Orthopedic With Answer Hi Review | Dr Hutaif General Or -...
14 Apr 2026
53 min read
118 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic With Answer Hi Review | Dr Hutaif ...
00:00
Start Quiz
Question 1High Yield
Haversian bone is composed of vascular channels surrounded circumferentially by lamellar bone. Which of the following terms is used to describe the unit of bone composed of a neurovascular channel surrounded by a cell-permeated layer of bone matrix:
Explanation
The osteon is a unique arrangement of bone cells and matrix surrounding a blood vessel. The osteon is an irregular branching, anastomosing cylinder composed of a centrally placed neurovascular canal surrounded by cell-permeated layers of bone matrix.
The bone remodeling unit refers to the cutting cone of leading osteoclasts and following osteoblasts.
Plexiform bone is a structural type of bone found in large animals where rapid bone growth occurs. There are alternating layers of lamellar and woven bone.
Volkman canals are the channels connecting different osteons or Haversian units.
Canaliculi are small channels through which the cell processes of the osteocytes connect to each other. Correct Answer: Osteon
The bone remodeling unit refers to the cutting cone of leading osteoclasts and following osteoblasts.
Plexiform bone is a structural type of bone found in large animals where rapid bone growth occurs. There are alternating layers of lamellar and woven bone.
Volkman canals are the channels connecting different osteons or Haversian units.
Canaliculi are small channels through which the cell processes of the osteocytes connect to each other. Correct Answer: Osteon
Question 2High Yield
During a posterior cruciate ligament (PCL)-retaining total knee arthroplasty, a critical principle to remember
is to
is to
Explanation
Maintenance of the joint line and accurately tensioning the PCL are critical in the proper execution of a PCL-retaining total knee arthroplasty. Appropriate tension helps ensure femoral rollback and avoid stiffness or instability. Raising the joint line to help ensure full extension should be avoided in cruciate- retaining knees, because doing so creates an unfavorable kinematic environment. The three important principles of surgical technique needed to maintain appropriate tensioning of the PCL include 1) choosing the proper femur size to reproduce the native femoral anterior/posterior dimension, 2) reproducing the joint line by resecting as much tibia from the healthy side as will be replaced by the smallest thickness of the tibial component and, 3) ensuring that full extension is achieved by soft-tissue releases and not by taking additional distal femur, as may be done in a posterior stabilized approach. Another important principle is to re-create the natural degree of the patient’s posterior tibial slope to avoid tightness in
flexion.
flexion.
Question 3High Yield
Figure 1 is the weight-bearing PA radiograph of a 67-year-old woman undergoing total knee arthroplasty (TKA). During surgery, it is observed that she remains tight laterally in extension only while trialing components. What is the most appropriate next step?
Explanation
Gap balance during TKA is best achieved with an understanding of which structures contribute to which gaps. Studies have shown that the popliteus tendon contributes to flexion gap tightness laterally and that the IT band contributes to extension gap tightness laterally.
49
Resecting additional femur would raise the joint line and would affect both the medial and lateral extension gaps equally. Release of the posterior capsule would also affect both gaps equally. Release of the lateral collateral ligament would likely require an increased level of constraint and, although it would affect only the lateral extension and flexion gaps, it is not the most appropriate next step.
49
Resecting additional femur would raise the joint line and would affect both the medial and lateral extension gaps equally. Release of the posterior capsule would also affect both gaps equally. Release of the lateral collateral ligament would likely require an increased level of constraint and, although it would affect only the lateral extension and flexion gaps, it is not the most appropriate next step.
Question 4High Yield
The anterior approach to the hip (iliofemoral or Smith-Peterson) puts which of the following anatomic structures at greatest risk?
Explanation
DISCUSSION: The anterior approach to the hip involves a dissection between the sartorius and the tensor fascia lata (TFL) superficially, followed by a deep dissection between the rectus femoris and gluteus medius. The lateral femoral cutaneous nerve generally enters the top of the thigh overlying the sartorius, and then usually crosses the interval between the sartorius muscle and the tensor fascia lata more distally. As the fascia between the sartorius and the TFL is incised, the nerve is at risk. The ascending branch of the lateral femoral circumflex artery is also at risk during this approach. The femoral nerve should not be in the plane of dissection as it lies medial to the sartorius.
REFERENCE: Hoppenfeld S, DeBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippinocott, 1984, pp 301-315.
REFERENCE: Hoppenfeld S, DeBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippinocott, 1984, pp 301-315.
Question 5High Yield
Axonotmesis involves injury to which of the following structure:
Explanation
Axonotmesis as described in Seddon classification implies injury to the axon and myelin sheath. It is neurotmesis that involves injury to all the three layers.
Question 6High Yield
A 9-year-old boy is examined due to a closed distal forearm fracture. The radius and ulna are both fractured and translated
100%. After manipulation twice with sedation, the translation cannot be reduced. There is 10-mm shortening of the radius and 5- mm shortening of the ulna. The distal radial angulation on the anteroposterior view is 5° less than normal. The next step in treatment should include:
100%. After manipulation twice with sedation, the translation cannot be reduced. There is 10-mm shortening of the radius and 5- mm shortening of the ulna. The distal radial angulation on the anteroposterior view is 5° less than normal. The next step in treatment should include:
Explanation
The translation and shortening are not problems and the amount of angulation will easily remodel with this fracture. There is nothing to be gained from operative reduction.
Question 7High Yield
In the pediatric population, CECS most commonly presents in females involved in running sports. In this cohort, recurrence occurs at a rate of 18%. Wound complications are the next most common at a rate of 11.2%.
A 15-year-old male ice hockey player is hit in the chest by a puck and immediately falls to the ground unconscious. What has been shown to predict survival in the treatment of this condition?
A 15-year-old male ice hockey player is hit in the chest by a puck and immediately falls to the ground unconscious. What has been shown to predict survival in the treatment of this condition?
Explanation
The hockey player is suffering from commotio cordis, in which a cardiac arrhythmia occurs after a sudden blunt impact to the chest. Treatment of commotio cordis is defibrillation. As the time to defibrillation increases, the likelihood of survival decreases. In animal models, chest protectors have not shown efficacy
against ventricular fibrillation. The velocity of the projectile (most commonly baseball, hockey puck or lacrosse ball) has also not been shown to alter survival.
against ventricular fibrillation. The velocity of the projectile (most commonly baseball, hockey puck or lacrosse ball) has also not been shown to alter survival.
Question 8High Yield
A 25-year-old football player sustained an injury to his ankle 2 months ago. He has ankle pain upon dorsiflexion and external rotation. A radiograph demonstrates widening of the tibiofibular syndesmosis and a 3-mm space between the medial talus and the medial malleolus. The recommended treatment is:
Explanation
It is imperative that any diastasis of the tibiofibular joint is repaired to prevent the late sequelae (e.g., arthritis), particularly in the athlete. Arthroscopy is not sufficient, other than evaluation for additional joint pathology, and syndesmosis arthrodesis would
rarely be indicated for this condition. There is no evidence of a high fibula fracture, although this must be a concern and should always be considered.
rarely be indicated for this condition. There is no evidence of a high fibula fracture, although this must be a concern and should always be considered.
Question 9High Yield
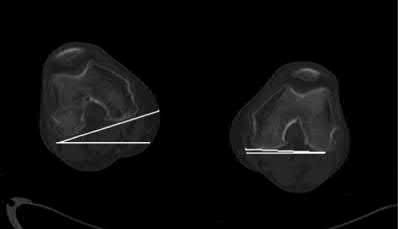
A 23-year-old man undergoes intramedullary nailing for a comminuted right femur fracture. Three weeks after surgery, CT scans are performed to assess for rotational malalignment. In Figure A, the angular rotation of the right femoral neck is internal rotation of 13° while the angular rotation of the left femoral neck is external rotation of 13°. In Figure B, the angular rotation of the right and left femoral condyles is external rotation of 17° and 3°, respectively. At revision surgery, in order to correct the rotational malalignment, the right distal femur must be rotated which of the following?

Explanation
This patient has an external rotation deformity of 40° of the distal fragment of the right femur. Correction would entail rotating the distal fragment internally by 40°.
The right femoral neck (RFN) is internally rotated (IR) by 13° to the horizontal (IR13). The left femoral neck (LFN) is externally rotated (ER) by 13° to the horizontal (ER13). The right distal fragment (RDF) is ER17. The left distal fragment (LDF) is ER3. Bringing both femoral necks to ER0/IR0 gives the absolute amount of rotation of the distal fragment to the horizontal. To do this, the RFN has to EXTERNALLY rotate 13° and the LFN has to INTERNALLY rotate 13°. Thus, RDF has a total of ER(13+17)=ER30, and LDF has IR(13-3)=IR10 to the horizontal. To correct the RDF from ER30 to IR10, internal rotation of 40° must occur.
Malrotation is the most common cause of limb deformity after nailing. To avoid this, patients should be examined for rotation and limb length after insertion of static interlocks, before leaving the operating room. Correction is easier to perform prior to fracture union. Drill-hole cutout is possible if correction<20° if the previous distal locking site is to be used because of the proximity of the new interlock to the previous interlock. To avoid this, (1) use alternative locking holes or the dynamic locking slot, or (2) advance or retract the nail to avoid previous locking sites.
Lindsey et al. reviewed rotational malalignment after femoral nailing. The incidence of rotational malalignment was 27.6%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is 11-13°. Some patients have up to 15° difference in version between limbs.
Jaarsma et al. reviewed rotational malalignment after nailing of 76 femoral fractures. The incidence of rotational malalignment >=15° was 28%. Patients with an ER malalignment (n = 12) had more functional problems than patients with a IR malalignment (n = 9).
Incorrect Answers:
Answer 1: This answer would be correct if LFN was IR13, and LDF was IR3, giving absolute LDF rotation of ER10. Then to correct ER30 (right) to ER10 (left), internal rotation of 20° would be needed.
Answers 2, 4: The RDF is more externally rotated. Correction must involve internal rotation.
Answer 3: This answer would be correct if LFN was IR13, giving absolute LDF rotation of ER16. Then to correct ER30 (right) to ER16 (left), internal rotation of 14° must occur.
The right femoral neck (RFN) is internally rotated (IR) by 13° to the horizontal (IR13). The left femoral neck (LFN) is externally rotated (ER) by 13° to the horizontal (ER13). The right distal fragment (RDF) is ER17. The left distal fragment (LDF) is ER3. Bringing both femoral necks to ER0/IR0 gives the absolute amount of rotation of the distal fragment to the horizontal. To do this, the RFN has to EXTERNALLY rotate 13° and the LFN has to INTERNALLY rotate 13°. Thus, RDF has a total of ER(13+17)=ER30, and LDF has IR(13-3)=IR10 to the horizontal. To correct the RDF from ER30 to IR10, internal rotation of 40° must occur.
Malrotation is the most common cause of limb deformity after nailing. To avoid this, patients should be examined for rotation and limb length after insertion of static interlocks, before leaving the operating room. Correction is easier to perform prior to fracture union. Drill-hole cutout is possible if correction<20° if the previous distal locking site is to be used because of the proximity of the new interlock to the previous interlock. To avoid this, (1) use alternative locking holes or the dynamic locking slot, or (2) advance or retract the nail to avoid previous locking sites.
Lindsey et al. reviewed rotational malalignment after femoral nailing. The incidence of rotational malalignment was 27.6%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is 11-13°. Some patients have up to 15° difference in version between limbs.
Jaarsma et al. reviewed rotational malalignment after nailing of 76 femoral fractures. The incidence of rotational malalignment >=15° was 28%. Patients with an ER malalignment (n = 12) had more functional problems than patients with a IR malalignment (n = 9).
Incorrect Answers:
Answer 1: This answer would be correct if LFN was IR13, and LDF was IR3, giving absolute LDF rotation of ER10. Then to correct ER30 (right) to ER10 (left), internal rotation of 20° would be needed.
Answers 2, 4: The RDF is more externally rotated. Correction must involve internal rotation.
Answer 3: This answer would be correct if LFN was IR13, giving absolute LDF rotation of ER16. Then to correct ER30 (right) to ER16 (left), internal rotation of 14° must occur.
Question 10High Yield
Figure 1 Figure 2
A 66-year-old woman has experienced the gradual onset of a flatfoot deformity over the past 10 years. She notes that the condition is bilateral, although worse on one side. Presented are clinical and radiographic images of her condition. This is associated with pain upon ambulation and difficulty with shoe wear. The most likely cause of this flatfoot deformity is:
A 66-year-old woman has experienced the gradual onset of a flatfoot deformity over the past 10 years. She notes that the condition is bilateral, although worse on one side. Presented are clinical and radiographic images of her condition. This is associated with pain upon ambulation and difficulty with shoe wear. The most likely cause of this flatfoot deformity is:
Explanation
Although posterior tibial tendon insufficiency is a more common cause of adult acquired flatfoot, in this patient the associated clinical and radiographic deformity makes the diagnosis of tarsometatarsal arthritis more likely.
Question 11High Yield
Use of titanium elastic nailing for treatment of pediatric femur fractures is associated with a higher complication rate among


Explanation
Studies of titanium elastic nailing for femur fractures demonstrated a higher rate of complications, including angular deformity and construct failure, among patients weighing more than 50 kg (100 pounds). Other methods of fixation are recommended for these patients. Flexible nails are not commonly needed, but they also are not associated with a higher complication rate in children younger than age 6.5. Titanium elastic nailing works well in closed or minimally open transverse midshaft fractures, even in the setting of early or immediate weight bearing.
Video 8a
Video 8b
Video 8a
Video 8b
Question 12High Yield
Figures below show the clinical photograph and radiograph obtained from a 62-year-old man who has
deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?
deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?

Explanation
Figure 1 reveals an external rotation deformity of the right lower extremity. This deformity can have numerous causes, including extra-articular deformity. Figure 2 reveals a loose, subsided femoral component. Femoral stems typically subside into retroversion due to proximal femoral biomechanics, which cause a compensatory external rotation deformity. The combined findings from both images suggest an external rotation deformity most likely related to subsidence into retroversion.
Question 13High Yield
An 18-year-old collegiate football player injures his right shoulder during a tackle. He reports pain and numbness in the shoulder and numbness radiating to his fingers. His symptoms improve within 15 minutes and he has no residual symptoms. This condition is best known as
Explanation
**
**
DISCUSSION: The condition described in this case is known as a stinger or burner. It is caused by stretching the upper trunk of the brachial plexus in the C5 and C6 nerve roots. The symptoms are temporary and last 15 to 20 minutes. There are no residual deficits, unless the patient has had multiple repetitive injuries. Once motor and sensory examination findings and reflexes have normalized, the athlete can return to play. Acute spinal cord injury may cause temporary complete paralysis in the upper and lower extremities with resolution of symptoms within 24 hours. Central cord syndrome affects the upper more than lower extermities and affects mostly elderly patients. Nerve root avulsions lead to permanent deficits and have a poor prognosis for return of function. Guillain-BarDe syndrome is an autoimmune disease that presents as an ascending paralysis with weakness in the legs that spreads to the upper limbs and the face along with complete loss of deep tendon reflexes.
REFERENCES: Safran MR: Nerve injury about the shoulder in athletes. Part 2: Long thoracic nerve, spinal accessory nerve, burners/stingers, thoracic outlet syndrome. Am J Sports Med 2004;32:1063-1076. Aval SM, Durand P Jr, Shankwiler JA: Neurovascular injuries to the athlete’s shoulder: Part I. J Am Acad Orthop Surg 2007;15:249-256.
**
DISCUSSION: The condition described in this case is known as a stinger or burner. It is caused by stretching the upper trunk of the brachial plexus in the C5 and C6 nerve roots. The symptoms are temporary and last 15 to 20 minutes. There are no residual deficits, unless the patient has had multiple repetitive injuries. Once motor and sensory examination findings and reflexes have normalized, the athlete can return to play. Acute spinal cord injury may cause temporary complete paralysis in the upper and lower extremities with resolution of symptoms within 24 hours. Central cord syndrome affects the upper more than lower extermities and affects mostly elderly patients. Nerve root avulsions lead to permanent deficits and have a poor prognosis for return of function. Guillain-BarDe syndrome is an autoimmune disease that presents as an ascending paralysis with weakness in the legs that spreads to the upper limbs and the face along with complete loss of deep tendon reflexes.
REFERENCES: Safran MR: Nerve injury about the shoulder in athletes. Part 2: Long thoracic nerve, spinal accessory nerve, burners/stingers, thoracic outlet syndrome. Am J Sports Med 2004;32:1063-1076. Aval SM, Durand P Jr, Shankwiler JA: Neurovascular injuries to the athlete’s shoulder: Part I. J Am Acad Orthop Surg 2007;15:249-256.
Question 14High Yield
A 72-year-old man undergoes an uncomplicated cementless total hip arthroplasty for advanced osteoarthritis. At his 6-week postoperative follow-up, he has minimal pain and is progressing well with his mobility. Radiographs show early formation of Brooker grade III heterotopic bone around his hip. What is the best treatment of the heterotopic bone at this time?

Explanation
DISCUSSION: The development of heterotopic bone occurs early after hip arthroplasty. The process begins within days after surgery; therefore, prophylactic treatment must be in the early postoperative period (preoperative radiation given within 24 hours of surgery, or postoperative radiation given within 72 hours of surgery, or nonsteroidal anti- inflammatory drugs (NSAIDs) given postoperatively for 7 to 21 days - longer duration has not been shown to be of any additional benefit). At 6 weeks, prophylactic treatment with NSAIDs or radiation is no longer effective. Surgery at 10 weeks would be premature because the patient is currently asymptomatic with regards to the heterotopic bone, and surgery prior to full maturation of the bone may increase the risk for more abundant recurrence of bone.
REFERENCES: Balboni TA, Gobezie R, Mamon HJ: Heterotopic ossification: Pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys 2006;65:1289-1299. Fransen M, Neal B: Non-steroidal anti-inflammatory drugs for preventing heterotopic bone formation after hip arthroplasty. Cochrane Database Syst Rev 2004;3:CD001160.
Neal BC, Rodgers A, Clark T, et al: A systematic survey of 13 randomized trials of non-steroidal antiinflammatory
drugs for the prevention of heterotopic bone formation after major hip surgery. Acta Orthop Scand 2000;71:122-128.
Figure 64
DISCUSSION: The development of heterotopic bone occurs early after hip arthroplasty. The process begins within days after surgery; therefore, prophylactic treatment must be in the early postoperative period (preoperative radiation given within 24 hours of surgery, or postoperative radiation given within 72 hours of surgery, or nonsteroidal anti- inflammatory drugs (NSAIDs) given postoperatively for 7 to 21 days - longer duration has not been shown to be of any additional benefit). At 6 weeks, prophylactic treatment with NSAIDs or radiation is no longer effective. Surgery at 10 weeks would be premature because the patient is currently asymptomatic with regards to the heterotopic bone, and surgery prior to full maturation of the bone may increase the risk for more abundant recurrence of bone.
REFERENCES: Balboni TA, Gobezie R, Mamon HJ: Heterotopic ossification: Pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys 2006;65:1289-1299. Fransen M, Neal B: Non-steroidal anti-inflammatory drugs for preventing heterotopic bone formation after hip arthroplasty. Cochrane Database Syst Rev 2004;3:CD001160.
Neal BC, Rodgers A, Clark T, et al: A systematic survey of 13 randomized trials of non-steroidal antiinflammatory
drugs for the prevention of heterotopic bone formation after major hip surgery. Acta Orthop Scand 2000;71:122-128.
Figure 64
Question 15High Yield
A patient with spondyloepiphyseal dysplasia congenita reaches the age of 5 without being able to walk with a walker. She has five beats of clonus in both ankles. Her reflexes are brisk and her toes are upgoing. The most likely problem that accounts for these findings is:
Explanation
Atlantoaxial instability, sometimes combined with stenosis of the atlas, is a frequent cause of myelopathy in spondyloepiphyseal dysplasia congenita.
Scoliosis does not account for developmental delay or myelopathy.
Foramen magnum stenosis is rare in spondyloepiphyseal dysplasia congenita.
Lumbar stenosis is rare with spondyloepiphyseal dysplasia congenita and would not account for myelopathy. Thoracolumbar kyphosis severe enough to cause myelopathy is rare in spondyloepiphyseal dysplasia congenita condition.
Scoliosis does not account for developmental delay or myelopathy.
Foramen magnum stenosis is rare in spondyloepiphyseal dysplasia congenita.
Lumbar stenosis is rare with spondyloepiphyseal dysplasia congenita and would not account for myelopathy. Thoracolumbar kyphosis severe enough to cause myelopathy is rare in spondyloepiphyseal dysplasia congenita condition.
Question 16High Yield
What is the primary concern regarding resolution of this fracture?
Explanation
- Blood supply to this area
Question 17High Yield
Which of the following activities can improve posterior capsular contractures?
Explanation
Posterior capsule stretching is performed in the cross-chest and behind the back positions. Stretching in internal rotation in the abducted shoulder will further stretch the posterior capsule. Wide grip stretch, and anterior capsule and strengthening exercises will not necessarily stretch the capsule.
REFERENCES: Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
Kibler WB, McMullen J, Uhl J: Shoulder rehabilitation strategies, guidelines, and practice. Op Tech Sports Med 2000;8:258-267.
REFERENCES: Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
Kibler WB, McMullen J, Uhl J: Shoulder rehabilitation strategies, guidelines, and practice. Op Tech Sports Med 2000;8:258-267.
Question 18High Yield
If aspiration findings are negative or equivocal, the diagnosis can be established with
Explanation
- arthroscopy._
Question 19High Yield
Which type of thoracolumbar injury typically involves all three columns, is most mechanically unstable, and is most associated with complete spinal cord injury?
Explanation
■
Translation-rotation injuries typically yield fracture dislocations. This injury pattern involves the disruption of skeletal and ligamentous elements of the spine to cause a maximum loss of stability, subsequent deformity in three planes (coronal, axial, and sagittal), and catastrophic neurologic injury.
Compression injuries occur when a force is applied in flexion and injures the anterior column. Compression injuries are usually stable and rarely have neurologic sequelae. Burst fractures occur through axially applied forces, which in turn cause injury to the anterior and middle columns of the vertebrae at minimum. Neurologic injury can occur through direct compression of the neural elements by bone fragments or hematoma or by absorption of the transferred energy. Flexion distraction injuries typically occur as forces are transmitted from anterior to posterior, causing injury to the middle and posterior columns.
Translation-rotation injuries typically yield fracture dislocations. This injury pattern involves the disruption of skeletal and ligamentous elements of the spine to cause a maximum loss of stability, subsequent deformity in three planes (coronal, axial, and sagittal), and catastrophic neurologic injury.
Compression injuries occur when a force is applied in flexion and injures the anterior column. Compression injuries are usually stable and rarely have neurologic sequelae. Burst fractures occur through axially applied forces, which in turn cause injury to the anterior and middle columns of the vertebrae at minimum. Neurologic injury can occur through direct compression of the neural elements by bone fragments or hematoma or by absorption of the transferred energy. Flexion distraction injuries typically occur as forces are transmitted from anterior to posterior, causing injury to the middle and posterior columns.
Question 20High Yield
Examination of the shoulder seen in Figure 52 shows atrophy and tenderness of the infraspinous fossa and profound weakness in external rotation. The supraspinous fossa shows normal muscle bulk. What is the most likely cause of this condition?
Explanation
Compression of the suprascapular nerve by a ganglion cyst is a well-documented cause of pain and weakness in the shoulder. Isolated involvement of the infraspinatus indicates that the area of entrapment is at the spinoglenoid notch and not the suprascapular notch. The majority of ganglion cysts found in the shoulder are related to tears of the labrum. When such a compressive lesion is found, decompression can be accomplished through either an open or arthroscopic approach. Several authors have shown the value of arthroscopy in the treatment of this condition. It has been shown that it is technically possible to decompress a paralabral ganglion cyst using arthroscopy; this method is usually followed by repair of the torn labrum. Alternatively, arthroscopic repair of the labrum can be performed and the cyst may be aspirated at the time of surgery. Open cyst excision through a posterior approach is also an acceptable method of treatment.
REFERENCES: Schickendantz MS, Ho CP: Suprascapular nerve compression by a ganglion cyst: Diagnosis by magnetic resonance imaging. J Shoulder Elbow Surg 1993;2:110-114.
Thompson RC, Schneider W, Kennedy T: Entrapment neuropathy of the inferior branch of the suprascapular nerve by ganglia. Clin Orthop 1982;166:185-187.
Iannotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
**1****.**
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
REFERENCES: Schickendantz MS, Ho CP: Suprascapular nerve compression by a ganglion cyst: Diagnosis by magnetic resonance imaging. J Shoulder Elbow Surg 1993;2:110-114.
Thompson RC, Schneider W, Kennedy T: Entrapment neuropathy of the inferior branch of the suprascapular nerve by ganglia. Clin Orthop 1982;166:185-187.
Iannotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
**1****.**
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
Question 21High Yield
Figures 1 and 2 are the clinical photographs of a 36-year-old woman who cannot fully extend the metacarpophalangeal (MP) joints of her long and ring fingers 9 months after the removal of a plate from the proximal radius via a dorsal approach. What is the most likely cause of this problem?
---
---







Explanation
Plating of the proximal radius from a dorsal or Thompson approach (between the extensor carpi radialis brevis and extensor digitorum communis) allows complete visualization of the PIN through the supinator. Going through the same incision from proximal to distal produces a scar-filled proximal approach, and it is not uncommon to drift ulnarly and injure an individual nerve to the extensor digitorum communis muscle, resulting in the deformity seen in Figures 1 and 2.Postsurgical tendon adhesions rarely involve only 2 tendons. Complete tendon lacerations are rare at this level in the proximal forearm, as is a complete laceration of the PIN. Neuropraxias are common but usually resolve after 3 months. The gossamer-thin branch of the PIN to the EDC can be easily damaged in scar tissue, resulting in an inability to fully extend the MP joints of the long and ring fingers. The proprius tendons allow the patient to fully extend the index and little finger MP joints. Connecting the EDC of the long finger to the _extensor indicis proprius_ and the EDC of the ring finger to the _extensor digiti quinti_ proprius can correct the deformity. To avoid the problem, the surgeon should start the incision distally in normal anatomy, and the interval between the _mobile wad and the digital extensors will be more easily found._
Question 22High Yield
A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
Explanation
End-stage posttraumatic or inflammatory elbow arthritis in active, high-demand patients remains difficult to treat. Traditional total elbow arthroplasty is discouraged in this demographic secondary to concerns about implant longevity. Soft-tissue interposition arthroplasty does not necessitate the same activity and weight restrictions for patients after surgery and remains a reasonable salvage procedure. Larson and Morrey published their findings on
38 patients with a mean age of 39 years following soft-tissue interposition arthroplasty for posttraumatic and inflammatory end-stage elbow arthritis. These investigators reported a significant improvement in Mayo Elbow Performance Score in addition to improvement in the flexion-extension arc from 51° to 97° after surgery. They reported worse results and elevated incidence of complications for patients with presurgical elbow instability. Retained hardware from prior surgery was not deemed a contraindication.
32
38 patients with a mean age of 39 years following soft-tissue interposition arthroplasty for posttraumatic and inflammatory end-stage elbow arthritis. These investigators reported a significant improvement in Mayo Elbow Performance Score in addition to improvement in the flexion-extension arc from 51° to 97° after surgery. They reported worse results and elevated incidence of complications for patients with presurgical elbow instability. Retained hardware from prior surgery was not deemed a contraindication.
32
Question 23High Yield
A 72-year-old female presents to the office 5 weeks after distal radius fracture surgery with the findings seen in Figure A. She performed daily cleansing with soap and water and dry dressings.
Which of the following has been shown to decrease the risk of developing this complication?
Which of the following has been shown to decrease the risk of developing this complication?

Explanation
There is no difference between daily showers with soap, water and dry dressings, and solutions comprising (1) saline and chlorhexidine, or (2) saline and hydrogen peroxide.
The risks of external fixation include cellulitis, pin-track drainage, osteomyelitis and pin loosening. The rate of complications is about 20%. Chlorhexidine gluconate has broad spectrum activity against gram-positive and negative bacteria by disrupting cell membranes. It is not affected by blood and has low skin irritancy. Studies show that simple pin-site care (showers, dry dressings) maintains a low infection rate.
Egol et al. performed a randomized trial examining external fixation pin tracts about the wrist. They compared (1) weekly dry dressings, (2) daily pin care with half normal saline (NS) and hydrogen peroxide (H2O2) and (3) chlorhexidine discs with weekly changes. They found pin-site complications in 19%, with no difference between the 3 groups. They do not recommend additional wound care beyond sterile dressings.
Stinner et al. performed a survey on the use of half-pins by the limb lengthening and reconstruction society. They found that most respondents preferred hydroxyapatite coating (81%) because of improved fixation and decreased loosening (less radiographic pin-tract rarefaction and greater extraction torque, which may lead to lower infection rates). Most encouraged
shower (60%) and washing solution (67%)(soap and water, peroxide or saline) for pin site care.
Figure A shows an external fixator around the wrist with cellulitis around the proximal half-pins.
Incorrect Answers
Answers 1-4: Hydrogen peroxide and chlorhexidine based solutions have not been conclusively shown to decrease the rate of pin site complications.
The risks of external fixation include cellulitis, pin-track drainage, osteomyelitis and pin loosening. The rate of complications is about 20%. Chlorhexidine gluconate has broad spectrum activity against gram-positive and negative bacteria by disrupting cell membranes. It is not affected by blood and has low skin irritancy. Studies show that simple pin-site care (showers, dry dressings) maintains a low infection rate.
Egol et al. performed a randomized trial examining external fixation pin tracts about the wrist. They compared (1) weekly dry dressings, (2) daily pin care with half normal saline (NS) and hydrogen peroxide (H2O2) and (3) chlorhexidine discs with weekly changes. They found pin-site complications in 19%, with no difference between the 3 groups. They do not recommend additional wound care beyond sterile dressings.
Stinner et al. performed a survey on the use of half-pins by the limb lengthening and reconstruction society. They found that most respondents preferred hydroxyapatite coating (81%) because of improved fixation and decreased loosening (less radiographic pin-tract rarefaction and greater extraction torque, which may lead to lower infection rates). Most encouraged
shower (60%) and washing solution (67%)(soap and water, peroxide or saline) for pin site care.
Figure A shows an external fixator around the wrist with cellulitis around the proximal half-pins.
Incorrect Answers
Answers 1-4: Hydrogen peroxide and chlorhexidine based solutions have not been conclusively shown to decrease the rate of pin site complications.
Question 24High Yield
Stieda fracture
Explanation
- Figure 13e
Question 25High Yield
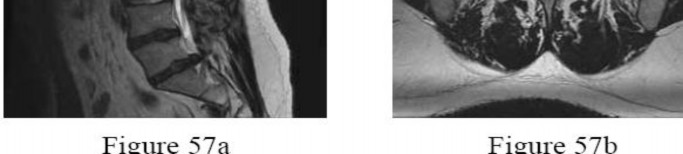
A 28-year-old man has had a 2-week history of right posterior leg pain, with numbness and tingling in the same distribution. He denies any problems with bowel or bladder function. Examination shows intact motor strength in his bilateral lower extremities, with numbness to light touch in the lateral border of his right foot. Over the past 2 weeks, his leg pain has improved significantly. MRI scans are shown in Figures 57a and 57b. What is the most appropriate course of management?
---
---

Explanation
The patient has an L5-S1 disk herniation, which has a favorable prognosis without surgical intervention. Most acute lumbar disk herniations resolve with nonsurgical management. The most appropriate course of initial treatment should be analgesics and activity modification, followed by rehabilitation as the symptoms allow. Although the MRI scan indicates a large disk herniation, he has no symptoms or signs that
would warrant urgent surgical decompression. Planned elective discectomy should be considered only if nonsurgical management fails to provide relief. Epidural injections could be considered if the initial course of treatment fails to give the patient significant relief. Posterior laminectomy and fusion is not indicated without the presence of instability.
would warrant urgent surgical decompression. Planned elective discectomy should be considered only if nonsurgical management fails to provide relief. Epidural injections could be considered if the initial course of treatment fails to give the patient significant relief. Posterior laminectomy and fusion is not indicated without the presence of instability.
Question 26High Yield
Skeletal muscle may remain viable (electrically responsive) following a period of total ischemia. Which of the following is the correct time interval for the tolerance to total muscle ischemia (complete recovery can be expected):
Explanation
Skeletal muscle tolerates periods of complete muscle ischemia for 3 to 4 hours without irreversible damage. Variable recovery occurs with ischemia for 6 to 8 hours. When the period of ischemia is more than 8 hours, there is irreversible muscle damage. After 8 hours, the muscle cells degenerate and, grossly, the muscle contracts as the muscle cells are replaced with scar tissue and contracture may result.
Remember to let a tourniquet down after 2 hours of ischemia. One does not want to enter the tolerance period of 3 to 4 hours. Correct Answer: 3 to 4 hours
Remember to let a tourniquet down after 2 hours of ischemia. One does not want to enter the tolerance period of 3 to 4 hours. Correct Answer: 3 to 4 hours
Question 27High Yield
Figure 37 shows the radiograph of a 23-year-old football player who sustained a blow to the anterior aspect of his shoulder. Examination reveals pain and limited rotation. He is unable to flex the arm above the shoulder. Management should include which of the following studies?
Explanation
The patient has a posterior dislocation. The radiograph reveals marked internal rotation, but fails to show whether the humeral head is posteriorly displaced. Therefore, an axillary radiograph should be obtained to help confirm the diagnosis. Transverse view CT or MRI scans also may be useful. The other studies will not help confirm the diagnosis. In addition to a direct posterior blow, a shoulder dislocation may be caused by a seizure disorder or electrocution.
REFERENCES: Bloom MH, Obata WG: Diagnosis of posterior dislocation of the shoulder with the use of Velpeau axillary and angle-up roentgenographic views. J Bone Joint Surg Am 1967;49:943-949.
Rockwood CA: Subluxations and dislocations about the shoulder, in Rockwood CA, Green DP (eds): Fractures in Adults, ed 2. Philadelphia, PA, JB Lippincott, 1984, vol 1, pp 806-856.
REFERENCES: Bloom MH, Obata WG: Diagnosis of posterior dislocation of the shoulder with the use of Velpeau axillary and angle-up roentgenographic views. J Bone Joint Surg Am 1967;49:943-949.
Rockwood CA: Subluxations and dislocations about the shoulder, in Rockwood CA, Green DP (eds): Fractures in Adults, ed 2. Philadelphia, PA, JB Lippincott, 1984, vol 1, pp 806-856.
Question 28High Yield
A 55-year-old man presents with pain in his great toe that began 2 days ago. On physical exam, his first metatarsophalangeal (MTP) joint is red, warm, and tender to palpation (Figure A). His skin is intact with no evidence of ulceration. He reports pain with range of motion. He denies recent fevers and his admission temperature is 37.9°C. Labs are drawn and significant for a WBC of 15K (reference range [rr], 4500-11000 µL), ESR of 90 (rr, 0-20 mm/h), and CRP of 6.5 (rr, 0.08-
3.1 mg/L). A radiograph of his foot is shown in Figure B. Which of the following is the next best step?
3.1 mg/L). A radiograph of his foot is shown in Figure B. Which of the following is the next best step?


Explanation
This patient presents with a painful 1st MTP joint and elevated inflammatory markers concerning for septic arthritis vs. an inflammatory process such as gout. A joint aspiration to determine the etiology of his toe pain would be the next best step. Aspiration results for this patient confirmed septic arthritis of the 1st MTP joint.
Septic arthritis of the 1st MTP joint can arise from local inoculation or hematogenous spread. Patients typically present with an acutely swollen, warm, erythematous joint; inability to bear weight; and severe pain with micromotion. Radiographs may be normal or may reveal a subtle joint effusion. Inflammatory markers (ESR and CRP) are usually elevated and can, therefore, be used to rule out a diagnosis of septic arthritis. Joint aspiration, however, remains as the gold standard for diagnosis and is useful for differentiating septic arthritis from gout.
Anakwenze et al. reviewed the diagnosis and management of foot and ankle infections. They report that 3-7% of septic arthritis cases occur in the foot and ankle, with the tibiotalar joint and 1st MTP joint being the most commonly affected and with staph aureus being the most common causative organism.
They state that in cases with sufficient clinical suspicion for septic arthritis, joint aspiration is the diagnostic tool of choice.
Carpenter et al. performed a systematic review to describe the diagnostic characteristics of history, physical examination, and bedside laboratory tests for nongonococcal septic arthritis, and to quantify test and treatment thresholds. They found that, with the exception of joint surgery or skin infection overlying a prosthetic joint, history, physical examination, and serum tests do not significantly alter post-test probability. Serum inflammatory markers such as white blood cell (WBC) counts, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) were also found to be not useful acutely.
However, extreme values of synovial WBC (> 50,000) can increase, but not decrease, the probability of septic arthritis.
Figure A is a clinical picture of a red, swollen 1st MTP joint. Figure B is an AP radiograph of a normal foot with no evidence of fracture, arthritis, or erosions.
Incorrect Answers:
Answer 2: Joint irrigation and debridement would be warranted only after a diagnosis of septic arthritis has been confirmed by joint aspiration.
Answer 3: Outpatient oral antibiotics would be appropriate to treat cellulitis, but only after a diagnosis of gout and septic arthritis has been eliminated.
Answer 4: Oral indomethacin is the treatment of choice for gout and would be appropriate after confirmation of the diagnosis via joint aspiration.
Answer 5: MRI is more effective than radiography for diagnosing sepsis with or with osteomyelitis. However, joint aspiration is the best next step for this patient.
Septic arthritis of the 1st MTP joint can arise from local inoculation or hematogenous spread. Patients typically present with an acutely swollen, warm, erythematous joint; inability to bear weight; and severe pain with micromotion. Radiographs may be normal or may reveal a subtle joint effusion. Inflammatory markers (ESR and CRP) are usually elevated and can, therefore, be used to rule out a diagnosis of septic arthritis. Joint aspiration, however, remains as the gold standard for diagnosis and is useful for differentiating septic arthritis from gout.
Anakwenze et al. reviewed the diagnosis and management of foot and ankle infections. They report that 3-7% of septic arthritis cases occur in the foot and ankle, with the tibiotalar joint and 1st MTP joint being the most commonly affected and with staph aureus being the most common causative organism.
They state that in cases with sufficient clinical suspicion for septic arthritis, joint aspiration is the diagnostic tool of choice.
Carpenter et al. performed a systematic review to describe the diagnostic characteristics of history, physical examination, and bedside laboratory tests for nongonococcal septic arthritis, and to quantify test and treatment thresholds. They found that, with the exception of joint surgery or skin infection overlying a prosthetic joint, history, physical examination, and serum tests do not significantly alter post-test probability. Serum inflammatory markers such as white blood cell (WBC) counts, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) were also found to be not useful acutely.
However, extreme values of synovial WBC (> 50,000) can increase, but not decrease, the probability of septic arthritis.
Figure A is a clinical picture of a red, swollen 1st MTP joint. Figure B is an AP radiograph of a normal foot with no evidence of fracture, arthritis, or erosions.
Incorrect Answers:
Answer 2: Joint irrigation and debridement would be warranted only after a diagnosis of septic arthritis has been confirmed by joint aspiration.
Answer 3: Outpatient oral antibiotics would be appropriate to treat cellulitis, but only after a diagnosis of gout and septic arthritis has been eliminated.
Answer 4: Oral indomethacin is the treatment of choice for gout and would be appropriate after confirmation of the diagnosis via joint aspiration.
Answer 5: MRI is more effective than radiography for diagnosing sepsis with or with osteomyelitis. However, joint aspiration is the best next step for this patient.
Question 29High Yield
A 21-year-old hockey player who has recurrent shoulder subluxations undergoes an anterior capsulorrhaphy under general anesthesia, and an interscalene block is used to relieve postoperative pain. At the 1-week follow-up examination, he reports loss of sensation over the lateral region of the shoulder and is unable to actively contract the deltoid muscle. The remainder of the examination is normal. What is the best course of action at this time?
Explanation
The patient has an axillary nerve injury, which is relatively uncommon after surgery for instability. This type of injury generally is the result of a stretch injury rather than transection or a hematoma. Therefore, observation is indicated in the early postoperative period. After approximately 6 weeks, electromyography can be used to confirm and document the point of injury. Interscalene blocks can cause prolonged nerve injury but usually are not limited to the axillary nerve.
REFERENCE: Ho E, Cofield RH, Balm MR, et al: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
REFERENCE: Ho E, Cofield RH, Balm MR, et al: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
Question 30High Yield
Slide 1
A 43-year-old construction worker sustained a work-related injury to his foot 7 months ago. He was initially treated with cast immobilization and limited weight bearing. He has lateral foot pain and inability to walk comfortably. He has limited walking endurance. Upon examination, pain is present laterally along the course of the peroneal tendons, and no motion of the subtalar joint is present. The recommendation is:
A 43-year-old construction worker sustained a work-related injury to his foot 7 months ago. He was initially treated with cast immobilization and limited weight bearing. He has lateral foot pain and inability to walk comfortably. He has limited walking endurance. Upon examination, pain is present laterally along the course of the peroneal tendons, and no motion of the subtalar joint is present. The recommendation is:
Explanation
A worker who sustains a calcaneus fracture must be returned to the work force as soon as possible. Although these alternatives for treatment may be considered in the patient with limited activity and low demands, the longer the time from injury to salvage surgery with arthrodesis, the less likely it is that the injured worker will ever return to gainful employment. Therefore, subtalar arthrodesis should be performed.
Question 31High Yield
1223) A 46-year-old male sustains a patella fracture and is treated with cannulated screws and a tension band construct. Which of the following is correct regarding this treatment?

Explanation
Fixation of patella fractures with tension band constructs leads to a need to remove implants in over 50% of cases in multiple studies.
Tension band constructs result in absolute stability when performed correctly. This technique works by converting tension from muscle pull into compressive force on the articular side of the fracture. Tension band constructs require a fracture pattern or bone that is able to withstand compression, an intact cortical buttress opposite to the tension band, and fixation that withstands tensile forces.
LeBrun et al. and associates evaluated functional outcomes of surgically isolated patella fractures. They reported that 52% of patients underwent surgery for hardware removal, and 38% of patients who retained their hardware reported pain at some time. They also found that nearly 20% had extensor lag, and almost 38% had restricted flexion. Extension power on testing showed significant mean deficits when compared to the contralateral side.
Bayar et al. evaluated 20 patients with patella fractures and found that articular incongruity of >1mm was the largest risk factor for quadriceps weakness at a mean of 30 months postoperatively. No significant differences were seen with sex, fracture pattern, or time from injury to surgery.
Illustration A shows patella fixation with plate/screw construct. Incorrect Answers:
Answer 1: Knee flexion arc is generally limited more than the non-injured side.
Answer 2: Extensor lag can be permanent with this treatment method. Answer 4: Quadriceps weakness is common after tension band fixation of patella fractures.
Answer 5: Patients generally have poorer outcomes after patella tension band fixation, regardless of implant maintenance or removal.
Tension band constructs result in absolute stability when performed correctly. This technique works by converting tension from muscle pull into compressive force on the articular side of the fracture. Tension band constructs require a fracture pattern or bone that is able to withstand compression, an intact cortical buttress opposite to the tension band, and fixation that withstands tensile forces.
LeBrun et al. and associates evaluated functional outcomes of surgically isolated patella fractures. They reported that 52% of patients underwent surgery for hardware removal, and 38% of patients who retained their hardware reported pain at some time. They also found that nearly 20% had extensor lag, and almost 38% had restricted flexion. Extension power on testing showed significant mean deficits when compared to the contralateral side.
Bayar et al. evaluated 20 patients with patella fractures and found that articular incongruity of >1mm was the largest risk factor for quadriceps weakness at a mean of 30 months postoperatively. No significant differences were seen with sex, fracture pattern, or time from injury to surgery.
Illustration A shows patella fixation with plate/screw construct. Incorrect Answers:
Answer 1: Knee flexion arc is generally limited more than the non-injured side.
Answer 2: Extensor lag can be permanent with this treatment method. Answer 4: Quadriceps weakness is common after tension band fixation of patella fractures.
Answer 5: Patients generally have poorer outcomes after patella tension band fixation, regardless of implant maintenance or removal.
Question 32High Yield
-
Which of the following conditions is associated é the highest mortality in patients é a pelvic fracture?
Which of the following conditions is associated é the highest mortality in patients é a pelvic fracture?
Explanation
No detailed explanation provided for this question.
Question 33High Yield
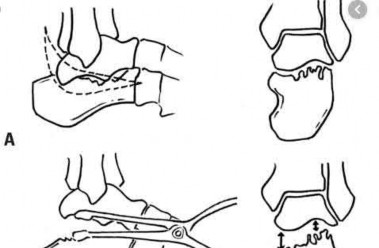
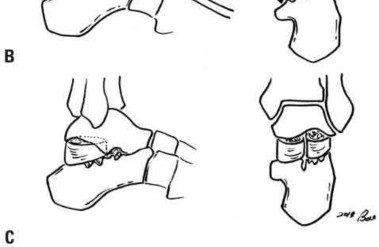
A 27-year-old man presents to the emergency department with an ankle fracture. CT scans note anteromedial marginal impaction.
Which radiograph (Figures A-E) would best correlate with this finding?
Which radiograph (Figures A-E) would best correlate with this finding?







Explanation
This patient has anteromedial marginal impaction seen on CT scans. This is characteristic of a supination-adduction ankle fracture (Figure D).
In the Lauge-Hansen classification, ankle fractures are classified into supination-adduction (SA), supination-external rotation, pronation-abduction, pronation-external rotation. Certain considerations exist when treating SA fractures with marginal impaction: (1) An anteromedial approach will aid in visualizing and reducing the impaction (instead of standard medial approach).
(2) Disimpaction of the articular fragment and possibly bone grafting of the resulting defect may be necessary rather than simple percutaneous fixation.
McConnell et al. reviewed marginal plafond impaction in supination adduction injuries. Supination-adduction injuries comprised 5% of 500 fractures (44 fractures), and 42% (8 fractures) of these had marginal impaction.
Illustration A is another example of a SA fracture depicting vertical fracture of the medial malleolus in association with marginal impaction of the plafond
(arrow). Illustration B is an axial CT showing increased density at the level of the subchondral bone, characteristic of anteromedial marginal impaction.
Illustration C is a coronal CT showing showing articular depression of the impacted segment and tibiotalar incongruity.
Incorrect Answers:
Answer 1: Figure A shows a pronation-abduction ankle fracture. Answer 2: Figure B shows a talar body fracture.
Answer 3: Figure C shows a pronation-external rotation ankle fracture Answer 5: Figure E shows a supination-external rotation ankle fracture. Marginal impaction is not characteristic of these injuries.
In the Lauge-Hansen classification, ankle fractures are classified into supination-adduction (SA), supination-external rotation, pronation-abduction, pronation-external rotation. Certain considerations exist when treating SA fractures with marginal impaction: (1) An anteromedial approach will aid in visualizing and reducing the impaction (instead of standard medial approach).
(2) Disimpaction of the articular fragment and possibly bone grafting of the resulting defect may be necessary rather than simple percutaneous fixation.
McConnell et al. reviewed marginal plafond impaction in supination adduction injuries. Supination-adduction injuries comprised 5% of 500 fractures (44 fractures), and 42% (8 fractures) of these had marginal impaction.
Illustration A is another example of a SA fracture depicting vertical fracture of the medial malleolus in association with marginal impaction of the plafond
(arrow). Illustration B is an axial CT showing increased density at the level of the subchondral bone, characteristic of anteromedial marginal impaction.
Illustration C is a coronal CT showing showing articular depression of the impacted segment and tibiotalar incongruity.
Incorrect Answers:
Answer 1: Figure A shows a pronation-abduction ankle fracture. Answer 2: Figure B shows a talar body fracture.
Answer 3: Figure C shows a pronation-external rotation ankle fracture Answer 5: Figure E shows a supination-external rotation ankle fracture. Marginal impaction is not characteristic of these injuries.
Question 34High Yield
A 10-year-old patient with Hurler syndrome has undergone a bone marrow transplant and is currently medically stable. He has developed a painful thoracolumbar kyphosis that measures 50° with 25% subluxation T12 on L1. Recommended treatment includes which of the following:
Explanation
Anterior and posterior fusion will correct the translation, instability, and ensure a solid fusion.
Exercises will not correct the subluxation, which is the cause of the pain. A thoracolumbar orthosis is not corrective or well tolerated.
There is no need for halo traction.
Posterior fusion alone is not enough to control this focal instability if the patient is well enough to tolerate a more involved procedure.
Exercises will not correct the subluxation, which is the cause of the pain. A thoracolumbar orthosis is not corrective or well tolerated.
There is no need for halo traction.
Posterior fusion alone is not enough to control this focal instability if the patient is well enough to tolerate a more involved procedure.
Question 35High Yield
When evaluating a patient with hallux rigidus, what is the most important clinical factor indicating the need for an arthrodesis as opposed to a cheilectomy?
Explanation
Cheilectomy has been shown to provide satisfactory pain relief and improved function in long-term studies. It is important to select patients appropriately when choosing a cheilectomy versus an arthrodesis. Pain at the midrange of motion and loss of more than 50% of the metatarsal head cartilage are predictors of a poor outcome following cheilectomy, and these patients should receive an arthrodesis.
REFERENCES: Coughlin MJ, Shurnas PS: Hallux rigidus: Grading and long-term results of operative treatment. J Bone Joint Surg Am 2003;85:2072-2088.
Easley ME, Davis WH, Anderson RB: Intermediate to long-term follow-up of medial-approach dorsal cheilectomy for hallux rigidus. Foot Ankle Int 1999;20:147-152.
REFERENCES: Coughlin MJ, Shurnas PS: Hallux rigidus: Grading and long-term results of operative treatment. J Bone Joint Surg Am 2003;85:2072-2088.
Easley ME, Davis WH, Anderson RB: Intermediate to long-term follow-up of medial-approach dorsal cheilectomy for hallux rigidus. Foot Ankle Int 1999;20:147-152.
Question 36High Yield
A 16-year-old high school football player who sustained an acute forceful dorsiflexion ankle injury reported that he felt a pop and then noted immediate swelling over the lateral malleolus. Examination 24 hours later reveals moderate swelling and tenderness along the lateral malleolus. The external rotation, squeeze, anterior drawer, and talar tilt tests are negative. Subluxation of the peroneal tendons is palpable over the peroneal groove of the fibula. Radiographs reveal a small cortical avulsion off the distal rim of the fibula. The stress views show no instability. Initial management for this injury should include
Explanation
The patient has an acute peroneal tendon dislocation. The evaluation for syndesmotic injury and lateral ankle instability is negative. The cortical avulsion off the distal tip of the lateral malleolus, a rim fracture, is characteristic of peroneal tendon dislocations. The sensation of apprehension or frank subluxation of the peroneal tendons with active dorsiflexion of the foot while the foot is held in plantar flexion confirms the diagnosis. Based on these findings, initial management should consist of cast immobilization and protected weight bearing. If a recurrent or chronic condition develops, surgery is the most reliable treatment option.
REFERENCES: Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Marti R: Dislocation of the peroneal tendons. Am J Sports Med 1977;5:19-22.
REFERENCES: Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Marti R: Dislocation of the peroneal tendons. Am J Sports Med 1977;5:19-22.
Question 37High Yield
A 36-year-old right-hand dominant butcher presents with a 6-week history of medial elbow pain. On physical examination, she is tender to palpation over the anteroinferior aspect of the medial epicondyle. Pain is reproduced with combined elbow extension/resisted wrist flexion. Nonsurgical treatment of this pathology results in pain relief within one year in what percentage of individuals?
Explanation
The patient has medial epicondylitis. Nonsurgical treatment is the hallmark of treatment and has been shown to relieve pain in approximately 90% of cases within one year. Nonsurgical modalities include bracing, physical therapy, nonsteroidal anti-inflammatory medications, activity modification, and injections.
12
12
Question 38High Yield
Figures 1 and 2 are the MRI arthrograms of a 14-year-old male baseball player who notes medial-sided elbow pain that occurs during the early acceleration phase of throwing. Pain has continued for one year. Pain improves with rest but worsens once he returns to throw. The longest he has rested is 3 months. He has completed a physical therapy program focusing on elbow strengthening and range of motion. He denies mechanical symptoms. Physical examination shows full elbow range of motion, no tenderness, and pain with moving valgus stress test, although there is no instability noted. There is no pain with resisted wrist flexion. What is the best next step?
Explanation
44
The patient has a clinical history and physical examination consistent with UCL pathology. In an overhead athlete, deficits in the kinetic chain can contribute to the development of medial elbow pathology due to increased force transmission across the elbow. As a result, it is important to examine the shoulder to ensure that total arc of motion remains equivalent to the contralateral arm. Decreases in total arc of motion, commonly associated with glenohumeral internal rotation deficits (GIRD), can predispose athletes to medial elbow injuries. These shoulder deficits can be addressed with physical therapy. The MRI scan shows a structurally intact UCL, therefore, UCL repair or reconstruction is not indicated. The MRI scans demonstrate no evidence of osteochondral injury, which would be an indication for arthroscopic debridement and microfracture.
The patient has a clinical history and physical examination consistent with UCL pathology. In an overhead athlete, deficits in the kinetic chain can contribute to the development of medial elbow pathology due to increased force transmission across the elbow. As a result, it is important to examine the shoulder to ensure that total arc of motion remains equivalent to the contralateral arm. Decreases in total arc of motion, commonly associated with glenohumeral internal rotation deficits (GIRD), can predispose athletes to medial elbow injuries. These shoulder deficits can be addressed with physical therapy. The MRI scan shows a structurally intact UCL, therefore, UCL repair or reconstruction is not indicated. The MRI scans demonstrate no evidence of osteochondral injury, which would be an indication for arthroscopic debridement and microfracture.
Question 39High Yield
Figures 1 through 3 are the radiographs and 3D reconstruction of a 13-year-old right-hand dominant boy who landed onto a flexed right elbow and now has pain, swelling, and crepitation in the right elbow.
The most appropriate treatment would be
The most appropriate treatment would be


Explanation
■
Imaging demonstrates a displaced, T-type intra-articular distal humerus fracture. Anatomic restoration of the articular surface and stable fixation to enable early motion are imperative in this fracture pattern. Thus, open reduction enables articular reduction, safe identification, and protection of the ulnar nerve, and plate osteosynthesis of both condylar fragments. Olecranon osteotomy is not required, given the lack of comminution and large size of the condylar fracture fragments. The proximal position and lateral plane obliquity of the transverse metaphyseal fracture line render stable percutaneous pinning of the distal fragments to the shaft difficult. Additionally, interfragmentary compression of the articular surface is not attainable with percutaneous Kirschner wire fixation. Traction is of historical interest only and not an appropriate treatment at this time.
■
Imaging demonstrates a displaced, T-type intra-articular distal humerus fracture. Anatomic restoration of the articular surface and stable fixation to enable early motion are imperative in this fracture pattern. Thus, open reduction enables articular reduction, safe identification, and protection of the ulnar nerve, and plate osteosynthesis of both condylar fragments. Olecranon osteotomy is not required, given the lack of comminution and large size of the condylar fracture fragments. The proximal position and lateral plane obliquity of the transverse metaphyseal fracture line render stable percutaneous pinning of the distal fragments to the shaft difficult. Additionally, interfragmentary compression of the articular surface is not attainable with percutaneous Kirschner wire fixation. Traction is of historical interest only and not an appropriate treatment at this time.
Question 40High Yield
An 11-year-old obese boy has a 5-month history of unilateral knee pain and a limp. An examination reveals obligate external rotation with flexion and pain with attempted hip internal rotation.
Explanation
- Abnormal femoral head-neck junction offset
Question 41High Yield
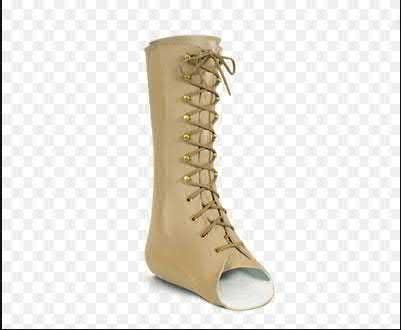
A 36-year-old male sustains the closed injury shown in Figure A after falling from a ladder. He is treated nonoperatively. Two years following the injury he presents to the clinic complaining of laterally based hindfoot pain which is worsened when walking on uneven surfaces. His tibiotalar motion remains pain-free. He obtains good pain relief with a steroid injection into the sinus tarsi. What additional treatment modality is appropriate at this time?

Explanation
The gauntlet ankle brace, commercially known as an Arizona brace, or a solid ankle-foot orthosis and continued nonoperative treatment is appropriate for early subtalar arthritis.
Subtalar arthritis is a common complication following surgical and nonsurgical treatment of intra-articular calcaneus fractures. Nonoperative treatment modalities for the condition include ankle bracing which limits hindfoot inversion-eversion, corticosteroid injections, NSAIDs, and physical therapy.
This is a successful mitigation strategy for many patients. Ultimately if surgical intervention is warranted, with failed nonoperative treatment, a subtalar arthrodesis with or without a bone block can be considered.
Griffin et al. performed a randomized control trial comparing operative and non-operative treatment of intra-articular calcaneus fractures. They found equivalent pain and function results at two years post-injury but did find a higher complication rate following surgical intervention. It should be noted that all operative patients in this cohort were treated with an extensile lateral approach.
Hsu et al. reviewed the recent surgical advances in the treatment of calcaneus fractures. They note that the less invasive techniques, including the sinus tarsi approach, have resulted in an overall decreased complication rate.
Jackson et al. evaluated the use of distraction bone block arthrodesis for malunion correction following calcaneus fractures. In addition to the standard requirement of lateral wall exostectomy, a bone block is required to correct the loss of height and restore the normal talar declination. This technique can aid in symptom relief in patients who are having anterior ankle impingement secondary to loss of calcaneal height.
Figure A is a lateral radiograph showing and intra-articular calcaneus fracture. Illustration A is a schematic of a bone block arthrodesis. Illustration B is a clinical photograph of a gauntlet ankle brace.
Incorrect Answers:
Answer 1: An ASO or lace-up ankle brace may be attempted, but typically does not provide the inversion/eversion stability required for pain relief.
Answer 3: An orthotic with arch support and medial wedging is typically used for pes planovalgus.
Answer 4: The University of California Biomechanics Lab orthotic does not sufficiently limit subtalar motion.
Answer 5: This patient should undergo further non-operative treatment before surgical considerations.
Subtalar arthritis is a common complication following surgical and nonsurgical treatment of intra-articular calcaneus fractures. Nonoperative treatment modalities for the condition include ankle bracing which limits hindfoot inversion-eversion, corticosteroid injections, NSAIDs, and physical therapy.
This is a successful mitigation strategy for many patients. Ultimately if surgical intervention is warranted, with failed nonoperative treatment, a subtalar arthrodesis with or without a bone block can be considered.
Griffin et al. performed a randomized control trial comparing operative and non-operative treatment of intra-articular calcaneus fractures. They found equivalent pain and function results at two years post-injury but did find a higher complication rate following surgical intervention. It should be noted that all operative patients in this cohort were treated with an extensile lateral approach.
Hsu et al. reviewed the recent surgical advances in the treatment of calcaneus fractures. They note that the less invasive techniques, including the sinus tarsi approach, have resulted in an overall decreased complication rate.
Jackson et al. evaluated the use of distraction bone block arthrodesis for malunion correction following calcaneus fractures. In addition to the standard requirement of lateral wall exostectomy, a bone block is required to correct the loss of height and restore the normal talar declination. This technique can aid in symptom relief in patients who are having anterior ankle impingement secondary to loss of calcaneal height.
Figure A is a lateral radiograph showing and intra-articular calcaneus fracture. Illustration A is a schematic of a bone block arthrodesis. Illustration B is a clinical photograph of a gauntlet ankle brace.
Incorrect Answers:
Answer 1: An ASO or lace-up ankle brace may be attempted, but typically does not provide the inversion/eversion stability required for pain relief.
Answer 3: An orthotic with arch support and medial wedging is typically used for pes planovalgus.
Answer 4: The University of California Biomechanics Lab orthotic does not sufficiently limit subtalar motion.
Answer 5: This patient should undergo further non-operative treatment before surgical considerations.
Question 42High Yield
MRI results are shown in Figure 1 for a 22-year-old, right-hand dominant collegiate athlete who reports a 6-month history of progressive weakness in his right arm. He denies any specific traumatic event. He has altered his weight-lifting activities and tried over-the-counter ibuprofen without benefit. No appreciable deformity or atrophy is found on examination of the upper extremities. He demonstrates full active shoulder range of motion, and there is no weakness with abduction in the plane of the scapula. Belly press test findings are normal, but weakness is seen in external rotation with the arm in adduction. He does not demonstrate anterior apprehension, and there is no instability with load and shift testing. Radiographs are unremarkable. What is the best surgical option?
Explanation
This patient’s clinical and MRI findings are consistent with a posterior paralabral cyst with compression of the suprascapular nerve, specifically at the spinoglenoid notch. Compression of the suprascapular nerve can occur at either the suprascapular or spinoglenoid notch. Compression of the nerve at the suprascapular notch affects innervation to both the supraspinatus and infraspinatus muscles, resulting in weakness in both shoulder abduction and external rotation. However, compression at the spinoglenoid notch only affects innervation to the infraspinatus muscle, resulting in isolated weakness in external rotation.
Compression at the spinoglenoid notch often is seen in overhead athletes, and studies have shown associated posterior labral tears (Piatt and associates). Several studies have addressed nonsurgical and surgical treatment options. The treatment decision should focus on the underlying cause (Martin and associates)—in this patient, the cyst. Nonsurgical treatment in the presence of a known lesion has been associated with a higher failure rate than addressing the lesion, which can result in functional improvement (Chen and associates, Cummins and associates). The best response in this scenario is decompression of the cyst at the spinoglenoid notch with possible labral repair.
42
Compression at the spinoglenoid notch often is seen in overhead athletes, and studies have shown associated posterior labral tears (Piatt and associates). Several studies have addressed nonsurgical and surgical treatment options. The treatment decision should focus on the underlying cause (Martin and associates)—in this patient, the cyst. Nonsurgical treatment in the presence of a known lesion has been associated with a higher failure rate than addressing the lesion, which can result in functional improvement (Chen and associates, Cummins and associates). The best response in this scenario is decompression of the cyst at the spinoglenoid notch with possible labral repair.
42
Question 43High Yield
Figures 91a through 91c are the radiographs of a 10-year-old boy who has a 6-month history of progressive heel pain. The patient is a year-round soccer player and now experiences pain with most every step. What is the most appropriate management?
Explanation
The patient has calcaneal apophysitis, an overuse syndrome common in children ages 9 to12 years. Symptoms are usually the result of excess tension and a tight heel cord. Management includes activity modification, as well as heel cord stretching, nonsteroidal anti-inflammatory drugs, icing, and other modalities. Radiographs are typically negative; MRI is unnecessary. Custom orthotics are not indicated. The condition is self-limiting, in that the symptoms fully resolve once the apophyses fuses,such that surgery is rarely indicated.
Question 44High Yield
Figure 13 shows the MRI scan of a 29-year-old rock climber who reports increasing shoulder pain and weakness. Based on these findings, atrophy will most likely occur in which of the following muscles?**
Explanation
The MRI scan shows a cyst at the spinoglenoid notch. These cysts are often associated with a labral injury, such as a superior labrum anterior and posterior (SLAP) lesion. The suprascapular nerve passes through the suprascapular notch and sends motor branches to the supraspinatus and sensory branches to the capsule. At the spinoglenoid notch, the infraspinatus branch of the suprascapular nerve is compressed by the cyst, leading to isolated infraspinatus atrophy. The teres minor and the deltoid are innervated by the axillary nerve.
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Ianotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Tirman PF, Feller JF, Janzen DL, Peterfy CG, Bergman AG: Association of glenoid labral cysts and labral tears in glenohumeral instability: Radiologic findings and clinical significance. Radiology 1994;190:653-658.
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Ianotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Tirman PF, Feller JF, Janzen DL, Peterfy CG, Bergman AG: Association of glenoid labral cysts and labral tears in glenohumeral instability: Radiologic findings and clinical significance. Radiology 1994;190:653-658.
Question 45High Yield
Which of the following is not considered to be a risk factor for peroneal tendon tears:
Explanation
A shallow retrofibular groove and ligamentous laxity predispose to subluxation of the peroneal tendons causing attritional tears over the posterolateral fibular ridge. Varus hindfoot alignment places patients at risk for inversion sprains, which may cause trauma to the peroneal tendons when they are put on stretch. Heel chord contracture has not been implicated in the development of peroneal tendon tears.
Question 46High Yield
A 68-year-old right-hand-dominant woman has experienced progressive right elbow pain and loss of motion for several years. She has failed nonsurgical treatment and elects to undergo a total elbow arthroplasty (TEA). In comparison to a linked prosthesis, an unlinked prosthesis has which reported distinction with extended follow-up?
Explanation
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
RECOMMENDED READINGS
63. [Kudo H, Iwano K. Total elbow arthroplasty with a non-constrained surface-replacement prosthesis in patients who have rheumatoid arthritis. A long-term follow-up study. J Bone Joint Surg Am. 1990 Mar;72(3):355-62. PubMed PMID: 2312530.](http://www.ncbi.nlm.nih.gov/pubmed/2312530)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2312530)
64. [Plaschke HC, Thillemann TM, Brorson S, Olsen BS. Implant survival after total elbow arthroplasty: a retrospective study of 324 procedures performed from 1980 to 2008. J Shoulder Elbow Surg. 2014 Jun;23(6):829-36. doi: 10.1016/j.jse.2014.02.001. Epub 2014 Apr 22. ](http://www.ncbi.nlm.nih.gov/pubmed/24766794)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24766794)
65. [Dos Remedios C, Chantelot C, Giraud F, Migaud H, Fontaine C. Results with Kudo elbow prostheses in non-traumatic indications : a study of 36 cases. Acta Orthop Belg. 2005 Jun;71(3):273-88. PubMed PMID: 16035700. ](http://www.ncbi.nlm.nih.gov/pubmed/16035700)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16035700)
RECOMMENDED READINGS
63. [Kudo H, Iwano K. Total elbow arthroplasty with a non-constrained surface-replacement prosthesis in patients who have rheumatoid arthritis. A long-term follow-up study. J Bone Joint Surg Am. 1990 Mar;72(3):355-62. PubMed PMID: 2312530.](http://www.ncbi.nlm.nih.gov/pubmed/2312530)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2312530)
64. [Plaschke HC, Thillemann TM, Brorson S, Olsen BS. Implant survival after total elbow arthroplasty: a retrospective study of 324 procedures performed from 1980 to 2008. J Shoulder Elbow Surg. 2014 Jun;23(6):829-36. doi: 10.1016/j.jse.2014.02.001. Epub 2014 Apr 22. ](http://www.ncbi.nlm.nih.gov/pubmed/24766794)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24766794)
65. [Dos Remedios C, Chantelot C, Giraud F, Migaud H, Fontaine C. Results with Kudo elbow prostheses in non-traumatic indications : a study of 36 cases. Acta Orthop Belg. 2005 Jun;71(3):273-88. PubMed PMID: 16035700. ](http://www.ncbi.nlm.nih.gov/pubmed/16035700)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16035700)
Question 47High Yield
Slide 1 Slide 2
The patient presented (Slide 1 and Slide 2) has a hereditary sensory motor neuropathy. Based upon the photographs, a surgeon should be able to determine the pattern of muscle weakness. Weakness in which muscle is most likely the cause of this deformity:
The patient presented (Slide 1 and Slide 2) has a hereditary sensory motor neuropathy. Based upon the photographs, a surgeon should be able to determine the pattern of muscle weakness. Weakness in which muscle is most likely the cause of this deformity:
Explanation
Although the anterior tibial muscle is weak, the cavus is the predominant deformity of this condition, caused by weakness of the peroneus brevis. The peroneus longus is functioning and is responsible for the plantarflexion of the first metatarsal.
Question 48High Yield
81
Figures 94a and 94b show T1 sagittal and coronal MR images of the right shoulder of a 45-year-old woman. She has insidious onset of dull, aching right shoulder pain localized at the superior aspect of her shoulder. The nerve that supplies the atrophied muscle arises from the upper trunk from contributions of which nerve roots?
A
B
Figures 94a and 94b show T1 sagittal and coronal MR images of the right shoulder of a 45-year-old woman. She has insidious onset of dull, aching right shoulder pain localized at the superior aspect of her shoulder. The nerve that supplies the atrophied muscle arises from the upper trunk from contributions of which nerve roots?
A
B
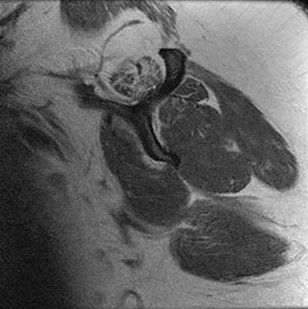
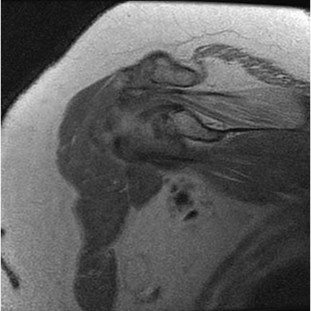
Explanation
The suprascapular nerve innervates the supraspinatus muscle. Patients with suprascapular neuropathy usually have insidious onset of dull, aching shoulder pain at the superior or posterior aspect of the shoulder. There can be several causes of nerve compression, and the nerve is susceptible to compression at the suprascapular and spinoglenoid notches. Extrinsic compression can be secondary to joint-related fluid filled cysts of soft-tissue masses. Traction neuropathy may occur as the result of excessive nerve excursion during athletic activity (usually overhead sports) or after a massive, retracted rotator cuff tear. The suprascapular nerve originates from the upper trunk from predominantly the C5 and C6 nerve roots, with an occasional contribution from the C4 nerve root.
RECOMMENDED READINGS
1. Boykin RE, Friedman DJ, Higgins LD, Warner JJ. Suprascapular neuropathy. J Bone Joint Surg Am. 2010 Oct 6;92(13):2348-64. doi: 10.2106/JBJS.I.01743. Review. 81
[PubMed PMID: 20926731. ](http://www.ncbi.nlm.nih.gov/pubmed/20926731)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20926731)
2. [Piasecki DP, Romeo AA, Bach BR Jr, Nicholson GP. Suprascapular neuropathy. J Am Acad Orthop Surg. 2009 Nov;17(11):665-76. Review. PubMed PMID: 19880677 ](http://www.ncbi.nlm.nih.gov/pubmed/19880677)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19880677)
RECOMMENDED READINGS
1. Boykin RE, Friedman DJ, Higgins LD, Warner JJ. Suprascapular neuropathy. J Bone Joint Surg Am. 2010 Oct 6;92(13):2348-64. doi: 10.2106/JBJS.I.01743. Review. 81
[PubMed PMID: 20926731. ](http://www.ncbi.nlm.nih.gov/pubmed/20926731)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20926731)
2. [Piasecki DP, Romeo AA, Bach BR Jr, Nicholson GP. Suprascapular neuropathy. J Am Acad Orthop Surg. 2009 Nov;17(11):665-76. Review. PubMed PMID: 19880677 ](http://www.ncbi.nlm.nih.gov/pubmed/19880677)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19880677)
Question 49High Yield
A 31-year-old female presents to the trauma bay following a motorcycle crash. Her blood pressure is 95/70 mmHg, heart rate is 115 bpm. Lactate measured in the trauma bay is 10 mmol/L. She has multiple rib fractures, pulmonary contusions, and a positive FAST exam requiring immediate exploratory laparotomy. After laparotomy her lacate remains unchanged. She has a closed right femur fracture and an open right tibia fracture as seen in Figures A and B. Besides antibiotics and thorough irrigation and debridement, which of the following would be an appropriate step in the immediate management of her fractures?


Explanation
This patient is suffering from multiple injuries and has evidence of chest injury and incomplete resuscitation. The immediate treatment of her fractures should be external fixation for both the tibia and the femur.
For polytraumatized patients with multiple injuries including extremity fractures, damage control orthopaedics dictates that long bone fractures should be temporarily stabilized. Either inadequate stabilization, or early total care, such as a reamed or unreamed nails, can exacerbate the patient's condition and increase the risk of a second-hit phenomenon. For this patient with pulmonary contusions and continued elevation of lactate indicating end-organ hypoperfusion her extremities should have staged treatment according to damage control principles.
Morshed et al. present a retrospective review of polytraumatized patients with femur fractures and compared outcomes based on the time frame in which their fractures were definitively treated. They found delaying treatment at least 12 hours to allow appropriate resuscitation and treatment of other traumatic injuries led to a decrease in mortality of 50%. Patients with intra-abdominal injuries benefited most from staged treatment of the extremities.
Figure A is a radiograph showing a closed right femur fracture. Figure B is a radiograph of an open right tibia fracture.
Incorrect answers:
Answers 1-3: Immediate intramedullary nailing, either reamed or unreamed, in this patient would increase her risk of fat emboli syndrome, and should not be done acutely.
Answer 4: A posterior slab splint would not adequately stabilize the tibia fracture seen, and should not be used instead of external fixation. Splints would also make it more difficult to monitor this patient's skin, compartments, and her traumatic wound. Similarly, skeletal traction alone of the femur fracture would be insufficient.
For polytraumatized patients with multiple injuries including extremity fractures, damage control orthopaedics dictates that long bone fractures should be temporarily stabilized. Either inadequate stabilization, or early total care, such as a reamed or unreamed nails, can exacerbate the patient's condition and increase the risk of a second-hit phenomenon. For this patient with pulmonary contusions and continued elevation of lactate indicating end-organ hypoperfusion her extremities should have staged treatment according to damage control principles.
Morshed et al. present a retrospective review of polytraumatized patients with femur fractures and compared outcomes based on the time frame in which their fractures were definitively treated. They found delaying treatment at least 12 hours to allow appropriate resuscitation and treatment of other traumatic injuries led to a decrease in mortality of 50%. Patients with intra-abdominal injuries benefited most from staged treatment of the extremities.
Figure A is a radiograph showing a closed right femur fracture. Figure B is a radiograph of an open right tibia fracture.
Incorrect answers:
Answers 1-3: Immediate intramedullary nailing, either reamed or unreamed, in this patient would increase her risk of fat emboli syndrome, and should not be done acutely.
Answer 4: A posterior slab splint would not adequately stabilize the tibia fracture seen, and should not be used instead of external fixation. Splints would also make it more difficult to monitor this patient's skin, compartments, and her traumatic wound. Similarly, skeletal traction alone of the femur fracture would be insufficient.
Question 50High Yield
A 58-year-old woman returns for an evaluation of right knee pain after a twisting injury. A small pop was felt at the time of injury. Her pain is medial and she is unable to bear weight. A complete physical examination demonstrated range of motion is 0°to 125°; significant medial joint line tenderness; negative flexion McMurray; negative Lachman; stable to varus and valgus stress at 0° and 30° and negative posterior drawer. Based on her history, physical examination, and the MRI scan shown in Figure 1, what is the diagnosis?
Explanation
63
The low likelihood that common symptoms associated with meniscal body injury will manifest in patients with root tears makes clinical diagnoses challenging. For instance, patients with a posterior root tear injury may experience joint line pain, but the absence of mechanical symptoms such as locking or catching is probable. Meniscal root tears are also not typically associated with an inciting traumatic event. MRI has become increasingly used in the diagnosis of meniscal root tears. Telltale signs of a root tear include the presence or absence of a ghost sign, which is the absence of an identifiable meniscus in the sagittal plane or high signal replacing the normal dark meniscal signal. The posterior meniscus is seen in sagittal MRI view in all images up to the one that shows the PCL. The posterior root of the medial meniscus attaches anterior to the posterior cruciate ligament (PCL).
The low likelihood that common symptoms associated with meniscal body injury will manifest in patients with root tears makes clinical diagnoses challenging. For instance, patients with a posterior root tear injury may experience joint line pain, but the absence of mechanical symptoms such as locking or catching is probable. Meniscal root tears are also not typically associated with an inciting traumatic event. MRI has become increasingly used in the diagnosis of meniscal root tears. Telltale signs of a root tear include the presence or absence of a ghost sign, which is the absence of an identifiable meniscus in the sagittal plane or high signal replacing the normal dark meniscal signal. The posterior meniscus is seen in sagittal MRI view in all images up to the one that shows the PCL. The posterior root of the medial meniscus attaches anterior to the posterior cruciate ligament (PCL).
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon