Orthopedic With Answer Pa Review | Dr Hutaif General Or -...
14 Apr 2026
76 min read
127 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic With Answer Pa Review | Dr Hutaif ...
00:00
Start Quiz
Question 1High Yield
A 17-year-old football player continues to have discomfort after sustaining a blow to his midthigh during a game 8 weeks ago. A plain radiograph is shown in Figure 13. What is the most appropriate management?
Explanation
The patient has myositis ossificans. Rest of the involved area is important to help limit the continued irritation of the muscle, but range-of-motion exercises are important to limit stiffness. While immobilization for 1 or 2 days following a muscle contusion is appropriate, longer periods of immobilization result in muscle atrophy and fibrosis. Injections and irradiation have not been found to be of benefit for myositis ossificans. Excision is rarely required, and if performed, it should not be performed prior to maturation of the lesion, which is a minimum of 6 months.
REFERENCES: Lipscomb AB, Thomas ED, Johnston RK: Treatment of myositis ossificans traumatica in athletes. Am J Sports Med 1976;4:111-120.
Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
Ryan JB, Wheeler JH, Hopkins WJ, et al: Quadriceps contusions: West Point update. Am J Sports Med 1991;19:299-304.
REFERENCES: Lipscomb AB, Thomas ED, Johnston RK: Treatment of myositis ossificans traumatica in athletes. Am J Sports Med 1976;4:111-120.
Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
Ryan JB, Wheeler JH, Hopkins WJ, et al: Quadriceps contusions: West Point update. Am J Sports Med 1991;19:299-304.
Question 2High Yield
If growth arrest is suspected after the fracture shown in the radiographs in Figures 17a through 17c, what is the most appropriate imaging modality to verify the presence of a physeal bar?



Explanation
Premature growth arrest of a physis may occur after fracture, infection, or ischemia. In the setting of fracture this is relatively rare, although certain physes have proven more susceptible than others. In the distal radius, premature growth arrest is more common after wide displacement, redisplacement, or manipulation after a fracture has begun to heal (> 7-10 days after injury). Arrest may take 6 to 12 months to become evident on radiographs and it may take even longer for a patient to experience pain or deformity, depending upon the rate of growth at the time of arrest. Surveillance should take place during the 6- to 12-month time frame with radiographs.
A physeal bar is difficult to rule in or out on radiographs because of natural undulations in the physis or a residual angular deformity after fracture that causes the physis to be less clearly visible. Often, the best clue that indicates physeal arrest after distal radius fracture is clinical prominence of the ulna head or increasing ulna-positive variance. The posteroanterior view of the wrist should be taken with the shoulder abducted to 90 degrees and elbow flexed to 90 degrees. This places the forearm in neutral rotation, and changes in ulnar variance can more accurately be detected. Comparison views of the other side may be warranted.
If a growth arrest is suspected, CT scan and MRI are both effective modalities for imaging the size and location of the bar. The bar is most easily detected on the T1-weighted MR images. Early, unossified cartilaginous bars also may be detected on some MRI sequences. MRI with 3D mapping functions is now used to map the size and location into an easy-to-visualize format, but the computer programs are not yet mainstream. A CT scan can demonstrate the bar but is not as acceptable because of the high dose of radiation (compared to MRI).
The physis has 3 main zones. The zone that is most important and susceptible to injury is the resting zone, where pluripotent chondrocytes reside. This layer is immediately adjacent to the epiphysis. If this layer is disrupted or ischemic, there is permanent growth arrest of that physis section. The central layer is the proliferative zone. The hypertrophic zone is the layer adjacent to the metaphysis and is subdivided into 3 layers: maturation, degeneration, and provisional calcification. The weakest link is the junction between the provisional calcification layer and the metaphysis. Most physeal fractures occur through this layer. Thus, growth arrest after fracture is rare because the level of injury typically is as far as possible from the delicate resting zone.
If growth arrest occurs after distal radius fracture, surgical intervention is tailored to the situation. If the child is young, an attempt at bar resection and interposition of fat or bone wax is appropriate. If a teenage child is asymptomatic and ulna variance is a few millimeters positive, simple ulna epiphysiodesis is appropriate. If there is deformity of the distal radius, corrective osteotomy may be best.
RECOMMENDED READINGS
6. [Abzug JM, Little K, Kozin SH. Physeal arrest of the distal radius. J Am Acad Orthop Surg. 2014 Jun;22(6):381-9. doi: 10.5435/JAAOS-22-06-381. Review. PubMed PMID: 24860134. ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860134)
7. [Craig JG, Cramer KE, Cody DD, Hearshen DO, Ceulemans RY, van Holsbeeck MT, Eyler WR. Premature partial closure and other deformities of the growth plate: MR imaging and three-dimensional modeling. Radiology. 1999 Mar;210(3):835-43. PubMed PMID: 10207489. ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10207489)
8. [Ecklund K, Jaramillo D. Patterns of premature physeal arrest: MR imaging of 111 children. AJR Am J Roentgenol. 2002 Apr;178(4):967-72. PubMed PMID: 11906884. ](http://www.ncbi.nlm.nih.gov/pubmed/11906884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11906884)
A physeal bar is difficult to rule in or out on radiographs because of natural undulations in the physis or a residual angular deformity after fracture that causes the physis to be less clearly visible. Often, the best clue that indicates physeal arrest after distal radius fracture is clinical prominence of the ulna head or increasing ulna-positive variance. The posteroanterior view of the wrist should be taken with the shoulder abducted to 90 degrees and elbow flexed to 90 degrees. This places the forearm in neutral rotation, and changes in ulnar variance can more accurately be detected. Comparison views of the other side may be warranted.
If a growth arrest is suspected, CT scan and MRI are both effective modalities for imaging the size and location of the bar. The bar is most easily detected on the T1-weighted MR images. Early, unossified cartilaginous bars also may be detected on some MRI sequences. MRI with 3D mapping functions is now used to map the size and location into an easy-to-visualize format, but the computer programs are not yet mainstream. A CT scan can demonstrate the bar but is not as acceptable because of the high dose of radiation (compared to MRI).
The physis has 3 main zones. The zone that is most important and susceptible to injury is the resting zone, where pluripotent chondrocytes reside. This layer is immediately adjacent to the epiphysis. If this layer is disrupted or ischemic, there is permanent growth arrest of that physis section. The central layer is the proliferative zone. The hypertrophic zone is the layer adjacent to the metaphysis and is subdivided into 3 layers: maturation, degeneration, and provisional calcification. The weakest link is the junction between the provisional calcification layer and the metaphysis. Most physeal fractures occur through this layer. Thus, growth arrest after fracture is rare because the level of injury typically is as far as possible from the delicate resting zone.
If growth arrest occurs after distal radius fracture, surgical intervention is tailored to the situation. If the child is young, an attempt at bar resection and interposition of fat or bone wax is appropriate. If a teenage child is asymptomatic and ulna variance is a few millimeters positive, simple ulna epiphysiodesis is appropriate. If there is deformity of the distal radius, corrective osteotomy may be best.
RECOMMENDED READINGS
6. [Abzug JM, Little K, Kozin SH. Physeal arrest of the distal radius. J Am Acad Orthop Surg. 2014 Jun;22(6):381-9. doi: 10.5435/JAAOS-22-06-381. Review. PubMed PMID: 24860134. ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860134)
7. [Craig JG, Cramer KE, Cody DD, Hearshen DO, Ceulemans RY, van Holsbeeck MT, Eyler WR. Premature partial closure and other deformities of the growth plate: MR imaging and three-dimensional modeling. Radiology. 1999 Mar;210(3):835-43. PubMed PMID: 10207489. ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10207489)
8. [Ecklund K, Jaramillo D. Patterns of premature physeal arrest: MR imaging of 111 children. AJR Am J Roentgenol. 2002 Apr;178(4):967-72. PubMed PMID: 11906884. ](http://www.ncbi.nlm.nih.gov/pubmed/11906884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11906884)
Question 3High Yield
Which of the following are characteristic signs of PIN palsy:
Explanation
Painless finger drop is characteristic of posterior interosseous nerve palsy. This syndrome may also involve elbow tenderness in the absence of other clinical findings. Pain in the dorsum of the hand is not associated with this condition because the posterior interosseous nerve contains no sensory component.
Question 4High Yield
In injured tissues, ischemia begins when the tissue pressure within the compartment comes within mm Hg of the diastolic pressure.
Explanation
Normal tissues have adequate tissue perfusion with increases in compartment pressure to within 10 mm Hg of the diastolic pressure. In damaged tissue (eg, tibia fracture), perfusion can be impaired when the diastolic pressure reaches within 20 mm Hg of the diastolic pressure.
One should remember that hypotensive patients with extremity injuries are prone to compartment syndromes. Correct Answer: 20
One should remember that hypotensive patients with extremity injuries are prone to compartment syndromes. Correct Answer: 20
Question 5High Yield
Indicates the lateral center edge angle
Explanation
- Figure 51a_
Question 6High Yield
A 73-year-old man goes to the emergency department after tripping and falling down roughly thirteen steps at home. Prior to the injury, the patient had well-controlled medical comorbidities and was independent with all activities of daily living. Figures 1 through 3 show the injury sustained by the patient. What is the most appropriate definitive treatment for this patient?

Explanation
■
The patient has a C1 burst fracture, as well as a grossly displaced C2 fracture. Surgical treatment should be considered for this patient who has good baseline function and wellcontrolled medical comorbidities. A cervical collar would not offer adequate stabilization for this fracture. Anterior reduction of this C2 fracture would be difficult, and screw fixation of C2 would not address the C1-C2 instability. A halo vest is considered a relative contraindication in the older patient population. Therefore, posterior C1-C2 fixation is the most appropriate choice.
The patient has a C1 burst fracture, as well as a grossly displaced C2 fracture. Surgical treatment should be considered for this patient who has good baseline function and wellcontrolled medical comorbidities. A cervical collar would not offer adequate stabilization for this fracture. Anterior reduction of this C2 fracture would be difficult, and screw fixation of C2 would not address the C1-C2 instability. A halo vest is considered a relative contraindication in the older patient population. Therefore, posterior C1-C2 fixation is the most appropriate choice.
Question 7High Yield
A 57-year-old woman who is undergoing right total hip arthroplasty is found to have a femoral neck shaft angle of 110° for both hips. She has no measurable leg length discrepancy preoperatively. The femoral component that is selected for the reconstruction has a neck angle of 130°. During surgery, if baseline neck length is maintained, the right hip is prone to
Explanation
There is coxa vara of the hips and, by reconstructing the hip with a more valgus neck angle and maintaining the neck length, the reconstruction would reduce offset and increase leg length relative to the opposite hip.
90
90
Question 8High Yield
The asterisks on Figures 98a through 98c represent which anatomic structure?
A
B
C
A
B
C



Explanation
The popliteus muscle arises from the posteromedial part of the tibia, and the tendon continues to attach to the lateral femoral condyle. The tendon is an intra-articular, extra synovial structure coursing through the popliteus hiatus, then deep to the fibular collateral ligament before inserting in the anterior portion of the popliteal sulcus.
RECOMMENDED READINGS
1. Clarke HD, Scott WN, Insall JN, et al. Anatomy. In: Insall JN, Scott WN, eds. Surgery of the Knee. Vol 1. 4th ed. Philadelphia, PA: Churchill Livingstone; 2006:3-66.
2. Miller TT: Magnetic resonance imaging of the knee. In: Insall JN, Scott WN, eds. Surgery of the Knee. Vol 1. 4th ed. Philadelphia, PA: Churchill Livingstone; 2006:201-224.
RECOMMENDED READINGS
1. Clarke HD, Scott WN, Insall JN, et al. Anatomy. In: Insall JN, Scott WN, eds. Surgery of the Knee. Vol 1. 4th ed. Philadelphia, PA: Churchill Livingstone; 2006:3-66.
2. Miller TT: Magnetic resonance imaging of the knee. In: Insall JN, Scott WN, eds. Surgery of the Knee. Vol 1. 4th ed. Philadelphia, PA: Churchill Livingstone; 2006:201-224.
Question 9High Yield
A 10-year-old boy has had a prominent scapula for the past year. He reports crepitus and aching over the area, but only when he is active. A radiograph and CT scans are shown in Figures 37a through 37c. What is the most likely diagnosis?
Explanation
The findings are typical for an osteochondroma. It is found as an outgrowth of bone and cartilage from those bones that arise from enchondral ossification. It may be flat, verrucous, or with a long stalk and cauliflower-like cap. Osteochondromas can become symptomatic secondary to irritation of the adjacent musculature. They cease to proliferate when epiphyseal growth ceases.
REFERENCE: Schmade GA, Conrad EV III, Raskind WH: The natural history of hereditary multiple exostoses. J Bone Joint Surg Am 1994;76:986-992.
REFERENCE: Schmade GA, Conrad EV III, Raskind WH: The natural history of hereditary multiple exostoses. J Bone Joint Surg Am 1994;76:986-992.
Question 10High Yield
Figure 14 is a sagittal-cut MR image from the hindfoot of a 54-year-old woman who has had plantar heel pain for 3 months. There is no history of trauma. Her pain is worse when she rises and at the end of the day. Upon examination she has localizable tenderness over the plantar medial tubercle of the calcaneus. The Achilles is intact and nontender, and subtalar joint motion is full and painless. A Tinel test result is negative. What is the most likely diagnosis?
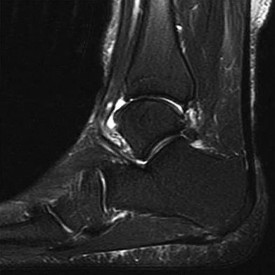



Explanation
Plantar fasciitis is inflammation of the plantar fascia at its insertion onto the medial calcaneus. The T2-weighted sagittal MR image reveals thickening of the plantar fascia with no evidence of a calcaneal stress fracture, coalition, or inflammation of the insertion of the Achilles tendon.
RECOMMENDED READINGS
Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW. Plantar and medial heel pain: diagnosis and management. J Am Acad Orthop Surg. 2014 Jun;22(6):372-80. doi: 10.5435/JAAOS-22-06-
[372/. PubMed PMID: 24860133. ](http://www.ncbi.nlm.nih.gov/pubmed/24860133)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860133)
Covey CJ, Mulder MD. Plantar fasciitis: How best to treat? J Fam Pract. 2013 Sep;62(9):466-
[71/. PubMed PMID: 24080555. ](http://www.ncbi.nlm.nih.gov/pubmed/%2024080555)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2024080555)
CLINICAL SITUATION FOR QUESTIONS 15 THROUGH 18
Figures 15a through 15c are the initial injury radiographs of a 32-year-old man who sustained a closed injury to his right lower extremity after a fall from a curb. Initial examination reveals a swollen painful ankle with pain both medially and laterally at the level of the malleoli.
15A
B
C
RECOMMENDED READINGS
Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW. Plantar and medial heel pain: diagnosis and management. J Am Acad Orthop Surg. 2014 Jun;22(6):372-80. doi: 10.5435/JAAOS-22-06-
[372/. PubMed PMID: 24860133. ](http://www.ncbi.nlm.nih.gov/pubmed/24860133)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860133)
Covey CJ, Mulder MD. Plantar fasciitis: How best to treat? J Fam Pract. 2013 Sep;62(9):466-
[71/. PubMed PMID: 24080555. ](http://www.ncbi.nlm.nih.gov/pubmed/%2024080555)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2024080555)
CLINICAL SITUATION FOR QUESTIONS 15 THROUGH 18
Figures 15a through 15c are the initial injury radiographs of a 32-year-old man who sustained a closed injury to his right lower extremity after a fall from a curb. Initial examination reveals a swollen painful ankle with pain both medially and laterally at the level of the malleoli.
15A
B
C
Question 11High Yield
The clinical photograph in Figure 27 shows a palsy of what nerve/associated muscle?
Explanation
DISCUSSION: The clinical picture reveals medial scapular winging, which involves the serratus anterior muscle, potentially due to an injury to the long thoracic nerve that innervates this muscle. Injury to the long thoracic nerve is usually due to closed trauma, direct compression, traction or stretching injury, a direct blow, or, very rarely, viral infection such as Parsonage-Tumer syndrome. The nerve is easily injured in surgical dissection of the axilla, and is predisposed to injury due to its relatively long course, it is small in diameter, and it has little surrounding connective tissue. If rehabilitation and time are unsuccessful, both nerve and muscle transfers have been described with mixed results.
REFERENCES: Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop Relat Res 1999;368:17 - 27.
Warner JJ, Navarro RA: Serratus anterior dysfunction: Recognition and treatment. Clin Orthop Relat Res 1998;349:139-148.
REFERENCES: Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop Relat Res 1999;368:17 - 27.
Warner JJ, Navarro RA: Serratus anterior dysfunction: Recognition and treatment. Clin Orthop Relat Res 1998;349:139-148.
Question 12High Yield
A 25-year-old man underwent a Putti-Platt repair for recurrent anterior dislocation of his right shoulder 9 months ago. He reports no further episodes of instability but continues to have severely restricted motion, with external rotation limited to less than 0 degrees with the arm at the side. He has pain at the ends of range of motion and restricted activities of daily living despite undergoing nearly 9 months of physical therapy. Radiographs of the shoulder show no arthritic changes. Management should now consist of
Explanation
Open release allows lengthening of the shortened subscapularis and is preferred when there are extra-articular contractures. Arthroscopic release, combined with the use of an interscalene catheter postoperatively, is an excellent treatment for capsular contractures but is contraindicated after procedures that result in extracapsular shortening (ie, Magnuson-Stack, Putti-Platt). Additional physical therapy or manipulation under anesthesia is not likely to be helpful. Shoulder hemiarthroplasty is contraindicated with normal articular surfaces, but prosthetic arthroplasty is sometimes necessary for arthritis associated with instability or overly tight instability repairs.
REFERENCES: Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147.
Warner JJ: Frozen shoulder: Diagnosis and management. J Am Acad Orthop Surg 1997;5:130-140.
Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
MacDonald PB, Hawkins RJ, Fowler PJ, Miniaci A: Release of the subscapularis for internal rotation contracture and pain after anterior repair for recurrent anterior dislocation of the shoulder. J Bone Joint Surg Am 1992;74:734-737.
REFERENCES: Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147.
Warner JJ: Frozen shoulder: Diagnosis and management. J Am Acad Orthop Surg 1997;5:130-140.
Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
MacDonald PB, Hawkins RJ, Fowler PJ, Miniaci A: Release of the subscapularis for internal rotation contracture and pain after anterior repair for recurrent anterior dislocation of the shoulder. J Bone Joint Surg Am 1992;74:734-737.
Question 13High Yield
This is the definition of translocation. Examples of translocation include Ewing's sarcoma, Rhabdomyosarcoma, and Synovial sarcoma
In the treatment of rheumatoid arthritis, which medication is an antagonist of tumor necrosis factor-alpha?
In the treatment of rheumatoid arthritis, which medication is an antagonist of tumor necrosis factor-alpha?











Explanation
Etanercept is a biochemically designed tumor necrosis factor receptor immunoglobulin G fusion protein, which binds to TNF-alpha and is thus a TNF- alpha antagonist.
TNF-alpha is considered to be one of the major cytokines involved in rheumatoid arthritis pathology. As a result, many biologic agents used to treat rheumatoid arthritis (RA) are manufactured to block TNF-alpha or its
receptors. This has been shown to reduce inflammation and stop disease progression. In the USA, Etanercept is approved to treat rheumatoid arthritis, juvenile rheumatoid arthritis and psoriatic arthritis, plaque psoriasis and ankylosing spondylitis. The route of administration is subcutaneous.
Bongartz et al. used a randomized control trial to asses the risk of infection and
malignancy rates in RA treated with TNF-alpha antagonist. Overall, patients with RA appear to have an approximately 2-fold increased risk of serious infection compared to the general population and non-RA controls, irrespective of TNF-alpha antagonist use. The pooled odds ratio for malignancy was 3.3 (95% confidence interval [CI], 1.2-9.1) and for serious infection was
2.0 (95% CI, 1.3-3.1) with use of TNF-alpha antagonist.
Howe et al. review the medical management of patients with RA who underwent orthopaedic procedures. They state that while there is conflicting information regarding TNF-alpha antagonists, they recommend holding them prior to major orthopaedic interventions.
Incorrect Answers:
: Rituximab is a monoclonal antibody to CD20 antigen (inhibits B cells). It is often used with good clinical outcomes as monotherapy in patients who are intolerant of methotrexate or have contraindications to methotrexate or other DMARDs.
Answer 3: Abatacept is a selective costimulation modulator that binds to CD80 and CD86 (inhibits T cells). It is often prescribed for treatment of moderate to severe rheumatoid arthritis, or after failure of a disease-modifying anti- rheumatic agent (DMARD), like methotrexate but it can be used as first-line therapy.
Answer 4: Methotrexate is a folic acid analogue. It binds dihydrofolate reductase and prevents synthesis of tetrahydrofolate. It is usually a first line treatment for moderate to severe rheumatoid arthritis.
Answer 5: Leflunomide is an inhibitor of pyrimidine synthesis. It is approved to treat adult moderate to severe rheumatoid arthritis, usually as a monotherapy or failure of other DMARDs.
Cortical bone demonstrates viscoelastic behavior as its mechanical properties are sensitive to strain rate and duration of applied load. Regarding longitudinal strain in cortical bone, which of the following statements regarding this characteristic is true?
1) As strain rate increases, both elastic modulus and ultimate strength increase
2) As strain rate increases, elastic modulus remains unchanged but ultimate strength increases
3) As strain rate increases, elastic modulus increases but ultimate strength decreases
4) As strain rate increases, both elastic modulus and ultimate strength decrease
5) As strain rate increases, elastic modulus increases but ultimate strength remains unchanged
As strain rate increases, both elastic modulus and ultimate strength increase. For LOW strain rates typical of normal activity (physiological strain rates of
0.1/s, high impact trauma), bone is VISCOELASTIC and BRITTLE (low ultimate strain with increasing strain rate). Bone also becomes stronger and stiffer (higher modulus, steeper slope of stress- strain plot) as strain rate increases. This viscoelastic property helps in damping muscle contracture.
Natali and Meroi reviewed studies examining mechanical properties of bone. Mechanical properties are correlated with moisture, deformation rate, density and region of bone.
Mechanical adaptation of bone is affected by strain rate (rate at which bone is deformed), strain mode (tension, compression, shear), strain direction (direction of strain relative to bone surface), strain frequency (cycles/second), stimulus duration (period over which deformation cycles are applied), strain distribution (pattern of strain magnitude across bone section) and strain energy (energy stored during deformation).
Illustration A shows the mechanical properties of bone with increasing strain rates. Illustration B shows that the ultimate strength and elastic modulus increase with rapid loading or deformation. The ultimate strength increases by roughly a factor of 3, while the elastic modulus increases by a factor of
approximately 2 over the strain rate range.
Incorrect Answers:
Answers 2, 3, 4, 5: As strain rate increases, elastic modulus and ultimate strength increase. During normal activity, as strain rate increases, bone is more ductile. With high impact trauma, bone is more brittle.
In regards to a genetic disorder, which of the following is an example of "anticipation?"
1) Gene characteristics more severe and earlier in onset in subsequent generations
2) A disorder inherited from a genetic mutation specific to maternal DNA
3) Gene characteristics expressed to varying degrees in different individuals
4) Variation in the relative frequency of a genotype due to chance
5) The presence of an extra copy of a chromosome
Genetic anticipation is a phenomenon in which a genetic disorder becomes progressively more severe and earlier in onset with each generation. Examples of disorders exhibiting anticipation include Huntington's disease and myotonic dystrophy.
Genetic anticipation is an important concept in understanding the development and genetic implications of many heritable disorders. It is a common phenomenon in trinucleotide repeat expansion disorders. These disorders are due to unstable microsatellite trinucleotide repeats that expand beyond the normal threshold. In subsequent generations these expansions become longer and thus express disease characteristics at a younger age of onset, and often with greater severity.
Martorell et al. investigated the development of CTG trinucleotide repeats in patients with myotonic dystrophy type 1 (DM1) and their relatives. They discovered unaffected individuals carry a pre-mutation sequence which can lead to trinucleotide repeat expansion in subsequent generations and thus produce offspring with the disorder.
Kamsteeg et al. compare the characteristics of DM1 and DM2. Both are due to trinucleotide repeat expansions. However, while DM1 can present with earlier onset and increasing severity in each generation, DM2 does not exhibit this genetic anticipation.
Incorrect Answers
Answer 2: "Genomic imprinting" is when a disorder is linked to a parent- specific origin. An example of maternal genomic imprinting is Angelman Syndrome. An example of paternal genomic imprinting is Prader Willi.
Answer 3: "Variable penetrance" is when gene characteristics are expressed in varying degrees.
Answer 4: "Genetic drift" is the chance variation in the relative frequency of a genotype within a population.
Answer 5: "Trisomy" is the presence of an extra copy of a chromosome. Down Syndrome is trisomy 21, which is due to an extra copy of chromosome 21.
A researcher is working on Medication A, a drug FDA-approved for the treatment of osteoporosis in men and women. It is an anti- resorptive agent that inhibits the formation, function and survival of osteoclasts. It does not bind to calcium hydroxyapatite. At 1-year after the initial dose, tissue levels are non- detectable. It can be used in the presence of cancer metastases to bone. What is Medication A?
1) Denosumab
2) Alendronate
3) Abaloparatide
4) Teriparatide
5) Strontium ranelate
Denosumab is FDA-approved for the treatment of osteoporosis in men and women. It inhibits the formation, function and survival of osteoclasts (OC). It does not bind to calcium hydroxyapatite. At 1-year after the initial dose, tissue levels are non-detectable.
Denosumab is a human monoclonal antibody against RANKL. By binding RANKL, it prevents interaction of RANKL with RANK (on OC and osteoclast precursors, OCP), and inhibits OC-mediated bone resorption, and the formation, function and survival of OC. In contrast, bisphosphonates bind to calcium hydroxyapatite in bone, and decrease resorption by decreasing function and survival (but not formation) of OC.
Vaananen et al. reviewed the cell biology of OC. During bone resorption, 3 membrane domains appear: ruffled border, sealing zone and functional secretory domain. The resorption cycle starts with migration, bone attachment, polarization (formation of membrane domains), dissolution of hydroxyapatite, degradation of organic matrix, removal of degradation
products from resorption lacuna, and apoptosis of the OC or return to the non- resorbing stage.
Boyce et al. reviewed the regulation of osteoclasts and their functions. OCPs are held in bone marrow by chemokines e.g. stroma-derived factor-1 (SDF1) and attracted to blood by sphingosine-1 phosphate (S1P) (increased in synovial fluid of patients with RA). All aspects of osteoclast formation and functions are regulated by M-CSF and RANKL. More recent studies indicate that osteoclasts and their precursors regulate immune
responses and
osteoblast formation and functions by means of direct cell-cell contact through ligands and receptors, such as ephrins and Ephs, and semaphorins and
plexins, and through expression of clastokines.
Warriner and Saag reviewed the diagnosis and treatment of osteoporosis. They defined osteoporosis as T-score of = -2.5 or a history of fragility fracture. Incident hip and vertebral fractures increase future risk of these fractures (hazard ratio 7.3 and 3.5, respectively).
Cummings et al. compared subcutaneous denosumab (60mg every 6mths) vs placebo in prevention of fractures in 7868 osteoporotic (T-score -2.5 to -4.0) postmenopausal women. They found that denosumab reduced risk of vertebral fracture by 68% (risk ratio, 0.32), hip fracture by 40% (hazard ratio 0.6), nonvertebral fracture by 20% (hazard ratio 0.8). There was no increased risk of cancer, infection, delayed fracture healing, cardiovascular disease, osteonecrosis of the jaw or adverse reactions. They concluded that it was useful for reduction of fractures in osteoporotic women.
The video shows the action of denosumab (prolia). Illustration A shows the different osteoclast zones.
Incorrect Answers:
Answers 2: Alendronate (and other bisphosphnates) inhibit resorption of bone, decrease function and survival of osteoclasts. Because of binding to calcium hydroxyapatite, they are detectable years after dosing. They reduce function and survival of OC, but do not affect the formation of osteoclasts.
Answer 3: Abaloparatide is a PTH analog that has completed phase III trials for osteoporosis. As of mid-2016, it is not yet approved for treatment of osteoporosis. Answer 4: Teriparatide (recombinant PTH 1-34) is the only anabolic (not antiresorptive) agent approved for osteoporosis treatment. It is administered by daily subcutaneous injection. Osteosarcoma, cancer metastases to bone and Paget's disease are contraindications.
Answer 5: Strontium ranelate (marketed as Protelos or Protos) both increases deposition of new bone by osteoblasts and reduces the resorption of bone by osteoclasts ("dual action bone agent", DABA). It is not FDA approved for use in the United States. Increased risk of myocardial infarction has been detected.
Which specific legislative Act in the United States was created to require reporting of annual monetary gifts or compensation of more than $10 by orthopaedic implant companies to physicians?
1) Patient Protection and Affordable Care Act
2) Medicare Payment Reform Act
3) Physician Financial Transparency Act
4) Physician Payments Sunshine Act
5) Health Insurance Portability and Accountability Act
The Physician Payments Sunshine Act requires all payments by corporations to physicians beyond $10 per year to be reported to the Centers for Medicare and Medicaid Services.
Under this Act, all manufacturers of drugs and devices covered under Medicare, Medicaid, and SCHIP are obliged to federally report payments beyond $10 annually to physicians and academic centers. The Act was first introduced in 2007, enacted in 2010, and in 2014 the first data (from 2012) was reported publicly online in the Open Payment Program of the Centers for Medicare and Medicaid Services website.
Samuel et al analyze orthopedic surgeons available data from the Sunshine Act regarding industry payments and find over 110 million USD paid to approximately 15,000 orthopedic surgeons over the 5-month study period. No long term data exists to determine if these payments have any affect in healthcare.
Incorrect Answers:
Answers 1: The Patient Protection and Affordable Care Act (PPACA), known also by its shorter name of the Affordable Care Act (ACA) or it's nickname
"Obamacare", was passed in March 2010. The Sunshine Act was one of many provisions passed within the PPACA (after the Sunshine Act failed to pass on its own in prior years), but the PPACA focused primarily on improving the quality and affordability of healthcare insurance and lowering the costs of healthcare.
Answer 2: The Medicare Payment Reform Act of 1983 was a quickly drafted revision to the way Medicare payments were made, changing from fee-for- service to prospective payments allowing Medicare to determine payment amount rather than providers/hospitals.
Answer 3: This is a fictitious act.
Answer 5: HIPPA is the 1996 legislation defining standards and protections for patient private health information and electronic exchange of records.
Which of the following materials best approximates the Young's modulus of elasticity of cortical bone?
1) Titanium
2) Cobalt-chrome alloy
3) Alumina
4) Zirconia
5) Stainless steel
Of the materials listed titanium (100GPa) has an elastic modulus closest to cortical bone (approximately 18GPa) as well as cancellous bone (approximately 2GPa).
Titanium is a material that is light, highly ductile, strong and corrosion resistant. However, titanium has poor wear resistance and is notch sensitive. It is commonly used as an orthopaedic implant materials because it has torsional and axial stiffness (moduli) that most closely mimics bone. Young’s modulus is constant and different for each material and represents the material's ability to maintain shape under external loading.
Rho et al found that the average Young's modulus for trabecular bone measured ultrasonically and mechanically was 14.8 GPa (S.D. 1.4) and 10.4 (S.D. 3.5), respectively. The average Young's modulus of microspecimens of cortical bone measured ultrasonically and mechanically was 20.7 GPa (S.D.
1.9) and 18.6 GPa (S.D. 3.5), respectively.
Illustration A depicts a stress vs. strain curve. The slope of the line in the elastic zone represents the Young Modulus of Elasticity.
Incorrect Answers:
Answer 2: Cobalt-chrome alloy is approximately 240 GPa Answer 3: Alumina is approximately 340 GPa
Answer 4: Zirconia (Ceramic) = 248 GPa
Answer 5: Stainless steel is approximately 240 GPa
The difference between vitamin D-dependent rickets type I (VDDR I) and vitamin D-dependent rickets type II (VDDR II) is
1) VDDR I is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3. VDDR II is a deficiency of an enzyme predominantly found in the kidney.
2) VDDR I is caused by an activating mutation of the receptor for 1,25 (OH)2 vitamin D3. VDDR II is a deficiency of an enzyme predominantly found in the kidney.
3) VDDR I is a deficiency of an enzyme predominantly found in the kidney. VDDR II is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3.
4) VDDR I is a deficiency of an enzyme predominantly found in the kidney. VDDR II is caused by an activating mutation of the receptor for 1,25 (OH)2 vitamin D3.
5) VDDR I is a deficiency of an enzyme predominantly found in the liver. VDDR II is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3.
VDDR I is a deficiency of an enzyme predominantly found in the kidney. VDDR II is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3.
VDDR I is a deficiency of 1a-hydroxylase [converts 25(OH)D to
1a,25(OH)2D3]. Lab tests show hypocalcemia, secondary hyperparathyroidism, elevated alkaline phosphatase (ALP) and low or undetectable calcitriol in the presence of adequate 25(OH)D levels. VDDR II or hereditary vitamin D resistant rickets (HVDRR) (autosomal recessive) is an inactivating mutation in the vitamin D receptor (VDR). Lab tests show low serum calcium and phosphate, elevated ALP and secondary hyperparathyroidism. Serum 25(OH)D values are normal and the 1,25(OH)2D levels are elevated (key difference from VDDR I).
Malloy et al. reviewed genetic disorders in vitamin D action. They state that VDDR I is an inborn error of vitamin D metabolism coded by the gene CYP27B1. Children with VDDR I present with joint pain/deformity, hypotonia, muscle weakness, growth failure, and hypocalcemic seizures or fractures in early infancy. Treatment is with calcitriol or 1a-hydroxyvitamin D (NOT cholecalciferol). Children with VDDR II present with bone pain, muscle weakness, hypotonia, hypocalcemic convulsions, growth retardation, severe dental caries or teeth hypoplasia. Affected children are resistant to therapy and supra-physiologic doses of all forms of vitamin D.
Illustration A shows the differences between VDDR I and VDDR II. Incorrect Answers
Answers 1, 2, 4, 5: VDDR I is a deficiency of 1a-hydroxylase (predominantly
found in the kidney). The liver enzyme vitamin D 25-hydroxylase (found in hepatocytes) is not responsible for VDDR. VDDR II is caused by an inactivating mutation (rather than an activating mutation).
A 73-year-old female sustains a left hip fracture that is treated with hemiarthroplasty. She has continued pain two months after surgery, and comes to you for a second opinion. Her radiograph is shown in Figure A. Which of the following best describes your responsibility in disclosing to the patient that the pain may be from a medical error?
1) You do not need to disclose this information
2) You legally must disclose this information to the patient
3) You legally must disclose this information to the original hospital's peer review panel
4) You ethically must disclose this information to the patient
5) You ethically must disclose this information to the original surgeon
As a practicing orthopaedic surgeon, you ethically are required to disclose the potential impact of medical errors on patient outcome.
The orthopaedic surgeon is bound ethically but not legally to give his or her best medical opinion, regardless of whether the orthopaedist is the treating physician or the physician who is asked to render a second or additional medical opinion. The best interest of the patient should clearly remain the guiding principal. It is illegal to slander the original physician if the slanderous
information is known or can be proven to be false.
Bhattacharyya et al. review the importance of documentation and ethical treatment of patients when providing second opinions. They note that it is unethical for the consulting orthopaedic surgeon to solicit care of the patient. However, at the sole discretion of the patient, the patient ethically may choose to terminate his or her relationship with his or her treating physician and then enter into another treatment relationship with the consulting
orthopaedic surgeon.
Figure A shows a left hip hemiarthroplasty with the distal component perforated through the medial proximal femur.
Incorrect Answers:
1) This information must be disclosed per ethical recommendations. 2 and 3) There is no legal requirement to disclose this information.
5) There is no documented ethical requirement to disclose this to the original surgeon.
A patient is consented for a right wrist open reduction and internal fixation. After the patient is prepped and draped, a skin incision is made. It is recognized intra-operatively, however, that a skin incision was made on the incorrect side (left). Subsequent right wrist open reduction and internal fixation goes uneventfully. What is the next best course of action?
1) do not tell the patient or family
2) contact the Risk Management department
3) immediately discuss the situation with the patient and family
4) alter the medical record
5) only discuss the situation with the patient if he or she brings it up.
Patients should be approached after a medical error and all errors must be promptly and completely disclosed. The physician should take the lead in the disclosure and not wait for the patient to ask. Risk management should be called as well, but the patient and family should be informed first. It is never appropriate to alter the medical record.
A 14-year-old female has anal hemorrhoids. The General Surgical team has asked for a consultation in regards to her history of hand, wrist, and ankle joint pain and swelling over the past 3 years. Her physical examination reveals a swollen left wrist, right knee and left ankle. Lab work shows low hemoglobin, low albumin, elevated erythrocyte sedimentation rate (ESR), elevated antinuclear antibody (ANA) count, and a negative rheumatoid factor. Radiography of the affected joints are normal. What additional work up is required prior
**to her rectal surgery?**
1) C-reactive protein (CRP)
2) Synovial fluid analysis of affected joints
3) Blood cultures
4) Cervical radiographs
5) Bethesda assay
This patient has a diagnosis of Juvenile Idiopathic Arthritis (JIA). Flexion- extension c-spine radiographs should be ordered to rule out atlantoaxial instability prior to surgery.
JIA is a persistent autoimmune inflammatory arthritis lasting more than 6 weeks in a patient younger than 16 years of age. Serologic testing for this condition will usually show elevated ESR/CRP, low hemoglobin, low albumin and an elevated anti-nuclear antibody (ANA) count, as well as negative rheumatoid factor and positive HLA-B27. Radiographs of the c-spine should be considered in patients undergoing intubation as cervical kyphosis, facet ankylosis, and atlantoaxial subluxation is associated with this condition.
Punaro et al. reviewed rheumatologic conditions in children. The typical patient with oligoarticular JIA is a white female (5:1, F:M), with a peak onset between ages 1 and 3 years. Nearly half of patients have monoarticular involvement, with the knee and ankle being most commonly involved. Uveitis is typically chronic, bilateral, and asymptomatic.
Borchers et al. reviewed juvenile idiopathic arthritis (JIA). They state that no laboratory test can conclusively establish a rheumatic diagnosis. They state that laboratory tests will be negative for systemic inflammation and antinuclear antibody (ANA) test has no use in screening for JIA, as it has a high false positive rate.
Incorrect Answers:
Answer 1: Both ESR and CRP are usually elevated in this condition and provide no further benefit for the operative management of this patient.
Answer 2: This patient has chronic joint swelling and pain. Joint aspirates and synovial fluid analysis would not be required.
Answer 3: There is no suspicion for an acute infection. Therefore, blood cultures are not required.
Answer 5: A Bethesda assay is used to measure the amount of factor VIII or IX antibody in the blood, for patients with hemophilia.
Induction coupling stimulates bone growth through all of the following direct effects EXCEPT:
1) Increased proliferation of osteoblasts
2) Decreased osteoclast differentiation
3) Increase release of TGF-beta1
4) Increased expression of BMP2
5) Increased expression of BMP7
Induction coupling stimulates bone growth by increasing expression of BMP7, BMP2, TGF-beta1, and by increasing osteoblasts proliferation. Induction coupling has not been shown to have the effect of decreasing osteoclast differentiation.
In basic science studies, electrical stimulation (i.e. induction coupling), has been shown to promote bone healing via release of growth factors that induce osteoblast differentiation/proliferation. Electrical current can be placed around bone in various ways, creating a current to stimulate growth factor release and subsequent osteoblast proliferation.
Aaron et al. summarized, in a systematic review, the effects of various types of electrical stimulation on bone and bone healing. Regardless of type (i.e. inductive coupling, capacitive coupling, direct current), they report electricity and/or electromagnetic fields promote gene expression of growth factors that promote an osteogenic environment.
Illustration A depicts a cathode placed directly to allograft with a subcutaneously placed electrical stimulator. Illustration B depicts cathodes placed anteriorly and posteriorly around the hip, connected to an outside power source to create the necessary current. Illustration C depicts an inductive coil placed laterally on the skin in order to create an electrical current.
Incorrect answers:
Answers 1,3-5: All are true effects of electrical stimulation on bone.
Two patients are discharged from a surgicenter after upper extremity procedures. The surgeon gives them prescriptions for oral opioid analgesics. Patient A had open reduction and internal fixation of a distal radius fracture. Patient B had cubital tunnel release without transposition. Which of the following is most likely true regarding analgesic use?
1) Patient A will use more medication than Patient B
2) Patient A will use less medication than Patient B
3) Analgesic use will be similar between Patients A and B
4) Both patients will consume more than 30 pills
5) A reasonable prescription is 40 pills with 1 refill for Patient A, and 40 pills with no refills for Patient B
A patient that has had ORIF will require MORE oral analgesia than a patient who has had a cubital tunnel release.
Patients undergoing bony procedures (e.g. ORIF and arthroplasty) require more analgesia than patients undergoing soft tissue procedures (e.g. carpal/cubital tunnel release, trigger finger release, elbow or shoulder arthroscopy). Overprescribing of opioid analgesia is a common problem. Many opioids are unused in the postoperative period by the patients for whom they were prescribed.
Rodgers et al. reviewed opioid use (oxycodone, hydrocodone, propoxyphene) after outpatient upper extremity surgery. Patients undergoing bony procedures used the most analgesia (14 pills) while those undergoing soft tissue
procedures used the least (9 pills). Half took medication for =
What property of titanium alloys accounts for their high corrosion resistance in vivo?
1) Self-passivation
2) Ductility
3) Hardness
4) Modulus of elasticity
5) Conductivity
In both room temperature air and physiologic fluids, titanium alloys self- passivate or spontaneously form a layer of titanium oxide very rapidly. This layer makes titanium alloys resistant to surface breakdown.
Embolic material generated during total knee arthroplasty (TKA) shown in Figure 29 is composed of which of the following substances?
1) Fat only
2) Fat and air
3) Fat and marrow
4) Fat and cement
5) Fat and bone
Emboli are created during TKA. Usually there is an increased incidence with
the use of intramedullary rods that disrupt the marrow contents. These are not fat emboli per se. They are material composed of fat cells and marrow that act like pulmonary emboli
to obstruct small arterioles in the lung. They are different from free fat emboli that are seen in fractures and that lead to chemical injury to the lung rather than obstructive injury.
There is increasing concern about the ethical relationship of orthopaedists to the orthopaedic equipment industry. Which of the following describes the most appropriate relationship?
1) Industry-paid travel, hotel (for the surgeon and spouse), and registration at a university- sponsored CME course
2) Industry-paid travel and hotel for a faculty member at an industry- sponsored meeting that is not CME approved
3) Consultation agreement ($50,000/annum) between the surgeon and the company for evaluation of the implant system with required oral reporting of impressions
4) A restricted grant from a company to an orthopaedic residency program with the stipulation that the third year residents be sent to an industry- sponsored course
5) Industry-paid dinner at a premium restaurant ($200/person) for surgeon and office staff at which a new set of surgical instrumentation is presented
It is appropriate for orthopaedic surgeons to have relationships with industry as long as the relationship is for the good of the patient and no “quid pro quo” intent exists. A grant to cover registration at a CME event is appropriate but travel and hotel for a spouse is not.
For orthopaedists who are faculty at a meeting sponsored by industry, it is appropriate for travel and expenses to be covered for that faculty member. Care must be exercised that the faculty member contributes in an amount appropriate for the expenses paid. The faculty member must ensure that information presented is unbiased and based on reasonable data and opinion. Consulting agreements should spell out specifically the duties of the agreement and payment should be appropriate for the time spent. There should be a defined work product for the consulting. Agreements that are thinly veiled payments for use of a company’s products must be avoided. In all cases, the agreements must stand up to public
scrutiny. Restricted grants for specific industry-sponsored programs aimed at residents are not appropriate. Unrestricted grants intended for attendance at approved CME courses are appropriate. Dinners at which information is presented about topics that can aid in patient care are appropriate as long as the expense is reasonable ($100 or less/person) and the guest list includes individuals who can use the information in a patient case. Clearly a “premium” dinner for office staff to review new surgical instrumentation would not pass this test.
Figure 33 shows the venogram of a patient who has a long history of alcohol abuse. Warfarin should be used cautiously because of the interaction with which of the following factors?
1) IV
2) V
3) VI
4) VII
5) VIII
Warfarin acts by inhibiting clotting factors II, VII, IX, X. The actual mechanism of action is by inhibition of hepatic enzymes, vitamin K epoxide, and perhaps vitamin K reductase.
This inhibition results in lack of carboxylation of vitamin
K-dependent proteins (II, VII, IX, X). The anticoagulant effect of warfarin can be reversed with vitamin K or fresh-frozen plasma. The use of alcohol may lead to liver dysfunction and an even more limited margin of available factors.
Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
1) It is a disease caused by an abnormality of platelets that leads to increased blood clotting.
2) It is a disease caused by an abnormality of vascular endothelium that leads to increased blood clotting.
3) It is a disease caused by an abnormality of hepatic metabolism that leads to decreased production of factor V and decreased blood clotting.
4) It is a disease caused by an abnormality of factor V that leads to decreased inactivation of factor Va by activated protein C (aPC) and increased blood clotting.
5) It is a familial, genetic disease that requires placement of a Greenfield filter in all
individuals who have the abnormality, prior to surgery.
Factor V Leiden is a disease caused by an abnormality of factor V in which a single amino acid substitution of glutamine for arginine in the protein C cleavage region leads to decreased inactivation of factor V and thus a greater tendency to form clots. More than half of all individuals with Factor V Leiden will develop deep venous thrombosis in the presence of a single additional risk factor such as long bone fracture or total joint arthroplasty.
Which of the following terms best describes the probability of finding a significant association in a research study when one truly exists?
1) Type-1 (alpha) error
2) Type-2 (beta) error
3) Power
4) Alpha level
5) Relative Risk
**
The power of a study is an estimate of the probability of finding a significant association in a research study when one truly exists.
The
Etanercept is a biochemically designed tumor necrosis factor receptor immunoglobulin G fusion protein, which binds to TNF-alpha and is thus a TNF- alpha antagonist.
TNF-alpha is considered to be one of the major cytokines involved in rheumatoid arthritis pathology. As a result, many biologic agents used to treat rheumatoid arthritis (RA) are manufactured to block TNF-alpha or its
receptors. This has been shown to reduce inflammation and stop disease progression. In the USA, Etanercept is approved to treat rheumatoid arthritis, juvenile rheumatoid arthritis and psoriatic arthritis, plaque psoriasis and ankylosing spondylitis. The route of administration is subcutaneous.
Bongartz et al. used a randomized control trial to asses the risk of infection and
malignancy rates in RA treated with TNF-alpha antagonist. Overall, patients with RA appear to have an approximately 2-fold increased risk of serious infection compared to the general population and non-RA controls, irrespective of TNF-alpha antagonist use. The pooled odds ratio for malignancy was 3.3 (95% confidence interval [CI], 1.2-9.1) and for serious infection was
2.0 (95% CI, 1.3-3.1) with use of TNF-alpha antagonist.
Howe et al. review the medical management of patients with RA who underwent orthopaedic procedures. They state that while there is conflicting information regarding TNF-alpha antagonists, they recommend holding them prior to major orthopaedic interventions.
Incorrect Answers:
: Rituximab is a monoclonal antibody to CD20 antigen (inhibits B cells). It is often used with good clinical outcomes as monotherapy in patients who are intolerant of methotrexate or have contraindications to methotrexate or other DMARDs.
Answer 3: Abatacept is a selective costimulation modulator that binds to CD80 and CD86 (inhibits T cells). It is often prescribed for treatment of moderate to severe rheumatoid arthritis, or after failure of a disease-modifying anti- rheumatic agent (DMARD), like methotrexate but it can be used as first-line therapy.
Answer 4: Methotrexate is a folic acid analogue. It binds dihydrofolate reductase and prevents synthesis of tetrahydrofolate. It is usually a first line treatment for moderate to severe rheumatoid arthritis.
Answer 5: Leflunomide is an inhibitor of pyrimidine synthesis. It is approved to treat adult moderate to severe rheumatoid arthritis, usually as a monotherapy or failure of other DMARDs.
Cortical bone demonstrates viscoelastic behavior as its mechanical properties are sensitive to strain rate and duration of applied load. Regarding longitudinal strain in cortical bone, which of the following statements regarding this characteristic is true?
1) As strain rate increases, both elastic modulus and ultimate strength increase
2) As strain rate increases, elastic modulus remains unchanged but ultimate strength increases
3) As strain rate increases, elastic modulus increases but ultimate strength decreases
4) As strain rate increases, both elastic modulus and ultimate strength decrease
5) As strain rate increases, elastic modulus increases but ultimate strength remains unchanged
As strain rate increases, both elastic modulus and ultimate strength increase. For LOW strain rates typical of normal activity (physiological strain rates of
0.1/s, high impact trauma), bone is VISCOELASTIC and BRITTLE (low ultimate strain with increasing strain rate). Bone also becomes stronger and stiffer (higher modulus, steeper slope of stress- strain plot) as strain rate increases. This viscoelastic property helps in damping muscle contracture.
Natali and Meroi reviewed studies examining mechanical properties of bone. Mechanical properties are correlated with moisture, deformation rate, density and region of bone.
Mechanical adaptation of bone is affected by strain rate (rate at which bone is deformed), strain mode (tension, compression, shear), strain direction (direction of strain relative to bone surface), strain frequency (cycles/second), stimulus duration (period over which deformation cycles are applied), strain distribution (pattern of strain magnitude across bone section) and strain energy (energy stored during deformation).
Illustration A shows the mechanical properties of bone with increasing strain rates. Illustration B shows that the ultimate strength and elastic modulus increase with rapid loading or deformation. The ultimate strength increases by roughly a factor of 3, while the elastic modulus increases by a factor of
approximately 2 over the strain rate range.
Incorrect Answers:
Answers 2, 3, 4, 5: As strain rate increases, elastic modulus and ultimate strength increase. During normal activity, as strain rate increases, bone is more ductile. With high impact trauma, bone is more brittle.
In regards to a genetic disorder, which of the following is an example of "anticipation?"
1) Gene characteristics more severe and earlier in onset in subsequent generations
2) A disorder inherited from a genetic mutation specific to maternal DNA
3) Gene characteristics expressed to varying degrees in different individuals
4) Variation in the relative frequency of a genotype due to chance
5) The presence of an extra copy of a chromosome
Genetic anticipation is a phenomenon in which a genetic disorder becomes progressively more severe and earlier in onset with each generation. Examples of disorders exhibiting anticipation include Huntington's disease and myotonic dystrophy.
Genetic anticipation is an important concept in understanding the development and genetic implications of many heritable disorders. It is a common phenomenon in trinucleotide repeat expansion disorders. These disorders are due to unstable microsatellite trinucleotide repeats that expand beyond the normal threshold. In subsequent generations these expansions become longer and thus express disease characteristics at a younger age of onset, and often with greater severity.
Martorell et al. investigated the development of CTG trinucleotide repeats in patients with myotonic dystrophy type 1 (DM1) and their relatives. They discovered unaffected individuals carry a pre-mutation sequence which can lead to trinucleotide repeat expansion in subsequent generations and thus produce offspring with the disorder.
Kamsteeg et al. compare the characteristics of DM1 and DM2. Both are due to trinucleotide repeat expansions. However, while DM1 can present with earlier onset and increasing severity in each generation, DM2 does not exhibit this genetic anticipation.
Incorrect Answers
Answer 2: "Genomic imprinting" is when a disorder is linked to a parent- specific origin. An example of maternal genomic imprinting is Angelman Syndrome. An example of paternal genomic imprinting is Prader Willi.
Answer 3: "Variable penetrance" is when gene characteristics are expressed in varying degrees.
Answer 4: "Genetic drift" is the chance variation in the relative frequency of a genotype within a population.
Answer 5: "Trisomy" is the presence of an extra copy of a chromosome. Down Syndrome is trisomy 21, which is due to an extra copy of chromosome 21.
A researcher is working on Medication A, a drug FDA-approved for the treatment of osteoporosis in men and women. It is an anti- resorptive agent that inhibits the formation, function and survival of osteoclasts. It does not bind to calcium hydroxyapatite. At 1-year after the initial dose, tissue levels are non- detectable. It can be used in the presence of cancer metastases to bone. What is Medication A?
1) Denosumab
2) Alendronate
3) Abaloparatide
4) Teriparatide
5) Strontium ranelate
Denosumab is FDA-approved for the treatment of osteoporosis in men and women. It inhibits the formation, function and survival of osteoclasts (OC). It does not bind to calcium hydroxyapatite. At 1-year after the initial dose, tissue levels are non-detectable.
Denosumab is a human monoclonal antibody against RANKL. By binding RANKL, it prevents interaction of RANKL with RANK (on OC and osteoclast precursors, OCP), and inhibits OC-mediated bone resorption, and the formation, function and survival of OC. In contrast, bisphosphonates bind to calcium hydroxyapatite in bone, and decrease resorption by decreasing function and survival (but not formation) of OC.
Vaananen et al. reviewed the cell biology of OC. During bone resorption, 3 membrane domains appear: ruffled border, sealing zone and functional secretory domain. The resorption cycle starts with migration, bone attachment, polarization (formation of membrane domains), dissolution of hydroxyapatite, degradation of organic matrix, removal of degradation
products from resorption lacuna, and apoptosis of the OC or return to the non- resorbing stage.
Boyce et al. reviewed the regulation of osteoclasts and their functions. OCPs are held in bone marrow by chemokines e.g. stroma-derived factor-1 (SDF1) and attracted to blood by sphingosine-1 phosphate (S1P) (increased in synovial fluid of patients with RA). All aspects of osteoclast formation and functions are regulated by M-CSF and RANKL. More recent studies indicate that osteoclasts and their precursors regulate immune
responses and
osteoblast formation and functions by means of direct cell-cell contact through ligands and receptors, such as ephrins and Ephs, and semaphorins and
plexins, and through expression of clastokines.
Warriner and Saag reviewed the diagnosis and treatment of osteoporosis. They defined osteoporosis as T-score of = -2.5 or a history of fragility fracture. Incident hip and vertebral fractures increase future risk of these fractures (hazard ratio 7.3 and 3.5, respectively).
Cummings et al. compared subcutaneous denosumab (60mg every 6mths) vs placebo in prevention of fractures in 7868 osteoporotic (T-score -2.5 to -4.0) postmenopausal women. They found that denosumab reduced risk of vertebral fracture by 68% (risk ratio, 0.32), hip fracture by 40% (hazard ratio 0.6), nonvertebral fracture by 20% (hazard ratio 0.8). There was no increased risk of cancer, infection, delayed fracture healing, cardiovascular disease, osteonecrosis of the jaw or adverse reactions. They concluded that it was useful for reduction of fractures in osteoporotic women.
The video shows the action of denosumab (prolia). Illustration A shows the different osteoclast zones.
Incorrect Answers:
Answers 2: Alendronate (and other bisphosphnates) inhibit resorption of bone, decrease function and survival of osteoclasts. Because of binding to calcium hydroxyapatite, they are detectable years after dosing. They reduce function and survival of OC, but do not affect the formation of osteoclasts.
Answer 3: Abaloparatide is a PTH analog that has completed phase III trials for osteoporosis. As of mid-2016, it is not yet approved for treatment of osteoporosis. Answer 4: Teriparatide (recombinant PTH 1-34) is the only anabolic (not antiresorptive) agent approved for osteoporosis treatment. It is administered by daily subcutaneous injection. Osteosarcoma, cancer metastases to bone and Paget's disease are contraindications.
Answer 5: Strontium ranelate (marketed as Protelos or Protos) both increases deposition of new bone by osteoblasts and reduces the resorption of bone by osteoclasts ("dual action bone agent", DABA). It is not FDA approved for use in the United States. Increased risk of myocardial infarction has been detected.
Which specific legislative Act in the United States was created to require reporting of annual monetary gifts or compensation of more than $10 by orthopaedic implant companies to physicians?
1) Patient Protection and Affordable Care Act
2) Medicare Payment Reform Act
3) Physician Financial Transparency Act
4) Physician Payments Sunshine Act
5) Health Insurance Portability and Accountability Act
The Physician Payments Sunshine Act requires all payments by corporations to physicians beyond $10 per year to be reported to the Centers for Medicare and Medicaid Services.
Under this Act, all manufacturers of drugs and devices covered under Medicare, Medicaid, and SCHIP are obliged to federally report payments beyond $10 annually to physicians and academic centers. The Act was first introduced in 2007, enacted in 2010, and in 2014 the first data (from 2012) was reported publicly online in the Open Payment Program of the Centers for Medicare and Medicaid Services website.
Samuel et al analyze orthopedic surgeons available data from the Sunshine Act regarding industry payments and find over 110 million USD paid to approximately 15,000 orthopedic surgeons over the 5-month study period. No long term data exists to determine if these payments have any affect in healthcare.
Incorrect Answers:
Answers 1: The Patient Protection and Affordable Care Act (PPACA), known also by its shorter name of the Affordable Care Act (ACA) or it's nickname
"Obamacare", was passed in March 2010. The Sunshine Act was one of many provisions passed within the PPACA (after the Sunshine Act failed to pass on its own in prior years), but the PPACA focused primarily on improving the quality and affordability of healthcare insurance and lowering the costs of healthcare.
Answer 2: The Medicare Payment Reform Act of 1983 was a quickly drafted revision to the way Medicare payments were made, changing from fee-for- service to prospective payments allowing Medicare to determine payment amount rather than providers/hospitals.
Answer 3: This is a fictitious act.
Answer 5: HIPPA is the 1996 legislation defining standards and protections for patient private health information and electronic exchange of records.
Which of the following materials best approximates the Young's modulus of elasticity of cortical bone?
1) Titanium
2) Cobalt-chrome alloy
3) Alumina
4) Zirconia
5) Stainless steel
Of the materials listed titanium (100GPa) has an elastic modulus closest to cortical bone (approximately 18GPa) as well as cancellous bone (approximately 2GPa).
Titanium is a material that is light, highly ductile, strong and corrosion resistant. However, titanium has poor wear resistance and is notch sensitive. It is commonly used as an orthopaedic implant materials because it has torsional and axial stiffness (moduli) that most closely mimics bone. Young’s modulus is constant and different for each material and represents the material's ability to maintain shape under external loading.
Rho et al found that the average Young's modulus for trabecular bone measured ultrasonically and mechanically was 14.8 GPa (S.D. 1.4) and 10.4 (S.D. 3.5), respectively. The average Young's modulus of microspecimens of cortical bone measured ultrasonically and mechanically was 20.7 GPa (S.D.
1.9) and 18.6 GPa (S.D. 3.5), respectively.
Illustration A depicts a stress vs. strain curve. The slope of the line in the elastic zone represents the Young Modulus of Elasticity.
Incorrect Answers:
Answer 2: Cobalt-chrome alloy is approximately 240 GPa Answer 3: Alumina is approximately 340 GPa
Answer 4: Zirconia (Ceramic) = 248 GPa
Answer 5: Stainless steel is approximately 240 GPa
The difference between vitamin D-dependent rickets type I (VDDR I) and vitamin D-dependent rickets type II (VDDR II) is
1) VDDR I is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3. VDDR II is a deficiency of an enzyme predominantly found in the kidney.
2) VDDR I is caused by an activating mutation of the receptor for 1,25 (OH)2 vitamin D3. VDDR II is a deficiency of an enzyme predominantly found in the kidney.
3) VDDR I is a deficiency of an enzyme predominantly found in the kidney. VDDR II is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3.
4) VDDR I is a deficiency of an enzyme predominantly found in the kidney. VDDR II is caused by an activating mutation of the receptor for 1,25 (OH)2 vitamin D3.
5) VDDR I is a deficiency of an enzyme predominantly found in the liver. VDDR II is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3.
VDDR I is a deficiency of an enzyme predominantly found in the kidney. VDDR II is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3.
VDDR I is a deficiency of 1a-hydroxylase [converts 25(OH)D to
1a,25(OH)2D3]. Lab tests show hypocalcemia, secondary hyperparathyroidism, elevated alkaline phosphatase (ALP) and low or undetectable calcitriol in the presence of adequate 25(OH)D levels. VDDR II or hereditary vitamin D resistant rickets (HVDRR) (autosomal recessive) is an inactivating mutation in the vitamin D receptor (VDR). Lab tests show low serum calcium and phosphate, elevated ALP and secondary hyperparathyroidism. Serum 25(OH)D values are normal and the 1,25(OH)2D levels are elevated (key difference from VDDR I).
Malloy et al. reviewed genetic disorders in vitamin D action. They state that VDDR I is an inborn error of vitamin D metabolism coded by the gene CYP27B1. Children with VDDR I present with joint pain/deformity, hypotonia, muscle weakness, growth failure, and hypocalcemic seizures or fractures in early infancy. Treatment is with calcitriol or 1a-hydroxyvitamin D (NOT cholecalciferol). Children with VDDR II present with bone pain, muscle weakness, hypotonia, hypocalcemic convulsions, growth retardation, severe dental caries or teeth hypoplasia. Affected children are resistant to therapy and supra-physiologic doses of all forms of vitamin D.
Illustration A shows the differences between VDDR I and VDDR II. Incorrect Answers
Answers 1, 2, 4, 5: VDDR I is a deficiency of 1a-hydroxylase (predominantly
found in the kidney). The liver enzyme vitamin D 25-hydroxylase (found in hepatocytes) is not responsible for VDDR. VDDR II is caused by an inactivating mutation (rather than an activating mutation).
A 73-year-old female sustains a left hip fracture that is treated with hemiarthroplasty. She has continued pain two months after surgery, and comes to you for a second opinion. Her radiograph is shown in Figure A. Which of the following best describes your responsibility in disclosing to the patient that the pain may be from a medical error?
1) You do not need to disclose this information
2) You legally must disclose this information to the patient
3) You legally must disclose this information to the original hospital's peer review panel
4) You ethically must disclose this information to the patient
5) You ethically must disclose this information to the original surgeon
As a practicing orthopaedic surgeon, you ethically are required to disclose the potential impact of medical errors on patient outcome.
The orthopaedic surgeon is bound ethically but not legally to give his or her best medical opinion, regardless of whether the orthopaedist is the treating physician or the physician who is asked to render a second or additional medical opinion. The best interest of the patient should clearly remain the guiding principal. It is illegal to slander the original physician if the slanderous
information is known or can be proven to be false.
Bhattacharyya et al. review the importance of documentation and ethical treatment of patients when providing second opinions. They note that it is unethical for the consulting orthopaedic surgeon to solicit care of the patient. However, at the sole discretion of the patient, the patient ethically may choose to terminate his or her relationship with his or her treating physician and then enter into another treatment relationship with the consulting
orthopaedic surgeon.
Figure A shows a left hip hemiarthroplasty with the distal component perforated through the medial proximal femur.
Incorrect Answers:
1) This information must be disclosed per ethical recommendations. 2 and 3) There is no legal requirement to disclose this information.
5) There is no documented ethical requirement to disclose this to the original surgeon.
A patient is consented for a right wrist open reduction and internal fixation. After the patient is prepped and draped, a skin incision is made. It is recognized intra-operatively, however, that a skin incision was made on the incorrect side (left). Subsequent right wrist open reduction and internal fixation goes uneventfully. What is the next best course of action?
1) do not tell the patient or family
2) contact the Risk Management department
3) immediately discuss the situation with the patient and family
4) alter the medical record
5) only discuss the situation with the patient if he or she brings it up.
Patients should be approached after a medical error and all errors must be promptly and completely disclosed. The physician should take the lead in the disclosure and not wait for the patient to ask. Risk management should be called as well, but the patient and family should be informed first. It is never appropriate to alter the medical record.
A 14-year-old female has anal hemorrhoids. The General Surgical team has asked for a consultation in regards to her history of hand, wrist, and ankle joint pain and swelling over the past 3 years. Her physical examination reveals a swollen left wrist, right knee and left ankle. Lab work shows low hemoglobin, low albumin, elevated erythrocyte sedimentation rate (ESR), elevated antinuclear antibody (ANA) count, and a negative rheumatoid factor. Radiography of the affected joints are normal. What additional work up is required prior
**to her rectal surgery?**
1) C-reactive protein (CRP)
2) Synovial fluid analysis of affected joints
3) Blood cultures
4) Cervical radiographs
5) Bethesda assay
This patient has a diagnosis of Juvenile Idiopathic Arthritis (JIA). Flexion- extension c-spine radiographs should be ordered to rule out atlantoaxial instability prior to surgery.
JIA is a persistent autoimmune inflammatory arthritis lasting more than 6 weeks in a patient younger than 16 years of age. Serologic testing for this condition will usually show elevated ESR/CRP, low hemoglobin, low albumin and an elevated anti-nuclear antibody (ANA) count, as well as negative rheumatoid factor and positive HLA-B27. Radiographs of the c-spine should be considered in patients undergoing intubation as cervical kyphosis, facet ankylosis, and atlantoaxial subluxation is associated with this condition.
Punaro et al. reviewed rheumatologic conditions in children. The typical patient with oligoarticular JIA is a white female (5:1, F:M), with a peak onset between ages 1 and 3 years. Nearly half of patients have monoarticular involvement, with the knee and ankle being most commonly involved. Uveitis is typically chronic, bilateral, and asymptomatic.
Borchers et al. reviewed juvenile idiopathic arthritis (JIA). They state that no laboratory test can conclusively establish a rheumatic diagnosis. They state that laboratory tests will be negative for systemic inflammation and antinuclear antibody (ANA) test has no use in screening for JIA, as it has a high false positive rate.
Incorrect Answers:
Answer 1: Both ESR and CRP are usually elevated in this condition and provide no further benefit for the operative management of this patient.
Answer 2: This patient has chronic joint swelling and pain. Joint aspirates and synovial fluid analysis would not be required.
Answer 3: There is no suspicion for an acute infection. Therefore, blood cultures are not required.
Answer 5: A Bethesda assay is used to measure the amount of factor VIII or IX antibody in the blood, for patients with hemophilia.
Induction coupling stimulates bone growth through all of the following direct effects EXCEPT:
1) Increased proliferation of osteoblasts
2) Decreased osteoclast differentiation
3) Increase release of TGF-beta1
4) Increased expression of BMP2
5) Increased expression of BMP7
Induction coupling stimulates bone growth by increasing expression of BMP7, BMP2, TGF-beta1, and by increasing osteoblasts proliferation. Induction coupling has not been shown to have the effect of decreasing osteoclast differentiation.
In basic science studies, electrical stimulation (i.e. induction coupling), has been shown to promote bone healing via release of growth factors that induce osteoblast differentiation/proliferation. Electrical current can be placed around bone in various ways, creating a current to stimulate growth factor release and subsequent osteoblast proliferation.
Aaron et al. summarized, in a systematic review, the effects of various types of electrical stimulation on bone and bone healing. Regardless of type (i.e. inductive coupling, capacitive coupling, direct current), they report electricity and/or electromagnetic fields promote gene expression of growth factors that promote an osteogenic environment.
Illustration A depicts a cathode placed directly to allograft with a subcutaneously placed electrical stimulator. Illustration B depicts cathodes placed anteriorly and posteriorly around the hip, connected to an outside power source to create the necessary current. Illustration C depicts an inductive coil placed laterally on the skin in order to create an electrical current.
Incorrect answers:
Answers 1,3-5: All are true effects of electrical stimulation on bone.
Two patients are discharged from a surgicenter after upper extremity procedures. The surgeon gives them prescriptions for oral opioid analgesics. Patient A had open reduction and internal fixation of a distal radius fracture. Patient B had cubital tunnel release without transposition. Which of the following is most likely true regarding analgesic use?
1) Patient A will use more medication than Patient B
2) Patient A will use less medication than Patient B
3) Analgesic use will be similar between Patients A and B
4) Both patients will consume more than 30 pills
5) A reasonable prescription is 40 pills with 1 refill for Patient A, and 40 pills with no refills for Patient B
A patient that has had ORIF will require MORE oral analgesia than a patient who has had a cubital tunnel release.
Patients undergoing bony procedures (e.g. ORIF and arthroplasty) require more analgesia than patients undergoing soft tissue procedures (e.g. carpal/cubital tunnel release, trigger finger release, elbow or shoulder arthroscopy). Overprescribing of opioid analgesia is a common problem. Many opioids are unused in the postoperative period by the patients for whom they were prescribed.
Rodgers et al. reviewed opioid use (oxycodone, hydrocodone, propoxyphene) after outpatient upper extremity surgery. Patients undergoing bony procedures used the most analgesia (14 pills) while those undergoing soft tissue
procedures used the least (9 pills). Half took medication for =
What property of titanium alloys accounts for their high corrosion resistance in vivo?
1) Self-passivation
2) Ductility
3) Hardness
4) Modulus of elasticity
5) Conductivity
In both room temperature air and physiologic fluids, titanium alloys self- passivate or spontaneously form a layer of titanium oxide very rapidly. This layer makes titanium alloys resistant to surface breakdown.
Embolic material generated during total knee arthroplasty (TKA) shown in Figure 29 is composed of which of the following substances?
1) Fat only
2) Fat and air
3) Fat and marrow
4) Fat and cement
5) Fat and bone
Emboli are created during TKA. Usually there is an increased incidence with
the use of intramedullary rods that disrupt the marrow contents. These are not fat emboli per se. They are material composed of fat cells and marrow that act like pulmonary emboli
to obstruct small arterioles in the lung. They are different from free fat emboli that are seen in fractures and that lead to chemical injury to the lung rather than obstructive injury.
There is increasing concern about the ethical relationship of orthopaedists to the orthopaedic equipment industry. Which of the following describes the most appropriate relationship?
1) Industry-paid travel, hotel (for the surgeon and spouse), and registration at a university- sponsored CME course
2) Industry-paid travel and hotel for a faculty member at an industry- sponsored meeting that is not CME approved
3) Consultation agreement ($50,000/annum) between the surgeon and the company for evaluation of the implant system with required oral reporting of impressions
4) A restricted grant from a company to an orthopaedic residency program with the stipulation that the third year residents be sent to an industry- sponsored course
5) Industry-paid dinner at a premium restaurant ($200/person) for surgeon and office staff at which a new set of surgical instrumentation is presented
It is appropriate for orthopaedic surgeons to have relationships with industry as long as the relationship is for the good of the patient and no “quid pro quo” intent exists. A grant to cover registration at a CME event is appropriate but travel and hotel for a spouse is not.
For orthopaedists who are faculty at a meeting sponsored by industry, it is appropriate for travel and expenses to be covered for that faculty member. Care must be exercised that the faculty member contributes in an amount appropriate for the expenses paid. The faculty member must ensure that information presented is unbiased and based on reasonable data and opinion. Consulting agreements should spell out specifically the duties of the agreement and payment should be appropriate for the time spent. There should be a defined work product for the consulting. Agreements that are thinly veiled payments for use of a company’s products must be avoided. In all cases, the agreements must stand up to public
scrutiny. Restricted grants for specific industry-sponsored programs aimed at residents are not appropriate. Unrestricted grants intended for attendance at approved CME courses are appropriate. Dinners at which information is presented about topics that can aid in patient care are appropriate as long as the expense is reasonable ($100 or less/person) and the guest list includes individuals who can use the information in a patient case. Clearly a “premium” dinner for office staff to review new surgical instrumentation would not pass this test.
Figure 33 shows the venogram of a patient who has a long history of alcohol abuse. Warfarin should be used cautiously because of the interaction with which of the following factors?
1) IV
2) V
3) VI
4) VII
5) VIII
Warfarin acts by inhibiting clotting factors II, VII, IX, X. The actual mechanism of action is by inhibition of hepatic enzymes, vitamin K epoxide, and perhaps vitamin K reductase.
This inhibition results in lack of carboxylation of vitamin
K-dependent proteins (II, VII, IX, X). The anticoagulant effect of warfarin can be reversed with vitamin K or fresh-frozen plasma. The use of alcohol may lead to liver dysfunction and an even more limited margin of available factors.
Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
1) It is a disease caused by an abnormality of platelets that leads to increased blood clotting.
2) It is a disease caused by an abnormality of vascular endothelium that leads to increased blood clotting.
3) It is a disease caused by an abnormality of hepatic metabolism that leads to decreased production of factor V and decreased blood clotting.
4) It is a disease caused by an abnormality of factor V that leads to decreased inactivation of factor Va by activated protein C (aPC) and increased blood clotting.
5) It is a familial, genetic disease that requires placement of a Greenfield filter in all
individuals who have the abnormality, prior to surgery.
Factor V Leiden is a disease caused by an abnormality of factor V in which a single amino acid substitution of glutamine for arginine in the protein C cleavage region leads to decreased inactivation of factor V and thus a greater tendency to form clots. More than half of all individuals with Factor V Leiden will develop deep venous thrombosis in the presence of a single additional risk factor such as long bone fracture or total joint arthroplasty.
Which of the following terms best describes the probability of finding a significant association in a research study when one truly exists?
1) Type-1 (alpha) error
2) Type-2 (beta) error
3) Power
4) Alpha level
5) Relative Risk
**
The power of a study is an estimate of the probability of finding a significant association in a research study when one truly exists.
The
Scientific References
- by Kocher and Wojtys are excellent reviews of basic biostatistic principles. Incorrect Answers:
Answer 1: The power is defined by 1 - probability of type-II (beta) error, and is often set at 80%. For example, a power of 80% means that if the
intervention works, the study has an 80% chance of detecting this and a 20% chance of randomly missing it.
Answer 2: A type-II or beta error occurs when one falsely concludes that there is no significant association when there actually is an association (resulting in
a false-negative study that rejects a true alternative hypothesis). The type-II or beta error can be determined if Type I error rate and sample size are known. A type-I or alpha error occurs when a significant association is found when there is no true association (resulting in a false-positive study that rejects a true null hypothesis).
Answer 4:The alpha level refers to the probability of a type-I (alpha) error and is usually set for most studies at 0.05.
Answer 5:The relative risk is a term used in prospective cohorts studies and is the risk of developing disease for people with known exposure compared to risk of developing disease without exposure.
Which of the following substances makes up the majority by weight of the extracellular matrix for articular cartilage?
1) Keratin sulfate
2) Collagen type II
3) Water
4) Protein
5) Chondroitin sulfate
The extracellular matrix consists of water, proteoglycans, and collagen. Water makes up the majority (approximately 65% to 80%) of wet weight; 95% of the collage is type II with much smaller amounts of other collagens, including types IV, VI, IX, X, and XI. The exact functions of these other collagens are unknown, but they are believed to be important in matrix attachment and stabilization of the diameter of collagen fibrils.
A pediatric orthopaedic surgeon refers a child to a neurologist. The neurologist’s office requests the office records of the pediatric orthopaedic surgeon. To maintain Health Insurance Portability and Accountability Act (HIPAA) compliance, what must the surgeon obtain from the parent(s) prior to sending records?
1) No additional consent needed
2) Verbal approval
3) Written approval
4) Written approval with notarization
5) Telephone consent witnessed by a nurse
The privacy rules do not require an individual’s written authorization for certain permitted or required uses and disclosures of the medical records. Patient or parental authorization is not required for disclosures for certain purposes related to treatment, payment, or health care operations. Specifically, HIPAA does not require a covered entity to obtain patient authorization for many of the health care industry’s most fundamental activities such as providing care.
What is the most important consideration in the preoperative evaluation of a child with polyarticular or systemic juvenile rheumatoid arthritis (JRA)?
1) Cervical spine assessment
2) Temporomandibular joint (TMJ)/jaw assessment
3) Dental assessment
4) Stress dosing with corticosteroids
5) Opthalmology examination
**
The cervical spine may be involved in a child with polyarticular or systemic JRA; fusion or instability can occur. Radiographic assessment of the cervical spine should include lateral flexion-extension views. The potential exists for spinal cord injury during intubation or positioning in t
he presence of an unstable cervical spine. Limitations of the TMJ and micrognathia may affect ease of intubation and administration of anesthesia via a mask. If the TMJ and jaw are involved, some patients may have dental findings such as dental caries and even abscesses which can affect surgery. Some children, particularly those with systemic arthritis, may be taking corticosteroids long- term and may need stress dosing with complex surgeries. Although it is important to routinely check for uveitis and iritis in children with JRA, this usually is not needed preoperatively. Uveitis and iritis are less likely in a child with systemic JRA.
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
Question 14High Yield
Following an open reduction and internal fixation (Figures 99a and 99b), radiographs shown in Figures 99c and 99d reveal a nonreduced radial head. An attempted closed reduction of the radial head is unsuccessful. What is the best next step?

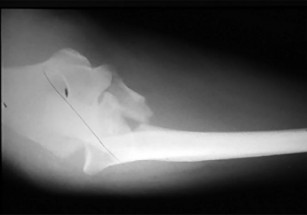





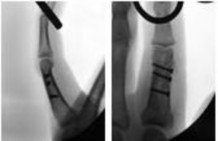
Explanation
A comminuted proximal ulnar fracture is often plated in a shortened position, forcing the radial head into a nonanatomical position. Attempted reduction and pin fixation without addressing the length of the ulna often results in failure, even with a ligament reconstruct. Radial head excision is a salvage procedure. A helpful technique for comminuted proximal ulna fractures is to first pin the radial head in a reduced position and then plate the ulnar out to length.
RECOMMENDED READINGS
15. Heim U. [Combined fractures of the radius and the ulna at the elbow level in the adult. Analysis of 120 cases after more than 1 year]. Rev Chir Orthop Reparatrice Appar Mot. 1998 Apr;84(2):142-53. Review. French. PubMed PMID: 9775058.
16. Morrey BF: Surgical exposures of the elbow. In Morrey BF, ed. The Elbow and its Disorders. 2nd ed. Philadelphia, PA: WB Saunders, 1993:139-166.
17. Ring D, Jupiter JB. Reconstruction of posttraumatic elbow instability. Clin Orthop Relat Res. 2000 Jan;(370):44-56. Review. PubMed PMID: 10660701.
18. Ring D, Jupiter JB, Waters PM. Monteggia fractures in children and adults. J Am Acad Orthop Surg. 1998 Jul-Aug;6(4):215-24. Review. PubMed PMID: 9682084.
**
RECOMMENDED READINGS
15. Heim U. [Combined fractures of the radius and the ulna at the elbow level in the adult. Analysis of 120 cases after more than 1 year]. Rev Chir Orthop Reparatrice Appar Mot. 1998 Apr;84(2):142-53. Review. French. PubMed PMID: 9775058.
16. Morrey BF: Surgical exposures of the elbow. In Morrey BF, ed. The Elbow and its Disorders. 2nd ed. Philadelphia, PA: WB Saunders, 1993:139-166.
17. Ring D, Jupiter JB. Reconstruction of posttraumatic elbow instability. Clin Orthop Relat Res. 2000 Jan;(370):44-56. Review. PubMed PMID: 10660701.
18. Ring D, Jupiter JB, Waters PM. Monteggia fractures in children and adults. J Am Acad Orthop Surg. 1998 Jul-Aug;6(4):215-24. Review. PubMed PMID: 9682084.
**
Question 15High Yield
Reconstruction of the injured structure is performed. After surgery, the patient initially notes limitation in motion, and later develops recurrent instability of the knee. Which factor most likely contributed to the development of instability?
Explanation
The anteromedial bundle originates on the anterior and proximal aspect of the lateral femoral condyle and inserts on the anteromedial aspect of the anterior cruciate ligament (ACL) footprint on the proximal tibia. The posterolateral bundle originates posterior and distal to 63 the anteromedial bundle and inserts on the posterolateral aspect of the tibial footprint. The fibers are parallel when the knee is in an extended position. As the knee moves into flexion,
the fibers of the anteromedial bundle rotate externally with respect to the posterolateral bundle. The anteromedial bundle is tensioned in both flexion and extension. The posteromedial bundle is tensioned in extension, but relaxes as the knee moves into flexion.
The lateral meniscus is more commonly injured with an acute injury to the ACL. The medial meniscus is injured more commonly when the ACL is chronically unstable.
The ACL is an intra-articular and intrasynovial structure. It is innervated by posterior articular branches from the tibial nerve. Innervation of the ACL involves several types of mechanoreceptors (Ruffini, Pacini, Golgi tendon, and free-nerve endings) that may contribute to proprioceptive function of the knee and modulation of quadriceps function.
Injury to the ACL is predominantly associated with instability to anterior translation of the tibia in extension. The ACL plays a secondary role to limit internal rotation of the tibia, and a loss of ACL stability is confirmed by the reduction of the tibia from a position of anterior translation and internal rotation (pivot shift). The radiographs demonstrate anterior placement of the femoral tunnel. The convex shape of the lateral femoral condyle can make it more difficult to visualize the anatomic femoral origin of the ACL. Failure to identify the
anatomic footprint can result in anterior placement of the femoral tunnel. Anterior ACL graft placement can result in its impingement against the posterior cruciate ligament and early limitation of knee flexion. Over time, impingement on the graft may result in stretching of the graft and recurrent knee instability symptoms.
RECOMMENDED READINGS
1. [Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):204-13. Epub 2005 Oct 19. Review. PubMed PMID: 16235056. ](http://www.ncbi.nlm.nih.gov/pubmed/16235056)[View](http://www.ncbi.nlm.nih.gov/pubmed/16235056)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16235056)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16235056)
2. [Zantop T, Petersen W, Sekiya JK, Musahl V, Fu FH. Anterior cruciate ligament anatomy and function relating to anatomical reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006 Oct;14(10):982-92. Epub 2006 Aug 5. Review. PubMed PMID: 16897068. ](http://www.ncbi.nlm.nih.gov/pubmed/16897068)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16897068)
the fibers of the anteromedial bundle rotate externally with respect to the posterolateral bundle. The anteromedial bundle is tensioned in both flexion and extension. The posteromedial bundle is tensioned in extension, but relaxes as the knee moves into flexion.
The lateral meniscus is more commonly injured with an acute injury to the ACL. The medial meniscus is injured more commonly when the ACL is chronically unstable.
The ACL is an intra-articular and intrasynovial structure. It is innervated by posterior articular branches from the tibial nerve. Innervation of the ACL involves several types of mechanoreceptors (Ruffini, Pacini, Golgi tendon, and free-nerve endings) that may contribute to proprioceptive function of the knee and modulation of quadriceps function.
Injury to the ACL is predominantly associated with instability to anterior translation of the tibia in extension. The ACL plays a secondary role to limit internal rotation of the tibia, and a loss of ACL stability is confirmed by the reduction of the tibia from a position of anterior translation and internal rotation (pivot shift). The radiographs demonstrate anterior placement of the femoral tunnel. The convex shape of the lateral femoral condyle can make it more difficult to visualize the anatomic femoral origin of the ACL. Failure to identify the
anatomic footprint can result in anterior placement of the femoral tunnel. Anterior ACL graft placement can result in its impingement against the posterior cruciate ligament and early limitation of knee flexion. Over time, impingement on the graft may result in stretching of the graft and recurrent knee instability symptoms.
RECOMMENDED READINGS
1. [Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):204-13. Epub 2005 Oct 19. Review. PubMed PMID: 16235056. ](http://www.ncbi.nlm.nih.gov/pubmed/16235056)[View](http://www.ncbi.nlm.nih.gov/pubmed/16235056)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16235056)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16235056)
2. [Zantop T, Petersen W, Sekiya JK, Musahl V, Fu FH. Anterior cruciate ligament anatomy and function relating to anatomical reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006 Oct;14(10):982-92. Epub 2006 Aug 5. Review. PubMed PMID: 16897068. ](http://www.ncbi.nlm.nih.gov/pubmed/16897068)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16897068)
Question 16High Yield
Figures 1 and 2 are the radiographs of a 16-year-old boy who falls following a seizure. He is unable to bear weight on the right lower extremity following the fall. Over the subsequent 24 hours, his leg becomes progressively more painful and swollen. He is taken to the emergency department where on initial assessment his pain is out of proportion, positive stretch pain, tense leg swelling, and decreased motor function of his foot muscles with decreased sensations throughout the foot. Toes are warm and well-perfused. What is the best next step in management of this patient?

Explanation
■
The radiographs reveal an Ogden type 4 tibial tubercle fracture. The clinical examination of the patient is highly suggestive of compartment syndrome.
Tibial tubercle fractures have been associated with the development of compartment syndrome, with rates as high as 10% reported in literature. It is caused by disruption of the branches of the recurrent anterior tibial artery, which travels on the lateral border of the tubercle. At the time of injury, the artery may be injured and retract under the fascia in the anterior compartment of the leg, leading to excessive bleeding in the anterior compartment. Patients with compartment syndrome should be emergently taken to the OR for fasciotomy and ORIF of the fracture.
Emergent fasciotomy of the leg with posterior splint is not called for, as this fracture needs anatomic reduction and fixation to prevent procurvatum deformity of proximal tibia. CT scan of the knee is not appropriate because this is compartment syndrome, which needs emergent fasciotomy.
This situation needs ORIF for anatomic reduction of the fracture with emergent fasciotomy for compartment syndrome of the leg. Closed reduction and percutaneous screw fixation is not the right option here.
■
The radiographs reveal an Ogden type 4 tibial tubercle fracture. The clinical examination of the patient is highly suggestive of compartment syndrome.
Tibial tubercle fractures have been associated with the development of compartment syndrome, with rates as high as 10% reported in literature. It is caused by disruption of the branches of the recurrent anterior tibial artery, which travels on the lateral border of the tubercle. At the time of injury, the artery may be injured and retract under the fascia in the anterior compartment of the leg, leading to excessive bleeding in the anterior compartment. Patients with compartment syndrome should be emergently taken to the OR for fasciotomy and ORIF of the fracture.
Emergent fasciotomy of the leg with posterior splint is not called for, as this fracture needs anatomic reduction and fixation to prevent procurvatum deformity of proximal tibia. CT scan of the knee is not appropriate because this is compartment syndrome, which needs emergent fasciotomy.
This situation needs ORIF for anatomic reduction of the fracture with emergent fasciotomy for compartment syndrome of the leg. Closed reduction and percutaneous screw fixation is not the right option here.
Question 17High Yield
What is the most common cause for late revision (> 2 years post op) total knee arthroplasty?

Explanation
DISCUSSION: There are multiple causes for failure of total knee arthroplasty, and more than one may exist at the same time. Sharkey and associates reviewed a series of revision total knee arthroplasties, and found that polyethylene failure was the most common cause of failure followed closely by component loosening. The most common cause of early failure (< 2 years post op) was infection. Instability and malalignment are both complications of surgical technique, and if these categories are combined, they would be the most common cause of all total knee failures.
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
Figure 59a Figure 59b
DISCUSSION: There are multiple causes for failure of total knee arthroplasty, and more than one may exist at the same time. Sharkey and associates reviewed a series of revision total knee arthroplasties, and found that polyethylene failure was the most common cause of failure followed closely by component loosening. The most common cause of early failure (< 2 years post op) was infection. Instability and malalignment are both complications of surgical technique, and if these categories are combined, they would be the most common cause of all total knee failures.
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
Figure 59a Figure 59b
Question 18High Yield
Which of the following variables has not been shown to be increased in patients who sustain bilateral femoral shaft fractures as compared to patients with unilateral femoral shaft fractures?
Explanation
Bilateral femur fractures have not been shown to have increased rates of thoracic/chest wall injury. They have been shown to have increased rates of initial hypotension, mortality, open skull fractures, and pelvic fractures.
Due to their high-energy nature, bilateral femur fractures have increased rates of initial hypotension or hemodynamic instability, mortality, head injuries, abdominal injuries, pulmonary injuries, and other orthopaedic injuries.
Copeland et al. performed a retrospective analysis using their trauma registry data on consecutive blunt trauma patients with unilateral (800 patients) or bilateral (85 patients) femoral shaft fractures. Patients with bilateral femoral fractures had a significantly higher Injury Severity Score (30.2 versus 24.5, p
< 0.05) and higher mortality rate (25.9 vs 11.7%, p < 0.014) than patients with unilateral femoral fractures. Bilateral fracture patients also had significantly more closed head injuries, open skull fractures, intra-abdominal injuries requiring surgical intervention, and pelvic fractures. Regression analysis of variables evident on admission revealed a significant correlation between bilateral femoral fractures and death; however, other factors (shock, closed head injury, and thoracic injury) had much stronger correlations with mortality. No increase in risk of thoracic injury was seen with bilateral injuries as compared to unilateral injuries.
Kobbe et al. also reviewed their trauma registry data on 776 patients with unilateral and 118 patients with bilateral femoral shaft fractures. They found that bilateral femur fracture patients has a higher ISS score, higher incidence of delayed pulmonary failure and multiple organ failure, and higher mortality. They also noted that patients with bilateral femoral shaft fractures have
significantly more often severe abdominal injuries as well as severe blood loss which may account for the increased mortality rate.
Incorrect Answers:
Answer 1: Increased rates of hypotension upon admission are seen in the bilateral group.
Answer 2: Increased mortality rates have been reported in bilateral femur patients.
Answer 4: Increased rates of open and closed head injuries are noted in bilateral femur patients.
Answer 5: Increased rates of pelvic and other orthopaedic injuries are reported in the bilateral group.
Due to their high-energy nature, bilateral femur fractures have increased rates of initial hypotension or hemodynamic instability, mortality, head injuries, abdominal injuries, pulmonary injuries, and other orthopaedic injuries.
Copeland et al. performed a retrospective analysis using their trauma registry data on consecutive blunt trauma patients with unilateral (800 patients) or bilateral (85 patients) femoral shaft fractures. Patients with bilateral femoral fractures had a significantly higher Injury Severity Score (30.2 versus 24.5, p
< 0.05) and higher mortality rate (25.9 vs 11.7%, p < 0.014) than patients with unilateral femoral fractures. Bilateral fracture patients also had significantly more closed head injuries, open skull fractures, intra-abdominal injuries requiring surgical intervention, and pelvic fractures. Regression analysis of variables evident on admission revealed a significant correlation between bilateral femoral fractures and death; however, other factors (shock, closed head injury, and thoracic injury) had much stronger correlations with mortality. No increase in risk of thoracic injury was seen with bilateral injuries as compared to unilateral injuries.
Kobbe et al. also reviewed their trauma registry data on 776 patients with unilateral and 118 patients with bilateral femoral shaft fractures. They found that bilateral femur fracture patients has a higher ISS score, higher incidence of delayed pulmonary failure and multiple organ failure, and higher mortality. They also noted that patients with bilateral femoral shaft fractures have
significantly more often severe abdominal injuries as well as severe blood loss which may account for the increased mortality rate.
Incorrect Answers:
Answer 1: Increased rates of hypotension upon admission are seen in the bilateral group.
Answer 2: Increased mortality rates have been reported in bilateral femur patients.
Answer 4: Increased rates of open and closed head injuries are noted in bilateral femur patients.
Answer 5: Increased rates of pelvic and other orthopaedic injuries are reported in the bilateral group.
Question 19High Yield
She completes the necessary testing and wishes to proceed with revision surgery. The most appropriate surgical option in this scenario involves implant removal and
Explanation
- reverse total shoulder arthroplasty (rTSA)._
Question 20High Yield
According to clinical and biomechanical studies, the most appropriate position for a headless scaphoid compression screw for repair of a scaphoid waist fracture is
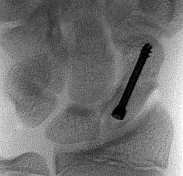
Explanation
The position of a scaphoid screw for scaphoid fracture repair (Figure 1) is as critical as the position of a sliding hip screw for intertrochanteric fracture repair. Positioning the screw deep in the center of the densest portion of cancellous bone is beneficial for both of these fracture types.Trumble and associates have shown time to union for scaphoid nonunions to be decreased for centrally placed scaphoid screws. McCallister and associates documented improved biomechanical stability for scaphoid waist fractures repaired with a centrally placed screw vs an eccentrically placed screw. Dodds and associates
---
demonstrated significantly improved biomechanical stability with centrally placed long screws vs centrally placed short screws. The screw may be placed retrograde or antegrade. Although the screw position may be relatively parallel to the radial inclination as the shape of the scaphoid body follows the contour of the radial styloid, screw position should be assessed relative to the scaphoid’s own architecture. Placing the screw in a retrograde fashion can force the treating surgeon to start the screw eccentrically in an attempt to avoid the interference of the trapezium lying over the distal pole of the scaphoid. This may result in noncentral screw placement.
---
demonstrated significantly improved biomechanical stability with centrally placed long screws vs centrally placed short screws. The screw may be placed retrograde or antegrade. Although the screw position may be relatively parallel to the radial inclination as the shape of the scaphoid body follows the contour of the radial styloid, screw position should be assessed relative to the scaphoid’s own architecture. Placing the screw in a retrograde fashion can force the treating surgeon to start the screw eccentrically in an attempt to avoid the interference of the trapezium lying over the distal pole of the scaphoid. This may result in noncentral screw placement.
Question 21High Yield
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0° F (35° C). What is the recommended treatment of the femoral fracture at this time?
Explanation
This is a “borderline trauma” patient where serious consideration for damage control orthopaedic surgery is required. His prolonged hypotension, abdominal injury, and chest injury put him at higher risk for serious postinjury complications. Further surgery, such as definitive fracture fixation, adds metabolic load and injury to his system. It is prudent to consider femoral fracture stabilization with an external fixator until he is physiologically recovered as evidenced by a normal base excess and/or lactate acid levels, as well as all other parameters of resuscitation. A borderline patient has been described as polytrauma with an ISS > 20 and thoracic trauma (AIS > 2); polytrauma and abdominal/pelvic trauma (Moore > 3) and hemodynamic shock (initial BP 40; bilateral lung contusions on radiographs; initial mean pulmonary arterial pressure > 24 mm Hg; pulmonary artery pressure increase during intramedullary nailing > 6 mm Hg. Factors that worsen the situation following surgery include multiple long bones and truncal injury (AIS > 2), estimated surgery time of more than 6 hours, arterial injury and hemodynamic instability, and exaggerated inflammatory response (eg, Il-6 > 800 pg/mL). It is incumbent on the orthopaedic surgeon who is a member of the trauma team to make sure that he or she is aware of these factors and guides the team to the best patient care.
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Bosse M, Kellam JF: Orthopaedic decision making in the multiple trauma patient, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 133-146.
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Bosse M, Kellam JF: Orthopaedic decision making in the multiple trauma patient, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 133-146.
Question 22High Yield
What is the most common non-anesthetic-related reversible cause of sustained changes in intraoperative neurophysiologic monitoring signals during spinal surgery?
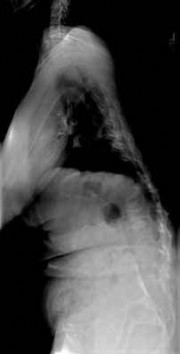
Explanation
Patient positioning that results in local nerve compression, plexus traction, or improper neck alignment is the most common non-anesthetic-related cause of changes in intraoperative neurophysiologic monitoring data during spinal surgery. Pedicle screw malpositioning, spinal cord ischemia, and retractor placement are all less common causes. Hypotension, not hypertension, can be a cause of intraoperative neurophysiologic changes.
---
---
Question 23High Yield
You are asked to consult on a 4-day-old neonate admitted because of failure to thrive. She has swelling of her left shoulder. Examination reveals limited motion of her hips and left shoulder. Radiographs of the shoulder and pelvis are negative. Laboratory studies show a WBC count of 24,000/mm3, an erythrocyte sedimentation rate of 50/h, and C-reactive protein is 16.4. What is the next most appropriate step in management?
Explanation
DISCUSSION: Ultrasound of both the hip and the shoulder can show the presence of septic arthritis and osteomyelitis. Multiple sites of infection are common in neonates. A bone scan can be used to identify other areas of involvement.
REFERENCES: Wong M, Isaacs D, Howman-Giles R, et al: Clinical and diagnostic features of osteomyelitis occurring in the first three months of life. Pediatr Infect Dis J 1995;14:1047-1053.
Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 57-73.
REFERENCES: Wong M, Isaacs D, Howman-Giles R, et al: Clinical and diagnostic features of osteomyelitis occurring in the first three months of life. Pediatr Infect Dis J 1995;14:1047-1053.
Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 57-73.
Question 24High Yield
A 23-year-old student complains of recurrent left shoulder instability. He first dislocated his shoulder in high school while playing lacrosse and was managed with physical therapy. A second dislocation occurred one year later while skiing. He has since sustained two more dislocations and says that his shoulder feels “loose.” Examination reveals grade II anterior load and shift, positive apprehension and relocation tests, and normal rotator cuff strength. An MRI arthrogram is ordered and surgical treatment is recommended. What factor would most strongly represent an indication for a procedure including bone augmentation (e.g. Latarjet) rather than a soft-tissue-only stabilization (isolated labral repair/capsulorrhaphy)?
Explanation
There is much debate in the literature regarding optimal techniques for treatment of shoulder instability. Barring other factors or concomitant pathology, however, there is no persuasive literature to suggest routine use of bone augmentation for contact athletes. Extensive labral involvement (here specifically implying posterior labral involvement, as well) will require a more extensive repair but does not, in and of itself, suggest the necessity for
glenoid bone augmentation. A large Hill-Sachs lesion may be an indication for glenoid augmentation, primarily if it is in a location/orientation that engages the anterior glenoid rim. These are referred to as “off-track” lesions. Of these choices, the strongest indication for a Latarjet coracoid transfer or similar bone augmentation (other options include iliac crest autograft or distal tibial allograft) is high-grade glenoid bone loss. Classically, this is performed through an open approach, although arthroscopic techniques are increasing in popularity. Although the critical amount of bone loss is debated, most surgeons and studies suggest a cut-off of approximately 20% to 25%, above
which isolated soft-tissue stabilization alone is less likely to be successful in the long-term.
glenoid bone augmentation. A large Hill-Sachs lesion may be an indication for glenoid augmentation, primarily if it is in a location/orientation that engages the anterior glenoid rim. These are referred to as “off-track” lesions. Of these choices, the strongest indication for a Latarjet coracoid transfer or similar bone augmentation (other options include iliac crest autograft or distal tibial allograft) is high-grade glenoid bone loss. Classically, this is performed through an open approach, although arthroscopic techniques are increasing in popularity. Although the critical amount of bone loss is debated, most surgeons and studies suggest a cut-off of approximately 20% to 25%, above
which isolated soft-tissue stabilization alone is less likely to be successful in the long-term.
Question 25High Yield
Figure 1
A 21-year-old man presents for evaluation of high arches, which have been present his entire life. C urrently, he is experiencing some discomfort with running activities. His brother and mother have high arches. He does not recall any trauma as a child, or any other pertinent childhood musculoskeletal problems. C linical examination reveals a rigid deformity bilaterally. What structure is responsible for plantarflexion of the first metatarsal:
A 21-year-old man presents for evaluation of high arches, which have been present his entire life. C urrently, he is experiencing some discomfort with running activities. His brother and mother have high arches. He does not recall any trauma as a child, or any other pertinent childhood musculoskeletal problems. C linical examination reveals a rigid deformity bilaterally. What structure is responsible for plantarflexion of the first metatarsal:
Explanation
The peroneus longus passes under the cuboid to function as a plantar flexor of the first metatarsal. It is a primary deforming force in the development of the cavus foot.
Question 26High Yield
Which key factor that induces osteoclastogenesis is secreted by osteoblasts in response to inflammatory stimuli?
Explanation
**
Osteoclasts are derived from cells of the monocyte/macrophage lineage. They are multinucleated and develop by fusion of mononuclear precursors, a process that requires receptor activator for nuclear factor kappa-B ligand (RANKL) and macrophage-colony stimulating factor (M-CSF). RANKL is secreted by osteoblasts in response to inflammatory signals and is a key component of inflammation-mediated osteolysis. OPG binds to and sequesters RANKL, thus inhibiting osteoclast differentiation and activity.
BMP and IGF-1 are potent regulators of osteoblast differentiation and activation. TNF is a cytokine secreted by macrophages and degranulating platelets infiltrated in the fracture site and impacts a variety of cells, not osteoclasts.
Osteoclasts are derived from cells of the monocyte/macrophage lineage. They are multinucleated and develop by fusion of mononuclear precursors, a process that requires receptor activator for nuclear factor kappa-B ligand (RANKL) and macrophage-colony stimulating factor (M-CSF). RANKL is secreted by osteoblasts in response to inflammatory signals and is a key component of inflammation-mediated osteolysis. OPG binds to and sequesters RANKL, thus inhibiting osteoclast differentiation and activity.
BMP and IGF-1 are potent regulators of osteoblast differentiation and activation. TNF is a cytokine secreted by macrophages and degranulating platelets infiltrated in the fracture site and impacts a variety of cells, not osteoclasts.
Question 27High Yield
A 45-year-old man underwent a fingertip amputation through the distal phalanx after his ring finger was caught in a garage door. He was treated in the emergency department with a revision amputation by advancement of the flexor digitorum profundus (FDP) tendon to the extensor mechanism. Three months following the injury, he is able to fully flex his injured ring finger to touch his palm, but he reports that it is difficult for him to make a tight fist due to decreased flexion of his other fingers. What is this complication called?
Explanation
The quadrigia effect can occur due to over-advancement of the FDP tendon during repair (usually greater than 1 cm), development of FDP tendon adhesions, and (as in this case) "over the top" repair of the FDP tendon to the extensor tendon after amputation at the distal phalanx level. All of these conditions result in a functionally shortened FDP tendon of the injured digit. Because the FDP tendons of the long, ring, and small digits share a common muscle belly, excursion of the combined tendons is equal to the shortest tendon. Therefore, the uninjured digits will not have full excursion of their respective FDP tendons and will not be able to close into a full fisting position. Treatment of this condition is most commonly release
of the injured FDP tendon. A lumbrical plus deformity can occur in amputations distal to the flexor digitorum superficialis insertion through the middle phalanx. The FDP tendon retracts and increases tension on the lumbrical muscle, which leads to paradoxical interphalangeal (IP) joint extension with attempted flexion. Intrinsic tightness and interphalangeal joint contractures can be caused by hand trauma _but would not lead to the clinical condition this patient has._
of the injured FDP tendon. A lumbrical plus deformity can occur in amputations distal to the flexor digitorum superficialis insertion through the middle phalanx. The FDP tendon retracts and increases tension on the lumbrical muscle, which leads to paradoxical interphalangeal (IP) joint extension with attempted flexion. Intrinsic tightness and interphalangeal joint contractures can be caused by hand trauma _but would not lead to the clinical condition this patient has._
Question 28High Yield
Figure 1 is the MRI scan of a high school hockey player who is checked from behind and falls forward to the ice onto his flexed knees. He complains of swelling and posterior knee pain. Nonoperative treatment of the injured structure will most likely result in increased risk of degenerative change in
Explanation
The injury mechanism and MRI scans demonstrate an isolated posterior cruciate ligament (PCL) tear. PCL injury may result in posterior translational macro-instability of the knee, but may
also result in more subtle and subclinical increases in varus and posterior tibial translation during normal gait and other activities of daily living. These changes result in increased contact stresses in the medial (due to varus forces) and patellofemoral (due to posterior forces) compartments, leading to an increased risk of degenerative chondrosis in these areas.
5
also result in more subtle and subclinical increases in varus and posterior tibial translation during normal gait and other activities of daily living. These changes result in increased contact stresses in the medial (due to varus forces) and patellofemoral (due to posterior forces) compartments, leading to an increased risk of degenerative chondrosis in these areas.
5
Question 29High Yield
Figures 52a through 52c show the biopsy of this lesion. Based on the clinical history, radiograph, and biopsy, which diagnosis is most likely?
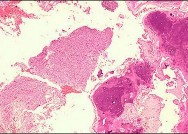
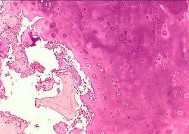
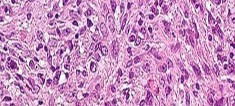
Explanation
- Dedifferentiated chondrosarcoma_
Question 30High Yield
Figure 1 is the anteroposterior radiograph of a 20-year-old dancer who fell during his routine and injured his right foot. What is the most appropriate treatment?
Explanation
This patient has sustained a Lisfranc fracture dislocation of the forefoot. To fully restore foot function, an open reduction and internal fixation should be performed to anatomically reduce this dislocation. Closed reduction is unlikely to restore normal foot biomechanics and would likely result in delayed arthritis and joint incongruity. Posterior splint immobilization, CAM walker ambulation, and in situ percutaneous pinning will not adequately reduce the fracture and restore normal function to the foot.
Question 31High Yield
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality
and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?
and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?

Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 32High Yield
Figure 6 shows the radiograph of a 72-year-old woman who underwent a primary total hip arthroplasty
17 years ago. She now reports groin pain. Optimal surgical management should consist of which of the following?
17 years ago. She now reports groin pain. Optimal surgical management should consist of which of the following?
Explanation
DISCUSSION: Polyethylene wear is evident due to the superiorly eccentric position of the femoral head within the acetabulum. Despite proximal femoral osteolysis, the component appears well fixed, as does the acetabulum. The acetabular component appears to be well positioned. Therefore, an isolated synovectomy and polyethylene liner exchange is indicated. If the hip is stable, there is no need for more extensive revision work.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 521-528.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 521-528.
Question 33High Yield
In the MRI scan shown in Figure 1, what is it about this fracture pattern that increases its risk of nonunion?

Explanation
■
The patient has sustained a type 2 odontoid fracture. This is a common injury in elderly patients secondary to a hyperextension injury. The blood supply is tenuous and posterior displacement has been found to increase the risk of a nonunion.
The patient has sustained a type 2 odontoid fracture. This is a common injury in elderly patients secondary to a hyperextension injury. The blood supply is tenuous and posterior displacement has been found to increase the risk of a nonunion.
Question 34High Yield
A 6-year-old boy with spina bifida and L3 motor level presents to the clinic with bilateral swollen legs (below the knees). His legs have been swollen for the past 3 days and his knees are warm. The patient has an oral temperature of 38.1°C . He denies any pain. There is no history of systemic infection or of any other trauma. The problem may be most likely diagnosed by ordering:
Explanation
Low-energy fractures are the most likely cause of the patientâs bilateral swollen legs. The fractures may occur with everyday activities, and they do not cause pain because of the patientâs high neurologic level. If plain radiographs do not give the diagnosis, stress radiographs should be obtained to detect undisplaced physeal fractures.
Deep vein thrombosis is rare in this age group, especially bilaterally.
Spontaneous joint infection and spontaneous osteomyelitis are not any more likely in patients with spina bifida than in the general population.
Deep vein thrombosis is rare in this age group, especially bilaterally.
Spontaneous joint infection and spontaneous osteomyelitis are not any more likely in patients with spina bifida than in the general population.
Question 35High Yield
Figures 88a through 88d are the radiographs and biopsy specimens of a 65-year-old woman with a history of breast cancer who has been experiencing 6 weeks of increasing left hip pain. She denies any injury. What is the most likely diagnosis?
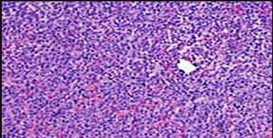
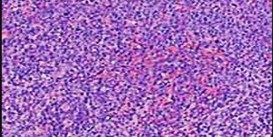


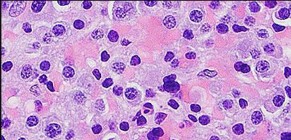
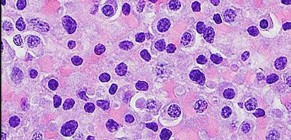
Explanation
Radiographs reveal a destructive lesion. A differential diagnosis would include metastatic disease, myeloma, lymphoma, or primary sarcoma of bone. Histology shows sheets of plasma cells with eccentric nuclei, coarsely clumped nuclear chromatin, and a perinuclear halo. This pathology is consistent with myeloma. Metastatic disease would reveal nests of epithelia cells in a fibrous
background. Fibrous dysplasia would reveal irregular bony trabecular without rimming osteoblasts. Osteosarcoma would reveal malignant cells making osteoid.
RECOMMENDED READINGS
80. [Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011 Mar 17;364(11):1046-60. doi: 10.1056/NEJMra1011442. Review. PubMed PMID: 21410373. ](http://www.ncbi.nlm.nih.gov/pubmed/21410373)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21410373)
81. Swerdlow S, Campo E, Harris N, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW, eds. _WHO Classification of Tumors of Haematopoietic and Lymphoid Tissues_ , 4th ed. Lyon, France: IARC Press; 2008.
background. Fibrous dysplasia would reveal irregular bony trabecular without rimming osteoblasts. Osteosarcoma would reveal malignant cells making osteoid.
RECOMMENDED READINGS
80. [Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011 Mar 17;364(11):1046-60. doi: 10.1056/NEJMra1011442. Review. PubMed PMID: 21410373. ](http://www.ncbi.nlm.nih.gov/pubmed/21410373)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21410373)
81. Swerdlow S, Campo E, Harris N, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW, eds. _WHO Classification of Tumors of Haematopoietic and Lymphoid Tissues_ , 4th ed. Lyon, France: IARC Press; 2008.
Question 36High Yield
Treatment should address predictable
Explanation
- instability of the fracture.
Question 37High Yield
A 17-year-old high school basketball player reports chronic pain in the posterior aspect of the right ankle. He denies any injury. His pain is made worse by jumping and “taking off’ the right leg while doing layups. Examination reveals no discernible swelling. He has full active and passive range of motion of the ankle, although maximal passive plantar flexion is painful posteriorly. He is unable to do a single-leg toe raise. He has no tenderness or palpable mass over the Achilles tendon. Motor function to the foot is within normal limits, and his neurovascular examination is intact. A lateral radiograph is shown in Figure 63a and an MRI scan is shown in Figure 63b. Which of the following treatment options has the highest likelihood of success for this condition?
Explanation
DISCUSSION: The patient’s history, examination, and imaging studies are consistent with the os trigonum syndrome. The os trigonum is an accessory ossification center of the posterior process of the talus. It can become painful in some athletes after ankle dorsiflexion or jumping, and is most common in ballet dancers and basketball players. Traumatic disruption of the synchondrosis between the os trigonum and the talus can lead to pain. MRI imaging of these injuries typically shows fluid surrounding the os with associated marrow
edema. There is usually no marrow edema in the talus to suggest an acute fracture of the posterior process. These injuries are definitively managed with excision (either open or arthroscopic) of the inflamed os trigonum with return to sports expected within 2 to 3 months. Physical therapy may provide short-term relief but is unlikely to provide permanent relief. Corticosteroid injection is not recommended in this location.
Surgical fixation is not indicated for this entity.
REFERENCES: Chao W: Os trigonum. Foot Ankle Clin 2004;9:787-796.
Kadel N: Excision of os trigonum. Operative Techniques in Orthopaedics 2004; 14:1-5. Davies M: The os trigonum syndrome. Foot 2004; 14:119-123.
edema. There is usually no marrow edema in the talus to suggest an acute fracture of the posterior process. These injuries are definitively managed with excision (either open or arthroscopic) of the inflamed os trigonum with return to sports expected within 2 to 3 months. Physical therapy may provide short-term relief but is unlikely to provide permanent relief. Corticosteroid injection is not recommended in this location.
Surgical fixation is not indicated for this entity.
REFERENCES: Chao W: Os trigonum. Foot Ankle Clin 2004;9:787-796.
Kadel N: Excision of os trigonum. Operative Techniques in Orthopaedics 2004; 14:1-5. Davies M: The os trigonum syndrome. Foot 2004; 14:119-123.
Question 38High Yield
Six months after surgical repair, the patient reports that when tapping over her central midfoot incision, paresthesias to the third and fourth toes occur. What is the most likely diagnosis?
Explanation
- Neuritis of the superficial peroneal nerve
Question 39High Yield
-Reverse total shoulder arthroplasty improves kinematics in the rotator cuff deficient joint by what directional change to the center of rotation?
Explanation
No detailed explanation provided for this question.
Question 40High Yield
A 72-year-old female sustains a displaced intracapsular femoral neck fracture. Which of the following is TRUE regarding the long term differences between possible treatment options for this injury?
Explanation
Elderly patients with femoral neck fractures (FNF) undergoing total hip arthroplasty (THA) are less likely to require reoperation than those undergoing internal fixation.
Intracapsular FNF are common in elderly patients after a fall from standing height. Treatment depends on physiological age and displacement (Garden's classification). For displaced fractures, physiologically young patients are treated with internal fixation while physiologically old patients are treated with
either hemiarthroplasty (debilitated, less active patients) or THA (more active patients, those with acetabular disease or preexisting inflammatory arthritis).
Chammout et al. retrospectively compared the long term (17 years) results of THA (cemented both component) and ORIF (2 cannulated screws) in elderly patients (>65 years). They found no difference in mortality. But hip scores were higher and pain was better in the THA group, while reoperation rates were higher in the ORIF group. Walking speed was initially faster in the THA group, but later did not differ between groups. They recommend THA for elderly patients with displaced FNF.
Rogmark et al. prospectively compared closed reduction and internal fixation (CRIF) with arthroplasty (combining hemiarthroplasty and THA) at 2 years in elderly patients (>70 years). Failure rates were higher, pain was worse, and walking was more impaired after CRIF. They recommend arthroplasty for patients >70 with FNF.
Incorrect Answers:
Answer 1: Patients undergoing THA are more likely to have less pain than internal fixation.
Answer 3: Patients undergoing THA have superior functional outcome scores. Answer 4: Patients undergoing THA perform ADL better in the short term. In the long term, there is no difference in ADL between the groups.
Answer 5: Mortality rates are similar after the two procedures.
Intracapsular FNF are common in elderly patients after a fall from standing height. Treatment depends on physiological age and displacement (Garden's classification). For displaced fractures, physiologically young patients are treated with internal fixation while physiologically old patients are treated with
either hemiarthroplasty (debilitated, less active patients) or THA (more active patients, those with acetabular disease or preexisting inflammatory arthritis).
Chammout et al. retrospectively compared the long term (17 years) results of THA (cemented both component) and ORIF (2 cannulated screws) in elderly patients (>65 years). They found no difference in mortality. But hip scores were higher and pain was better in the THA group, while reoperation rates were higher in the ORIF group. Walking speed was initially faster in the THA group, but later did not differ between groups. They recommend THA for elderly patients with displaced FNF.
Rogmark et al. prospectively compared closed reduction and internal fixation (CRIF) with arthroplasty (combining hemiarthroplasty and THA) at 2 years in elderly patients (>70 years). Failure rates were higher, pain was worse, and walking was more impaired after CRIF. They recommend arthroplasty for patients >70 with FNF.
Incorrect Answers:
Answer 1: Patients undergoing THA are more likely to have less pain than internal fixation.
Answer 3: Patients undergoing THA have superior functional outcome scores. Answer 4: Patients undergoing THA perform ADL better in the short term. In the long term, there is no difference in ADL between the groups.
Answer 5: Mortality rates are similar after the two procedures.
Question 41High Yield
Compared with the medial parapatellar approach for total knee arthroplasty (TKA), quadriceps-sparing approaches are associated with
Explanation
Quadriceps-sparing approaches for TKA have shown higher risk of implant malalignment compared with the traditional medial parapatellar approach. No consistent clinically significant benefit to patient-reported outcomes has been demonstrated with quadriceps-sparing TKA, nor is there a significant improvement in postoperative quadriceps strength. Longer surgical and tourniquet times have been observed with “minimally invasive” approaches.
Question 42High Yield
Figure 29Figure 29 is the radiograph of a 30-year-old man who sustained an isolated tibial shaft fracture. What is the most common deformity with nonsurgical management?
Explanation
No detailed explanation provided for this question.
Question 43High Yield
Figures 1 and 2 are the MRI scans of a 21-year-old swimmer who has had pain in the lateral shoulder for 6 months. It is worse while swimming and with reaching overhead. Twelve weeks of physical therapy and a single corticosteroid injection have failed to improve her symptoms. What is the best next step?
18
18
Explanation
In the MRI scans, the patient has a high-grade tear of the undersurface of the superior rotator cuff. This is known as a partial articular-sided tendon avulsion lesion. This is often seen in overhead athletes and is associated with internal impingement. Given the length of symptoms, failure to respond to nonsurgical treatment, and the high-grade nature of the tear in a young patient, an arthroscopic repair should be performed. The available images do not demonstrate evidence of SLAP tear, Bankart lesion, or suprascapular nerve compression.
Question 44High Yield
The likely detached ligamentous lesion is tightest when the position of the shoulder is
Explanation
- 90-degree abduction, external rotation._
Question 45High Yield
A 21-year-old Division 1 collegiate track and field athlete has had acute worsening right anterior shin pain for the past week. He reports having shin pain since sophomore year of high school but has continued to run through the pain. Upon presentation, he was diagnosed with a tibial stress fracture and underwent 8 weeks of nonoperative treatment and correction of vitamin D levels. His follow-up radiograph is shown in Figure
Explanation
The case and radiograph describe a chronic anterior tibial stress fracture with radiographic evidence of the "dreaded black line". Both tibial IM nailing and compression plating are acceptable treatment options in the high-level athlete and are associated with a high rate of return to sport. Compression plating results in a higher rate of symptomatic hardware (20%) as compared with tibial IM nailing. Time to radiographic union may be faster with compression plating. This may be due to the mechanical advantage of neutralizing tensile forces and fracture micromotion. Plating avoids disruption of the knee extensor mechanism and the anterior knee pain associated with IM nailing. There are several reports of fracture completion after tibial IM nailing, requiring revision open reduction and internal fixation.
Question 46High Yield
Which of the following noncollagenous proteins aid in regulating the maturation of bone mineral crystals:
Explanation
Bone sialoproteins are important in the initiation of mineralization of collagen. They promote apatite nucleation and growth of the crystals. Osteocalcin (bone Gla protein) is important for mineral proliferation and maturation.
Note the role of promoters and inhibitors: Apatite nucleation and growth Promoters
Type I collagen Bone sialoprotein Matrix vesicles Phosphoproteins Proteolipids Biglycan
Inhibitors
Large proteoglycans Pyrophosphate Adenosine triphosphate Citrate
Mineral proliferation
Regulators
Osteocalcin Phosphoproteins Proteoglycans
Note the role of promoters and inhibitors: Apatite nucleation and growth Promoters
Type I collagen Bone sialoprotein Matrix vesicles Phosphoproteins Proteolipids Biglycan
Inhibitors
Large proteoglycans Pyrophosphate Adenosine triphosphate Citrate
Mineral proliferation
Regulators
Osteocalcin Phosphoproteins Proteoglycans
Question 47High Yield
Figures 33a through 33d are the radiograph, MR images, and biopsy specimen of a 66-year-old woman with a several-month history of an enlarging thigh mass after “pulling a muscle” while playing softball. Several weeks ago her physician aspirated the cyst, but the result is no change. Treatment of this lesion should include

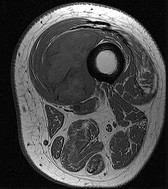
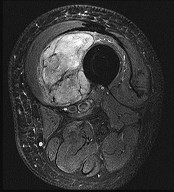
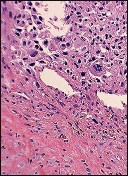
Explanation
This patient’s imaging and biopsy specimen are consistent with a high-grade undifferentiated pleomorphic sarcoma (UPS). Histologically, UPS is characterized by high cellularity, marked nuclear pleomorphism, abundant mitotic activity (including atypical mitoses), and a spindle cell morphology. Necrosis is common and characteristic of high-grade lesions. Treatment consists of wide surgical excision and, in almost all cases, radiation. Radiation eliminates the need for limb amputation, and there is level I evidence to show that it leads to equivalent rates of survival. Radiation may be delivered either before or after surgery depending on the surgeon’s and multidisciplinary tumor board’s recommendations. There may be a role for presurgical embolization in some cases of high-grade soft-tissue sarcoma, but this is not appropriate as a standalone treatment. Chemotherapy provides limited survival improvement in adults with high-grade soft-tissue sarcomas.
RECOMMENDED READINGS
13. [Bell RS, O'Sullivan B, Davis A, Langer F, Cummings B, Fornasier VL. Functional outcome in patients treated with surgery and irradiation for soft tissue tumours. J Surg Oncol. 1991 Dec;48(4):224-31. PubMed PMID: 1745046. ](http://www.ncbi.nlm.nih.gov/pubmed/1745046)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1745046)
14. [O'Sullivan B, Wylie J, Catton C, Gutierrez E, Swallow CJ, Wunder J, Gullane P, Neligan P, Bell R. The local management of soft tissue sarcoma. Semin Radiat Oncol. 1999 Oct;9(4):328-48. Review. PubMed PMID: 10516380. ](http://www.ncbi.nlm.nih.gov/pubmed/10516380)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10516380)
RECOMMENDED READINGS
13. [Bell RS, O'Sullivan B, Davis A, Langer F, Cummings B, Fornasier VL. Functional outcome in patients treated with surgery and irradiation for soft tissue tumours. J Surg Oncol. 1991 Dec;48(4):224-31. PubMed PMID: 1745046. ](http://www.ncbi.nlm.nih.gov/pubmed/1745046)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1745046)
14. [O'Sullivan B, Wylie J, Catton C, Gutierrez E, Swallow CJ, Wunder J, Gullane P, Neligan P, Bell R. The local management of soft tissue sarcoma. Semin Radiat Oncol. 1999 Oct;9(4):328-48. Review. PubMed PMID: 10516380. ](http://www.ncbi.nlm.nih.gov/pubmed/10516380)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10516380)
Question 48High Yield
Figure 58 is the radiograph of a laborer who has hindfoot and ankle pain. He is a type 1 diabetic, and has a BMI of 25 and a Hgb A1c of 6. What is the most appropriate management at this time?
Explanation
The radiograph shows Charcot changes in the subtalar joint. In the absence of gross deformity, the initial treatment is nonsurgical, consisting of total contact casting, with frequent cast changes and progression to weight bearing when swelling subsides and early consolidation is seen radiographically. A walking boot will not provide sufficient immobilization, whereas bed rest carries the risk of significant deconditioning in an otherwise active patient with well-controlled diabetes. Surgery as the initial treatment is not indicated in the absence of gross deformity or ulceration.
Question 49High Yield
What is the most likely diagnosis?
Explanation
- Fracture dislocation of the Chopart joint
Question 50High Yield
A tailorâs bunion is an abnormal prominence of the lateral aspect of the 5th metatarsal head. Similar to hallux valgus deformities, tailorâs bunions can be due to a widened intermetatarsal angle between the 4th and 5th metatarsal shafts. The normal 4-5 intermetatarsal angle is:
Explanation
4-5 intermetarsal angle in normal feet averages 6.2 degrees. Different authors believe an abnormally wide 4-5 intermetatarsal angle to be anything greater than 8°-9°.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon