Orthopedic With Answer An Review | Dr Hutaif General Or -...
14 Apr 2026
91 min read
98 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic With Answer An Review | Dr Hutaif ...
00:00
Start Quiz
Question 1High Yield
A 32-year-old powerlifter who was performing a dead lift 3 days ago noted a sharp pain in the front of his dominant right arm just after beginning to lower the weight. He now reports pain in the anterior aspect of the arm that worsens when he opens a door. Examination reveals moderate ecchymosis and swelling of the forearm and tenderness in the antecubital fossa. The MRI scans are shown in Figures 15a and 15b. If the injury is left unrepaired, the greatest functional deficit will most likely be the loss of
Explanation
A complete tear of the distal biceps brachii most often occurs from a large, rapid eccentric elbow extension load. A pop or tearing sensation usually occurs, and a palpable defect in the antecubital fossa is often present on examination. The treatment of choice is a direct primary repair by a two-incision technique. If left unrepaired, the most disabling consequence is the loss of forearm supination strength. It is unlikely that significant elbow or forearm motion will be lost if the rupture is left unrepaired and early motion exercises are initiated. Elbow flexion strength tends to return with time, but the loss of forearm supination strength remains problematic.
REFERENCES: D’Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119.
Agins HJ, Chess JL, Hoekstra DV, Teitge RA: Rupture of the distal insertion of the biceps brachii tendon. Clin Orthop 1988;234:34-38.
REFERENCES: D’Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119.
Agins HJ, Chess JL, Hoekstra DV, Teitge RA: Rupture of the distal insertion of the biceps brachii tendon. Clin Orthop 1988;234:34-38.
Question 2High Yield
Figure 58 is the radiograph of a laborer who has hindfoot and ankle pain. He is a type 1 diabetic, and has a BMI of 25 and a Hgb A1c of 6. What is the most appropriate management at this time?
Explanation
The radiograph shows Charcot changes in the subtalar joint. In the absence of gross deformity, the initial treatment is nonsurgical, consisting of total contact casting, with frequent cast changes and progression to weight bearing when swelling subsides and early consolidation is seen radiographically. A walking boot will not provide sufficient immobilization, whereas bed rest carries the risk of significant deconditioning in an otherwise active patient with well-controlled diabetes. Surgery as the initial treatment is not indicated in the absence of gross deformity or ulceration.
Question 3High Yield
An 11-year-old boy stepped on a nail and sustained a puncture to the right forefoot 6 days ago. He was wearing tennis shoes at the time of injury. Treatment in the emergency department consisted of local debridement and tetanus prophylaxis; a radiograph was negative for foreign body, chondral defect, or fracture. He was discharged with a 3-day prescription of amoxicillin and clavulanate. The patient now has increasing pain and tenderness at the puncture site. What is the best course of action?
Explanation
The initial treatment consisting of oral antibiotics was appropriate but with progressive symptoms, surgical debridement is necessary. Ciprofloxacin is contraindicated in children, and at this stage, oral antibiotics are inadequate. Intravenous antibiotics may be necessary, but surgical debridement is paramount. Failure to respond to the initial management precludes further observation.
REFERENCES: Riegler HP, Routson T: Complications of deep puncture wounds of the foot.
J Trauma 1979;19:18-22.
Green NE: Musculoskeletal infections in children: Part IV. Pseudomonas infections of the foot following puncture wounds. Instr Course Lect 1983;32:43-46.
REFERENCES: Riegler HP, Routson T: Complications of deep puncture wounds of the foot.
J Trauma 1979;19:18-22.
Green NE: Musculoskeletal infections in children: Part IV. Pseudomonas infections of the foot following puncture wounds. Instr Course Lect 1983;32:43-46.
Question 4High Yield
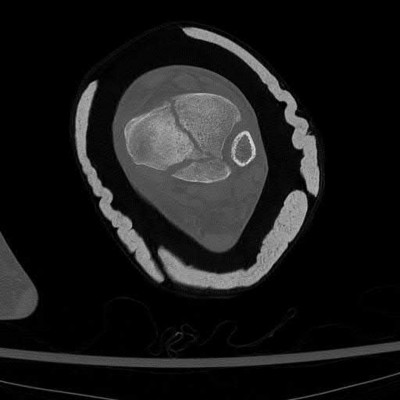
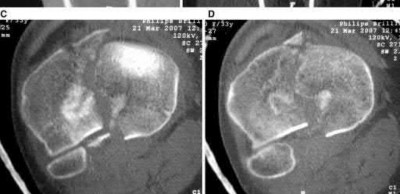
Figure 1 is an MRI scan of the right hip of a 19-year-old woman with a 6-month history of right groin pain. She was diagnosed with a stress fracture and was treated with 3 months of limited weight bearing. Figure 2 is a repeat MRI scan in which the edema pattern changed minimally but the pain worsened. Ibuprofen alleviates most of her pain. What is the best next step?
---
---








Explanation
An osteoid osteoma is a benign bone tumor. Osteoid osteomas tend to be small—typically <1.5 cm. Regardless of their size, they cause a large amount of reactive bone to form around them, and they make a new type of abnormal bone material called osteoid bone. This osteoid bone, along with the tumor
cells, forms the nidus of the tumor, which is easily identified on CT scans.
cells, forms the nidus of the tumor, which is easily identified on CT scans.
Question 5High Yield
A 63-year-old man has long-standing type 2 diabetes. He has had associated ongoing neuropathy for approximately 5 years. He now reports a red, hot, swollen right foot for the past 2 days. You place him supine in your office with the foot elevated for 30 minutes. You return to see that the redness has dissipated. What is the most likely diagnosis?
Explanation
Charcot arthropathy is a progressive condition of the musculoskeletal system that is characterized by joint dislocations, pathologic fractures, and debilitating deformities. This disorder results in progressive destruction of bone and soft tissues at weight-bearing joints; in its most severe form, it may cause significant disruption of the bony architecture. In patients with diabetes, the incidence of acute Charcot arthropathy of the foot and ankle ranges from 0.15% to 2.5%. Acute Charcot arthropathy almost always appears with signs of inflammation. Profound unilateral swelling, an increase in local skin temperature (generally, an increase of 3° to 7° above the nonaffected foot’s skin temperature), erythema,joint effusion, and bone resorption in an insensate foot are present. These characteristics, in the presence of intact skin and a loss of protective
sensation, are often pathognomonic of acute Charcot arthropathy.Cellulitis is an infection of the skin and osteomyelitis is an infection of the bone; examination of the limb would remain unchanged after 30 minutes of elevation. Reynaud and Sjogren syndromes are rheumatologic conditions that do not have these symptoms.
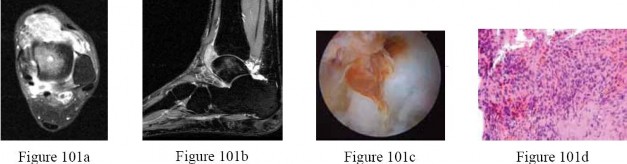
CLINICAL SITUATION FOR QUESTIONS 101 THROUGH 103
A 27-year-old woman has had pain in her right ankle for 2 years. Examination reveals a slightly warmjoint, without erythema. Ankle range of motion is limited by pain.
Radiographs are unremarkable.Because management consisting of immobilization, nonsteroidal anti-inflammatory drugs, and physiotherapy has failed to provide relief, MRI scans are obtained and shown in Figures 101a and 101b.An intraoperative image and the histology are shown in Figures 101c and 101d.
---
sensation, are often pathognomonic of acute Charcot arthropathy.Cellulitis is an infection of the skin and osteomyelitis is an infection of the bone; examination of the limb would remain unchanged after 30 minutes of elevation. Reynaud and Sjogren syndromes are rheumatologic conditions that do not have these symptoms.
CLINICAL SITUATION FOR QUESTIONS 101 THROUGH 103
A 27-year-old woman has had pain in her right ankle for 2 years. Examination reveals a slightly warmjoint, without erythema. Ankle range of motion is limited by pain.
Radiographs are unremarkable.Because management consisting of immobilization, nonsteroidal anti-inflammatory drugs, and physiotherapy has failed to provide relief, MRI scans are obtained and shown in Figures 101a and 101b.An intraoperative image and the histology are shown in Figures 101c and 101d.
---
Question 6High Yield
A 57-year-old man has end-stage osteoarthritis of his right knee. To mechanically align the total knee arthroplasty (TKA) with a neutral coronal plane axis, the surgeon should cut the
Explanation
Standard cuts for a mechanically aligned TKA with a 0 axis in the coronal plane would include a distal femoral cut of 4° to 6° of valgus with respect to the anatomic axis of the femur. The tibial cut should be measured at 0° with respect to the anatomic or mechanical axis of the tibia, because they are often the same in the tibia. A 90° cut of the femur with respect to the anatomic axis would place the knee in significant valgus.
Question 7High Yield
A 3-year-old girl has had pain and swelling in her left thigh for the past 3 weeks. Her mother states she has had a temperature as high as 100.4 degrees F (38 degrees C) and a weight loss of 5 pounds. A CBC shows a WBC count of 11,000/mm3, an erythrocyte sedimentation rate of 13 mm/h, and a C-reactive protein of 0.3. A radiograph is shown in Figure 2. What is the next step in management?
Explanation
The history and laboratory studies indicate that this is not an infection. A lesion in this location and in this age group is likely a Ewing’s sarcoma. The presentation is usually a painful mass. About 20% of patients have a fever. The radiograph shows a typical mottled, permeative lesion with periosteal reaction. An MRI scan should be obtained to further evaluate the soft-tissue mass. Staging of the lesion should take place before biopsy, which should be done by the surgeon who would be performing the next stage of surgical treatment, ideally an orthopaedic oncologist.
REFERENCES: Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Meyer JS, Nadel HR, Marina N, et al: Imaging guidelines for children with Ewing sarcoma and osteosarcoma: A report from the Children’s Oncology Group Bone Tumor Committee. Pediatr Blood Cancer 2008;51:163-170.
T
_AL-Madena Copy_
REFERENCES: Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Meyer JS, Nadel HR, Marina N, et al: Imaging guidelines for children with Ewing sarcoma and osteosarcoma: A report from the Children’s Oncology Group Bone Tumor Committee. Pediatr Blood Cancer 2008;51:163-170.
T
_AL-Madena Copy_
Question 8High Yield
Figure 26 is the MR image of a 55-year-old man who sustained an acute traumatic injury to his right shoulder and loss of active range of motion. He was initially evaluated by his primary care physician and treated with physical therapy without success. He was referred to an orthopaedist for surgical consultation 8 weeks after sustaining the injury. The orthopaedic surgeon performs a successful arthroscopic repair but notes poor tendon quality at the repair site. The treating surgeon keeps the patient in a sling full time for 6 weeks without formal therapy. One year after surgery, in comparison to early therapy, this rehabilitation program will likely result in

Explanation
Historically, orthopaedic surgeons considered early range-of-motion programs following rotator cuff surgery secondary to concerns about potential postsurgical stiffness. Although this may have been a primary open repair concern, arthroscopic surgery appears to substantially decrease this risk. More recently, investigators are reporting similar results in terms of range of motion, retear rate, and functional outcome scores among patients who undergo early and delayed rehabilitation programs.
RECOMMENDED READINGS
25. [Parsons BO, Gruson KI, Chen DD, Harrison AK, Gladstone J, Flatow EL. Does slower rehabilitation after arthroscopic rotator cuff repair lead to long-term stiffness? J Shoulder Elbow Surg. 2010 Oct;19(7):1034-9. doi: 10.1016/j.jse.2010.04.006. Epub 2010 Jul 24. ](http://www.ncbi.nlm.nih.gov/pubmed/20655763)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20655763)
26. [Cuff DJ, Pupello DR. Prospective randomized study of arthroscopic rotator cuff repair using an early versus delayed postoperative physical therapy protocol. J Shoulder Elbow Surg. 2012 Nov;21(11):1450-5. doi: 10.1016/j.jse.2012.01.025. Epub 2012 May 2. ](http://www.ncbi.nlm.nih.gov/pubmed/22554876)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22554876)
27. [Jarrett CD, Schmidt CC. Arthroscopic treatment of rotator cuff disease. J Hand Surg Am. 2011 Sep;36(9):1541-52; quiz 1552. doi: 10.1016/j.jhsa.2011.06.026. Epub 2011 Aug 6. Review. PubMed PMID: 21821368. ](http://www.ncbi.nlm.nih.gov/pubmed/21821368)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21821368)
28. [Chan K, MacDermid JC, Hoppe DJ, Ayeni OR, Bhandari M, Foote CJ, Athwal GS. Delayed versus early motion after arthroscopic rotator cuff repair: a meta-analysis. J Shoulder Elbow Surg. 2014 Nov;23(11):1631-9. doi: 10.1016/j.jse.2014.05.021. Epub 2014 Aug 13. ](http://www.ncbi.nlm.nih.gov/pubmed/25127908)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25127908)
RECOMMENDED READINGS
25. [Parsons BO, Gruson KI, Chen DD, Harrison AK, Gladstone J, Flatow EL. Does slower rehabilitation after arthroscopic rotator cuff repair lead to long-term stiffness? J Shoulder Elbow Surg. 2010 Oct;19(7):1034-9. doi: 10.1016/j.jse.2010.04.006. Epub 2010 Jul 24. ](http://www.ncbi.nlm.nih.gov/pubmed/20655763)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20655763)
26. [Cuff DJ, Pupello DR. Prospective randomized study of arthroscopic rotator cuff repair using an early versus delayed postoperative physical therapy protocol. J Shoulder Elbow Surg. 2012 Nov;21(11):1450-5. doi: 10.1016/j.jse.2012.01.025. Epub 2012 May 2. ](http://www.ncbi.nlm.nih.gov/pubmed/22554876)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22554876)
27. [Jarrett CD, Schmidt CC. Arthroscopic treatment of rotator cuff disease. J Hand Surg Am. 2011 Sep;36(9):1541-52; quiz 1552. doi: 10.1016/j.jhsa.2011.06.026. Epub 2011 Aug 6. Review. PubMed PMID: 21821368. ](http://www.ncbi.nlm.nih.gov/pubmed/21821368)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21821368)
28. [Chan K, MacDermid JC, Hoppe DJ, Ayeni OR, Bhandari M, Foote CJ, Athwal GS. Delayed versus early motion after arthroscopic rotator cuff repair: a meta-analysis. J Shoulder Elbow Surg. 2014 Nov;23(11):1631-9. doi: 10.1016/j.jse.2014.05.021. Epub 2014 Aug 13. ](http://www.ncbi.nlm.nih.gov/pubmed/25127908)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25127908)
Question 9High Yield
A 54-year-old woman undergoes an interposition arthroplasty that fails and requires conversion to a total elbow arthroplasty. She has progressive elbow pain and radiographic loosening. Erythrocyte sedimentation rate and C-reactive protein are normal. Joint aspiration is positive for Staphylococcus epidermidis. What surgical treatment would best optimize function and decrease risk of recurrence?
Explanation
DISCUSSION
The most reliable surgical option in this case for eradicating a deep infection following a total elbow arthroplasty is a two-stage revision. One study, however, reported that staged reimplantation of an infected total elbow replacement could be successful in the setting of organisms other than S epidermidis. Arthroscopic debridement is not a viable option with poorly fixed or loose components. A single-stage revision, while considered an option in hip and knee arthroplasty, has not been definitively proven to be an option for revision total elbow arthroplasty. Single-stage revision has shown moderate success in the setting of Staphylococcus aureus infections, although with only short-term follow-up. A resection arthroplasty would likely be successful in managing the deep infection but would not optimize the functional result. Resection arthroplasty
is best reserved for low-demand or infirm patients.
DISCUSSION
The most reliable surgical option in this case for eradicating a deep infection following a total elbow arthroplasty is a two-stage revision. One study, however, reported that staged reimplantation of an infected total elbow replacement could be successful in the setting of organisms other than S epidermidis. Arthroscopic debridement is not a viable option with poorly fixed or loose components. A single-stage revision, while considered an option in hip and knee arthroplasty, has not been definitively proven to be an option for revision total elbow arthroplasty. Single-stage revision has shown moderate success in the setting of Staphylococcus aureus infections, although with only short-term follow-up. A resection arthroplasty would likely be successful in managing the deep infection but would not optimize the functional result. Resection arthroplasty
is best reserved for low-demand or infirm patients.
Question 10High Yield
The peroneus brevis is the primary antagonist to which of the following structures?
Explanation
The primary function of the peroneus brevis is eversion of the foot, thus acting as the primary antagonist of the posterior tibialis, which inverts the foot, and secondarily plantar flexes the ankle.The anterior tibialis secondarily inverts the foot and only acts as a partial antagonist of the posterior tibialis. The peroneus longus plantar flexes the first ray.
Question 11High Yield
-Clinical staging of osteomyelitis using the Cierney-Mader classification system takes into account which of the following factors?
Explanation
No detailed explanation provided for this question.
Question 12High Yield
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
Subscapularis tears can be associated with disruption of the transverse ligament supporting the biceps. The remaining aspects of the rotator cuff, superior labrum, and capsule can be intact with this injury.
REFERENCES: Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
REFERENCES: Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
Question 13High Yield
With the use of perineural catheters, improvement in all of the following outcomes can be anticipated except:
Explanation
Double blind placebo controlled randomized trials the use of perineural catheters led to improved pain scores, decreased narcotiCusage and narcotiCrelated side effects, and fewer sleep disturbances.
Length of stay was shortened by the use of perineural catheters as compared to epidural or IV PCA analgesia in several studies. In pilot studies, the use of perineural catheters in carefully selected patients allowed ambulatory total shoulder arthroplasty and single day admissions for total hip arthroplasty and total knee arthroplasty
Length of stay was shortened by the use of perineural catheters as compared to epidural or IV PCA analgesia in several studies. In pilot studies, the use of perineural catheters in carefully selected patients allowed ambulatory total shoulder arthroplasty and single day admissions for total hip arthroplasty and total knee arthroplasty
Question 14High Yield
..Figures 78a and 78b are the radiographs of a 47-year-old right-hand-dominant woman who has a 3-month history of gradually progressive right shoulder pain. She reports no previous trauma, but does report pain at night and with activity such as weight training. Examination demonstrates active and passive range of motion to be 110 degrees forward elevation, external rotation to 20 degrees, and internal rotation to the sacrum. The next treatment step should include
Explanation
- a home stretching program and corticosteroid injection.
RESPONSES FOR QUESTIONS 79 THROUGH 82
RESPONSES FOR QUESTIONS 79 THROUGH 82
Question 15High Yield
A 10-year-old girl fell from her bike and now reports pain and swelling in the left knee and pain with weight bearing. Examination reveals a left knee effusion and pain with range of motion. A radiograph is shown in Figure 85. Treatment should consist of
Explanation
DISCUSSION: The child has a type III tibial spine avulsion fracture. When the avulsed fragment is completely displaced, the preferred treatment is open or arthroscopic reduction of the fragment and internal fixation with sutures or screws. Type I fractures are nondisplaced and can be treated with a long leg cast; type II fractures are hinged and can be treated in a long leg cast if closed reduction is successful. Many patients have some objective anterior cruciate ligament laxity after a tibial spine avulsion fracture; however, with adequate treatment most patients do not have symptomatic laxity.
REFERENCES: Mah JY, Adili A, Otsuka NY, et al: Follow-up study of arthroscopic reduction and fixation of type III tibial-eminence fractures. J Pediatr Orthop 1998; 18:475-477.
McLennen JG: Lessons learned after second-look arthroscopy in type III fractures of the tibial spine. J Pediatr Orthop 1995;15:59-62.
Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
72 • American Academy of Orthopaedic Surgeons
DISCUSSION: The child has a type III tibial spine avulsion fracture. When the avulsed fragment is completely displaced, the preferred treatment is open or arthroscopic reduction of the fragment and internal fixation with sutures or screws. Type I fractures are nondisplaced and can be treated with a long leg cast; type II fractures are hinged and can be treated in a long leg cast if closed reduction is successful. Many patients have some objective anterior cruciate ligament laxity after a tibial spine avulsion fracture; however, with adequate treatment most patients do not have symptomatic laxity.
REFERENCES: Mah JY, Adili A, Otsuka NY, et al: Follow-up study of arthroscopic reduction and fixation of type III tibial-eminence fractures. J Pediatr Orthop 1998; 18:475-477.
McLennen JG: Lessons learned after second-look arthroscopy in type III fractures of the tibial spine. J Pediatr Orthop 1995;15:59-62.
Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
72 • American Academy of Orthopaedic Surgeons
Question 16High Yield
You have a 25-year-old male patient who fell from a 20-foot wall and is brought in by EMS. His only complaint is severe left heel pain. After seeing the patient, you make your diagnosis and decided that non-operative treatment is the best option. When counseling your patient, what should you tell him is the most common complication of non-operative treatment for this injury?
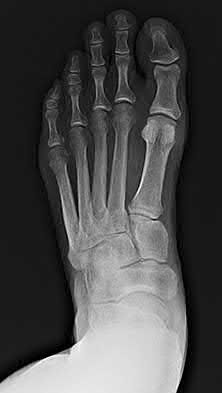


Explanation
Calcaneal fractures that are treated non-operatively most commonly will have associated subtalar arthritis.
Calcaneal fractures comprise 65% of tarsal bone fractures and require a significant amount of force to produce. The force of the calcaneus being pushed into the talus often results in post-traumatic arthritis. 75% of calcaneal fractures have an intra-articular extension, with the posterior facet being most
commonly affected. The treatment for severe post-traumatic arthritis of the subtalar joint is subtalar fusion.
Hsu et al. reviewed current methods of calcaneus surgical fixation. Previous L-shaped lateral approaches had high complication and infection rates postoperatively at 37% and 20% respectively. New methods including limited sinus tarsi, percutaneous fixation, and arthroscopic-assisted reduction. With these methods, there is decreased complication rates and less soft tissue injury.
Jackson et al. reviewed distraction subtalar arthrodesis. Calcaneal fractures often have a loss of height, which results in anterior impingement of the tibiotalar joint. Restoration of subtalar height can be done via open approach, use of a distractor to regain height and placement of graft to fill the void. With this method, there have been significant improvements in functional outcome scores and >90% patient satisfaction.
Buckley and Tough reviewed displaced intraarticular calcaneal fractures and factors that affect surgical outcomes. Smoking and workers compensation are risk factors for poor outcomes, while female gender and age less than 60 have better outcomes with surgical intervention. Heavy laborers have quicker return to work and lower incidence of late fusion. A Bohler's angle >15 predicts better fuctional outcomes in both surgical and nonsurgical patients. While Sanders II and III patients had better outcomes with surgery.
Figures A-C show the AP, oblique and lateral of the foot. On the lateral, you can see the intraarticular calcaneal fracture with depression of the posterior facet and loss of calcaneal pitch.
Incorrect answers:
Answer 1: Nonunion of calcaneal fractures is exceedingly rare.
Answer 3: Although associated with severely comminuted calcaneal fractures, foot compartment syndrome occurs in about 10% of patients.
Answer 4: Avascular necrosis is more associated with talar neck fractures than calcaneal fractures.
Answer 5: Calcaneal fractures typically develop a varus deformity due to the tuberosity fragment being pulled into varus.
Calcaneal fractures comprise 65% of tarsal bone fractures and require a significant amount of force to produce. The force of the calcaneus being pushed into the talus often results in post-traumatic arthritis. 75% of calcaneal fractures have an intra-articular extension, with the posterior facet being most
commonly affected. The treatment for severe post-traumatic arthritis of the subtalar joint is subtalar fusion.
Hsu et al. reviewed current methods of calcaneus surgical fixation. Previous L-shaped lateral approaches had high complication and infection rates postoperatively at 37% and 20% respectively. New methods including limited sinus tarsi, percutaneous fixation, and arthroscopic-assisted reduction. With these methods, there is decreased complication rates and less soft tissue injury.
Jackson et al. reviewed distraction subtalar arthrodesis. Calcaneal fractures often have a loss of height, which results in anterior impingement of the tibiotalar joint. Restoration of subtalar height can be done via open approach, use of a distractor to regain height and placement of graft to fill the void. With this method, there have been significant improvements in functional outcome scores and >90% patient satisfaction.
Buckley and Tough reviewed displaced intraarticular calcaneal fractures and factors that affect surgical outcomes. Smoking and workers compensation are risk factors for poor outcomes, while female gender and age less than 60 have better outcomes with surgical intervention. Heavy laborers have quicker return to work and lower incidence of late fusion. A Bohler's angle >15 predicts better fuctional outcomes in both surgical and nonsurgical patients. While Sanders II and III patients had better outcomes with surgery.
Figures A-C show the AP, oblique and lateral of the foot. On the lateral, you can see the intraarticular calcaneal fracture with depression of the posterior facet and loss of calcaneal pitch.
Incorrect answers:
Answer 1: Nonunion of calcaneal fractures is exceedingly rare.
Answer 3: Although associated with severely comminuted calcaneal fractures, foot compartment syndrome occurs in about 10% of patients.
Answer 4: Avascular necrosis is more associated with talar neck fractures than calcaneal fractures.
Answer 5: Calcaneal fractures typically develop a varus deformity due to the tuberosity fragment being pulled into varus.
Question 17High Yield
Figures 18a and 18b show the radiographs of a 13-year-old baseball player who sustained a patellar dislocation with an associated lateral femoral condyle fracture. What ligament is attached to this fragment?
Explanation
The anterior cruciate ligament is attached to a portion of the lateral femoral condyle. The posterior cruciate ligament attaches to the medial femoral condyle. The lateral collateral and oblique popliteal ligaments attach proximal to this fragment. The intermeniscal ligament attaches the anterior horns of the menisci.
REFERENCES: Jobe CM, Wright M: Anatomy of the knee, in Fu FH, Harner CD, Vince KG (eds): Knee Surgery. Baltimore, MD, Williams & Wilkins, 1994, pp 1-54.
Moore KL, Dalley AF: Lower limb, in Moore KL, Dalley AF (eds): Clinically Oriented Anatomy, ed 4. Philadelphia, PA, Lippincott, Williams & Wilkins, 1999, pp 503-664.
REFERENCES: Jobe CM, Wright M: Anatomy of the knee, in Fu FH, Harner CD, Vince KG (eds): Knee Surgery. Baltimore, MD, Williams & Wilkins, 1994, pp 1-54.
Moore KL, Dalley AF: Lower limb, in Moore KL, Dalley AF (eds): Clinically Oriented Anatomy, ed 4. Philadelphia, PA, Lippincott, Williams & Wilkins, 1999, pp 503-664.
Question 18High Yield
A 35-year-old woman presents with an elbow injury which includes a coronoid fracture involving more than 50%, a comminuted
radial head fracture, and an elbow dislocation. What is the most appropriate treatment?
radial head fracture, and an elbow dislocation. What is the most appropriate treatment?
Explanation
A terrible triad of the elbow includes dislocation of the elbow with associated fractures of the radial head and the coronoid process. Ring et al. stressed that these injuries are prone to complications and advised against resection of the radial head due to instability, and instead recommended a radial head replacement if too comminuted for ORIF. Coronoid fractures compromise elbow stability as well and require open reduction and internal fixation as with the lateral collateral ligament. McKee et al. showed stable elbows in 34/36 with mean Mayo elbow score of 88 when the standard protocol of coronoid ORIF, radial head repair/replacement, and LCL repair were employed.
Question 19High Yield
A 32-year-old woman has had pain and a visibly growing mass in the shoulder for 3 years but denies any history of trauma. Examination reveals a swollen, boggy shoulder mass. The AP radiograph and MRI scan are shown in Figures 20a and 20b. Figures 20c through 20e show a portion of the excised mass and the photomicrographs of the biopsy specimen. What is the most likely diagnosis?
Explanation
The radiographic findings are classic for synovial chondromatosis because of the small calcified opacities within the joint surrounding the synovium. The histologic findings show cartilaginous foci of metaplasia, which may be markedly cellular. However, unlike low-grade chondrosarcoma, it lacks cellular and nuclear pleomorphism.
REFERENCES: Murphy FP, Dahlin DC, Sullivan CR: Articular synovial chondromatosis. J Bone Joint Surg Am 1982;44:77-86.
Milgram JW: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801.
REFERENCES: Murphy FP, Dahlin DC, Sullivan CR: Articular synovial chondromatosis. J Bone Joint Surg Am 1982;44:77-86.
Milgram JW: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801.
Question 20High Yield
All of the following medications have been associated with an increased risk of osteoporosis EXCEPT:
Explanation
**
Numerous drugs are associated with an increased risk of osteoporosis in
adults, including oral corticosteroids, androgen-deprivation therapy, aromatase inhibitors, protease inhibitors, selective serotonin reuptake inhibitors,
prolactin-raising antiepileptic agents and many cytotoxic agents.
Additionally, a number of disease states are associated with osteoporosis, including endocrinopathies such as hyperparathyroidism, thyrotoxicosis and type I diabetes, hypogonadism, chronic glucocorticoid therapy, malnutrition, malabsorption states, chronic immobilization, rheumatoid arthritis, alcoholism, vitamin D deficiency, and multiple myeloma.
NSAIDs have not been shown to increase risk of osteoporosis.
Numerous drugs are associated with an increased risk of osteoporosis in
adults, including oral corticosteroids, androgen-deprivation therapy, aromatase inhibitors, protease inhibitors, selective serotonin reuptake inhibitors,
prolactin-raising antiepileptic agents and many cytotoxic agents.
Additionally, a number of disease states are associated with osteoporosis, including endocrinopathies such as hyperparathyroidism, thyrotoxicosis and type I diabetes, hypogonadism, chronic glucocorticoid therapy, malnutrition, malabsorption states, chronic immobilization, rheumatoid arthritis, alcoholism, vitamin D deficiency, and multiple myeloma.
NSAIDs have not been shown to increase risk of osteoporosis.
Question 21High Yield
A right-handed 24-year-old professional baseball player injured his left shoulder 6 weeks ago when he dove forward and landed hard with the arm extended. He reports that the shoulder “slipped out” and “went back in.” The shoulder did not need to be reduced. He now reports deep pain in the front of the shoulder when batting on either side and is hesitant to raise his left arm up over his head to catch a ball. Examination reveals no obvious deformities of the shoulder and a somewhat guarded, limited range of motion in all planes. Provocative tests for the rotator cuff and labrum are equivocal. MRI scans are shown in Figures 16a and 16b. What is the best course of action?
Explanation
A hard fall on an outstretched arm often results in injury to the glenoid labrum. A significant tear of the anterior/inferior labrum often leads to instability, pain, and mechanical symptoms of the shoulder. The MRI scan shows no obvious labral tear or Hill-Sachs lesion to suggest an anterior dislocation. Recent clinical studies have suggested that early stabilization of initial anterior dislocations may lead to better results than nonsurgical management in young, athletic patients. However, there are no data to support early surgery for anterior labral tears resulting from traumatic subluxation without dislocation. Initial treatment should consist of a short period of rest and immobilization, followed by a physical therapy rehabilitation program designed to restore motion, strength, and dynamic stability to the shoulder. If the athlete cannot return to play following nonsurgical management, surgical repair of the labrum, either through an open or arthroscopic approach, is indicated. There is no role for immediate thermal capsular shift in this setting.
REFERENCES: Abrams JS, Savoie FH III, Tauro JC, et al: Recent advances in the evaluation and treatment of shoulder instability: Anterior, posterior and multidirectional. Arthroscopy 2002;18:1-13.
DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
REFERENCES: Abrams JS, Savoie FH III, Tauro JC, et al: Recent advances in the evaluation and treatment of shoulder instability: Anterior, posterior and multidirectional. Arthroscopy 2002;18:1-13.
DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
Question 22High Yield
Four months after sustaining a severe crush injury to his dominant right hand, a 28-year-old man continues to report painless hand stiffness with limited grip strength. Initial and subsequent radiographs demonstrate no fracture. He has been treated with 12 weeks of supervised hand therapy without experiencing substantial improvement and has not received surgical treatment. An examination reveals no substantial hand swelling. There is a noteworthy limitation of proximal interphalangeal (PIP) flexion with the metacarpophalangeal (MP) joints in extension, with near-full PIP motion with the MP joints flexed. The most appropriate course of treatment is
Explanation
This patient has classic intrinsic tightness following a severe crush injury to the hand. It is possible that there has been an unrecognized compartment syndrome of the hand as a result of the trauma. An examination reveals findings consistent with intrinsic tightness with limited PIP flexion while the MP joints are fully extended, with greater PIP flexion with the MP joints flexed. Considering
that this patient’s condition has not improved with 12 weeks of supervised therapy, it is unlikely that further therapy will be of benefit. Because his stiffness is not associated with pain, complex regional pain syndrome is not a consideration. Extensor tenolysis is not an appropriate treatment option because the examination is not consistent with extensor tendon tightness. The most appropriate treatment consists of distal intrinsic releases followed by supervised hand therapy. Subtle degrees of intrinsic tightness are often missed, and a high index of suspicion must be maintained when patients describe weakness and stiffness following hand trauma.
RECOMMENDED READINGS
12. BUNNELL S. Ischaemic contracture, local, in the hand. J Bone Joint Surg Am. 1953 Jan;35-A(1):88-
101/. PubMed PMID: 13022710. View Abstract at PubMed
13. HARRIS C Jr, RIORDAN DC. Intrinsic contracture in the hand and its surgical treatment. J Bone Joint Surg Am. 1954 Jan;36-A(1):10-20. PubMed PMID: 13130583.Abstract at PubMed
14. Smith RJ. Balance and kinetics of the fingers under normal and pathological conditions. Clin Orthop Relat Res. 1974 Oct;(104):92-111. PubMed PMID: 4412165.Abstract at PubMed
that this patient’s condition has not improved with 12 weeks of supervised therapy, it is unlikely that further therapy will be of benefit. Because his stiffness is not associated with pain, complex regional pain syndrome is not a consideration. Extensor tenolysis is not an appropriate treatment option because the examination is not consistent with extensor tendon tightness. The most appropriate treatment consists of distal intrinsic releases followed by supervised hand therapy. Subtle degrees of intrinsic tightness are often missed, and a high index of suspicion must be maintained when patients describe weakness and stiffness following hand trauma.
RECOMMENDED READINGS
12. BUNNELL S. Ischaemic contracture, local, in the hand. J Bone Joint Surg Am. 1953 Jan;35-A(1):88-
101/. PubMed PMID: 13022710. View Abstract at PubMed
13. HARRIS C Jr, RIORDAN DC. Intrinsic contracture in the hand and its surgical treatment. J Bone Joint Surg Am. 1954 Jan;36-A(1):10-20. PubMed PMID: 13130583.Abstract at PubMed
14. Smith RJ. Balance and kinetics of the fingers under normal and pathological conditions. Clin Orthop Relat Res. 1974 Oct;(104):92-111. PubMed PMID: 4412165.Abstract at PubMed
Question 23High Yield
When the elbow is extended and an axial load is applied, what percent of stress distribution occurs across the ulnohumeral and radiohumeral articular surface, respectively?
Explanation
When load is applied to the wrist, most of the stress is absorbed by the radius. As the load is transferred through the forearm, the interosseous membrane transfers some of the load from the radius to the ulna. The load at the elbow is distributed with 40% at the ulnohumeral articulation and 60% at the radiohumeral articulation.
REFERENCES: Halls AA, Travill R: Transmission of pressure across the elbow joint. Anat Rec 1964;150:243.
Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000.
REFERENCES: Halls AA, Travill R: Transmission of pressure across the elbow joint. Anat Rec 1964;150:243.
Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000.
Question 24High Yield
A 65-year-old woman with type II diabetes mellitus (most recent Hgb A1C was 8.2) has had 3 days of left knee pain. Physical examination of the left knee reveals erythema, warmth and a large effusion. Range of motion is painful and limited to 30 degrees of flexion. She is found to be hypotensive and not responding to volume resuscitation. She requires phenylephrine to maintain Mean Arterial Pressure (MAP) of 70. ESR and CRP are elevated and Lactate is 3.1 mmol/L. What is the next best intervention for this patient’s treatment?
Explanation
The patient is demonstrating signs of septic shock. Administration of antibiotics should not be delayed. Aspirating the knee joint and obtaining blood cultures can be rapidly accomplished to obtain accurate specimens. This should be followed immediately by administration of broad spectrum IV antibiotics. Patients with septic shock can be identified with a clinical construct of sepsis with persisting hypotension requiring vasopressors to maintain mean arterial pressure (MAP) ≥ 65 mmHg and having a serum lactate level > 2mmol/L (18 mg/dL) despite adequate volume resuscitation. With these criteria, hospital mortality is in excess of 40%.
Question 25High Yield
A 65-year-old woman with an unstable C2 fracture undergoes posterior fixation with a C1 lateral mass and C2 pars screw technique. Pulsatile bleeding is encountered while placing the C1 screw, which was placed across both cortices. Which artery is most likely injured?
Explanation
General principles can be used as bunion surgery guidelines even though there is extensive debate on the topic. A distal metatarsal osteotomy is most appropriate for patients with mild deformity and no transfer metatarsalgia. A proximal osteotomy potentially can correct more severe deformities. A lapidus procedure, or tarsometatarsal fusion, provides the highest potential to correct deformity plus the advantage of stabilizing the first tarsometatarsal joint and limiting or eliminating transfer metatarsalgia. A first MTP fusion is most appropriate for patients with severe first MTP arthrosis.
RECOMMENDED READINGS
3. [Simsek S, Yigitkanli K, Turba UC, Comert A, Seçkin H, Tekdemir I, Elhan A.Safe zone for C1 lateral mass screws: anatomic and radiological study.Neurosurgery. 2009 Dec;65(6):1154-60; discussion 1160. doi:10.1227/01.NEU.0000351779.58845.62. ](http://www.ncbi.nlm.nih.gov/pubmed/19934975)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19934975)
4. [Murakami S, Mizutani J, Fukuoka M, Kato K, Sekiya I, Okamoto H, Abumi K, Otsuka T. Relationship between screw trajectory of C1 lateral mass screw and internal carotid artery. Spine (Phila Pa 1976). 2008 Nov 15;33(24):2581-5. doi:10.1097/BRS.0b013e318186b2fd. ](http://www.ncbi.nlm.nih.gov/pubmed/19011539)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19011539)
_**This is the last question of the exam.**_
_**GOOD LUCK**_
RECOMMENDED READINGS
3. [Simsek S, Yigitkanli K, Turba UC, Comert A, Seçkin H, Tekdemir I, Elhan A.Safe zone for C1 lateral mass screws: anatomic and radiological study.Neurosurgery. 2009 Dec;65(6):1154-60; discussion 1160. doi:10.1227/01.NEU.0000351779.58845.62. ](http://www.ncbi.nlm.nih.gov/pubmed/19934975)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19934975)
4. [Murakami S, Mizutani J, Fukuoka M, Kato K, Sekiya I, Okamoto H, Abumi K, Otsuka T. Relationship between screw trajectory of C1 lateral mass screw and internal carotid artery. Spine (Phila Pa 1976). 2008 Nov 15;33(24):2581-5. doi:10.1097/BRS.0b013e318186b2fd. ](http://www.ncbi.nlm.nih.gov/pubmed/19011539)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19011539)
_**This is the last question of the exam.**_
_**GOOD LUCK**_
Question 26High Yield
As the most direct and predictable preoperative diagnostiCtest for hip infection, the false-positive rate for hip aspiration is:
Explanation
Hip aspiration has a false-positive rate of 0% to 15%. Many authors have warned against its routine use before revision surgery
Question 27High Yield
Figures 14a through 14c are the MR images of a 72-year-old man who has had a slow-growing asymptomatic mass in his thigh for more than 5 years. Cytogenetic testing on the mass reveals a ring chromosome and MDM2 expression with no 12;16 translocation. What is the most likely diagnosis?

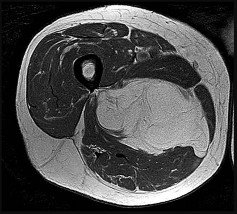
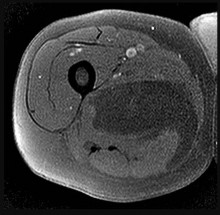
Explanation
This slowly growing mass has lipomatous features on MRI with a fat signal noted on T1 and T2 fat-suppressed images. Some thin striations seen on MRI may suggest an atypical lipomatous tumor. The molecular changes confirm that this is not a simple lipoma. High-grade sarcomas are generally rapidly growing and typically do not have the significant amount of largely homogenous fat signal as seen on this MRI. The negative result of a 12;16 translocation makes the diagnosis of myxoid liposarcoma unlikely. Atypical lipomas typically have a ring chromosome and express MDM2 but do not have the 12;16 translocation, as demonstrated in this patient. Atypical lipomas are synonymous with well-differentiated liposarcomas and pose risk for local recurrence but do not pose significant risk for metastatic spread.
RECOMMENDED READINGS
22. [Binh MB, Sastre-Garau X, Guillou L, de Pinieux G, Terrier P, Lagacé R, Aurias A, Hostein I, Coindre JM. MDM2 and CDK4 immunostainings are useful adjuncts in diagnosing well-differentiated and dedifferentiated liposarcoma subtypes: a comparative analysis of 559 soft tissue neoplasms with genetic data. Am J Surg Pathol. 2005 Oct;29(10):1340-7. PubMed PMID: 16160477. ](http://www.ncbi.nlm.nih.gov/pubmed/16160477)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/16160477)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16160477)
23. Dei Tos AP. Liposarcomas: diagnostic pitfalls and new insights. Histopathology. 2014 Jan;64(1):38-
[52/. doi: 10.1111/his.12311. Epub 2013 Dec 6. Review. PubMed PMID: 24118009. ](http://www.ncbi.nlm.nih.gov/pubmed/24118009)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/24118009)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24118009)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24118009)
24. [Iwasaki H, Ishiguro M, Nishio J, Aoki M, Yokoyama R, Yokoyama K, Taguchi K, Nabeshima K. Extensive lipoma-like changes of myxoid liposarcoma: morphologic, immunohistochemical, and molecular cytogenetic analyses. Virchows Arch. 2015 Apr;466(4):453-64. doi: 10.1007/s00428-015-1721-z. Epub 2015 Feb 4. PubMed PMID: 25650275. ](http://www.ncbi.nlm.nih.gov/pubmed/25650275)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25650275)
RECOMMENDED READINGS
22. [Binh MB, Sastre-Garau X, Guillou L, de Pinieux G, Terrier P, Lagacé R, Aurias A, Hostein I, Coindre JM. MDM2 and CDK4 immunostainings are useful adjuncts in diagnosing well-differentiated and dedifferentiated liposarcoma subtypes: a comparative analysis of 559 soft tissue neoplasms with genetic data. Am J Surg Pathol. 2005 Oct;29(10):1340-7. PubMed PMID: 16160477. ](http://www.ncbi.nlm.nih.gov/pubmed/16160477)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/16160477)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16160477)
23. Dei Tos AP. Liposarcomas: diagnostic pitfalls and new insights. Histopathology. 2014 Jan;64(1):38-
[52/. doi: 10.1111/his.12311. Epub 2013 Dec 6. Review. PubMed PMID: 24118009. ](http://www.ncbi.nlm.nih.gov/pubmed/24118009)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/24118009)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24118009)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24118009)
24. [Iwasaki H, Ishiguro M, Nishio J, Aoki M, Yokoyama R, Yokoyama K, Taguchi K, Nabeshima K. Extensive lipoma-like changes of myxoid liposarcoma: morphologic, immunohistochemical, and molecular cytogenetic analyses. Virchows Arch. 2015 Apr;466(4):453-64. doi: 10.1007/s00428-015-1721-z. Epub 2015 Feb 4. PubMed PMID: 25650275. ](http://www.ncbi.nlm.nih.gov/pubmed/25650275)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25650275)
Question 28High Yield
A 15-day-old boy presents with deformity of the right hand. The boy was delivered prematurely and underwent an urgent arterial switch for transposition of great vessels. The patient is in stable condition. He has a radial club hand, and because the radial head cannot be palpated, total absence of radius is suspected. The thumb is absent and the index finger has camptodactyly. The forearm is short compared to the left side, and the patient flexes his elbow upon stimulation. Spontaneous finger motion is also present. A thorough physical examination is performed and a set of investigations is ordered. The results are as follows: complete blood count 10,000 mcu/L; platelet 254×103 mcu/L; neutophils 50%; Hb 14.2 mg/dL; lymphocytes
40%; Hct 45; and monocytes 10%. No renal abnormalities were noted on ultrasonogram of the abdomen. A radiograph of the spine is normal.
C entralization will be performed on the patient. All of the following statements are true about centralization except:
40%; Hct 45; and monocytes 10%. No renal abnormalities were noted on ultrasonogram of the abdomen. A radiograph of the spine is normal.
C entralization will be performed on the patient. All of the following statements are true about centralization except:
Explanation
In a centralization procedure, the forearm is aligned with the third metacarpal, not the second.
Question 29High Yield
Hip pain of 1-month duration has developed in a 72-year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000
cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. What is this patient's
prognosis for infection resolution?
cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. What is this patient's
prognosis for infection resolution?
Explanation
---
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 30High Yield
Figures 1 through 3 are the MRI scans of a 26-year-old man who injured his knee wrestling one day prior. He has a moderate effusion, medial knee pain and an inability to extend his knee actively or passively. What is the most appropriate definitive treatment option?
Explanation
The images show a bucket handle medial meniscus tear, which is likely responsible for the block to motion. Therefore, surgery should be recommended with a meniscus repair if possible. Physical therapy or knee aspiration/manipulation under anesthesia is not the best definitive treatment.
Question 31High Yield
ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2B
ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2B
ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2B










































Explanation
This patient has a posterior knee dislocation with an ischemic limb that does not reverse following reduction. Emergent vascular exploration and reconstruction is indicated.
Knee dislocations are associated with popliteal artery injury in 18-45% of cases and range from intimal tears to complete transection. Amputation rates of 85% have been reported if revascularization is delayed greater than 6 to 8 hours.
Neurologic injury occurs in 15-40% of cases and is most common after posterolateral dislocation. The peroneal nerve is more commonly injured.
Rihn et al. reviewed the acutely dislocated knee. They recommend a vascular consult if pulses are weak, or ABI is compromised. They warn that in arterial injury, pulses, temperature and capillary refill can be normal. If the limb remains ischemic, surgical exploration and revascularization is indicated.
Medina et al. systematically reviewed neurovascular injury after knee dislocation in 862 patients. Vascular injury rate was 18%, and nerve injury rate was 25%. Repair was performed in 80% of vascular injuries, and amputation in 12%. The most vascular injury was seen in KDIIIL injuries (32%) and posterior dislocation (25%).
Figure A is an AP radiograph of a posterior knee dislocation. Figure B is a lateral showing the same injury.
Incorrect Answers:
: The limb remains ischemic. Splinting and observation alone are inappropriate.
Answer 3: External fixation is appropriate for immobilization following reduction, especially for very obese patients (BMI>50) where casting/splinting is not possible, and especially to protect a vascular reconstruction. However, the MOST important next step is vascular exploration to attempt revascularization.
Answers 4 and 5: CT angiography and standard angiography will only serve to delay vascular exploration of the ischemic limb. On-table angiograms will be performed during the surgery, obviating the need for preoperative angiography outside the operating room (OR).
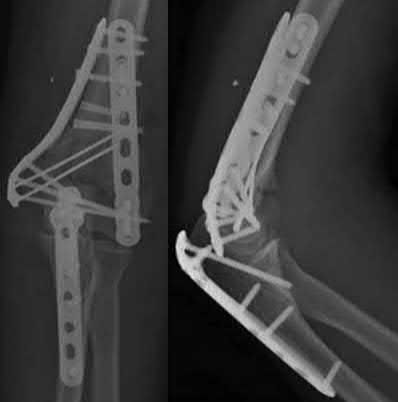
A 51-year-old carpenter presents with a distal humerus nonunion (Figures A and B). After repair of the nonunion, he is lost to follow up for 3 months and then presents to your clinic pain-free and with evidence of fracture union. On examination the elbow arc of motion is 10-80 degrees. Following a brief failed trial of conservative management, you recommend:
1) Open release of the posterior bundle of the MCL and excision of osteophytes
2) Complete open release of the MCL and LCL complexes with radiation for heterotopic ossification prophylaxis
3) Arthroscopic release of the anterior capsule with removal of hardware
4) Removal of hardware and dome osteotomy
5) Functional bracing and recommendation for job retraining
Limited flexion outside a functional range of motion (30-130 degrees) can be quite debilitating, and it is often addressed with open release of the posterior bundle of the MCL and posterior capsule and excision of osteophytes.
A frequent complication of distal humerus fractures is post-traumatic stiffness. This patient has had multiple procedures about the distal humerus, and the question stem implies that he did not complete a structured range of motion protocol following the repair of his nonunion. Beyond a trial of conservative management, there are many techniques described for capsule and soft tissue releases as well as bony resections if heterotopic ossification is present. This patient's severely limited flexion would best be addressed with a release of the posterior bundle of the MCL, and with flexion
A 51-year-old female presents with an acute inability to extend her thumb, four months after she was treated with cast immobilization for a minimally-displaced distal radius fracture. What is the most appropriate treatment at this time?
1) Occupational therapy for strengthening
2) Extensor carpi radialis longus transfer to extensor pollicus longus
3) Extensor pollicis brevis transfer to extensor pollicus longus
4) Extensor indicis proprius transfer to extensor pollicus longus
5) Primary repair of extensor pollicus longus
A rare complication of non-displaced or minimally displaced fractures of the distal radius treated with a cast is a delayed rupture of the extensor pollicis longus (EPL) tendon. The EPL is the primary extensor of the interphalangeal joint of the thumb and also assists with metacarpophalangeal extension.
Extensor indicis proprius transfer to the EPL is the most widely used and reported treatment for this condition.
Magnussen et al. reviewed results of EIP transfer following ruptures of the EPL, with 19/21 good results. None of the cases had any loss of independent index finger extension although index extensor strength reduced to half of that of the contralateral side.
Hove et al. reported a similar satisfaction rate following treatment of 15 patients. In his series of 4,400 distal radius fractures treated over a 5 year period, the incidence of delayed tendon rupture following distal radius fracture was 0.3 percent.
A 25-year-old female is involved in a motor vehicle collision. She presents with the isolated injury seen in Figures A through D. Her leg is swollen but her skin is intact. She has no clinical signs of compartment syndrome. Which of the following treatment options will allow for maintenance of fracture alignment and minimize the risk of soft tissue complications?
1) Closed reduction and long-leg non-weight bearing cast
2) Immediate open reduction of the tibia through an anterolateral approach
3) Percutaneous fixation of the articular surface and intramedullary nailing
4) Definitive uniplanar external fixator
5) Immediate open reduction of the tibia through an anteromedial approach
The patient presents with a closed distal third metaphyseal-diaphyseal distal tibia fracture with simple intra-articular extension. Immediate intramedullary nailing along with percutaneous fixation of the articular component provides appropriate restoration of length, rotation and alignment and minimizes the risk of wound complication.
Displaced distal third tibia fractures may be associated with simple intraarticular extension. Operative treatment of intra-articular distal tibia fractures has historically been performed with open reduction and internal fixation. Early open reduction and plate fixation of pilon fractures has been associated with high rates of infection and wound complication. In select patterns with simple articular extension, percutaneous screw fixation and medullary nailing may provide appropriate reduction with minimal soft-tissue risk.
Marcus et al. evaluated the outcomes of immediate intramedullary nailing and percutaneous fixation of simple intra-articular distal tibia fractures (AO/OTA 43 C1 and C2). The authors found excellent rates of union and alignment, however caution against broad application of this technique until more rigorous randomized studies can be performed.
Sirkin et al. retrospectively evaluated the results of a staged approach to management of intra-articular distal tibia fractures with temporary bridging external fixation followed by open reduction and internal fixation (ORIF). The authors found decreased rates of wound complication and infection compared with prior studies.
Figures A and B demonstrate a distal third tibial shaft fracture with simple intra-articular extension. The axial and coronal CT cuts in Figures C and D further clarify the articular injury. Illustrations A and B demonstrate a comminuted distal third tibial fracture with simple intra-articular extension. Illustrations C and D are fluoroscopic images of the same injury after intramedullary nailing and percutaneous fixation of the articular component.
Incorrect Answers:
Answer 1: Closed reduction and casting of this injury results in increased rates of malalignment
Answers 2 and 5: Immediate open reduction of pilon fractures has historically been associated with high rates of infection and wound complications
Answer 4: This fracture pattern would be difficult to control with a uniplanar fixator. A circular or multiplanar fixator would be a potential treatment option
A 24-year-old woman is thrown from her motorcycle and sustains the closed injury shown in Figures A through C. Open reduction and internal fixation is planned. What surgical technique will best allow visualization of the joint surface and allow early range of motion?
1) Bryan-Morrey approach and parallel plating
2) Triceps reflecting anconeus pedicle approach and parallel plating
3) Triceps reflecting anconeus pedicle approach and orthogonal plating on the posteromedial and lateral surfaces
4) Olecranon osteotomy and parallel plating
5) Olecranon osteotomy and orthogonal plating on the posteromedial and lateral surfaces
Access to complex intra-articular fractures is best achieved by an olecranon osteotomy (OO). Fixation can be with parallel plating or orthogonal plating.
Bicolumnar fixation of distal humerus fractures should follow the principles outlined by O'Driscoll: Distal fragments should be held by as many screws as possible; every screw in the distal fragments should pass through a plate; each screw should engage as many articular fragments as possible.
Galano et al. review treatment for bicolumnar distal humerus fractures. They note that the olecranon osteotomy, Alonso-Llames triceps sparing and Campbell triceps splitting approaches expose 57%, 46% and 35% of the articular surface, respectively. The OO and paratricipital (triceps sparing)
approaches allow for early ROM. Protected motion is required for the O'Driscoll TRAP and Bryan-Morrey approaches for tendon-to-bone healing.
Coles et al. retrospectively reviewed the OO in fixation of 70 fractures. Osteotomy fixation was with an intramedullary screw and dorsal ulnar wiring, or with a plate. The rate of OO increased with fracture difficulty (from AO type C1-C3). There was 1 delayed union but no nonunions.
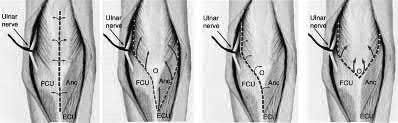
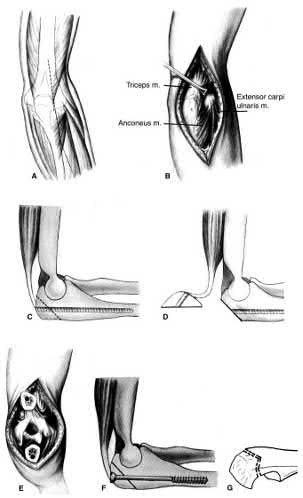
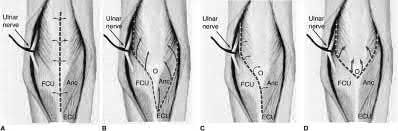
Figures A and B show a AO/OTA type C2 intraarticular distal humerus fracture. Figure C is a coronal CT scan showing intraarticular comminution. Illustration A shows fixation of the fracture with bicolumnar plating through an olecranon osteotomy approach. Illustration B shows the various approaches to the distal humerus (left, Campbell triceps splitting; center left, O'Driscoll triceps reflecting anconeus pedicle; center right, Bryan-Morrey approach, leaving the triceps attached laterally to the fasciocutaneous flap, but elevating it off the ulna; right, olecranon osteotomy). Illustration C shows 3 methods of olecranon osteotomy (A and B, Intra-articular transverse; C-F, Extra-articular oblique; G, Intra-articular chevron).
Incorrect Answers:
Answer 1: The Bryan-Morrey approach provides excellent medial exposure, but inadequate lateral exposure. The triceps is lifted subperiosteally, and the anconeus is released subperiosteally. Triceps repair depends on tendon-bone healing.
Answer 2: The O'Driscoll TRAP approach detaches triceps and anconeus from their distal insertions in a V-shaped flap that is reflected proximally. Repair to bone is via drill holes in the ulna. Early mobilization is not recommended.
Answers 3 and 5: Orthogonal plating is performed on the POSTEROLATERAL and MEDIAL surfaces.
A 31-year-old male sustains an isolated handgun injury shown in Figure A. On physical examination, he has a 0.5 cm wound over the anteromedial aspect of his thigh, with no gross contamination of the skin edges. He is neurovascularly intact. The patient has received tetanus prophylaxis and antibiotics in the emergency department.
What would next best step in treatment?
1) External fixation and IV antibiotics for 6 weeks
2) Irrigation and debridement of wound and external fixation for 6 weeks
3) Reamed antegrade or retrograde intramedullary nail
4) Irrigation and debridement of wound, reamed antegrade nail and IV antibiotics for 6 weeks
5) Irrigation and debridement of wound, reamed retrograde nail and IV antibiotics for 6 weeks
This patient has sustained a low-velocity gunshot to the right femoral diaphysis. The next best step in treatment would be insertion of a reamed antegrade or retrograde intramedullary nail. During surgery, the gunshot wound could be closed primarily if it was considered clean, or allowed to heal by secondary intention if it was there was any concern.
Low-velocity gunshot wounds are typically treated as closed fractures, since the risk of osteomyelitis is very low. These are typically bullets from handguns that travel 600 meters per second). The timing and direction (e.g. antegrade or retrograde) of nail insertion has not shown to
affect outcomes.
Cannada et al. reviewed 74 cases of femoral diaphyseal fractures caused by gunshots. All were treated with reamed, retrograde, statically locked intramedullary nailing, without formal irrigation and debridement in the operating room. Outcomes showed low incidence of shortening, angular deformity and infection rate.
Dougherty et al. compared retrograde vs. antegrade intramedullary nailing for the treatment of gunshot diaphyseal femur fractures. No significant differences were found between groups with regards to operative time, blood loss, or radiographic union. They conclude that immediate retrograde or antegrade nailing is safe for the early treatment of gunshot femur fractures.
Figure A shows an AP radiograph of the right femur. There is a gunshot fracture in the proximal femoral shaft with retained bullet fragments. The leg has been placed in temporary traction.
Incorrect Answers:
Answer 1: External fixation would be considered for treatment of femur fractures in damage control orthopaedics.
Answer 2: IV antibiotics for 6 weeks would not be necessary with low velocity gunshot wounds with clean wounds.
Answer 4 and 5: The direction of nail entry does not seem to affect outcomes with these fractures. Irrigation and debridement of wound, as well as IV antibiotics, wound not be necessary, aforementioned.
Figure A shows a radiograph of a 19-year-old male with an isolated shotgun injury. On physical examination, he has a 3 cm wound over the posterolateral aspect of his arm. In addition, he has weakness with wrist and finger extension, but no sensory deficits. The patient has received tetanus prophylaxis and antibiotics in the emergency department. What would be the next best steps in treatment?
1) Urgent open reduction internal fixation and fibular osteoseptocutaneous flap
2) Irrigation and debridement and external fixation
3) Irrigation and debridement, repair of the radial nerve and retrograde intramedullary nail
4) CT scan, urgent open reduction internal fixation and IV antibiotics for 6 weeks
5) Closed reduction, CT scan, immobilization in a coaptation splint
This patient has sustained a shotgun blast to the midshaft humerus. The next best step would be irrigation and debridement, and external fixation of the fracture.
Shotgun injuries are typically treated as open fractures, whereas low-energy gunshot wounds are treated as closed fractures. The initial operative treatment of shotgun wounds should include irrigation and debridement and stabilization with external fixation. The goal of treatment is to stabilize the severe soft-tissue injury and bone loss, as well as to aggressively debride devitalized tissue and gross contamination.
Dougherty et al. reviewed gunshot fractures to the humerus. They report that
peripheral nerve injuries are relatively common with these injuries, with a more common incidence in distal injuries than proximal.
Joshi et al. looked at low velocity gunshot fractures to the humerus. They found that these injuries can be safely treated as closed fractures with local wound care, fracture brace and oral antibiotics. The time to union was similar in the non-operative and open treatment group.
Berick et al. examined the indications for nerve exploration with humerus gunshot fractures. They recommend continued observation of isolated nerve palsies associated with gunshot fractures of the humerus. However, consider early nerve exploration of palsies when associated with a concomitant vascular injury.
Figure A shows a high velocity shotgun fracture to the left humerus with retained buck fragments. Illustration A shows a similar injury stabilized with external fixation.
Incorrect Answers:
Answer 1: Due to the severity of soft tissue injury, external fixation should be considered for initial stabilization. Vascularized fibular grafts has been expanded to an osteoseptocutaneous flap by including a cutaneous flap on the lateral aspect of the lower leg. These are not typically used in the acute setting.
Answer 3: Retrograde intramedullary nail would not be the ideal implant for this injury, acutely.
Answer 4 and 5: There is no indication for a CT scan or prolonged antibiotics. The fracture and soft-tissue injury should be initially stabilized with external fixation. Coaptation splinting will interfere with soft tissue care.
A 34-year-old male sustains the closed injury seen in Figure A as a result of a high-speed motor vehicle collision. What is the most appropriate next step in treatment?
1) Open reduction and internal fixation
2) Spanning external fixation
3) Percutaneous internal fixation
4) Closed reduction and cast placement
5) Ankle arthrodesis
The radiograph shows a comminuted pilon fracture, which is associated with high-energy trauma and significant soft tissue injury. The tested concept here is the importance of avoiding definitive reduction and fixation of this high-energy injury, which has been shown to be associated with an increased risk of wound complications and deep infections (as compared to staged treatment with usage of a spanning external fixator).
Patterson et al. reviewed 23 consecutive patients with comminuted distal tibia fractures. They showed 0% infections or wound-healing problems in their patient population treated with a two-staged protocol. Their protocol involved fibula fixation with an intramedullary implant and application of a medial external fixator to to regain length and restore anatomic alignment. Reevaluation of the limb occurred ten to fourteen days later for definitive fixation.
Sirkin et al. retrospectively reviewed 40 closed and 17 open pilon fractures (AO types 43A-C) that were treated with staged surgical management (avg. time from ext. fix. to formal reconstruction was 14 days (range 4 to 31) They reported 17% post-operative wound complication in the closed group and 11% post-operative wound complication in the open group (Gustilo Type I-III). They suggest the technique was successful in both closed and open pilon fractures.
A 72-year-old woman falls down stairs and sustains the injury shown in Figure A. Additional radiographs are performed in Figure B to help assess the fracture pattern. These additional radiographs represent which of the following?
1) Oblique radiographs
2) In-situ radiographs under anesthesia
3) Traction radiographs
4) Fracture flexion radiographs
5) Fracture extension radiographs
Additional traction radiographs are performed in distal humerus fractures to better understand the fracture configuration.
Traction radiographs help align the fracture fragments for better visualization. This is useful in comminuted fractures where distal fragments are telescoped or flexed on the proximal fragments, making CT scan visualization difficult.
Proper visualization can help determine (1) the approach to the distal humerus, (2) whether to perform ORIF or total elbow arthroplasty (in select patients), (3) whether to add a 3rd plate (lateral column), (4) whether to add tricortical bone graft to augment distal fixation and restore trochlear width.
Doornberg et al. examined whether 3D CT improved fracture characterization. They found that 3D CT improved interobserver and intraobserver reliability for fracture characterization and classification. It also improved intraobserver accuracy for fracture characteristics, but not interobserver accuracy. They concluded that 3D CT is helpful for preoperative planning.
Galano et al. reviewed treatment strategies for bicolumnar distal humerus fractures. They state that 3D CT compensates for oblique scans from formatting in an incorrect plane, and allows for subtraction of the radius/ulna to properly demonstrate articular incongruity, degree of comminution and column involvement.
Figures A and B show a distal humerus fracture without traction (A) and with traction (B) applied. Illustration A shows the same fracture after bicolumnar plating. Illustration B shows the different surgical approaches to the distal humerus (A, Campbell triceps splitting; B, O'Driscoll triceps reflecting anconeus pedicle [TRAP]; C, Bryan-Morrey triceps reflecting; D, olecranon osteotomy)
Incorrect Answers:
Answer 1: These radiographs aren't oblique images.
Answer 2: Radiographs under anesthesia do not add further information unless traction is applied.
Answers 4 and 5: Flexion and extension will further impact and displaced fragments and will not improve alignment.
Mirror therapy is indicated for which of the following clinical conditions?
1) Impaired proprioception after lower extremity injury
2) Two-stage flexor tendon reconstruction
3) Plumbism
4) Anterior cruciate ligament reconstruction
5) Phantom pain
Mirror therapy is a useful technique to improve phantom pain in amputees. Phantom limb pain is a painful sensation that is perceived within a body part that no longer exists.
Under mirror therapy, a patient is allowed to feel the imaginary movement of the removed body part behaving as normal body movement through a mirror. The mirror image of the normal body part helps reorganize and integrate the mismatch between proprioception and visual feedback of the amputated segment.
Tilak et al. performed a randomized controlled trial of 26 patients with phantom limb pain, and found that mirror therapy as well as transcutaneous electrical nerve stimulation both significantly improved pain scores, but no difference was seen between the two groups. They recommend use of both modalities in treatment of phantom limb pain, as they are noninvasive and inexpensive.
Chan et al. reviewed 22 patients utilizing mirror therapy for amputation related phantom limb pain, and found that patients reported a significant decrease in pain when utilizing this treatment modality as compared to covered mirror therapy or mental imagery therapy.
Illustration A shows a patient with an upper extremity amputation using a mirror to perform movements during a mirror therapy session.
Incorrect Answers:
Answer 1: Mirror therapy is not indicated for proprioception training. Answer 2: Mirror therapy is not indicated for flexor tendon injuries. Answer 3: Mirror therapy is not indicated for lead poisoning.
Answer 4: Mirror therapy is not indicated for ACL reconstruction.
A patient presents to the emergency department with the injury seen in Figure A. Which of the following is true about radial nerve palsies associated with isolated humeral shaft fractures after low velocity gunshot wounds?
1) The initial treatment involves debridement, irrigation, nerve exploration, and osteosynthesis.
2) The radial nerve palsy is often a result of neurotmesis.
3) Initial treatment involves splinting and observation for return of neurologic function.
4) Electrophysiologic testing for radial nerve palsies is indicated after 2-3 weeks without improvement.
5) The radial nerve palsy will not resolve regardless of attempted interventions.
When a patient sustains an isolated humeral shaft fracture and radial nerve palsy from a GSW, the initial treatment involves splinting with observation.
The majority of humeral shaft fractures are treated initially with a coaptation splint and then transitioned to a functional brace. Absolute surgical indications for operative management include: open fracture, brachial plexus injury, compartment syndrome, floating elbow, or vascular injury. A radial nerve palsy is not an indication for surgical management of an isolated humeral shaft fracture. Radial nerve injury from a low-velocity GSW is similar to that of blunt force trauma and thus, immediate exploration is not necessary. Instead, nerve function should be observed. Seventy percent of these nerve injuries will resolve spontaneously. Additionally, the patient should receive a short course of antibiotics as any low velocity GSW would be treated.
Guo et al retrospectively reviewed the electrophysiologic data for 40 radial nerve palsies caused by GSWs and blunt trauma. After characterizing the palsies by level of injury, completeness of nerve injury, and other associated nerves injured, they found there to be no difference in any of these variables between GSW induced radial nerve palsies and blunt trauma induced palsies.
Vaidya et al retrospectively reviewed the outcomes of 54 patients with humeral shaft fractures resulting from low velocity GSWs comparing operative and nonoperative treatments. They found that patients receiving non-operative management did well and that 70% of radial nerve palsies in the non-operative treatment group resolved on their own. They recommended non-operative treatment for the majority of isolated humeral shaft fractures resulting from civilian gunshot wounds.
Figure A is a radiograph of a humeral shaft fracture after a GSW. Illustration A is a radiograph of a humeral shaft fracture with a coaptation in place.
Illustration B is an example of a functional brace.
Incorrect answers:
Answer 1: This is the initial treatment for an open humeral shaft fracture associated with an radial nerve palsy.
Answer 2: Radial nerve palsy from a low velocity GSW is usually axonotmesis. Neurotmesis the most common injury in open fractures.
Answer 4:EMG testing is not indicated until 3-4 months of radial nerve palsy with no neural recovery.
Answer 5: Seventy percent of radial nerve palsies will spontaneously resolve
A 76-year-old male community ambulatory presented to clinic complaining of pain in the left groin that has been persistent for the last 8 months. Radiographs obtained from clinic are seen in Figure A. You suspect a femoral neck nonunion and obtain a CT scan which confirmed it. Which of the following statements is true?
1) Total hip arthroplasty will provide patient with the best long term outcomes
2) Valgus malreduction is closely correlated with failure of fixation after reduction and cannulated screw fixation
3) The patient's best outcome would be with an open reduction, bone grafting, and changing to an inverted triangle configuration of screws
4) The most appropriate treatment is a valgus osteotomy to correct malreduction
5) Providing this patient with a hemiarthroplasty increases rates of postoperative dislocation when comparing to total hip arthroplasty
A total hip arthroplasty (THA) after nonunion of a femoral neck fracture would provide the best long term outcomes in a 76-year-old male who is a community ambulator.
After nonunion of a femoral neck fracture, hemiarthroplasty and THA are good salvage option for the physiologically older patients. When deciding between these two options, THA is better for active and cognitively intact patients. THA is also indicated in patients with radiographic evidence of degenerative disease about the acetabulum. Hemiarthroplasty is advocated for patients who are older and less active.
Yang et al. retrospectively investigated the risk factors for nonunion in patients treated with cannulated screws. They reviewed 202 patients who had femoral neck fractures and were treated with internal fixation with cannulated screws. They identified that triangle configuration, displaced fracture, borderline or unacceptable reduction, and increased screw shaft subchondral purchase over the femoral neck were all risk factors for nonunion after internal fixation.
Inverted triangle configuration was found to increase rate of union.
Archibeck et al. retrospectively reviewed the outcomes of 102 THAs after failed internal fixation for a hip fracture (including both femoral neck and intertrochanteric). They concluded that the conversion of failed hip internal fixation has elevated risks compared to a primary THA, however, it may still be successful. The biggest concern for these patients postoperatively are periprosthetic fracture and dislocation.
Figures and Illustrations:
Figure A is an AP pelvic radiograph demonstrating a nonunion of a femoral neck fracture after suboptimal fixation with 3 cannulated screws in a triangle configuration.
Illustration A is an AP radiograph of the left hip in this patient following conversion to THA.
Illustration B is a radiograph demonstrating a valgus osteotomy. Illustration C shows an example of a femoral neck nonunion with varus malreduction.
Incorrect Answers:
Answer 2: Varus reduction is closely correlated with failure in this fixation method.
Answer 3: The patient's best outcome would be with THA.
Answer 4: This would be a good option in a younger patient, but given age and functional capacity, the best option is THA.
Answer 5: Patients with hemiarthroplasty have lower rates of dislocation.
A 22-year-old male cyclist was struck by a car. He complains of right knee pain and swelling, as well as reduced sensation and weakness in his right foot. His leg compartments are soft and not tender. Distal pulses in the extremity are palpable. Radiographs of the knee, as shown in Figures A and B, were taken after a closed reduction maneuver was performed. What would be the next best step in management of this patient?
1) Non-operative managment, but arrange for early follow-up in clinic
2) Intra-compartmental pressure measurements
3) Ankle-brachial index measurements
4) Knee spanning external fixation
5) Open reduction internal fixation
This patient presents with a Schatzker IV tibia plateau fracture with lower extremity neurologic deficits. The next best step would be to investigate for an acute vascular injury with ankle-brachial index measurements.
Fracture-dislocations of the knee must be suspected with all Schatzker type IV injuries as this fracture pattern is usually associated with high energy trauma. Identifying this injury should prompt a thorough assessment of the neurovascular structures across the knee. After closed reduction and emergent immobilization of the knee, ankle brachial indices (ABI) must be immediately performed. If
A 25-year-old woman sustains a fall on an outstretched hand. She complains of elbow pain. Examination reveals tenderness over the lateral elbow and pain on elbow motion. Injury radiographs and CT scans are shown in Figures A and B, respectively. What is the next best step?
1) Splint until swelling subsides, then long-arm cast
2) Excision of fracture fragments
3) Closed reduction and percutaneous pinning
4) Open reduction and internal fixation (ORIF)
5) Radial head replacement
This patient has Mason II radial head fracture. ORIF will give the best results.
Non-/minimally displaced radial head fractures without a block to rotation can be managed nonoperatively. Complete articular fractures with >=3 fragments do better with radial head replacement. Indications for ORIF include large articular surface fragments, > 2 mm of displacement, mechanical block to forearm rotation, or associated fractures or ligament injuries requiring surgery.
Pike et al. retrospectively compared patients undergoing ORIF for isolated radial head fractures with radial fractures associated with other fractures/dislocations. They found no differences in pain/disability and complications or secondary capsular release between groups.
Yoon et al. retrospectively compared isolated partial articular displaced (2-5mm) radial head fractures treated nonoperatively vs ORIF. They found no clinical benefit with ORIF compared to non-operative management. The ORIF
group had more complications. Younger patient age and larger fracture displacement favored operative intervention. Younger patients fared worse.
Figures A and B are radiographs and 3D reformatted CT images showing a displaced partial articular radial head fracture.
Incorrect Answers:
Answer 1: Nonoperative management is indicated for non-/minimally displaced fractures.
Answer 2: Excision is an option for small partial articular fragments = 3 fragments.
When placing an intramedullary nail for closed distal tibia shaft fractures, all of the following methods are described techniques to aid anatomic reduction EXCEPT:
1) Plating of a concomitant fibula fracture
2) Percutaneous placement of reduction foreceps at the fracture site
3) Placing a Poller screw
4) Placing a small-fragment plate at the fracture site
5) Placing syndesmotic fixation
Of the choices above, syndesmotic fixation would not help anatomically reduce these fractures.
Fractures of the distal tibia are challenging fractures to achieve an anatomic reduction. The medullary canals at either end of the tibia are capacious compared to the mid-diaphysis thus inhibiting an endosteal fit. These fractures have a tendency to become mal-aligned unless certain steps are taken to ensure restoration of the length, alignment, and rotation. Using a Poller or blocking screw can function to narrow the space available for the nail to guide the nail or correct deformity. The use of large pointed-reduction forceps or a small frag plate may also be used for provisional fixation. Additionally, plating concomitant fibula fractures may help indirectly restore length and reduce the tibia fracture. Concomitant syndesmotic injuries are not commonly seen and fixation for these is not required unless stress exam clearly demonstrates it.
Casstevens et al. reviewed the surgical management of distal tibia fractures using either plates/screws or intramedullary nails. Current literature shows near equivalence of either technique regarding union and alignment. They recommend treating each fracture on a case-by-case basis with consideration of the soft tissues and fracture pattern when determining fixation choices.
Tejwani et al. reviewed surgical techniques for managing metaphyseal and meta-diaphysial tibia fractures. Advances in tibial nail design have helped tremendously in negotiating these fractures. Though current supporting literature is based mostly on case series, the use of suprapatellar entry intramedullary nails may help avoid the common deformity of procurvatum and valgus seen with proximal tibia fractures.
Egol et al. retrospectively reviewed distal tibial shaft fracture undergoing intramedullary nailing, with and without concomitant fibula fracture plate fixation. They found fractures with fibular fixation maintained better alignment beyond 12 week post-operatively than those without fixation. Given these findings they recommended fibular plating for all distal tibial shaft fractures.
Illustration A shows a fibula fracture that was plated prior to tibia IMN placement. Illustrations B and C show the use of pointed reduction forceps placed percutaneously to reduce the fracture. Illustration D shows the use of a blocking screw (denoted by the arrow) to keep the nail lateralized and the fracture out of valgus. Illustration E shows the use of a plate to reduce the fracture prior to nail placement.
Incorrect Answers:
Answers 1, 2, 3, and 4: All of these have been described in the literature to help aid in reducing these fractures
A 70-year-old woman falls down a flight of stairs and sustains the injury shown in Figures A and B to her dominant upper extremity. She lives alone and has no other medical history. Which of the following surgical options is best to minimize complications for this fracture pattern?
1) Open reduction and internal fixation with a long locking plate
2) Uncemented reverse total shoulder arthroplasty with tuberosity repair
3) Cemented reverse total shoulder arthroplasty without tuberosity repair
4) Cemented reverse total shoulder arthroplasty with tuberosity repair
5) Proximal humeral resection with endoprosthetic replacement
This patient has a complex proximal humerus fracture with metaphyseal comminution and poor bone stock. Cemented reverse total shoulder arthroplasty (rTSA) using a long stem prosthesis and tuberosity repair is indicated.
Proximal humerus fragility fractures are hard to treat because of comminution and poor bone stock. AVN is common with glenohumeral fracture-dislocation. Hemiarthroplasty (and standard total shoulder arthroplasty, TSA) is unreliable because of dependence on tuberosity healing. rTSA is recommended for fractures in patients >70 years with severely comminuted fractures, high likelihood of head AVN, and poor tuberosity bone quality (osteoporosis or comminution).
Bufquin et al. retrospectively reviewed the use of rTSA for treatment of 43 patients with 3- and 4-part proximal humerus fractures. They found satisfactory elevation (97°), ER in abduction (30°), constant scores (44) and modified Constant scores (66%). Complications included calcification (90%), tuberosity displacement (53%) and scapular notching (25%). They concluded that rTSA was a good procedure because it provides pain relief and easier functional recovery in spite of failed tuberosity healing.
Anakwenze et al. systematically reviewed acute proximal humerus fractures. Frequency weighted range of motion was flexion 122°, abduction 97°, ER at neutral 18°. Tuberosity repair yielded higher ER compared to no repair.
Scapular notching was the most common complication (32%). They concluded that rTSA patients tended to be elderly women with 4-part fractures, had good pain control but residual dysfunction.
Jobin et al. reviewed rTSA for management of proximal humerus 3- and 4-part fractures. They note >50% of cases have tuberosity resorption. They recommend repairing the greater tuberosity to restore infraspinatus/teres minor function which improves external rotation strength. Greater tuberosity malunion is not a result of secondary displacement, but rather, from intraoperative malreduction. Lesser tuberosity repair should be performed if there is significant bone loss or intraoperative anterior instability.
Figures A and B are AP radiograph and 3D reformatted CT scan showing comminuted proximal humerus fracture dislocation. Illustration A shows rTSA performed with distal cementation of a long stem prosthesis and cerclage fixation of the proximal shaft and the tuberosity fragments.
Incorrect Answers:
Answer 1: ORIF has potential complications of screw cut out, AVN, fracture collapse, tuberosity resorption and loss of fixation. The risk of AVN (and resultant screw cut out) is high because of comminuted fracture-dislocation. Answer 2: Cementing is indicated because metaphyseal fracture bone loss compromises stem fixation.
Answer 3: Greater tuberosity repair improves external rotation strength. Lesser tuberosity repair adds to anterior stability.
Answer 5: Proximal humeral replacement is only necessary for tumor or unreconstructable fractures. They have poorer outcomes because of loss of rotator cuff function.
A 26-year-old male underwent statically locked intramedullary nail fixation for a comminuted left femur fracture. An early post-
operative computed tomography (CT) scanogram was taken to check rotational alignment, as shown in Figure A. What would be the next best step in the management of this patient?
1) Observation and close follow-up
2) Dynamization of the intramedullary nail
3) Revision surgery, internally rotate distal fragment by 19 degrees
4) Revision surgery, externally rotate distal fragment by 8 degrees
5) Revision surgery, internally rotate proximal fragment by 11 degrees
The CT scanogram shows the operative left femur is 8 degrees externally rotated compared to the native right femur. No correction is required unless malalignment is >15 degrees and symptomatic. Therefore, the most appropriate next step would be to continue with postoperative observation and close follow-up.
The primary purpose of CT scanogram is to measure the angle of rotation of the femoral neck relative to the femoral condyle. To do this, the right and left femurs must be scanned together using a 5mm helical slice scanner at the hip and knee. The first slice should reveal the alignment of the femoral neck, so as to allow for measurement of the femoral neck-to-horizontal (FNH) angle. The second slice should reveal the alignment of the posterior femoral condyles.
This allows measurement of the posterior condyle-to-horizontal (PCH) angle. Finally, to calculate the rotational alignment (RA), the FNH angle and PCH angles are subtracted (e.g., RA = FNH - PCH). Normal RA is usually +5 to +20 degrees, which is also referred to as 5 to 20 degrees of femoral anteversion.
Lindsey et al. reviewed femoral malrotation following intramedullary nail fixation. They showed the incidence of rotational malalignment was ~28%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is ~11-13°. However, they noted that some patients have up to 15° difference in rotation in native limbs.
Therefore 15 degrees and symptomatic.
Which of the following images shows an injury pattern most consistent with a lateral compression type 3 pelvic ring injury?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Figure C is an axial CT scan of a lateral compression type 3 (LC3) pelvic ring injury.
Classically, LC3 injuries demonstrate an ipsilateral lateral compression and a contralateral APC (windswept pelvis) fracture pattern. The most common mechanism of injury in these cases is a rollover MVC or pedestrian vs. auto. LC1 injuries are characterized by an oblique or transverse ramus fracture and ipsilateral anterior sacral ala compression fracture, while LC2 injuries consist of a rami fracture and ipsilateral posterior ilium fracture dislocation (crescent fracture). While LC1 injuries can often initially be managed conservatively with protected weight-bearing and close observation, LC2 and LC3 pelvic ring injuries are almost universally operative.
Pennal et al. discuss a radiologic technique for assessing the forces producing pelvic disruption and its use in logically classifying pelvic injury. Based on this radiologic assessment and along with some biomechanical studies, they propose a classification system involving three major forces producing injury that can also be helpful in the management of these patients.
Young et al. performed a retrospective analysis of the plain radiographs of 142 cases of pelvic fractures and identified four patterns of force that presented with distinctive, recognizable radiographic appearances. They describe a classification system for pelvic fractures based on radiographic and clinical findings that correlates with associated injury to soft-tissue structures and enables the surgeon to begin corrective procedures rapidly.
Incorrect Answers:
Answer 1: This represents a lateral compression type 2 injury. Answer 2: This represents a lateral compression type 1 injury.
Answer 4: This represents an anterior posterior compression type 2 injury. Answer 5: This represents an anterior posterior compression type 3 injury.
For a patient with an unstable pelvic fracture, the amount of blood tranfusions required in the first 24 hours has shown to be most predictive for what variable?
1) Length of hospital stay
2) Association with neurological deficit(s)
3) Length of intensive care stay
4) Cardiac collapse
5) Mortality
Unstable pelvic fractures can be devastating injuries often resulting in significant morbidity and even death.
According to the referenced study by Smith et al, fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased ISS or RTS scores. Deaths were most commonly from exsanguination (24 hours).
Incorrect Answers: Choices 1-4 do not correlate with increased blood transfusions to the extent of Option 5.
A healthy 27 year-old-male is brought into the emergency department after a fall from height. He has a suspected left C8-T1 nerve injury. Which of the following findings would most suggest a root avulsion injury rather than a brachial plexus injury at this level?
1) Reduced radial artery pulse
2) Double break in the ipsilateral superior shoulder suspensory complex
3) Elevated hemidiaphragm
4) Musculocutaneous nerve deficit
5) Drooping of the left eyelid
Drooping of the left eyelid is a presenting feature of Horner's syndrome. Horner's syndrome represents a disruption of the sympathetic chain via C8 and/or T1 root avulsion after trauma.
Brachial plexus injuries are often classified as preganglionic vs. postganglionic injuries. Preganglionic injuries are typically avulsion injuries proximal to the dorsal root ganglion. Clinical features suggestive of lower root avulsion injury include a person falling from height clutching on object to save himself, Horner’s syndrome (drooping of the eyelid (ptosis), pupillary constriction (miosis) and anhidrosis), absence of a Tinel sign or tenderness to percussion in the neck, and a normal histamine test (C8-T1 sympathetic ganglion - intact triple response (redness, wheal, flare)).
Caporrino et al. reviewed 102 patients to assess the best modality (e.g. physical examination, MRI and nerve conduction studies [NCSs]) for diagnosing and localizing brachial plexus injuries. They found the best diagnostic performance with physical examination (sensitivity = 97.8%; specificity = 30.8%) and NCSs (sensitivity = 98.9%; specificity = 23.1%). MRI had inferior performance for all measurements. They conclude that NCSs exhibited superior performance to MRI, and should be considered a more reliable supporting tool after detailed physical examination.
Incorrect Answers:
Answer 1, 2: The superior shoulder suspensory complex (SSSC) is located in close proximity to the brachial plexus. Disruption of the SSSC may affect the local anatomy and cause local brachial plexus or vascular injury.
Answer 3: Elevated hemidiaphragm (Phrenic nerve C3,4,5) may be suggestive an upper brachial plexus root avulsion, e.g. C5, C6 injury.
Answer 4: Musculocutaneous nerve deficiency (C5 deficiency) results in weakness to the biceps.
A 46-year-old competitive cyclist falls while racing and suffers an isolated fracture as seen in Figure A. He is positioned on a fracture table and a closed reduction maneuver is attempted, unsuccessfully.
Which of the following treatment plans is most appropriate?
1) Obtain a CT scan intraoperatively to reassess the quality of reduction
2) Perform additional closed reduction maneuvers until the reduction is adequate for percutaneous fixation
3) As long as the stepoff is less than 7mm in any plane of imaging, it is appropriate to proceed with percutaneous fixation
4) Perform an open reduction and internal fixation using a sliding hip screw
5) Perform an acute total hip arthroplasty through a direct anterior approach since the patient is on the fracture table
When standard closed reduction maneuvers using a traction table are unsuccessful, displaced femoral neck fracture in young adults (10 degrees varus/valgus or anteversion/retroversion) or has
significant displacement (5 mm or more in ANY view) is unacceptable, and an open reduction should be performed. Of course, this can be very difficult to assess in the operating room, where uncalibrated fluoroscopy with difficult to obtain tangential imaging is heavily relied upon to make this assessment.
Accordingly, when the quality of closed reduction is questionable, the best treatment plan is to obtain a better reduction with direct visualization of the femoral neck prior to fixation.
A systematic review of the literature by Pauyo, et al. cites numerous studies showing a higher incidence of osteonecrosis of the femoral head in patients with displaced femoral neck fractures treated with unsatisfactory reductions. Furthermore, performing multiple closed reduction attempts is also associated with a higher risk of osteonecrosis.
Upadhyay et al. performed a randomized controlled trial of 102 patients with femoral neck fractures treated with closed or open reductions, which were randomized. The groups had similar rates of nonunions and osteonecrosis of the femoral head; however, subanalysis revealed a "poor" reduction was the highest predictor of poor outcome, whether the reduction was attempted open or closed. Interestingly, the quality of reduction was more important than the implant used or the timing of surgery (including surgeries performed > 48h after injury).
Figure A shows a pre-operative AP x-ray of the patient's high-energy femoral neck fracture. Illustrations A and B are intraoperative fluoroscopic and postoperative CT scans of this same patient, highlighting that fluoroscopy may "hide" the degree of residual displacement.
Incorrect Answers:
Knee dislocations are associated with popliteal artery injury in 18-45% of cases and range from intimal tears to complete transection. Amputation rates of 85% have been reported if revascularization is delayed greater than 6 to 8 hours.
Neurologic injury occurs in 15-40% of cases and is most common after posterolateral dislocation. The peroneal nerve is more commonly injured.
Rihn et al. reviewed the acutely dislocated knee. They recommend a vascular consult if pulses are weak, or ABI is compromised. They warn that in arterial injury, pulses, temperature and capillary refill can be normal. If the limb remains ischemic, surgical exploration and revascularization is indicated.
Medina et al. systematically reviewed neurovascular injury after knee dislocation in 862 patients. Vascular injury rate was 18%, and nerve injury rate was 25%. Repair was performed in 80% of vascular injuries, and amputation in 12%. The most vascular injury was seen in KDIIIL injuries (32%) and posterior dislocation (25%).
Figure A is an AP radiograph of a posterior knee dislocation. Figure B is a lateral showing the same injury.
Incorrect Answers:
: The limb remains ischemic. Splinting and observation alone are inappropriate.
Answer 3: External fixation is appropriate for immobilization following reduction, especially for very obese patients (BMI>50) where casting/splinting is not possible, and especially to protect a vascular reconstruction. However, the MOST important next step is vascular exploration to attempt revascularization.
Answers 4 and 5: CT angiography and standard angiography will only serve to delay vascular exploration of the ischemic limb. On-table angiograms will be performed during the surgery, obviating the need for preoperative angiography outside the operating room (OR).
A 51-year-old carpenter presents with a distal humerus nonunion (Figures A and B). After repair of the nonunion, he is lost to follow up for 3 months and then presents to your clinic pain-free and with evidence of fracture union. On examination the elbow arc of motion is 10-80 degrees. Following a brief failed trial of conservative management, you recommend:
1) Open release of the posterior bundle of the MCL and excision of osteophytes
2) Complete open release of the MCL and LCL complexes with radiation for heterotopic ossification prophylaxis
3) Arthroscopic release of the anterior capsule with removal of hardware
4) Removal of hardware and dome osteotomy
5) Functional bracing and recommendation for job retraining
Limited flexion outside a functional range of motion (30-130 degrees) can be quite debilitating, and it is often addressed with open release of the posterior bundle of the MCL and posterior capsule and excision of osteophytes.
A frequent complication of distal humerus fractures is post-traumatic stiffness. This patient has had multiple procedures about the distal humerus, and the question stem implies that he did not complete a structured range of motion protocol following the repair of his nonunion. Beyond a trial of conservative management, there are many techniques described for capsule and soft tissue releases as well as bony resections if heterotopic ossification is present. This patient's severely limited flexion would best be addressed with a release of the posterior bundle of the MCL, and with flexion
A 51-year-old female presents with an acute inability to extend her thumb, four months after she was treated with cast immobilization for a minimally-displaced distal radius fracture. What is the most appropriate treatment at this time?
1) Occupational therapy for strengthening
2) Extensor carpi radialis longus transfer to extensor pollicus longus
3) Extensor pollicis brevis transfer to extensor pollicus longus
4) Extensor indicis proprius transfer to extensor pollicus longus
5) Primary repair of extensor pollicus longus
A rare complication of non-displaced or minimally displaced fractures of the distal radius treated with a cast is a delayed rupture of the extensor pollicis longus (EPL) tendon. The EPL is the primary extensor of the interphalangeal joint of the thumb and also assists with metacarpophalangeal extension.
Extensor indicis proprius transfer to the EPL is the most widely used and reported treatment for this condition.
Magnussen et al. reviewed results of EIP transfer following ruptures of the EPL, with 19/21 good results. None of the cases had any loss of independent index finger extension although index extensor strength reduced to half of that of the contralateral side.
Hove et al. reported a similar satisfaction rate following treatment of 15 patients. In his series of 4,400 distal radius fractures treated over a 5 year period, the incidence of delayed tendon rupture following distal radius fracture was 0.3 percent.
A 25-year-old female is involved in a motor vehicle collision. She presents with the isolated injury seen in Figures A through D. Her leg is swollen but her skin is intact. She has no clinical signs of compartment syndrome. Which of the following treatment options will allow for maintenance of fracture alignment and minimize the risk of soft tissue complications?
1) Closed reduction and long-leg non-weight bearing cast
2) Immediate open reduction of the tibia through an anterolateral approach
3) Percutaneous fixation of the articular surface and intramedullary nailing
4) Definitive uniplanar external fixator
5) Immediate open reduction of the tibia through an anteromedial approach
The patient presents with a closed distal third metaphyseal-diaphyseal distal tibia fracture with simple intra-articular extension. Immediate intramedullary nailing along with percutaneous fixation of the articular component provides appropriate restoration of length, rotation and alignment and minimizes the risk of wound complication.
Displaced distal third tibia fractures may be associated with simple intraarticular extension. Operative treatment of intra-articular distal tibia fractures has historically been performed with open reduction and internal fixation. Early open reduction and plate fixation of pilon fractures has been associated with high rates of infection and wound complication. In select patterns with simple articular extension, percutaneous screw fixation and medullary nailing may provide appropriate reduction with minimal soft-tissue risk.
Marcus et al. evaluated the outcomes of immediate intramedullary nailing and percutaneous fixation of simple intra-articular distal tibia fractures (AO/OTA 43 C1 and C2). The authors found excellent rates of union and alignment, however caution against broad application of this technique until more rigorous randomized studies can be performed.
Sirkin et al. retrospectively evaluated the results of a staged approach to management of intra-articular distal tibia fractures with temporary bridging external fixation followed by open reduction and internal fixation (ORIF). The authors found decreased rates of wound complication and infection compared with prior studies.
Figures A and B demonstrate a distal third tibial shaft fracture with simple intra-articular extension. The axial and coronal CT cuts in Figures C and D further clarify the articular injury. Illustrations A and B demonstrate a comminuted distal third tibial fracture with simple intra-articular extension. Illustrations C and D are fluoroscopic images of the same injury after intramedullary nailing and percutaneous fixation of the articular component.
Incorrect Answers:
Answer 1: Closed reduction and casting of this injury results in increased rates of malalignment
Answers 2 and 5: Immediate open reduction of pilon fractures has historically been associated with high rates of infection and wound complications
Answer 4: This fracture pattern would be difficult to control with a uniplanar fixator. A circular or multiplanar fixator would be a potential treatment option
A 24-year-old woman is thrown from her motorcycle and sustains the closed injury shown in Figures A through C. Open reduction and internal fixation is planned. What surgical technique will best allow visualization of the joint surface and allow early range of motion?
1) Bryan-Morrey approach and parallel plating
2) Triceps reflecting anconeus pedicle approach and parallel plating
3) Triceps reflecting anconeus pedicle approach and orthogonal plating on the posteromedial and lateral surfaces
4) Olecranon osteotomy and parallel plating
5) Olecranon osteotomy and orthogonal plating on the posteromedial and lateral surfaces
Access to complex intra-articular fractures is best achieved by an olecranon osteotomy (OO). Fixation can be with parallel plating or orthogonal plating.
Bicolumnar fixation of distal humerus fractures should follow the principles outlined by O'Driscoll: Distal fragments should be held by as many screws as possible; every screw in the distal fragments should pass through a plate; each screw should engage as many articular fragments as possible.
Galano et al. review treatment for bicolumnar distal humerus fractures. They note that the olecranon osteotomy, Alonso-Llames triceps sparing and Campbell triceps splitting approaches expose 57%, 46% and 35% of the articular surface, respectively. The OO and paratricipital (triceps sparing)
approaches allow for early ROM. Protected motion is required for the O'Driscoll TRAP and Bryan-Morrey approaches for tendon-to-bone healing.
Coles et al. retrospectively reviewed the OO in fixation of 70 fractures. Osteotomy fixation was with an intramedullary screw and dorsal ulnar wiring, or with a plate. The rate of OO increased with fracture difficulty (from AO type C1-C3). There was 1 delayed union but no nonunions.
Figures A and B show a AO/OTA type C2 intraarticular distal humerus fracture. Figure C is a coronal CT scan showing intraarticular comminution. Illustration A shows fixation of the fracture with bicolumnar plating through an olecranon osteotomy approach. Illustration B shows the various approaches to the distal humerus (left, Campbell triceps splitting; center left, O'Driscoll triceps reflecting anconeus pedicle; center right, Bryan-Morrey approach, leaving the triceps attached laterally to the fasciocutaneous flap, but elevating it off the ulna; right, olecranon osteotomy). Illustration C shows 3 methods of olecranon osteotomy (A and B, Intra-articular transverse; C-F, Extra-articular oblique; G, Intra-articular chevron).
Incorrect Answers:
Answer 1: The Bryan-Morrey approach provides excellent medial exposure, but inadequate lateral exposure. The triceps is lifted subperiosteally, and the anconeus is released subperiosteally. Triceps repair depends on tendon-bone healing.
Answer 2: The O'Driscoll TRAP approach detaches triceps and anconeus from their distal insertions in a V-shaped flap that is reflected proximally. Repair to bone is via drill holes in the ulna. Early mobilization is not recommended.
Answers 3 and 5: Orthogonal plating is performed on the POSTEROLATERAL and MEDIAL surfaces.
A 31-year-old male sustains an isolated handgun injury shown in Figure A. On physical examination, he has a 0.5 cm wound over the anteromedial aspect of his thigh, with no gross contamination of the skin edges. He is neurovascularly intact. The patient has received tetanus prophylaxis and antibiotics in the emergency department.
What would next best step in treatment?
1) External fixation and IV antibiotics for 6 weeks
2) Irrigation and debridement of wound and external fixation for 6 weeks
3) Reamed antegrade or retrograde intramedullary nail
4) Irrigation and debridement of wound, reamed antegrade nail and IV antibiotics for 6 weeks
5) Irrigation and debridement of wound, reamed retrograde nail and IV antibiotics for 6 weeks
This patient has sustained a low-velocity gunshot to the right femoral diaphysis. The next best step in treatment would be insertion of a reamed antegrade or retrograde intramedullary nail. During surgery, the gunshot wound could be closed primarily if it was considered clean, or allowed to heal by secondary intention if it was there was any concern.
Low-velocity gunshot wounds are typically treated as closed fractures, since the risk of osteomyelitis is very low. These are typically bullets from handguns that travel 600 meters per second). The timing and direction (e.g. antegrade or retrograde) of nail insertion has not shown to
affect outcomes.
Cannada et al. reviewed 74 cases of femoral diaphyseal fractures caused by gunshots. All were treated with reamed, retrograde, statically locked intramedullary nailing, without formal irrigation and debridement in the operating room. Outcomes showed low incidence of shortening, angular deformity and infection rate.
Dougherty et al. compared retrograde vs. antegrade intramedullary nailing for the treatment of gunshot diaphyseal femur fractures. No significant differences were found between groups with regards to operative time, blood loss, or radiographic union. They conclude that immediate retrograde or antegrade nailing is safe for the early treatment of gunshot femur fractures.
Figure A shows an AP radiograph of the right femur. There is a gunshot fracture in the proximal femoral shaft with retained bullet fragments. The leg has been placed in temporary traction.
Incorrect Answers:
Answer 1: External fixation would be considered for treatment of femur fractures in damage control orthopaedics.
Answer 2: IV antibiotics for 6 weeks would not be necessary with low velocity gunshot wounds with clean wounds.
Answer 4 and 5: The direction of nail entry does not seem to affect outcomes with these fractures. Irrigation and debridement of wound, as well as IV antibiotics, wound not be necessary, aforementioned.
Figure A shows a radiograph of a 19-year-old male with an isolated shotgun injury. On physical examination, he has a 3 cm wound over the posterolateral aspect of his arm. In addition, he has weakness with wrist and finger extension, but no sensory deficits. The patient has received tetanus prophylaxis and antibiotics in the emergency department. What would be the next best steps in treatment?
1) Urgent open reduction internal fixation and fibular osteoseptocutaneous flap
2) Irrigation and debridement and external fixation
3) Irrigation and debridement, repair of the radial nerve and retrograde intramedullary nail
4) CT scan, urgent open reduction internal fixation and IV antibiotics for 6 weeks
5) Closed reduction, CT scan, immobilization in a coaptation splint
This patient has sustained a shotgun blast to the midshaft humerus. The next best step would be irrigation and debridement, and external fixation of the fracture.
Shotgun injuries are typically treated as open fractures, whereas low-energy gunshot wounds are treated as closed fractures. The initial operative treatment of shotgun wounds should include irrigation and debridement and stabilization with external fixation. The goal of treatment is to stabilize the severe soft-tissue injury and bone loss, as well as to aggressively debride devitalized tissue and gross contamination.
Dougherty et al. reviewed gunshot fractures to the humerus. They report that
peripheral nerve injuries are relatively common with these injuries, with a more common incidence in distal injuries than proximal.
Joshi et al. looked at low velocity gunshot fractures to the humerus. They found that these injuries can be safely treated as closed fractures with local wound care, fracture brace and oral antibiotics. The time to union was similar in the non-operative and open treatment group.
Berick et al. examined the indications for nerve exploration with humerus gunshot fractures. They recommend continued observation of isolated nerve palsies associated with gunshot fractures of the humerus. However, consider early nerve exploration of palsies when associated with a concomitant vascular injury.
Figure A shows a high velocity shotgun fracture to the left humerus with retained buck fragments. Illustration A shows a similar injury stabilized with external fixation.
Incorrect Answers:
Answer 1: Due to the severity of soft tissue injury, external fixation should be considered for initial stabilization. Vascularized fibular grafts has been expanded to an osteoseptocutaneous flap by including a cutaneous flap on the lateral aspect of the lower leg. These are not typically used in the acute setting.
Answer 3: Retrograde intramedullary nail would not be the ideal implant for this injury, acutely.
Answer 4 and 5: There is no indication for a CT scan or prolonged antibiotics. The fracture and soft-tissue injury should be initially stabilized with external fixation. Coaptation splinting will interfere with soft tissue care.
A 34-year-old male sustains the closed injury seen in Figure A as a result of a high-speed motor vehicle collision. What is the most appropriate next step in treatment?
1) Open reduction and internal fixation
2) Spanning external fixation
3) Percutaneous internal fixation
4) Closed reduction and cast placement
5) Ankle arthrodesis
The radiograph shows a comminuted pilon fracture, which is associated with high-energy trauma and significant soft tissue injury. The tested concept here is the importance of avoiding definitive reduction and fixation of this high-energy injury, which has been shown to be associated with an increased risk of wound complications and deep infections (as compared to staged treatment with usage of a spanning external fixator).
Patterson et al. reviewed 23 consecutive patients with comminuted distal tibia fractures. They showed 0% infections or wound-healing problems in their patient population treated with a two-staged protocol. Their protocol involved fibula fixation with an intramedullary implant and application of a medial external fixator to to regain length and restore anatomic alignment. Reevaluation of the limb occurred ten to fourteen days later for definitive fixation.
Sirkin et al. retrospectively reviewed 40 closed and 17 open pilon fractures (AO types 43A-C) that were treated with staged surgical management (avg. time from ext. fix. to formal reconstruction was 14 days (range 4 to 31) They reported 17% post-operative wound complication in the closed group and 11% post-operative wound complication in the open group (Gustilo Type I-III). They suggest the technique was successful in both closed and open pilon fractures.
A 72-year-old woman falls down stairs and sustains the injury shown in Figure A. Additional radiographs are performed in Figure B to help assess the fracture pattern. These additional radiographs represent which of the following?
1) Oblique radiographs
2) In-situ radiographs under anesthesia
3) Traction radiographs
4) Fracture flexion radiographs
5) Fracture extension radiographs
Additional traction radiographs are performed in distal humerus fractures to better understand the fracture configuration.
Traction radiographs help align the fracture fragments for better visualization. This is useful in comminuted fractures where distal fragments are telescoped or flexed on the proximal fragments, making CT scan visualization difficult.
Proper visualization can help determine (1) the approach to the distal humerus, (2) whether to perform ORIF or total elbow arthroplasty (in select patients), (3) whether to add a 3rd plate (lateral column), (4) whether to add tricortical bone graft to augment distal fixation and restore trochlear width.
Doornberg et al. examined whether 3D CT improved fracture characterization. They found that 3D CT improved interobserver and intraobserver reliability for fracture characterization and classification. It also improved intraobserver accuracy for fracture characteristics, but not interobserver accuracy. They concluded that 3D CT is helpful for preoperative planning.
Galano et al. reviewed treatment strategies for bicolumnar distal humerus fractures. They state that 3D CT compensates for oblique scans from formatting in an incorrect plane, and allows for subtraction of the radius/ulna to properly demonstrate articular incongruity, degree of comminution and column involvement.
Figures A and B show a distal humerus fracture without traction (A) and with traction (B) applied. Illustration A shows the same fracture after bicolumnar plating. Illustration B shows the different surgical approaches to the distal humerus (A, Campbell triceps splitting; B, O'Driscoll triceps reflecting anconeus pedicle [TRAP]; C, Bryan-Morrey triceps reflecting; D, olecranon osteotomy)
Incorrect Answers:
Answer 1: These radiographs aren't oblique images.
Answer 2: Radiographs under anesthesia do not add further information unless traction is applied.
Answers 4 and 5: Flexion and extension will further impact and displaced fragments and will not improve alignment.
Mirror therapy is indicated for which of the following clinical conditions?
1) Impaired proprioception after lower extremity injury
2) Two-stage flexor tendon reconstruction
3) Plumbism
4) Anterior cruciate ligament reconstruction
5) Phantom pain
Mirror therapy is a useful technique to improve phantom pain in amputees. Phantom limb pain is a painful sensation that is perceived within a body part that no longer exists.
Under mirror therapy, a patient is allowed to feel the imaginary movement of the removed body part behaving as normal body movement through a mirror. The mirror image of the normal body part helps reorganize and integrate the mismatch between proprioception and visual feedback of the amputated segment.
Tilak et al. performed a randomized controlled trial of 26 patients with phantom limb pain, and found that mirror therapy as well as transcutaneous electrical nerve stimulation both significantly improved pain scores, but no difference was seen between the two groups. They recommend use of both modalities in treatment of phantom limb pain, as they are noninvasive and inexpensive.
Chan et al. reviewed 22 patients utilizing mirror therapy for amputation related phantom limb pain, and found that patients reported a significant decrease in pain when utilizing this treatment modality as compared to covered mirror therapy or mental imagery therapy.
Illustration A shows a patient with an upper extremity amputation using a mirror to perform movements during a mirror therapy session.
Incorrect Answers:
Answer 1: Mirror therapy is not indicated for proprioception training. Answer 2: Mirror therapy is not indicated for flexor tendon injuries. Answer 3: Mirror therapy is not indicated for lead poisoning.
Answer 4: Mirror therapy is not indicated for ACL reconstruction.
A patient presents to the emergency department with the injury seen in Figure A. Which of the following is true about radial nerve palsies associated with isolated humeral shaft fractures after low velocity gunshot wounds?
1) The initial treatment involves debridement, irrigation, nerve exploration, and osteosynthesis.
2) The radial nerve palsy is often a result of neurotmesis.
3) Initial treatment involves splinting and observation for return of neurologic function.
4) Electrophysiologic testing for radial nerve palsies is indicated after 2-3 weeks without improvement.
5) The radial nerve palsy will not resolve regardless of attempted interventions.
When a patient sustains an isolated humeral shaft fracture and radial nerve palsy from a GSW, the initial treatment involves splinting with observation.
The majority of humeral shaft fractures are treated initially with a coaptation splint and then transitioned to a functional brace. Absolute surgical indications for operative management include: open fracture, brachial plexus injury, compartment syndrome, floating elbow, or vascular injury. A radial nerve palsy is not an indication for surgical management of an isolated humeral shaft fracture. Radial nerve injury from a low-velocity GSW is similar to that of blunt force trauma and thus, immediate exploration is not necessary. Instead, nerve function should be observed. Seventy percent of these nerve injuries will resolve spontaneously. Additionally, the patient should receive a short course of antibiotics as any low velocity GSW would be treated.
Guo et al retrospectively reviewed the electrophysiologic data for 40 radial nerve palsies caused by GSWs and blunt trauma. After characterizing the palsies by level of injury, completeness of nerve injury, and other associated nerves injured, they found there to be no difference in any of these variables between GSW induced radial nerve palsies and blunt trauma induced palsies.
Vaidya et al retrospectively reviewed the outcomes of 54 patients with humeral shaft fractures resulting from low velocity GSWs comparing operative and nonoperative treatments. They found that patients receiving non-operative management did well and that 70% of radial nerve palsies in the non-operative treatment group resolved on their own. They recommended non-operative treatment for the majority of isolated humeral shaft fractures resulting from civilian gunshot wounds.
Figure A is a radiograph of a humeral shaft fracture after a GSW. Illustration A is a radiograph of a humeral shaft fracture with a coaptation in place.
Illustration B is an example of a functional brace.
Incorrect answers:
Answer 1: This is the initial treatment for an open humeral shaft fracture associated with an radial nerve palsy.
Answer 2: Radial nerve palsy from a low velocity GSW is usually axonotmesis. Neurotmesis the most common injury in open fractures.
Answer 4:EMG testing is not indicated until 3-4 months of radial nerve palsy with no neural recovery.
Answer 5: Seventy percent of radial nerve palsies will spontaneously resolve
A 76-year-old male community ambulatory presented to clinic complaining of pain in the left groin that has been persistent for the last 8 months. Radiographs obtained from clinic are seen in Figure A. You suspect a femoral neck nonunion and obtain a CT scan which confirmed it. Which of the following statements is true?
1) Total hip arthroplasty will provide patient with the best long term outcomes
2) Valgus malreduction is closely correlated with failure of fixation after reduction and cannulated screw fixation
3) The patient's best outcome would be with an open reduction, bone grafting, and changing to an inverted triangle configuration of screws
4) The most appropriate treatment is a valgus osteotomy to correct malreduction
5) Providing this patient with a hemiarthroplasty increases rates of postoperative dislocation when comparing to total hip arthroplasty
A total hip arthroplasty (THA) after nonunion of a femoral neck fracture would provide the best long term outcomes in a 76-year-old male who is a community ambulator.
After nonunion of a femoral neck fracture, hemiarthroplasty and THA are good salvage option for the physiologically older patients. When deciding between these two options, THA is better for active and cognitively intact patients. THA is also indicated in patients with radiographic evidence of degenerative disease about the acetabulum. Hemiarthroplasty is advocated for patients who are older and less active.
Yang et al. retrospectively investigated the risk factors for nonunion in patients treated with cannulated screws. They reviewed 202 patients who had femoral neck fractures and were treated with internal fixation with cannulated screws. They identified that triangle configuration, displaced fracture, borderline or unacceptable reduction, and increased screw shaft subchondral purchase over the femoral neck were all risk factors for nonunion after internal fixation.
Inverted triangle configuration was found to increase rate of union.
Archibeck et al. retrospectively reviewed the outcomes of 102 THAs after failed internal fixation for a hip fracture (including both femoral neck and intertrochanteric). They concluded that the conversion of failed hip internal fixation has elevated risks compared to a primary THA, however, it may still be successful. The biggest concern for these patients postoperatively are periprosthetic fracture and dislocation.
Figures and Illustrations:
Figure A is an AP pelvic radiograph demonstrating a nonunion of a femoral neck fracture after suboptimal fixation with 3 cannulated screws in a triangle configuration.
Illustration A is an AP radiograph of the left hip in this patient following conversion to THA.
Illustration B is a radiograph demonstrating a valgus osteotomy. Illustration C shows an example of a femoral neck nonunion with varus malreduction.
Incorrect Answers:
Answer 2: Varus reduction is closely correlated with failure in this fixation method.
Answer 3: The patient's best outcome would be with THA.
Answer 4: This would be a good option in a younger patient, but given age and functional capacity, the best option is THA.
Answer 5: Patients with hemiarthroplasty have lower rates of dislocation.
A 22-year-old male cyclist was struck by a car. He complains of right knee pain and swelling, as well as reduced sensation and weakness in his right foot. His leg compartments are soft and not tender. Distal pulses in the extremity are palpable. Radiographs of the knee, as shown in Figures A and B, were taken after a closed reduction maneuver was performed. What would be the next best step in management of this patient?
1) Non-operative managment, but arrange for early follow-up in clinic
2) Intra-compartmental pressure measurements
3) Ankle-brachial index measurements
4) Knee spanning external fixation
5) Open reduction internal fixation
This patient presents with a Schatzker IV tibia plateau fracture with lower extremity neurologic deficits. The next best step would be to investigate for an acute vascular injury with ankle-brachial index measurements.
Fracture-dislocations of the knee must be suspected with all Schatzker type IV injuries as this fracture pattern is usually associated with high energy trauma. Identifying this injury should prompt a thorough assessment of the neurovascular structures across the knee. After closed reduction and emergent immobilization of the knee, ankle brachial indices (ABI) must be immediately performed. If
A 25-year-old woman sustains a fall on an outstretched hand. She complains of elbow pain. Examination reveals tenderness over the lateral elbow and pain on elbow motion. Injury radiographs and CT scans are shown in Figures A and B, respectively. What is the next best step?
1) Splint until swelling subsides, then long-arm cast
2) Excision of fracture fragments
3) Closed reduction and percutaneous pinning
4) Open reduction and internal fixation (ORIF)
5) Radial head replacement
This patient has Mason II radial head fracture. ORIF will give the best results.
Non-/minimally displaced radial head fractures without a block to rotation can be managed nonoperatively. Complete articular fractures with >=3 fragments do better with radial head replacement. Indications for ORIF include large articular surface fragments, > 2 mm of displacement, mechanical block to forearm rotation, or associated fractures or ligament injuries requiring surgery.
Pike et al. retrospectively compared patients undergoing ORIF for isolated radial head fractures with radial fractures associated with other fractures/dislocations. They found no differences in pain/disability and complications or secondary capsular release between groups.
Yoon et al. retrospectively compared isolated partial articular displaced (2-5mm) radial head fractures treated nonoperatively vs ORIF. They found no clinical benefit with ORIF compared to non-operative management. The ORIF
group had more complications. Younger patient age and larger fracture displacement favored operative intervention. Younger patients fared worse.
Figures A and B are radiographs and 3D reformatted CT images showing a displaced partial articular radial head fracture.
Incorrect Answers:
Answer 1: Nonoperative management is indicated for non-/minimally displaced fractures.
Answer 2: Excision is an option for small partial articular fragments = 3 fragments.
When placing an intramedullary nail for closed distal tibia shaft fractures, all of the following methods are described techniques to aid anatomic reduction EXCEPT:
1) Plating of a concomitant fibula fracture
2) Percutaneous placement of reduction foreceps at the fracture site
3) Placing a Poller screw
4) Placing a small-fragment plate at the fracture site
5) Placing syndesmotic fixation
Of the choices above, syndesmotic fixation would not help anatomically reduce these fractures.
Fractures of the distal tibia are challenging fractures to achieve an anatomic reduction. The medullary canals at either end of the tibia are capacious compared to the mid-diaphysis thus inhibiting an endosteal fit. These fractures have a tendency to become mal-aligned unless certain steps are taken to ensure restoration of the length, alignment, and rotation. Using a Poller or blocking screw can function to narrow the space available for the nail to guide the nail or correct deformity. The use of large pointed-reduction forceps or a small frag plate may also be used for provisional fixation. Additionally, plating concomitant fibula fractures may help indirectly restore length and reduce the tibia fracture. Concomitant syndesmotic injuries are not commonly seen and fixation for these is not required unless stress exam clearly demonstrates it.
Casstevens et al. reviewed the surgical management of distal tibia fractures using either plates/screws or intramedullary nails. Current literature shows near equivalence of either technique regarding union and alignment. They recommend treating each fracture on a case-by-case basis with consideration of the soft tissues and fracture pattern when determining fixation choices.
Tejwani et al. reviewed surgical techniques for managing metaphyseal and meta-diaphysial tibia fractures. Advances in tibial nail design have helped tremendously in negotiating these fractures. Though current supporting literature is based mostly on case series, the use of suprapatellar entry intramedullary nails may help avoid the common deformity of procurvatum and valgus seen with proximal tibia fractures.
Egol et al. retrospectively reviewed distal tibial shaft fracture undergoing intramedullary nailing, with and without concomitant fibula fracture plate fixation. They found fractures with fibular fixation maintained better alignment beyond 12 week post-operatively than those without fixation. Given these findings they recommended fibular plating for all distal tibial shaft fractures.
Illustration A shows a fibula fracture that was plated prior to tibia IMN placement. Illustrations B and C show the use of pointed reduction forceps placed percutaneously to reduce the fracture. Illustration D shows the use of a blocking screw (denoted by the arrow) to keep the nail lateralized and the fracture out of valgus. Illustration E shows the use of a plate to reduce the fracture prior to nail placement.
Incorrect Answers:
Answers 1, 2, 3, and 4: All of these have been described in the literature to help aid in reducing these fractures
A 70-year-old woman falls down a flight of stairs and sustains the injury shown in Figures A and B to her dominant upper extremity. She lives alone and has no other medical history. Which of the following surgical options is best to minimize complications for this fracture pattern?
1) Open reduction and internal fixation with a long locking plate
2) Uncemented reverse total shoulder arthroplasty with tuberosity repair
3) Cemented reverse total shoulder arthroplasty without tuberosity repair
4) Cemented reverse total shoulder arthroplasty with tuberosity repair
5) Proximal humeral resection with endoprosthetic replacement
This patient has a complex proximal humerus fracture with metaphyseal comminution and poor bone stock. Cemented reverse total shoulder arthroplasty (rTSA) using a long stem prosthesis and tuberosity repair is indicated.
Proximal humerus fragility fractures are hard to treat because of comminution and poor bone stock. AVN is common with glenohumeral fracture-dislocation. Hemiarthroplasty (and standard total shoulder arthroplasty, TSA) is unreliable because of dependence on tuberosity healing. rTSA is recommended for fractures in patients >70 years with severely comminuted fractures, high likelihood of head AVN, and poor tuberosity bone quality (osteoporosis or comminution).
Bufquin et al. retrospectively reviewed the use of rTSA for treatment of 43 patients with 3- and 4-part proximal humerus fractures. They found satisfactory elevation (97°), ER in abduction (30°), constant scores (44) and modified Constant scores (66%). Complications included calcification (90%), tuberosity displacement (53%) and scapular notching (25%). They concluded that rTSA was a good procedure because it provides pain relief and easier functional recovery in spite of failed tuberosity healing.
Anakwenze et al. systematically reviewed acute proximal humerus fractures. Frequency weighted range of motion was flexion 122°, abduction 97°, ER at neutral 18°. Tuberosity repair yielded higher ER compared to no repair.
Scapular notching was the most common complication (32%). They concluded that rTSA patients tended to be elderly women with 4-part fractures, had good pain control but residual dysfunction.
Jobin et al. reviewed rTSA for management of proximal humerus 3- and 4-part fractures. They note >50% of cases have tuberosity resorption. They recommend repairing the greater tuberosity to restore infraspinatus/teres minor function which improves external rotation strength. Greater tuberosity malunion is not a result of secondary displacement, but rather, from intraoperative malreduction. Lesser tuberosity repair should be performed if there is significant bone loss or intraoperative anterior instability.
Figures A and B are AP radiograph and 3D reformatted CT scan showing comminuted proximal humerus fracture dislocation. Illustration A shows rTSA performed with distal cementation of a long stem prosthesis and cerclage fixation of the proximal shaft and the tuberosity fragments.
Incorrect Answers:
Answer 1: ORIF has potential complications of screw cut out, AVN, fracture collapse, tuberosity resorption and loss of fixation. The risk of AVN (and resultant screw cut out) is high because of comminuted fracture-dislocation. Answer 2: Cementing is indicated because metaphyseal fracture bone loss compromises stem fixation.
Answer 3: Greater tuberosity repair improves external rotation strength. Lesser tuberosity repair adds to anterior stability.
Answer 5: Proximal humeral replacement is only necessary for tumor or unreconstructable fractures. They have poorer outcomes because of loss of rotator cuff function.
A 26-year-old male underwent statically locked intramedullary nail fixation for a comminuted left femur fracture. An early post-
operative computed tomography (CT) scanogram was taken to check rotational alignment, as shown in Figure A. What would be the next best step in the management of this patient?
1) Observation and close follow-up
2) Dynamization of the intramedullary nail
3) Revision surgery, internally rotate distal fragment by 19 degrees
4) Revision surgery, externally rotate distal fragment by 8 degrees
5) Revision surgery, internally rotate proximal fragment by 11 degrees
The CT scanogram shows the operative left femur is 8 degrees externally rotated compared to the native right femur. No correction is required unless malalignment is >15 degrees and symptomatic. Therefore, the most appropriate next step would be to continue with postoperative observation and close follow-up.
The primary purpose of CT scanogram is to measure the angle of rotation of the femoral neck relative to the femoral condyle. To do this, the right and left femurs must be scanned together using a 5mm helical slice scanner at the hip and knee. The first slice should reveal the alignment of the femoral neck, so as to allow for measurement of the femoral neck-to-horizontal (FNH) angle. The second slice should reveal the alignment of the posterior femoral condyles.
This allows measurement of the posterior condyle-to-horizontal (PCH) angle. Finally, to calculate the rotational alignment (RA), the FNH angle and PCH angles are subtracted (e.g., RA = FNH - PCH). Normal RA is usually +5 to +20 degrees, which is also referred to as 5 to 20 degrees of femoral anteversion.
Lindsey et al. reviewed femoral malrotation following intramedullary nail fixation. They showed the incidence of rotational malalignment was ~28%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is ~11-13°. However, they noted that some patients have up to 15° difference in rotation in native limbs.
Therefore 15 degrees and symptomatic.
Which of the following images shows an injury pattern most consistent with a lateral compression type 3 pelvic ring injury?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Figure C is an axial CT scan of a lateral compression type 3 (LC3) pelvic ring injury.
Classically, LC3 injuries demonstrate an ipsilateral lateral compression and a contralateral APC (windswept pelvis) fracture pattern. The most common mechanism of injury in these cases is a rollover MVC or pedestrian vs. auto. LC1 injuries are characterized by an oblique or transverse ramus fracture and ipsilateral anterior sacral ala compression fracture, while LC2 injuries consist of a rami fracture and ipsilateral posterior ilium fracture dislocation (crescent fracture). While LC1 injuries can often initially be managed conservatively with protected weight-bearing and close observation, LC2 and LC3 pelvic ring injuries are almost universally operative.
Pennal et al. discuss a radiologic technique for assessing the forces producing pelvic disruption and its use in logically classifying pelvic injury. Based on this radiologic assessment and along with some biomechanical studies, they propose a classification system involving three major forces producing injury that can also be helpful in the management of these patients.
Young et al. performed a retrospective analysis of the plain radiographs of 142 cases of pelvic fractures and identified four patterns of force that presented with distinctive, recognizable radiographic appearances. They describe a classification system for pelvic fractures based on radiographic and clinical findings that correlates with associated injury to soft-tissue structures and enables the surgeon to begin corrective procedures rapidly.
Incorrect Answers:
Answer 1: This represents a lateral compression type 2 injury. Answer 2: This represents a lateral compression type 1 injury.
Answer 4: This represents an anterior posterior compression type 2 injury. Answer 5: This represents an anterior posterior compression type 3 injury.
For a patient with an unstable pelvic fracture, the amount of blood tranfusions required in the first 24 hours has shown to be most predictive for what variable?
1) Length of hospital stay
2) Association with neurological deficit(s)
3) Length of intensive care stay
4) Cardiac collapse
5) Mortality
Unstable pelvic fractures can be devastating injuries often resulting in significant morbidity and even death.
According to the referenced study by Smith et al, fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased ISS or RTS scores. Deaths were most commonly from exsanguination (24 hours).
Incorrect Answers: Choices 1-4 do not correlate with increased blood transfusions to the extent of Option 5.
A healthy 27 year-old-male is brought into the emergency department after a fall from height. He has a suspected left C8-T1 nerve injury. Which of the following findings would most suggest a root avulsion injury rather than a brachial plexus injury at this level?
1) Reduced radial artery pulse
2) Double break in the ipsilateral superior shoulder suspensory complex
3) Elevated hemidiaphragm
4) Musculocutaneous nerve deficit
5) Drooping of the left eyelid
Drooping of the left eyelid is a presenting feature of Horner's syndrome. Horner's syndrome represents a disruption of the sympathetic chain via C8 and/or T1 root avulsion after trauma.
Brachial plexus injuries are often classified as preganglionic vs. postganglionic injuries. Preganglionic injuries are typically avulsion injuries proximal to the dorsal root ganglion. Clinical features suggestive of lower root avulsion injury include a person falling from height clutching on object to save himself, Horner’s syndrome (drooping of the eyelid (ptosis), pupillary constriction (miosis) and anhidrosis), absence of a Tinel sign or tenderness to percussion in the neck, and a normal histamine test (C8-T1 sympathetic ganglion - intact triple response (redness, wheal, flare)).
Caporrino et al. reviewed 102 patients to assess the best modality (e.g. physical examination, MRI and nerve conduction studies [NCSs]) for diagnosing and localizing brachial plexus injuries. They found the best diagnostic performance with physical examination (sensitivity = 97.8%; specificity = 30.8%) and NCSs (sensitivity = 98.9%; specificity = 23.1%). MRI had inferior performance for all measurements. They conclude that NCSs exhibited superior performance to MRI, and should be considered a more reliable supporting tool after detailed physical examination.
Incorrect Answers:
Answer 1, 2: The superior shoulder suspensory complex (SSSC) is located in close proximity to the brachial plexus. Disruption of the SSSC may affect the local anatomy and cause local brachial plexus or vascular injury.
Answer 3: Elevated hemidiaphragm (Phrenic nerve C3,4,5) may be suggestive an upper brachial plexus root avulsion, e.g. C5, C6 injury.
Answer 4: Musculocutaneous nerve deficiency (C5 deficiency) results in weakness to the biceps.
A 46-year-old competitive cyclist falls while racing and suffers an isolated fracture as seen in Figure A. He is positioned on a fracture table and a closed reduction maneuver is attempted, unsuccessfully.
Which of the following treatment plans is most appropriate?
1) Obtain a CT scan intraoperatively to reassess the quality of reduction
2) Perform additional closed reduction maneuvers until the reduction is adequate for percutaneous fixation
3) As long as the stepoff is less than 7mm in any plane of imaging, it is appropriate to proceed with percutaneous fixation
4) Perform an open reduction and internal fixation using a sliding hip screw
5) Perform an acute total hip arthroplasty through a direct anterior approach since the patient is on the fracture table
When standard closed reduction maneuvers using a traction table are unsuccessful, displaced femoral neck fracture in young adults (10 degrees varus/valgus or anteversion/retroversion) or has
significant displacement (5 mm or more in ANY view) is unacceptable, and an open reduction should be performed. Of course, this can be very difficult to assess in the operating room, where uncalibrated fluoroscopy with difficult to obtain tangential imaging is heavily relied upon to make this assessment.
Accordingly, when the quality of closed reduction is questionable, the best treatment plan is to obtain a better reduction with direct visualization of the femoral neck prior to fixation.
A systematic review of the literature by Pauyo, et al. cites numerous studies showing a higher incidence of osteonecrosis of the femoral head in patients with displaced femoral neck fractures treated with unsatisfactory reductions. Furthermore, performing multiple closed reduction attempts is also associated with a higher risk of osteonecrosis.
Upadhyay et al. performed a randomized controlled trial of 102 patients with femoral neck fractures treated with closed or open reductions, which were randomized. The groups had similar rates of nonunions and osteonecrosis of the femoral head; however, subanalysis revealed a "poor" reduction was the highest predictor of poor outcome, whether the reduction was attempted open or closed. Interestingly, the quality of reduction was more important than the implant used or the timing of surgery (including surgeries performed > 48h after injury).
Figure A shows a pre-operative AP x-ray of the patient's high-energy femoral neck fracture. Illustrations A and B are intraoperative fluoroscopic and postoperative CT scans of this same patient, highlighting that fluoroscopy may "hide" the degree of residual displacement.
Incorrect Answers:
Question 32High Yield
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5° of angulation. When the MCP joint is flexed 30°, a radially directed stress produces 45° of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
Injuries to the ulnar collateral ligament of the MCP joint of the thumb commonly occur in recreational skiers. Historically, this injury has been referred to as “gamekeeper’s thumb.” The ligament consists of the proper collateral ligament and the more volar accessory collateral ligament. In extension, the accessory ligament is taut, and in flexion, the proper ligament is taut. For a complete tear of the ligament complex to occur, there must be laxity in full extension. Incomplete tears respond well to thumb spica splinting or casting for 2 to 3 weeks and gradual resumption of range of motion. Prolonged immobilization of incomplete injuries leads to higher rates of MCP joint stiffness.
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
Question 33High Yield
Left shoulder MR imaging results are shown in Figure 19 for a 22-year-old, right-hand-dominant collegiate athlete who reports a 6-month history of weakness in his right arm that first was noticed during weight training. He reports the weakness seems worse now than several months ago. He denies any specific traumatic event, has altered his weight-lifting activities, and has tried over-the-counter ibuprofen without experiencing any benefit. Upon examination of the bilateral upper extremities, there is no appreciable deformity or atrophy. He demonstrates full active shoulder range of motion, and there is no weakness with abduction in the plane of the scapula. Belly press test findings are normal, but there is weakness in external rotation with the arm in adduction. He does not demonstrate anterior apprehension, and there is no instability with load and shift testing. He has normal sensation and pulses to the upper extremity. A standard radiographic shoulder series yields unremarkable results. What is the best surgical option?
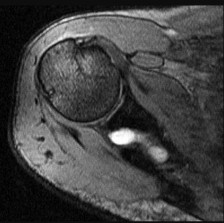
Explanation
This patient’s clinical and MR imaging findings are consistent with a posterior paralabral cyst with compression of the suprascapular nerve, specifically at the spinoglenoid notch. Compression of the suprascapular nerve can occur at either the suprascapular or spinoglenoid notch. Compression of the nerve at the suprascapular notch affects innervation to both the supraspinatus and infraspinatus muscles, resulting in weakness in both shoulder abduction and external rotation. However, compression at the spinoglenoid notch only affects innervation to the infraspinatus muscle, resulting in isolated weakness in external rotation.
Compression at the spinoglenoid notch often is seen in overhead athletes, and studies have shown associated posterior labral tears (Piatt and associates). Several studies have addressed nonsurgical and surgical treatment options. The treatment decision should focus on the underlying cause (Martin and associates)—in this patient, the cyst. Nonsurgical treatment in the presence of a known lesion has been associated with a higher failure rate than addressing the lesion, which can result in functional improvement (Chen and associates, Cummins and associates). The best response in this scenario is decompression of the cyst at the spinoglenoid notch with possible labral repair.
RECOMMENDED READINGS
7. [Piasecki DP, Romeo AA, Bach BR Jr, Nicholson GP. Suprascapular neuropathy. J Am Acad Orthop Surg. 2009 Nov;17(11):665-76. Review. PubMed PMID: 19880677.](http://www.ncbi.nlm.nih.gov/pubmed/19880677)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19880677)
8. [Piatt BE, Hawkins RJ, Fritz RC, Ho CP, Wolf E, Schickendantz M. Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg. 2002 Nov-Dec;11(6):600-4. PubMed PMID: 12469086.](http://www.ncbi.nlm.nih.gov/pubmed/12469086)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12469086)
9. [Martin SD, Warren RF, Martin TL, Kennedy K, O'Brien SJ, Wickiewicz TL. Suprascapular neuropathy. Results of non-operative treatment. J Bone Joint Surg Am. 1997 Aug;79(8):1159-65. PubMed PMID: 9278075.](http://www.ncbi.nlm.nih.gov/pubmed/9278075)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9278075)
10. [Chen AL, Ong BC, Rose DJ. Arthroscopic management of spinoglenoid cysts associated with SLAP lesions and suprascapular neuropathy. Arthroscopy. 2003 Jul-Aug;19(6):E15-21. PubMed PMID: 12861219. ](http://www.ncbi.nlm.nih.gov/pubmed/12861219)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12861219)
11. [Cummins CA, Messer TM, Nuber GW. Suprascapular nerve entrapment. J Bone Joint Surg Am. 2000 Mar;82(3):415-24. Review. PubMed PMID: 10724234.](http://www.ncbi.nlm.nih.gov/pubmed/10724234)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10724234)
Compression at the spinoglenoid notch often is seen in overhead athletes, and studies have shown associated posterior labral tears (Piatt and associates). Several studies have addressed nonsurgical and surgical treatment options. The treatment decision should focus on the underlying cause (Martin and associates)—in this patient, the cyst. Nonsurgical treatment in the presence of a known lesion has been associated with a higher failure rate than addressing the lesion, which can result in functional improvement (Chen and associates, Cummins and associates). The best response in this scenario is decompression of the cyst at the spinoglenoid notch with possible labral repair.
RECOMMENDED READINGS
7. [Piasecki DP, Romeo AA, Bach BR Jr, Nicholson GP. Suprascapular neuropathy. J Am Acad Orthop Surg. 2009 Nov;17(11):665-76. Review. PubMed PMID: 19880677.](http://www.ncbi.nlm.nih.gov/pubmed/19880677)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19880677)
8. [Piatt BE, Hawkins RJ, Fritz RC, Ho CP, Wolf E, Schickendantz M. Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg. 2002 Nov-Dec;11(6):600-4. PubMed PMID: 12469086.](http://www.ncbi.nlm.nih.gov/pubmed/12469086)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12469086)
9. [Martin SD, Warren RF, Martin TL, Kennedy K, O'Brien SJ, Wickiewicz TL. Suprascapular neuropathy. Results of non-operative treatment. J Bone Joint Surg Am. 1997 Aug;79(8):1159-65. PubMed PMID: 9278075.](http://www.ncbi.nlm.nih.gov/pubmed/9278075)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9278075)
10. [Chen AL, Ong BC, Rose DJ. Arthroscopic management of spinoglenoid cysts associated with SLAP lesions and suprascapular neuropathy. Arthroscopy. 2003 Jul-Aug;19(6):E15-21. PubMed PMID: 12861219. ](http://www.ncbi.nlm.nih.gov/pubmed/12861219)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12861219)
11. [Cummins CA, Messer TM, Nuber GW. Suprascapular nerve entrapment. J Bone Joint Surg Am. 2000 Mar;82(3):415-24. Review. PubMed PMID: 10724234.](http://www.ncbi.nlm.nih.gov/pubmed/10724234)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10724234)
Question 34High Yield
A 50-year-old woman has had acute weakness in her dominant hand for 6 weeks. Before noticing the onset of weakness, she experienced several weeks of vague discomfort in her shoulder and forearm, generalized fatigue, and a low-grade fever. There is no history of trauma. An examination reveals weakness of thumb and index finger distal interphalangeal (DIP) joint flexion. Electrodiagnostic testing shows fibrillations and positive sharp waves in the flexor pollicis longus and index flexor digitorum profundus muscles. The next appropriate step is
Explanation
This clinical scenario describes anterior interosseous nerve (AIN) syndrome. Identifying factors include weakness of the muscles innervated by the AIN, which include the flexor pollicis longus, index flexor digitorum profundus, and pronator quadratus. The same findings are present when fascicles contributing to the AIN are affected more proximally in the median nerve or brachial plexus, at which the findings are referred to as pseudo-anterior interosseous syndrome.
AIN syndrome can be present following blunt or penetrating trauma. It can also be seen in the absence of trauma, in which case there may be a prodrome of upper extremity discomfort, generalized fatigue, and/or fever. Clinical findings include weakness of the thumb interphalangeal (IP) joint and index DIP joint flexion, sometimes referred to as the “Playboy bunny sign.” Pronator quadratus weakness is also present; however, there is uncertainty as to the validity of manual muscle testing in determining pronator quadratus weakness. Electrodiagnostic studies demonstrate evidence of denervation of the muscles supplied by the AIN.
In the setting of acute trauma exploration, decompression and repair of the AIN is indicated early. In the case of a spontaneous and sudden onset of symptoms, especially when associated with other indications of an inflammatory process, a viral or inflammatory neuritis is much more likely. In these cases, multiple studies demonstrate a high incidence of spontaneous resolution over 6 to 12 months. Although systemic corticosteroids may be of benefit in the case of inflammatory neuritis, there are no data to support their use and no data to support the use of AIN corticosteroid injection. Although surgical exploration is supported in the literature for patients who do not show improvement within 3 months of onset, immediate surgical exploration at 6 weeks is not indicated. Tendon transfers are indicated only if recovery fails to occur spontaneously or after surgical exploration of the AIN.
RECOMMENDED READINGS
12. Miller-Breslow A, Terrono A, Millender LH. Nonoperative treatment of anterior interosseous nerve paralysis. J Hand Surg Am. 1990 May;15(3):493-6. PubMed PMID: 2348073.
13. Chi Y, Harness NG. Anterior interosseous nerve syndrome. J Hand Surg Am. 2010 Dec;35(12):2078-
80/. doi: 10.1016/j.jhsa.2010.08.018. Epub 2010 Oct 20. PubMed PMID: 20961706.
14. Sood MK, Burke FD. Anterior interosseous nerve palsy. A review of 16 cases. J Hand Surg Br. 1997 Feb;22(1):64-8. PubMed PMID: 9061529.
AIN syndrome can be present following blunt or penetrating trauma. It can also be seen in the absence of trauma, in which case there may be a prodrome of upper extremity discomfort, generalized fatigue, and/or fever. Clinical findings include weakness of the thumb interphalangeal (IP) joint and index DIP joint flexion, sometimes referred to as the “Playboy bunny sign.” Pronator quadratus weakness is also present; however, there is uncertainty as to the validity of manual muscle testing in determining pronator quadratus weakness. Electrodiagnostic studies demonstrate evidence of denervation of the muscles supplied by the AIN.
In the setting of acute trauma exploration, decompression and repair of the AIN is indicated early. In the case of a spontaneous and sudden onset of symptoms, especially when associated with other indications of an inflammatory process, a viral or inflammatory neuritis is much more likely. In these cases, multiple studies demonstrate a high incidence of spontaneous resolution over 6 to 12 months. Although systemic corticosteroids may be of benefit in the case of inflammatory neuritis, there are no data to support their use and no data to support the use of AIN corticosteroid injection. Although surgical exploration is supported in the literature for patients who do not show improvement within 3 months of onset, immediate surgical exploration at 6 weeks is not indicated. Tendon transfers are indicated only if recovery fails to occur spontaneously or after surgical exploration of the AIN.
RECOMMENDED READINGS
12. Miller-Breslow A, Terrono A, Millender LH. Nonoperative treatment of anterior interosseous nerve paralysis. J Hand Surg Am. 1990 May;15(3):493-6. PubMed PMID: 2348073.
13. Chi Y, Harness NG. Anterior interosseous nerve syndrome. J Hand Surg Am. 2010 Dec;35(12):2078-
80/. doi: 10.1016/j.jhsa.2010.08.018. Epub 2010 Oct 20. PubMed PMID: 20961706.
14. Sood MK, Burke FD. Anterior interosseous nerve palsy. A review of 16 cases. J Hand Surg Br. 1997 Feb;22(1):64-8. PubMed PMID: 9061529.
Question 35High Yield
Patients with homocystinuria phenotypically resemble patients with:
Explanation
Patients with homocystinuria may phenotypically resemble patients with Marfan syndrome. Patients with homocystinuria and
Marfan syndrome are tall with long limbs, arachnodactyly, scoliosis, chest wall deformities, and lens dislocations.
Achondroplasia is characterized by short stature, frontal bossing, and rhizomelic shortening of the limbs. Larsen's syndrome is a disorder characterized by short stature and multiple joint dislocations.
Gaucher's disease is a lysosomal storage disease characterized by accumulation of cerebroside in cells of the reticuloendothelial system. As in patients with homocystinuria, patients with Gaucher's disease have osteoporosis, however, they do not develop any of the other phenotypic features seen in homocystinuria.
Noonan's syndrome effects boys and clinical features include short stature, a webbed neck, and cubitus valgus deformities.
Marfan syndrome are tall with long limbs, arachnodactyly, scoliosis, chest wall deformities, and lens dislocations.
Achondroplasia is characterized by short stature, frontal bossing, and rhizomelic shortening of the limbs. Larsen's syndrome is a disorder characterized by short stature and multiple joint dislocations.
Gaucher's disease is a lysosomal storage disease characterized by accumulation of cerebroside in cells of the reticuloendothelial system. As in patients with homocystinuria, patients with Gaucher's disease have osteoporosis, however, they do not develop any of the other phenotypic features seen in homocystinuria.
Noonan's syndrome effects boys and clinical features include short stature, a webbed neck, and cubitus valgus deformities.
Question 36High Yield
The pediatric service orders an MRI, and findings are unremarkable. Results from the tests ordered above are pending. The clinician should recommend
Explanation
- initiation of intravenous (IV) antibiotics.
Question 37High Yield
Figure 23 shows the radiograph of an elderly man who fell on his right arm. What is the most important determinate of a good outcome following this injury?
Explanation
Minimally displaced fractures of the proximal humerus have a good outcome if physical therapy is initiated within 2 weeks of the injury. Results are not affected by age, open reduction and internal fixation, or involvement of the greater tuberosity. Immobilization for longer than 3 weeks will often result in stiffness.
REFERENCES: Koval KJ, Gallagher MA, Marsicano JG, et al: Functional outcome after minimally displaced fractures of the proximal part of the humerus. J Bone Joint Surg Am 1997;79:203-207.
Hodgson SA, Mawson SJ, Stanley D: Rehabilitation after two-part fractures of the neck of the humerus. J Bone Joint Surg Br 2003;85:419-422.
REFERENCES: Koval KJ, Gallagher MA, Marsicano JG, et al: Functional outcome after minimally displaced fractures of the proximal part of the humerus. J Bone Joint Surg Am 1997;79:203-207.
Hodgson SA, Mawson SJ, Stanley D: Rehabilitation after two-part fractures of the neck of the humerus. J Bone Joint Surg Br 2003;85:419-422.
Question 38High Yield
A 2-year-old child refused to walk 3 days prior to being seen because of pain in the left hip. The pain has gradually subsided and the child is now walking. He is afebrile and has full motion of the hips. Laboratory studies show a normal CBC with differential and C-reactive protein. An ultrasound shows a joint effusion in the right hip. What is the most likely diagnosis?

Explanation
DISCUSSION: The most likely diagnosis is toxic synovitis, and the normal C-reactive protein supports that diagnosis. Juvenile inflammatory arthritis is extremely rare to present with hip involvement. The child most likely does not have a bacterial infection because he has improved rapidly without treatment. A normal CBC with differential precludes the diagnosis of leukemia.
REFERENCES: Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2068-2070.
Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between
**2010 Pediatric Orthopaedic Examination Answer Book • 11**
septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004:86:1629-1635.
**12 • American Academy of Orthopaedic Surgeons**
Figure 7a Figure 7b
REFERENCES: Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2068-2070.
Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between
**2010 Pediatric Orthopaedic Examination Answer Book • 11**
septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004:86:1629-1635.
**12 • American Academy of Orthopaedic Surgeons**
Figure 7a Figure 7b
Question 39High Yield
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
Coleman block testing, performed by placing an elevation under the lateral border of the foot, is used to determine if the forefoot and/or plantar flexed first ray is causing a compensatory varus in the hindfoot. The block is placed under the lateral border of the foot, and therefore does not have any relation to the Achilles tendon and suppleness of the hindfoot.
REFERENCES: Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
REFERENCES: Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 40High Yield
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient
is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. What is the most appropriate course of action for this patient’s condition?
is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. What is the most appropriate course of action for this patient’s condition?
Explanation
The anterior drawer test is performed with the ankle in 10° of plantar flexion, which results in the greatest amount of translation. The test investigates the integrity of the anterior talofibular ligament with a key distance of translation being 8 to 10 mm. While the patient is sitting and has her knees flexed over the edge of a table or bench, the physician uses one hand to stabilize the distal leg and with the other hand applies an anterior force to the heel in an attempt to gap the talus anteriorly from under the tibia. The anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The
diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization and a guided rehabilitation program that emphasizes proprioceptive stability.
diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization and a guided rehabilitation program that emphasizes proprioceptive stability.
Question 41High Yield
A 56-year-old man sustained a nondisplaced extra-articular fracture of the proximal aspect of the third metatarsal after dropping a heavy object on his left foot. Management should consist of
Explanation
This injury pattern is one of a direct trauma to the mid aspect of the foot. Without additional forces involved, capsular ligamentous injury is not anticipated; therefore, the injury should be a stable pattern. Treatment should consist of protected weight bearing as tolerated in a walking boot or walking cast. Surgical intervention with open reduction and internal fixation, percutaneous pinning, or open reduction and internal fixation with primary tarsometatarsal joint fusion is not indicated with this pattern of injury. The use of external bone stimulation in this acute fracture setting is not indicated. With injuries to the midfoot area where the exact mechanism of injury is uncertain, there should be a high index of suspicion for an associated injury to the tarsometatarsal joint, and standing radiographs or stress radiographs should be obtained.
REFERENCES: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Early JS: Fractures and dislocations of the midfoot and forefoot, in Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 2181-2245.
REFERENCES: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Early JS: Fractures and dislocations of the midfoot and forefoot, in Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 2181-2245.
Question 42High Yield
A 29-year-old man reports severe knee instability and popliteal pain. History reveals that he had polio of the left lower extremity as a child and has been brace-free his entire life. Examination reveals that he walks with 40° of knee hyperextension and has a fixed ankle equinus deformity of 30° . He has no active motors about the knee or ankle. Which of the following methods will provide knee stability and pain relief?
Explanation
The ankle equinus allows the patient to keep his weight-bearing line anterior to the axis of the hyperextended knee joint. With time, pain has developed because of continued stretching and now incompetence of the posterior capsule of the knee joint. Several soft-tissue and bony procedures have been designed to provide knee stability in this situation; however, the results have been either short-lived or inconsistent. Tenodeses, capsular plications, and bony blocks have had limited success and generally fail over time. Current orthotic technology makes soft-tissue release and orthotic control the most predictable option. To decrease the hyperextension moment on the knee joint, the ankle deformity also must be corrected. The most predictable method of achieving stability and diminished pain during walking is with soft-tissue release of the ankle and a knee-ankle-foot orthosis with a locked ankle and drop-lock knee joint.
REFERENCE: Michael JW: Lower limb orthoses, in Goldberg B, Hsu JD (eds): Atlas of Orthoses and Assistive Devices. St Louis, MO, Mosby, 1997, pp 209-224.
REFERENCE: Michael JW: Lower limb orthoses, in Goldberg B, Hsu JD (eds): Atlas of Orthoses and Assistive Devices. St Louis, MO, Mosby, 1997, pp 209-224.
Question 43High Yield
A 6-year-old girl with osteogenesis imperfecta has severe bowing of both femurs. The family is interested in surgery to correct the condition. This method will give her the longest interval between procedures in the future:
Explanation
Telescoping or Bailey-Dubow rods are able to grow with the patient and maintain stabilization for a mean of 4 years between operations in growing children.
Without the addition of internal fixation, bowing is likely to resume.
Although a single rod is likely to provide current stability, bowing is likely to occur as the patient grows and the bone becomes longer than the rod.
Parallel rods do not interlock and are likely to splay and lose fixation.
There are no reports of large segment allograft replacement for diaphyses in osteogenesis imperfecta. In the absence of internal fixation, bowing is likely to resume as growth occurs.
Without the addition of internal fixation, bowing is likely to resume.
Although a single rod is likely to provide current stability, bowing is likely to occur as the patient grows and the bone becomes longer than the rod.
Parallel rods do not interlock and are likely to splay and lose fixation.
There are no reports of large segment allograft replacement for diaphyses in osteogenesis imperfecta. In the absence of internal fixation, bowing is likely to resume as growth occurs.
Question 44High Yield
In addition to MR imaging, what is the most appropriate additional radiographic study at this time?
Explanation
- Long-standing radiograph of the entire spine
Question 45High Yield
Figures 1 and 2 are the radiographs of a 48-year-old right-hand dominant man who reports progressive pain and stiffness of the elbow. He sustained a fracture dislocation 10 years ago, which was treated with surgical reconstruction. On examination, range of motion is from 40° extension to 110° flexion, with pain at end-range of motion, but no pain through mid-range. A previous corticosteroid injection temporarily improved his pain but did not improve range of motion. The patient elects to undergo an arthroscopic osteocapsular arthroplasty. What structures need to be addressed to improve elbow extension?
65
65
Explanation
The patient is young, active, and has evidence of post-traumatic elbow osteoarthritis. His motion is limited by capsular contracture and large osteophytes in the anterior and posterior compartments. He has failed nonoperative treatment, and surgery is indicated to improve his range of motion and function. Arthroscopic osteocapsular arthroplasty allows removal of impinging osteophytes and release of hypertrophied capsule and has been shown to be effective at relieving pain and improving motion in patients with mild to moderate osteoarthritis. Anterior capsular contracture and posterior bony impingement limit extension and must be addressed to improve motion. Posterior capsular contracture and anterior osteophytes limit flexion.
Question 46High Yield
A
B
C
Figures 30a through 30c are the radiograph and MR images of a 54-year-old woman who has severe leg pain with walking. Her treatment has included 12 weeks of
physical therapy, anti-inflammatory medications, and narcotic pain relievers, and she is interested in surgery. Minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) is recommended. When compared with open TLIF, MIS TLIF is associated with
B
C
Figures 30a through 30c are the radiograph and MR images of a 54-year-old woman who has severe leg pain with walking. Her treatment has included 12 weeks of
physical therapy, anti-inflammatory medications, and narcotic pain relievers, and she is interested in surgery. Minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) is recommended. When compared with open TLIF, MIS TLIF is associated with
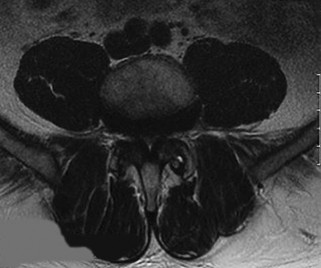


Explanation
MIS TLIF involves a steep learning curve but is associated with similar longterm outcomes as open TLIF, arguably comparable or possibly lower complication rates, and equivalent fusion rates. The major distinguishing feature comparing open to minimally invasive surgery for this and other spinal diagnoses has been shorter hospital stays.
RECOMMENDED READINGS
[Peng CW, Yue WM, Poh SY, Yeo W, Tan SB. Clinical and radiological outcomes of minimally invasive versus open transforaminal lumbar interbody fusion. Spine (Phila Pa 1976). 2009 Jun 1;34(13):1385-9. doi: 10.1097/BRS.0b013e3181a4e3be. PubMed PMID: 19478658. ](http://www.ncbi.nlm.nih.gov/pubmed/19478658)[View](http://www.ncbi.nlm.nih.gov/pubmed/19478658)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19478658)
Lee KH, Yue WM, Yeo W, Soeharno H, Tan SB. Clinical and radiological outcomes of open versus minimally invasive transforaminal lumbar interbody fusion. Eur Spine J. 2012 Nov;21(11):2265-70. doi: 10.1007/s00586-012-2281-4. Epub 2012 Mar 28. PubMed PMID:
[22453894/. ](http://www.ncbi.nlm.nih.gov/pubmed/22453894)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22453894)
[Lau D, Lee JG, Han SJ, Lu DC, Chou D. Complications and perioperative factors associated with learning the technique of minimally invasive transforaminal lumbar interbody fusion (TLIF). J Clin Neurosci. 2011 May;18(5):624-7. doi: 10.1016/j.jocn.2010.09.004. Epub 2011 Feb 23. PubMed PMID: 21349719. ](http://www.ncbi.nlm.nih.gov/pubmed/21349719)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21349719)
RECOMMENDED READINGS
[Peng CW, Yue WM, Poh SY, Yeo W, Tan SB. Clinical and radiological outcomes of minimally invasive versus open transforaminal lumbar interbody fusion. Spine (Phila Pa 1976). 2009 Jun 1;34(13):1385-9. doi: 10.1097/BRS.0b013e3181a4e3be. PubMed PMID: 19478658. ](http://www.ncbi.nlm.nih.gov/pubmed/19478658)[View](http://www.ncbi.nlm.nih.gov/pubmed/19478658)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19478658)
Lee KH, Yue WM, Yeo W, Soeharno H, Tan SB. Clinical and radiological outcomes of open versus minimally invasive transforaminal lumbar interbody fusion. Eur Spine J. 2012 Nov;21(11):2265-70. doi: 10.1007/s00586-012-2281-4. Epub 2012 Mar 28. PubMed PMID:
[22453894/. ](http://www.ncbi.nlm.nih.gov/pubmed/22453894)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22453894)
[Lau D, Lee JG, Han SJ, Lu DC, Chou D. Complications and perioperative factors associated with learning the technique of minimally invasive transforaminal lumbar interbody fusion (TLIF). J Clin Neurosci. 2011 May;18(5):624-7. doi: 10.1016/j.jocn.2010.09.004. Epub 2011 Feb 23. PubMed PMID: 21349719. ](http://www.ncbi.nlm.nih.gov/pubmed/21349719)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21349719)
Question 47High Yield
Figures 1 and 2 are the radiographs of a 64-year-old woman with a history of rheumatoid arthritis (RA) who complains of right elbow pain. She has been treated with tumor necrosis factor-alpha inhibitors and oral corticosteroids for several years. What process is primarily responsible for the radiographic joint destruction?
Explanation
RA is a systemic inflammatory disorder marked by erosive arthritis in multiple joints. Elbow involvement is common. The pathologic lesion in RA is pannus, a hyperplastic synovial proliferation that ultimately results in proteoglycan and collagen digestion. Rheumatoid factor mutations, traumatic insults resulting in complement activation, and osteoblast paracrine signaling are not involved in the pathologic process. The Larsen classification assesses the progression of rheumatoid changes in the elbow. Stage I is characterized by osteopenia without joint space narrowing. Stage II indicates joint space narrowing but a normal joint contour. Stage III is marked by joint space loss. This patient has stage IV disease, as seen by the advanced erosive changes with trochlear groove deepening and resulting deformity. Stage V is ankylosis.
68
68
Question 48High Yield
Figures 63a and 63b show the radiographs of a 38-year-old man who reports low back and bilateral lower extremity pain. The spondylolisthesis is best classified as which of the following?
Explanation
Spondylolisthesis can be classified into five types. Type I, dysplastic, occurs at the lumbosacral junction as a result of congenital abnormalities of the upper sacrum and/or the arch of L5.Type II, isthmic, refers to those involving a lesion in the pars interarticularis. Type IIA, lytic, represents fatigue fractures of the pars. Type IIB describes those with elongated, but intact pars. Type IIC describes those that are a result of an acute fracture of the pars. Type III, degenerative spondylolisthesis, results from longstanding intersegmental disease. Type IV, traumatic, refers to those resulting from fractures in regions other than the pars, such as the pedicles. Type V, pathologic, refers to spondylolisthesis resulting from generalized or local bone disease. The radiographs demonstrate type II, isthmic spondylolisthesis.
Question 49High Yield
Figure 68 is the radiograph of a 33-year-old runner who recently decided to begin running barefoot on trails. Since his transition to running without shoes 3 months ago, he has been having pain in the second metatarsophalangeal (MTP) joint. He feels like he is walking on a stone, notes edema in the ball of his foot, and has started to see a deviation of the second toe. What is the most likely etiology of these symptoms and findings?

Explanation
Lesser-toe plantar plate injuries are becoming increasingly recognized. Patients typically have an increase in pain, a positive Lachman test result upon examination, and deviation of the MTP joint. On radiograph, MTP subluxation can be appreciated. Nonsurgical treatment with a metatarsal pad may be attempted. Many patients who have surgery will have a partial or full tear of the plantar plate. The repair necessitates reinsertion of the plantar plate to the base of the proximal phalanx.
RECOMMENDED READINGS
[Doty JF, Coughlin MJ, Weil L Jr, Nery C. Etiology and management of lesser toe metatarsophalangeal joint instability. Foot Ankle Clin. 2014 Sep;19(3):385-405. doi: 10.1016/j.fcl.2014.06.013. Epub 2014 Jul 10. PubMed PMID: 25129351. ](http://www.ncbi.nlm.nih.gov/pubmed/25129351)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/25129351)[ ](http://www.ncbi.nlm.nih.gov/pubmed/25129351)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25129351)
Nery C, Coughlin MJ, Baumfeld D, Raduan FC, Mann TS, Catena F. Prospective evaluation of protocol for surgical treatment of lesser MTP joint plantar plate tears. Foot Ankle Int. 2014 Sep;35(9):876-85. doi: 10.1177/1071100714539659. Epub 2014 Jun 23. PubMed PMID:
[24958766/. ](http://www.ncbi.nlm.nih.gov/pubmed/24958766)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24958766)
[Chalayon O, Chertman C, Guss AD, Saltzman CL, Nickisch F, Bachus KN. Role of plantar plate and surgical reconstruction techniques on static stability of lesser metatarsophalangeal joints: a biomechanical study. Foot Ankle Int. 2013 Oct;34(10):1436-42. doi: 10.1177/1071100713491728. Epub 2013 Jun 17. PubMed PMID: 23774466. ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23774466)
RECOMMENDED READINGS
[Doty JF, Coughlin MJ, Weil L Jr, Nery C. Etiology and management of lesser toe metatarsophalangeal joint instability. Foot Ankle Clin. 2014 Sep;19(3):385-405. doi: 10.1016/j.fcl.2014.06.013. Epub 2014 Jul 10. PubMed PMID: 25129351. ](http://www.ncbi.nlm.nih.gov/pubmed/25129351)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/25129351)[ ](http://www.ncbi.nlm.nih.gov/pubmed/25129351)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25129351)
Nery C, Coughlin MJ, Baumfeld D, Raduan FC, Mann TS, Catena F. Prospective evaluation of protocol for surgical treatment of lesser MTP joint plantar plate tears. Foot Ankle Int. 2014 Sep;35(9):876-85. doi: 10.1177/1071100714539659. Epub 2014 Jun 23. PubMed PMID:
[24958766/. ](http://www.ncbi.nlm.nih.gov/pubmed/24958766)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24958766)
[Chalayon O, Chertman C, Guss AD, Saltzman CL, Nickisch F, Bachus KN. Role of plantar plate and surgical reconstruction techniques on static stability of lesser metatarsophalangeal joints: a biomechanical study. Foot Ankle Int. 2013 Oct;34(10):1436-42. doi: 10.1177/1071100713491728. Epub 2013 Jun 17. PubMed PMID: 23774466. ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23774466)
Question 50High Yield
Figure 1 is the radiograph of a 31-year-old man who had left shoulder pain after a fall during a snowboarding jump. Residual displacement of 5 mm after closed reduction is most likely to result in
---
---

Explanation
Humerus fractures account for 11% of all fractures among snowboarders and are the second-most-common upper-extremity fracture after radius fractures (48%). Surgical fixation is recommended for fractures with residual displacement >5 mm, or >3 mm in active patients involved in frequent overhead activity. Malunion can result in a mechanical block to shoulder abduction or external rotation and altered rotator cuff mechanics, causing weakness. A rich arterial network provides a favorable healing environment for greater tuberosity fractures. Consequently, nonunion and osteonecrosis are uncommon.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon