral plate.
Illustration A shows the five basic and 5 associated acetabular fractures. Incorrect Answers:
Answer 1. Kocher-Langenbeck: access for posterior wall and column fractures
Answer 2. Watson-Jones: anterolateral approach best for the hip, not the anterior column of the acetabulum.
Answer 3. Extended iliofemoral: visualization for both column fractures Answer 5. Hardinge approach: lateral approach for THA
A 28-year-old female is struck by a motor vehicle while crossing the street and suffers the injury seen in Figure A. What technical adjunct could have prevented the operative complication seen in Figure B?
1) Nail of a lesser radius of curvature
2) Nail with a more distal Herzog curve
3) Application of an anterior unicortical plate
4) Nailing while in a hyperflexed position
5) A more distal and medial nail entry site
The patient has a proximal tibia fracture that has been malreduced in procurvatum with anterior translation of the proximal fragment as seen in Figures A and B. Intramedullary nailing of proximal tibia fractures may result in malalignment such as valgus, procurvatum and anterior translation of the proximal fragment.Techniques such as anterior unicortical plating have been described to maintain reduction while placing a locked intramedullary implant.
Nork et al retrospectively review their results using several different intraoperative adjuncts to maintain reduction while nailing proximal tibia fractures including anterior unicortical plates and femoral distractors. They report that, despite high rates of segmental comminution (59.5%) and open fractures (35.1%), acceptable alignment and primary union were achieved in more than 90% of patients.
Dunbar et al describe their technique for application of a provisional unicortical plate through the traumatic wound to maintain reduction during intramedullary nailing of Gustilo-Anderson Type III open tibia fractures. The authors advocate that further soft tissue stripping during plate placement should be avoided, and found excellent results in terms of coronal and sagittal plane alignment for fractures treated with this technique.
Matthews et al review their experience with unicortical plating to maintain reduction during intramedullary nailing of tibia fractures. Similar to the other referenced studies, the authors found the technique assisted with maintaining reduction intraoperatively.
Illustrations A and B demonstrate maintenance of reduction of a proximal tibia fracture using an anterior unicortical plate as a reduction tool during intramedullary nailing.
Incorrect Answers:
Answer 1: Nail of a lesser radius of curvature. Unlike femoral nails, tibial nails are straight to match the coronal/sagittal axis of the tibia and therefore a nail with a lesser radius of curvature (more bend) would not match the anatomy and likely lead to malalignment
Answer 2: Nail with a more distal Herzog curve. The proximal bend for tibial IM nails, known as the Herzog curve, may cause malalignment in proximal tibia fractures due to a phenomenon known as the "wedge effect". Nails with more distal Herzog curves have been implicated in anterior translation of the proximal fragment.
Answer 4: Nailing in a hyperflexed position would cause extension of the proximal fragment due to tension on the extensor mechanism
Answer 5: A more distal and medial entry site would likely lead to further deformity and possible nail cut out through the anterior cortex. A more proximal and lateral entry site is preferred for nailing proximal tibia fractures
A 32-year-old male sustains an APC-III pelvic ring disruption after a motor vehicle collision. Which of the following imaging techniques best describes the correct utilization of intraoperative flouroscopy for percutaneous iliosacral screw placement across S1?
1) Inlet view helps best guide superior-inferior orientation
2) AP pelvis best guides anterior-posterior screw orientation
3) AP pelvis best guides superior-inferior screw orientation
4) Outlet view best guides anterior-posterior screw orientation
5) Outlet view best guides superior-inferior screw orientation
The outlet view best guides superior-inferior screw orientation during percutaneous S1 screw placement. This is due to the relative forward flexion of the sacrum and pelvis due to pelvic incidence. A lateral sacral view and an inlet pelvis view would best guide anterior-posterior screw orientation.
Routt et al did a review of percutaneous techniques of pelvic surgery. Although anterior pelvic external fixation remains the most common form of percutaneous pelvic fixation, iliosacral screws have the advantage of stabilizing pelvic disruptions directly while diminishing operative blood loss and operative time. They stress importance of a thorough knowledge of pelvic osseous anatomy, injury patterns, deformities, and their fluoroscopic correlations for surgical success.
Routt et al also looked at the complications that can result from percutaneous iliosacral screw placement. Complications ranged from inability for adequate imaging due to patient obesity, L5 nerve root injuries, fixation failure, and sacral nonunions. They support quality triplanar fluoroscopic imaging during iliosacral screw insertions to help accurately reduce injured posterior pelvic rings.
Illustration A is an example of an outlet view image status post anterior pelvic ring plating and percutaneous iliosacral screw. This outlet view allows superior S1 neural foramen visualization to help guide screw placement and avoid nerve injury.
Which of the following methods accurately describes the measurement of tip-apex-distance as it relates to placement of a lag screw in the femoral head?
1) Summation of the distance between the end of the screw and the apex of the femoral head on AP and lateral radiographs
2) Distance from the acetabular teardrop to the tip of the screw on an AP radiograph of the hip
3) Multiplication of the distance between the end of the screw and the apex of the femoral head on AP and lateral radiographs
4) Distance from the center of the lesser trochanter to the tip of the screw on an AP hip radiograph
5) Summation of the distance between the tip of the greater trochanter and end of the screw on AP and lateral hip radiographs
Tip-apex distance (TAD) as it relates to a lag screw in the femoral head is the summation of the distance between the end of the screw and the apex of the femoral head on AP and lateral radiographs, corrected for radiographic magnification of the image. This is shown in Illustration A.
TAD is a useful intraoperative indicator of deep and central placement of the lag screw in the femoral head, regardless of whether a nail or a plate is chosen to fix a fracture. A TAD of 25mm as well as with increasing fracture severity. They concluded that TAD is a valuable consideration for intramedullary devices as well.
Illustrations B and C show a lag screw with an excessive TAD, and subsequent failure of fixation.
Incorrect Answers:
Answers 2-5: TAD is defined as the sum of the distance between the end of the lag screw and the apex of the femoral head on the AP and lateral radiographs, corrected for radiographic magnification of the image.
A 25-year-old man presents one year after undergoing open reduction and internal fixation of the fracture seen in Figure A. Current radiographs demonstrate a united fracture with no evidence of ostenecrosis, subtalar or tibiotalar arthritis. Physical exam is notable for ambulation on the lateral border of the right foot with hindfoot varus, midfoot supination and diminished subtalar motion compared with the contralateral side. Which of the following is an option for reconstruction of this patient's deformity?
1) Total ankle arthroplasty
2) Lateral calcaneus closing wedge osteotomy
3) Calcaneal neck opening wedge osteotomy
4) Talar neck opening medial wedge osteotomy
5) Triple arthrodesis
The most common position of talar neck malunion is varus and this deformity can lock the subtalar and transverse tarsal joints leading to diminished motion and ultimately subtalar arthrosis. Medial opening wedge osteotomy of the talar neck has been described to restore the anatomy of the talus and preserve hindfoot motion.
Daniels et al performed a biomechanical study of hindfoot motion following medial osteotomy and varus malalignment of the talar neck. The authors found a direct correlation between the degree of varus malalignment and diminished forefoot and subtalar motion, and caution against compressive fixation of the medial talus in the presence of comminution.
Monroe and Manoli present a case report of talar neck malunion and describe their technique for osteotomy of the talar neck with insertion of a tricortical iliac crest bone graft to correct the deformity. They found a significant improvement in the AOFAS ankle-hindfoot score and no evidence of
osteonecrosis with follow-up greater than 4 years.
Huang and Cheng retrospectively review their results with anatomic reconstruction of the talar neck in 9 patients who presented a minimum of four weeks after the initial injury with a malreduced or neglected talar neck fracture. They found favorable outcomes with delayed reconstruction as determined by the AOFAS ankle-hindfoot score at an average follow up of 53 months, however note that six patients subsequently developed radiographic hindfoot arthrosis.
Figure A demonstrates a lateral radiograph of a comminuted talar neck fracture with subluxation of the subtalar joint.
Incorrect Answers:
Answer 1: Total ankle arthroplasty is reserved for patients with end-stage tibiotalar arthritis. This patient has an intact and functional tibiotalar joint Answer 2: Lateral calcaneus closing wedge osteotomy would correct some hindfoot varus, however would not address the talar neck deformity leading to diminished motion.
Answer 3: Calcaneal neck opening wedge osteotomy would exacerbate the patient's deformity
Answer 5: Triple arthrodesis would be not be a viable option in a patient with a preserved tibiotalar and subtalar joint.
Which of the following descriptions is true regarding APC-II (anterior-posterior compression) pelvic injuries as classified by Young and Burgess?
1) Pubic symphysis diastasis, intact anterior sacroiliac ligaments, intact sacrotuberous ligament, intact posterior sacroiliac ligaments
2) Pubic symphysis diastasis, torn anterior sacroiliac ligaments, intact sacrotuberous ligament intact posterior sacroiliac ligaments
3) Pubic symphysis diastasis, intact anterior sacroiliac ligaments, torn sacrotuberous ligament, intact posterior sacroiliac ligaments
4) Pubic symphysis diastasis, torn anterior sacroiliac ligaments, torn sacrotuberous ligament, intact posterior sacroiliac ligaments
5) Pubic symphysis diastasis, intact anterior sacroiliac ligaments, torn sacrotuberous ligament, torn posterior sacroiliac ligaments
APC II injuries are unstable injuries and occur as a result of high-energy trauma. Anatomic structures which are injured or torn include the pubic symphysis, anterior iliosacral ligaments, and the sacrotuberous ligaments. The posterior sacroiliac ligaments are spared in APC-II injuries, and differentiate an APC-II injury from an APC-III injury, in which the posterior ligaments are also torn.
Burgess et al review the classifications of pelvic ring disruptions and their association with mortality. They concluded that APC injuries required more blood replacement and were related to death more often than lateral compression, vertical shear, or combined mechanism pelvic injuries.
Tile studied the anatomy of anterior to posterior pelvic ring injuries. Although the anterior structures, the symphysis pubis and the pubic rami, contribute to 40% to the stiffness of the pelvis, clinical and biomechanical studies have shown that the posterior sacroiliac complex is more important to pelvic-ring stability. The posterior sacroiliac ligamentous complex is more important to pelvic-ring stability than the anterior structures and therefore, the classification of pelvic fractures is based on the stability of the posterior lesion.
Illustration A shows the APC classification.
Which of the following deformities is most likely to occur with dynamic hip screw fixation of unstable left sided standard obliquity hip fractures?
1) Posterior spike displacement of the proximal fragment
2) Anterior spike displacement of the proximal fragment
3) Lateral displacement of the proximal fragment relative to the distal fragment
4) Shortening of the proximal fragment relative to the distal fragment
5) Medial displacement of the proximal fragment in relation to the distal fragment
Left-sided unstable intertrochanteric hip fractures are at increased risk of malreduction compared to unstable right-sided fractures fixed with dynamic hip screws. In left-sided fractures the rotational torque imparted to the proximal head and neck fragment can cause loss of reduction leading to potential failures of fixation. With these left sided injuries, the rotational torque can cause an anterior spike, whereas with right-sided injuries the rotational torque causes compression and reduction of the fracture. In addition, if a nail is used for these injuries and the proximal fracture fragment is not being held by the nail itself, this phenomenon can be seen as well.
Mohan et al conducted a study to assess the effect of clockwise rotational torque onto the fracture configuration in unstable and stable intertrochanteric fractures fixed with a dynamic hip screw construct. They found that 11 out of 30 unstable fractures showed an anterior spike (flexion malreduction) in left-sided fixations due to clockwise torque. This malreduction was not present in right-sided or stable fractures.
Illustrations A and B are images from Mohan et al's study showing the rotational affect on the fracture with placement of a dynamic hip screw.
A 45-year-old male sustains a proximal third tibia fracture as an isolated injury and elects to undergo operative treatment with intramedullary nailing. Post-operative radiographs show excessive procurvatum deformity. Which of the following operative techniques would have helped to best avoid the procurvatum deformity?
1) Tibial nailing with increased knee flexion
2) Lateral blocking screw in the proximal fragment
3) Medial blocking screw in the proximal fragment
4) Anterior blocking screw in the proximal fragment
5) Posterior blocking screw in the proximal fragment
Posterior blocking screws in the proximal tibial segement help to avoid tibial procurvatum deformity and malunion. Proximal third tibia fractures are often times difficult to reduce anatomically due to the tendency for both valgus and flexion deformity at the fracture site. The posterior blocking screw helps to eliminate the tendency for the nail to be too posterior and cause the fracture to flex. Blocking screws should be placed on the concavity of the deformity to minimize the procurvatum and valgus deformities of this fracture pattern.
Krettek et al looked at the importance of using blocking screws during intramedullary nailing of metaphyseal fractures using small diameter nails. They found less procurvatum deformity and malunions associated with using of blocking screws and found no complication with their utilization.
Ricci et al reviewed fractures of the proximal third of the tibial shaft treated with intramedullary nails and blocking screws. Their results supported that blocking screws were effective in maintaining alignment of fractures of the proximal third of the tibial shaft treated by intramedullary nailing.
Hiesterman et al review different reduction techniques to avoid malalignment, including the use of a proper starting point and insertion angle, blocking screws, unicortical plates, and a universal distractor.
Illustration A shows a radiograph utilizing posterior proximal and distal blocking screws to prevent procurvatum deformity.
Incorrect Answers:
Grimshaw and Moed retrospectively reviewed the results of patients with posterior wall acetabular fractures managed nonoperatively after evaluation with dynamic fluoroscopic stress tests. At two year follow up, all had good to excellent Merle d’Aubigne clinical scores for hip function and no evidence of post-traumatic hip arthritis on AP pelvis radiographs.
Tornetta retrospectively reviewed his results managing patients with dynamic fluoroscopic stress examination for acetabular fractures which met radiographic nonoperative criteria. Good-to-excellent clinical results were seen in 91% of patients managed nonoperatively.
Tornetta reviewed management of acetabular fractures and Tornetta and Mostafavi separately reviewed management of hip dislocations. In both
articles, emphasis is placed on dynamic examination of posterior wall fractures as instability has been seen with fractures comprising as little as 15% of the posterior wall.
Illustration A demonstrates two fluoroscopic images from a dynamic stress exam of a patient with a posterior wall fracture. The image obtained in the obturator oblique view clearly demonstrates that the femoral head loses congruency with the acetabular dome.
Incorrect Answers:
Answers 1 & 2: Posterior wall fragment size less than 40% was historically used as an indirect measure of stability, however measurements of fragment size may be unreliable and instability has been seen with fractures much smaller than 40%
: A history of hip dislocation was thought to indicate a more unstable fracture. In the level IV study by Grimshaw and Moed, patients with an associated hip dislocation who were stable under stress exam had no significant difference in outcome with nonoperative management.
Answer 5: The iliac oblique view is used to evaluate the anterior wall and posterior column. Displacement or instability of the posterior wall would not be seen with this view
A 64-year-old woman is thrown off a horse, sustaining the injury shown in Figures A and B. She undergoes surgical fixation as seen in Figures C through E. What is the most commonly reported complication of this procedure?
1) Axillary nerve injury
2) Valgus migration of the fracture
3) Nonunion
4) Hardware failure
5) Screw penetration
The patient in the scenario has a 2-part proximal humerus fracture treated with a locking plate as seen in Figures A-E. The most common complication with the use of this implant is screw penetration. The terms screw cut out and penetration are often used interchangeably in the literature with cut out appearing more frequently in reports regarding intertrochanteric fractures.
Owsley et al retrospectively reviewed 53 proximal humerus fractures treated with locking plates and the same post-operative protocol. The most common complication was screw cut out or penetration, followed by varus displacement. They concluded that 3 and 4-part fractures in patients over 60 years have a higher incidence of failure.
Agudelo et al retrospectively reviewed 153 patients at a level-one trauma center treated with proximal humerus locking plates, investigating modes of failure for the implant. They determined that varus malreduction (head-shaft angle
A 25-year-old male sustained a closed midshaft femur fracture following a motor vehicle collision. He is taken to the operating room for supine intramedullary nail fixation of the fracture. Figure A is a lateral fluoroscopic view of the distal femur taken just prior to distal interlocking screw placement. What change in position (with the Carm stationary) would be expected to produce a perfect lateral view of the interlocking hole?
1) Raising the leg
2) Lowering the leg
3) Internal (or external) rotation of the leg
4) Abduction (or adduction) of the leg
5) Fluoroscopic magnification
Interlocking of intramedullary nails using fluoroscopy requires attention to detail. A true lateral of the intramedullary nail is present when "perfect circle" views of interlocking holes are present. Once perfect circles are obtained, the drill can be advanced parallel to the fluoroscopic beam.
Knowledge of the implications of the appearance of the interlocking holes when "perfect circles" are not present can be helpful in minimizing the number of manipulations and fluoroscopic exposure. Widening of the interlocking hole in the proximal-distal direction (as is seen in this case) signifies the need for an adjustment in the abduction/adduction plane. Similarly, widening of the interlocking hole in the anterior-posterior plane signifies the need for an adjustment in the internal/external rotation plane (Answer 3).
Raising or lowering the leg (Answer A and B) should not have major effects of the appearance of the interlocking hole. Similarly, magnification of the C-arm (Answer D) will not affect the appearance. Internal/external rotation will result in widening in the anterior-posterior plane (as this dimension is currently adequate). Abduction or adduction will result in creating "perfect circles" (Answer 4). The position of the leg may hint to which of these is correct. If further widening occurs in the proximal-distal direction, the opposite maneuver will correct to the proper position.
A 46-year-old male is involved in a motor vehicle accident and suffers a proximal humerus fracture. Operative treatment is recommended, and plate fixation is performed through an extended anterolateral acromial approach. Which of the following structures is at increased risk of injury using this surgical exposure compared to the deltopectoral approach?
1) Musculocutaneous nerve
2) Posterior humeral circumflex artery
3) Axillary nerve
4) Cephalic vein
5) Anterior humeral circumflex artery
The anterolateral acromial approach was developed to allow less invasive treatment of proximal humerus fractures. The plane of the avascular anterior
deltoid raphe is utilized, and the axillary nerve is at particular risk of injury and must be identified and protected. With this approach, anterior dissection near the critical blood supply is avoided, substantial muscle retraction is minimized, and the lateral plating zone is directly accessed.
Gardner et al evaluated 23 patients who had acute displaced fractures of the proximal humerus treated with the anterolateral acromial approach and either a locking plate or an intramedullary nail. At one year post-op, there were no axillary nerve deficits, and they found that the approach allowed direct access to the lateral fracture planes for fracture reduction and plate placement or safe nail and interlocking screw placement.
Gardner et al, in another study, performed cadveric dissection using the extended anterolateral acromial approach and measured multiple parameters regarding the axillary nerve. The nerve was predictably found approximately 35 mm from the prominence of the greater tuberosity.
Morgan et al performed a cadaveric study to describe the anatomic insertion point of the deltoid onto the proximal humerus. They found that the deltoid insertion is long and broad, and that placement of 4.5-mm plate would result in detaching 13.5 mm of its insertional footprint. This would leave half of the insertion still attached to the humerus.
Illustration A shows the position of the axillary nerve in relation to the approach.
Which of the following statements is true regarding brake travel time after surgical treatment of complex lower extremity trauma?
1) Brake travel time is significantly increased until 6 weeks after patient begins weight bearing
2) Return of normal brake travel time takes longer after long bone fracture compared to articular fractures
3) Normal brake travel time correlates with improved short musculoskeletal
functional assessment scores
4) Brake travel time is significantly reduced until 8 weeks after patient begins weight bearing
5) Brake travel time returns to normal when weight bearing begins
Brake travel time (BTT) has been shown to be significantly increased until 6 weeks after initiation of weight bearing in both long bone and articular fractures of the right lower extremity.
Egol et al used a computerized driving simulator to compare BTT in three groups of patients; 1)control group, 2)long bone lower extremity fracture group, 3)lower extremity articular fracture group. They concluded that BTT was significantly increased until 6 weeks after initiation of weight bearing in both long bone and articular fractures of the right lower extremity, and that short musculoskeletal functional assessment scores improved with respect to function and other indexes, but did not correlate with improvement in BTT.
An earlier study by Egol et al looked at total brake time as it related to distance traveled by the automobile before braking at 6, 9, and 12 weeks after operative fixation of a right ankle fracture. When compared with controls, braking time was shown to return to normal by 9 weeks post-operatively, and no significant association was found between the functional scores and this normalization.
Giddins et al provide a review of the literature, the law and the views of the major motor insurers related to driving after injury or operations.
What acetabular component is best appreciated on an obturator oblique radiograph of the pelvis as seen in Figure A?
1) Ilioischial line
2) Posterior column
3) Posterior wall
4) Anterior wall
5) Sacroiliac joint
Letournel and Judet developed a schematic representation of the acetabulum as being contained within asymmetric long anterior and short posterior arms of an inverted “Y”.
On the bony pelvis, the ilioischial component becomes that posterior column and the iliopectineal line becomes the anterior column. The Judet-Letournel classification system is based on this scheme. By careful evaluation of landmarks on a standard AP pelvis radiograph, as well as on 45-degree oblique obturator and iliac views, the extent of injury can be determined accurately.
The AP view usually demonstrates the six fundamental landmarks relatively well as seen in illustration A. The obturator oblique view reveals additional information about the anterior column and posterior wall(see illustration A(B),
B). In an obturator oblique view the x-ray beam is centered on and almost perpendicular to the obturator foramen. The iliac oblique view visualizes the posterior column and anterior wall (illustration A(C), C). This view also shows the best detail of the iliac wing as the radiographic beam is roughly perpendicular to the iliac wing. Inclusion of the opposite hip is essential for evaluation of symmetrical contours that may have slight individual variations
and to evaluate the width of the normal articular cartilage in each view in a pelvic series (AP, Judet's) .
Which of the following fractures seen in Figures A through E would be amenable to fixation with a construct using tension band principles?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
In order for a fracture to be successfully treated with tension band principles the bone must be eccentrically loaded, the construct must be applied on the tensile side, and the opposite cortex must be able to withstand compressive
forces. Of the fractures seen in Figures A-E, the subtrochanteric fracture seen in Figure A best meets the criteria for stabilization according to tension band principles.
Kinast et al retrospectively compared their results with 95 degree blade plate fixation of subtrochanteric fractures utilizing the blade plate as a dynamic tension band. They performed either wide exposure of the fracture site with autogenous bone grafting according to AO technique at the time (group 1), or indirect reduction techniques without bone grafting the medial side as advocated by Mast et al (group 2). The authors found 100% union rates at six months with indirect reduction techniques without bone grafting (group 2), and emphasize the key concepts of preservation of the medial soft tissues and intraoperative pretensioning of the plate.
Illustration A demonstrates the principles of tension band fixation specifically applied to the femur. Within Illustration A, Figure C shows the correct application of a plate along the lateral cortex to resist tensile forces, along with incorrect application of the plate along the medial cortex (Figure D) or in a fracture pattern with an absent opposite cortex (Figure E). Illustration B shows an example of blade plate fixation of a subtrochanteric fracture.
Incorrect Answers:
Answer 2. Figure B demonstrates a comminuted proximal tibia fracture. Although the tibia is eccentrically loaded and an implant applied to anterior cortex could function as a tension band, the posterior comminution would lead to collapse.
Answer 3. Figure C demonstrates a comminuted distal humeral shaft fracture. Again,the comminution prevents application of a tension band construct Answer 4: Figure D shows a valgus impacted proximal humerus fracture.
Eccentric loading is absent for this type of fracture
Answer 5: Figure E demonstrates a comminuted olecranon fracture with extension distal to the coronoid process. Although tension band constructs are commonly used for olecranon fractures, the comminution and distal extension of this fracture would prevent application of a tension band.
Which of the following is an advantage of computer-assisted navigation used to place medullary nail interlocking screws compared to a freehand techinque?
1) Reduced fluoroscopy time
2) More reliable placement of interlocking screws through the nail
3) Reduced procedure time
4) Increased quality of fluoroscopic images
5) Improved accuracy of screw length
Computer-assisted navigation has been shown to reduce radiation exposure for surgeons when performing interlocking of medullary nails compared to freehand technique.
Ricci et al compared two fluoroscopic navigation tracking technologies, optical and electromagnetic versus standard freehand fluoroscopic targeting, in a standardized foam block model for placement of interlocking screws. They found that fluoroscopy time (seconds) and number of fluoroscopy images were significantly less when using the computer-guided systems than for freehand-unguided insertion. Average distance of pin placement from the target in the foam blocks was significantly greater for controls than for each of the navigated systems.
Suhm et al performed a prospective controlled clinical study to compare fluoroscopic guidance with fluoroscopy-based surgical navigation for distal locking of intramedullary implants. The surgical navigation group showed increased procedure time, but equivalent precision with reduced radiation exposure. There was no significant difference in the technical reliability
between both groups.
An 82-year-old nursing home resident falls onto his elbow while rising from a seated position. He has pain and swelling at the elbow without evidence of instability. His radiographs show a comminuted displaced olecranon fracture involving 25% of the articular surface with global osteopenia. Which of the following treatment options has a low risk of complications and a high likelihood of a functional elbow outcome?
1) Cast immobilization in 45 degrees of flexion for 8 weeks
2) Closed reduction and percutaneous pinning
3) ORIF with a tension band construct
4) ORIF with a locking plate
5) Cast immobilization in 90 degrees flexion
The patient in the scenario is a low-demand, elderly patient with a comminuted olecranon fracture. Recent studies have demonstrated good outcomes with
non-operative treatment of olecranon fractures in this patient population.
Hak (jaos'00) reviewed the treatment of olecranon fractures, recommending ORIF for displaced intra-articular fractures, either via tension band wiring or plate osteosynthesis based on fracture pattern and associated ligamentous disruption. For elderly, low-demand, osteoporotic patients, triceps advancement and fragment excision is an option in the case of severely comminuted, osteoporotic patients with a fracture involving
A 47-year-old male presents with a one month history of heel pain after starting marathon training. The heel is tender when squeezed. A foot radiograph is shown in Figure A, and an MRI is obtained which is shown in Figures B and C. What is the most likely diagnosis?
1) Osteomyelitis
2) Acute fracture
3) Subtalar arthritis
4) Achilles tendinitis
5) Stress fracture
The patients history, physical exam, and MRI findings are most consistent with the diagnosis of a stress fracture. Low signal on T1 and increased signal on T2-weighted images is the classic appearance of a stress fracture on magnetic resonance images. Usually the fracture appears as a linear signal band that arises from the cortex of the bone and extends perpendicular to the surface of the bone. Figures A and B show a linear area of enhancement in the posterior aspect of the calcaneus signifying a likely stress reaction from recent overtraining.
Boden et al review the pathogenesis and treatment of stress fractures. With regard to diagnosis, they state that it is primarily clinical, but imaging modalities such as plain radiography, scintigraphy, computed tomography, and magnetic resonance imaging may provide confirmation.
Gehrmann et al review stress fractures of the foot, and state that with regards to calcaneal stress injuries, MRI studies should be obtained for definitive diagnosis when radiographs are negative, and pain persists. With regards to
treatment, they state that these injuries usually heal with activity restrictions, heel-pad inserts, and protected weightbearing for a short period of time.
A 35-year-old right hand dominant man falls from a ladder and sustains the injury seen in Figure A. When discussing the risks and benefits of operative versus nonoperative treatment for his fracture, which of the following is true?
1) No difference in shoulder function
2) Higher risk of nonunion with operative management
3) Higher risk of symptomatic malunion or nonunion with nonoperative management
4) Earlier return to sport with nonoperative management
5) No difference in union rates
Historically, displaced midshaft clavicle fractures, as seen in Figure A, were managed nonoperatively. Recent literature has demonsrated improved outcomes with operative management of these fractures.
Khan et al review current concepts in the management of clavicle fractures. For displaced midshaft clavice fractures, operative treatment seems to result in improved patient and surgeon-based outcomes, decreased rates of malunion and nonunion, and shorter time to union.
Kim and McKee review recent evidence regarding the management of clavicle fractures. For midshaft clavicle fractures, the incidence of nonunion and symptomatic malunion with nonoperative management is higher than
previously believed. They state that risk factors include 100% displacement, comminution, increasing age and female gender.
Incorrect Answers
Answer 1. Recent randomized prospective trials have shown improved short term shoulder function with operative management of displaced midshaft clavicle fractures.
Answer 2. Nonunion rates of 7-15% have been shown with nonoperative management versus 2% with operative fixation
Answer 4. Earlier return to activities has been reported with operative management
Answer 5. As with answer 2, there is a significantly higher rate of nonunion with nonoperative management
Assuming the images represent isolated injuries, which of the following Figures demonstrates a Pipkin II femoral head fracture?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Figure D represents a Pipkin II femoral head fracture, which is defined as a fracture which is superior to the fovea. Differentiation between Pipkin I and Pipkin II fractures can be important, as suprafoveal injuries often require surgical fixation. Illustration A demonstrates the Pipkin fracture types.
Droll et al review femoral head fracture evaluation and treatment. They discuss non-operative indications (typically reserved for Pipkin I injuries) which include an anatomic or near anatomic reduction (
A 20-year-old female presents following a motor vehicle collision with the injuries seen in Figures A and B. She was initially hypotensive and tachycardic however she now has stable vital signs following a 2 liter bolus of saline and 2 units of packed red blood cells. Which of the following would indicate that this patient has occult end-organ hypoperfusion and should be further resuscitated prior to definitive fixation?
1) Heart rate of 80 beats per minute
2) Systolic blood pressure of 120 mmHg
3) Base deficit of -1.8 mEq/L
4) Serum lactate of 5 mmol/Liter
5) Urine output of 40ml/hour
Figure A demonstrates an unstable pelvic fracture and subtrochanteric femur fracture and Figure B shows a scapular body and mutliple rib fractures. These high-energy fractures, along with the patient's initial hypotension and tacchycardia indicate a multiply injured patient in shock. Serum markers such as lactate (normal
An 80-year-old female falls and sustains the fracture seen in Figure A. She is treated with an antegrade cephalomedullary nail. Which of the following led to the complication seen in Figure B?
1) Nail with a lesser radius of curvature
2) Nail with a greater radius of curvature
3) Piriformis entry portal
4) Trochanteric entry portal
5) Lateral decubitus patient position
The image in Figure A shows an unstable intertrochanteric fracture and the image in Figure B shows perforation of the anterior cortex of the femur by the intramedullary implant. This complication is due to a mismatch of the curvature of the nail with the anterior bow of the femur, and was likely caused by a nail of a greater radius of curvature (eg, straighter than the femur).
Egol et al measured the radius of curvature for 474 matched cadaveric femurs and found the average anterior radius of curvature to be 120cm (+/- 36cm). In contrast, the radii of curvature for the measured intramedullary nails ranged from 186cm to 300cm, demonstrating that the nails were straighter than the femurs. The authors advocate for a decreased radius of curvature (more curve) for intramedullary nails, especially larger diameter implants designed for fractures about the hip
Ostrum and Levy present a case series of 3 patients with subtrochanteric
fractures who had anterior penetration of the femoral cortex. They state that the mismatch in femoral bow between the bone and the implant is a contributing factor to distal femoral anterior cortex penetration in intramedullary nailing of subtrochanteric fractures.
Simonian et al present 4 iatrogenic femoral neck fractures that occured during a series of 315 femoral nails. The authors attempted to reproduce the iatrogenic fractures with cadaveric femurs and felt that the iatrogenic fractures may be due to a combination of a valgus femoral neck and impingement from the AO insertion jig used at the time.
Harper and Carson examined 14 cadaveric femurs and intramedullary implants at the time. Similar to Egol et al, they found a mismatch between the radius of curvature of the femurs and the intramedullary nails.
Illustration A shows the difference between a lesser and greater radius of curvature. Illustration B demonstrates how to calculate radius of curvature based on an implant with an exaggerated bow. Illustration C shows the anterior bow of a synthetic femoral model compared with several intramedullary implants.
Bridge plating of the olecranon is MOST appropriate in which of the following clinical scenarios?
1) Fixation of an olecranon osteotomy used for distal humerus surgery in a 24-year-old male
2) Simple transverse olecranon fracture in 33-year-old female
3) Comminuted olecranon fracture in 45-year-old male
4) Severely comminuted proximal olecranon fracture in an osteoporotic 91-year-old female
5) Aphophyseal elbow fracture in 6-year-old male
Bridge plating is most appropriately used for fixation of comminuted fractures which are not able to be fixed anatomically. Of the choices listed above, this would be most appropriate in a comminuted fracture in a 45-year-old male. In contrast, literature shows that severely comminuted, osteoporotic low-demand elderly are best treated with olecranon fracture excision and triceps advancement when possible.
Bailey et al looked at the outcome of plate fixation of olecranon fractures. They concluded that plate fixation is effective for displaced olecranon fractures and leads to good functional outcome. There were low incidence of complications, although 20% did have removal of hardware due to irritation.
Hak et al reviewed the fixation options for olecranon fractures. In their review, they state that comminuted olecranon fractures can be treated by limited-contact dynamic-compression plates. They also supported the use of supplemental bone graft to support comminuted depressed articular fragments. Fragment excision and triceps advancement is appropriate in selected cases in which open reduction seems unlikely to be successful, such as in osteoporotic elderly patients with severely comminuted fractures.
A 75-year-old ambulatory male who lives independently presents with the fracture shown in Figure A. Which of the following is true regarding timing of surgical fixation and post-operative mortality?
1) 30 day mortality is decreased if surgery is delayed 4-7 days
2) 1 year mortality is increased if surgery is delayed greater than 4 days
3) Delay of surgery due to treatment of acute medical comorbidities has no effect on post-operative mortality rates
4) 90 day mortality rate is decreased if surgery is delayed greater than 7 days
5) Timing of surgical fixation has no statistically significant affect on postoperative mortality
Figure A shows a displaced femoral neck fracture.
Moran et al studied 2660 elderly patients who underwent surgical treatment of a hip fracture to determine whether a delay in surgery affects postoperative mortality. The 30-day mortality for patients for whom the surgery had been delayed for more than 4 days was 10.7%, compared to 7.3% in those delayed 1-4 days. The group delayed >4 days also had significantly increased mortality at 90 days and 1 year. Patients who had been admitted with an acute medical comorbidity that required treatment prior to the surgery had a 30-day mortality of 17%, which was nearly 2.5 times greater than that for patients without and acute comorbidity. The study concluded that patients with medical comorbidities that delayed surgery had 2.5 times the risk of death within 30 days after the surgery compared with patients without comorbidities. Mortality was not increased when the surgery was delayed up to four days for patients who were otherwise fit for hip fracture surgery, however, a delay of more than four days significantly increased mortality.
Healy et al examined 120 patients who underwent surgical treatment of 186 displaced femoral neck fractures with either internal fixation, hemiarthroplasty, or total hip arthroplasty. Arthroplasty was associated with more independent living, and was more cost-effective than internal fixation. There was no difference in rates of reoperation or mortality, but arthroplasty produced a longer interval to reoperation or death. They concluded that total hip arthroplasty was the best treatment for displaced fractures of the femoral neck in their series.
Illustration A shows a scoring system developed by Rogmark et al to aid in decision making.
A 35-year-old male suffers an anterior column acetabular fracture during a motor vehicle collision, and subsequently undergoes percutaneous acetabular fixation. Intraoperatively, fluoroscopy is positioned to obtain an obturator oblique-inlet view while placing a supraacetabular screw. Which of the following screw relationships is best evaluated with this view?
1) Intraarticular penetration of the screw
2) Position of the screw cephalad to the sciatic notch
3) Screw starting point at the anterior inferior iliac spine
4) Screw starting point at the gluteal pillar
5) Screw position between the inner and outer tables of the ilium
The obturator oblique-inlet view, as seen in Illustration A, best demonstrates the position of a supra-acetabular screw or pin relative to the tables of the ilium.
Starr et al review their initial results and technique of closed or limited open reduction and percutaneous fixation of acetabular fractures. They defined two groups of patients who may benefit from this technique; elderly patients with multiple comorbidities to facilitate early mobilization and restore hip morphology, and young patients with elementary fracture patterns and multiple associated injuries.
Starr et al describe their operative technique and outcomes for a case series of 3 patients using percutaneous acetabular fixation to augment open reduction of acetabular fractures. The authors state that, for placement of an anterior colum ramus screw, an iliac oblique-inlet (not obturator oblique-inlet) will ensure that the screw is within the medullary canal of the ramus and does not exit anterior or posterior.
Gardner and Nork describe a technique for placement of a large femoral distractor in the supra-acetabular region to compress displaced posterior pelvic ring injuries. They note that the obturator oblique-inlet view is necessary to view the entire length of the pin as well as to ensure that pin remains in bone.
Incorrect answers:
Answer 1: Relationshiop of the screw to the acetabulum is best evaluated with the obturator oblique-outlet view as well as the iliac oblique view
Answer 2: The iliac oblique view is used to ensure the trajectory of the screw is superior to the sciatic notch
Answer 3: The Obturator oblique-outlet view, otherwise known as the "teepee" or "tear drop" view, is used to identify the start for supra-acetabular implant placement
Answer 4: The gluteal pillar is not utilized as a start point when placing supraacetabular fixation, and the obturator oblique-inlet view would not be ideal to visualize this region of the pelvis
A 74-year-old man falls, sustaining the injury shown in Figures A through C. In surgical planning, what is the best surgical approach to treat this injury?
1) Kocher-Langenbeck
2) Watson-Jones
3) Extended iliofemoral
4) Ilioinguinal
5) Hardinge
Figures A through C depict and AP pelvis and Judet views of a T-type fracture of the right acetabulum. The ilioinguinal approach provides access to the anterior wall and anterior column for fracture fixation, in addition to allowing fixation of the nondisplaced posterior transverse fracture line. The lateral femoral cutaneous nerve (LFCN) is at risk in the superficial part of the dissection. Another option for the approach would be the modified Stoppa, which would also allow excellent access to the anterior column as well as the internal aspect of the iliac wing and quadrilateral plate.
Illustration A shows the five basic and 5 associated acetabular fractures. Incorrect Answers:
Answer 1. Kocher-Langenbeck: access for posterior wall and column fractures
Answer 2. Watson-Jones: anterolateral approach best for the hip, not the anterior column of the acetabulum.
Answer 3. Extended iliofemoral: visualization for both column fractures Answer 5. Hardinge approach: lateral approach for THA
A 28-year-old female is struck by a motor vehicle while crossing the street and suffers the injury seen in Figure A. What technical adjunct could have prevented the operative complication seen in Figure B?
1) Nail of a lesser radius of curvature
2) Nail with a more distal Herzog curve
3) Application of an anterior unicortical plate
4) Nailing while in a hyperflexed position
5) A more distal and medial nail entry site
The patient has a proximal tibia fracture that has been malreduced in procurvatum with anterior translation of the proximal fragment as seen in Figures A and B. Intramedullary nailing of proximal tibia fractures may result in malalignment such as valgus, procurvatum and anterior translation of the proximal fragment.Techniques such as anterior unicortical plating have been described to maintain reduction while placing a locked intramedullary implant.
Nork et al retrospectively review their results using several different intraoperative adjuncts to maintain reduction while nailing proximal tibia fractures including anterior unicortical plates and femoral distractors. They report that, despite high rates of segmental comminution (59.5%) and open fractures (35.1%), acceptable alignment and primary union were achieved in more than 90% of patients.
Dunbar et al describe their technique for application of a provisional unicortical plate through the traumatic wound to maintain reduction during intramedullary nailing of Gustilo-Anderson Type III open tibia fractures. The authors advocate that further soft tissue stripping during plate placement should be avoided, and found excellent results in terms of coronal and sagittal plane alignment for fractures treated with this technique.
Matthews et al review their experience with unicortical plating to maintain reduction during intramedullary nailing of tibia fractures. Similar to the other referenced studies, the authors found the technique assisted with maintaining reduction intraoperatively.
Illustrations A and B demonstrate maintenance of reduction of a proximal tibia fracture using an anterior unicortical plate as a reduction tool during intramedullary nailing.
Incorrect Answers:
Answer 1: Nail of a lesser radius of curvature. Unlike femoral nails, tibial nails are straight to match the coronal/sagittal axis of the tibia and therefore a nail with a lesser radius of curvature (more bend) would not match the anatomy and likely lead to malalignment
Answer 2: Nail with a more distal Herzog curve. The proximal bend for tibial IM nails, known as the Herzog curve, may cause malalignment in proximal tibia fractures due to a phenomenon known as the "wedge effect". Nails with more distal Herzog curves have been implicated in anterior translation of the proximal fragment.
Answer 4: Nailing in a hyperflexed position would cause extension of the proximal fragment due to tension on the extensor mechanism
Answer 5: A more distal and medial entry site would likely lead to further deformity and possible nail cut out through the anterior cortex. A more proximal and lateral entry site is preferred for nailing proximal tibia fractures
A 32-year-old male sustains an APC-III pelvic ring disruption after a motor vehicle collision. Which of the following imaging techniques best describes the correct utilization of intraoperative flouroscopy for percutaneous iliosacral screw placement across S1?
1) Inlet view helps best guide superior-inferior orientation
2) AP pelvis best guides anterior-posterior screw orientation
3) AP pelvis best guides superior-inferior screw orientation
4) Outlet view best guides anterior-posterior screw orientation
5) Outlet view best guides superior-inferior screw orientation
The outlet view best guides superior-inferior screw orientation during percutaneous S1 screw placement. This is due to the relative forward flexion of the sacrum and pelvis due to pelvic incidence. A lateral sacral view and an inlet pelvis view would best guide anterior-posterior screw orientation.
Routt et al did a review of percutaneous techniques of pelvic surgery. Although anterior pelvic external fixation remains the most common form of percutaneous pelvic fixation, iliosacral screws have the advantage of stabilizing pelvic disruptions directly while diminishing operative blood loss and operative time. They stress importance of a thorough knowledge of pelvic osseous anatomy, injury patterns, deformities, and their fluoroscopic correlations for surgical success.
Routt et al also looked at the complications that can result from percutaneous iliosacral screw placement. Complications ranged from inability for adequate imaging due to patient obesity, L5 nerve root injuries, fixation failure, and sacral nonunions. They support quality triplanar fluoroscopic imaging during iliosacral screw insertions to help accurately reduce injured posterior pelvic rings.
Illustration A is an example of an outlet view image status post anterior pelvic ring plating and percutaneous iliosacral screw. This outlet view allows superior S1 neural foramen visualization to help guide screw placement and avoid nerve injury.
Which of the following methods accurately describes the measurement of tip-apex-distance as it relates to placement of a lag screw in the femoral head?
1) Summation of the distance between the end of the screw and the apex of the femoral head on AP and lateral radiographs
2) Distance from the acetabular teardrop to the tip of the screw on an AP radiograph of the hip
3) Multiplication of the distance between the end of the screw and the apex of the femoral head on AP and lateral radiographs
4) Distance from the center of the lesser trochanter to the tip of the screw on an AP hip radiograph
5) Summation of the distance between the tip of the greater trochanter and end of the screw on AP and lateral hip radiographs
Tip-apex distance (TAD) as it relates to a lag screw in the femoral head is the summation of the distance between the end of the screw and the apex of the femoral head on AP and lateral radiographs, corrected for radiographic magnification of the image. This is shown in Illustration A.
TAD is a useful intraoperative indicator of deep and central placement of the lag screw in the femoral head, regardless of whether a nail or a plate is chosen to fix a fracture. A TAD of 25mm as well as with increasing fracture severity. They concluded that TAD is a valuable consideration for intramedullary devices as well.
Illustrations B and C show a lag screw with an excessive TAD, and subsequent failure of fixation.
Incorrect Answers:
Answers 2-5: TAD is defined as the sum of the distance between the end of the lag screw and the apex of the femoral head on the AP and lateral radiographs, corrected for radiographic magnification of the image.
A 25-year-old man presents one year after undergoing open reduction and internal fixation of the fracture seen in Figure A. Current radiographs demonstrate a united fracture with no evidence of ostenecrosis, subtalar or tibiotalar arthritis. Physical exam is notable for ambulation on the lateral border of the right foot with hindfoot varus, midfoot supination and diminished subtalar motion compared with the contralateral side. Which of the following is an option for reconstruction of this patient's deformity?
1) Total ankle arthroplasty
2) Lateral calcaneus closing wedge osteotomy
3) Calcaneal neck opening wedge osteotomy
4) Talar neck opening medial wedge osteotomy
5) Triple arthrodesis
The most common position of talar neck malunion is varus and this deformity can lock the subtalar and transverse tarsal joints leading to diminished motion and ultimately subtalar arthrosis. Medial opening wedge osteotomy of the talar neck has been described to restore the anatomy of the talus and preserve hindfoot motion.
Daniels et al performed a biomechanical study of hindfoot motion following medial osteotomy and varus malalignment of the talar neck. The authors found a direct correlation between the degree of varus malalignment and diminished forefoot and subtalar motion, and caution against compressive fixation of the medial talus in the presence of comminution.
Monroe and Manoli present a case report of talar neck malunion and describe their technique for osteotomy of the talar neck with insertion of a tricortical iliac crest bone graft to correct the deformity. They found a significant improvement in the AOFAS ankle-hindfoot score and no evidence of
osteonecrosis with follow-up greater than 4 years.
Huang and Cheng retrospectively review their results with anatomic reconstruction of the talar neck in 9 patients who presented a minimum of four weeks after the initial injury with a malreduced or neglected talar neck fracture. They found favorable outcomes with delayed reconstruction as determined by the AOFAS ankle-hindfoot score at an average follow up of 53 months, however note that six patients subsequently developed radiographic hindfoot arthrosis.
Figure A demonstrates a lateral radiograph of a comminuted talar neck fracture with subluxation of the subtalar joint.
Incorrect Answers:
Answer 1: Total ankle arthroplasty is reserved for patients with end-stage tibiotalar arthritis. This patient has an intact and functional tibiotalar joint Answer 2: Lateral calcaneus closing wedge osteotomy would correct some hindfoot varus, however would not address the talar neck deformity leading to diminished motion.
Answer 3: Calcaneal neck opening wedge osteotomy would exacerbate the patient's deformity
Answer 5: Triple arthrodesis would be not be a viable option in a patient with a preserved tibiotalar and subtalar joint.
Which of the following descriptions is true regarding APC-II (anterior-posterior compression) pelvic injuries as classified by Young and Burgess?
1) Pubic symphysis diastasis, intact anterior sacroiliac ligaments, intact sacrotuberous ligament, intact posterior sacroiliac ligaments
2) Pubic symphysis diastasis, torn anterior sacroiliac ligaments, intact sacrotuberous ligament intact posterior sacroiliac ligaments
3) Pubic symphysis diastasis, intact anterior sacroiliac ligaments, torn sacrotuberous ligament, intact posterior sacroiliac ligaments
4) Pubic symphysis diastasis, torn anterior sacroiliac ligaments, torn sacrotuberous ligament, intact posterior sacroiliac ligaments
5) Pubic symphysis diastasis, intact anterior sacroiliac ligaments, torn sacrotuberous ligament, torn posterior sacroiliac ligaments
APC II injuries are unstable injuries and occur as a result of high-energy trauma. Anatomic structures which are injured or torn include the pubic symphysis, anterior iliosacral ligaments, and the sacrotuberous ligaments. The posterior sacroiliac ligaments are spared in APC-II injuries, and differentiate an APC-II injury from an APC-III injury, in which the posterior ligaments are also torn.
Burgess et al review the classifications of pelvic ring disruptions and their association with mortality. They concluded that APC injuries required more blood replacement and were related to death more often than lateral compression, vertical shear, or combined mechanism pelvic injuries.
Tile studied the anatomy of anterior to posterior pelvic ring injuries. Although the anterior structures, the symphysis pubis and the pubic rami, contribute to 40% to the stiffness of the pelvis, clinical and biomechanical studies have shown that the posterior sacroiliac complex is more important to pelvic-ring stability. The posterior sacroiliac ligamentous complex is more important to pelvic-ring stability than the anterior structures and therefore, the classification of pelvic fractures is based on the stability of the posterior lesion.
Illustration A shows the APC classification.
Which of the following deformities is most likely to occur with dynamic hip screw fixation of unstable left sided standard obliquity hip fractures?
1) Posterior spike displacement of the proximal fragment
2) Anterior spike displacement of the proximal fragment
3) Lateral displacement of the proximal fragment relative to the distal fragment
4) Shortening of the proximal fragment relative to the distal fragment
5) Medial displacement of the proximal fragment in relation to the distal fragment
Left-sided unstable intertrochanteric hip fractures are at increased risk of malreduction compared to unstable right-sided fractures fixed with dynamic hip screws. In left-sided fractures the rotational torque imparted to the proximal head and neck fragment can cause loss of reduction leading to potential failures of fixation. With these left sided injuries, the rotational torque can cause an anterior spike, whereas with right-sided injuries the rotational torque causes compression and reduction of the fracture. In addition, if a nail is used for these injuries and the proximal fracture fragment is not being held by the nail itself, this phenomenon can be seen as well.
Mohan et al conducted a study to assess the effect of clockwise rotational torque onto the fracture configuration in unstable and stable intertrochanteric fractures fixed with a dynamic hip screw construct. They found that 11 out of 30 unstable fractures showed an anterior spike (flexion malreduction) in left-sided fixations due to clockwise torque. This malreduction was not present in right-sided or stable fractures.
Illustrations A and B are images from Mohan et al's study showing the rotational affect on the fracture with placement of a dynamic hip screw.
A 45-year-old male sustains a proximal third tibia fracture as an isolated injury and elects to undergo operative treatment with intramedullary nailing. Post-operative radiographs show excessive procurvatum deformity. Which of the following operative techniques would have helped to best avoid the procurvatum deformity?
1) Tibial nailing with increased knee flexion
2) Lateral blocking screw in the proximal fragment
3) Medial blocking screw in the proximal fragment
4) Anterior blocking screw in the proximal fragment
5) Posterior blocking screw in the proximal fragment
Posterior blocking screws in the proximal tibial segement help to avoid tibial procurvatum deformity and malunion. Proximal third tibia fractures are often times difficult to reduce anatomically due to the tendency for both valgus and flexion deformity at the fracture site. The posterior blocking screw helps to eliminate the tendency for the nail to be too posterior and cause the fracture to flex. Blocking screws should be placed on the concavity of the deformity to minimize the procurvatum and valgus deformities of this fracture pattern.
Krettek et al looked at the importance of using blocking screws during intramedullary nailing of metaphyseal fractures using small diameter nails. They found less procurvatum deformity and malunions associated with using of blocking screws and found no complication with their utilization.
Ricci et al reviewed fractures of the proximal third of the tibial shaft treated with intramedullary nails and blocking screws. Their results supported that blocking screws were effective in maintaining alignment of fractures of the proximal third of the tibial shaft treated by intramedullary nailing.
Hiesterman et al review different reduction techniques to avoid malalignment, including the use of a proper starting point and insertion angle, blocking screws, unicortical plates, and a universal distractor.
Illustration A shows a radiograph utilizing posterior proximal and distal blocking screws to prevent procurvatum deformity.
Incorrect Answers:
Question 34High Yield
Which of the following are characteristic of osteoarthritis:
Explanation
The characteristic findings in osteoarthritis are:
Asymmetric loss of the joint space Subchondral sclerosis and cysts Osteophyte formation
As the cartilage degenerates, progressive bone remodeling occurs. The other responses refer to other synovial proliferative disorders:
Pigmented villonodular synovitis: Synovial proliferation, cysts/erosions on both sides of the joint
Rheumatoid arthritis: Synovial proliferation with lymphocytic infiltration, periarticular osteopenia, symmetric joint space loss
C harcot neuropathy: Subluxation, bone fragmentation, dissolution of the articular surfaces
Gout: Periarticular erosions, soft tissue masses, preservation of the articular surfaces
Asymmetric loss of the joint space Subchondral sclerosis and cysts Osteophyte formation
As the cartilage degenerates, progressive bone remodeling occurs. The other responses refer to other synovial proliferative disorders:
Pigmented villonodular synovitis: Synovial proliferation, cysts/erosions on both sides of the joint
Rheumatoid arthritis: Synovial proliferation with lymphocytic infiltration, periarticular osteopenia, symmetric joint space loss
C harcot neuropathy: Subluxation, bone fragmentation, dissolution of the articular surfaces
Gout: Periarticular erosions, soft tissue masses, preservation of the articular surfaces
Question 35High Yield
Orthopedic MCQS online Shoulder and Elbow 017
SHOULDER AND ELBOW SELF-
SCORED SELF-ASSESSMENT EXAMINATION
_AAOS 2017_
CLINICAL SITUATION FOR QUESTIONS 1 THROUGH 4
A 55-year-old man falls on his outstretched arm and sustains the injury shown in the 3-dimensional CT scans in Figures 1a and 1b.
Which ligamentous structure attaches to the fracture fragment?
SHOULDER AND ELBOW SELF-
SCORED SELF-ASSESSMENT EXAMINATION
_AAOS 2017_
CLINICAL SITUATION FOR QUESTIONS 1 THROUGH 4
A 55-year-old man falls on his outstretched arm and sustains the injury shown in the 3-dimensional CT scans in Figures 1a and 1b.
Which ligamentous structure attaches to the fracture fragment?









Explanation
Varus posteromedial rotatory instability is a complex injury pattern that starts with varus stress resulting in a fracture of the anteromedial coronoid. The anterior MCL attaches to the sublime tubercle, which is part of the anteromedial coronoid facet. The posterior MCL attaches to the posterior medial aspect of the ulna. The radial collateral and lateral ulnar collateral attach to the ulna at the crista supinatoris. The bony landmark is the sublime tubercle; as noted above, the crista supinatoris is lateral on the ulna. The radial notch is also lateral and is the articulation between the proximal ulna and proximal radius. The anteromedial coronoid facet is part of the coronoid, which extends more lateral and anterior than the anteromedial facet. The anteromedial facet represents the critical weight-bearing portion of the ulnohumeral joint. Damage to this structure causes posteromedial subluxation that often results in severe progressive arthritis. The coronoid is the larger structure of which the anteromedial coronoid facet is a portion. The posteromedial coronoid facet does not appear to be critical in weight bearing. The radial notch is not associated with increased stress with weight bearing. The treatment of displaced fractures of this structure is open reduction and internal fixation utilizing buttress plating. Closed treatment is acceptable only for nondisplaced fractures with appropriate radiographic follow-up. Suture fixation is not advocated because of inadequate strength.
RECOMMENDED READINGS
1. Pollock JW, Brownhill J, Ferreira L, McDonald CP, Johnson J, King G. The effect of anteromedial facet fractures of the coronoid and lateral collateral ligament injury on elbow stability and kinematics. J Bone Joint Surg Am. 2009 Jun;91(6):1448-58. doi: 10.2106/JBJS.H.00222.
2. Sanchez-Sotelo J, O'Driscoll SW, Morrey BF. Anteromedial fracture of the coronoid process of the ulna. J Shoulder Elbow Surg. 2006 Sep-Oct;15(5):e5-8. Epub 2006 Jul 26. Erratum in: J Shoulder Elbow Surg. 2007 Jan-Feb;16(1):127. PubMed PMID: 16979044.
RECOMMENDED READINGS
1. Pollock JW, Brownhill J, Ferreira L, McDonald CP, Johnson J, King G. The effect of anteromedial facet fractures of the coronoid and lateral collateral ligament injury on elbow stability and kinematics. J Bone Joint Surg Am. 2009 Jun;91(6):1448-58. doi: 10.2106/JBJS.H.00222.
2. Sanchez-Sotelo J, O'Driscoll SW, Morrey BF. Anteromedial fracture of the coronoid process of the ulna. J Shoulder Elbow Surg. 2006 Sep-Oct;15(5):e5-8. Epub 2006 Jul 26. Erratum in: J Shoulder Elbow Surg. 2007 Jan-Feb;16(1):127. PubMed PMID: 16979044.
Question 36High Yield
The net effect of 1,25 dihydroxyvitamin D3 on the calcium and phosphate concentration of the extracellular fluid and serum is:
Explanation
Parathyroid hormone, the active form of vitamin D (1,25 dihydroxyvitamin D), and calcitonin each have a net effect on calcium and phosphorus concentrations in extracellular fluid and serum:
Net Effect
Parathyroid hormone Increased serum calcium
Decreased serum phosphate
Vitamin D3 (1,25 dihydroxyvitamin D) Increased serum calcium
Increased serum phosphate
Calcitonin Decreased serum calcium
(transient) Correct Answer: Increased calcium, increased phosphate
Net Effect
Parathyroid hormone Increased serum calcium
Decreased serum phosphate
Vitamin D3 (1,25 dihydroxyvitamin D) Increased serum calcium
Increased serum phosphate
Calcitonin Decreased serum calcium
(transient) Correct Answer: Increased calcium, increased phosphate
Question 37High Yield
Figures 60a and 60b show the radiographs of the ankle and distal leg of an 1-
2. year-old girl after she twisted her ankle while playing soccer. She has no
3. history of ankle or leg pain. Examination reveals localized swelling and
4. tenderness over the lateral ankle, and the tibia is not tender. The bone lesion
5. identified in the tibia most likely is
6. 1- osteoblastoma.
7. 2- osteoid osteoma.
8. 3- ossifying fibroma.
9. 4- fibrous dysplasia.
10. 5- nonossifying fibroma.
2. year-old girl after she twisted her ankle while playing soccer. She has no
3. history of ankle or leg pain. Examination reveals localized swelling and
4. tenderness over the lateral ankle, and the tibia is not tender. The bone lesion
5. identified in the tibia most likely is
6. 1- osteoblastoma.
7. 2- osteoid osteoma.
8. 3- ossifying fibroma.
9. 4- fibrous dysplasia.
10. 5- nonossifying fibroma.
Explanation
1.
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Bertoni F, Calderoni P, Bacchim P, et al: Benign fibrous histiocytoma of bone. J Bone Joint Surg 1986;68A:1225-1230. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 4. Philadelphia, PA, JB Lippincott, 1996, pp 360-365.
#
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Bertoni F, Calderoni P, Bacchim P, et al: Benign fibrous histiocytoma of bone. J Bone Joint Surg 1986;68A:1225-1230. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 4. Philadelphia, PA, JB Lippincott, 1996, pp 360-365.
#
Question 38High Yield
A 24-year-old collegiate pitcher has had increasing pain over his medial elbow for 3 months. He has point tenderness over his medial epicondyle and reproduction of his symptoms with a valgus stress test. Which phase of the throwing cycle shown in Figure 1 will most likely reproduce his symptoms?
---
---
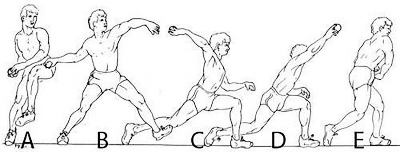
Explanation
This patient is experiencing soreness over his medial (ulnar) collateral ligament. Valgus overload is likely to reproduce his symptoms and is most pronounced during the late cocking phase of the throwing cycle. In windup, very little elbow torque is required. In early cocking, the arm is getting loaded, and maximum valgus is not yet achieved at the elbow. In acceleration and deceleration, more force is _generated at the level of the shoulder joint._
Question 39High Yield
A 10-year-old boy hit a tree with his sled and is seen in the emergency department with extreme left hip pain and inability to ambulate. He has no history of pain in the left groin, thigh, or knee. Radiographs are seen in Figures 29a and 29b. What is the most common complication resulting from this injury?
Explanation
The child has a type I hip fracture without associated dislocation. This is an acute hip fracture through the proximal femoral physis, and can occur with or without associated dislocation. He had no prodrome of hip or thigh pain and no femoral neck changes to indicate that this is an unstable slipped capital femoral epiphysis. Osteonecrosis in these transepiphyseal hip fractures is the most common and most devastating complication. The rate of osteonecrosis is most dependent on the initial displacement of the fracture. These fractures should be treated emergently, and decompression of the hip joint is recommended by many authors.
REFERENCES: Moon ES, Mehlman CT: Risk factors for avascular necrosis after femoral neck fractures in children: 25 Cincinnati cases and meta analysis of 360 cases. J Orthop Trauma 2006;20:323-329. Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
REFERENCES: Moon ES, Mehlman CT: Risk factors for avascular necrosis after femoral neck fractures in children: 25 Cincinnati cases and meta analysis of 360 cases. J Orthop Trauma 2006;20:323-329. Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
Question 40High Yield
Figure 68 is the MR image of an 85-year-old patient who cannot ambulate unless leaning over things. While sitting, the patient has minimal pain. Which structure is the arrow pointing to?
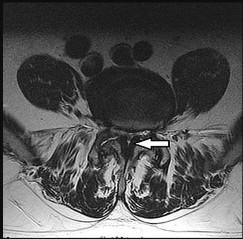



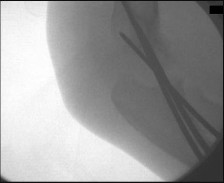
Explanation
This patient has neurogenic claudication and spinal stenosis. On this axial image, the spinal canal is narrowed. The arrow points to the ligamentum flavum (yellow ligament). The ligament connects the laminae of adjacent vertebrae and blends in with the facet caspule. In spinal stenosis, the ligamentum flavum is the primary cause of spinal nerve root compression, and surgical removal of the ligamentum flavum is a critical component of treatment. The inferior articular process is dorsal to the ligament on this axial image, while the inferior articular process is lateral to the arrow. The cauda equina refers to the lumbosacral nerve roots distal to the conus medullaris.
RECOMMENDED READINGS
6. Lurie JD, Tosteson TD, Tosteson A, Abdu WA, Zhao W, Morgan TS, Weinstein JN. Long-term outcomes of lumbar spinal stenosis: eight-year results of the Spine Patient Outcomes Research Trial (SPORT). Spine (Phila Pa 1976). 2015 Jan 15;40(2):63-76. doi: 10.1097/BRS.0000000000000731.
[PubMed PMID: 25569524.](http://www.ncbi.nlm.nih.gov/pubmed/25569524)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25569524)
7. [Weinstein JN, Lurie JD, Tosteson TD, Zhao W, Blood EA, Tosteson AN, Birkmeyer N, Herkowitz H, Longley M, Lenke L, Emery S, Hu SS. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am. 2009 Jun;91(6):1295-304. doi: 10.2106/JBJS.H.00913. PubMed PMID: 19487505. ](http://www.ncbi.nlm.nih.gov/pubmed/19487505)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19487505)
**
RECOMMENDED READINGS
6. Lurie JD, Tosteson TD, Tosteson A, Abdu WA, Zhao W, Morgan TS, Weinstein JN. Long-term outcomes of lumbar spinal stenosis: eight-year results of the Spine Patient Outcomes Research Trial (SPORT). Spine (Phila Pa 1976). 2015 Jan 15;40(2):63-76. doi: 10.1097/BRS.0000000000000731.
[PubMed PMID: 25569524.](http://www.ncbi.nlm.nih.gov/pubmed/25569524)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25569524)
7. [Weinstein JN, Lurie JD, Tosteson TD, Zhao W, Blood EA, Tosteson AN, Birkmeyer N, Herkowitz H, Longley M, Lenke L, Emery S, Hu SS. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am. 2009 Jun;91(6):1295-304. doi: 10.2106/JBJS.H.00913. PubMed PMID: 19487505. ](http://www.ncbi.nlm.nih.gov/pubmed/19487505)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19487505)
**
Question 41High Yield
Figures 73a through 73c are the radiographs of a 14-year-old girl who sustained an ankle injury in a fall.What ligament is attached to the displaced fragment?
---
---
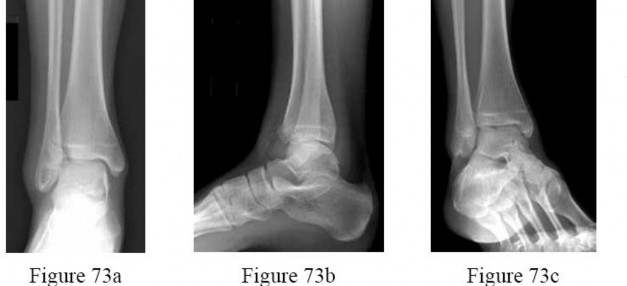
Explanation
The patient has sustained a Tillaux fracture. This fracture of the anterolateral portion of the distal tibia epiphysis occurs in early adolescence. The medial portion of the growth plate fuses first.The anterior inferior tibiofibular ligament attaches to the anterolateral portion of the tibial epiphysis and avulses the fragment, usually in response to an external rotation force. The other named ligaments are lateral in location but do not attach to the shown tibial fragment.
Question 42High Yield
A 50-year-old pipefitter falls from a ladder at work and dislocates his non-dominant shoulder. His MRI scan shows supraspinatus and infraspinatus tears with retraction to the glenoid. He cannot actively raise his arm away from his side. He denies prior shoulder symptoms before his fall. Three weeks of physical therapy have failed to improve his function. Which factor has been demonstrated to result in a poor clinical outcome following surgical intervention?
Explanation
DISCUSSION
Several studies have demonstrated that patients with work-related injuries do not do as well as those whose injuries are not work-related after repair of the rotator cuff. This patient’s age and gender are not negative prognostic indicators. The acute nature of the tear does not lead to an inferior outcome.
DISCUSSION
Several studies have demonstrated that patients with work-related injuries do not do as well as those whose injuries are not work-related after repair of the rotator cuff. This patient’s age and gender are not negative prognostic indicators. The acute nature of the tear does not lead to an inferior outcome.
Question 43High Yield
Patients treated with zoledronic acid within 90 days of a hip fracture, followed up with annual treatment, will most likely show:
Explanation
A large prospective, randomized study showed a reduction in vertebral and nonvertebral fractures when patients were treated with intravenous (IV) zoledronic acid within 90 days of a hip fracture, followed up with annual treatment.
Important points to remember about this study:
Study: Zoledronic acid (5 mg, IV) within 90 days of hip fracture and then annually (1,000 patients in each group) New fractures: 8.6% vs 13.9% (absolute risk reduction, 5.3%; relative risk reduction, 35%)
New fractures
  o   Vertebral: 1.7% vs 3.8% (P = .02)
  o   Nonvertebral: 7.6% vs 10.7% (P = .03)
  o   Hip: 2.0% vs 3.5% (relative risk 30%, not significant)   o   Divergence of fracture-free survival at 12 months BMD
  o   12 month: 2.6% vs -1.0%   o   24 month: 4.7% vs -0.7%   o   36 month: 5.5% vs -0.9% Death
  o   Hazard ratio: -0.72 (0.56 to 0.93 C I, P = .01) Adverse advents
  o   Pyrexia: 8.7% vs 3.1%   o   Myalgia: 4.9% vs 2.7%
  o   Bone pain: 3.2% vs 1.0%
C orrect Answer: Decreased vertebral fractures, decreased nonvertebral fracture, and improved survival
Important points to remember about this study:
Study: Zoledronic acid (5 mg, IV) within 90 days of hip fracture and then annually (1,000 patients in each group) New fractures: 8.6% vs 13.9% (absolute risk reduction, 5.3%; relative risk reduction, 35%)
New fractures
  o   Vertebral: 1.7% vs 3.8% (P = .02)
  o   Nonvertebral: 7.6% vs 10.7% (P = .03)
  o   Hip: 2.0% vs 3.5% (relative risk 30%, not significant)   o   Divergence of fracture-free survival at 12 months BMD
  o   12 month: 2.6% vs -1.0%   o   24 month: 4.7% vs -0.7%   o   36 month: 5.5% vs -0.9% Death
  o   Hazard ratio: -0.72 (0.56 to 0.93 C I, P = .01) Adverse advents
  o   Pyrexia: 8.7% vs 3.1%   o   Myalgia: 4.9% vs 2.7%
  o   Bone pain: 3.2% vs 1.0%
C orrect Answer: Decreased vertebral fractures, decreased nonvertebral fracture, and improved survival
Question 44High Yield
Initial treatment for De Quervain disease involves:
Explanation
Initial treatment for De Quervain tenosynovitis involves rest and splinting with steroid injection into the first dorsal compartment. The splint should be worn as much as possible for 3 to 4 weeks. The extensor carpi radialis brevis has been implicated in lateral epicondulitis. The extensor pollicis longus can be a source of pain as it wraps over the wrist extensor giving the classic symptoms of intersection syndrome between the second and third dorsal compartments. Surgical release is only indicated in persistent cases that have failed conservative management. In 20% to 30% of cases, the first compartment is divided by longitudinal septations into two distinct tunnels. C are must be taken to identify and release both of these tunnels, as well as any multiple tendinous slips, when performing a surgical release.
Question 45High Yield
Figure 1 is the radiograph of a 6-year-old boy who falls off a tire swing and sustains an isolated left femur fracture that is treated with submuscular plating (Figure 2). He went on to uneventful union and full return to activity without disability. Recommendations should include

Explanation
■
Submuscular plating of pediatric femur fractures is a reliable technique for length in unstable fractures in the 5- to 10-year-old age group. Several reports have demonstrated a propensity for late valgus development with a contoured lateral plate adjacent to the distal femoral physis and recommend for routine implant removal following fracture union and remodeling prior to development of this sequelae, rather than observation and additional treatment once it occurs. This fracture carries no significant risk of avascular necrosis; thus, future arthroplasty is not relevant to this decision making. Activity restriction is recommended for 4 to 6 weeks following implant removal to minimize the risk of pathologic fracture through a screw hole.
■
Submuscular plating of pediatric femur fractures is a reliable technique for length in unstable fractures in the 5- to 10-year-old age group. Several reports have demonstrated a propensity for late valgus development with a contoured lateral plate adjacent to the distal femoral physis and recommend for routine implant removal following fracture union and remodeling prior to development of this sequelae, rather than observation and additional treatment once it occurs. This fracture carries no significant risk of avascular necrosis; thus, future arthroplasty is not relevant to this decision making. Activity restriction is recommended for 4 to 6 weeks following implant removal to minimize the risk of pathologic fracture through a screw hole.
Question 46High Yield
A patient presents for treatment of a painful hallux. The pain is over the dorsal surface of the hallux metatarsophalangeal joint and is worsened with plantar flexion of the toe. The passive range of motion is 30° of dorsiflexion and 10° of plantarflexion. The radiographs confirm the presence of mild arthritis of the metatarsophalangeal joint, with dorsal osteophytes on the metatarsal head. Which of the following procedures is most likely to be associated with a long-term satisfactory outcome:
Explanation
The pain present in plantarflexion is common and associated with friction of the capsule against the dorsal osteophytes. This patient has noted only mild arthritis of the metatarsophalangeal joint. An arthrodesis is not a necessary treatment, although it is a reasonable alternative. Implant and interposition arthroplasty are alternatives for the treatment of arthritis of the metatarsophalangeal joint but preferably only when the condition is advanced.
Question 47High Yield
Which of the following defects occurs in Albright hereditary osteodystrophy (pseudohypoparathyroidism):
Explanation
Pseudohypoparathyroidism (PHP) (Albright Hereditary Osteodystrophy [AHO]) - end organ insensitivity; in AHO, germline mutation that leads to loss of function of Galpha S (GNAS1); causes end-organ resistance to PTH (Zaleske).
1/. PHP - short stature, short metacarpals (4th and 5th), rounded facies a. Mental retardation, tetany
b. Sex-linked dominant
2/. Laboratory features a. Hypocalcemia
b. Hyperphopshatemia c. Normal PTH
3/. Other features
The other responses refer to:
Metaphyseal chondrodysplasia (Schmid type): Type X collagen
Diastrophic dysplasia: Sulfate transporter gene
Gaucher's disease: Beta glucosidase
Osteopetrosis: C arbonic anhydrase type II, proton pump
1/. PHP - short stature, short metacarpals (4th and 5th), rounded facies a. Mental retardation, tetany
b. Sex-linked dominant
2/. Laboratory features a. Hypocalcemia
b. Hyperphopshatemia c. Normal PTH
3/. Other features
The other responses refer to:
Metaphyseal chondrodysplasia (Schmid type): Type X collagen
Diastrophic dysplasia: Sulfate transporter gene
Gaucher's disease: Beta glucosidase
Osteopetrosis: C arbonic anhydrase type II, proton pump
Question 48High Yield
Pigmented villonodular synovitis PREFERRED RESPONSE: 3
DISCUSSION: The MRI scans show a cystic structure within the anterior cruciate ligament. It is fluid filled as seen on the T2 sequence. Ganglion cysts of the cruciate ligaments are rare. The most common presentation is pain with occasional loss of motion. Instability is not a chief complaint and often there is no evidence of laxity on examination. If nonsurgical management fails, arthroscopic debridement of the cyst is the accepted method of treatment.
REFERENCES: Liu SH, Osti L, Mirzayan R: Ganglion cysts of the anterior cruciate ligament: A case report and review of the literature. Arthroscopy 1994; 10:110-112.
Parish EN, Dixon P, Cross MJ: Ganglion cysts of the anterior cruciate ligament: A series of 15 cases. Arthroscopy 2005;21:445-447.
Figure 56
Figure 56 shows an arthroscopic view of the long head of the biceps; it has an incompetent biceps sling and is unstable, and an axial glenohumeral MRI scan reveals that it is dislocated medially out of the intertubercular groove. What structure is also most likely injured?
DISCUSSION: The MRI scans show a cystic structure within the anterior cruciate ligament. It is fluid filled as seen on the T2 sequence. Ganglion cysts of the cruciate ligaments are rare. The most common presentation is pain with occasional loss of motion. Instability is not a chief complaint and often there is no evidence of laxity on examination. If nonsurgical management fails, arthroscopic debridement of the cyst is the accepted method of treatment.
REFERENCES: Liu SH, Osti L, Mirzayan R: Ganglion cysts of the anterior cruciate ligament: A case report and review of the literature. Arthroscopy 1994; 10:110-112.
Parish EN, Dixon P, Cross MJ: Ganglion cysts of the anterior cruciate ligament: A series of 15 cases. Arthroscopy 2005;21:445-447.
Figure 56
Figure 56 shows an arthroscopic view of the long head of the biceps; it has an incompetent biceps sling and is unstable, and an axial glenohumeral MRI scan reveals that it is dislocated medially out of the intertubercular groove. What structure is also most likely injured?




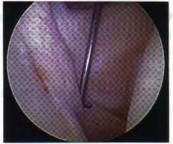

Explanation
The supplement is creatine. Approximately 17% of high school athletes and about 30% of high school football players use creatine. Creatine is a protein synthesized in the liver and the kidney, circulates in the bloodstream, and is incorporated into muscle. Its use is associated with increased muscle mass, short-term improvement in sprinting, and may allow for increased anaerobic resistance performance. Caffeine and ephedrine are taken orally but do not increase muscle mass. Testosterone and human growth hormone are both associated with increased body mass but must be injected.
REFERENCES: McGuine TA, Sullivan JC, Bernhardt DT: Creatine supplementation in high school football players. Clin J Sports Med 2001 ;11:247-253.
Rawson ES, Gunn B, Clarkson PM: The effects of creatine supplementation on exercise-induced muscle damage. J Strength Cond Res 2001; 15:178-184.
Branch JD: Effect of creatine supplementation on body composition and performance: A meta-analysis.
Int J Sport Nutr Exerc Metab 2003;13:198-226.
An 11-year-old boy who is a Little League pitcher has a 3-month history of right elbow pain, made worse after several innings of pitching. The pain is in the posterior and medial aspect of the elbow joint but is without clicking or mechanical symptoms. There are no signs of infection or swelling, and range of motion is full.
There is tenderness over the medial aspect of the elbow distal to the humeral epicondyle over the proximal olecranon. Valgus stress testing of the elbow is normal. What is the most likely diagnosis?
1) Olecranon bursitis
2) Osteochondritis dissecans of the capitellum
3) Ulnar collateral ligament insufficiency
4) Medial epicondylitis
5) Olecranon stress fracture
The patient has an olecranon stress fracture due to overuse injury from pitching. The repetitive forceful contraction of the triceps coupled with varus and valgus torques about the elbow are felt to cause the olecranon epiphysis to separate from the adjacent epiphyseal plate as reported by Torg and Moyer. This may persist into late adolescence; Charlton and Chandler described five throwing athletes between the ages of 16 to 20 years with delayed closure of the olecranon epiphysis and inability to throw. The ulnar collateral ligament was intact in all. The patients in their study underwent open reduction and internal fixation with tension band wire, screw fixation, and autogenous bone graft in some of the cases.
At 32 months, all were asymptomatic despite a prolonged preoperative course (> 30 months) of limiting pain. It is important to recognize stress fractures about the elbow in a young pitching population and treat accordingly first with rest and cessation of throwing activities. If prolonged, surgical fixation provides reliable results.
REFERENCES: Charlton WP, Chandler RW: Persistence of the olecranon physis in baseball players: Results following operative management. J Shoulder Elbow Surg 2003;12:59-62.
Torg JS, Moyer RA: Non-union of a stress fracture through the olecranon epiphyseal plate observed in an
adolescent baseball pitcher. J Bone Joint Surg Am 1977;59:264-265.
Rettig AC, Wurth TR, Mieling P: Nonunion of olecranon stress fractures in adolescent baseball pitchers: A case series of 5 athletes. Am J Sports Med 2006;34:653-656.
What is the most common physical finding in a patient with femoroacetabular impingement (FAI)?
1) Increased external rotation
2) Increased abduction
3) Decreased external rotation
4) Decreased flexion and internal rotation
5) Decreased adduction
reproduction of symptoms. Occasionally, a posterior impingement test will be positive with extension and external rotation. There are a variety of causes of FAI; however, the pathology limits motion as the femur (cam) and acetabulum (pincer) contact one another. Also, only one location needs to be present, such as cam-type or pincer-type versus both cam-pincer lesions to cause symptoms.
REFERENCES: Philippon MJ, Stubbs AJ, Schenker ML, et al: Arthroscopic management of femoroacetabular impingement: Osteoplasty technique and literature review. Am J Sports Med 2007;35:1571 -1580, Siebenrock KA, Schoeniger R, Ganz R: Anterior femoroacetabular impingement due to acetabular retroversion: Treatment with periacetabular osteotomy. J Bone Joint Surg Am 2003;85:278 -286. Kubiak-Langer M, Tannast M, Murphy SB, et al: Range of motion in anterior femoroacetabular impingement. Clin Orthop Relat Res 2007;458:117-124.
Which of the following diseases has documented transmission by allograft tissue transplantation in the last 20 years?
1) Tuberculosis
2) Hepatitis B
3) HIV
4) West Nile virus
5) Clostridium
The only reported cases of HIV transmission with tissue transplantation occurred more than 20 years ago. The only reported cases of tuberculosis and hepatitis B occurred more than 50 years ago. The donor-associated clostridium infection occurred in 2001. The facility was not AATB-accredited (American Association of Tissue Banks) and the local A ATB facility refused the graft. It is necessary for the surgeon using the allograft tissue to be aware of the current status of tissue regulation, and procurement and processing procedures.
REFERENCES: McAllister DR, Joyce MJ, Mann BJ, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;35:2148-2158.
Safety of tissue transplants. American Association of Tissue Banks, 2006.
Which of the following types of intra-articular pathology is associated with lateral meniscal cysts?
REFERENCES: McGuine TA, Sullivan JC, Bernhardt DT: Creatine supplementation in high school football players. Clin J Sports Med 2001 ;11:247-253.
Rawson ES, Gunn B, Clarkson PM: The effects of creatine supplementation on exercise-induced muscle damage. J Strength Cond Res 2001; 15:178-184.
Branch JD: Effect of creatine supplementation on body composition and performance: A meta-analysis.
Int J Sport Nutr Exerc Metab 2003;13:198-226.
An 11-year-old boy who is a Little League pitcher has a 3-month history of right elbow pain, made worse after several innings of pitching. The pain is in the posterior and medial aspect of the elbow joint but is without clicking or mechanical symptoms. There are no signs of infection or swelling, and range of motion is full.
There is tenderness over the medial aspect of the elbow distal to the humeral epicondyle over the proximal olecranon. Valgus stress testing of the elbow is normal. What is the most likely diagnosis?
1) Olecranon bursitis
2) Osteochondritis dissecans of the capitellum
3) Ulnar collateral ligament insufficiency
4) Medial epicondylitis
5) Olecranon stress fracture
The patient has an olecranon stress fracture due to overuse injury from pitching. The repetitive forceful contraction of the triceps coupled with varus and valgus torques about the elbow are felt to cause the olecranon epiphysis to separate from the adjacent epiphyseal plate as reported by Torg and Moyer. This may persist into late adolescence; Charlton and Chandler described five throwing athletes between the ages of 16 to 20 years with delayed closure of the olecranon epiphysis and inability to throw. The ulnar collateral ligament was intact in all. The patients in their study underwent open reduction and internal fixation with tension band wire, screw fixation, and autogenous bone graft in some of the cases.
At 32 months, all were asymptomatic despite a prolonged preoperative course (> 30 months) of limiting pain. It is important to recognize stress fractures about the elbow in a young pitching population and treat accordingly first with rest and cessation of throwing activities. If prolonged, surgical fixation provides reliable results.
REFERENCES: Charlton WP, Chandler RW: Persistence of the olecranon physis in baseball players: Results following operative management. J Shoulder Elbow Surg 2003;12:59-62.
Torg JS, Moyer RA: Non-union of a stress fracture through the olecranon epiphyseal plate observed in an
adolescent baseball pitcher. J Bone Joint Surg Am 1977;59:264-265.
Rettig AC, Wurth TR, Mieling P: Nonunion of olecranon stress fractures in adolescent baseball pitchers: A case series of 5 athletes. Am J Sports Med 2006;34:653-656.
What is the most common physical finding in a patient with femoroacetabular impingement (FAI)?
1) Increased external rotation
2) Increased abduction
3) Decreased external rotation
4) Decreased flexion and internal rotation
5) Decreased adduction
reproduction of symptoms. Occasionally, a posterior impingement test will be positive with extension and external rotation. There are a variety of causes of FAI; however, the pathology limits motion as the femur (cam) and acetabulum (pincer) contact one another. Also, only one location needs to be present, such as cam-type or pincer-type versus both cam-pincer lesions to cause symptoms.
REFERENCES: Philippon MJ, Stubbs AJ, Schenker ML, et al: Arthroscopic management of femoroacetabular impingement: Osteoplasty technique and literature review. Am J Sports Med 2007;35:1571 -1580, Siebenrock KA, Schoeniger R, Ganz R: Anterior femoroacetabular impingement due to acetabular retroversion: Treatment with periacetabular osteotomy. J Bone Joint Surg Am 2003;85:278 -286. Kubiak-Langer M, Tannast M, Murphy SB, et al: Range of motion in anterior femoroacetabular impingement. Clin Orthop Relat Res 2007;458:117-124.
Which of the following diseases has documented transmission by allograft tissue transplantation in the last 20 years?
1) Tuberculosis
2) Hepatitis B
3) HIV
4) West Nile virus
5) Clostridium
The only reported cases of HIV transmission with tissue transplantation occurred more than 20 years ago. The only reported cases of tuberculosis and hepatitis B occurred more than 50 years ago. The donor-associated clostridium infection occurred in 2001. The facility was not AATB-accredited (American Association of Tissue Banks) and the local A ATB facility refused the graft. It is necessary for the surgeon using the allograft tissue to be aware of the current status of tissue regulation, and procurement and processing procedures.
REFERENCES: McAllister DR, Joyce MJ, Mann BJ, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;35:2148-2158.
Safety of tissue transplants. American Association of Tissue Banks, 2006.
Which of the following types of intra-articular pathology is associated with lateral meniscal cysts?
Question 49High Yield
A 40-year-old woman with no history of back problems has a symptomatic L4-5 disk herniation with an L5 radiculopathy that has failed to respond to 12 weeks of nonsurgical management. In the preoperative discussion, the surgeon advises the patient that the chance of recurrence of the herniation after successful diskectomy is what percent?
Explanation
DISCUSSION: The incidence of recurrent disk herniation after a successful diskectomy is approximately 5% to 10%. Indications for surgical diskectomy for a recurrence are the same as for a primary diskectomy.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 685-698.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 127-139.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 685-698.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 127-139.
Question 50High Yield
Which of the following describes the inheritance pattern of hypophosphatasia:
Explanation
Structural defects are usually transmitted by an autosomal-dominant pattern. In contrast, with metabolic or enzyme deficiencies, the condition is usually transmitted in an autosomal-recessive pattern.
Remember the major autosomal-recessive conditions: Sickle cell disease
Osteogenesis imperfecta (Types II, III)
Hypophosphatasia Homocystinuria Gaucher's disease
Remember the major autosomal-recessive conditions: Sickle cell disease
Osteogenesis imperfecta (Types II, III)
Hypophosphatasia Homocystinuria Gaucher's disease
Question 51High Yield
A 10-year-old boy hit a tree with his sled and is seen in the emergency department with extreme left hip pain and inability to ambulate. He has no history of pain in the left groin, thigh, or knee. Radiographs are seen in Figures 29a and 29b. What is the most common complication resulting from this injury?
Explanation
DISCUSSION: The child has a type I hip fracture without associated dislocation. This is an acute hip fracture through the proximal femoral physis, and can occur with or without associated dislocation. He had no prodrome of hip or thigh pain and no femoral neck changes to indicate that this is an unstable slipped capital femoral epiphysis. Osteonecrosis in these transepiphyseal hip fractures is the most common and most devastating complication. The rate of osteonecrosis is most dependent on the initial displacement of the fracture. These fractures should be treated emergently, and decompression of the hip joint is recommended by many authors.
REFERENCES: Moon ES, Mehlman CT: Risk factors for avascular necrosis after femoral neck fractures in children: 25 Cincinnati cases and meta analysis of 360 cases. J Orthop Trauma 2006;20:323-329. Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
**2010 Pediatric Orthopaedic Examination Answer Book • 29**
REFERENCES: Moon ES, Mehlman CT: Risk factors for avascular necrosis after femoral neck fractures in children: 25 Cincinnati cases and meta analysis of 360 cases. J Orthop Trauma 2006;20:323-329. Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
**2010 Pediatric Orthopaedic Examination Answer Book • 29**
Question 52High Yield
Androgens prevent bone resorption. Receptors for androgens are found on which of the following cells:
Explanation
Osteoblasts have receptors for androgens. Although androgens prevent bone resorption and may increase bone mass, the process is not understood at this time
Question 53High Yield
A patient underwent a right hip arthroscopy, CAM resection, and labral repair while positioned supine on a fracture table with a perineal post. The leg was in traction for 4 hours, and no intrasurgical complications were noted. At the 2‐week follow‐up appointment, the patient was experiencing numbness and tingling in the perineum on the surgical side and noted pain predominantly while sitting. What is the likely cause of these symptoms?
25
25
Explanation
Although all of these responses are known complications related to hip arthroscopy, the symptoms of perineal numbness and pain associated with prolonged traction time indicate a compression injury to the pudendal nerve against the perineal post used to provide counter traction. Perineal numbness usually occurs on the surgical side, with pain in the area of the anus to the penis/clitoris. Pain is predominantly experienced while sitting, but is relieved when sitting on a toilet. Pain can be relieved with a diagnostic pudendal nerve block. This injury is not unique to hip arthroscopy; it also is described in the trauma literature. To prevent compression‐type injuries, a well‐padded post larger than 9 cm in diameter should be positioned against the medial thigh. Traction force should be kept to a minimum and the extremity positioned in slight abduction. Continuous traction time should not exceed 2 hours, with intermittent traction used during prolonged procedures.
Question 54High Yield
What is the zone of injury?
Explanation
- Hypertrophic zone
Question 55High Yield
..A 21-year-old college swimmer presents with an inability to compete for longer than 1 year because of right shoulder pain and subjective symptoms of instability despite physical therapy. Recent radiographs and an MRI scan of her shoulder demonstrate an intact labral complex. Her symptoms are reproduced with sulcus testing and load and shift maneuvers in both anterior and posterior directions. What is the most appropriate next treatment step?
Explanation
- Open capsular shift
Question 56High Yield
The daily elemental calcium requirement for a pregnant woman is:
Explanation
The guidelines for the daily elemental calcium requirement are as follows:
Children 500 mg to 700 mg
Growth spurt to young adult
(10 to 25 years of age)
1,300 mg
Adult male 750 mg
Adult female
Postmenopausal Elderly Pregnancy Lactation
  Â
1,500 mg
1,200 mg
1,500 mg
2,000 mg
Note: 1 daily equivalent = 250 mg elemental calcium (one glass of milk) Correct Answer: 1,500 mg
Children 500 mg to 700 mg
Growth spurt to young adult
(10 to 25 years of age)
1,300 mg
Adult male 750 mg
Adult female
Postmenopausal Elderly Pregnancy Lactation
  Â
1,500 mg
1,200 mg
1,500 mg
2,000 mg
Note: 1 daily equivalent = 250 mg elemental calcium (one glass of milk) Correct Answer: 1,500 mg
Question 57High Yield
Which of the following fractures occurs through a single application of force:
Explanation
The femoral neck fracture, metatarsal fracture, rib fracture, and the tibial fracture are stress fractures that result from repetitive loading.
In contrast, the humeral fracture in the baseball catcher is secondary to failure of the humerus secondary to a pure torsional force. Long bones are at their weakest when loaded in pure torsion.
In contrast, the humeral fracture in the baseball catcher is secondary to failure of the humerus secondary to a pure torsional force. Long bones are at their weakest when loaded in pure torsion.
Question 58High Yield
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?
Explanation
The patient has a volar displaced two-part intra-articular distal radial fracture-dislocation of the wrist. Although a closed reduction is usually easily obtained, it is very difficult to maintain the reduction without internal fixation. The approach is determined by the direction of the dislocation, in this case volar. Stabilization with a buttress plate neutralizes the axial loading forces on the fractured fragment. A dorsal placed angular stable plate will not provide this buttress effect and will make the reduction difficult.
REFERENCE: Cohen M, McMurtry RY, Jupiter JB: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1328-1335.
REFERENCE: Cohen M, McMurtry RY, Jupiter JB: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1328-1335.
Question 59High Yield
Which treatment of the current fracture will provide the best long-term outcome?




Explanation
Many patients with mild dominant OI (the most common type) appear “normal,” and a diagnosis cannot be made without a careful personal history, family history, and observance of blue sclera. More than 3 fractures during childhood places someone outside of the mean and should merit further investigation. There is no sign of rickets on this radiograph (physeal widening/cupping). Similarly, the history and examination finding of blue sclera in the patient and his mother should raise concern for OI. Many parents of children with OI have inappropriately been accused of abuse despite obvious examination, radiograph, and family history findings that suggest OI. Low-energy mechanisms that create displaced fractures are a hallmark of OI and do not in isolation raise suspicion for nonaccidental trauma.
Based on the history and examination, mild-form OI caused by a defect in the type I collagen gene is most likely. Defects in type II collagen genes affect articular cartilage and cause epiphyseal dysplasia. Defects in the LEPRE cause severe-form OI involving clinically bowed limbs, marked short stature, and white sclera. There is no sign on radiographs of rickets, so severe vitamin D deficiency is not present. The history, examination, and radiographs all point toward OI/osteoporosis rather than nonaccidental trauma.
Peri-implant fractures occur because of a difference in elasticity between the bone with implants and the bone adjacent to it without implants. This is particularly important in the setting of osteoporotic bone in which the difference in elasticity and rigidity will be much more pronounced than in normal bone. Load-sharing implants are preferred when possible. The original fracture occurred proximal to the current fracture in the middle of the plated bone and looks healed with no sign of infection.
This fracture is in unacceptable alignment with subluxation of the radiocapitellar joint. The plates are bent, so closed reduction will not solve the alignment problem. In early childhood, load-sharing implants (flexible rods or wires) should be used to solve the elasticity mismatch that contributed to the current fracture.
Figure 51a
Figure 51b
Figure 51c
CLINICAL SITUATION FOR QUESTIONS 51 THROUGH 54
Figures 51a through 51c are the radiographs of an 8-year-old boy with a shoulder deformity and limited cervical range of motion. He has no significant medical problems and plays baseball, pitching with his right arm. His active shoulder abduction is 180 degrees on the left and 150 degrees on the right.
Based on the history and examination, mild-form OI caused by a defect in the type I collagen gene is most likely. Defects in type II collagen genes affect articular cartilage and cause epiphyseal dysplasia. Defects in the LEPRE cause severe-form OI involving clinically bowed limbs, marked short stature, and white sclera. There is no sign on radiographs of rickets, so severe vitamin D deficiency is not present. The history, examination, and radiographs all point toward OI/osteoporosis rather than nonaccidental trauma.
Peri-implant fractures occur because of a difference in elasticity between the bone with implants and the bone adjacent to it without implants. This is particularly important in the setting of osteoporotic bone in which the difference in elasticity and rigidity will be much more pronounced than in normal bone. Load-sharing implants are preferred when possible. The original fracture occurred proximal to the current fracture in the middle of the plated bone and looks healed with no sign of infection.
This fracture is in unacceptable alignment with subluxation of the radiocapitellar joint. The plates are bent, so closed reduction will not solve the alignment problem. In early childhood, load-sharing implants (flexible rods or wires) should be used to solve the elasticity mismatch that contributed to the current fracture.
Figure 51a
Figure 51b
Figure 51c
CLINICAL SITUATION FOR QUESTIONS 51 THROUGH 54
Figures 51a through 51c are the radiographs of an 8-year-old boy with a shoulder deformity and limited cervical range of motion. He has no significant medical problems and plays baseball, pitching with his right arm. His active shoulder abduction is 180 degrees on the left and 150 degrees on the right.
Question 60High Yield
The optimal position for hallux interphalangeal joint arthrodesis is:
Explanation
The optimal position for hallux interphalangeal joint arthrodesis is 5° to 10° of plantarflexion, neutral varus-valgus, and neutral rotation. The plantarflexion helps the toe pad to contact the ground during gait.
Question 61High Yield
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?
Explanation
The avulsed fragment represents the origin of the rectus femoris from the anterior inferior iliac spine and the brim of the acetabulum. Avulsion of the anterior inferior iliac spine is much less common than avulsion of the anterior superior iliac spine with its origin of the sartorius. The origin of the gluteus minimus is from the outer cortex of the iliac wing and has not been reported as a source of bony avulsion. The hip capsule is composed of the ischiofemoral and pubofemoral ligaments, in addition to the iliofemoral ligament. The pelvic attachment of the ischiofemoral ligament is from the ischial part of the acetabulum posteriorly, while the pubofemoral ligament attaches to the pubic portion inferiorly. Technically, ligaments do not have origins and insertions as muscle tendon groups do, but have attachment sites.
REFERENCES: Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Mader TJ: Avulsion of the rectus femoris tendon: An unusual type of pelvic fracture. Pediatr Emerg Care 1990;6:198-199.
REFERENCES: Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Mader TJ: Avulsion of the rectus femoris tendon: An unusual type of pelvic fracture. Pediatr Emerg Care 1990;6:198-199.
Question 62High Yield
A 35-year-old woman presents with an elbow injury which includes a coronoid fracture involving more than 50%, a comminuted
radial head fracture, and an elbow dislocation. What is the most appropriate treatment?
radial head fracture, and an elbow dislocation. What is the most appropriate treatment?
Explanation
A terrible triad of the elbow includes dislocation of the elbow with associated fractures of the radial head and the coronoid process. Ring et al. stressed that these injuries are prone to complications and advised against resection of the radial head due to instability, and instead recommended a radial head replacement if too comminuted for ORIF. Coronoid fractures compromise elbow stability as well and require open reduction and internal fixation as with the lateral collateral ligament. McKee et al. showed stable elbows in 34/36 with mean Mayo elbow score of 88 when the standard protocol of coronoid ORIF, radial head repair/replacement, and LCL repair were employed.
Question 63High Yield
A 9-year-old boy is examined due to a closed distal forearm fracture. The radius and ulna are both fractured and translated
100%. After manipulation twice with sedation, the translation cannot be reduced. There is 10-mm shortening of the radius and 5- mm shortening of the ulna. The distal radial angulation on the anteroposterior view is 5° less than normal. The least invasive treatment which would produce acceptable results is:
100%. After manipulation twice with sedation, the translation cannot be reduced. There is 10-mm shortening of the radius and 5- mm shortening of the ulna. The distal radial angulation on the anteroposterior view is 5° less than normal. The least invasive treatment which would produce acceptable results is:
Explanation
The translation and shortening are not problems and the amount of angulation will easily remodel with this fracture. There is nothing to be gained from operative reduction.
Question 64High Yield
A 15-year-old boy has a fracture of the proximal tibia extending from the apophysis of the tubercle up through the posterior part of the proximal tibial epiphysis and into the joint. What is the most likely mechanism of injury?
Explanation
Tibial Tuberosity Fractures Fractures of the tibial tuberosity are uncommon avulsion injuries. Most are sportsrelated and occur in older adolescents. Type I fractures represent an avulsion of a small fragment of the tuberosity. Type II fractures involve the entire anterior tuberosity with extension proximally to the level of the horizontal portion of the proximal tibial physis. Type III injuries involve the entire tuberosity with extension proximally into the articular surface, a SalterHarris type III fracture. Patients present with pain, swelling, and tenderness over the tuberosity. Patella alta may be present. Surgical treatment of type I fractures is needed if patella alta (compared to the normal uninjured side) and a significant bony prominence are present. Displaced types II and III fractures are treated with open reduction and internal fixation. A cancellous interfragmentary screw may be placed through the tuberosity into the metaphysis. Because this injury occurs in patients near skeletal maturity, growth arrest with secondary genu recurvatum is rare.
Question 65High Yield
Figures 23a and 23b show
2. radiographs of a 52-year-old man
3. with diabetes who has had purulent
4. drainage from the medial side of his
5. right great toe for 3 weeks. He was
6. recently started on insulin.
7. Examination reveals a good dorsalis
8. pedis pulse but poor sensation from
9. the malleoli to the toes. Treatment
10. should consist of
11. 1- amputation of the great toe.
12. 2- bone culture and 6 weeks of IV
13. antibiotics.
14. 3- joint aspiration and 2 weeks of IV
15. antibiotics.
16. 4- excision interphalangeal arthroplasty.
17. 5- excision of infected bone and
18. interphalangeal joint arthrodesis.
2. radiographs of a 52-year-old man
3. with diabetes who has had purulent
4. drainage from the medial side of his
5. right great toe for 3 weeks. He was
6. recently started on insulin.
7. Examination reveals a good dorsalis
8. pedis pulse but poor sensation from
9. the malleoli to the toes. Treatment
10. should consist of
11. 1- amputation of the great toe.
12. 2- bone culture and 6 weeks of IV
13. antibiotics.
14. 3- joint aspiration and 2 weeks of IV
15. antibiotics.
16. 4- excision interphalangeal arthroplasty.
17. 5- excision of infected bone and
18. interphalangeal joint arthrodesis.
Explanation
1.
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Penn I: Infections in the diabetic foot, in Samarco GJ (ed): The Foot in Diabetes. Philadelphia, PA, Lea & Febiger, 1991, pp 109-121. Wagner FW: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981, pp 66-122.
#
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Penn I: Infections in the diabetic foot, in Samarco GJ (ed): The Foot in Diabetes. Philadelphia, PA, Lea & Febiger, 1991, pp 109-121. Wagner FW: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981, pp 66-122.
#
Question 66High Yield
-Pelvic packing for a hemodynamically unstable patient with a pelvic ring fracture is best described by which of the following techniques?
Explanation
No detailed explanation available.
Question 67High Yield
A 3-year-old child sustains a T2/T3 fracture-dislocation with complete paraplegia secondary to a car accident in which the child was an unrestrained passenger. What is the likelihood that this child will develop subsequent spinal deformity in the future?
Explanation
More than than 90% of preadolescent children who sustain a significant spinal cord injury subsequently develop scoliosis. Conversely, progressive paralytic spinal deformity is uncommon in the postadolescent patient. Bracing has not been shown to be effective in the prevention of scoliosis in the preadolescent patient with spinal cord injury.
REFERENCES: Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411.
Dearolf WW III, Betz RR. Vogl LC, et al: Scoliosis in pediatric spinal cord-injured patients. J Pediatr Orthop 1990;10:214-218.
Mehta S, Betz RR. Mulcahey MJ, et al: Effect of bracing on paralytic scoliosis secondary to spinal cord injury. J Spinal Cord Med 2004;27:S88-S92.
REFERENCES: Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411.
Dearolf WW III, Betz RR. Vogl LC, et al: Scoliosis in pediatric spinal cord-injured patients. J Pediatr Orthop 1990;10:214-218.
Mehta S, Betz RR. Mulcahey MJ, et al: Effect of bracing on paralytic scoliosis secondary to spinal cord injury. J Spinal Cord Med 2004;27:S88-S92.
Question 68High Yield
The most common risk factors for stress fractures is:
Explanation
Numerous risk factors for stress fracture exist. Most commonly, the scenario is doing âtoo much too soon.â Survey data have shown 86% of runners suffering stress fracture have had a change in duration, frequency, or intensity of training immediately prior to injury. The best independent predictors for stress fracture development in women appear to be age of menarche and calf girth
Question 69High Yield
A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management?
Explanation
Nonsurgical management of OCD of the talus in skeletally immature individuals frequently results in a fairly rapid decrease in symptoms, but radiographic abnormalities can frequently be found even 6 months after treatment. Spontaneous resolution of this condition is rare. Hyperbaric oxygen treatment has not been shown to be beneficial for this condition. Progression of the condition to the point of requiring ankle fusion is rare.
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
Question 70High Yield
Figure 1 is the clinical photograph of an 11-year-old otherwise healthy boy who presents to the emergency department following 3 days of progressive left lateral ankle pain, difficulty bearing weight, swelling, and fever. He has a temperature of 102°F and other vitals are normal. He denies other areas of pain. He tolerates gentle ankle motion, and has exquisite point tenderness overlying the region of the distal fibular metaphysis. Radiographs of the ankle are normal. CRP is 32 mg/dL, ESR is 17, WBC count is 10.4. An MRI (Figure

Explanation
■
The clinical photograph and MRI image demonstrate focal swelling and a subperiosteal fluid collection, consistent with osteomyelitis and subperiosteal abscess. Appropriate management includes surgical drainage and antibiotics. Beginning antibiotics are both part of the treatment process, prompt identification of the subperiosteal abscess and decompression is a critical step. Neither waiting on cultures nor outpatient treatment provide sufficient treatment for the abscess. Infectious disease consultation may be utilized for antibiotic guidance; however, surgical management is necessary and takes priority.
■
The clinical photograph and MRI image demonstrate focal swelling and a subperiosteal fluid collection, consistent with osteomyelitis and subperiosteal abscess. Appropriate management includes surgical drainage and antibiotics. Beginning antibiotics are both part of the treatment process, prompt identification of the subperiosteal abscess and decompression is a critical step. Neither waiting on cultures nor outpatient treatment provide sufficient treatment for the abscess. Infectious disease consultation may be utilized for antibiotic guidance; however, surgical management is necessary and takes priority.
Question 71High Yield
Figures 1 and 2 are the radiographs of a 5-year-old boy who was treated for a nondisplaced ulna fracture. Eight months later, he complains of a painful prominence over the elbow, causing pain with direct trauma during activity, occurring for several months. What is the best next step in the management of this patient?

Explanation
■
The images are of a chronic, missed Monteggia lesion. MRI demonstrates that the head is still concave, so reconstruction is still feasible. In late deformity, the ulna has to be overcorrected to pull the radial head back into appropriate alignment, making up for the elongation of the previously torn interosseous ligament, and stabilizing it. Osteotomy of the radius is not indicated, as there is no deformity present.
Excision of the radial head is inappropriate for a traumatic condition such as a Monteggia, which will continue to develop radial-ulnar mismatch and progressive wrist and elbow deformities if this is done while significant growth remains. Reconstruction is preferable in this case to salvage.
Annular ligament reconstruction alone will not restore stability in this injury; persistent deformity of the ulna is present.
■
The images are of a chronic, missed Monteggia lesion. MRI demonstrates that the head is still concave, so reconstruction is still feasible. In late deformity, the ulna has to be overcorrected to pull the radial head back into appropriate alignment, making up for the elongation of the previously torn interosseous ligament, and stabilizing it. Osteotomy of the radius is not indicated, as there is no deformity present.
Excision of the radial head is inappropriate for a traumatic condition such as a Monteggia, which will continue to develop radial-ulnar mismatch and progressive wrist and elbow deformities if this is done while significant growth remains. Reconstruction is preferable in this case to salvage.
Annular ligament reconstruction alone will not restore stability in this injury; persistent deformity of the ulna is present.
Question 72High Yield
Human calcium absorption occurs in the
Explanation
Dietary calcium is absorbed in the small intestine. This absorption is stimulated by 1,25 dihydroxyvitamin D3. Correct Answer: Small intestine
Question 73High Yield
Which of the following features is associated with type 2 osteoporosis:
Explanation
Type 1 osteoporosis is the most common form of osteoporosis and is found in women during postmenopausal years. Type 1 osteoporosis is related to estrogen deficiency rather than a problem in calcium intake or absorption.
Features of type 1 osteoporosis include:
Female to male ratio is 6:1
High turnover osteoporosis
Bone loss rate of 2% to 3% per year for 6 to 10 years following menopause
Trabecular bone is most affected
Related to estrogen deficiency rather than calcium intake
Type 2 osteoporosis, also called senile or involutional osteoporosis, is a low turnover osteoporosis and principally occurs in patients older than 75 years of age.
Features of type 2 osteoporosis include: Female to male ratio is 2:1
Patients older than 75 years of age
Low turnover osteoporosis
Trabecular and cortical bone affected
Associated with hip fractures
Related to a lifelong deficiency of calcium
Features of type 1 osteoporosis include:
Female to male ratio is 6:1
High turnover osteoporosis
Bone loss rate of 2% to 3% per year for 6 to 10 years following menopause
Trabecular bone is most affected
Related to estrogen deficiency rather than calcium intake
Type 2 osteoporosis, also called senile or involutional osteoporosis, is a low turnover osteoporosis and principally occurs in patients older than 75 years of age.
Features of type 2 osteoporosis include: Female to male ratio is 2:1
Patients older than 75 years of age
Low turnover osteoporosis
Trabecular and cortical bone affected
Associated with hip fractures
Related to a lifelong deficiency of calcium
Question 74High Yield
A 63-year-old man has long-standing type 2 diabetes. He has had associated ongoing neuropathy for approximately 5 years. He now reports a red, hot, swollen right foot for the past 2 days. You place him supine in your office with the foot elevated for 30 minutes. You return to see that the redness has dissipated. What is the most likely diagnosis?
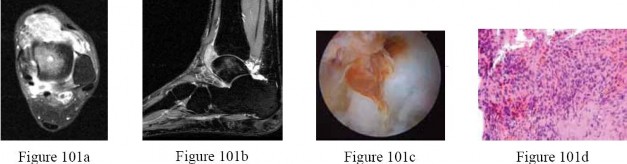
Explanation
Charcot arthropathy is a progressive condition of the musculoskeletal system that is characterized by joint dislocations, pathologic fractures, and debilitating deformities. This disorder results in progressive destruction of bone and soft tissues at weight-bearing joints; in its most severe form, it may cause significant disruption of the bony architecture. In patients with diabetes, the incidence of acute Charcot arthropathy of the foot and ankle ranges from 0.15% to 2.5%. Acute Charcot arthropathy almost always appears with signs of inflammation. Profound unilateral swelling, an increase in local skin temperature (generally, an increase of 3° to 7° above the nonaffected foot’s skin temperature), erythema,joint effusion, and bone resorption in an insensate foot are present. These characteristics, in the presence of intact skin and a loss of protective
sensation, are often pathognomonic of acute Charcot arthropathy.Cellulitis is an infection of the skin and osteomyelitis is an infection of the bone; examination of the limb would remain unchanged after 30 minutes of elevation. Reynaud and Sjogren syndromes are rheumatologic conditions that do not have these symptoms.
CLINICAL SITUATION FOR QUESTIONS 101 THROUGH 103
A 27-year-old woman has had pain in her right ankle for 2 years. Examination reveals a slightly warmjoint, without erythema. Ankle range of motion is limited by pain.
Radiographs are unremarkable.Because management consisting of immobilization, nonsteroidal anti-inflammatory drugs, and physiotherapy has failed to provide relief, MRI scans are obtained and shown in Figures 101a and 101b.An intraoperative image and the histology are shown in Figures 101c and 101d.
---
sensation, are often pathognomonic of acute Charcot arthropathy.Cellulitis is an infection of the skin and osteomyelitis is an infection of the bone; examination of the limb would remain unchanged after 30 minutes of elevation. Reynaud and Sjogren syndromes are rheumatologic conditions that do not have these symptoms.
CLINICAL SITUATION FOR QUESTIONS 101 THROUGH 103
A 27-year-old woman has had pain in her right ankle for 2 years. Examination reveals a slightly warmjoint, without erythema. Ankle range of motion is limited by pain.
Radiographs are unremarkable.Because management consisting of immobilization, nonsteroidal anti-inflammatory drugs, and physiotherapy has failed to provide relief, MRI scans are obtained and shown in Figures 101a and 101b.An intraoperative image and the histology are shown in Figures 101c and 101d.
---
Question 75High Yield
A 14-year-old boy sustains an intercondylar fracture of the distal humerus. There is a single fracture line into the joint between the capitellum and the trochlea. The medial column of the distal humerus is comminuted, but the lateral column is not. All fragments are highly displaced. Neurovascular status is normal. The recommended treatment is:
Explanation
A posterior approach (Bryan-Morrey or olecranon osteotomy) will facilitate anatomic reduction and rigid fixation sufficient for early range of motion.
Prolonged traction and cast will result in an incomplete reduction and excessive stiffness. A cast alone will result in an incomplete reduction and excessive stiffness.
Rigid fixation with plates, rather than pins, is required to maintain reduction of these fractures and allow early range of motion.
An anterior approach will not allow adequate exposure of the distal humerus for articular fixation.
Prolonged traction and cast will result in an incomplete reduction and excessive stiffness. A cast alone will result in an incomplete reduction and excessive stiffness.
Rigid fixation with plates, rather than pins, is required to maintain reduction of these fractures and allow early range of motion.
An anterior approach will not allow adequate exposure of the distal humerus for articular fixation.
Question 76High Yield
C ardinal signs of evenomation include all of the following except:
Explanation
The cardinal signs of evenomation appear between 10 minutes and 4 hours after a person is bitten. The signs include fang marks, pain, swelling, and local necrosis. C yanosis is not considered a cardinal sign of evenomation.
Question 77High Yield
Figures 67a and 67b are the radiographs of a 58-year-old man who has a painful left shoulder. Three months ago he underwent an anatomic total shoulder arthroplasty (TSA) for glenohumeral osteoarthritis. He was doing some yardwork when he felt a pop in his shoulder. What is the most likely diagnosis?


Explanation
Rupture of the subscapularis tendon after TSA has been reported in 1% to 6% of patients. Rupture usually is attributable to stressful activity too soon after surgery or after certain tendon-lengthening procedures. There is usually weakness with internal rotation and increased external rotation. The subscapularis tendon and capsule provide anterior stability to the glenohumeral joint. On the axillary radiograph, the shoulder is clearly dislocated anteriorly. This is only 3 months after surgery; although infection may be a possible cause of this tendon rupture, there is no loosening of the prosthesis. An axillary nerve injury could allow inferior subluxation attributable to loss of deltoid tension and would not be the reason for anterior escape.
RECOMMENDED READINGS
4. Aldinger PR, Raiss P, Rickert M, Loew M. Complications in shoulder arthroplasty: an analysis of 485 cases. Int Orthop. 2010 Apr;34(4):517-24. doi: 10.1007/s00264-009-0780-7. Epub 2009 Apr 28.
[PubMed PMID: 19396634.](http://www.ncbi.nlm.nih.gov/pubmed/19396634)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19396634)
5. [Miller BS, Joseph TA, Noonan TJ, Horan MP, Hawkins RJ. Rupture of the subscapularis tendon after shoulder arthroplasty: diagnosis, treatment, and outcome. J Shoulder Elbow Surg. 2005 Sep-Oct;14(5):492-6. PubMed PMID: 16194740. ](http://www.ncbi.nlm.nih.gov/pubmed/16194740)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16194740)
RECOMMENDED READINGS
4. Aldinger PR, Raiss P, Rickert M, Loew M. Complications in shoulder arthroplasty: an analysis of 485 cases. Int Orthop. 2010 Apr;34(4):517-24. doi: 10.1007/s00264-009-0780-7. Epub 2009 Apr 28.
[PubMed PMID: 19396634.](http://www.ncbi.nlm.nih.gov/pubmed/19396634)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19396634)
5. [Miller BS, Joseph TA, Noonan TJ, Horan MP, Hawkins RJ. Rupture of the subscapularis tendon after shoulder arthroplasty: diagnosis, treatment, and outcome. J Shoulder Elbow Surg. 2005 Sep-Oct;14(5):492-6. PubMed PMID: 16194740. ](http://www.ncbi.nlm.nih.gov/pubmed/16194740)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16194740)
Question 78High Yield
An 18-month-old boy is brought to your office for a clawing deformity of his right hand. The parents inform you that he was born full term after a difficult delivery complicated by shoulder dystocia. The boy weighed 9½ lbs at birth. The child had a brief episode of apnea with an APGAR score of 5 at birth and needed resuscitation and admission to the natal intensive care unit. Parents recall having noted a bump on his right clavicle, which was tender and was diagnosed as clavicle fracture. They also noticed a week later that the child did not flex the fingers of his right hand. The neonatologist had informed them that the
fracture is managed conservatively and the absence of finger flexion is due to the fracture and shall recover. They were warned that the recovery can be prolonged and can take up to 2 years. The boy has grown well and has achieved his milestones on time. His immunization is complete for his age.
You find a healthy, playful boy who tends to use his left hand to reach for objects. His right hand has extension at all the metacarpophalangeal (MC P) joints of the fingers while his proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints are flexed. His thumb is an adducted position and it is difficult to passively bring it to full abduction. There is obvious wasting of the hand and forearm. The child is able to move the arm well with no abnormalities noticed at the shoulder, elbow, and the wrist. The x-ray of his chest shows a healed clavicle fracture with no evidence of diaphragmatic paralysis. There is no evidence of Horner Syndrome and the grasp reflex is absent.
The diagnosis of this boyâs condition is:
fracture is managed conservatively and the absence of finger flexion is due to the fracture and shall recover. They were warned that the recovery can be prolonged and can take up to 2 years. The boy has grown well and has achieved his milestones on time. His immunization is complete for his age.
You find a healthy, playful boy who tends to use his left hand to reach for objects. His right hand has extension at all the metacarpophalangeal (MC P) joints of the fingers while his proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints are flexed. His thumb is an adducted position and it is difficult to passively bring it to full abduction. There is obvious wasting of the hand and forearm. The child is able to move the arm well with no abnormalities noticed at the shoulder, elbow, and the wrist. The x-ray of his chest shows a healed clavicle fracture with no evidence of diaphragmatic paralysis. There is no evidence of Horner Syndrome and the grasp reflex is absent.
The diagnosis of this boyâs condition is:
Explanation
This is a case of obstetric brachial plexus injury involving the C 8, T1 roots (Klumpke Palsy). Erbâs palsy involves upper roots only. C ombined nerve injuries can present in a similar fashion; however, low ulnar and median nerve lesions will not have weakness of flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS).
History of large baby, shoulder dystocia and clavicle fracture point to a difficult labor. The most common type of brachial plexus injury related to birth is Erbâs palsy, which is usually associated with a breech presentation. Isolated Klumpkeâs palsy is rare, and involvement of C 8, T1 usually occurs as part of global plexus injury.
History of large baby, shoulder dystocia and clavicle fracture point to a difficult labor. The most common type of brachial plexus injury related to birth is Erbâs palsy, which is usually associated with a breech presentation. Isolated Klumpkeâs palsy is rare, and involvement of C 8, T1 usually occurs as part of global plexus injury.
Question 79High Yield
A 22-year-old male soccer player reports left hip and groin pain. He states that symptoms began before a preseason tournament but have worsened steadily for the past 2 weeks. He denies any recent fever or sickness and is otherwise healthy. Examination reveals tenderness over the symphysis pubis and pain with resisted rectus abdominus testing. Radiographs are negative. What is the next step in the proper management of this patient?
Explanation
DISCUSSION: Appropriate management of osteitis pubis includes rest, nonsteroidal anti-inflammatory drugs, directed rehabilitation, and gradual return to sports. Lack of fever or chills excludes osteomyelitis as a source of pain. Examination with tenderness over the symphysis pubis and pain with resisted rectus abdominus testing is consistent with osteitis pubis as opposed to a sports hernia, where a patient would be tender in the abdomen, not the pubis. There is no symphyseal instability that would require symphyseal plating.
REFERENCES: Fricker PA, Taunton JE, Ammann W: Osteitis pubis in athletes. Sports Med 1991 ;12:266-
2010 Sports Medicine Examination Answer Book * 65
279.
Williams PR, Thomas DP, Downes EM: Osteitis pubis and instability of the pubic symphysis: When nonoperative measures fail. Am J Sports Med 2000;28:350-355.
REFERENCES: Fricker PA, Taunton JE, Ammann W: Osteitis pubis in athletes. Sports Med 1991 ;12:266-
2010 Sports Medicine Examination Answer Book * 65
279.
Williams PR, Thomas DP, Downes EM: Osteitis pubis and instability of the pubic symphysis: When nonoperative measures fail. Am J Sports Med 2000;28:350-355.
Question 80High Yield
Figures 1 and 2 are the T2-weighted MR images of a 54-year-old woman with medial knee pain and catching of 6 months’ duration. Which treatment option is most likely to be associated with a favorable outcome?

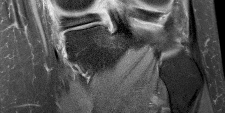
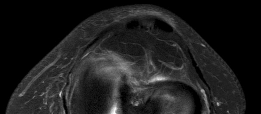
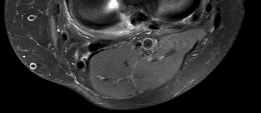
Explanation
MR images reveal a posterior horn root tear of the medial meniscus. LaPrade and associates found that outcomes after posterior meniscal root repair significantly improved postoperatively and patient satisfaction was high, regardless of age or meniscal laterality. Patients aged <50 years had outcomes similar to those of patients ≥50 years, as did patients who underwent medial versus lateral root repair. In patients undergoing pullout fixation for posterior medial meniscus root tear, Chung and associates (in “Pullout Fixation of Posterior Medial Meniscus Root Tears”) found that patients with decreased meniscus extrusion at postoperative 1 year have more favorable clinical scores and radiographic findings at midterm follow-up than those with increased extrusion at 1 year. Krych and associates found that nonoperative treatment of medial meniscus posterior horn root tears is associated with poor clinical outcome, worsening arthritis, and a relatively high rate of arthroplasty at 5-year follow-up. Reconstruction would have no role _in the setting of a reparable meniscal root tear._
Question 81High Yield
Figures 7a and 7b show the wound and radiograph
2. of a 44-year-old man who underwent plating for a
3. closed fracture of his tibia 7 months ago. The
4. wound has been draining for 4 months, and cultures
5. are positive for Staphylococcus aureus. In addition
6. to antibiotics, metal removal, and debridement,
7. treatment should include
8. 1- electrical stimulation and casting.
9. 2- soft-tissue coverage and replating with a bone graft.
10. 3- bone grafting, soft-tissue coverage, and application
11. of a cast.
12. 4- external fixation, staged soft-tissue coverage, and
13. bone grafting.
14. 5- intramedullary rodding, staged soft-tissue coverage,
15. and bone grafting.
2. of a 44-year-old man who underwent plating for a
3. closed fracture of his tibia 7 months ago. The
4. wound has been draining for 4 months, and cultures
5. are positive for Staphylococcus aureus. In addition
6. to antibiotics, metal removal, and debridement,
7. treatment should include
8. 1- electrical stimulation and casting.
9. 2- soft-tissue coverage and replating with a bone graft.
10. 3- bone grafting, soft-tissue coverage, and application
11. of a cast.
12. 4- external fixation, staged soft-tissue coverage, and
13. bone grafting.
14. 5- intramedullary rodding, staged soft-tissue coverage,
15. and bone grafting.
Explanation
1.
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Patzakis MJ: Management of osteomyelitis, in Operative Orthopaedics. Philadelphia, PA, JB Lippincott, 1993, p 3335.
#
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Patzakis MJ: Management of osteomyelitis, in Operative Orthopaedics. Philadelphia, PA, JB Lippincott, 1993, p 3335.
#
Question 82High Yield
A surgeon prepares a medial gastrocnemius rotational flap to cover a medial proximal tibia defect at the
time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
Explanation
The medial sural arteries vascularize the gastrocnemius, plantaris, and soleus muscles proximally. These arteries arise from the popliteal artery. If this artery is not adequately mobilized, a gastrocnemius soleus flap can be devascularized.
Question 83High Yield
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?
Explanation
Internal impingement of the shoulder is now a well-recognized cause of shoulder pain in the throwing athlete. First described by Walch and associates, it involves contact of the rotator cuff and labrum in the maximally externally rotated and abducted shoulder, such as in the late cocking phase of the throwing motion. Schickendantz and associates have shown this contact to be physiologic in most patients and becoming pathologic with repetitive overhead activity.
REFERENCES: Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
McFarland EG, Hsu CY, Neira C, O’Neil O: Internal impingement of the shoulder: A clinical and arthroscopic analysis. J Shoulder Elbow Surg 1999;8:458-460.
REFERENCES: Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
McFarland EG, Hsu CY, Neira C, O’Neil O: Internal impingement of the shoulder: A clinical and arthroscopic analysis. J Shoulder Elbow Surg 1999;8:458-460.
Question 84High Yield
Recurrence of osteochondroma is likely if:
Explanation
The cartilaginous portion of an osteochondroma is the neoplastic part; its complete excision is essential to avoid recurrences.
Question 85High Yield
A 33-year-old woman reports a 3-month history of pain in both feet while running. Examination reveals bilateral point tenderness over the plantar fascia at its origin, and the pain is accentuated when the ankle is dorsiflexed. Management should consist of
Explanation
This question refers to plantar fascitis. Heel spurs are noted in approximately 50% of the cases of subcalcaneal pain syndrome. In this patient, diagnosis should rule out lumbar radiculopathy since the symptoms are bilateral.
The most common site for heel pain is where the plantar fascia and intrinsic muscles arise from the medial calcaneal tuberosity on the anteromedial aspect of the heel.
First line treatment is NSAID’s, Physical therapy involving heel cord stretching and an orthosis. Second line therapy after these treatments are unsuccessful involve steroid injection and plaster immobilization. Surgical intervention should be the very last choice in the options given.
The most common site for heel pain is where the plantar fascia and intrinsic muscles arise from the medial calcaneal tuberosity on the anteromedial aspect of the heel.
First line treatment is NSAID’s, Physical therapy involving heel cord stretching and an orthosis. Second line therapy after these treatments are unsuccessful involve steroid injection and plaster immobilization. Surgical intervention should be the very last choice in the options given.
Question 86High Yield
A 23-year-old national team rower reports pain over the radial dorsum of the forearm that is made worse with flexion and extension of the wrist during competition. His primary physician initially diagnosed de Quervain’s tenosynovitis, and a subsequent corticosteroid injection into the first dorsal compartment at the wrist provided no relief. The patient continues to report pain and audible crepitus that is noted 5 cm proximal to the wrist joint, on the radial aspect. What structures are involved in the continued pathology?
Explanation
DISCUSSION: Intersection syndrome is also known as “squeakers wrist,” “oarsmen wrist,” and crossover tendinitis. It occurs where the first and second dorsal wrist compartment structures pass over one another, resulting in fibrosis, muscular changes, and inflammation of the bursa in this area. The structures involved are the abductor pollicis longus and extensor pollicis brevis (first dorsal compartment) that pass across the second compartment structures (extensor carpi radialis brevis and extensor carpi radialis longus). An audible “squeak” is occasional y heard at the intersection point, which is approximately 4 to 5 cm proximal to the proximal dorsal wrist crease.
REFERENCES: Grundberg AB, Reagan DS: Pathologic anatomy of the forearm: Intersection syndrome. J Hand Surg Am 1985; 10:299-302.
Thorson E, Szabo RM: Common tendinitis problems in the hand and forearm. Orthop Clin North Am 1992;23:65-74.
Williams JG: Surgical management of traumatic non-infective tenosynovitis of the wrist extensors. J Bone Joint Surg Br 1977;59:408-410.
Wood MB, Dobyns JH: Sports-related extraarticular wrist syndromes. Clin Orthop Relat Res 1986;202:93-102.
DISCUSSION: Intersection syndrome is also known as “squeakers wrist,” “oarsmen wrist,” and crossover tendinitis. It occurs where the first and second dorsal wrist compartment structures pass over one another, resulting in fibrosis, muscular changes, and inflammation of the bursa in this area. The structures involved are the abductor pollicis longus and extensor pollicis brevis (first dorsal compartment) that pass across the second compartment structures (extensor carpi radialis brevis and extensor carpi radialis longus). An audible “squeak” is occasional y heard at the intersection point, which is approximately 4 to 5 cm proximal to the proximal dorsal wrist crease.
REFERENCES: Grundberg AB, Reagan DS: Pathologic anatomy of the forearm: Intersection syndrome. J Hand Surg Am 1985; 10:299-302.
Thorson E, Szabo RM: Common tendinitis problems in the hand and forearm. Orthop Clin North Am 1992;23:65-74.
Williams JG: Surgical management of traumatic non-infective tenosynovitis of the wrist extensors. J Bone Joint Surg Br 1977;59:408-410.
Wood MB, Dobyns JH: Sports-related extraarticular wrist syndromes. Clin Orthop Relat Res 1986;202:93-102.
Question 87High Yield
A 36-year-old softball player sustains a shoulder dislocation making a diving catch. The shoulder is successfully reduced in the emergency department. A postreduction MRI is shown in Figure 35. What anatomic lesion is a result of the dislocation?
Explanation
DISCUSSION: The MRI scan reveals a HAGL lesion. It more commonly affects older patients and is associated with more violent trauma.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 53-54.
Bokor DJ, Conboy VB, Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the
glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br 1999;81:93-96. Question 36
An 18-year-old woman injures her left knee playing soccer. At the time of anterior cruciate ligament (ACL) reconstruction, she was noted to have an irreparable posterior horn medial meniscus tear. Partial meniscectomy will have what primary effect?
1. #### Increase medial compartment peak loads
2. #### Increase medial compartment contact area
3. #### Decrease in situ forces in the ACL graft
4. #### Decrease anterior tibial translation
5. #### Increase posterior tibial translation PREFERRED RESPONSE: 1
DISCUSSION: The medial meniscus distributes force through the medial compartment. Peak loads in the affected compartment are increased by partial and complete meniscectomy. The posterior horn of the medial meniscus is also an important secondary restraint to anterior tibial translation in the ACL-deficient knee. In situ forces in the reconstructed ACL are increased with loss of the posterior horn of the medial meniscus.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 199-201.
Greis PE, Bardana DD, Holmstrom MC, et al: Meniscal injury: I. Basic science and evaluation. J Am Acad Orthop Surg 2002; 10:168-176.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 53-54.
Bokor DJ, Conboy VB, Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the
glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br 1999;81:93-96. Question 36
An 18-year-old woman injures her left knee playing soccer. At the time of anterior cruciate ligament (ACL) reconstruction, she was noted to have an irreparable posterior horn medial meniscus tear. Partial meniscectomy will have what primary effect?
1. #### Increase medial compartment peak loads
2. #### Increase medial compartment contact area
3. #### Decrease in situ forces in the ACL graft
4. #### Decrease anterior tibial translation
5. #### Increase posterior tibial translation PREFERRED RESPONSE: 1
DISCUSSION: The medial meniscus distributes force through the medial compartment. Peak loads in the affected compartment are increased by partial and complete meniscectomy. The posterior horn of the medial meniscus is also an important secondary restraint to anterior tibial translation in the ACL-deficient knee. In situ forces in the reconstructed ACL are increased with loss of the posterior horn of the medial meniscus.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 199-201.
Greis PE, Bardana DD, Holmstrom MC, et al: Meniscal injury: I. Basic science and evaluation. J Am Acad Orthop Surg 2002; 10:168-176.
Question 88High Yield
Figures below show the clinical photograph and radiograph obtained from a 62-year-old man who has
deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?
deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?

Explanation
Figure 1 reveals an external rotation deformity of the right lower extremity. This deformity can have numerous causes, including extra-articular deformity. Figure 2 reveals a loose, subsided femoral component. Femoral stems typically subside into retroversion due to proximal femoral biomechanics, which cause a compensatory external rotation deformity. The combined findings from both images suggest an external rotation deformity most likely related to subsidence into retroversion.
Question 89High Yield
Scoliosis in Marfan syndrome, as compared to idiopathic scoliosis, is characterized by which of the following:
Explanation
Scoliosis curves are much more likely to begin in the juvenile period than idiopathic scoliosis.
There is no significant difference in the likelihood of left thoracic curves in Marfan syndrome. Brace treatment is less likely to be successful in Marfan syndrome than in idiopathic scoliosis. Marfan patients with scoliosis are more likely to have back pain.
Marfan curves are more likely to progress in adulthood.
There is no significant difference in the likelihood of left thoracic curves in Marfan syndrome. Brace treatment is less likely to be successful in Marfan syndrome than in idiopathic scoliosis. Marfan patients with scoliosis are more likely to have back pain.
Marfan curves are more likely to progress in adulthood.
Question 90High Yield
An 88-year-old nursing home resident is seen in the emergency department after a fall. At the time of admission, physical examination of the affected extremity reveals absent pulses and inadequate capillary refill. A radiograph is seen in Figure 48. Appropriate management includes which of the following?
Explanation
The patient has a Vancouver type B3 periprosthetic femur fracture (fracture around a total hip prosthesis with a loose stem and poor proximal bone stock). This type of periprosthetic fracture necessitates revision of the femoral component as well as fracture fixation. This patient has diminished blood flow in the extremity that necessitates emergent vascular surgical evaluation.
REFERENCES: Brady OH, Garbuz DS, Masri BA, et al: Classification of the hip. Orthop Clin North Am 1999;30;215-220,
Klein GR, Parvizi J, Rapuri V, et al: Proximal femoral replacement for the treatment of periprosthetic fractures. J
Bone Joint Surg Am 2005;87:1777-1781. Question 49
An otherwise healthy 58-year-old woman reports hip pain after undergoing total hip arthroplasty 8 months ago. She gives a history of prolonged wound drainage after surgery treated with antibiotics.
Hip aspiration is positive for methicillin-resistant coagulase-negative staphylococcus. Appropriate management at this point includes which of the following?
1. Arthroscopic irrigation followed by appropriate antibiotic treatment
2. Treatment with 6 weeks of IV vancomycin and oral rifampin
3. Treatment with 6 weeks of IV vancomycin and oral rifampin, followed by indefinite oral antibiotic suppression
4. Open debridement with exchange of the polyethylene insert, followed by appropriate antibiotic
treatment
5. Open debridement with removal of the implants and insertion of an antibiotic spacer
PREFERRED RESPONSE: 5
DISCUSSION: The patient has a late chronic periprosthetic infection. The history points to a missed postoperative infection where the patient was treated with antibiotics for prolonged wound drainage. A low virulent organism, such as coagulase-negative staphylococcus, is often the pathogen. In an otherwise healthy patient with a reasonable life expectancy, the goal of treatment should be cure of the infection. Treatment for late chronic infection requires removal of the implants. Treatment with antibiotics alone, or debridement without removal of the implants is generally unsuccessful. Controversy exists regarding one- stage treatment with immediate reimplantation versus two-stage treatment with delayed reimplantation. Generally, a higher cure rate is achieved with a two-stage reimplantation (approximately 90% to 93%) than with one-stage reimplantation (75% to 80%).
REFERENCES: Hanssen AD, Spangehl MJ: Treatment of the infected hip replacement. Clin Orthop Relat Res 2004;420:63-71.
Isiklar ZU, Demirors H, Akpinar S, et al: Two-stage treatment of chronic staphylococcal orthopaedic
implant-related infections using vancomycin impregnated PMMA spacer and rifampin containing antibiotic protocol. Bull Hosp Jt Dis 1999;58:79-85.
REFERENCES: Brady OH, Garbuz DS, Masri BA, et al: Classification of the hip. Orthop Clin North Am 1999;30;215-220,
Klein GR, Parvizi J, Rapuri V, et al: Proximal femoral replacement for the treatment of periprosthetic fractures. J
Bone Joint Surg Am 2005;87:1777-1781. Question 49
An otherwise healthy 58-year-old woman reports hip pain after undergoing total hip arthroplasty 8 months ago. She gives a history of prolonged wound drainage after surgery treated with antibiotics.
Hip aspiration is positive for methicillin-resistant coagulase-negative staphylococcus. Appropriate management at this point includes which of the following?
1. Arthroscopic irrigation followed by appropriate antibiotic treatment
2. Treatment with 6 weeks of IV vancomycin and oral rifampin
3. Treatment with 6 weeks of IV vancomycin and oral rifampin, followed by indefinite oral antibiotic suppression
4. Open debridement with exchange of the polyethylene insert, followed by appropriate antibiotic
treatment
5. Open debridement with removal of the implants and insertion of an antibiotic spacer
PREFERRED RESPONSE: 5
DISCUSSION: The patient has a late chronic periprosthetic infection. The history points to a missed postoperative infection where the patient was treated with antibiotics for prolonged wound drainage. A low virulent organism, such as coagulase-negative staphylococcus, is often the pathogen. In an otherwise healthy patient with a reasonable life expectancy, the goal of treatment should be cure of the infection. Treatment for late chronic infection requires removal of the implants. Treatment with antibiotics alone, or debridement without removal of the implants is generally unsuccessful. Controversy exists regarding one- stage treatment with immediate reimplantation versus two-stage treatment with delayed reimplantation. Generally, a higher cure rate is achieved with a two-stage reimplantation (approximately 90% to 93%) than with one-stage reimplantation (75% to 80%).
REFERENCES: Hanssen AD, Spangehl MJ: Treatment of the infected hip replacement. Clin Orthop Relat Res 2004;420:63-71.
Isiklar ZU, Demirors H, Akpinar S, et al: Two-stage treatment of chronic staphylococcal orthopaedic
implant-related infections using vancomycin impregnated PMMA spacer and rifampin containing antibiotic protocol. Bull Hosp Jt Dis 1999;58:79-85.
Question 91High Yield
A 46-year-old woman sustains an extra-articular fracture of the distal radius and undergoes open reduction and internal fixation with a volar plate and screw construct. During postoperative recovery from this injury, what benefit does formal physical therapy have as compared to a patient-guided home exercise program?
Explanation
There are no significant benefits demonstrated with formal physical therapy following distal radius fracture ORIF compared to a patient-guided home exercise program.
The reference by Wakefield and McQueen is a randomized controlled trial of 96 patients, comparing formal hand physiotherapy to a home exercise regimen.
There was no difference in grip strength, pronation/supination, radial/ulnar deviation, or hand function. The authors concluded that there were no significant benefits to formal physiotherapy.
The study by Souer et al is a level I study evaluating formal therapy and patient-guided exercise program for patients who underwent ORIF of a distal radius fracture with a volar plate and screw construct. This study showed a significant decrease in wrist ROM and grip strength with formal therapy. There were no differences in arm-specific disability (DASH score) at any time point.
The reference by Wakefield and McQueen is a randomized controlled trial of 96 patients, comparing formal hand physiotherapy to a home exercise regimen.
There was no difference in grip strength, pronation/supination, radial/ulnar deviation, or hand function. The authors concluded that there were no significant benefits to formal physiotherapy.
The study by Souer et al is a level I study evaluating formal therapy and patient-guided exercise program for patients who underwent ORIF of a distal radius fracture with a volar plate and screw construct. This study showed a significant decrease in wrist ROM and grip strength with formal therapy. There were no differences in arm-specific disability (DASH score) at any time point.
Question 92High Yield
Which of the following leg muscles often has its own fascial envelope (separate compartment):
Explanation
Of the four compartments, the deep posterior compartment is the most difficult to release. The surgeon must release the soleus muscle from the tibia to decompress the deep posterior compartment.
The tibialis posterior muscle often has its own fascial sheath in the deep posterior compartment. When a surgeon releases the deep posterior compartment, this fascial sheath (if present) should be released.
The tibialis posterior muscle often has its own fascial sheath in the deep posterior compartment. When a surgeon releases the deep posterior compartment, this fascial sheath (if present) should be released.
Question 93High Yield
Figures 74a and 74b are the MR images of a 36-year-old man with a 3-month history of excruciating left leg pain. Which finding upon examination would be most consistent with the MR images?


Explanation
The MR images show a classic posterolateral disk herniation at L5-S1. This location affects the traversing nerve root (at L5-S1, the S1 nerve root). The S1 dermatome innervates the plantar aspect of the foot and primarily contributes to ankle plantar flexion and foot eversion. Hip adduction and quadriceps are controlled via the obturator nerve L2-4 innervation, and ankle dorsiflexion is controlled via L4 or L5 innervation. The L2 and L3 dermatomes provide sensation in the anteromedial thigh, L4 provides sensation along the anterolateral leg down to the medial malleolus, L5 provides sensation along the anterolateral leg to the dorsum of the foot, and S1 provides sensation along the posterior leg to the lateral foot.
RECOMMENDED READINGS
14. [Rhee JM, Schaufele M, Abdu WA. Radiculopathy and the herniated lumbar disk: controversies regarding pathophysiology and management. Instr Course Lect.2007;56:287-99. Review. PubMed PMID: 17472314. ](http://www.ncbi.nlm.nih.gov/pubmed/17472314)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17472314)
15. Mixter WJ, Barr JS. Rupture of the intervertebral disk with involvement of the spinal canal. N Engl J Med. 1934: 211: 210-5.
RECOMMENDED READINGS
14. [Rhee JM, Schaufele M, Abdu WA. Radiculopathy and the herniated lumbar disk: controversies regarding pathophysiology and management. Instr Course Lect.2007;56:287-99. Review. PubMed PMID: 17472314. ](http://www.ncbi.nlm.nih.gov/pubmed/17472314)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17472314)
15. Mixter WJ, Barr JS. Rupture of the intervertebral disk with involvement of the spinal canal. N Engl J Med. 1934: 211: 210-5.
Question 94High Yield
A 72-year-old man with a history of Parkinson’s disease, stable coronary artery disease, and mild renal insufficiency is seen for hip arthroplasty. Which of the following is considered the most appropriate bearing of choice?
Explanation
The most appropriate bearing of those listed would be a large diameter metal head on cross-linked polyethylene. Because of the renal insufficiency, metal-on-metal should be avoided because metal ions are renally excreted. Ceramic-on-ceramic implants are not necessary in this patient because of the patient’s limited activity and life expectancy, as well as the downside of increased cost, the small but definite risk of ceramic fracture, and the increased technical demands of inserting ceramic implants. A highly cross-linked liner is favored to allow for maximum head size as the patient may be at increased risk of dislocation because of his neurologic disorder.
REFERENCES: Bragdon CR, Greene ME, Freiberg AA, et al: Radiostereometric analysis comparison of wear of highly cross-linked polyethylene against 36- vs 28-mm femoral heads. J Arthroplasty 2007;22:125-129.
MacDonald SJ: Metal-on-metal total hip arthroplasty: The concerns. Clin Orthop Relat Res 2004;429:86- 93.
REFERENCES: Bragdon CR, Greene ME, Freiberg AA, et al: Radiostereometric analysis comparison of wear of highly cross-linked polyethylene against 36- vs 28-mm femoral heads. J Arthroplasty 2007;22:125-129.
MacDonald SJ: Metal-on-metal total hip arthroplasty: The concerns. Clin Orthop Relat Res 2004;429:86- 93.
Question 95High Yield
-is the initial lateral radiograph of the foot of a 55-year-old woman who felt a pop in her left foot as she stepped off the curb. She subsequently had severe heel pain and could not bear weight.Examination in the emergency department revealed a bony prominence over the posterior aspect of the heel with blanching of the surrounding skin. What is the most appropriate orthopaedic management?

Explanation
No detailed explanation available.
Question 96High Yield
A 24-year-old female soccer player has had lateral joint line pain and a recurrent effusion in the left knee after sustaining a twisting injury 6 weeks ago. She reports that symptoms worsen with athletic activities. MRI scans are shown in Figures 2a through 2c. What is the most likely diagnosis?
Explanation
The MRI scans show the typical findings of a torn discoid lateral meniscus. The average transverse diameter of the lateral meniscus is 11 or 12 mm. A discoid lateral meniscus is suggested when three or more contiguous 5-mm sagittal sections on the MRI scan show continuity of the menicus between the anterior and posterior horns, or when two adjacent peripheral sagittal 5-mm sections show equal meniscal height. Normally the black “bow tie” would be seen on two contiguous sagittal sections. The presence of a discoid meniscus can be further confirmed if coronal views reveal increased width.
REFERENCES: Jordan MR: Lateral meniscal variants: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:191-200.
Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 625-630.
REFERENCES: Jordan MR: Lateral meniscal variants: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:191-200.
Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 625-630.
Question 97High Yield
What surgical technique has been associated with increased risk for recurrent dislocation after revision total hip arthroplasty?
Explanation
When addressing recurrent dislocation after total hip arthroplasty, surgical considerations that must be addressed include approach, soft-tissue tension, component positioning, impingement, head size, and acetabular liner profile. These considerations most often involve tensioning or augmentation of soft tissues, as in capsulorrhaphy or trochanteric advancement; correction of malpositioned components; use of larger femoral head sizes that increase motion before impingement; improving the head-to-neck ratio; and increasing femoral offset. The use of a larger-diameter acetabular component may lead to soft-tissue overgrowth around the liner, causing impingement and increasing the risk for recurrent dislocation.
Question 98High Yield
A 17-year-old football player is tackled with an opposing player's helmet hitting him hard in the abdomen. He is knocked backwards and suffers a diaphyseal femur fracture. He denies any loss of consciousness. Vital signs reveal a heart rate of 118, mean arterial pressure (MAP) of 68, and a respiration rate of 32 per minute. A FAST ultrasound study shows trace free fluid in the perisplenic space. A CBC taken prior to bolus IV fluids reveals a hematocrit of 48%, and a blood gas shows a lactate level of 1.8 and a base excess of -2.0. Which of the follow statements regarding the patient's hemodynamic status is correct?
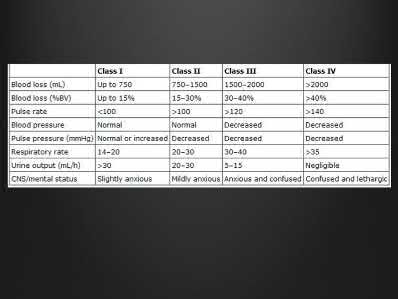
Explanation
Normal lactate levels or base excess indicate adequate tissue perfusion.
Hypovolemic shock leads to poor tissue perfusion due to inadequate flow or oxygenation. If a patient is in compensated shock (i.e. normal vital signs), there may be ongoing inadequate perfusion of some end-organs. Elevated lactate or a base deficit are markers of poor end-organ perfusion, thus when normalized indicate appropriate end-organ perfusion even if vital sign derangements persist.
Rossaint et al. wrote a comprehensive review article in 2006 in which they discuss principles of fluid management, coagulopathy, hypothermia and tissue oxygenation in hypovolemic shock. In addition to prolonged elevated lactate levels correlating to mortality, lactate levels (or base deficits) can be used to evaluate for compensated shock in the setting of normal hemodynamic status.
Illustration A shows the classification of hypovolemic shock. Note the percent of blood loss required for vital sign abnormalities.
Incorrect Answers:
Answer 1: While an arterial line is often helpful in the setting of
uncompensated hemodynamic shock, it would not be as important as measures of adequate tissue perfusion for ruling out compensated shock. Answer 2: The hematocrit is expected to stay normal for a short time even in the setting of massive blood loss. The hematocrit only changes once the patient has physiologic or iatrogenic fluid shifts in response to the blood loss. Answer 3: Vital sign derangements indicate uncompensated shock, but do not directly measure tissue perfusion or end-organ damage
Answer 5: Though uncommon, bleeding from isolated femur fractures can lead to Class II shock (blood loss 15-30%)
Hypovolemic shock leads to poor tissue perfusion due to inadequate flow or oxygenation. If a patient is in compensated shock (i.e. normal vital signs), there may be ongoing inadequate perfusion of some end-organs. Elevated lactate or a base deficit are markers of poor end-organ perfusion, thus when normalized indicate appropriate end-organ perfusion even if vital sign derangements persist.
Rossaint et al. wrote a comprehensive review article in 2006 in which they discuss principles of fluid management, coagulopathy, hypothermia and tissue oxygenation in hypovolemic shock. In addition to prolonged elevated lactate levels correlating to mortality, lactate levels (or base deficits) can be used to evaluate for compensated shock in the setting of normal hemodynamic status.
Illustration A shows the classification of hypovolemic shock. Note the percent of blood loss required for vital sign abnormalities.
Incorrect Answers:
Answer 1: While an arterial line is often helpful in the setting of
uncompensated hemodynamic shock, it would not be as important as measures of adequate tissue perfusion for ruling out compensated shock. Answer 2: The hematocrit is expected to stay normal for a short time even in the setting of massive blood loss. The hematocrit only changes once the patient has physiologic or iatrogenic fluid shifts in response to the blood loss. Answer 3: Vital sign derangements indicate uncompensated shock, but do not directly measure tissue perfusion or end-organ damage
Answer 5: Though uncommon, bleeding from isolated femur fractures can lead to Class II shock (blood loss 15-30%)
Question 99High Yield
Organisms survive on biosynthetiCsurfaces, such as total hips, because of:
Explanation
AntibiotiCresistance, the organismâs ability to form a glycocalyx or polysaccharide biofilm, and a slime layer enable the organism to survive on implants. This is one of the reasons why it is difficult to clear up an infection using only antibiotics
Question 100High Yield
2010 Pediatric Orthopaedic Examination Answer Book *15
Achondroplasia is caused by an abnormality of which of the following?
Achondroplasia is caused by an abnormality of which of the following?
Explanation
Achondroplasia results from mutation of the fibroblast growth factor receptor 3. Bone morphogenic proteins are regulators of growth differentiation and morphogenic embryology. Anomalies of this protein are seen in increasing defects in limbs distally. Parathyroid-related protein is seen in Jensen-type metaphyseal chondrodysplasia. Transforming growth factors and the morphogenic proteins affect the production of matrix.
REFERENCES: Leet Al, Chomey GS: The physis, in Cramer KE, Scherl SA, Einhom TA (eds): Orthopaedic Surgery Essentials: Pediatrics. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 327-332.
van der Eerden BC, Karperian M, Wit JM: Systemic and local regulators of the growth plate. Endocr Rev 2003;24:782-801.
Figure 12
REFERENCES: Leet Al, Chomey GS: The physis, in Cramer KE, Scherl SA, Einhom TA (eds): Orthopaedic Surgery Essentials: Pediatrics. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 327-332.
van der Eerden BC, Karperian M, Wit JM: Systemic and local regulators of the growth plate. Endocr Rev 2003;24:782-801.
Figure 12
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon