Orthopedic Review | Dr Hutaif General Orthopedics Revie -...
14 Apr 2026
52 min read
69 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Review | Dr Hutaif General Orthope...
00:00
Start Quiz
Question 1High Yield
A 20-year-old woman sustained the closed injury shown in Figures 49a and 49b in a motor vehicle accident. Examination reveals that this is an isolated injury; however, she has a complete radial nerve palsy. Management should consist of
Explanation
Lacerated radial nerves are associated with open humeral fractures. All open humeral fractures with radial nerve palsy should be managed with radial nerve exploration and skeletal stabilization. Closed humeral fractures with associated radial nerve palsy usually have an intact nerve with neurapraxia. Most of these patients recover without surgical treatment. If the patient has multiple injuries, skeletal stabilization may be indicated to improve mobilization. For an isolated closed humeral fracture with a radial nerve palsy, the treatment of choice is splinting for 1 to 2 weeks, followed by a humeral fracture brace.
REFERENCES: Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high-energy humeral shaft fractures. J Hand Surg Am 2004;29:144-147.
Foster RJ, Swiontkowski MF, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
REFERENCES: Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high-energy humeral shaft fractures. J Hand Surg Am 2004;29:144-147.
Foster RJ, Swiontkowski MF, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
Question 2High Yield
All of the following strategies are used to reduce the micromotion between the flexible bone of the femur and a stiff femoral implant except:
Explanation
Providing external porous coatings to the tip of the stem, reducing contact between the tip of the stem and cortical bone, and tapering the stem tip are strategies that have been used to reduce micromotion. Cementing the femoral component will also reduce micromotion
Question 3High Yield
A 50-year-old patient who plays tennis sustained the deformity shown in Figure 27 following a high volley. Further diagnostic work-up should include**
Explanation
The patient has a rupture of the long head of the biceps; however, patients older than age 45 years are at greater risk of having an associated rotator cuff tear. An MRI scan should be ordered to avoid missing concomitant rotator cuff pathology. While patients may report pain radiating down the arm at the time of the tendon rupture, an EMG is not indicated. The short head of the biceps is intact and needs no further work-up, even though the muscle descends in most cases. The anterior labrum can be injured but is not associated with this deformity.
REFERENCES: Neer CS II, Bigliani LU, Hawkins RJ: Rupture of the long head of the biceps related to the subacromial impingement. Orthop Trans 1977;1:114.
Hawkins RJ, Murnaghan JP: The shoulder, in Gruess RL, Ronnie WRJ (eds): Adult Orthopaedics. New York, NY, Churchill Livingstone, 1984, pp 945-1054.
REFERENCES: Neer CS II, Bigliani LU, Hawkins RJ: Rupture of the long head of the biceps related to the subacromial impingement. Orthop Trans 1977;1:114.
Hawkins RJ, Murnaghan JP: The shoulder, in Gruess RL, Ronnie WRJ (eds): Adult Orthopaedics. New York, NY, Churchill Livingstone, 1984, pp 945-1054.
Question 4High Yield
Video 100 is the presurgical lateral ankle examination of a 45-year-old woman who has had pain and discomfort for 2 years along the posterolateral ankle following a sudden dorsiflexion injury. She notes occasional clicking and popping, and she has not experienced resolution of her symptoms despite immobilization and physical therapy. Examination reveals a stable ankle-to-anterior drawer and inversion stress testing. No strength deficit is noted, but
she has apprehension with resisted eversion. MR images do not reveal evidence of tendonosis or tear. The most appropriate surgical intervention is
she has apprehension with resisted eversion. MR images do not reveal evidence of tendonosis or tear. The most appropriate surgical intervention is




Explanation
This patient has a clear history of dorsiflexion injury complicated by chronic peroneal tendon dislocation. The symptoms and findings are consistent with dislocation in this particular case. Groove deepening of the posterior fibula with associated imbrication of the peroneal retinaculum is the most effective surgical procedure. Associated synovitis or tendonosis should be addressed. However, failure to deepen the groove and imbricate the retinaculum will result in continued discomfort. Consequently, both responses that involve isolated tendon surgery are not appropriate. Associated subjective instability can be noted in these patients. The examination is critical to determine the stability of the lateral collateral complex, which is intact in this case (so
imbrication is not indicated). A sense of apprehension is a common examination finding because patients sense that the peroneals will subluxate with resisted eversion. Placement of the examiner's hands on the peroneals to stabilize the tendons should relieve this apprehension. A patient may not be able to voluntarily dislocate the tendon. Dynamic ultrasound is the most sensitive radiographic examination for detection of dislocation. Intrasheath peroneal subluxation may also occur and is treated similarly.
RECOMMENDED READINGS
Raikin SM. Intrasheath subluxation of the peroneal tendons. Surgical technique. J Bone Joint Surg Am. 2009 Mar 1;91 Suppl 2 Pt 1:146-55. doi: 10.2106/JBJS.H.01356. PubMed PMID:
[19255207.](http://www.ncbi.nlm.nih.gov/pubmed/19255207)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19255207)
[Philbin TM, Landis GS, Smith B. Peroneal tendon injuries. J Am Acad Orthop Surg. 2009 May;17(5):306-17. Review. PubMed PMID: 19411642. ](http://www.ncbi.nlm.nih.gov/pubmed/19411642)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19411642)
[Ogawa BK, Thordarson DB. Current concepts review: peroneal tendon subluxation and dislocation. Foot Ankle Int. 2007 Sep;28(9):1034-40. Review. PubMed PMID: 17880883. ](http://www.ncbi.nlm.nih.gov/pubmed/17880883)[View](http://www.ncbi.nlm.nih.gov/pubmed/17880883)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17880883)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17880883)
This is the last question of the exam.
imbrication is not indicated). A sense of apprehension is a common examination finding because patients sense that the peroneals will subluxate with resisted eversion. Placement of the examiner's hands on the peroneals to stabilize the tendons should relieve this apprehension. A patient may not be able to voluntarily dislocate the tendon. Dynamic ultrasound is the most sensitive radiographic examination for detection of dislocation. Intrasheath peroneal subluxation may also occur and is treated similarly.
RECOMMENDED READINGS
Raikin SM. Intrasheath subluxation of the peroneal tendons. Surgical technique. J Bone Joint Surg Am. 2009 Mar 1;91 Suppl 2 Pt 1:146-55. doi: 10.2106/JBJS.H.01356. PubMed PMID:
[19255207.](http://www.ncbi.nlm.nih.gov/pubmed/19255207)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19255207)
[Philbin TM, Landis GS, Smith B. Peroneal tendon injuries. J Am Acad Orthop Surg. 2009 May;17(5):306-17. Review. PubMed PMID: 19411642. ](http://www.ncbi.nlm.nih.gov/pubmed/19411642)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19411642)
[Ogawa BK, Thordarson DB. Current concepts review: peroneal tendon subluxation and dislocation. Foot Ankle Int. 2007 Sep;28(9):1034-40. Review. PubMed PMID: 17880883. ](http://www.ncbi.nlm.nih.gov/pubmed/17880883)[View](http://www.ncbi.nlm.nih.gov/pubmed/17880883)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17880883)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17880883)
This is the last question of the exam.
Question 5High Yield
Figure 1 is the axial MRI scan of a 45-year-old brick mason who experienced acute right elbow pain after attempting to lift a wheelbarrow. Examination reveals pain and swelling in the antecubital fossa, weakness with forearm supination, and an abnormal hook test. The surgeon performs an anterior repair with two anchors. Three months after surgery, the patient has appropriate strength and range of motion but reports persistent radiating paresthesias along the radial side of the forearm. What is the best next step in management?
Explanation
This is a classic presentation of an acute traumatic distal biceps tendon rupture. In the dominant extremity of a manual laborer, this injury can result in approximately 40% loss of supination strength. Although not required, an MRI scan can confirm
the diagnosis. In general, a single incision anterior or two incision anterior/ posterior repair can be utilized for surgical intervention with similar success rates. Although the percentage of complications is similar between surgical approaches, the type of complications can vary. Anterior only repairs have a
20
higher risk of traction injury to the lateral antebrachial cutaneous nerve (LABC) secondary to the degree of retraction required for exposure in muscular patients. Posterior repairs have a higher risk for radiographic heterotopic bone formation. Fortunately, most LABC injuries are neuropraxias and resolve with observation, but resolution may take up to 6 months. In this case, ongoing observation is appropriate, with surgical exploration being considered only in chronic cases. Patients should be appropriately counseled about this issue prior to surgery.
the diagnosis. In general, a single incision anterior or two incision anterior/ posterior repair can be utilized for surgical intervention with similar success rates. Although the percentage of complications is similar between surgical approaches, the type of complications can vary. Anterior only repairs have a
20
higher risk of traction injury to the lateral antebrachial cutaneous nerve (LABC) secondary to the degree of retraction required for exposure in muscular patients. Posterior repairs have a higher risk for radiographic heterotopic bone formation. Fortunately, most LABC injuries are neuropraxias and resolve with observation, but resolution may take up to 6 months. In this case, ongoing observation is appropriate, with surgical exploration being considered only in chronic cases. Patients should be appropriately counseled about this issue prior to surgery.
Question 6High Yield
A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
Explanation
This represents a terrible triad injury, with elbow dislocation, radial head fracture, and coronoid fracture. The LCL complex is typically disrupted in this injury pattern. Repair or reconstruction of this structure provides the greatest increase in rotational stability of the elbow.
Question 7High Yield
A patient with a transverse femur fracture undergoes statically locked antegrade intramedullary nailing. Postoperatively, the patient appears to have a rotational deformity of greater than 25 degrees. The surgeon informs the patient, who chooses to undergo corrective treatment with removal of distal interlocking screws, rotational correction, and relocking of the screws. The patient goes on to heal
but has persistent hip pain and a limp that does not improve completely after extensive rehabilitation. There is complete healing, no evidence of infection, no hardware issues, no ectopic bone, and rotational studies indicate less than 2 degrees of malrotation. Functional capacity testing reveals the affected abductor and quadriceps function to be about 85% of the uninjured side and the patient returns to work and most of his recreational activities except rock climbing. Two days before the statute of limitations, the patient
files a malpractice suit alleging negligence of surgery, loss of function, consortium, and pain and suffering due to the surgeon's efforts. What action should the surgeon and the defense team take?
but has persistent hip pain and a limp that does not improve completely after extensive rehabilitation. There is complete healing, no evidence of infection, no hardware issues, no ectopic bone, and rotational studies indicate less than 2 degrees of malrotation. Functional capacity testing reveals the affected abductor and quadriceps function to be about 85% of the uninjured side and the patient returns to work and most of his recreational activities except rock climbing. Two days before the statute of limitations, the patient
files a malpractice suit alleging negligence of surgery, loss of function, consortium, and pain and suffering due to the surgeon's efforts. What action should the surgeon and the defense team take?
Explanation
**
To establish negligence, certain criteria must be met. 1) A duty was owed by the surgeon (in this case, yes, a relationship was established). 2) The duty was breached, where the provider failed to meet the standard of care (there
was a technical error, but it was corrected). 3) The breach caused an injury. In this case, the patient had an outcome that was very acceptable, as
documented with outcome studies, for femur fractures. Also, the rotational error and locking distally would have had little impact on the hip, whereas antegrade nailing itself is expected to result in some objective impairment of the hip in some patients. 4) Damages were incurred as a result. In this case, the patient returned to work and could not rock climb which could be reasonably expected with a femur fracture in some patients, and cannot be causally linked to the corrective surgery. For all practical purposes, the patient had a very acceptable outcome. Thus, settling the case for an error would be rather permissive and the important issue is that the surgeon recognized the problem, addressed it, and fulfilled his or her postoperative responsibility. The case is very defendable, and thus it is unlikely to be lost. Defending the case and alleging no error is incorrect because there was an error. The surgeon should never function outside of his or her legal counsel once a suit is filed.
To establish negligence, certain criteria must be met. 1) A duty was owed by the surgeon (in this case, yes, a relationship was established). 2) The duty was breached, where the provider failed to meet the standard of care (there
was a technical error, but it was corrected). 3) The breach caused an injury. In this case, the patient had an outcome that was very acceptable, as
documented with outcome studies, for femur fractures. Also, the rotational error and locking distally would have had little impact on the hip, whereas antegrade nailing itself is expected to result in some objective impairment of the hip in some patients. 4) Damages were incurred as a result. In this case, the patient returned to work and could not rock climb which could be reasonably expected with a femur fracture in some patients, and cannot be causally linked to the corrective surgery. For all practical purposes, the patient had a very acceptable outcome. Thus, settling the case for an error would be rather permissive and the important issue is that the surgeon recognized the problem, addressed it, and fulfilled his or her postoperative responsibility. The case is very defendable, and thus it is unlikely to be lost. Defending the case and alleging no error is incorrect because there was an error. The surgeon should never function outside of his or her legal counsel once a suit is filed.
Question 8High Yield
Figures 1 and 2 are the AP and lateral radiographs of a 5-year-old African-American boy who has a 1-month history of pain and swelling in his upper arm. His mother reports a medical history that includes sickle cell disease. Laboratory studies demonstrate elevated erythrocyte sedimentation rate and C-reactive protein level, and a white blood cell count of 17,000. What organism is most likely associated with this process in the patient?

Explanation
■
Although patients with sickle cell disease are at far higher risk of developing salmonella osteomyelitis than the general population, Staphylococcus aureus remains the most common organism causing osteomyelits in children of this age group.
■
Although patients with sickle cell disease are at far higher risk of developing salmonella osteomyelitis than the general population, Staphylococcus aureus remains the most common organism causing osteomyelits in children of this age group.
Question 9High Yield
A 16-year-old boy who is a competitive basketball player (Figure 43)

Explanation
- Meniscal repair
Question 10High Yield
Which of the following molecules play an important role in cartilage hypertrophy during growth plate development and ossification in fracture healing:
Explanation
Important concepts to remember regarding signaling proteins include:
Indian hedgehog (IHH) and core binding factor alpha 1 (Cbfa1) influence embryoniCbone formation and fracture healing. Vascular endothelial growth factor (VEGF) plays a role in cartilage hypertrophy at the growth plate and during fracture healing.
Transforming growth factor-beta (TGF-B) and platelet derived growth factor (PDGF) are found in early fracture hematoma, and these factors modulate cell proliferation and differentiation.
Bone morphogenetiCprotein and interleukin 1 and 6 are expressed during cartilage formation. Correct Answer: Vascular endothelial growth factor (VEGF)
Indian hedgehog (IHH) and core binding factor alpha 1 (Cbfa1) influence embryoniCbone formation and fracture healing. Vascular endothelial growth factor (VEGF) plays a role in cartilage hypertrophy at the growth plate and during fracture healing.
Transforming growth factor-beta (TGF-B) and platelet derived growth factor (PDGF) are found in early fracture hematoma, and these factors modulate cell proliferation and differentiation.
Bone morphogenetiCprotein and interleukin 1 and 6 are expressed during cartilage formation. Correct Answer: Vascular endothelial growth factor (VEGF)
Question 11High Yield
In infantile idiopathic scoliosis, which of the following factors suggests progression?
Explanation
DISCUSSION: Infantile idiopathic scoliosis occurs more commonly in boys, with a 3 to 1 male to female ratio. Neural axis abnormalities, hip dysplasia, and congenital heart disease are all associated with the condition; spontaneous correction frequently occurs. Curve progression can be predicted by the rib vertebral angle difference or the phase of the rib head. Rib overlap of the apical vertebral body or a rib vertebral angle difference of greater than 20 degrees indicates that the curve is likely to progress. Gender, family history, and age at presentation have not been found to be risk factors for progression.
REFERENCES: Mehta MH: The rib-vertebra angle in the early diagnosis between resolving and progressive infantile scoliosis. J Bone Joint Surg Br 1972;54:230-243.
Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, p 697.
70 • American Academy of Orthopaedic Surgeons
DISCUSSION: Infantile idiopathic scoliosis occurs more commonly in boys, with a 3 to 1 male to female ratio. Neural axis abnormalities, hip dysplasia, and congenital heart disease are all associated with the condition; spontaneous correction frequently occurs. Curve progression can be predicted by the rib vertebral angle difference or the phase of the rib head. Rib overlap of the apical vertebral body or a rib vertebral angle difference of greater than 20 degrees indicates that the curve is likely to progress. Gender, family history, and age at presentation have not been found to be risk factors for progression.
REFERENCES: Mehta MH: The rib-vertebra angle in the early diagnosis between resolving and progressive infantile scoliosis. J Bone Joint Surg Br 1972;54:230-243.
Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, p 697.
70 • American Academy of Orthopaedic Surgeons
Question 12High Yield
Exposure of tendons to ciprofloxacin in vitro causes all of the following except:
Explanation
C iprofloxacin was shown to cause a decrease in fibroblast proliferation, proteoglycan synthesis, and collagen synthesis. Matrix degrading proteolytic activity was increased.
Question 13High Yield
A 14-year-old boy with a history of cerebral palsy has a clawed hallux, cavus foot deformity, and associated pain. Examination reveals pain under the first metatarsal head and a rigid first tarsometatarsal joint. Treatment should consist of
Explanation
In a retrospective study for clawing of the hallux with associated cavus foot deformities, the modified Robert Jones tendon transfer was shown to be effective in relieving symptoms related to clawing of the hallux in 90% of patients but was not reliable in relieving pain under the first metatarsal head, with success in only 43% of patients. In three patients, pain under the metatarsal head was relieved initially but recurred by 18 months. The return of symptoms in these cases is the result of stretching of the muscle and tendon of the extensor hallucis longus by the more powerful peroneus longus. Basal dorsal wedge osteotomy at the time of the modified Robert Jones procedure is recommended.
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 79-100.
Tynan MC, Klenerman L: The modified Robert Jones tendon transfer in cases of pes cavus and clawed hallux. Foot Ankle Int 1994;15:68-71.
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 79-100.
Tynan MC, Klenerman L: The modified Robert Jones tendon transfer in cases of pes cavus and clawed hallux. Foot Ankle Int 1994;15:68-71.
Question 14High Yield
When performing an ulnar nerve decompression at the elbow, the surgeon must be aware of the
Explanation
The medial antebrachial cutaneous and medial brachial cutaneous are nerves that can be injured during ulnar nerve decompression at the elbow. The medial antebrachial cutaneous nerve crosses the surgical field at an average of 3.1 cm distal to the medial epicondyle. The medial brachial cutaneous nerve crosses the field 7 cm proximal to the medial epicondyle and arborizes into two to three terminal branches. Because the surgical approach involves dissection on the medial side, the posterior antebrachial cutaneous nerve is distant from the exposure. Although the median nerve potentially can be located in the deep dissection of a submuscular transposition, it is considered distant to an in situ decompression.
Question 15High Yield
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?
Explanation
Anterior dislocation is the most common type of sternoclavicular dislocation. The medial end of the clavicle is displaced anterior or anterosuperior to the anterior margin of the sternum. In a study by Omer, 31% of athletic injuries have been known to cause a dislocation of the sternoclavicular joint. The serendipity view can show this dislocation, as will CT of the chest. This view requires the x-ray beam to be aimed at the manubrium with 40 degrees of cephalic tilt. An anterior sternoclavicular joint dislocation will appear superiorly displaced, while a posterior sternoclavicular joint dislocation is inferiorly displaced on the serendipity view.
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Omer GE Jr: Osteotomy of the clavicle in surgical reduction of anterior sternoclavicular dislocation. J Trauma 1967;7:584-590.
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Omer GE Jr: Osteotomy of the clavicle in surgical reduction of anterior sternoclavicular dislocation. J Trauma 1967;7:584-590.
Question 16High Yield
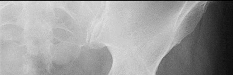
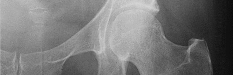
Figures 1 and 2 are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg. What is the most likely diagnosis for the source of this patient's pain?
---
---








Explanation
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement. Surgical treatment for cam impingement can be effective for symptomatic patients. Even among high-level athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable with those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment. Byrd and Jones described five patients who developed transient neurapraxias that resolved uneventfully. The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a _periacetabular osteotomy can develop a more retroverted acetabulum as well._
---
---
Question 17High Yield
A
B
C
What is the appropriate first step when confirming the diagnosis of a neurologically intact, 73-year-old man who has the images shown in Figures 25a through 25c?
B
C
What is the appropriate first step when confirming the diagnosis of a neurologically intact, 73-year-old man who has the images shown in Figures 25a through 25c?




Explanation
The radiograph and MR images show an osteoblastic lesion in the T9 and T8 vertebral bodies. In an older man, this finding most likely reveals metastatic prostate cancer. The first and least invasive diagnostic step is to order a PSA level. Gleave and associates found in a retrospective review of patients with prostate cancer that isolated levels of PSA lower than 10 to 20 micrograms per liter are rarely associated with bone metastasis. Vis and associates documented that 10-year prostate cancer survival in a screened population was higher than 60%, and in an unscreened population it was 24%. In a neurologically intact patient with no evidence of neural compression or instability, surgery is not indicated. Fine-needle aspiration may be performed, but the diagnostic yield in a blastic lesion is low. A bone scan may be indicated to complete the metastatic workup, but it will not aid in the diagnosis of tissue source.
RECOMMENDED READINGS
[Gleave ME, Coupland D, Drachenberg D, Cohen L, Kwong S, Goldenberg SL, Sullivan LD. Ability of serum prostate-specific antigen levels to predict normal bone scans in patients with newly diagnosed prostate cancer. Urology. 1996 May;47(5):708-12. PubMed PMID: 8650870. ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[View ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8650870)
[Vis AN, Roemeling S, Reedijk AM, Otto SJ, Schröder FH. Overall survival in the intervention arm of a randomized controlled screening trial for prostate cancer compared with a clinically diagnosed cohort. Eur Urol. 2008 Jan;53(1):91-8. Epub 2007 Jun 12. PubMed PMID: 17583416. ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[View ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17583416)
Cronen GA, Emery SE. Benign and malignant lesions of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:351-366.
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29
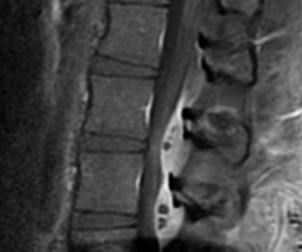
Figures 26a and 26b are the MR images with gadolinium enhancement of a 40-year-old man who arrives at the emergency department with a 4-day history of fevers and severe back pain without radiation. He is normotensive at presentation with a heart rate of 86 beats per minute. Upon examination he is neurologically intact with normal sensory and motor function. He has a history of alcohol and cocaine abuse. His white blood cell (WBC) count is 12000 (reference range [rr], 4500-11000 /µL) and his C-reactive protein (CRP) level is 100 mg/L (rr, 0.08-3.1 mg/L)
RECOMMENDED READINGS
[Gleave ME, Coupland D, Drachenberg D, Cohen L, Kwong S, Goldenberg SL, Sullivan LD. Ability of serum prostate-specific antigen levels to predict normal bone scans in patients with newly diagnosed prostate cancer. Urology. 1996 May;47(5):708-12. PubMed PMID: 8650870. ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[View ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8650870)
[Vis AN, Roemeling S, Reedijk AM, Otto SJ, Schröder FH. Overall survival in the intervention arm of a randomized controlled screening trial for prostate cancer compared with a clinically diagnosed cohort. Eur Urol. 2008 Jan;53(1):91-8. Epub 2007 Jun 12. PubMed PMID: 17583416. ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[View ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17583416)
Cronen GA, Emery SE. Benign and malignant lesions of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:351-366.
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29
Figures 26a and 26b are the MR images with gadolinium enhancement of a 40-year-old man who arrives at the emergency department with a 4-day history of fevers and severe back pain without radiation. He is normotensive at presentation with a heart rate of 86 beats per minute. Upon examination he is neurologically intact with normal sensory and motor function. He has a history of alcohol and cocaine abuse. His white blood cell (WBC) count is 12000 (reference range [rr], 4500-11000 /µL) and his C-reactive protein (CRP) level is 100 mg/L (rr, 0.08-3.1 mg/L)
Question 18High Yield
Diagnostic work-up concluded that the patient has metastatic lymphoma. He has no neurologic deficit.Based on these findings, what is the most appropriate management for this spinal condition?
Explanation
_
_
DISCUSSION FOR QUESTIONS 107 THROUGH 109:
Patients with no prior diagnosis of cancer may present with vertebral lesions. After obtaining initial radiographs, the next most appropriate step is to obtain an MRI with gadolinium. To determine the primary site of the disease, a CT of the chest, abdomen, and pelvis is the next step in establishing a diagnosis. Radiation therapy is the first line of treatment in spinal metastatic disease from lymphoma because it is a highly radiosensitive tumor.
_
DISCUSSION FOR QUESTIONS 107 THROUGH 109:
Patients with no prior diagnosis of cancer may present with vertebral lesions. After obtaining initial radiographs, the next most appropriate step is to obtain an MRI with gadolinium. To determine the primary site of the disease, a CT of the chest, abdomen, and pelvis is the next step in establishing a diagnosis. Radiation therapy is the first line of treatment in spinal metastatic disease from lymphoma because it is a highly radiosensitive tumor.
Question 19High Yield
The incidence of ipsilateral phrenic nerve blockade after an interscalene
block approaches
block approaches
Explanation
The most common side effect of an interscalene block is ipsilateral phrenic nerve blockade. The phrenic nerve arises chiefly from the fourth cervical ramus (with contributions from the third and fifth) and is the sole motor supply to the diaphragm. Phrenic nerve palsy usually is well tolerated in healthy patients but should be avoided in patients with limited pulmonary function (severe restrictive or obstructive lung disease, myasthenia gravis, or contralateral hemidiaphragmatic dysfunction). The incidence of ipsilateral phrenic nerve blockade afer interscalene block approaches 100%.
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14;546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14;546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
Question 20High Yield
A 4-year-old boy with recent onset of limping and right hip pain is diagnosed with Perthes disease. His radiographs reveal femoral head epiphysis fragmentation and partial collapse consistent with lateral pillar classification B and mild lateral extrusion. His prognosis strongly correlates with his
Explanation
■
Legg-Calve-Perthes disease (LCPD) is a childhood disorder of unknown etiology that can produce permanent deformity of the femoral head. Although LCPD can affect a wide range of children, it is most commonly seen in children aged 5 to 8 years. The male to female ratio is approximately 5:1, and bilateral disease occurs in 10% to 15% of patients. Treatment of patients with LCPD requires an understanding of the natural history of the disease, prognostic factors, and the effectiveness of various treatment methods.
Some of the prognostic indicators of outcome in patients with LCPD includes extent of the femoral head deformity and loss of hip joint congruity at maturity (Stulberg classification), age at onset, lateral pillar height at the fragmentation stage (lateral pillar classification), and premature physeal closure.
Existing studies show a difference in outcome depending on patient age at disease onset. Most patients in whom disease onset occurs younger than age 6 years achieve Stulberg I/II hips at maturity regardless of the type of treatment. These studies show no added benefits in outcome with surgical management in this age group. The treatment results for children aged 6 to 8 years are less clear, though treatment compared with no treatment (brace, range of motion, surgery) may yield better results. For children in whom disease onset occurs older than age 8 years, surgery compared with nonsurgical treatment could be beneficial for the lateral pillar B and B/C border groups but not for patients classified as group C.
Legg-Calve-Perthes disease (LCPD) is a childhood disorder of unknown etiology that can produce permanent deformity of the femoral head. Although LCPD can affect a wide range of children, it is most commonly seen in children aged 5 to 8 years. The male to female ratio is approximately 5:1, and bilateral disease occurs in 10% to 15% of patients. Treatment of patients with LCPD requires an understanding of the natural history of the disease, prognostic factors, and the effectiveness of various treatment methods.
Some of the prognostic indicators of outcome in patients with LCPD includes extent of the femoral head deformity and loss of hip joint congruity at maturity (Stulberg classification), age at onset, lateral pillar height at the fragmentation stage (lateral pillar classification), and premature physeal closure.
Existing studies show a difference in outcome depending on patient age at disease onset. Most patients in whom disease onset occurs younger than age 6 years achieve Stulberg I/II hips at maturity regardless of the type of treatment. These studies show no added benefits in outcome with surgical management in this age group. The treatment results for children aged 6 to 8 years are less clear, though treatment compared with no treatment (brace, range of motion, surgery) may yield better results. For children in whom disease onset occurs older than age 8 years, surgery compared with nonsurgical treatment could be beneficial for the lateral pillar B and B/C border groups but not for patients classified as group C.
Question 21High Yield
A 20-year-old basketball player has tenderness and bruising after sustaining a blow to the knee. A radiograph is shown in Figure 15. What is the most likely diagnosis?
Explanation
The patient has a bipartite patella. The line between the fragment and the main patella is smooth and sclerotic, indicating a chronic, not acute, entity. The location is classic for a bipartite patella, not a tumor.
REFERENCES: Schmidt DR, Henry JH: Stress injuries of the adolescent extensor mechanism. Clin Sports Med 1989;8:343-355.
Weaver JK: Bipartite patellae as a cause of disability in the athlete. Am J Sports Med 1977;5:137-143.
REFERENCES: Schmidt DR, Henry JH: Stress injuries of the adolescent extensor mechanism. Clin Sports Med 1989;8:343-355.
Weaver JK: Bipartite patellae as a cause of disability in the athlete. Am J Sports Med 1977;5:137-143.
Question 22High Yield
A 55-year-old woman develops posttraumatic arthritis in the elbow following a distal humerus fracture. What is the most likely mid-term (5-10 years after surgery) complication following semiconstrained total elbow arthroplasty (TEA)?
Explanation
DISCUSSION:
TEA has been described for posttraumatic arthritis of the elbow and typically involves a young patient population with multiple previous operations on the affected elbow. Morrey and Schneeberger found aseptic component loosening to be uncommon (<10% of patients) and usually occurring >10 years after surgery. Prosthetic fracture, usually of the ulnar component, is also a late-term finding. Infection is the most common mode of early failure but usually occurs within the first 5 years and has an overall rate of approximately 5%. Bushing wear has been reported as the most common cause of mechanical TEA failure in this population at
intermediate-term follow-up.
DISCUSSION:
TEA has been described for posttraumatic arthritis of the elbow and typically involves a young patient population with multiple previous operations on the affected elbow. Morrey and Schneeberger found aseptic component loosening to be uncommon (<10% of patients) and usually occurring >10 years after surgery. Prosthetic fracture, usually of the ulnar component, is also a late-term finding. Infection is the most common mode of early failure but usually occurs within the first 5 years and has an overall rate of approximately 5%. Bushing wear has been reported as the most common cause of mechanical TEA failure in this population at
intermediate-term follow-up.
Question 23High Yield
Which treatment regimen for Ewing sarcoma most effectively controls disease?
Explanation
Patients with Ewing sarcoma need chemotherapy to treat micrometastatic disease. Historical outcomes of patients who receive local control alone without chemotherapy are dismal. Chemotherapy alone, however, is not adequate to control local bulky disease. Local control options include radiation therapy or wide surgical resection. Historically, it was believed that surgery should be recommended for expendable bones to minimize morbidity. More recent data support improved outcomes (vs outcomes associated with radiation alone to the primary site of disease) for patients who undergo wide surgical resection; consequently, chemotherapy plus wide surgical resection is the most effective regimen.
RECOMMENDED READINGS
19. [Rodriguez-Galindo C, Spunt SL, Pappo AS. Treatment of Ewing sarcoma family of tumors: current status and outlook for the future. Med Pediatr Oncol. 2003 May;40(5):276-87. Review. Erratum in: Med Pediatr Oncol. 2003 Dec;41(6):594. PubMed PMID: 12652615. ](http://www.ncbi.nlm.nih.gov/pubmed/12652615)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12652615)
20. Bacci G, Toni A, Avella M, Manfrini M, Sudanese A, Ciaroni D, Boriani S, Emiliani E, Campanacci
[M. Long-term results in 144 localized Ewing's sarcoma patients treated with combined therapy. Cancer. 1989 Apr 15;63(8):1477-86. PubMed PMID: 2924256. ](http://www.ncbi.nlm.nih.gov/pubmed/2924256)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2924256)
21. [Maheshwari AV, Cheng EY. Ewing sarcoma family of tumors. J Am Acad Orthop Surg. 2010 Feb;18(2):94-107. Review. PubMed PMID: 20118326. ](http://www.ncbi.nlm.nih.gov/pubmed/20118326)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20118326)
22. Weis L. Ewing’s Sarcoma. In: Simon MA, Springfield D, eds. _Surgery for Bone and Soft Tissue Tumors_. Philadelphia, PA: Lippincott-Raven; 1998:287-298.
23. DuBois SG, Krailo MD, Gebhardt MC, Donaldson SS, Marcus KJ, Dormans J, Shamberger RC, Sailer S, Nicholas RW, Healey JH, Tarbell NJ, Randall RL, Devidas M, Meyer JS, Granowetter L, Womer RB, Bernstein M, Marina N, Grier HE. Comparative evaluation of local control strategies in localized
Ewing sarcoma of bone: a report from the Children's Oncology Group. Cancer. 2015 Feb 1;121(3):467-
[75/. doi: 10.1002/cncr.29065. Epub 2014 Sep 23. PubMed PMID: 25251206. ](http://www.ncbi.nlm.nih.gov/pubmed/25251206)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25251206)
RECOMMENDED READINGS
19. [Rodriguez-Galindo C, Spunt SL, Pappo AS. Treatment of Ewing sarcoma family of tumors: current status and outlook for the future. Med Pediatr Oncol. 2003 May;40(5):276-87. Review. Erratum in: Med Pediatr Oncol. 2003 Dec;41(6):594. PubMed PMID: 12652615. ](http://www.ncbi.nlm.nih.gov/pubmed/12652615)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12652615)
20. Bacci G, Toni A, Avella M, Manfrini M, Sudanese A, Ciaroni D, Boriani S, Emiliani E, Campanacci
[M. Long-term results in 144 localized Ewing's sarcoma patients treated with combined therapy. Cancer. 1989 Apr 15;63(8):1477-86. PubMed PMID: 2924256. ](http://www.ncbi.nlm.nih.gov/pubmed/2924256)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2924256)
21. [Maheshwari AV, Cheng EY. Ewing sarcoma family of tumors. J Am Acad Orthop Surg. 2010 Feb;18(2):94-107. Review. PubMed PMID: 20118326. ](http://www.ncbi.nlm.nih.gov/pubmed/20118326)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20118326)
22. Weis L. Ewing’s Sarcoma. In: Simon MA, Springfield D, eds. _Surgery for Bone and Soft Tissue Tumors_. Philadelphia, PA: Lippincott-Raven; 1998:287-298.
23. DuBois SG, Krailo MD, Gebhardt MC, Donaldson SS, Marcus KJ, Dormans J, Shamberger RC, Sailer S, Nicholas RW, Healey JH, Tarbell NJ, Randall RL, Devidas M, Meyer JS, Granowetter L, Womer RB, Bernstein M, Marina N, Grier HE. Comparative evaluation of local control strategies in localized
Ewing sarcoma of bone: a report from the Children's Oncology Group. Cancer. 2015 Feb 1;121(3):467-
[75/. doi: 10.1002/cncr.29065. Epub 2014 Sep 23. PubMed PMID: 25251206. ](http://www.ncbi.nlm.nih.gov/pubmed/25251206)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25251206)
Question 24High Yield
Which of the following most accurately approximates the estimated risk of a musculoskeletal allograft containing the human immunodeficiency virus (HIV) despite adequate screening?
Explanation
6,000,000
DISCUSSION: The calculated risk of a musculoskeletal allograft containing HIV despite adequate screening has been estimated to be approximately 1 in 1.6 million. This estimate is based on the risk of HIV in the population, projected population estimates, and current methods of donor screening.
REFERENCES: McAllister D, Joyce M, Mann B, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;2148-2158.
Buck B, Malinin T: Human bone and tissue allografts: Preparation and safety. Clin Orthop Relat Res 1994;303:8 -
17.
Buck B, Malinin T, Brown M: Bone transplantation and human immunodeficiency virus: An estimate of risk of acquired immunodeficiency syndrome (AIDS). Clin Orthop Relat Res 1989;240:129-136.
_A i;___
Figure 92
6,000,000
DISCUSSION: The calculated risk of a musculoskeletal allograft containing HIV despite adequate screening has been estimated to be approximately 1 in 1.6 million. This estimate is based on the risk of HIV in the population, projected population estimates, and current methods of donor screening.
REFERENCES: McAllister D, Joyce M, Mann B, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;2148-2158.
Buck B, Malinin T: Human bone and tissue allografts: Preparation and safety. Clin Orthop Relat Res 1994;303:8 -
17.
Buck B, Malinin T, Brown M: Bone transplantation and human immunodeficiency virus: An estimate of risk of acquired immunodeficiency syndrome (AIDS). Clin Orthop Relat Res 1989;240:129-136.
_A i;___
Figure 92
Question 25High Yield
Figure 35 is the radiograph of a 37-year-old woman who began having right forefoot pain about 4 weeks ago after increasing her daily running mileage. She denies any specific injury. Upon examination she has tenderness over the medial forefoot with mild swelling. In addition to her activity level, what is the primary etiology of the radiograph finding?

Explanation
Stress fractures are the result of physiological bone response to increased stress. Increased stress on bone triggers an increase in remodeling, which begins with resorption of bone at the site of stress. Ongoing stress can overwhelm bone strength, resulting in a fracture. In the foot this most commonly is seen in the second metatarsal at the junction of the middle and distal thirds. Contributing factors to increased loading of the second metatarsal include hallux valgus (decreased hallux loading transfers to the second metatarsal head), hallux rigidus (offloading of the hallux attributable to pain increases second metatarsal loading), and a long second metatarsal (increased duration of contact during push-off in the stance phase).
RECOMMENDED READINGS
Shindle MK, Endo Y, Warren RF, Lane JM, Helfet DL, Schwartz EN, Ellis SJ.
Stress fractures about the tibia, foot, and ankle. J Am Acad Orthop Surg. 2012 Mar;20(3):167-
[76/. doi: 10.5435/JAAOS-20-03-167. Review. PubMed PMID: 22382289. ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[ ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22382289)
[Donahue SW, Sharkey NA. Strains in the metatarsals during the stance phase of gait: implications for stress fractures. J Bone Joint Surg Am. 1999 Sep;81(9):1236-44. PubMed PMID: 10505520. ](http://www.ncbi.nlm.nih.gov/pubmed/10505520)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10505520)
RECOMMENDED READINGS
Shindle MK, Endo Y, Warren RF, Lane JM, Helfet DL, Schwartz EN, Ellis SJ.
Stress fractures about the tibia, foot, and ankle. J Am Acad Orthop Surg. 2012 Mar;20(3):167-
[76/. doi: 10.5435/JAAOS-20-03-167. Review. PubMed PMID: 22382289. ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[ ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22382289)
[Donahue SW, Sharkey NA. Strains in the metatarsals during the stance phase of gait: implications for stress fractures. J Bone Joint Surg Am. 1999 Sep;81(9):1236-44. PubMed PMID: 10505520. ](http://www.ncbi.nlm.nih.gov/pubmed/10505520)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10505520)
Question 26High Yield
A 38-year-old man has winging of the ipsilateral scapula after undergoing a transaxillary resection of the first rib 3 weeks ago. What is the most likely cause of this finding?
Explanation
During transaxillary resection of the first rib, the long thoracic nerve is at risk as it passes either through or posterior to the middle scalene muscle. Injury to this nerve may occur as the result of overly aggressive retraction of the middle scalene during the procedure.
REFERENCES: Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Todd TW: The descent of the shoulder after birth: Its significance in the production of pressure-symptoms on the lowest brachial trunk. Anat Anz 1912;41:385-397.
REFERENCES: Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Todd TW: The descent of the shoulder after birth: Its significance in the production of pressure-symptoms on the lowest brachial trunk. Anat Anz 1912;41:385-397.
Question 27High Yield
Atraumatic neuropathy of the suprascapular nerve usually occurs at what
anatomic location?
anatomic location?
Explanation
The suprascapular nerve passes through the suprascapular notch and the spinoglenoid notch before innervating the infraspinatus muscle. At both locations, the suprascapular nerve is prone to nerve compression, which often results from a ganglion cyst. The other anatomic locations are not associated with suprascapular nerve impingement.
REFERENCES: Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Post M, Mayer J: Suprascapular nerve entrapment: Diagnosis and treatment. Clin Orthop 1987;223:126-136.
REFERENCES: Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Post M, Mayer J: Suprascapular nerve entrapment: Diagnosis and treatment. Clin Orthop 1987;223:126-136.
Question 28High Yield
A 63-year-old right-hand-dominant woman has a nontraumatic history of gradually progressive right shoulder pain. She describes a constant nagging pain that radiates to her deltoid insertion and has difficulty with overhead activities. Her examination and imaging studies confirm a rotator cuff tear. What is the mostly likely initiating anatomic location of her tear?
Explanation
Fundamental to understanding the pathogenesis of rotator cuff tears is an appreciation of the likely initiating site of the disease process. Although authors initially postulated that rotator cuff tears originated in the anterior margin of the supraspinatus tendon near the biceps tendon, recent research has challenged this notion. Kim and associates analyzed 360 full-thickness or partial-thickness rotator cuff tears using ultrasonograms. They separated stratified tears based on their anteroposterior size and whether they were partial- or full-thickness tears. The mean width and
length of tear size was 16.3 mm and 17 mm, respectively. Histograms showed that the most common tear location for all tears regardless of size was approximately 15 mm posterior to the biceps tendon. This corresponds to the center of the rotator crescent initially described by Burkhart and associates. This location is described as being more susceptible to degeneration secondary to its diminished vascular supply and mechanical properties. The rotator cable is an arch-shaped thick bundle of fibers that is thought to shield the crescent from stress.
RECOMMENDED READINGS
12. [Kim HM, Dahiya N, Teefey SA, Middleton WD, Stobbs G, Steger-May K, Yamaguchi K, Keener JD. Location and initiation of degenerative rotator cuff tears: an analysis of three hundred and sixty shoulders. J Bone Joint Surg Am. 2010 May;92(5):1088-96. doi: 10.2106/JBJS.I.00686. PubMed PMID: 20439653. ](http://www.ncbi.nlm.nih.gov/pubmed/20439653)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20439653)
13. [Burkhart SS, Esch JC, Jolson RS. The rotator crescent and rotator cable: an anatomic description of the shoulder's "suspension bridge". Arthroscopy. 1993;9(6):611-6. Erratum in: Arthroscopy 1994 Apr;10(2):239. PubMed PMID: 8305096. ](http://www.ncbi.nlm.nih.gov/pubmed/8305096)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8305096)
14. [Jarrett CD, Schmidt CC. Arthroscopic treatment of rotator cuff disease. J Hand Surg Am. 2011 Sep;36(9):1541-52; quiz 1552. doi: 10.1016/j.jhsa.2011.06.026. Epub 2011 Aug 6. Review. PubMed PMID: 21821368. ](http://www.ncbi.nlm.nih.gov/pubmed/21821368)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21821368)
15. [Mall NA, Kim HM, Keener JD, Steger-May K, Teefey SA, Middleton WD, Stobbs G, Yamaguchi K. Symptomatic progression of asymptomatic rotator cuff tears: a prospective study of clinical and sonographic variables. J Bone Joint Surg Am. 2010 Nov 17;92(16):2623-33. doi: 10.2106/JBJS.I.00506. PubMed PMID: 21084574. ](http://www.ncbi.nlm.nih.gov/pubmed/21084574)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21084574)
_This is the last question of the exam._
_GOOD LUCK_
length of tear size was 16.3 mm and 17 mm, respectively. Histograms showed that the most common tear location for all tears regardless of size was approximately 15 mm posterior to the biceps tendon. This corresponds to the center of the rotator crescent initially described by Burkhart and associates. This location is described as being more susceptible to degeneration secondary to its diminished vascular supply and mechanical properties. The rotator cable is an arch-shaped thick bundle of fibers that is thought to shield the crescent from stress.
RECOMMENDED READINGS
12. [Kim HM, Dahiya N, Teefey SA, Middleton WD, Stobbs G, Steger-May K, Yamaguchi K, Keener JD. Location and initiation of degenerative rotator cuff tears: an analysis of three hundred and sixty shoulders. J Bone Joint Surg Am. 2010 May;92(5):1088-96. doi: 10.2106/JBJS.I.00686. PubMed PMID: 20439653. ](http://www.ncbi.nlm.nih.gov/pubmed/20439653)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20439653)
13. [Burkhart SS, Esch JC, Jolson RS. The rotator crescent and rotator cable: an anatomic description of the shoulder's "suspension bridge". Arthroscopy. 1993;9(6):611-6. Erratum in: Arthroscopy 1994 Apr;10(2):239. PubMed PMID: 8305096. ](http://www.ncbi.nlm.nih.gov/pubmed/8305096)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8305096)
14. [Jarrett CD, Schmidt CC. Arthroscopic treatment of rotator cuff disease. J Hand Surg Am. 2011 Sep;36(9):1541-52; quiz 1552. doi: 10.1016/j.jhsa.2011.06.026. Epub 2011 Aug 6. Review. PubMed PMID: 21821368. ](http://www.ncbi.nlm.nih.gov/pubmed/21821368)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21821368)
15. [Mall NA, Kim HM, Keener JD, Steger-May K, Teefey SA, Middleton WD, Stobbs G, Yamaguchi K. Symptomatic progression of asymptomatic rotator cuff tears: a prospective study of clinical and sonographic variables. J Bone Joint Surg Am. 2010 Nov 17;92(16):2623-33. doi: 10.2106/JBJS.I.00506. PubMed PMID: 21084574. ](http://www.ncbi.nlm.nih.gov/pubmed/21084574)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21084574)
_This is the last question of the exam._
_GOOD LUCK_
Question 29High Yield
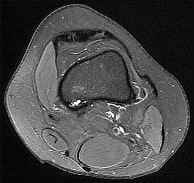
Figures 15a through 15c are the radiograph and MR images of a 16-year-old girl who experienced posterior knee pain after a dance recital 3 weeks ago; the pain resolved 1 week ago with ibuprofen use. What is the most appropriate treatment for this patient?


Explanation
The images reveal a small reactive-type lesion in the posteromedial aspect of the distal femur consistent with an avulsive cortical irregularity. Also referred to as a cortical desmoid, periosteal desmoid, or “tug lesion,” this lesion is seen most commonly in young adolescents, with a slight preponderance in boys, with one-third occurring bilaterally. It is thought to be related to repeated microtrauma from pulling of the adductor magnus or medial gastrocnemius on their respective periosteal attachment sites. Proper treatment involves recognition of this benign disorder without further workup. Often best seen on an oblique radiograph, the lack of soft-tissue mass or bone destruction leads to the benign diagnosis. Serial radiographs typically show complete resolution by age 20.
RECOMMENDED READINGS
25. [Gould CF, Ly JQ, Lattin GE Jr, Beall DP, Sutcliffe JB 3rd. Bone tumor mimics: avoiding misdiagnosis. Curr Probl Diagn Radiol. 2007 May-Jun;36(3):124-41. Review. PubMed PMID: 17484955. ](http://www.ncbi.nlm.nih.gov/pubmed/17484955)[View](http://www.ncbi.nlm.nih.gov/pubmed/17484955)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17484955)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17484955)
26. [Yamazaki T, Maruoka S, Takahashi S, Saito H, Takase K, Nakamura M, Sakamoto K. MR findings of avulsive cortical irregularity of the distal femur. Skeletal Radiol. 1995 Jan;24(1):43-6. PubMed PMID: 7709251. ](http://www.ncbi.nlm.nih.gov/pubmed/7709251)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7709251)
27. [Damron TA, Morris C, Rougraff B, Tamurian R. Diagnosis and treatment of joint-related tumors that mimic sports-related injuries. Instr Course Lect. 2009;58:833-47. PubMed PMID: 19385590. ](http://www.ncbi.nlm.nih.gov/pubmed/19385590)[View](http://www.ncbi.nlm.nih.gov/pubmed/19385590)[ ](http://www.ncbi.nlm.nih.gov/pubmed/19385590)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19385590)
RECOMMENDED READINGS
25. [Gould CF, Ly JQ, Lattin GE Jr, Beall DP, Sutcliffe JB 3rd. Bone tumor mimics: avoiding misdiagnosis. Curr Probl Diagn Radiol. 2007 May-Jun;36(3):124-41. Review. PubMed PMID: 17484955. ](http://www.ncbi.nlm.nih.gov/pubmed/17484955)[View](http://www.ncbi.nlm.nih.gov/pubmed/17484955)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17484955)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17484955)
26. [Yamazaki T, Maruoka S, Takahashi S, Saito H, Takase K, Nakamura M, Sakamoto K. MR findings of avulsive cortical irregularity of the distal femur. Skeletal Radiol. 1995 Jan;24(1):43-6. PubMed PMID: 7709251. ](http://www.ncbi.nlm.nih.gov/pubmed/7709251)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7709251)
27. [Damron TA, Morris C, Rougraff B, Tamurian R. Diagnosis and treatment of joint-related tumors that mimic sports-related injuries. Instr Course Lect. 2009;58:833-47. PubMed PMID: 19385590. ](http://www.ncbi.nlm.nih.gov/pubmed/19385590)[View](http://www.ncbi.nlm.nih.gov/pubmed/19385590)[ ](http://www.ncbi.nlm.nih.gov/pubmed/19385590)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19385590)
Question 30High Yield
Figure 1
A 59-year-old woman presents for treatment of a painful hallux valgus deformity. She has a prominent bunion, normal motion of the hallux metatarsophalangeal (MP) joint, and painful callosity under the second MP joint. Radiographs of the foot are
presented. The recommended treatment is:
A 59-year-old woman presents for treatment of a painful hallux valgus deformity. She has a prominent bunion, normal motion of the hallux metatarsophalangeal (MP) joint, and painful callosity under the second MP joint. Radiographs of the foot are
presented. The recommended treatment is:
Explanation
This patient has probable instability of the metatarsocuneiform joint manifested by the overload phenomenon of the second metatarsal. Although this is not a sufficient indication for performing an arthrodesis of the metatarsocuneiform joint (modified Lapidus procedure), other findings of second metatarsal overload, including thickening of the cortex of the second metatarsal and instability of the first metatatarsocuneiform joint, should be looked for in addition to hypermobility of the first ray.
Question 31High Yield
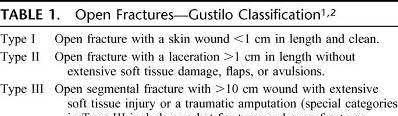
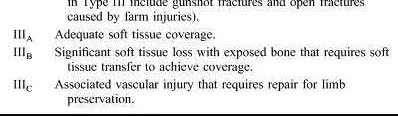
A 25-year-old male pedestrian sustained a Type II open tibia fracture after being struck by a car at 10:00PM. He was transported to a Level I trauma hospital where he was given intravenous antibiotics
and tetanus at 10:45PM. He underwent irrigation and debridement of the wound with 9L of saline solution and was treated with reamed intramedullary nail fixation at 11:45PM. A vacuum assisted dressing was placed over a 5x3cm skin deficit. What part of his overall treatment has shown to reduce the risk of infection THE MOST at the site of injury?
and tetanus at 10:45PM. He underwent irrigation and debridement of the wound with 9L of saline solution and was treated with reamed intramedullary nail fixation at 11:45PM. A vacuum assisted dressing was placed over a 5x3cm skin deficit. What part of his overall treatment has shown to reduce the risk of infection THE MOST at the site of injury?
Explanation
The most important factor shown to reduce the risk of infection at the site of an open fracture is early intravenous antibiotic administration.
Infection risk after Gustilo Type II open fractures ranges from 10-20% in large studies. Antibiotic treatment initiated within 3 hours from the time of injury has shown to significantly reduce the rate of infection. Antibiotic coverage for Type II open fractures should cover gram positive bacteria. Soil-contaminated wounds should include anaerobic coverage. The dose of antibiotic given must be within a therapeutic range and titrated to the patient's weight (e.g. Ancef 2 g IV for >70 kg). Duration of antibiotic therapy has been suggested to be between 1 and 3 days, although there is no agreement on a firm end point.
Pollak et al. reviewed a large cohort of open fractures treated at Level I trauma centers. They demonstrated a significant decrease in infection rate with either early direct admission (<2 hours) or transfer (<11 hours) for ONLY type III open tibia fractures. They did not not discuss timing of antibiotic treatment because this was not prospectively collected. Although they did not collect data on antibiotic treatment, the authors theorize that early transfer potentially resulted in earlier administration of antibiotics.
Patzakis et al. examined a series of 1104 open fractures to determine the factors contributing to infection. They showed the most important factor in reducing the infection rate was the early administration of antibiotics.
Illustration A is table showing the Gustilo classification of open fractures. Incorrect Answers
Answers 1,4: These responses have been shown to reduce the risk of infection
in open fractures, however, the most important factor has been shown to be
early antibiotic therapy.
Answer 3: Reamed intramedullary nailing has not been shown to decrease infection risk in open tibia fractures, however, skeletal stability will prevent ongoing soft tissue damage
Answer 5: Vacuum-assisted wound dressings (or negative pressure wound therapy) are controversial as to whether they provide any protective effect against infection.
Infection risk after Gustilo Type II open fractures ranges from 10-20% in large studies. Antibiotic treatment initiated within 3 hours from the time of injury has shown to significantly reduce the rate of infection. Antibiotic coverage for Type II open fractures should cover gram positive bacteria. Soil-contaminated wounds should include anaerobic coverage. The dose of antibiotic given must be within a therapeutic range and titrated to the patient's weight (e.g. Ancef 2 g IV for >70 kg). Duration of antibiotic therapy has been suggested to be between 1 and 3 days, although there is no agreement on a firm end point.
Pollak et al. reviewed a large cohort of open fractures treated at Level I trauma centers. They demonstrated a significant decrease in infection rate with either early direct admission (<2 hours) or transfer (<11 hours) for ONLY type III open tibia fractures. They did not not discuss timing of antibiotic treatment because this was not prospectively collected. Although they did not collect data on antibiotic treatment, the authors theorize that early transfer potentially resulted in earlier administration of antibiotics.
Patzakis et al. examined a series of 1104 open fractures to determine the factors contributing to infection. They showed the most important factor in reducing the infection rate was the early administration of antibiotics.
Illustration A is table showing the Gustilo classification of open fractures. Incorrect Answers
Answers 1,4: These responses have been shown to reduce the risk of infection
in open fractures, however, the most important factor has been shown to be
early antibiotic therapy.
Answer 3: Reamed intramedullary nailing has not been shown to decrease infection risk in open tibia fractures, however, skeletal stability will prevent ongoing soft tissue damage
Answer 5: Vacuum-assisted wound dressings (or negative pressure wound therapy) are controversial as to whether they provide any protective effect against infection.
Question 32High Yield
The nerve most commonly injured during total hip arthroplasty (THA) is the:
Explanation
The primary nerves of the region are the sciatic, femoral, inferior and superior gluteal, and obturator. The most common nerve injury during THA is to the peroneal division of the sciatiCnerve, followed by superior gluteal, obturator, and femoral nerves. Injury to these structures can lead to loss of function and poor outcomes
Question 33High Yield
Figure 1 is the radiograph of a 31-year-old man who had left shoulder pain after a fall during a snowboarding jump. Residual displacement of 5 mm after closed reduction is most likely to result in
---
---

Explanation
Humerus fractures account for 11% of all fractures among snowboarders and are the second-most-common upper-extremity fracture after radius fractures (48%). Surgical fixation is recommended for fractures with residual displacement >5 mm, or >3 mm in active patients involved in frequent overhead activity. Malunion can result in a mechanical block to shoulder abduction or external rotation and altered rotator cuff mechanics, causing weakness. A rich arterial network provides a favorable healing environment for greater tuberosity fractures. Consequently, nonunion and osteonecrosis are uncommon.
Question 34High Yield
Figure 7 shows the CT scan of a 25-year-old soccer player who has had posterior ankle pain with plantar flexion for the past 2 years. Immobilization has failed to provide relief. He is ambulatory. Management should consist of
Explanation
An os trigonum is usually asymptomatic, but this accessory bone has been associated with persistent posterior ankle pain, which has been described as os trigonum syndrome. This usually affects athletes and ballerinas. Forced plantar flexion leads to impingement of the os trigonum against the posterior tibial plafond, and flexor hallucis tendinitis may develop. It may be difficult to differentiate a fractured trigonal process from the os trigonum. MRI may reveal bone marrow edema that may aid in the diagnosis of os trigonum syndrome. Steroid injections may lead to tendon rupture. The results of excision of a symptomatic os trigonum through a posteromedial or lateral approach are favorable, with a rapid return to full function. The main complication of this procedure is sural nerve injury with a lateral approach.
REFERENCES: Hedrick MR, McBryde AM: Posterior ankle impingement. Foot Ankle Int 1994;15:2-8.
Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057.
REFERENCES: Hedrick MR, McBryde AM: Posterior ankle impingement. Foot Ankle Int 1994;15:2-8.
Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057.
Question 35High Yield
..A 55-year-old woman develops posttraumatic arthritis in the elbow following a distal humerus fracture. What is the most likely mid-term (5-10 years after surgery) complication following semiconstrained total elbow arthroplasty (TEA)?
Explanation
- Bushing wear
CLINICAL SITUATION FOR QUESTIONS 21 AND 22
A 21-year-old rugby player has had the sensation of shoulder instability while making tackles for 3 years. Two years ago, he had an arthroscopic Bankart repair and capsulorrhaphy that used 3 suture anchors after dislocating his shoulder while making a tackle. This procedure required an emergency department sedated reduction. After this dislocation, he had paresthesias in his arm and a sense of weakness. His numbness eventually resolved. He did well after surgery until 2 weeks ago, when he again felt his shoulder dislocate while tackling and had an emergency department reduction.
CLINICAL SITUATION FOR QUESTIONS 21 AND 22
A 21-year-old rugby player has had the sensation of shoulder instability while making tackles for 3 years. Two years ago, he had an arthroscopic Bankart repair and capsulorrhaphy that used 3 suture anchors after dislocating his shoulder while making a tackle. This procedure required an emergency department sedated reduction. After this dislocation, he had paresthesias in his arm and a sense of weakness. His numbness eventually resolved. He did well after surgery until 2 weeks ago, when he again felt his shoulder dislocate while tackling and had an emergency department reduction.
Question 36High Yield
At the time of arthroscopy, the posterior humeral head Hill-Sachs lesion substantially engages with the glenoid; CT and arthroscopic findings reveal minimal glenoid bone loss. In addition to arthroscopic Bankart repair, arthroscopic Hill-Sachs remplissage with suture anchors is performed. In combined Bankart repair with Hill-Sachs remplissage vs Bankart repair alone, which complication is of highest potential concern?
Explanation
- Loss of shoulder external rotation of approximately 10 degrees vs the uninjured shoulder_
Question 37High Yield
Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease that is characterized by
Explanation
CTE is a neurodegenerative disease that occurs years or decades after recovery from acute or postacute effects of head trauma. The exact relationship between concussion and CTE is not entirely clear; however, early behavioral manifestations of CTE have been described by family and providers to include apathy, irritability, and suicidal ideation. For some patients, cognitive difficulty such as poor episodic memory and executive function may be the first signs of CTE. Onset most often occurs in midlife after athletes have completed their sports careers, with mean age of onset at 42 years. The effects on the brain are degenerative, leading to a permanent state of derangement. Autopsy findings demonstrate multiple gross pathological findings. The condition is more common among contact athletes.
Question 38High Yield
A 58-year-old man has had a 3-year history of recurrent ulcerations of the left ankle and instability despite multiple attempts at custom bracing, contact casting, and surgical debridement. He has an ankle-brachial index of 0.76. A clinical photograph and radiographs are shown in Figures 16a through 16c. Treatment should now consist of
Explanation
Nonsurgical management has failed to provide relief; therefore, the treatment of choice is arthrodesis with an intramedullary nail. Amputation may be indicated if the arthrodesis fails. The patient does have adequate circulation for an attempt at salvage. Total ankle arthroplasty is not indicated in a neuropathic patient.
REFERENCES: Pinzur MS, Kelikian A: Charcot ankle fusion with a retrograde locked intramedullary nail. Foot Ankle Int 1997;18:699-704.
Herbst SA: External fixation of Charcot arthropathy. Foot Ankle Clin 2004;9:595-609.
REFERENCES: Pinzur MS, Kelikian A: Charcot ankle fusion with a retrograde locked intramedullary nail. Foot Ankle Int 1997;18:699-704.
Herbst SA: External fixation of Charcot arthropathy. Foot Ankle Clin 2004;9:595-609.
Question 39High Yield
Which of the following is a significant risk factor for a stress fracture:
Explanation
There are a number of risk factors for stress fractures:
A. Menstrual irregularity in women is perhaps the most significant risk factor.
1/. Remember the terrible triad in female patients:
a. Menstrual irregularity b. Eating disorders
c. Low bone mass
B. Increase in frequency and intensity of athletic training or activity
C . C hanges in athletic training are noted in 80% of athletes surveyed who have stress fractures. D. Decreased tibial width (smaller bone size)
E. Factors that have not been found to be statistically significant include:
1/. Testosterone levels in male athletes
2/. Age
a. Location by age is significant, but not etiology
3/. Training surfaces
4/. Flexibility
5/. Low calcium intake
C orrect Answer: Increase in frequency and intensity of training
A. Menstrual irregularity in women is perhaps the most significant risk factor.
1/. Remember the terrible triad in female patients:
a. Menstrual irregularity b. Eating disorders
c. Low bone mass
B. Increase in frequency and intensity of athletic training or activity
C . C hanges in athletic training are noted in 80% of athletes surveyed who have stress fractures. D. Decreased tibial width (smaller bone size)
E. Factors that have not been found to be statistically significant include:
1/. Testosterone levels in male athletes
2/. Age
a. Location by age is significant, but not etiology
3/. Training surfaces
4/. Flexibility
5/. Low calcium intake
C orrect Answer: Increase in frequency and intensity of training
Question 40High Yield
A patient has sustained the injury shown in the MRI scan in Figure

Explanation
■
The MRI cervical spine scan reveals a C4-C5 traumatic anterolisthesis with severe spinal stenosis. There is evidence of spinal cord swelling and myelomalacia at this level. A physical examination is provided. The ASIA scale provides grading of severity of a spinal cord injury.
The grading incorporates strength and motor function based on the spinal level.
ASIA A is a complete spinal cord injury with no motor or sensory function. ASIA B is an incomplete spinal cord injury with no motor function below the spinal level of injury and sacral sparing of sensation. ASIA C is an incomplete spinal cord injury with motor function <3 of 5 in more than half of the muscles below the spinal level of injury. ASIA D is an incomplete spinal cord injury with motor function >3 of 5 in at least half of the muscles below the spinal level of injury. ASIA E is normal sensation and motor function.
The MRI cervical spine scan reveals a C4-C5 traumatic anterolisthesis with severe spinal stenosis. There is evidence of spinal cord swelling and myelomalacia at this level. A physical examination is provided. The ASIA scale provides grading of severity of a spinal cord injury.
The grading incorporates strength and motor function based on the spinal level.
ASIA A is a complete spinal cord injury with no motor or sensory function. ASIA B is an incomplete spinal cord injury with no motor function below the spinal level of injury and sacral sparing of sensation. ASIA C is an incomplete spinal cord injury with motor function <3 of 5 in more than half of the muscles below the spinal level of injury. ASIA D is an incomplete spinal cord injury with motor function >3 of 5 in at least half of the muscles below the spinal level of injury. ASIA E is normal sensation and motor function.
Question 41High Yield
A 20-year-old woman is involved in a high-speed motor vehicle collision and sustains bilateral tibial plateau fractures as well as the clavicle fracture shown in Figure A. What is the most appropriate management of the clavicular injury?

Explanation
The radiograph shows a comminuted clavicle fracture with significant displacement. Indications for surgical fixation of clavicle fractures include: open fractures, underlying neurovascular injury, or impending open fracture from internal bony pressure causing skin compromise. Relative indications for fixation include: greater than 15 mm of shortening, greater than 100% displacement (no bony contact), highly comminuted fractures, and polytrauma patients.
Jeray et al review the evaluation and treatment of midshaft clavicle fractures. They state "when midshaft clavicular fractures are completely displaced or comminuted, and when they occur in elderly patients or females, the risk of nonunion, cosmetic deformity, and poor outcome may be markedly higher.
Thus, some surgeons propose surgical stabilization of a complex midshaft
clavicular fracture with either plate-and-screw fixation or intramedullary devices. Further randomized, prospective trials are needed to provide better data on which to base treatment decisions."
Jeray et al review the evaluation and treatment of midshaft clavicle fractures. They state "when midshaft clavicular fractures are completely displaced or comminuted, and when they occur in elderly patients or females, the risk of nonunion, cosmetic deformity, and poor outcome may be markedly higher.
Thus, some surgeons propose surgical stabilization of a complex midshaft
clavicular fracture with either plate-and-screw fixation or intramedullary devices. Further randomized, prospective trials are needed to provide better data on which to base treatment decisions."
Question 42High Yield
A 63-year-old woman presents for treatment of pain and a burning/tingling sensation along the medial aspect of the foot and hallux. She underwent a tarsal tunnel release 12 months ago, but she has not experienced much symptomatic relief. Upon clinical examination, she has a positive percussion test (Tinel sign) along the course of the distal tibial nerve and pain upon pressure of the tarsal canal. There are no other pertinent clinical findings and a magnetic resonance image does not reveal any pathologic lesion. The next course of treatment is:
Explanation
This patient presents with symptoms of a tarsal tunnel syndrome, specifically involving the medial plantar nerve. Because she did not experience any initial pain relief from her surgery, one may suspect that an inadequate release was initially performed. C ortisone injection and physical therapy have no role in the management of a recurrent tarsal tunnel syndrome, although desensitization treatments with neuroleptic medication and manual massage are beneficial following surgery. It is important to rule out a sympathetically mediated pain syndrome prior to embarking on repeat surgery.
Question 43High Yield
A 65-year-old woman with diabetes has fever and erythema 2 weeks after undergoing instrumented spinal fusion.
Explanation
- Postoperative deep surgical site infection
Question 44High Yield
A 20-year-old collegiate baseball pitcher has persistent deep shoulder pain. Examination reveals normal strength, 130 degrees of external rotation in abduction, 10 degrees of internal rotation in abduction, mild dynamic scapular winging, and equivocal findings on provocative tests for labral tears. Management should consist of
Explanation
Although management of shoulder pain in the throwing athlete is controversial, there are some general principles. Initial management generally includes rest from throwing, restoring normal joint function, specifically motion and strength as well as eliminating pain. In this patient, examination reveals excessive external rotation and decreased internal rotation. This pattern is common in pitchers; however, the total arc of motion should remain close to 180 degrees in abduction. In this patient, the total arc is 140 degrees. Treatment should first focus on restoring a 180-degree arc with posterior scapular stretching, as well as pain control and muscle rehabilitation. Injections and surgery are generally reserved for patients who fail to respond to rest and rehabilitation.
REFERENCE: Burkhart SS, Morgan CD, Kibler WB: Shoulder injuries in overhead athletes: The “dead arm” revisited. Clin Sports Med 2000;19:125-158.
REFERENCE: Burkhart SS, Morgan CD, Kibler WB: Shoulder injuries in overhead athletes: The “dead arm” revisited. Clin Sports Med 2000;19:125-158.
Question 45High Yield
A 29-year-old woman reports dysesthesias and burning after undergoing bunion surgery that consisted of a proximal crescentic first metatarsal osteotomy 6 months ago. Examination reveals a positive Tinel’s sign at the proximal aspect of the healed incision. What injured nerve is responsible for her continued symptoms?
Explanation
Painful incisional neuromas after bunion surgery frequently involve the dorsomedial cutaneous branch of the superficial peroneal nerve. This is the medial branch of the superficial peroneal nerve that terminates as the dorsomedial cutaneous nerve to the hallux. Branches of the deep peroneal nerve to this area are rare, and no branches to this area exist from the sural nerve. The saphenous nerve branches are generally more proximal, and the medial plantar nerve lies plantarly.
REFERENCES: Kenzora JE: Sensory nerve neuromas: Leading to failed foot surgery. Foot Ankle 1986;7:110-117.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
REFERENCES: Kenzora JE: Sensory nerve neuromas: Leading to failed foot surgery. Foot Ankle 1986;7:110-117.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 46High Yield
Bacterial resistance to tetracycline is confirmed by ribosome protection, tetracycline modification, and
Explanation
**
Mutations of bacterial DNA gyrase can decrease the effectiveness of quinolones. Altered membrane-binding protein is observed with resistance to ?
-lactam antibiotics. Tetracyclines are antibiotics that inhibit bacterial growth by stopping protein synthesis. Three specific mechanisms of tetracycline
resistance have been identified: increased tetracycline efflux, ribosome protection, and tetracycline modification. Alteration of RNA polymerase is found in resistance to rifampin.
Mutations of bacterial DNA gyrase can decrease the effectiveness of quinolones. Altered membrane-binding protein is observed with resistance to ?
-lactam antibiotics. Tetracyclines are antibiotics that inhibit bacterial growth by stopping protein synthesis. Three specific mechanisms of tetracycline
resistance have been identified: increased tetracycline efflux, ribosome protection, and tetracycline modification. Alteration of RNA polymerase is found in resistance to rifampin.
Question 47High Yield
Contraindications to high tibial osteotomy include:
Explanation
Lateral compartment narrowing, lateral tibial subluxation of more than 1 cm, medial compartment bone loss of more than 3 mm, and ligament instability are contraindications to high tibial osteotomy
Question 48High Yield
Which of the following statements best characterizes a Dega osteotomy as a distinct osteotomy from a Salter osteotomy:
Explanation
The Dega osteotomy, originally described in Poland in 1964, is an incomplete transiliac osteotomy. The medial pelvic cortex is largely preserved, and the osteotomy hinges upon this point. Both osteotomies are best performed in young children, before triradiate cartilage closure. The Salter osteotomy is stabilized by pins, so the Dega needs no internal fixation. The Salter osteotomy lengthens the limb because it is a complete osteotomy.
Question 49High Yield
A 5-year-old girl with increasing lower extremity bowing and short stature is diagnosed to have X-linked hypophosphatemic rickets. The underlying pathology is due to

Explanation
■
X-linked hypophosphatemic rickets is the most common form of inheritable rickets and is inherited in an Xlinked dominant fashion. It is caused by mutations in the phosphate–regulating endopeptidase homolog Xlinked gene, which are expressed in osteocytes. Mutation of this gene results in an increase in fibroblast growth factor -23, which then leads to reduction of the proteins involved in renal phosphate reabsorption and 1,25OH vitamin D production. This leads to phosphaturia and ultimately in decreased mineralization of the long bones and teeth.
Alkaline phosphatase deficiency causes hypophosphatasia and is a recessive condition.1 α-hydroxylase deficiency patients cannot convert 25-hydroxyvitamin D3 to its active form 1,25 dihydroxyvitamin D3, and therefore develop clinical rickets. Carbonic anhydrase deficiency prevents the osteoclasts from acidifying the extracellular space at their ruffled border, which then leads to osteoclast dysfunction and diminished reabsorption of the bone and osteopetrosis.
X-linked hypophosphatemic rickets is the most common form of inheritable rickets and is inherited in an Xlinked dominant fashion. It is caused by mutations in the phosphate–regulating endopeptidase homolog Xlinked gene, which are expressed in osteocytes. Mutation of this gene results in an increase in fibroblast growth factor -23, which then leads to reduction of the proteins involved in renal phosphate reabsorption and 1,25OH vitamin D production. This leads to phosphaturia and ultimately in decreased mineralization of the long bones and teeth.
Alkaline phosphatase deficiency causes hypophosphatasia and is a recessive condition.1 α-hydroxylase deficiency patients cannot convert 25-hydroxyvitamin D3 to its active form 1,25 dihydroxyvitamin D3, and therefore develop clinical rickets. Carbonic anhydrase deficiency prevents the osteoclasts from acidifying the extracellular space at their ruffled border, which then leads to osteoclast dysfunction and diminished reabsorption of the bone and osteopetrosis.
Question 50High Yield
Figures 33a through 33d are the radiograph, MR images, and biopsy specimen of a 66-year-old woman with a several-month history of an enlarging thigh mass after “pulling a muscle” while playing softball. Several weeks ago her physician aspirated the cyst, but the result is no change. Treatment of this lesion should include

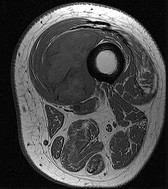
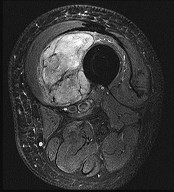
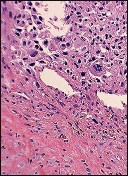
Explanation
This patient’s imaging and biopsy specimen are consistent with a high-grade undifferentiated pleomorphic sarcoma (UPS). Histologically, UPS is characterized by high cellularity, marked nuclear pleomorphism, abundant mitotic activity (including atypical mitoses), and a spindle cell morphology. Necrosis is common and characteristic of high-grade lesions. Treatment consists of wide surgical excision and, in almost all cases, radiation. Radiation eliminates the need for limb amputation, and there is level I evidence to show that it leads to equivalent rates of survival. Radiation may be delivered either before or after surgery depending on the surgeon’s and multidisciplinary tumor board’s recommendations. There may be a role for presurgical embolization in some cases of high-grade soft-tissue sarcoma, but this is not appropriate as a standalone treatment. Chemotherapy provides limited survival improvement in adults with high-grade soft-tissue sarcomas.
RECOMMENDED READINGS
13. [Bell RS, O'Sullivan B, Davis A, Langer F, Cummings B, Fornasier VL. Functional outcome in patients treated with surgery and irradiation for soft tissue tumours. J Surg Oncol. 1991 Dec;48(4):224-31. PubMed PMID: 1745046. ](http://www.ncbi.nlm.nih.gov/pubmed/1745046)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1745046)
14. [O'Sullivan B, Wylie J, Catton C, Gutierrez E, Swallow CJ, Wunder J, Gullane P, Neligan P, Bell R. The local management of soft tissue sarcoma. Semin Radiat Oncol. 1999 Oct;9(4):328-48. Review. PubMed PMID: 10516380. ](http://www.ncbi.nlm.nih.gov/pubmed/10516380)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10516380)
RECOMMENDED READINGS
13. [Bell RS, O'Sullivan B, Davis A, Langer F, Cummings B, Fornasier VL. Functional outcome in patients treated with surgery and irradiation for soft tissue tumours. J Surg Oncol. 1991 Dec;48(4):224-31. PubMed PMID: 1745046. ](http://www.ncbi.nlm.nih.gov/pubmed/1745046)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1745046)
14. [O'Sullivan B, Wylie J, Catton C, Gutierrez E, Swallow CJ, Wunder J, Gullane P, Neligan P, Bell R. The local management of soft tissue sarcoma. Semin Radiat Oncol. 1999 Oct;9(4):328-48. Review. PubMed PMID: 10516380. ](http://www.ncbi.nlm.nih.gov/pubmed/10516380)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10516380)
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon