Ortho Free Review | Dr Hutaif General Orthopedics Revie -...
14 Apr 2026
126 min read
83 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Ortho Free Review | Dr Hutaif General Orthope...
00:00
Start Quiz
Question 1High Yield
Figure 1 is the T2 coronal MRI scan of a 52-year-old woman with a 6- month history of shoulder pain. She does not recall a history of trauma. Physical therapy is recommended. What is the most significant predictor of failure of nonoperative treatment?
Explanation
The MRI reveals a large full thickness supraspinatus tear. A large, prospective study showed that physical therapy can be effective in the treatment of atraumatic full-thickness rotator cuff tears. Patient expectations regarding the role of rehabilitation were the strongest predictor of surgery. Other
factors associated with surgery were higher activity level and not smoking. Anatomic features of the rotator cuff tear and the severity of patient’s reported pain did not predict failure of nonoperative treatment. Patients who have low expectations regarding the effectiveness of physical therapy are more likely to fail nonoperative treatment.
factors associated with surgery were higher activity level and not smoking. Anatomic features of the rotator cuff tear and the severity of patient’s reported pain did not predict failure of nonoperative treatment. Patients who have low expectations regarding the effectiveness of physical therapy are more likely to fail nonoperative treatment.
Question 2High Yield
This series of lab values is consistent with a diagnosis of hypoparathroidism. 5-This series of lab values is consisten with a diagnosis of primary hyperparathryoidism.
A 28-year-old African-American male with a history of Sickle Cell Disease complains of progressive left hip pain for the past two years. He denies any causative injuries. His images are shown in Figures A and B. Which of the following mechanisms is most likely responsible for his symptoms?
A 28-year-old African-American male with a history of Sickle Cell Disease complains of progressive left hip pain for the past two years. He denies any causative injuries. His images are shown in Figures A and B. Which of the following mechanisms is most likely responsible for his symptoms?





















































Explanation
The clinical presentation and images are most consistent with left hip osteonecrosis as a result of coagulation and vascular occlusion caused by sickle cell anemia.
Sickle cell disease is a genetic disorder of hemoglobin synthesis characterized by 2 abnormal hemoglobin S alleles. Under low oxygen conditions the affected blood cells become "sickle shaped" and unable to pass through vessels. This results in vascular occlusion that may have a variety of clinical consequences depending on the body part affected.
Hernigou et al. review the natural history of symptomatic osteonecrosis in adults with sickle cell disease. Once symptomatic , osteonecrosis of the hip in sickle cell disease has a high likelihood of progressing and leading to femoral head collapse. Deterioration can be rapid and in most patients operative intervention is necessary to prevent further collapse or alleviate intractable pain.
Mont et al. performed a literature review on the natural history of untreated asymptomatic osteonecrosis of the femoral head. Their findings supported that asymptomatic osteonecrosis had a high prevalence of progression to symptomatic femoral head collapse. Small, medially located lesions had a low rate of progression, while medium to large sized osteonecrotic lesions did progress in a substantial number of patients. They recommended
consideration of joint-preserving surgical treatment in asymptomatic patients with a medium-sized or large, laterally located lesion.
Figure A shows an AP pelvis with left hip osteonecrosis. Figure B shows a T2 coronal MRI with left hip osteonecrosis. Illustration A shows an example of a hemoglobin molecule which has become "sickle shaped," and as a result is unable to pass through vessels efficiently.
Incorrect Answers:
: Progressive slippage of the physis though the hypertrophic zone describes
slipped capital femoral epiphysis.
Answer 3: These radiographs are most consistent with osteonecrosis of the femoral head. There is an increased incidence of Salmonella osteomyelitis in patient with Sickle Cell disease, but Staphylococcus aureus is still the most common organism.
Answer 4: Accumulation of glycosaminoglycan breakdown products describes lysosomal disorders.
Answer 5: COL5A1 or COL5A2 mutation describes the mutation of Ehlers Danlos syndrome.
What mechanism allows Staphylococcus epidermidis to adhere to surfaces and resist phagocytosis?
1) Creation of active efflux pumps
2) Methylation of 23s rRNA
3) Biofilm production
4) Alteration of cell wall permeability
5) Beta-lactamase production
Staphylococcus epidermidis is a gram-positive bacteria that utilizes a glycocalyx/biofilm to adhere to orthopedic implants and other surfaces and resist phagocytosis.
The biofilm creates a well-protected environment where bacteria can proliferate and thrive essentially undetected by the host immune system. This leads to chronic infections of orthopedic implants that can go undetected for years.
Arciola et al note that S. epidermidis can colonize surfaces in a self-generated viscous biofilm composed of polysaccharides and that the ica genes found in
56% of S. epidermidis isolates were associated with their ability to produce biofilm.
Olson et al discuss the importance of polysaccharide intercellular adhesin (PIA), a
substance produced by 50-60% of S. epidermidis strains, in the adherence of S. epidermidis to biomaterials through biofilm creation. PIA plays a critical role in initial adherence of S. epidermidis to biomaterials, biofilm
maturation and aggregation.
Illustration A shows microscopy of Staphylococcus epidermidis, which is a gram- positive, coagulase-negative cocci. Illustration B is an overview of the different classes of organisms in microbiology.
Incorrect Answers:
Answer 1,2,4,5: Efflux pump production, hydrolysis of B-lactam drugs with beta- lactamase, alteration in cell wall permeability, and ribosomal alteration are mechanisms that Staphylococcus uses to resists antibiotics.
Compared to cold-forged cobalt chrome, titanium alloys have which property?
1) Increased fatigue strength
2) Increased yield strength
3) Increased endurance limit
4) Decreased ductility
5) Decreased tensile strength
Titanium implants have decreased tensile (ultimate) strength when compared to cobalt chrome.
Ultimate strength, or tensile strength, is the maximum stress a material can withstand before undergoing breakage or failure. The ranking of ultimate strength, from highest to lowest is: 1) cobalt chrome, 2)titanium, 3)stainless steel, and 4) cortical bone.
Young's modulus of elasticity is defined as the measure of stiffness of a material in the elastic zone. A higher Young's modulus indicates a stiffer material. While titanium is highly biocompatible with a low modulus of elasticity (Young's modulus), it has poor wear characteristics making it non- suitable for femoral heads in total hip arthroplasty.
Long et al. present a review on titanium implants with a focus on bio- mechanical properties. Their study supports previous data which showed high rates of ultra-high molecular weight polyethylene wear due to accelerated breakdown when in contact with a titanium surface.
Incorrect Answers:
Answer 1: Fatigue strength, or the maximum cyclic load (10 million cycles) that a standard sized metal can absorb before fracture, is lower in titanium compared to cobalt chrome.
Answer 2: Yield strength, or the maximal stress a material can take before permanent deformation, is decreased in titanium compared to cobalt chrome. Answer 3: Endurance limit is another way of saying fatigue strength, which is discussed in incorrect answer 1. Answer 4: Ductility, or the measure of how much strain a material can take before rupturing, is higher for titanium than cobalt chrome
Peak bone mass attainment in both men and women is most dependent on which sex-steroid?
1) Testosterone
2) Progesterone
3) Growth Hormone
4) Estrogen
5) Cortisol
Estrogen has been shown to be important for both men and women in attaining peak bone mass.
Risk factors for osteoporosis are: increasing age, female sex, early menopause, fair-skinned, family history of hip fracture, low body weight, smoking, glucocorticoid use, excessive alcohol, low protein intake, and anticonvulsant or antidepressant use.
Which of the following contributes most to the ability of hyaline cartilage to attract water?
1) Aggrecan
2) Biglycan
3) Decorin
4) Fibromodulin
5) Osteocalcin
Aggrecan molecules bind to hyaluronic acid molecules via link proteins to form a macromolecule complex, known as a proteoglycan aggregate, which attracts water.
Proteoglycans are composed of subunits known as glycosaminoglycans. Glycosaminoglycans include two subtypes: chondroitin sulfate and keratin sulfate. These glycosaminoglycans link to a protein core by sugar bonds to form an aggrecan molecule. Link proteins then stabilize many of these aggrecan molecules to hyaluronic acid to form the proteoglycan aggregate. Cartilage also contains ancillary proteoglycans that are much smaller than the aggregating proteoglycans. These small proteoglycans include decorin, biglycan, and fibromodulin. They bind to other molecules (eg, type II collagen) and assist in matrix stabilization.
Ulrich-Vinther et al. authored a Level 5 review on cartilage structure. The negative charge present within the hyaline cartilage extracellular matrix attracts cations and results in an increase in tissue osmolality. This then attracts water, which decreases the osmolality. Thus, articular cartilage has a high tissue pressure, but the presence of type II collagen matrix prevents it from swelling.
Nap et al. present a basic science review article on aggrecans. They discus that the main function of aggrecan in cartilage is to resist compressive forces.
They note that the negative charge of the aggrecan molecule disaccharides create the high osmotic swelling pressure of cartilage.
Illustration A depicts the molecular organization of an aggregated proteoglycan molecule. Incorrect Answers:
Answer 2,3,4: These are small proteoglycans that bind to other molecules (eg, type II collagen) and assist in matrix stabilization.
Answer 5: Osteocalcin is the most prevalent noncollagenous protein in bone.
What effect do bisphosphonate medications have on spinal fusion surgery when taken in the postoperative period?
1) Any effect can be counteracted by taking calcium supplements
2) No effect
3) Increased risk of wound infection
4) Smaller fusion mass
5) Decreased fusion rate
Bisphosphonates (e.g. alendronate) are used to treat osteoporosis. The mechanism of action is inhibiting the formation of the ruffled border of osteoclasts, resulting in decreasing bone turnover.
Huang et al performed a rat study comparing alendronate to placebo and found that fusion rates were lower in those treated with alendronate. However,
the fusion masses were larger in the alendronate treated rats despite lower fusion rates (why #4 is incorrect).
Lehman et al in another placebo controlled rate study found that the fusion rates for placebo (76%) were greater than the alendronate group (45%). Alendronate works on osteoclasts and does not affect calcium directly. Taking calcium should have no effect on alendronate (why #1 is incorrect). At this time there are no formal recommendations of when to stop bisphosphonate medication prior to spinal fusion surgery.
A therapeutic study presents a systematic review of 15 high- quality randomized controlled trials with homogeneous results. What level of evidence is this considered?
1) I
2) II
3) III
4) IV
5) V
A systematic review of high-quality clinical trials is considered a Level I study.
A systematic review is a powerful tool used to identify, evaluate and appraise all high- quality research related to a specific question. Systematic reviews, in contrast to most narrative review articles, adhere to strict scientific design by following eight steps; 1) defining a question and developing inclusion criteria,
2) searching for studies, 3) selecting studies and collecting data, 4) assessing risk of bias, 5) data analysis and meta-analyses, 6) addressing biases, 7) presenting results, and 8) interpreting results and drawing conclusions. When the results from the systematic review are homogeneous (less variability between studies than would be expected by chance), the data from a systematic review can be combined into a meta- analysis.
Wright et al. discuss the levels of evidence in orthopaedic journals as presented by the AAOS Evidence-Based Practice Committee. Based on levels of evidence, the AAOS provides grades of recommendation (A, B, C, I). Grade A recommendations are supported by Level 1 studies with consistent findings, whereas Grade I do not have enough evidence to support a recommendation.
Illustration A shows an "evidence pyramid." MA = meta-analysis, SR = systematic review, RCT = randomized controlled trial.
Incorrect Answers:
Answer 2: An example of a Level II study is prospective comparative study. Answer 3: An example of a Level III study is a case control trial.
Answer 4: An example of a Level IV study is a case series.
Answer 5: An example of a Level V study is one based on expert opinion.
Progressive overloading of muscles in adults during exercise leads to which of the following?
1) Increased muscle fiber length
2) Decreased musculotendinous junction length
3) Slowed peak contraction velocity
4) Muscle fiber hypertrophy
5) Decreased sarcomere length
Strength training is achieved by incremental progressive loading of muscles, in effort to increase muscle fiber contraction coordination and eventually hypertrophy of the muscle fibers themselves.
Kraemer et al. provide an American College of Sports Medicine position statement on appropriate training regimens. They recommend that loads
corresponding to 8-12 repetition maximum (RM) be used in novice training. For intermediate to advanced training, it is recommended that individuals use a wider loading range, from 1-12 RM in a periodized fashion. For local muscular endurance training, it is recommended that light to moderate loads (40-60% of 1 RM) be performed for high repetitions (> 15) using short rest periods (
Which of the following would lead to accelerated maturation in the zone of hypertrophy at the physis?
1) An activating mutation in TGF-ß
2) A deactivating mutation in the parathyroid hormone-related peptide (PTHrP) receptor
3) A deactivating mutation in prostaglandin E2
4) An activating mutation in the SMAD-3 protein
5) An activating mutation in the Indian Hedgehog (Ihh) protein
A deactivating mutation in the parathyroid hormone-related peptide (PTHrP) receptor would lead to accelerated maturation in the zone of hypertrophy.
PTHrP has been shown to play an important role in the regulation of cell proliferation at the physis. It is postulated that physeal chondrocytes regulate the local production of PTHrP by secreting a protein called Indian Hedgehog (Ihh). Ihh stimulates the chondrocytes to produce PTHrP, which slows the maturation of proliferative
chondrocytes.
Ballock et al. discuss the biology of the growth plate. With regards to cell proliferation, they describe how the proliferation of chondrocytes in the growth plate is under the control of a feedback loop involving PTHrP, Indian
Hedgehog, and TGF-ß.
Illustration A shows the Ihh/PTHrP negative-feedback loop. Incorrect Answers:
Answer 1: TGF-ß is a potent inhibitor of maturation, including cell hypertrophy, Type-X collagen expression, and alkaline phosphatase activity. An activating mutation would lead to decelerated maturation at the physis.
Answer 3: Prostaglandin E2 has not been shown to affect cell proliferation and maturation at the physis.
Answer 4: SMAD-3 increases the activity of TGF-ß. This would lead to decelerated maturation at the physis.
Answer 5: As described above, Ihh controls the release of PTHrP from chondrocytes. Activating Ihh would lead to more production of PTHrP, which would delay maturation at the physis.
All of the following statements regarding sclerostin are true EXCEPT?
1) It is a product of the SOST gene
2) Overexpression results in decreased bone mass
3) It is thought to be associated with sclerosteosis and Van Buchem disease
4) It activates the Wnt pathway
5) It is derived from osteocytes
Sclerostin inhibits the Wnt pathway, making answer choice 4 the correct answer.
Sclerostin is an osteocyte-derived negative regulator of Wnt signaling in osteoblasts. Amongst other things, the Wnt pathway and the Wnt proteins are important regulators of bone mass. They are thought to work by stimulating the production of osteoblasts. By inhibiting the Wnt pathway, sclerostin leads to decreased bone mass.
Dijke et al. discuss the role of the SOST gene in the conditions sclerosteosis and Van Buchem disease. They describe the SOST as a gene that encodes sclerostin, which is a negative regulator of Wnt signaling in osteoblasts. The
authors argue that the high bone mass seen in sclerosteosis and Van Buchem disease may be caused by increased Wnt signaling.
Day et al. review the Wnt and hedgehog signaling pathways. The Wnt and hedgehog pathways, they describe, control the differentiation of progenitor cells into osteoblasts or chondrocytes. They found that up-regulation of Wnt signaling leads to suppression of chondrocyte formation and enhanced ossification, which may be important in fracture healing.
Illustration A shows the pathway by which Wnt promotes osteoblast formation. In addition to increasing osteoblast formation, the pathway upregulates OPG, which blocks osteoclastogenesis. Illustration B shows how sclerostin inhibits
the Wnt pathway, resulting in a net decrease in bone mass. Illustration C shows an example of Van Buchem disease, an autosomal recessive disorder characterized by hyperostosis of the skull, mandible, clavicles, ribs, and diaphyseal cortices of the long bone.
Incorrect Answers:
Answers 1, 2, 3, 5: These statements are all correct regarding sclerostin.
Which of the following is more likely to occur following a total knee arthroplasty without patellar resurfacing versus a total knee arthroplasty with patellar resurfacing in patients with rheumatoid arthritis?
1) Patellar dislocation
2) Anterior knee pain
3) Extensor tendon rupture
4) Decreased quadriceps strength
5) Patellar clunk syndrome
Patients with rheumatoid arthritis who undergo a total knee arthroplasty without patellar resurfacing are more likely to have anterior knee pain when compared to the same patient population with resurfaced patellas.
Resurfacing the patella during total knee arthroplasty is a topic of controversy. Those against resurfacing note minimal issues with patellar tilt and
overstuffing the patellofemoral joint. Supporters of resurfacing state that the patellofemoral joint will eventually become arthritic if not resurfaced, and that the rate of anterior knee pain is much higher. Multiple studies, however, have shown superior results in patients with rheumatoid arthritis that have had their patella resurfaced.
Burnett et al. review the indications for patellar resurfacing during total knee arthroplasty. They consider not resurfacing the patella in patients less than 60 with non-inflammatory arthritis and a maintained patellofemoral joint space.
Holt et al. also review the role of patellar resurfacing. They mention that patellar resurfacing should be routinely done in patients with rheumatoid arthritis, preoperative patellofemoral pain, height greater than 160cm, weight greater than 60kg, or advanced patellar changes either pre- or intra- operatively.
Illustration A shows plain anteroposterior (a) and lateral (b) radiographs of the knee in a patient with rheumatoid arthritis. Degenerative changes are present in all 3 joint compartments. There is collapse of the lateral compartment with resultant valgus deformity. Erosion of the anterior aspect of the distal femoral metaphysis due to pannus is also seen.
Incorrect Answers:
Answer 1: Patellar dislocation has not been found to be higher in patellas that are not resurfaced.
Answer 3: Extensor tendon rupture is more common in patients that have had their patella resurfaced.
Answer 4: Multiple studies have not shown a difference in quadriceps strength with or without resurfacing.
Answer 5: Patellar clunk syndrome is more common in patients who have had their patella resurfaced.
Which of the following pharmacologic treatments for osteoporosis has been associated with the potential risk for osteosarcoma development?
1) Ergocalciferol
2) Non-nitrogen containing bisphosphonate
3) Monoclonal Ig2 against RANKL
4) Nitrogen containing bisphosphonates
5) Recombinant parathyroid hormone (1-34)
Recombinant parathyroid hormone (1-34) (Forteo) has been demonstrated to cause osteosarcoma in animal models but has not been to shown to cause the same effect in humans.
1-34 amino terminal residues of parathyroid hormone(1-84) administered in daily subcutaneous injections leads to bone formation. Continuous infusion leads to bone resorption.
Subbiah et al. published a case report on a patient that developed osteosarcoma following external beam radiation and recombinant teriparatide use. They discuss that though there have been nearly a 1/2 million patients treated safely with recombinant terirparatide and it is important to recognize patients that are contraindicated for treatment with recombinant teriparatide.
The FDA's Black Box warning states the following: "In male and female rats, teriparatide caused an increase in the incidence of osteosarcoma (a malignant bone tumor) that was dependent on dose and treatment duration. The effect was observed in rats at systemic exposures to teriparatide ranging from 3 to
60 times the exposure in humans given a 20-mcg dose. Because of the uncertain relevance of the rat osteosarcoma finding to humans, teriparatide should be prescribed only to patients for whom the potential benefits are considered to outweigh the
potential risk. Teriparatide should not be prescribed for patients who are at increased baseline risk for osteosarcoma (including those with Paget's disease of bone or unexplained elevations of alkaline phosphatase, open epiphyses, or prior external beam or implant radiation therapy involving the skeleton)"
Incorrect Answers:
Answer 1: Ergocalciferol does not cause an increase in sarcoma
Answer 2 & 4: Bisphosphonates can cause esophagitis, dysphagia, gastric ulcers, osteonecrosis of the jaw (ONJ), and atypical subtrochanteric fractures. Answer 3: Denosumab (Prolia) can cause arthralgia, nasopharyngitis, and back pain.
While conducting a retrospective review of patients undergoing two different techniques for open reduction and internal fixation of ankle fractures, the investigator would like to assess whether there is any significant difference between the mean patient age in the two groups. The two groups are normally distributed. Which of the following tests would be most appropriate?
1) Student t-test
2) Analysis of Variance (ANOVA)
3) Fisher exact test
4) Kruskal-Wallis test
5) Chi-square test
A Student-test would be the most appropriate test for analyzing means of parametric (continuous) variables that are normally distributed between two groups.
Data can be characterized as non-parametric (categorical, ordinal) or parametric (continuous). Parametric data, such as age, are observations for which difference between the numbers have meaning on a numerical scale. Non-parametric data are observations which can be expressed as a
dichotomous (yes or no) outcome such as gender.
Kocher and Zurakowski present a Level 5 review of epidemiology and biostatistics. The authors state that univariate or bivariate analysis, such as the student t-test, is used to assess the relationship of a single independent and a single dependent variable.
Incorrect Answers:
Answer 2: Analysis of variance is used to evaluate means of parametric data between three or more groups when the data is normally distributed
Answer 3: Fisher exact test is used to compare proportions for non-parametric data when the expected frequency is small (less than five per group)
Answer 4: Kruskal-Wallis test is used to evaluate medians of three or more groups when the data are not normally distributed.
Answer 5: Chi-square test is used to compare proportions for categorical or ordinal data (non-parametric)
Which of the following arteries provides the blood supply to the outer third of a long bone diaphysis?
1) Nutrient artery
2) Periosteal arterioles
3) Medullary artery
4) Emissary artery
5) Perichondral artery of LaCroix
Periosteal arterioles (low pressure system) supply the outer third of the adult diaphyseal cortex.
Blood supply to long bone comes from three sources: 1) nutrient artery
system, 2) metaphyseal-epiphyseal system, and 3) periosteal system. Nutrient arteries (high pressure system) enter the long bone diaphyseal cortex and
then enter the medullary canal where it branches into ascending and descending arteries and supplies the inner 2/3 of the diaphysis via Haversian systems.
Bong et al. present a review article regarding intramedullary nail effects on bone healing. They report that intramedullary nails can have negative effects on endosteal and cortical blood flow but this is offset by an increase in extraosseous circulation. During early fracture healing blood flow is centripetal
(outside to inside) because high pressure nutrient artery system is often disrupted. Illustration A depicts the blood supply for the adult diaphsysis. Incorrect
Answers:
Answer 1: High pressure system that branches from major systemic arteries and supplies the inner 2/3 of mature bone.
Answer 3: The nutrient artery enters through the medullary canal and divides into ascending and descending arteries.
Answer 4: Cortical capillaries drain to the emissary venous system. There is no described emissary artery for long bones.
Answer 5: Perichondrial artery is the major source of nutrition of the growth plate
DNA methylation, histone modification, nucleosome location, or noncoding RNA are hypothesized to contribute to the process whereby inheritable genetic alterations occur that do not involve DNA mutation. Which of the following terms best defines this process?
1) Transgenes
2) Epigenetics
3) Gene enhancers
4) Gene promoters
5) Transformation
Epigenetic changes are defined as inheritable genetic alterations that do not involve DNA mutation.
The cells in a multicellular organism have almost identical DNA sequences, yet maintain different terminal phenotypes. This nongenetic cellular memory, which records developmental and environmental cues is the basis for epigenetics. DNA methylation, histone modification, nucleosome location, or noncoding RNA are hypothesized to contribute to the process.
Maher et al discuss epigenetic influences in the realm of orthopaedics. They report new data stating that increases in matrix metalloproteinase (MMP) expression in osteoarthritis is associated with altered methylation of key promoter sequences. They also report elevated levels of an enzyme involved in epigenetic gene silencing in osteoarthritis- affected chondrocytes, SIRT1, increased the expression of matrix genes and suppressed that of MMPs.
Incorrect Answers:
Answer 1: Transgenes are genes that are artificially introduced into a single- celled embryo and are present in all cells of that organism.
Answer 3: Gene enhancers are a region of a gene that positively regulates rates of transcription.
Answer 4: Gene promoters are a regulatory segment of DNA that controls start of transcription adjacent to the transcription initiation site of a gene.
Answer 5: Transformation refers to inserting a plasmid into a bacterium with added recombinant DNA.
A 72-year-old woman presents with severe hip pain after stepping off of a curb. She denies any trauma or prior history of hip pain. Her past medical history is reviewed including a list of her current medications. Which of the following of her medications would place her at increased risk for a non-traumatic hip fracture?
1) Phenytoin
2) Cephalexin
3) Simvastatin
4) Glipizide
5) Allopurinol
Phenytoin is an anticonvulsant which has been found to increase the risk of osteoporosis and, subsequently, nontraumatic fractures.
Possible mechanisms explaining the association between anticonvulsants and bone loss include hepatic induction of cytochrome P450 enzymes (increases vitamin D catabolism), direct osteoblast inhibition, impaired calcium absorption, elevated homocysteine, inhibition of response to PTH, hyperparathyroidism, reduced reproductive sex hormones, and reduced vitamin K level.
Lee et al. found that anticonvulsant use (phenobarbital, carbamazepine, phenytoin, and valproate) increases the risk of osteoporosis, and also increases the risk of fracture by 1.2 to 2.4 times.
Jette et al. found an increased fracture risk for carbamazepine, clonazepam, gabapentin, phenobarbital, and phenytoin. Odds ratios ranged from 1.24 (clonazepam) to 1.91 (phenytoin).
Incorrect Answers:
Answers 2-5: These medications do not place a patient at a significant risk for non- traumatic hip fracture.
What part of the articular cartilage has the highest concentration of proteoglycans and the lowest concentration of water?
1) Superficial
2) Transitional
3) Deep
4) Tidemark
5) Calcified cartilage
This question requires that you know the 4 zones of articular cartilage: the superficial zone, the transitional zone, the deep zone (also called middle or radial zone) and the zone of calcified cartilage. The deep zone has chondrocytes with a more spheroidal shape which align themselves perpendicular to the joint surface. This zone has the largest diameter collagen fibrils, the highest concentration of proteoglycans, and the lowest
concentration of water. The collagen fibers of this zone pass into the tidemark, a thin basophilic line seen of H&E stains that corresponds to the boundary between calcified and uncalcified cartilage. Lastly the calcified cartilage zone is a thin zone of calcified cartilage that separates the radial zone (uncalcified cartilage) and the subchondral bone. The cells in this region have a smaller
volume than the cells of the radial zone, and these cells have extremely low level of metabolic activity.
The cross-sectional area of a muscle is the factor most responsible for which of the following?
1) Amount of maximal tension
2) Speed of contraction
3) Duration of contraction
4) Type of contraction
5) Fatigability
Force generation, or the amount of maximal tension that can be generated by a given skeletal muscle is most dependent on the cross-sectional area of the muscle.
The cross-sectional area is the main determining factor in force generated by the muscle and is controlled by the number of myofibrils that contract. Weight lifting can lead to muscle hypertrophy, increased cross-sectional area, and increased force (ability to lift heavier weights). Fiber types have less to do with the force of contraction and more to do with the duration and speed of contraction.
Baroni et al. investigated the chronology of neural and morphological adaptations to knee extensor eccentric training. After 12 training weeks, significant increases in strength and anatomical cross-sectional area (19%) were seen.
Illustration A shows how muscle hypertrophy from strength training increases cross- sectional area.
Incorrect Responses:
The other functional attributes of a muscle, such as speed and duration of contraction and fatigability are more predicated on muscle fiber type than on the area.
An orthopaedic resident wants to answer a focused research question of whether mobile bearing knee arthroplasty has superior functional outcomes compared to fixed bearing knee arthroplasty. The resident mathematically combines the results from multiple retrospective cohort studies following QUORUM (Quality of Reporting of Meta-analyses) guidelines. What is the highest level of evidence that this meta-analysis can achieve?
1) Level I
2) Level II
3) Level III
4) Level IV
5) Level V
The level of evidence assigned to a meta-analysis is based on the lowest level of evidence of the included studies. In this case, the studies included in the meta-analysis were retrospective cohort (Level III) studies.
A meta-analysis is a systematic review that combines the results of multiple studies to answer a focused clinical question.
Clarke discusses the QUORUM guidelines which are intended to address standards for
improving the quality of reporting of meta-analyses of clinical randomized controlled trials. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement and MOOSE (Meta-analysis Of Observational Studies in Epidemiology) guidelines are similar standards. A
similar set of guidelines called CONSORT (Consolidated Standards of Reporting Trials) guidelines are available for randomized trials.
Incorrect Answers:
1: Level I studies include high-quality randomized controlled trials
2: Level II studies include lower-quality RCTs and prospective cohort studies.
4: Level IV studies include case-series or poor-quality cohort and case-control studies. 5: Level V studes are expert opinion articles.
An adolescent patient is treated with a 6mm solid intramedullary nail. Compared to a 12mm solid nail of the same material, the 6mm nail has:
1) 1/2 the torsional rigidity
2) 1/4 the torsional rigidity
3) 1/16 the torsional rigidity
4) 1/8 the torsional rigidity
5) the same torsional rigidity
Nail radius affects nail bending and torsional rigidity. For a solid circular nail, the torsional rigidity is proportional to the fourth power of the radius. Thus a nail with 1/2 the diameter (6mm compared to 12mm) and therefore 1/2 the radius (3mm compared to 6mm) would have(1/2)^4 = 1/16 the torsional rigidity (answer 3). Bong et al. performed a great review of the biomechanics and biology of intramedullary nailing of the lower extremity.
The ability of a study to detect the difference between two interventions if one in fact exists describes which of the following?
1) Positive predictive value
2) Hawthorne effect
3) Effect size
4) Power
5) P value
The study power is defined as the ability of a study to detect the difference between two interventions if one in fact exists.
The power of a statistical test is correlated to the magnitude of the treatment effect, the designated type I (alpha) and type II (beta) error rates, and the sample size n. The power is equal to (1-beta) whereby beta is the false negative rate.
Kocher et al. present a Level 5 review of epidemiology and biostatistics. The review discusses study design, hypothesis testing, diagnostic performance, measures of effect, outcomes assessment, evidence-based medicine, and biostatistics. They discuss that in the orthopaedic literature power is typically set at 80%, (leaving a 20% chance that the study will display no significant association when there is an actual association.) Illustration A shows the interaction of study variables on the power of a study. Incorrect Answers:
Answer 1: Positive predictive value is the probability that a patient with a positive test actually has the disease. This value is dependent on the prevalence of disease
Answer 2: Hawthorne effect is a behavior that is changed when participants have knowledge that their behavior is being monitored.
Answer 3: Effect size is the difference in outcome between the treatment group and the control group divided by the standard deviation.
Answer 5: P value is defined as the probability, under the assumption of no difference (null hypothesis), of obtaining a result equal to or more extreme than what was actually observed if the experiment were repeated over and over
Which of the following best describes the appearance of chondrocytes and orientation of collagen fibrils in the superficial zone of articular cartilage?
1) Round chondrocytes oriented parallel with the tidemark and collagen fibrils oriented perpendicular to the tidemark
2) Round chondrocytes oriented parallel with the tidemark and collagen fibrils oriented parallel to the tidemark
3) Flattened chondrocytes oriented parallel with the tidemark and collagen fibrils oriented perpendicular to the tidemark
4) Flattened chondrocytes oriented perpendicular with the tidemark and collagen fibrils oriented perpendicular to the tidemark
5) Flattened chondrocytes oriented parallel with the tidemark and collagen fibrils oriented parallel to the tidemark
Flattened chondrocytes oriented parallel with the tidemark and collagen fibrils oriented parallel to the tidemark best describes the orientation of collagen fibrils in the superficial zone of articular cartilage.
The primary orientation of the collagen fibers in the superficial zone is parallel with the joint surface, in order to resist compressive and sheer forces. This zone is the thinnest one, and it sometimes is referred to as the gliding zone. The surface layer, known as the lamina splendens, is cell-free and composed mainly of randomly oriented, flat bundles of fine collagen fibrils. Deep to the lamina splendens are more densely packed collagen fibers interspersed with elongated, oval chondrocytes oriented parallel to the articular surface.
Sophia Fox et al. in a review article state that the superficial zone comprises 10-20% of articular cartilage and is composed of mostly type II and IX collagen.
Illustration A displays that articular cartilage has four distinct zones: (1) a superficial (tangential) zone, (2) a middle (transitional) zone, (3) a deep (radial) zone, and (4) the calcified zone. Illustration B demonstrates the collagen orientation and chondrocyte appearance in the different articular cartilage layers.
Incorrect Answers:
Answer 1-4: None of these accurately describe the appearance of
chondrocytes and orientation of collagen fibrils in the superficial zone of articular cartilage.
A 52-year-old male underwent a right total knee arthroplasty 3 days ago and reports new onset dyspnea. His vitals signs include a temperature of 98.8, pulse of 133, blood pressure of 130/77, respiratory rate of 28, and oxygen saturation of 91% on room air. A chest radiograph shows atelectasis. Which of the following findings is most likely also present?
1) Hyperchloremic metabolic acidosis
2) Jugular venous distention with tracheal deviation
3) EKG demonstrating S-wave in lead I Q-wave in lead III T-wave inversion in lead III
4) Pleural effusion with pleural/serum protein >0.5 and pleural/serum LDH > 0.6
5) Increased carbon monoxide diffusing capacity (DLCO)
The patient's clinical presentation is consistent with a pulmonary embolism and an EKG demonstrating S-wave in lead I Q-wave in lead III T-wave inversion in lead III is most likely associated with this diagnosis.
The most commonly seen signs in the EKG associated with PE are sinus tachycardia, right axis deviation and right bundle branch block. Sinus tachycardia is however only found in 8–69% of people with PE. The S1Q3T3 pattern discussed here is from acute right heart strain and is termed the "McGinn-White sign" after the initial describers but is only found in about 10-
20% of people with a PE. Patients undergoing total knee arthroplasty (TKA) without DVT prophylaxis have symptomatic PE at a rate of approximately 8%. Patients undergoing TKA have a higher risk for the presence of DVT but are at a lower risk for symptomatic PE than patients undergoing total hip arthroplasty.
Stein et al. present a study that found that dyspnea or tachypnea occurred in
92% of patients diagnosed with a pulmonary embolism. They also report that dyspnea or tachypnea was less commonly encountered in elderly patients with no previous cardiopulmonary disease.
Illustration A is a table that describes some of the characteristic findings of pulmonary embolism on a chest radiograph.
Incorrect answers:
Answer 1: Non-saddle pulmonary emboli are most often associated with respiratory alkalosis due to tachypnea.
Answer 2: Jugular venous distention with tracheal deviation is seen with tension pneumothorax.
Answer 4: Pleural effusion with pleural/serum protein >0.5 and pleural/serum LDH > 0.6 is consistent with an exudate such as pneumonia
Answer 5: Increased carbon monoxide diffusing capacity (DLCO) is not seen with pulmonary emboli.
The estimated range of values which likely includes the unknown parameter under investigation is defined as which of the following?
1) Standard deviation
2) Mode
3) Variance
4) Confidence interval
5) Incidence
When an unknown value is sought, the confidence interval gives the statistician a set of parameters within which the “true” value is located. The confidence interval is used to indicate the reliability of an estimate. The standard deviation is a quantity calculated to indicate the extent of deviation for a group as a whole. The mode is the value which
occurs most frequently in a given set of data. The variance is a quantity equal to the square of the standard deviation. The incidence is the frequency of an occurrence (or disease).
**Which of the following is true regarding the cell seen in Figure A?**
1) Originates from hematopoietic cells from a macrophage lineage
2) Derived from undifferentiated mesenchymal cells
3) They are former osteoblasts trapped in the matrix they produced
4) They become cartilage under intermediate strain and low oxygen tension
5) They form bone by producing non-mineralized matrix
The image shown in Figure A shows an osteoclast remodeling cortical bone through a cutting cone mechanism. Osteoclasts orginate from hematopoietic cells from a macrophage cell lineage.
Osteoclasts can be distinguished from other bone cells by their multinucleated giant cells and ruffled border on the cell periphery which increases the surface area for bone resorption. Their main function is to reabsorb bone after being stimulated by RANK-L and IL-1. A balance between osteoclast and osteoblast activity is necessary for a stable calcium level in the blood.
Caterson et al. review mesenchymal stem cells and their ability to regenerate musculoskeletal tissue. They state that potential applications include replacement of bone graft for segmental defects, nonunions, spinal fusions, and articular resurfacing.
Illustration A shows the differences between osteoblasts, osteoclasts and osteocytes. Video V describes the role and function of osteoblasts and osteocytes.
Incorrect Answers:
Answer 2: This is true of osteoblasts. Answer 3: This is true of osteocytes.
Answer 4: This is true of osteoprogenitor cells. Answer 5: This is true of osteoblasts.
What is the equation for determining specificity of a clinical test?
1) True negatives divided by the sum of the true negatives and false positives
2) True negatives divided by the sum of the true negatives and false negatives
3) True positives divided by the sum of the true negatives and false positives
4) True positives divided by the sum of the true positives and false negatives
5) True positives divided by the sum of the true positives and false positives
Specificity is the probability that a test result will be negative in patients without disease (answer 1). The sensitivity is the probability that a test result will be positive in patients with disease (answer 4). The positive predictive value is the number of patients with a positive test result who are correctly diagnosed and the negative predictive value is the opposite of this (answers 5 and 2, respectively). The referenced review article by Kocher describes many of the statistical tools useful for practicing orthopaedic surgeons.
Which of the following graft materials has the least potential to elicit an immune response?
1) Fresh irradiated corticocancellous bulk allograft
2) Fresh frozen fibular strut allograft
3) Fresh frozen Achilles tendon allograft
4) Fresh Achilles tendon allograft
5) Freeze dried cancellous bone chips
Of the options listed, freeze dried cancellous allograft has the least potential to elicit an immune response. Remember, all allograft tissue has more of an immune response generating capability than autograft tissue, which has the least of any of these materials.
All allograft materials carry immunogenic properties, which decrease as the material is processed via the various sterilizing, freezing, or drying process(es). As the processing increases, the mechanical characteristics of the graft tends to decrease.
Ahlmann et al. compared the complications associated with harvesting iliac crest bone graft from the anterior crest and posterior crest. They found the rates of both minor complications (p = 0.006) and all complications (p =
0.004) were significantly higher after the anterior harvest procedures than they were after the posterior procedures. They recommend that iliac crest bone graft be harvested posteriorly whenever possible.
Incorrect Answers:
Answer 1: Most bone and soft tissue allografts undergo irradiation to remove bacteria or other infectious agents, but this does not prevent an immune
response in itself.
Answer 2: Fresh frozen allografts have more immunogenic potential than freeze dried, but less than fresh materials. Fresh allograft is not typically utilized, as the processing of allograft (bone or soft tissue) provides the safety of minimizing infectious disease transmission.
Answer 3: Fresh frozen allografts have more immunogenic potential than freeze dried, but
less than fresh materials. Thus fresh Achilles tendon allograft has the highest immunogenicity.
Answer 4: Fresh Achilles tendon allograft will elicit the greatest immunogenic response.
**Which of the following statements is correct regarding Vitamin D?**
1) 1,25-dihydrocholecalciferol is the best laboratory study to determine a Vitamin D deficiency
2) 25-hydroxycholecalciferol is the active form of Vitamin D
3) 24,25-dihydroxycholecalciferol is an inactive form of Vitamin D
4) 1,25-dihydrocholecalciferol is converted to 25-hydroxycholecalciferol in the kidney
5) The half-life of 1,25-dihydrocholecalciferol is longer than 25- hydroxycholecalciferol
24,25-dihydroxycholecalciferol in an inactive form of Vitamin D. High levels of
1,25-dihydroxyvitamin D stimulate the enzymatic production of 24,25- dihydroxyvitamin D, the inactive form of vitamin D, thereby self-regulating the action of 1,25-dihydroxyvitamin D.
Vitamin D is paramount to proper calcium homeostasis and has important clinical implications in the orthopaedic patient. Vitamin D3 is synthesized in the skin and is converted to 25-hydroxycholecalciferol in the liver. 25- hydroxycholecalciferol is then converted in the kidney into 1,25- dihydroxycholecalciferol, the active form of vitamin D. The best test to determine Vitamin D deficiency is the measurement of 25- hydroxycholecalciferol, as it has a longer half-life and circulating levels are
1,000x more than 1,25-dihydrocholecalciferol.
Patton et al. review the importance of Vitamin D in the orthopaedic patient. They discuss the implications of Vitamin D deficiency, and urge orthopaedic surgeons to be proficient in both the diagnosis and treatment of the condition.
Bogunovic et al. measured the levels of 25-hydroxycholecalciferol in 723 patients who were to undergo orthopaedic surgery. 40% of these patients were noted to be deficient in Vitamin D, with the highest rates in patients scheduled to undergo trauma and sports surgery.
Illustration A reviews Vitamin D metabolism. 24,25-dihydroxycholecalciferol is referred to as pre-Vitamin D.
Incorrect Answers:
Answer 1: 25-hydroxycholecalciferol is the best laboratory study to determine
Vitamin D deficiency due to its long half-life and high circulating levels. Answer 2: 1,25- dihydroxycholecalciferol is the active form of Vitamin D. Answer 4: 25- hydroxycholecalciferol is then converted in the kidney into 1,25- dihydroxycholecalciferol. Answer 5: The half-life of 25-hydroxycholecalciferol is 2-3 weeks, while the
half-life of 1,25-dihydrocholecalciferol is only 4-6 hours.
You are the team physician for a collegiate football team and receive weekly injury reports from the athletic trainer. All players with sickle-cell trait are listed at the bottom to remind all on-field**
**personnel that they may need which of the following?
1) Oxygen supplementation and oral or IV hydration
2) Additonal layers of warm clothes
3) Increased pain medication
4) Avoidance of non-steroidal anti-inflammatory medicines
5) Days of rest due to increased joint pain
Players with a blood test indicating the presence of sickle-cell trait (SCT) are at risk for exertional sickling collapse which responds initially to rest, hydration and oxygen.
SCT is not a disease but a condition, resulting from inheritance of one gene for sickle hemoglobin (S) and one gene for normal hemoglobin (A).
The vital concern is exertional sickling collapse, which can be fatal, occurs in a variety of sports, and is a leading cause of death in college football.
According to the review by Eichner, sickling collapse is an “intensity”- associated syndrome that differs from the other common causes of collapse. The best approach in college football may be tailored precautions to prevent sickling collapse and enable athletes with SCT to thrive. Other clinical concerns in SCT are compartment syndromes and lumbar myonecrosis, splenic infarction, gross hematuria, hyposthenuria, and venous thromboembolism.
Kark et al. reviewed all cases of sudden death occurring among 2 million enlisted recruits during basic training in the U.S. Armed Forces from 1977 to
1981/. They concluded that "recruits in basic training with the sickle-cell trait have a substantially increased, age-dependent risk of exercise-related sudden death unexplained by any known preexisting cause".
Incorrect Responses:
2/. no research to support need for warmer clothes and cases occur year round. 3&5/. these are typical of sickle cell disease, not SCT.
4/. important in patients with renal impairment, which is not typically seen in SCT.
A physician is interested in using platelet-rich plasma (PRP) for treatment of osteochondral lesions of the talus. He is reviewing a prospective cohort study that compares 40 patients treated with PRP and cast immobilization for 6 weeks vs. 36 patients treated conservatively with cast immobilization for 6 weeks. All patients were treated at the same time and institution. The study was not randomized although treatment and control groups were matched
**appropriately to reduce selection bias. Follow-up in each group was**
> 80% over 1 year. The paper reported significant improvement with use of PRP based on three standard foot and ankle outcome scores (AOFAS, SF-36, FOAS). What is the level of evidence for this study?
1) Level I
2) Level II
3) Level III
4) Level IV
5) Level V
This is prospective cohort study with Level-II evidence.
Level of evidence provides guidance to the study quality. It is used to assess therapeutic studies (as with this question), prognostic studies, diagnostic studies and economic or decision models. When determining the level of evidence, readers must critically appraise the study question, treatment, intervention and outcomes of the study design. Level-II therapeutic studies consist of well-designed prospective cohort studies, poor-quality randomized controlled trials (follow-up less than 80%) and systematic review of Level-II studies or non-homogenous Level-I studies.
Wright et al. provided an excellent summary of clinical research study level of evidence. This has been provided as Illustration A.
Illustration A shows a chart of level of evidence. There is a column for each type of study which corresponds to a row that outlines the level of evidence based on study
design.
Incorrect Answers:
Answer 1: Level-I evidence include randomized controlled studies with follow- up>80% and systematic review of Level-I RTC studies (homogenous studies) Answer 3: Level-III evidence include case control studies, retrospective cohort studies and systematic review of Level-III studies
Answer 4: Level-IV evidence include case series with no control group (or compare to a historical control group)
Answer 5: Level V evidence include expert opinion
Low serum phosphate and normal calcium levels are found in what common etiology of hereditary rickets?
1) X-linked hypophosphatemic
2) Vitamin D-dependent, type I
3) Vitamin D-dependent, type II
4) Autosomal dominant hypophosphatemic
5) Jansen's metaphyseal chondrodysplasia
Low serum phosphate and normal calcium levels are found in X-linked hypophosphatemic rickets.
X-linked hypophosphatemic rickets is the most common form of hereditary rickets. It is an X-linked dominant disorder which has been linked to the PHEX gene. Laboratory findings
of this disorder include low serum phosphate, normal serum calcium and 25 hydroxycholecalciferol levels, and inappropriately low 1,25-dihydroxyvitamin D3.
Carpenter et al. showed hypophosphatemic rickets was initially referred to as “vitamin D resistant rickets” due to its lack of response to therapeutic vitamin D. Current treatment with activated vitamin D metabolites (calcitriol or
alfacalcidol) and phosphate salts have been shown to help with this condition.
Illustration A shows an insufficiency fracture of the proximal tibia in an adult patient with X-linked hypophosphatemic rickets. A stress fracture on the medial tibia may be a presenting feature of untreated disease.
Incorrect Answers:
Answer 2: Vitamin D-dependent rickets, type I, is a rare autosomal recessive disorder. Answer 3: Vitamin D-dependent rickets, type II, is a rare autosomal recessive disorder, most often caused by mutations in the vitamin D receptor gene. Answer 4: Autosomal dominant hypophosphatemic results from a rare mutation in the fibroblast growth factor 23 (FGF23) gene.
Answer 5: Jansen's metaphyseal chondrodysplasia is a skeletal dysplasia that results from ligand-independent activation of the type 1 parathyroid hormone
receptor (PTHR1).
A healthy patient undergoes routine pre-operative laboratory testing and is found to have a leukocyte count of 1.5 × 10(9) cells/L. When the historical records are examined, this is found to be the patients base-line level over a period of years. Which of the following statements is most likely to be true:
1) The patient is at a significantly higher risk of surgical infection
2) The patient is more likely to be of African than of European descent
3) The patient is more likely to be of European than of Middle Eastern descent
4) The patient is more likely to be a non-athlete than an athlete
5) The patient is more likely to be female than male
The clinical presentation is consistent with Benign Ethnic Neutropenia, a condition in which a patient has chronic, benign, inborn and lifelong absolute neutrophl count below population mean. This condition is found in the U.S. to be most common in African- Americans, some groups of Middle Eastern patients, males, children under 5 years old, and athletes compared to non- athletes.
A standardized level at present for abnormally low absolute neutrophil count (ANC) is below 1.5 x 10(9) cells/L, however this may not have clinical or scientific relevance as a cutoff point, particularly in the affected Ethnic groups. Fewer than 1% of all populations have absolute neutrophil count
A 14-year-old patient has sustained a complete ACL tear of his right knee. Which of the following options has shown to be the most limiting factor for access to pediatric orthopaedic management in the United States?
1) Sex of the patient
2) Type of health insurance
3) Child greater than 10 years of age
4) Acute knee injuries requiring operative treatment
5) Timing of the referral
The type of health insurance in the pediatric population has shown to be a significant factor for access to specialized healthcare in the United States.
Access to pediatric orthopaedic management has been well investigated. Numerous Level 4 studies have shown that orthopaedic offices in urban and rural areas prefer treating patients with private insurance over patients with Medicaid.
Iobst et al. telephoned 100 urban and rural orthopaedic outpatient offices to schedule an appointment for a 10-year-old patient with a forearm fracture. They showed that 8/100 offices would schedule an appointment within 1 week to the child with Medicaid insurance, as compared to 36/100 that gave an appointment to a child with private insurance.
Pierce et al. contacted 42 orthopaedic practices to schedule an appointment for a 14- year-old patient with an ACL injury. They showed that 38/42 offices scheduled an appointment for the child within 2 weeks with private insurance. This compared to 6/42 that scheduled an appointment for a similar child with Medicaid.
Incorrect Answers:
Answers 1,3,4,5: The limiting determinant to healthcare in the pediatric population has shown to be the type of health insurance. Sex, age of child, operative vs nonoperative injuries and timing of referral have not been shown to affect access to healthcare.
The perioperative use of which medication has been shown to increase the risk of post-operative infection following orthopaedic procedures in patients with rheumatoid arthritis (RA)?
1) Naproxen
2) Leflunomide
3) Sulfasalazine
4) Etanercept
5) Aspirin
Of the medications listed, only etanercept has been shown to increase the risk of post- operative infection following orthopaedic procedures in patients with RA.
Etanercept is a TNF-alpha antagonist with a short half-life that is administered once or twice weekly in patients with RA. Since TNF-alpha plays a central role in the pathogenesis of RA and is instrumental in causing joint destruction, the inhibition of this molecule has shown excellent results in controlling disease. The most powered study on TNF-alpha inhibitor use in the perioperative period following an orthopaedic procedures demonstrated a significant increase in
post-operative infection.
Howe et al. review the medical management of patients with RA who underwent orthopaedic procedures. They state that while there is conflicting information regarding TNF-alpha antagonists, they recommend holding them prior to major orthopaedic interventions.
Giles et al. review 91 patients with rheumatoid arthritis who underwent an orthopaedic procedure. They found TNF-alpha inhibitor therapy to be significantly associated with the development of a serious postoperative infection (p=.041)
Perhala et al. review 61 patients with RA who were treated with methotrexate during the perioperative period surrounding a total joint arthroplasty. They
failed to find a significant increase in complications in this patient group, stating the perioperative use of methotrexate does not affect wound healing or increase the likelihood of periprosthetic infection.
Illustration A shows the site of action of TNA-alpha inhibitors in the RA pathway.
Incorrect Answers:
Answer 1: Naproxen should be discontinued 3 days prior to surgery because of its ability to increase bleeding time and the subsequent potential for increased blood loss.
Answer 2: Leflunomide is an inhibitor of pyrimidine synthesis. It has not been shown to increase the risk of post-operative infection.
Answer 3: Sulfasalazine's mechanism of action is largely unknown, but it has not been shown to increase the risk of post-operative infection.
Answer 5: Aspirin has not been shown to increase infection if continued in the perioperative period.
Communication breakdown is the leading cause of which of the following?
1) Delayed diagnoses
2) Medication errors
3) Surgical site infections
4) 1 and 2
5) All of the above
Communication failures are the leading cause of wrong side surgeries, medication errors and diagnostic delays.
Poor communication sets up environments in which medical errors can take place. Per the Joint Commission, medical errors may be the among the top 10 causes of death in the United States. Establishing open lines of communication is critical to reduce the risk of error and enhance patient safety.
Gandhi et al. designed a framework to study missed or delayed diagnoses and their causes. The most significant factors contributing to errors were poor handoffs, failures in judgment, failures in memory and failures in knowledge.
O’Daniel et al. review the importance of professional communication and collaborative team efforts. They note that patient safety is at risk when poor communication is in place. The leading cause for medication errors, treatment delays and wrong-site surgeries is communication failure.
Illustration A shows the leading causes of death in the United States. This includes “preventable errors” as a cause.
Incorrect Answers:
Answers 1, 2: Communication failures can lead to delays in diagnosis and
treatment, medication errors and wrong side surgery
Answers 3, 5: Communication failure is not a direct contributor to surgical site infection
**Which of the following is true regarding osteoprotegerin (OPG)?**
1) It is secreted by osteoclasts
2) It increases bone resorption
3) Binds to prostoglandin E2 before stimulating osteoclasts
4) Osteoprotegerin knock-out mice develop osteopetrosis
5) Binds to and sequesters RANKL
Osteoprotegerin is a decoy receptor for RANKL. Binding to RANKL causes decreased production of osteoclasts by inhibiting the differentiation of osteoclast precursors.
Bone resporption/remodeling is a complex process regulated by a large variety of molecules. Molecules that have shown to inhibit osteoclasts include OPG, calcitonin, estrogen, TGF-B, and IL-10. Corticosteroids have been shown to decrease production of OPG, thereby enhancing osteoclast formation and longevity. Prolia, or denosumab, is a newly approved drug used to treat osteoporosis and has a mechanism of action similar to osteoprotegerin
(inhibits binding of RANKL to RANK).
Boyle et al. review osteoclast differentiation and activation. The authors state that targeted disruption of OPG causes increased osteoclastogenesis and/or activation resulting in osteopenia.
Illustration A shows how OPG binds to RANKL inhibiting the stimulation of osteoclasts.
Incorrect Answers:
Answer 1: OPG is secreted by osteoblasts.
Answer 2: OPG decreases bone resorption by inactivating RANKL. Answer 3: OPG does not bind to prostoglandin E2, nor does it stimulate osteoclasts.
Answer 4: RANKL knock-out mice creates an osteopetrosis-like condition.
A 55-year-old woman has T-score -2.0 at the femoral neck. According to the World Health Organization Fracture Risk Assessment Tool (FRAX), she has a ten- year probability of sustaining a hip fracture of 1.5% and a ten-year probability of sustaining a major osteoporotic fracture of 8.9%. Which of the following statements is true regarding her antiresorptive therapy management?
1) Antiresorptive therapy should be started based on her T-score
2) Antiresorptive therapy should be started based on her risk of hip fracture alone
3) Antiresorptive therapy should be started based on her risk of major osteoporotic fracture alone
4) Antiresorptive therapy should not be started
5) Antiresorptive therapy should be started based on her risks of both hip fracture and major osteoporotic fracture
This patient has osteopenia. Assessment by FRAX shows that ten-year risk of hip fracture is less than 3% and her ten-year risk of major osteoporosis- related fracture is less than 20%. Therefore, antiresorptive therapy is not indicated at this time.
According to the 2008 National Osteoporosis Foundation guidelines, pharmacologic treatment for osteoporosis should be considered if patients are
postmenopausal women or men greater than 50 years old AND meet one of the following criteria: (1) they have a prior hip or vertebral fracture, (2) they have a T score -2.5 or less at the femoral neck or spine, (3) they have a T score between -1.0 and -2.5 at the femoral neck or spine AND a 10-year risk of hip fracture greater than 3% or 10-year risk of major osteoporosis-related fracture greater than 20%.
FRAX (World Health Organization Fracture Risk Assessment Tool) calculates
10-year risk of fracture based on the following variables: age, sex, race, height, weight, BMI, history of fragility fracture, parental history of hip fracture, use of oral glucocorticoids, secondary osteoporosis and alcohol use to calculate 10-year risk of fracture.
Unnanuntana et al. reviewed the assessment of fracture risk. Besides FRAX score and T-score, they discussed biochemical markers of bone formation and resorption, which are useful for monitoring the efficacy of antiresorptive / anabolic therapy, and may help identify patients at high risk for fracture.
Ekman et al. reviewed the role of the orthopaedic surgeon in minimizing mortality and morbidity associated with fragility fractures. The surgeon should consider prescribing appropriate medications, physical therapy, assessing fall risk and preventing falls and changing lifestyle factors (exercise, smoking and alcohol).
Illustration A shows the FRAX online tool ([_http://www.shef.ac.uk/FRAX/tool.aspx?country_ _=__=9)._ Illustration B shows the](http://www.shef.ac.uk/FRAX/tool.aspx?country=9/)) clinical risk factors considered in FRAX calculation.
Incorrect Answers:
Answer 1: T-score of -2.0 is not an indication for initiating treatment. Answers 2, 3, 5: Her FRAX score does not show a risk of hip or osteoporosis- related fracture high enough to be an indication for initiating treatment.
A 32-year-old runner sustains a trimalleolar left ankle fracture. She undergoes open reduction and internal fixation and is kept non- weightbearing after surgery. At 2 months, what changes will occur in the articular cartilage of both her knees as a result of her current weightbearing regimen?
1) Cartilage thickening in the left (ipsilateral) knee and no change in cartilage thickness in the right (contralateral) knee
2) Cartilage thinning in both knees
3) Cartilage thinning in the left (ipsilateral) knee and no change in cartilage thickness in the right (contralateral) knee
4) Cartilage thinning in the left (ipsilateral) knee and increased cartilage thickness in the right (contralateral) knee
5) Increased cartilage thickness in both knees
After a period of off-loading, the off-loaded limb will experience cartilage thinning. The contralateral limb will not demonstrate any cartilage changes.
Physiologic loading of cartilage increases proteoglycan synthesis and cell proliferation and is chondroprotective. Joint immobilization leads to cartilage thinning, tissue softening, and reduced proteoglycan content, leading to cartilage erosion. Joint overuse leads to cartilage damage (in vitro only).
Hinterwimmer et al. examined cartilage atrophy after partial load bearing
using quantitative MRI. They found cartilage thinning in all knee compartments (greatest thinning, medial tibia; least thinning, patella). There was no change in cartilage morphology in the contralateral knee.
Sun reviewed the relationship between mechanical loading and cartilage degeneration. In OA, cartilage breakdown occurs at the articular surface, and is then fueled by synovial proteases and cytokines. In RA, synovial cells and macrophages are the source of degradative enzymes and incite cartilage destruction.
Milward-Sadler et al. examined mRNA levels following mechanical stimulation in normal and osteoarthritic chondrocytes. Normal chondrocytes showed increased aggrecan mRNA and decreased matrix metalloproteinase 3 (MMP-3) mRNA after stimulation. This
chondroprotective response was absent in osteoarthritic chondrocytes.
Illustration A shows pro- and anti-inflammatory mechanisms of mechanical loading on chondrocytes. Underloading and overloading induce cartilage damage through pathways involving the upregulation of MMPs and ADAMTSs (ADAMTS, a disintegrin and metalloproteinase with thrombospondin motifs, or aggrecanase). Physiological loading blocks these increases.
Incorrect Answers:
Answer 1: Cartilage THINNING (not thickening) will occur on the offloaded limb (left). Answers 2 and 5: There will be a difference in cartilage thickness between knees as a result of different weightbearing status on both lower extremities. Answer 4: Noticeable cartilage hypertrophy does not occur on the uninjured limb.
A morbidly obese 40-year-old man is scheduled to undergo hemilaminectomy for resection of an painful osteoid osteoma of the T6 lamina. He is positioned prone on a Jackson table and localization is performed with intraoperative fluoroscopy prior to the start of the case. At close to the end of the case, intraoperative frozen section reveals only normal bone fragment from the resected lamina. A probe is placed and a cross-table lateral radiograph reveals that the T7 lamina was resected instead of T6. At this point, the surgeon should**
**do all of the following EXCEPT
1) Complete the surgery
2) Abort the case and obtain further imaging
3) Apologize to the patient and family
4) Formally document the error in the operative report
5) Inform the patient and family immediately after the operation
should include a disclosure of known facts and an explanation as to the likely cause, as well as ongoing treatment, follow up care, and prognosis.
The AAOS Information Statement about Wrong Site Surgery identifies 3 treatment steps following discovery of an error during surgery under general anesthesia: Return the patient to his preoperative condition, perform the correct procedure at the correct site, and advise the patient and family of what occurred and the likely consequences, if any, of the wrong- site surgery.
The AAOS Information Statement on Communicating Adverse Events states that the surgeon has an ethical and professional obligation to disclose the error to the patient and/or family. Disclosure should include what happened, why it happened, health implications, and what measures are being instituted to prevent recurrences.
Incorrect Answers:
Answer 1: Completion of the surgery at the correct site is necessary unless proceeding with the surgery at the correct site would increase the risk associated with extended operating time, or if correct-site surgery would result in an additional unacceptable disability.
Answers 3: Many patients have expressed that an apology is important. In the apology, the physician should express support for the patient and family, show compassion and concern, and acknowledge their emotional response and needs. This will help to set clear goals for the future patient-physician interaction.
Answer 4: Full disclosure is recommended and there should be no attempt at concealment or obfuscation. This is especially true for the operative report. Answer 5: A composed dialogue between the surgeon and both patient and family after the event is preferred to a hurried call from the operating room which is prone to misunderstanding and leaves no room for questions and answers.
All of the following are Standards of Professionalism relating to interactions with industry for practicing orthopaedic surgeons EXCEPT:
1) Decline gifts from industry with a market value over $100 (unless they are medical textbooks or patient educational materials)
2) Disclose to the patient any financial arrangements with industry that relates to the patient's treatment
3) Accept no direct financial inducements from industry for utilizing a particular implant
4) Disclose any relationship with industry to colleagues who may be influenced by your work
5) Decline to participate in industry sponsored non-CME courses or
conferences
The AAOS has adopted the Standards of Professionalism (SOP). These SOP’s establish mandatory, minimum levels of acceptable conduct for fellows and members of the AAOS to engage in relationships with industry. There are 17 standards with relation to industry. Answer choice 5 is not a SOP as surgeons are allowed to participate in or consult in meetings that are conducive to the effective exchange of information. The SOP also stipulate that tuition, travel, and modest hospitality (including meals and receptions) are allowed to attend an industry-sponsored non-CME course.
A prospective randomized trial is conducted to test the efficacy of Vitamin C versus placebo in treating patients who develop chronic regional pain syndrome (CRPS) after distal radius fractures. At first follow-up, the rates of CRPS are 1% and 9% in the study and placebo group, respectively. Which statistical test is most appropriate to determine significance?
1) Single factor analysis of variance
2) Chi-square test
3) Student t-test
4) Mann-Whitney rank sum test
5) Wilcoxon rank sum test
In the study provided, we need to determine whether distributions of categorical variables differ from one another. The appropriate study is the chi- square test.
Data can be classified as numerical (continuous) or categorical (proportional). Responses to such questions as "What is your major?" or Do you own a car?" are categorical because they yield data such as "biology" or "no." In contrast, responses to such questions as "How tall are you?" or "What is your G.P.A.?" are numerical. When comparing two independent means from numeric data, a t-test is performed. However, if categorical data is being compared, the chi- square test will determine if the proportions are really different.
Kocher et al. review basic clinical epidemiology and biostatistics relevant to orthopaedic surgery. Amongst other things, they describe that data can be summarized in terms of measures of central tendency, such as mean, median, and mode, and in terms of measures of dispersion, such as range, standard deviation, and percentiles.
Illustration A shows an algorithm for determining which test to use for varying data. Incorrect Answers:
Answer 1: Analysis of variance (ANOVA) is used to compare means of three or more independent groups in which the data are normally distributed.
Answer 3: Student t-test is used for comparing means of continuous data that is normally
distributed.
Answer 4: The Mann-Whitney and Wilcoxon rank sum tests are used for comparing means of non-continuous data.
Answer 5: The Mann-Whitney and Wilcoxon rank sum tests are used for comparing means of non-continuous data.
A 35-year-old patient is involved in a motor vehicle accident and sustains multiple fractures including a closed comminuted proximal meta-diaphyseal tibia fracture. The surgeon is considering bridge plating the fracture using a minimally invasive approach. Which of the following is true regarding bridge plating?
1) A locked plate construct (locked screws) or hybrid construct (locked and non- locked screws) is necessary.
2) Periosteal stripping is performed through two incisions proximal and distal to the fracture.
3) Bridge plating is performed following direct reduction of the fracture.
4) AO Type A diaphyseal fractures are best treated with this technique.
5) Bridge plating with a long working length creates a flexible, axially stable construct.
In bridged plating, only the most proximal and distal screw holes are filled. This creates a flexible, axially stable construct.
Bridge plating is applicable to all long-bone fractures with complex fragmentation and where intramedullary nailing or conventional plate fixation is not suitable. The construct preserves the blood supply to the fracture fragments as the fracture site is undisturbed during the operative procedure. It provides RELATIVE stability, allowing for some motion at the fracture site, leading to callus formation and secondary bone healing. The construct is FLEXIBLE because of increased distance between the 2 screws closest to the fracture (long working length), allowing for stress distribution and permitting more motion at the fracture site. The construct is also AXIALLY STABLE because the plate acts as an extramedullary splint and resists axial compression.
Livani et al. advocate using an anterior or antero-lateral approach for minimally invasive plating of the humerus. They recommend that distal access is obtained first, allowing identification of the lateral antebrachial cutaneous nerve. For distal fractures, they recommend extending the plate down to the lateral column.
Apivatthakakul et al. defined minimally-invasive plate osteosynthesis (MIPO) danger zones from the lateral epicondyle. They found the musculocutaneous nerve averaged 18- 43% of the humeral length, the danger zone for the radial nerve averaged 36-59% of the humeral length, and the most dangerous screws that penetrated or touched the radial nerve lay 47-53% of the humeral length.
Illustration A shows a distal tibia fracture. Illustration B shows radiographs 5 months after bridge plating of this fracture. There is callus formation, characteristic of indirect bone healing.
Answer 1: Locked plates are not necessary for bridge plating. Conventional plate/screws may be used.
Answer 2: Bridge plating through a minimally invasive approach avoids periosteal stripping and the plate lies in a submuscular location. It is especially important where comminution is present and preservation of tenuous
periosteal blood supply is critical.
Answer 3: Bridge plating is usually applied following some form of indirect reduction. Indirect reduction involves manipulating fragments into the correct position without opening the fracture site, thus minimizing damage to the blood supply. The main principle of indirect reduction is distraction.
Answer 4: AO Type A simple diaphyseal fractures are best treated with intramedullary nailing (relative stability) or anatomic reduction and compression plate fixation (absolute stability).
Which of the following components of bone is most responsible for compressive strength?
1) Type I collagen
2) Osteocalcin
3) Proteoglycans
4) Osteonectin
5) Osteopontin
Proteoglycans, in addition to calcium hydroxyapatite [Ca10(PO4)6(OH)2], are most responsible for providing compressive strength.
Bone is composed of both organic and inorganic components. Inorganic components include calcium hydroxyapatite and osteocalcium phosphate. Organic components include collagen, proteoglycans, matrix proteins, cytokines and growth factors. While Type I collagen is responsible for providing the tensile strength of bone, proteoglycans and calcium hydroxyapatite [Ca10(PO4)6(OH)2] are most responsible for providing compressive strength. Proteoglycans contain a core protein with various
numbers of covalently attached side chains of glycosaminoglycans. In addition to providing compressive strength, they are also responsible for binding growth factors and inhibiting mineralization.
Knothe et al. review the osteocyte. They discuss that osteocytes are the most abundant
cells in bone, are actively involved in maintaining the bony matrix, and may act as mechanosensors.
Illustration A shows a proteoglycan aggregate, which can form when individual molecules link onto a chain of hyaluronic acid.
Incorrect Answers:
Answer 1: Type I collagen is responsible for the tensile strength of bone. Answer 2: Osteocalcin is the most abundant non-collagenous protein in the matrix and promotes the mineralization and formation of bone.
Answer 4: Osteonectin is believed to have a role in regulating calcium or organizing mineral in matrix.
Answer 5: Osteopontin is a cell-binding protein.
A prospective, randomized controlled trial of 150 patients undergoing total hip arthroplasty is performed to test whether repair of the capsule during a posterior approach reduces post-operative dislocations in the first three months. The study found no difference in dislocation rate if the capsule was repaired versus not repaired (p =**
**.34). Subsequently, a multicenter follow-up study of 2000 patients showed that repairing the capsule led to a decreased dislocation rate**
**in the first three months (p = .03). Assuming the second study reflects reality, which of the following errors occurred in the first study?
1) Observer bias
2) Type-II error
3) Alpha error
4) Type-I error
5) Confounding error
In this situation, the null hypothesis was accepted when it should have been rejected.
This is a type-II error.
A study can have two types of errors. Type-I errors, or alpha errors, occur when the null hypothesis is rejected when it should have been accepted. The alpha level refers to the probability of a type-I error. By convention, the alpha level of significance is set at 0.05, which means that we accept the finding of a significant association if there is less than a one in twenty chance that the observed association was due to chance alone. Type-II errors, or beta errors, occur when the null hypothesis is accepted when it should be rejected. This
often occurs when studies are underpowered. In the example above, the null hypothesis is that repair of the capsule does not reduce dislocations within the first three months. Since the first study did not show a statistically significant difference, the null hypothesis was accepted. Since a more powered study showed that repair of the capsule does reduce dislocations, the null hypothesis should have been rejected in the initial study (if it was adequately powered).
Fosgate et al. review the importance of sample size calculations when performing research. They state that sample size ensures statistical significance if the subsequent data collection is perfectly consistent with the assumptions made for the sample size calculation (assuming power was set as
50% or greater).
Illustration A shows the difference between type-I and type-II errors. Video V is a lecture discussing statistical definition review of PPV, NPV, sensitivity and specificity.
Incorrect Answers:
Answer 1: Observer bias is when the observer (usually the investigator) influences the results of an experiment as a result of their own bias. Answer 3: Alpha errors are the same as type I error (see below).
Answer 4: A type-I error would reject the null hypothesis when it is true. Answer 5: A confounder is a variable that has associations with both the dependent and independent variables, potentially distorting their relationship. Confounders are not technically considered "errors," but instead are variables
that properly constructed studies attempt to avoid.
**Which of the following is a potential cause of fretting corrosion?**
1) The micromotion at the femoral head-neck junction in a modular total hip replacement
2) A stainless-steel cerclage wire is in contact with a titanium-alloy femoral stem
3) Friction between polyethylene liner and femoral head leading to osteolysis
4) The formation of pits within a stainless-steel plate and the subsequent release of metal ions
5) The formation of an adherent oxide coating on titanium implants
Micromotion at the femoral head-neck junction can lead to fretting corrosion, one of the most common causes of failure of a modular implant.
Modular components give surgeons excellent intraoperative flexibility, but are susceptible to various types of corrosion. While titanium and cobalt-chrome contain a protective surface oxide layer, continued micromotion at the modular junction may disrupt the protective layer leading to fretting corrosion, defined as micromotion at contact sites under load. This may eventually lead to a painful synovitis that necessitates a revision procedure.
Srinivasan et al. review modularity in total hip arthroplasty. Amongst other things, they discuss the modularity of the femoral head/neck junction, describing the morse taper interlocking system that provides both axial and rotational stability.
Illustration A shows an example of corrosion at the head/neck junction of a total hip arthroplasty.
Incorrect Answers:
Answer 2: This is an example of galvanic corrosion, as two dissimilar metals are in contact with each other.
Answer 3: This is an example of adhesive wear.
Answer 4: This is an example of pitting corrosion, or crevice corrosion. Answer 5: This process is called self-passivization, enabling titanium to become corrosion resistant.
Which of the following situations is most likely to decrease sentinel event errors?
1) Physician and nurse training is lengthened by 20%
2) Resident hours are decreased to 55 hours per week
3) An environment is created where all members of the healthcare team feel empowered to express their concerns and beliefs
4) Holding individuals responsible for errors in clinical judgement
5) Physicians and nurses are assigned to a smaller number of patients
Creating an environment where all members of the healthcare team feel empowered to express their beliefs increases communication, the key element in decreasing sentinel events.
Research has shown that 70% of sentinel event errors are caused by improper communication. Specific ways to improve communication include effective clinical handover between shifts and breaking down the "hierarchy" so that all members of the team can discuss their expectations and concerns. Barriers to effective communication include distractions, cultural differences, power distance relationships, time pressures, and lack of organization.
Leonard et al. describe specific clinical experiences in the application of surgical briefings, properties of high reliability perinatal care, the value of critical event training and simulation, and benefits of a standardised communication process in the care of patients transferred from hospitals to skilled nursing facilities. They recommend embedding standardized tools and behaviors to bridge differences in communications styles between clinicians.
Incorrect Answers:
Answer 1: Increasing training time is unlikely to decrease sentinel event errors if effective communication is not established.
Answer 2: Some studies have shown increased error rates with decreased resident physician work hours.
Answer 4: Holding individuals responsible for errors in clinical judgement has not specifically been cited as a way to decrease errors within a healthcare setting.
Answer 5: While this may decrease sentinel event errors, this has not been to be as effective as improvements in communication.
Which of the following side effects is most strongly associated with the use of NSAIDs?
1) Hepatic dysfunction
2) Renal impairment
3) Prolonged QTc
4) Seizures
5) Hematuria
All NSAIDs have the potential to cause serious renal impairment.
NSAIDs work by inhibiting the cyclooxygenase pathway (COX), which is comprised of the COX-1 and COX-2 pathways. The COX-1 pathway is involved in prostaglandin E2– mediated gastric mucosal protection and thromboxane effects on coagulation, while the COX-2 pathway is mainly involved with the modulation of pain and fever without effect on platelet function. While selective COX-2 inhibitors have a decreased side effect profile, all NSAIDS
have the potential to cause renal impairment and their use should be limited in patients with underlying renal disease.
Horlocker et al. review multimodal pain management in the perioperative setting of a total joint arthroplasty. Specifically, they note that NSAIDs should be used cautiously in patients with underlying renal dysfunction who are to undergo a procedure with major blood loss.
Griffin et al. reviewed 1,799 patients hospitalized for acute renal failure. They found that NSAIDs increased the risk of renal failure by 58% and that NSAID use resulted in 25 excess hospital admissions per 10,000 years of use.
Illustration A shows the COX pathways and their inhibition by NSAIDs. Incorrect Answers:
Answers 1, 3, 4, 5: NSAIDs have not been shown to be strongly associated with these side effects.
It is recommended that invasive dental work be completed prior to the initiation of which of the following medications?
1) Glucosamine
2) Cholecalciferol
3) Levothyroxine
4) Teriparatide
5) Bisphosphonates
Bisphosphonate therapy combined with invasive dental work increases the risk for development osteonecrosis of the jaw.
Bisphosphonates are a class of drugs that prevent bone mass loss by inhibiting osteoclast resorption. They are used in the treatment of vertebral compression fractures, non- vertebral fragility fractures, osteogenesis imperfecta, multiple myeloma, and avascular necrosis. Because bisphosphonates have been associated with osteonecrosis of the jaw, it is suggested that all invasive
dental work be completed prior to initiation of treatment.
Pazianas et al. (2011) review the safety profile of bisphosphonates. Specifically, they cite gastrointestinal discomfort, atypical femur fractures, osteonecrosis of the jaw, ocular inflammation, and musculoskeletal pain as common side effects. They state there is limited evidence surrounding
bisphosphonate's association with esophageal cancer and atrial fibrillation.
Pazianas et al. (2007) reviewed 11 publications that reported 26 cases of osteonecrosis of the jaw following initiation of bisphosphonate treatment. Age
>60 years, female sex, and previous invasive dental treatment were the most common characteristics of those who developed ONJ.
Illustration A shows the various bisphosphonates and their mechanisms of action. Illustration B shows an example of osteonecrosis of the jaw, a side effect that has been linked to bisphonphonate treatment.
Incorrect Answers:
Answer 1: Glucosamine is a dietary supplement used in the management of osteoarthritis. It is not contraindicated prior to dental work.
Answer 2: Cholecalciferol is Vitamin D3. Toxicity and side effects are rare with Vitamin D therapy.
Answer 3: Levothyroxine is used in the treatment of hypothyroidism. It is not contraindicated prior to dental work.
Answer 4: Teriparatide (Forteo) has been used in the treatment of osteonecrosis of the jaw caused by bisphosphonates.
Figures A and B show radiographs of a 24-year-old female with a soccer injury. A physical examination reveals an isolated, closed injury with no clinical features of neurovascular injury or compartment syndrome. She has been consented to be treated with intramedullary nail fixation. A pre-operative note by the anaesthesiology team makes reference to the patients fair skin and natural red-hair color. How will this information affect the post-operative management of this patient?
1) Longer duration of anticoagulation due to increased risk of DVT
2) Avoiding anticoagulation medications due to increased risk of bleeding
3) Require higher dosages of post-operative analgesia
4) Longer period of non-weight bearing on surgical limb
5) Avoiding opioids due to higher risk of unrecognized allergies
Female patients with natural red-hair may require higher dosages of post- operative analgesia compared to other hair types.
Melanocortin-1-receptor (MC1R) is one of the key proteins involved in hair color and skin tone. Mutations of the MC1R alleles can render this protein non- functional, which results in a phenotype of red-hair and fair skin. Mutations of the MC1R have shown to modulate the pain response and opioid efficacy in these patients. Women are more commonly affected and often require more anaesthetic and higher dosages of opioid to achieve comparable MAC level and pain-relief, respectively, as women with other hair types.
Liem et al. showed that a greater concentration of induction and maintenance agents (sevoflurane and desflurane, respectively) were required to sustain comparable MAC levels in red-haired patients as dark haired patients.
Fillingim et al. reviewed the affect of gender, sex and pain. They concluded there is a biopsychosocial element of pain that is perceived differently by men and women. In terms of postoperative and procedural pain, the outcome might be more severe in women than men.
Delaney et al. looked at the involvement of the melanocortin-1 receptor in acute pain in mice. They found that while the MC1R is better known as a gene involved in mammalian hair colour, it was shown to be involved in the pain pathway of inflammatory but not neuropathic origin. Mutations of MC1R showed increased tolerance to noxious pain stimulus in mice.
Figures A and B are AP and lateral radiographs of a left tibia. There is a low energy, distal third shaft fracture with no cortical apposition on the AP view.
Incorrect Answers:
Answer 1,2: Mutations in the Melanocortin-1-receptor (MC1R) has not shown to affect the coagulation pathway, with no increased risk of bleeding or clotting.
Answer 4: Mutations in the Melanocortin-1-receptor (MC1R) does not affect fracture fixation or weight-bearing status post-operatively
Answer 5: There is not a higher risk of opioid allergy in these patients.
Which of the following medications used for thromboprophylaxis following orthoapedic surgery is a direct inhibitor of factor Xa?
1) Dextran
2) Rivaroxaban (Xarelto)
3) Coumadin
4) Fondaparinux (Arixtra)
5) Aspirin
Rivaroxaban (Xarelto), an oral anticoagulant, is a direct inhibitor of factor Xa.
Rivaroxaban (Xarelto) is a member of a new class of oral, direct (antithrombin- independent) factor Xa inhibitors, which restrict thrombin generation both in vitro and in vivo. Inhibition of Factor Xa interrupts the intrinsic and extrinsic pathway of the blood coagulation cascade, inhibiting both thrombin formation and development of thrombi.
Eriksson et al. compare rivaroxaban to enoxaparin for the prevention of symptomatic venous embolism following total hip arthroplasty. Major venous thromboembolism occurred in 4 of 1686 patients (0.2%) in the rivaroxaban group and in 33 of 1678 patients (2.0%) in the enoxaparin group. Additionally, major bleeding events were similar between the two groups.
Illustration A shows the mechanisms of action of various agents used for thromboprophylaxis.
Incorrect Answers:
Answer 1: The antithrombotic effect of dextran is mediated through its binding of erythrocytes, platelets, and vascular endothelium, increasing their electronegativity and thus reducing erythrocyte aggregation and platelet adhesiveness. Dextrans also reduce factor VIII-Ag Von Willebrand factor, thereby decreasing platelet function.
Answer 3: Coumadin inhibits vitamin K 2,3-epoxide reductase, thereby limiting the production of vitamin K-dependent clotting factors (II, VII, IX, X) as well
as Protein C and Protein S.
Answer 4: Fondaparinux is an indirect inhibitor of factor Xa, not direct.
Answer 5: Aspirin inhibits the production of prostaglandins and thromboxanes.
The origin of bovine derived grafts is particularly important to which of the following religious groups?
1) Christianity
2) Islam
3) Hinduism
4) Buddhism
5) Judaism
The origin of bovine-derived surgical implants should be discussed in further detail with patients ascribing to Hinduism.
Patients come from a variety of religious backgrounds. Depending on a patient’s religion, the origin of surgical implants may have implications for their use. In Hinduism, bovine animals are considered sacred. Use of cow by- products is considered purifying in nature. Subsequently, the origin of bovine derived implants should be discussed with patients ascribing to Hinduism.
Easterbrook et al. evaluated the utility of porcine and bovine surgical implants amongst those of Jewish, Muslim and Hindu faiths. Hindu religious leaders, who were surveyed, did not approve of the use of bovine surgical implants.
Enoch et al. evaluated the acceptability of biological products amongst various religious groups. The Hindu religious leaders were found to not have an objection to the use of biological implants derived from cows.
Illustration A shows a clinical photo of a fetal bovine derived dermal substitute. Incorrect Answers:
Answers 1, 2, 4, 5: While the origin of implants should be discussed with all patients prior to use, bovine derived implants may have specific implications with Hindu patients. Use of porcine-implants should be discussed with patients who are of Jewish and Muslim faiths.
Immunological testing of anti-cyclic citrullinated peptide antibodies (anti- CCP) is most commonly used for the diagnosis and prognosis of which immunological condition?
1) Ankylosis spondylitis
2) Rheumatoid arthritis
3) Psoriatic arthritis
4) Systemic lupus erythematosus
5) Reiter's syndrome
Anti-cyclic citrullinated peptide antibodies (anti-CCP) are commonly used as a marker for the diagnosis and prognosis of rheumatoid arthritis (RA).
Immunological studies are commonly performed to investigate cases of suspected rheumatoid arthritis. Rheumatoid factor has historically been used as a primary marker for RA. However, in more recent years, the use of anti- CCP antibodies has shown to be as sensitive as, and more specific than, rheumatoid factor (RF) in early and fully established disease. In general, anti-
CCP assays equate to a sensitivity of 50-75% and a specificity of 90-95%. High levels of anti-CCP have been shown to be indicative of a more erosive disease process and may be detected before the onset of arthritis.
Gardner and Kadel reviewed the laboratory studies most commonly used in rhuematologic diseases. Standard ordering for clinically suspected RA include Rf, anti- CCP, ESR/CRP as well as other markers of autoimmune diseases such as antinuclear antibodies, anticardiolipin antibodies and lupus anticoagulant, HLA-B27, and uric acid levels.
Illustration A shows the sensitivity and specificity of anti-CCP vs. RF in a variety of autoimmune diseases.
Incorrect Answers:
Answers 1,3-5: Anti-CCP is not routinely used to diagnose and monitor these conditions.
Vitamin C has been shown to decrease the likelihood of which of the following complications following surgery on the foot and ankle in non-diabetic patients?
1) Nonunion
2) Complex Regional Pain Syndrome, type II
3) Malunion
4) Complex Regional Pain Syndrome, type I
5) Wound infection
Vitamin C has been shown to decrease the likelihood of developing complex regional pain syndrome (CRPS), type 1, when given post-operatively to patients undergoing foot and ankle and wrist surgery.
CRPS is a frequent post-operative complication, with rates varying from 10-
37%. Type I CRPS does not have an identifiable nerve lesion, while type II has an identifiable nerve lesion. Multiple studies have shown that vitamin C decreases rates of CRPS following distal radius fractures, and more recently, the same has been shown following foot and ankle surgery. While the exact mechanism of CRPS is unknown, vitamin C has been shown to reduce lipid peroxidation, scavenge hydroxyl radicals, protect the capillary endothelium, and inhibit vascular permeability. All of these characteristics of vitamin C may play a role in modulating the pain pathway.
Zollinger et al. perform a double-blind, prospective, multicenter trial where
416 patients with 427 wrist fractures were randomly allocated to treatment with placebo or treatment with 200, 500, or 1500 mg of vitamin C daily for fifty days. The prevalence of complex regional pain syndrome was 2.4% in the vitamin C group and 10.1% in the placebo group.
Besse et al. compare two groups of patients undergoing surgery on the foot and ankle to determine the effect of vitamin C on the development of CRPS, type I. CRPS type I occurred in 18 cases (9.6%) in the group not given vitamin C, and 4 cases (1.7%) in the group given vitamin C.
Illustration A shows an example of a limb affected by CRPS. Note the increased swelling, a common physical exam finding in patients afflicted with the disease.
Incorrect Answers:
Answers 1, 2, 3, 5: Vitamin C has not been shown to decrease the incidence of these conditions.
A 25-year-old Spanish speaking male presents to the emergency department 6 hours after sustaining the injury seen in Figure A. He is grossly intoxicated and screaming in pain. Physical examination reveals a closed injury with overlying muscular compartments that are extremely firm to palpation. After sedating the patient, measurements of the intracompartmental pressures were all found to be**
**> 75mmHg. His wife is Spanish speaking and expected to arrive to the hospital in 2-3 hours with a relative to help with translation. No medical translator is**
**available. You attempt to outline the risk and benefits of surgery to the patient, but the he repeatedly interrupts you and yells out ,"No surgery!". An English-Spanish speaking friend is with the patient and says that he has known the patient for over 2 years and will help with any decision making. What would be the next most appropriate step in the management of this patient?
1) Delay surgery to monitor the patient for impending compartment syndrome
2) Proceed with surgery with urgent fasciotomy after documenting the necessity of treatment without consent
3) Delay the surgery until the wife arrives and able to give informed consent with the aid of a translator
4) Proceed with surgery for urgent fasciotomy after obtaining informed consent from the patients friend
5) Respect the patients autonomy and reassess the patient in the morning when he demonstrates capacity to accurately comprehend the proposed treatment
This patient is presenting with compartment syndrome of the right tibia. In a situation of required surgery for limb threatening injury without available legal consent the surgeon should confirm and document the necessity of care with a fellow colleague.
Physicians are responsible for whether a patient is able to reasonably understand their medical condition and the nature of any proposed medical procedure, including the risks, benefits, and available alternatives. If the patient lacks this capacity, disclosure imposed by the doctrine of informed
consent are excused because irreparable harm that may result from the physician’s hesitation to provide treatment. Detailed documentation is also important. In addition, the attending physician should contact the Risk Management Dept at the hospital for support prior to surgical intervention or have a medical translator involved to ensure information is being translated properly.
Katz et al. reviewed the medical decision making process of Hispanic people. They showed that Hispanic people are more likely to permit their physician to take the predominant role in making health decisions compared to Non- Hispanic people.
Figure A shows a comminuted tibia and fibula fracture. Incorrect Answers
Answer 1: This patient has confirmed compartmental syndrome. Surgical delay would be negligent.
Answer 3: Delay until his wife arrives would be necessary in non-life or-limb threatening conditions. In this case however, surgical delay could result in significant harm to the patient and therefore, the doctrine of informed consent can be excused.
Answer 4: Consent can only be given by a friend that has pre-existing notice of the patients views in the setting of emergencies and only when the dedicated decision maker is not available. The patients friend does not have enduring power of attorney and has not been appointed as a formal substitute decision-maker.
Answer 5: The patient does not demonstrate capacity to make an informed decision about his health. Therefore the views of his autonomy cannot be formulated.
A Spanish speaking child sustained the injury seen in Figure A after a fall at school. He was casted in the emergency department without the assistance of an interpreter and advised to return to see an orthopaedic surgeon in 1 week. However, the family returns to the emergency department with the child 3 months later, still in the cast. What is the most likely reason the child did not attend the recommended orthopaedic follow-up visit.?
1) The child is a victim of neglect
2) The child had no symptoms of pain
3) He was allowed to return to school wearing the cast
4) Concerns of cost
5) Follow-up instructions were not effectively communicated
The most likely reason the child did not attend the recommended orthopaedic follow-up visit was a language barrier preventing effective communication of the intended follow-up instructions.
Communication skills and cultural competence is a key element in good orthopaedic care. Poor communication can often lead to devastating outcomes. In this example, poor communication resulted in this patient being lost to
follow-up. Language barriers must be accommodated and alternative methods of communication must be utilized.
Levinson et al. examined how patients present their medical issues in clinical encounters and how physicians respond to these clues in routine primary care and surgical settings. They showed that good communication relies mostly on the physicians ability to identify patient clues within the clinical encounter.
Poor communication between the physician tended to delay clinical visits, poor follow-up and unsatisfactory outcomes.
Figure A is an AP radiograph of the elbow in a skeletally immature patient. Figure B is a lateral radiograph of the elbow with a posterior fat pad sign, suggestive of an occult fracture.
Incorrect Answers:
Answer 1,2,3,4: The most likely reason for loss to follow-up in this scenario is miscommunication regarding follow-up.
A 25-year-old female presents to the emergency room within increasing left shoulder pain after walking into a door 5 months ago. She previously sustained a femoral fracture 2 years ago after tripping on a rug. Relevant skeletal survey radiographs and tissue biopsy results are shown in Figures A through D. Laboratory investigations show normal glomerular filtration rate and creatinine clearance. Dual energy x-ray absorptiometry (DEXA) scan shows T-score of -1.4 and**
**-1.2 at the hip and lumbar spine, respectively. Which of the following laboratory values in Figure E most likely reflects this patient's condition?
1) A
2) B
3) C
4) D
5) E
This patient has primary hyperparathyroidism. Laboratory investigations are likely to show elevated serum intact parathyroid hormone (PTH), alkaline phosphatase (ALP) and ionized serum calcium, and low serum phosphate.
Primary hyperparathyroidism is most commonly caused by a single adenoma (80-90%). Besides the signs and symptoms of hypercalcemia, patients present
with calcification of menisci and articular cartilage, erosions in hand bones, "salt and pepper skull", and brown tumors (osteoclastomas), which appear as lytic regions expanding the cortex and causing pathological fractures, so named because of hemosiderin deposition.
Singhal et al. reviewed primary hyperparathyroidism. They advocate routine serum calcium levels for patients with pathologic fractures. If this is elevated, total and ionized calcium and intact PTH levels should be obtained. They feel that surgery for orthopaedic stabilization and parathyroidectomy should be performed simultaneously for better outcome.
Mankin et al. reviewed metabolic bone disease. They suggest that patients with mild disease with normal calcium levels do not require treatment. For patients with high calcium levels, treatment should include maintenance of fluid balance, localization and removal of the adenoma, bony stabilization, and medications (calcitonin, estrogen, bisphosphonates, and calcimimetics such as cinacalcet).
Figure A is an AP radiograph showing a lytic expansile lesion with pathological fracture in metadiaphyseal region of left humerus with similar lesion in the
fifth posterior rib. Figure B is an AP radiograph showing a lytic expansile lesion in the third metacarpal of the right hand and the fifth metacarpal of the left hand. Figure C is a low power micrograph of a brown tumor demonstrating a central zone of bone resorption, and filling with fibroblastic tissue, with a peripheral rim of osteoid production. Figure D is a high power micrograph of a brown tumor. In areas of bone resorption, there are numerous osteoclast-like giant cells amidst a fibrous stroma. This is unlike a true giant cell tumor, which lacks a fibrogenic stroma.
Incorrect Answers:
Answer 2: Elevated PTH and ALP, and low serum calcium and high serum phosphate are characteristic of secondary hyperparathyroidism. This occurs in chronic renal disease, where there is overproduction of PTH because of hyperphosphatemia, hypocalcemia,
and impaired 1,25-dihydroxyvitamin D production by the diseased kidneys. This patient has normal renal function. Answer 3: Elevated PTH, ALP, serum calcium and phosphate occur in tertiary hyperparathyroidism. This again occurs in chronic renal disease after prolonged chronic secondary hyperparathyroidism or after renal transplantation, where the parathyroid glands become autonomous and PTH levels do not normalize. This patient has normal renal function.
Answer 4: Normal PTH, low ALP and high serum calcium and phosphate occur in hypophosphatasia. The defect lies in tissue-nonspecific isoenzyme of alkaline phosphatase (TNSALP) and urine phosphoethanolamine levels are
elevated.
Answer 5: Low PTH, normal ALP, low serum calcium and high serum phosphate levels suggest hypoparathyroidism.
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
The clinical presentation and images are most consistent with left hip osteonecrosis as a result of coagulation and vascular occlusion caused by sickle cell anemia.
Sickle cell disease is a genetic disorder of hemoglobin synthesis characterized by 2 abnormal hemoglobin S alleles. Under low oxygen conditions the affected blood cells become "sickle shaped" and unable to pass through vessels. This results in vascular occlusion that may have a variety of clinical consequences depending on the body part affected.
Hernigou et al. review the natural history of symptomatic osteonecrosis in adults with sickle cell disease. Once symptomatic , osteonecrosis of the hip in sickle cell disease has a high likelihood of progressing and leading to femoral head collapse. Deterioration can be rapid and in most patients operative intervention is necessary to prevent further collapse or alleviate intractable pain.
Mont et al. performed a literature review on the natural history of untreated asymptomatic osteonecrosis of the femoral head. Their findings supported that asymptomatic osteonecrosis had a high prevalence of progression to symptomatic femoral head collapse. Small, medially located lesions had a low rate of progression, while medium to large sized osteonecrotic lesions did progress in a substantial number of patients. They recommended
consideration of joint-preserving surgical treatment in asymptomatic patients with a medium-sized or large, laterally located lesion.
Figure A shows an AP pelvis with left hip osteonecrosis. Figure B shows a T2 coronal MRI with left hip osteonecrosis. Illustration A shows an example of a hemoglobin molecule which has become "sickle shaped," and as a result is unable to pass through vessels efficiently.
Incorrect Answers:
: Progressive slippage of the physis though the hypertrophic zone describes
slipped capital femoral epiphysis.
Answer 3: These radiographs are most consistent with osteonecrosis of the femoral head. There is an increased incidence of Salmonella osteomyelitis in patient with Sickle Cell disease, but Staphylococcus aureus is still the most common organism.
Answer 4: Accumulation of glycosaminoglycan breakdown products describes lysosomal disorders.
Answer 5: COL5A1 or COL5A2 mutation describes the mutation of Ehlers Danlos syndrome.
What mechanism allows Staphylococcus epidermidis to adhere to surfaces and resist phagocytosis?
1) Creation of active efflux pumps
2) Methylation of 23s rRNA
3) Biofilm production
4) Alteration of cell wall permeability
5) Beta-lactamase production
Staphylococcus epidermidis is a gram-positive bacteria that utilizes a glycocalyx/biofilm to adhere to orthopedic implants and other surfaces and resist phagocytosis.
The biofilm creates a well-protected environment where bacteria can proliferate and thrive essentially undetected by the host immune system. This leads to chronic infections of orthopedic implants that can go undetected for years.
Arciola et al note that S. epidermidis can colonize surfaces in a self-generated viscous biofilm composed of polysaccharides and that the ica genes found in
56% of S. epidermidis isolates were associated with their ability to produce biofilm.
Olson et al discuss the importance of polysaccharide intercellular adhesin (PIA), a
substance produced by 50-60% of S. epidermidis strains, in the adherence of S. epidermidis to biomaterials through biofilm creation. PIA plays a critical role in initial adherence of S. epidermidis to biomaterials, biofilm
maturation and aggregation.
Illustration A shows microscopy of Staphylococcus epidermidis, which is a gram- positive, coagulase-negative cocci. Illustration B is an overview of the different classes of organisms in microbiology.
Incorrect Answers:
Answer 1,2,4,5: Efflux pump production, hydrolysis of B-lactam drugs with beta- lactamase, alteration in cell wall permeability, and ribosomal alteration are mechanisms that Staphylococcus uses to resists antibiotics.
Compared to cold-forged cobalt chrome, titanium alloys have which property?
1) Increased fatigue strength
2) Increased yield strength
3) Increased endurance limit
4) Decreased ductility
5) Decreased tensile strength
Titanium implants have decreased tensile (ultimate) strength when compared to cobalt chrome.
Ultimate strength, or tensile strength, is the maximum stress a material can withstand before undergoing breakage or failure. The ranking of ultimate strength, from highest to lowest is: 1) cobalt chrome, 2)titanium, 3)stainless steel, and 4) cortical bone.
Young's modulus of elasticity is defined as the measure of stiffness of a material in the elastic zone. A higher Young's modulus indicates a stiffer material. While titanium is highly biocompatible with a low modulus of elasticity (Young's modulus), it has poor wear characteristics making it non- suitable for femoral heads in total hip arthroplasty.
Long et al. present a review on titanium implants with a focus on bio- mechanical properties. Their study supports previous data which showed high rates of ultra-high molecular weight polyethylene wear due to accelerated breakdown when in contact with a titanium surface.
Incorrect Answers:
Answer 1: Fatigue strength, or the maximum cyclic load (10 million cycles) that a standard sized metal can absorb before fracture, is lower in titanium compared to cobalt chrome.
Answer 2: Yield strength, or the maximal stress a material can take before permanent deformation, is decreased in titanium compared to cobalt chrome. Answer 3: Endurance limit is another way of saying fatigue strength, which is discussed in incorrect answer 1. Answer 4: Ductility, or the measure of how much strain a material can take before rupturing, is higher for titanium than cobalt chrome
Peak bone mass attainment in both men and women is most dependent on which sex-steroid?
1) Testosterone
2) Progesterone
3) Growth Hormone
4) Estrogen
5) Cortisol
Estrogen has been shown to be important for both men and women in attaining peak bone mass.
Risk factors for osteoporosis are: increasing age, female sex, early menopause, fair-skinned, family history of hip fracture, low body weight, smoking, glucocorticoid use, excessive alcohol, low protein intake, and anticonvulsant or antidepressant use.
Which of the following contributes most to the ability of hyaline cartilage to attract water?
1) Aggrecan
2) Biglycan
3) Decorin
4) Fibromodulin
5) Osteocalcin
Aggrecan molecules bind to hyaluronic acid molecules via link proteins to form a macromolecule complex, known as a proteoglycan aggregate, which attracts water.
Proteoglycans are composed of subunits known as glycosaminoglycans. Glycosaminoglycans include two subtypes: chondroitin sulfate and keratin sulfate. These glycosaminoglycans link to a protein core by sugar bonds to form an aggrecan molecule. Link proteins then stabilize many of these aggrecan molecules to hyaluronic acid to form the proteoglycan aggregate. Cartilage also contains ancillary proteoglycans that are much smaller than the aggregating proteoglycans. These small proteoglycans include decorin, biglycan, and fibromodulin. They bind to other molecules (eg, type II collagen) and assist in matrix stabilization.
Ulrich-Vinther et al. authored a Level 5 review on cartilage structure. The negative charge present within the hyaline cartilage extracellular matrix attracts cations and results in an increase in tissue osmolality. This then attracts water, which decreases the osmolality. Thus, articular cartilage has a high tissue pressure, but the presence of type II collagen matrix prevents it from swelling.
Nap et al. present a basic science review article on aggrecans. They discus that the main function of aggrecan in cartilage is to resist compressive forces.
They note that the negative charge of the aggrecan molecule disaccharides create the high osmotic swelling pressure of cartilage.
Illustration A depicts the molecular organization of an aggregated proteoglycan molecule. Incorrect Answers:
Answer 2,3,4: These are small proteoglycans that bind to other molecules (eg, type II collagen) and assist in matrix stabilization.
Answer 5: Osteocalcin is the most prevalent noncollagenous protein in bone.
What effect do bisphosphonate medications have on spinal fusion surgery when taken in the postoperative period?
1) Any effect can be counteracted by taking calcium supplements
2) No effect
3) Increased risk of wound infection
4) Smaller fusion mass
5) Decreased fusion rate
Bisphosphonates (e.g. alendronate) are used to treat osteoporosis. The mechanism of action is inhibiting the formation of the ruffled border of osteoclasts, resulting in decreasing bone turnover.
Huang et al performed a rat study comparing alendronate to placebo and found that fusion rates were lower in those treated with alendronate. However,
the fusion masses were larger in the alendronate treated rats despite lower fusion rates (why #4 is incorrect).
Lehman et al in another placebo controlled rate study found that the fusion rates for placebo (76%) were greater than the alendronate group (45%). Alendronate works on osteoclasts and does not affect calcium directly. Taking calcium should have no effect on alendronate (why #1 is incorrect). At this time there are no formal recommendations of when to stop bisphosphonate medication prior to spinal fusion surgery.
A therapeutic study presents a systematic review of 15 high- quality randomized controlled trials with homogeneous results. What level of evidence is this considered?
1) I
2) II
3) III
4) IV
5) V
A systematic review of high-quality clinical trials is considered a Level I study.
A systematic review is a powerful tool used to identify, evaluate and appraise all high- quality research related to a specific question. Systematic reviews, in contrast to most narrative review articles, adhere to strict scientific design by following eight steps; 1) defining a question and developing inclusion criteria,
2) searching for studies, 3) selecting studies and collecting data, 4) assessing risk of bias, 5) data analysis and meta-analyses, 6) addressing biases, 7) presenting results, and 8) interpreting results and drawing conclusions. When the results from the systematic review are homogeneous (less variability between studies than would be expected by chance), the data from a systematic review can be combined into a meta- analysis.
Wright et al. discuss the levels of evidence in orthopaedic journals as presented by the AAOS Evidence-Based Practice Committee. Based on levels of evidence, the AAOS provides grades of recommendation (A, B, C, I). Grade A recommendations are supported by Level 1 studies with consistent findings, whereas Grade I do not have enough evidence to support a recommendation.
Illustration A shows an "evidence pyramid." MA = meta-analysis, SR = systematic review, RCT = randomized controlled trial.
Incorrect Answers:
Answer 2: An example of a Level II study is prospective comparative study. Answer 3: An example of a Level III study is a case control trial.
Answer 4: An example of a Level IV study is a case series.
Answer 5: An example of a Level V study is one based on expert opinion.
Progressive overloading of muscles in adults during exercise leads to which of the following?
1) Increased muscle fiber length
2) Decreased musculotendinous junction length
3) Slowed peak contraction velocity
4) Muscle fiber hypertrophy
5) Decreased sarcomere length
Strength training is achieved by incremental progressive loading of muscles, in effort to increase muscle fiber contraction coordination and eventually hypertrophy of the muscle fibers themselves.
Kraemer et al. provide an American College of Sports Medicine position statement on appropriate training regimens. They recommend that loads
corresponding to 8-12 repetition maximum (RM) be used in novice training. For intermediate to advanced training, it is recommended that individuals use a wider loading range, from 1-12 RM in a periodized fashion. For local muscular endurance training, it is recommended that light to moderate loads (40-60% of 1 RM) be performed for high repetitions (> 15) using short rest periods (
Which of the following would lead to accelerated maturation in the zone of hypertrophy at the physis?
1) An activating mutation in TGF-ß
2) A deactivating mutation in the parathyroid hormone-related peptide (PTHrP) receptor
3) A deactivating mutation in prostaglandin E2
4) An activating mutation in the SMAD-3 protein
5) An activating mutation in the Indian Hedgehog (Ihh) protein
A deactivating mutation in the parathyroid hormone-related peptide (PTHrP) receptor would lead to accelerated maturation in the zone of hypertrophy.
PTHrP has been shown to play an important role in the regulation of cell proliferation at the physis. It is postulated that physeal chondrocytes regulate the local production of PTHrP by secreting a protein called Indian Hedgehog (Ihh). Ihh stimulates the chondrocytes to produce PTHrP, which slows the maturation of proliferative
chondrocytes.
Ballock et al. discuss the biology of the growth plate. With regards to cell proliferation, they describe how the proliferation of chondrocytes in the growth plate is under the control of a feedback loop involving PTHrP, Indian
Hedgehog, and TGF-ß.
Illustration A shows the Ihh/PTHrP negative-feedback loop. Incorrect Answers:
Answer 1: TGF-ß is a potent inhibitor of maturation, including cell hypertrophy, Type-X collagen expression, and alkaline phosphatase activity. An activating mutation would lead to decelerated maturation at the physis.
Answer 3: Prostaglandin E2 has not been shown to affect cell proliferation and maturation at the physis.
Answer 4: SMAD-3 increases the activity of TGF-ß. This would lead to decelerated maturation at the physis.
Answer 5: As described above, Ihh controls the release of PTHrP from chondrocytes. Activating Ihh would lead to more production of PTHrP, which would delay maturation at the physis.
All of the following statements regarding sclerostin are true EXCEPT?
1) It is a product of the SOST gene
2) Overexpression results in decreased bone mass
3) It is thought to be associated with sclerosteosis and Van Buchem disease
4) It activates the Wnt pathway
5) It is derived from osteocytes
Sclerostin inhibits the Wnt pathway, making answer choice 4 the correct answer.
Sclerostin is an osteocyte-derived negative regulator of Wnt signaling in osteoblasts. Amongst other things, the Wnt pathway and the Wnt proteins are important regulators of bone mass. They are thought to work by stimulating the production of osteoblasts. By inhibiting the Wnt pathway, sclerostin leads to decreased bone mass.
Dijke et al. discuss the role of the SOST gene in the conditions sclerosteosis and Van Buchem disease. They describe the SOST as a gene that encodes sclerostin, which is a negative regulator of Wnt signaling in osteoblasts. The
authors argue that the high bone mass seen in sclerosteosis and Van Buchem disease may be caused by increased Wnt signaling.
Day et al. review the Wnt and hedgehog signaling pathways. The Wnt and hedgehog pathways, they describe, control the differentiation of progenitor cells into osteoblasts or chondrocytes. They found that up-regulation of Wnt signaling leads to suppression of chondrocyte formation and enhanced ossification, which may be important in fracture healing.
Illustration A shows the pathway by which Wnt promotes osteoblast formation. In addition to increasing osteoblast formation, the pathway upregulates OPG, which blocks osteoclastogenesis. Illustration B shows how sclerostin inhibits
the Wnt pathway, resulting in a net decrease in bone mass. Illustration C shows an example of Van Buchem disease, an autosomal recessive disorder characterized by hyperostosis of the skull, mandible, clavicles, ribs, and diaphyseal cortices of the long bone.
Incorrect Answers:
Answers 1, 2, 3, 5: These statements are all correct regarding sclerostin.
Which of the following is more likely to occur following a total knee arthroplasty without patellar resurfacing versus a total knee arthroplasty with patellar resurfacing in patients with rheumatoid arthritis?
1) Patellar dislocation
2) Anterior knee pain
3) Extensor tendon rupture
4) Decreased quadriceps strength
5) Patellar clunk syndrome
Patients with rheumatoid arthritis who undergo a total knee arthroplasty without patellar resurfacing are more likely to have anterior knee pain when compared to the same patient population with resurfaced patellas.
Resurfacing the patella during total knee arthroplasty is a topic of controversy. Those against resurfacing note minimal issues with patellar tilt and
overstuffing the patellofemoral joint. Supporters of resurfacing state that the patellofemoral joint will eventually become arthritic if not resurfaced, and that the rate of anterior knee pain is much higher. Multiple studies, however, have shown superior results in patients with rheumatoid arthritis that have had their patella resurfaced.
Burnett et al. review the indications for patellar resurfacing during total knee arthroplasty. They consider not resurfacing the patella in patients less than 60 with non-inflammatory arthritis and a maintained patellofemoral joint space.
Holt et al. also review the role of patellar resurfacing. They mention that patellar resurfacing should be routinely done in patients with rheumatoid arthritis, preoperative patellofemoral pain, height greater than 160cm, weight greater than 60kg, or advanced patellar changes either pre- or intra- operatively.
Illustration A shows plain anteroposterior (a) and lateral (b) radiographs of the knee in a patient with rheumatoid arthritis. Degenerative changes are present in all 3 joint compartments. There is collapse of the lateral compartment with resultant valgus deformity. Erosion of the anterior aspect of the distal femoral metaphysis due to pannus is also seen.
Incorrect Answers:
Answer 1: Patellar dislocation has not been found to be higher in patellas that are not resurfaced.
Answer 3: Extensor tendon rupture is more common in patients that have had their patella resurfaced.
Answer 4: Multiple studies have not shown a difference in quadriceps strength with or without resurfacing.
Answer 5: Patellar clunk syndrome is more common in patients who have had their patella resurfaced.
Which of the following pharmacologic treatments for osteoporosis has been associated with the potential risk for osteosarcoma development?
1) Ergocalciferol
2) Non-nitrogen containing bisphosphonate
3) Monoclonal Ig2 against RANKL
4) Nitrogen containing bisphosphonates
5) Recombinant parathyroid hormone (1-34)
Recombinant parathyroid hormone (1-34) (Forteo) has been demonstrated to cause osteosarcoma in animal models but has not been to shown to cause the same effect in humans.
1-34 amino terminal residues of parathyroid hormone(1-84) administered in daily subcutaneous injections leads to bone formation. Continuous infusion leads to bone resorption.
Subbiah et al. published a case report on a patient that developed osteosarcoma following external beam radiation and recombinant teriparatide use. They discuss that though there have been nearly a 1/2 million patients treated safely with recombinant terirparatide and it is important to recognize patients that are contraindicated for treatment with recombinant teriparatide.
The FDA's Black Box warning states the following: "In male and female rats, teriparatide caused an increase in the incidence of osteosarcoma (a malignant bone tumor) that was dependent on dose and treatment duration. The effect was observed in rats at systemic exposures to teriparatide ranging from 3 to
60 times the exposure in humans given a 20-mcg dose. Because of the uncertain relevance of the rat osteosarcoma finding to humans, teriparatide should be prescribed only to patients for whom the potential benefits are considered to outweigh the
potential risk. Teriparatide should not be prescribed for patients who are at increased baseline risk for osteosarcoma (including those with Paget's disease of bone or unexplained elevations of alkaline phosphatase, open epiphyses, or prior external beam or implant radiation therapy involving the skeleton)"
Incorrect Answers:
Answer 1: Ergocalciferol does not cause an increase in sarcoma
Answer 2 & 4: Bisphosphonates can cause esophagitis, dysphagia, gastric ulcers, osteonecrosis of the jaw (ONJ), and atypical subtrochanteric fractures. Answer 3: Denosumab (Prolia) can cause arthralgia, nasopharyngitis, and back pain.
While conducting a retrospective review of patients undergoing two different techniques for open reduction and internal fixation of ankle fractures, the investigator would like to assess whether there is any significant difference between the mean patient age in the two groups. The two groups are normally distributed. Which of the following tests would be most appropriate?
1) Student t-test
2) Analysis of Variance (ANOVA)
3) Fisher exact test
4) Kruskal-Wallis test
5) Chi-square test
A Student-test would be the most appropriate test for analyzing means of parametric (continuous) variables that are normally distributed between two groups.
Data can be characterized as non-parametric (categorical, ordinal) or parametric (continuous). Parametric data, such as age, are observations for which difference between the numbers have meaning on a numerical scale. Non-parametric data are observations which can be expressed as a
dichotomous (yes or no) outcome such as gender.
Kocher and Zurakowski present a Level 5 review of epidemiology and biostatistics. The authors state that univariate or bivariate analysis, such as the student t-test, is used to assess the relationship of a single independent and a single dependent variable.
Incorrect Answers:
Answer 2: Analysis of variance is used to evaluate means of parametric data between three or more groups when the data is normally distributed
Answer 3: Fisher exact test is used to compare proportions for non-parametric data when the expected frequency is small (less than five per group)
Answer 4: Kruskal-Wallis test is used to evaluate medians of three or more groups when the data are not normally distributed.
Answer 5: Chi-square test is used to compare proportions for categorical or ordinal data (non-parametric)
Which of the following arteries provides the blood supply to the outer third of a long bone diaphysis?
1) Nutrient artery
2) Periosteal arterioles
3) Medullary artery
4) Emissary artery
5) Perichondral artery of LaCroix
Periosteal arterioles (low pressure system) supply the outer third of the adult diaphyseal cortex.
Blood supply to long bone comes from three sources: 1) nutrient artery
system, 2) metaphyseal-epiphyseal system, and 3) periosteal system. Nutrient arteries (high pressure system) enter the long bone diaphyseal cortex and
then enter the medullary canal where it branches into ascending and descending arteries and supplies the inner 2/3 of the diaphysis via Haversian systems.
Bong et al. present a review article regarding intramedullary nail effects on bone healing. They report that intramedullary nails can have negative effects on endosteal and cortical blood flow but this is offset by an increase in extraosseous circulation. During early fracture healing blood flow is centripetal
(outside to inside) because high pressure nutrient artery system is often disrupted. Illustration A depicts the blood supply for the adult diaphsysis. Incorrect
Answers:
Answer 1: High pressure system that branches from major systemic arteries and supplies the inner 2/3 of mature bone.
Answer 3: The nutrient artery enters through the medullary canal and divides into ascending and descending arteries.
Answer 4: Cortical capillaries drain to the emissary venous system. There is no described emissary artery for long bones.
Answer 5: Perichondrial artery is the major source of nutrition of the growth plate
DNA methylation, histone modification, nucleosome location, or noncoding RNA are hypothesized to contribute to the process whereby inheritable genetic alterations occur that do not involve DNA mutation. Which of the following terms best defines this process?
1) Transgenes
2) Epigenetics
3) Gene enhancers
4) Gene promoters
5) Transformation
Epigenetic changes are defined as inheritable genetic alterations that do not involve DNA mutation.
The cells in a multicellular organism have almost identical DNA sequences, yet maintain different terminal phenotypes. This nongenetic cellular memory, which records developmental and environmental cues is the basis for epigenetics. DNA methylation, histone modification, nucleosome location, or noncoding RNA are hypothesized to contribute to the process.
Maher et al discuss epigenetic influences in the realm of orthopaedics. They report new data stating that increases in matrix metalloproteinase (MMP) expression in osteoarthritis is associated with altered methylation of key promoter sequences. They also report elevated levels of an enzyme involved in epigenetic gene silencing in osteoarthritis- affected chondrocytes, SIRT1, increased the expression of matrix genes and suppressed that of MMPs.
Incorrect Answers:
Answer 1: Transgenes are genes that are artificially introduced into a single- celled embryo and are present in all cells of that organism.
Answer 3: Gene enhancers are a region of a gene that positively regulates rates of transcription.
Answer 4: Gene promoters are a regulatory segment of DNA that controls start of transcription adjacent to the transcription initiation site of a gene.
Answer 5: Transformation refers to inserting a plasmid into a bacterium with added recombinant DNA.
A 72-year-old woman presents with severe hip pain after stepping off of a curb. She denies any trauma or prior history of hip pain. Her past medical history is reviewed including a list of her current medications. Which of the following of her medications would place her at increased risk for a non-traumatic hip fracture?
1) Phenytoin
2) Cephalexin
3) Simvastatin
4) Glipizide
5) Allopurinol
Phenytoin is an anticonvulsant which has been found to increase the risk of osteoporosis and, subsequently, nontraumatic fractures.
Possible mechanisms explaining the association between anticonvulsants and bone loss include hepatic induction of cytochrome P450 enzymes (increases vitamin D catabolism), direct osteoblast inhibition, impaired calcium absorption, elevated homocysteine, inhibition of response to PTH, hyperparathyroidism, reduced reproductive sex hormones, and reduced vitamin K level.
Lee et al. found that anticonvulsant use (phenobarbital, carbamazepine, phenytoin, and valproate) increases the risk of osteoporosis, and also increases the risk of fracture by 1.2 to 2.4 times.
Jette et al. found an increased fracture risk for carbamazepine, clonazepam, gabapentin, phenobarbital, and phenytoin. Odds ratios ranged from 1.24 (clonazepam) to 1.91 (phenytoin).
Incorrect Answers:
Answers 2-5: These medications do not place a patient at a significant risk for non- traumatic hip fracture.
What part of the articular cartilage has the highest concentration of proteoglycans and the lowest concentration of water?
1) Superficial
2) Transitional
3) Deep
4) Tidemark
5) Calcified cartilage
This question requires that you know the 4 zones of articular cartilage: the superficial zone, the transitional zone, the deep zone (also called middle or radial zone) and the zone of calcified cartilage. The deep zone has chondrocytes with a more spheroidal shape which align themselves perpendicular to the joint surface. This zone has the largest diameter collagen fibrils, the highest concentration of proteoglycans, and the lowest
concentration of water. The collagen fibers of this zone pass into the tidemark, a thin basophilic line seen of H&E stains that corresponds to the boundary between calcified and uncalcified cartilage. Lastly the calcified cartilage zone is a thin zone of calcified cartilage that separates the radial zone (uncalcified cartilage) and the subchondral bone. The cells in this region have a smaller
volume than the cells of the radial zone, and these cells have extremely low level of metabolic activity.
The cross-sectional area of a muscle is the factor most responsible for which of the following?
1) Amount of maximal tension
2) Speed of contraction
3) Duration of contraction
4) Type of contraction
5) Fatigability
Force generation, or the amount of maximal tension that can be generated by a given skeletal muscle is most dependent on the cross-sectional area of the muscle.
The cross-sectional area is the main determining factor in force generated by the muscle and is controlled by the number of myofibrils that contract. Weight lifting can lead to muscle hypertrophy, increased cross-sectional area, and increased force (ability to lift heavier weights). Fiber types have less to do with the force of contraction and more to do with the duration and speed of contraction.
Baroni et al. investigated the chronology of neural and morphological adaptations to knee extensor eccentric training. After 12 training weeks, significant increases in strength and anatomical cross-sectional area (19%) were seen.
Illustration A shows how muscle hypertrophy from strength training increases cross- sectional area.
Incorrect Responses:
The other functional attributes of a muscle, such as speed and duration of contraction and fatigability are more predicated on muscle fiber type than on the area.
An orthopaedic resident wants to answer a focused research question of whether mobile bearing knee arthroplasty has superior functional outcomes compared to fixed bearing knee arthroplasty. The resident mathematically combines the results from multiple retrospective cohort studies following QUORUM (Quality of Reporting of Meta-analyses) guidelines. What is the highest level of evidence that this meta-analysis can achieve?
1) Level I
2) Level II
3) Level III
4) Level IV
5) Level V
The level of evidence assigned to a meta-analysis is based on the lowest level of evidence of the included studies. In this case, the studies included in the meta-analysis were retrospective cohort (Level III) studies.
A meta-analysis is a systematic review that combines the results of multiple studies to answer a focused clinical question.
Clarke discusses the QUORUM guidelines which are intended to address standards for
improving the quality of reporting of meta-analyses of clinical randomized controlled trials. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement and MOOSE (Meta-analysis Of Observational Studies in Epidemiology) guidelines are similar standards. A
similar set of guidelines called CONSORT (Consolidated Standards of Reporting Trials) guidelines are available for randomized trials.
Incorrect Answers:
1: Level I studies include high-quality randomized controlled trials
2: Level II studies include lower-quality RCTs and prospective cohort studies.
4: Level IV studies include case-series or poor-quality cohort and case-control studies. 5: Level V studes are expert opinion articles.
An adolescent patient is treated with a 6mm solid intramedullary nail. Compared to a 12mm solid nail of the same material, the 6mm nail has:
1) 1/2 the torsional rigidity
2) 1/4 the torsional rigidity
3) 1/16 the torsional rigidity
4) 1/8 the torsional rigidity
5) the same torsional rigidity
Nail radius affects nail bending and torsional rigidity. For a solid circular nail, the torsional rigidity is proportional to the fourth power of the radius. Thus a nail with 1/2 the diameter (6mm compared to 12mm) and therefore 1/2 the radius (3mm compared to 6mm) would have(1/2)^4 = 1/16 the torsional rigidity (answer 3). Bong et al. performed a great review of the biomechanics and biology of intramedullary nailing of the lower extremity.
The ability of a study to detect the difference between two interventions if one in fact exists describes which of the following?
1) Positive predictive value
2) Hawthorne effect
3) Effect size
4) Power
5) P value
The study power is defined as the ability of a study to detect the difference between two interventions if one in fact exists.
The power of a statistical test is correlated to the magnitude of the treatment effect, the designated type I (alpha) and type II (beta) error rates, and the sample size n. The power is equal to (1-beta) whereby beta is the false negative rate.
Kocher et al. present a Level 5 review of epidemiology and biostatistics. The review discusses study design, hypothesis testing, diagnostic performance, measures of effect, outcomes assessment, evidence-based medicine, and biostatistics. They discuss that in the orthopaedic literature power is typically set at 80%, (leaving a 20% chance that the study will display no significant association when there is an actual association.) Illustration A shows the interaction of study variables on the power of a study. Incorrect Answers:
Answer 1: Positive predictive value is the probability that a patient with a positive test actually has the disease. This value is dependent on the prevalence of disease
Answer 2: Hawthorne effect is a behavior that is changed when participants have knowledge that their behavior is being monitored.
Answer 3: Effect size is the difference in outcome between the treatment group and the control group divided by the standard deviation.
Answer 5: P value is defined as the probability, under the assumption of no difference (null hypothesis), of obtaining a result equal to or more extreme than what was actually observed if the experiment were repeated over and over
Which of the following best describes the appearance of chondrocytes and orientation of collagen fibrils in the superficial zone of articular cartilage?
1) Round chondrocytes oriented parallel with the tidemark and collagen fibrils oriented perpendicular to the tidemark
2) Round chondrocytes oriented parallel with the tidemark and collagen fibrils oriented parallel to the tidemark
3) Flattened chondrocytes oriented parallel with the tidemark and collagen fibrils oriented perpendicular to the tidemark
4) Flattened chondrocytes oriented perpendicular with the tidemark and collagen fibrils oriented perpendicular to the tidemark
5) Flattened chondrocytes oriented parallel with the tidemark and collagen fibrils oriented parallel to the tidemark
Flattened chondrocytes oriented parallel with the tidemark and collagen fibrils oriented parallel to the tidemark best describes the orientation of collagen fibrils in the superficial zone of articular cartilage.
The primary orientation of the collagen fibers in the superficial zone is parallel with the joint surface, in order to resist compressive and sheer forces. This zone is the thinnest one, and it sometimes is referred to as the gliding zone. The surface layer, known as the lamina splendens, is cell-free and composed mainly of randomly oriented, flat bundles of fine collagen fibrils. Deep to the lamina splendens are more densely packed collagen fibers interspersed with elongated, oval chondrocytes oriented parallel to the articular surface.
Sophia Fox et al. in a review article state that the superficial zone comprises 10-20% of articular cartilage and is composed of mostly type II and IX collagen.
Illustration A displays that articular cartilage has four distinct zones: (1) a superficial (tangential) zone, (2) a middle (transitional) zone, (3) a deep (radial) zone, and (4) the calcified zone. Illustration B demonstrates the collagen orientation and chondrocyte appearance in the different articular cartilage layers.
Incorrect Answers:
Answer 1-4: None of these accurately describe the appearance of
chondrocytes and orientation of collagen fibrils in the superficial zone of articular cartilage.
A 52-year-old male underwent a right total knee arthroplasty 3 days ago and reports new onset dyspnea. His vitals signs include a temperature of 98.8, pulse of 133, blood pressure of 130/77, respiratory rate of 28, and oxygen saturation of 91% on room air. A chest radiograph shows atelectasis. Which of the following findings is most likely also present?
1) Hyperchloremic metabolic acidosis
2) Jugular venous distention with tracheal deviation
3) EKG demonstrating S-wave in lead I Q-wave in lead III T-wave inversion in lead III
4) Pleural effusion with pleural/serum protein >0.5 and pleural/serum LDH > 0.6
5) Increased carbon monoxide diffusing capacity (DLCO)
The patient's clinical presentation is consistent with a pulmonary embolism and an EKG demonstrating S-wave in lead I Q-wave in lead III T-wave inversion in lead III is most likely associated with this diagnosis.
The most commonly seen signs in the EKG associated with PE are sinus tachycardia, right axis deviation and right bundle branch block. Sinus tachycardia is however only found in 8–69% of people with PE. The S1Q3T3 pattern discussed here is from acute right heart strain and is termed the "McGinn-White sign" after the initial describers but is only found in about 10-
20% of people with a PE. Patients undergoing total knee arthroplasty (TKA) without DVT prophylaxis have symptomatic PE at a rate of approximately 8%. Patients undergoing TKA have a higher risk for the presence of DVT but are at a lower risk for symptomatic PE than patients undergoing total hip arthroplasty.
Stein et al. present a study that found that dyspnea or tachypnea occurred in
92% of patients diagnosed with a pulmonary embolism. They also report that dyspnea or tachypnea was less commonly encountered in elderly patients with no previous cardiopulmonary disease.
Illustration A is a table that describes some of the characteristic findings of pulmonary embolism on a chest radiograph.
Incorrect answers:
Answer 1: Non-saddle pulmonary emboli are most often associated with respiratory alkalosis due to tachypnea.
Answer 2: Jugular venous distention with tracheal deviation is seen with tension pneumothorax.
Answer 4: Pleural effusion with pleural/serum protein >0.5 and pleural/serum LDH > 0.6 is consistent with an exudate such as pneumonia
Answer 5: Increased carbon monoxide diffusing capacity (DLCO) is not seen with pulmonary emboli.
The estimated range of values which likely includes the unknown parameter under investigation is defined as which of the following?
1) Standard deviation
2) Mode
3) Variance
4) Confidence interval
5) Incidence
When an unknown value is sought, the confidence interval gives the statistician a set of parameters within which the “true” value is located. The confidence interval is used to indicate the reliability of an estimate. The standard deviation is a quantity calculated to indicate the extent of deviation for a group as a whole. The mode is the value which
occurs most frequently in a given set of data. The variance is a quantity equal to the square of the standard deviation. The incidence is the frequency of an occurrence (or disease).
**Which of the following is true regarding the cell seen in Figure A?**
1) Originates from hematopoietic cells from a macrophage lineage
2) Derived from undifferentiated mesenchymal cells
3) They are former osteoblasts trapped in the matrix they produced
4) They become cartilage under intermediate strain and low oxygen tension
5) They form bone by producing non-mineralized matrix
The image shown in Figure A shows an osteoclast remodeling cortical bone through a cutting cone mechanism. Osteoclasts orginate from hematopoietic cells from a macrophage cell lineage.
Osteoclasts can be distinguished from other bone cells by their multinucleated giant cells and ruffled border on the cell periphery which increases the surface area for bone resorption. Their main function is to reabsorb bone after being stimulated by RANK-L and IL-1. A balance between osteoclast and osteoblast activity is necessary for a stable calcium level in the blood.
Caterson et al. review mesenchymal stem cells and their ability to regenerate musculoskeletal tissue. They state that potential applications include replacement of bone graft for segmental defects, nonunions, spinal fusions, and articular resurfacing.
Illustration A shows the differences between osteoblasts, osteoclasts and osteocytes. Video V describes the role and function of osteoblasts and osteocytes.
Incorrect Answers:
Answer 2: This is true of osteoblasts. Answer 3: This is true of osteocytes.
Answer 4: This is true of osteoprogenitor cells. Answer 5: This is true of osteoblasts.
What is the equation for determining specificity of a clinical test?
1) True negatives divided by the sum of the true negatives and false positives
2) True negatives divided by the sum of the true negatives and false negatives
3) True positives divided by the sum of the true negatives and false positives
4) True positives divided by the sum of the true positives and false negatives
5) True positives divided by the sum of the true positives and false positives
Specificity is the probability that a test result will be negative in patients without disease (answer 1). The sensitivity is the probability that a test result will be positive in patients with disease (answer 4). The positive predictive value is the number of patients with a positive test result who are correctly diagnosed and the negative predictive value is the opposite of this (answers 5 and 2, respectively). The referenced review article by Kocher describes many of the statistical tools useful for practicing orthopaedic surgeons.
Which of the following graft materials has the least potential to elicit an immune response?
1) Fresh irradiated corticocancellous bulk allograft
2) Fresh frozen fibular strut allograft
3) Fresh frozen Achilles tendon allograft
4) Fresh Achilles tendon allograft
5) Freeze dried cancellous bone chips
Of the options listed, freeze dried cancellous allograft has the least potential to elicit an immune response. Remember, all allograft tissue has more of an immune response generating capability than autograft tissue, which has the least of any of these materials.
All allograft materials carry immunogenic properties, which decrease as the material is processed via the various sterilizing, freezing, or drying process(es). As the processing increases, the mechanical characteristics of the graft tends to decrease.
Ahlmann et al. compared the complications associated with harvesting iliac crest bone graft from the anterior crest and posterior crest. They found the rates of both minor complications (p = 0.006) and all complications (p =
0.004) were significantly higher after the anterior harvest procedures than they were after the posterior procedures. They recommend that iliac crest bone graft be harvested posteriorly whenever possible.
Incorrect Answers:
Answer 1: Most bone and soft tissue allografts undergo irradiation to remove bacteria or other infectious agents, but this does not prevent an immune
response in itself.
Answer 2: Fresh frozen allografts have more immunogenic potential than freeze dried, but less than fresh materials. Fresh allograft is not typically utilized, as the processing of allograft (bone or soft tissue) provides the safety of minimizing infectious disease transmission.
Answer 3: Fresh frozen allografts have more immunogenic potential than freeze dried, but
less than fresh materials. Thus fresh Achilles tendon allograft has the highest immunogenicity.
Answer 4: Fresh Achilles tendon allograft will elicit the greatest immunogenic response.
**Which of the following statements is correct regarding Vitamin D?**
1) 1,25-dihydrocholecalciferol is the best laboratory study to determine a Vitamin D deficiency
2) 25-hydroxycholecalciferol is the active form of Vitamin D
3) 24,25-dihydroxycholecalciferol is an inactive form of Vitamin D
4) 1,25-dihydrocholecalciferol is converted to 25-hydroxycholecalciferol in the kidney
5) The half-life of 1,25-dihydrocholecalciferol is longer than 25- hydroxycholecalciferol
24,25-dihydroxycholecalciferol in an inactive form of Vitamin D. High levels of
1,25-dihydroxyvitamin D stimulate the enzymatic production of 24,25- dihydroxyvitamin D, the inactive form of vitamin D, thereby self-regulating the action of 1,25-dihydroxyvitamin D.
Vitamin D is paramount to proper calcium homeostasis and has important clinical implications in the orthopaedic patient. Vitamin D3 is synthesized in the skin and is converted to 25-hydroxycholecalciferol in the liver. 25- hydroxycholecalciferol is then converted in the kidney into 1,25- dihydroxycholecalciferol, the active form of vitamin D. The best test to determine Vitamin D deficiency is the measurement of 25- hydroxycholecalciferol, as it has a longer half-life and circulating levels are
1,000x more than 1,25-dihydrocholecalciferol.
Patton et al. review the importance of Vitamin D in the orthopaedic patient. They discuss the implications of Vitamin D deficiency, and urge orthopaedic surgeons to be proficient in both the diagnosis and treatment of the condition.
Bogunovic et al. measured the levels of 25-hydroxycholecalciferol in 723 patients who were to undergo orthopaedic surgery. 40% of these patients were noted to be deficient in Vitamin D, with the highest rates in patients scheduled to undergo trauma and sports surgery.
Illustration A reviews Vitamin D metabolism. 24,25-dihydroxycholecalciferol is referred to as pre-Vitamin D.
Incorrect Answers:
Answer 1: 25-hydroxycholecalciferol is the best laboratory study to determine
Vitamin D deficiency due to its long half-life and high circulating levels. Answer 2: 1,25- dihydroxycholecalciferol is the active form of Vitamin D. Answer 4: 25- hydroxycholecalciferol is then converted in the kidney into 1,25- dihydroxycholecalciferol. Answer 5: The half-life of 25-hydroxycholecalciferol is 2-3 weeks, while the
half-life of 1,25-dihydrocholecalciferol is only 4-6 hours.
You are the team physician for a collegiate football team and receive weekly injury reports from the athletic trainer. All players with sickle-cell trait are listed at the bottom to remind all on-field**
**personnel that they may need which of the following?
1) Oxygen supplementation and oral or IV hydration
2) Additonal layers of warm clothes
3) Increased pain medication
4) Avoidance of non-steroidal anti-inflammatory medicines
5) Days of rest due to increased joint pain
Players with a blood test indicating the presence of sickle-cell trait (SCT) are at risk for exertional sickling collapse which responds initially to rest, hydration and oxygen.
SCT is not a disease but a condition, resulting from inheritance of one gene for sickle hemoglobin (S) and one gene for normal hemoglobin (A).
The vital concern is exertional sickling collapse, which can be fatal, occurs in a variety of sports, and is a leading cause of death in college football.
According to the review by Eichner, sickling collapse is an “intensity”- associated syndrome that differs from the other common causes of collapse. The best approach in college football may be tailored precautions to prevent sickling collapse and enable athletes with SCT to thrive. Other clinical concerns in SCT are compartment syndromes and lumbar myonecrosis, splenic infarction, gross hematuria, hyposthenuria, and venous thromboembolism.
Kark et al. reviewed all cases of sudden death occurring among 2 million enlisted recruits during basic training in the U.S. Armed Forces from 1977 to
1981/. They concluded that "recruits in basic training with the sickle-cell trait have a substantially increased, age-dependent risk of exercise-related sudden death unexplained by any known preexisting cause".
Incorrect Responses:
2/. no research to support need for warmer clothes and cases occur year round. 3&5/. these are typical of sickle cell disease, not SCT.
4/. important in patients with renal impairment, which is not typically seen in SCT.
A physician is interested in using platelet-rich plasma (PRP) for treatment of osteochondral lesions of the talus. He is reviewing a prospective cohort study that compares 40 patients treated with PRP and cast immobilization for 6 weeks vs. 36 patients treated conservatively with cast immobilization for 6 weeks. All patients were treated at the same time and institution. The study was not randomized although treatment and control groups were matched
**appropriately to reduce selection bias. Follow-up in each group was**
> 80% over 1 year. The paper reported significant improvement with use of PRP based on three standard foot and ankle outcome scores (AOFAS, SF-36, FOAS). What is the level of evidence for this study?
1) Level I
2) Level II
3) Level III
4) Level IV
5) Level V
This is prospective cohort study with Level-II evidence.
Level of evidence provides guidance to the study quality. It is used to assess therapeutic studies (as with this question), prognostic studies, diagnostic studies and economic or decision models. When determining the level of evidence, readers must critically appraise the study question, treatment, intervention and outcomes of the study design. Level-II therapeutic studies consist of well-designed prospective cohort studies, poor-quality randomized controlled trials (follow-up less than 80%) and systematic review of Level-II studies or non-homogenous Level-I studies.
Wright et al. provided an excellent summary of clinical research study level of evidence. This has been provided as Illustration A.
Illustration A shows a chart of level of evidence. There is a column for each type of study which corresponds to a row that outlines the level of evidence based on study
design.
Incorrect Answers:
Answer 1: Level-I evidence include randomized controlled studies with follow- up>80% and systematic review of Level-I RTC studies (homogenous studies) Answer 3: Level-III evidence include case control studies, retrospective cohort studies and systematic review of Level-III studies
Answer 4: Level-IV evidence include case series with no control group (or compare to a historical control group)
Answer 5: Level V evidence include expert opinion
Low serum phosphate and normal calcium levels are found in what common etiology of hereditary rickets?
1) X-linked hypophosphatemic
2) Vitamin D-dependent, type I
3) Vitamin D-dependent, type II
4) Autosomal dominant hypophosphatemic
5) Jansen's metaphyseal chondrodysplasia
Low serum phosphate and normal calcium levels are found in X-linked hypophosphatemic rickets.
X-linked hypophosphatemic rickets is the most common form of hereditary rickets. It is an X-linked dominant disorder which has been linked to the PHEX gene. Laboratory findings
of this disorder include low serum phosphate, normal serum calcium and 25 hydroxycholecalciferol levels, and inappropriately low 1,25-dihydroxyvitamin D3.
Carpenter et al. showed hypophosphatemic rickets was initially referred to as “vitamin D resistant rickets” due to its lack of response to therapeutic vitamin D. Current treatment with activated vitamin D metabolites (calcitriol or
alfacalcidol) and phosphate salts have been shown to help with this condition.
Illustration A shows an insufficiency fracture of the proximal tibia in an adult patient with X-linked hypophosphatemic rickets. A stress fracture on the medial tibia may be a presenting feature of untreated disease.
Incorrect Answers:
Answer 2: Vitamin D-dependent rickets, type I, is a rare autosomal recessive disorder. Answer 3: Vitamin D-dependent rickets, type II, is a rare autosomal recessive disorder, most often caused by mutations in the vitamin D receptor gene. Answer 4: Autosomal dominant hypophosphatemic results from a rare mutation in the fibroblast growth factor 23 (FGF23) gene.
Answer 5: Jansen's metaphyseal chondrodysplasia is a skeletal dysplasia that results from ligand-independent activation of the type 1 parathyroid hormone
receptor (PTHR1).
A healthy patient undergoes routine pre-operative laboratory testing and is found to have a leukocyte count of 1.5 × 10(9) cells/L. When the historical records are examined, this is found to be the patients base-line level over a period of years. Which of the following statements is most likely to be true:
1) The patient is at a significantly higher risk of surgical infection
2) The patient is more likely to be of African than of European descent
3) The patient is more likely to be of European than of Middle Eastern descent
4) The patient is more likely to be a non-athlete than an athlete
5) The patient is more likely to be female than male
The clinical presentation is consistent with Benign Ethnic Neutropenia, a condition in which a patient has chronic, benign, inborn and lifelong absolute neutrophl count below population mean. This condition is found in the U.S. to be most common in African- Americans, some groups of Middle Eastern patients, males, children under 5 years old, and athletes compared to non- athletes.
A standardized level at present for abnormally low absolute neutrophil count (ANC) is below 1.5 x 10(9) cells/L, however this may not have clinical or scientific relevance as a cutoff point, particularly in the affected Ethnic groups. Fewer than 1% of all populations have absolute neutrophil count
A 14-year-old patient has sustained a complete ACL tear of his right knee. Which of the following options has shown to be the most limiting factor for access to pediatric orthopaedic management in the United States?
1) Sex of the patient
2) Type of health insurance
3) Child greater than 10 years of age
4) Acute knee injuries requiring operative treatment
5) Timing of the referral
The type of health insurance in the pediatric population has shown to be a significant factor for access to specialized healthcare in the United States.
Access to pediatric orthopaedic management has been well investigated. Numerous Level 4 studies have shown that orthopaedic offices in urban and rural areas prefer treating patients with private insurance over patients with Medicaid.
Iobst et al. telephoned 100 urban and rural orthopaedic outpatient offices to schedule an appointment for a 10-year-old patient with a forearm fracture. They showed that 8/100 offices would schedule an appointment within 1 week to the child with Medicaid insurance, as compared to 36/100 that gave an appointment to a child with private insurance.
Pierce et al. contacted 42 orthopaedic practices to schedule an appointment for a 14- year-old patient with an ACL injury. They showed that 38/42 offices scheduled an appointment for the child within 2 weeks with private insurance. This compared to 6/42 that scheduled an appointment for a similar child with Medicaid.
Incorrect Answers:
Answers 1,3,4,5: The limiting determinant to healthcare in the pediatric population has shown to be the type of health insurance. Sex, age of child, operative vs nonoperative injuries and timing of referral have not been shown to affect access to healthcare.
The perioperative use of which medication has been shown to increase the risk of post-operative infection following orthopaedic procedures in patients with rheumatoid arthritis (RA)?
1) Naproxen
2) Leflunomide
3) Sulfasalazine
4) Etanercept
5) Aspirin
Of the medications listed, only etanercept has been shown to increase the risk of post- operative infection following orthopaedic procedures in patients with RA.
Etanercept is a TNF-alpha antagonist with a short half-life that is administered once or twice weekly in patients with RA. Since TNF-alpha plays a central role in the pathogenesis of RA and is instrumental in causing joint destruction, the inhibition of this molecule has shown excellent results in controlling disease. The most powered study on TNF-alpha inhibitor use in the perioperative period following an orthopaedic procedures demonstrated a significant increase in
post-operative infection.
Howe et al. review the medical management of patients with RA who underwent orthopaedic procedures. They state that while there is conflicting information regarding TNF-alpha antagonists, they recommend holding them prior to major orthopaedic interventions.
Giles et al. review 91 patients with rheumatoid arthritis who underwent an orthopaedic procedure. They found TNF-alpha inhibitor therapy to be significantly associated with the development of a serious postoperative infection (p=.041)
Perhala et al. review 61 patients with RA who were treated with methotrexate during the perioperative period surrounding a total joint arthroplasty. They
failed to find a significant increase in complications in this patient group, stating the perioperative use of methotrexate does not affect wound healing or increase the likelihood of periprosthetic infection.
Illustration A shows the site of action of TNA-alpha inhibitors in the RA pathway.
Incorrect Answers:
Answer 1: Naproxen should be discontinued 3 days prior to surgery because of its ability to increase bleeding time and the subsequent potential for increased blood loss.
Answer 2: Leflunomide is an inhibitor of pyrimidine synthesis. It has not been shown to increase the risk of post-operative infection.
Answer 3: Sulfasalazine's mechanism of action is largely unknown, but it has not been shown to increase the risk of post-operative infection.
Answer 5: Aspirin has not been shown to increase infection if continued in the perioperative period.
Communication breakdown is the leading cause of which of the following?
1) Delayed diagnoses
2) Medication errors
3) Surgical site infections
4) 1 and 2
5) All of the above
Communication failures are the leading cause of wrong side surgeries, medication errors and diagnostic delays.
Poor communication sets up environments in which medical errors can take place. Per the Joint Commission, medical errors may be the among the top 10 causes of death in the United States. Establishing open lines of communication is critical to reduce the risk of error and enhance patient safety.
Gandhi et al. designed a framework to study missed or delayed diagnoses and their causes. The most significant factors contributing to errors were poor handoffs, failures in judgment, failures in memory and failures in knowledge.
O’Daniel et al. review the importance of professional communication and collaborative team efforts. They note that patient safety is at risk when poor communication is in place. The leading cause for medication errors, treatment delays and wrong-site surgeries is communication failure.
Illustration A shows the leading causes of death in the United States. This includes “preventable errors” as a cause.
Incorrect Answers:
Answers 1, 2: Communication failures can lead to delays in diagnosis and
treatment, medication errors and wrong side surgery
Answers 3, 5: Communication failure is not a direct contributor to surgical site infection
**Which of the following is true regarding osteoprotegerin (OPG)?**
1) It is secreted by osteoclasts
2) It increases bone resorption
3) Binds to prostoglandin E2 before stimulating osteoclasts
4) Osteoprotegerin knock-out mice develop osteopetrosis
5) Binds to and sequesters RANKL
Osteoprotegerin is a decoy receptor for RANKL. Binding to RANKL causes decreased production of osteoclasts by inhibiting the differentiation of osteoclast precursors.
Bone resporption/remodeling is a complex process regulated by a large variety of molecules. Molecules that have shown to inhibit osteoclasts include OPG, calcitonin, estrogen, TGF-B, and IL-10. Corticosteroids have been shown to decrease production of OPG, thereby enhancing osteoclast formation and longevity. Prolia, or denosumab, is a newly approved drug used to treat osteoporosis and has a mechanism of action similar to osteoprotegerin
(inhibits binding of RANKL to RANK).
Boyle et al. review osteoclast differentiation and activation. The authors state that targeted disruption of OPG causes increased osteoclastogenesis and/or activation resulting in osteopenia.
Illustration A shows how OPG binds to RANKL inhibiting the stimulation of osteoclasts.
Incorrect Answers:
Answer 1: OPG is secreted by osteoblasts.
Answer 2: OPG decreases bone resorption by inactivating RANKL. Answer 3: OPG does not bind to prostoglandin E2, nor does it stimulate osteoclasts.
Answer 4: RANKL knock-out mice creates an osteopetrosis-like condition.
A 55-year-old woman has T-score -2.0 at the femoral neck. According to the World Health Organization Fracture Risk Assessment Tool (FRAX), she has a ten- year probability of sustaining a hip fracture of 1.5% and a ten-year probability of sustaining a major osteoporotic fracture of 8.9%. Which of the following statements is true regarding her antiresorptive therapy management?
1) Antiresorptive therapy should be started based on her T-score
2) Antiresorptive therapy should be started based on her risk of hip fracture alone
3) Antiresorptive therapy should be started based on her risk of major osteoporotic fracture alone
4) Antiresorptive therapy should not be started
5) Antiresorptive therapy should be started based on her risks of both hip fracture and major osteoporotic fracture
This patient has osteopenia. Assessment by FRAX shows that ten-year risk of hip fracture is less than 3% and her ten-year risk of major osteoporosis- related fracture is less than 20%. Therefore, antiresorptive therapy is not indicated at this time.
According to the 2008 National Osteoporosis Foundation guidelines, pharmacologic treatment for osteoporosis should be considered if patients are
postmenopausal women or men greater than 50 years old AND meet one of the following criteria: (1) they have a prior hip or vertebral fracture, (2) they have a T score -2.5 or less at the femoral neck or spine, (3) they have a T score between -1.0 and -2.5 at the femoral neck or spine AND a 10-year risk of hip fracture greater than 3% or 10-year risk of major osteoporosis-related fracture greater than 20%.
FRAX (World Health Organization Fracture Risk Assessment Tool) calculates
10-year risk of fracture based on the following variables: age, sex, race, height, weight, BMI, history of fragility fracture, parental history of hip fracture, use of oral glucocorticoids, secondary osteoporosis and alcohol use to calculate 10-year risk of fracture.
Unnanuntana et al. reviewed the assessment of fracture risk. Besides FRAX score and T-score, they discussed biochemical markers of bone formation and resorption, which are useful for monitoring the efficacy of antiresorptive / anabolic therapy, and may help identify patients at high risk for fracture.
Ekman et al. reviewed the role of the orthopaedic surgeon in minimizing mortality and morbidity associated with fragility fractures. The surgeon should consider prescribing appropriate medications, physical therapy, assessing fall risk and preventing falls and changing lifestyle factors (exercise, smoking and alcohol).
Illustration A shows the FRAX online tool ([_http://www.shef.ac.uk/FRAX/tool.aspx?country_ _=__=9)._ Illustration B shows the](http://www.shef.ac.uk/FRAX/tool.aspx?country=9/)) clinical risk factors considered in FRAX calculation.
Incorrect Answers:
Answer 1: T-score of -2.0 is not an indication for initiating treatment. Answers 2, 3, 5: Her FRAX score does not show a risk of hip or osteoporosis- related fracture high enough to be an indication for initiating treatment.
A 32-year-old runner sustains a trimalleolar left ankle fracture. She undergoes open reduction and internal fixation and is kept non- weightbearing after surgery. At 2 months, what changes will occur in the articular cartilage of both her knees as a result of her current weightbearing regimen?
1) Cartilage thickening in the left (ipsilateral) knee and no change in cartilage thickness in the right (contralateral) knee
2) Cartilage thinning in both knees
3) Cartilage thinning in the left (ipsilateral) knee and no change in cartilage thickness in the right (contralateral) knee
4) Cartilage thinning in the left (ipsilateral) knee and increased cartilage thickness in the right (contralateral) knee
5) Increased cartilage thickness in both knees
After a period of off-loading, the off-loaded limb will experience cartilage thinning. The contralateral limb will not demonstrate any cartilage changes.
Physiologic loading of cartilage increases proteoglycan synthesis and cell proliferation and is chondroprotective. Joint immobilization leads to cartilage thinning, tissue softening, and reduced proteoglycan content, leading to cartilage erosion. Joint overuse leads to cartilage damage (in vitro only).
Hinterwimmer et al. examined cartilage atrophy after partial load bearing
using quantitative MRI. They found cartilage thinning in all knee compartments (greatest thinning, medial tibia; least thinning, patella). There was no change in cartilage morphology in the contralateral knee.
Sun reviewed the relationship between mechanical loading and cartilage degeneration. In OA, cartilage breakdown occurs at the articular surface, and is then fueled by synovial proteases and cytokines. In RA, synovial cells and macrophages are the source of degradative enzymes and incite cartilage destruction.
Milward-Sadler et al. examined mRNA levels following mechanical stimulation in normal and osteoarthritic chondrocytes. Normal chondrocytes showed increased aggrecan mRNA and decreased matrix metalloproteinase 3 (MMP-3) mRNA after stimulation. This
chondroprotective response was absent in osteoarthritic chondrocytes.
Illustration A shows pro- and anti-inflammatory mechanisms of mechanical loading on chondrocytes. Underloading and overloading induce cartilage damage through pathways involving the upregulation of MMPs and ADAMTSs (ADAMTS, a disintegrin and metalloproteinase with thrombospondin motifs, or aggrecanase). Physiological loading blocks these increases.
Incorrect Answers:
Answer 1: Cartilage THINNING (not thickening) will occur on the offloaded limb (left). Answers 2 and 5: There will be a difference in cartilage thickness between knees as a result of different weightbearing status on both lower extremities. Answer 4: Noticeable cartilage hypertrophy does not occur on the uninjured limb.
A morbidly obese 40-year-old man is scheduled to undergo hemilaminectomy for resection of an painful osteoid osteoma of the T6 lamina. He is positioned prone on a Jackson table and localization is performed with intraoperative fluoroscopy prior to the start of the case. At close to the end of the case, intraoperative frozen section reveals only normal bone fragment from the resected lamina. A probe is placed and a cross-table lateral radiograph reveals that the T7 lamina was resected instead of T6. At this point, the surgeon should**
**do all of the following EXCEPT
1) Complete the surgery
2) Abort the case and obtain further imaging
3) Apologize to the patient and family
4) Formally document the error in the operative report
5) Inform the patient and family immediately after the operation
should include a disclosure of known facts and an explanation as to the likely cause, as well as ongoing treatment, follow up care, and prognosis.
The AAOS Information Statement about Wrong Site Surgery identifies 3 treatment steps following discovery of an error during surgery under general anesthesia: Return the patient to his preoperative condition, perform the correct procedure at the correct site, and advise the patient and family of what occurred and the likely consequences, if any, of the wrong- site surgery.
The AAOS Information Statement on Communicating Adverse Events states that the surgeon has an ethical and professional obligation to disclose the error to the patient and/or family. Disclosure should include what happened, why it happened, health implications, and what measures are being instituted to prevent recurrences.
Incorrect Answers:
Answer 1: Completion of the surgery at the correct site is necessary unless proceeding with the surgery at the correct site would increase the risk associated with extended operating time, or if correct-site surgery would result in an additional unacceptable disability.
Answers 3: Many patients have expressed that an apology is important. In the apology, the physician should express support for the patient and family, show compassion and concern, and acknowledge their emotional response and needs. This will help to set clear goals for the future patient-physician interaction.
Answer 4: Full disclosure is recommended and there should be no attempt at concealment or obfuscation. This is especially true for the operative report. Answer 5: A composed dialogue between the surgeon and both patient and family after the event is preferred to a hurried call from the operating room which is prone to misunderstanding and leaves no room for questions and answers.
All of the following are Standards of Professionalism relating to interactions with industry for practicing orthopaedic surgeons EXCEPT:
1) Decline gifts from industry with a market value over $100 (unless they are medical textbooks or patient educational materials)
2) Disclose to the patient any financial arrangements with industry that relates to the patient's treatment
3) Accept no direct financial inducements from industry for utilizing a particular implant
4) Disclose any relationship with industry to colleagues who may be influenced by your work
5) Decline to participate in industry sponsored non-CME courses or
conferences
The AAOS has adopted the Standards of Professionalism (SOP). These SOP’s establish mandatory, minimum levels of acceptable conduct for fellows and members of the AAOS to engage in relationships with industry. There are 17 standards with relation to industry. Answer choice 5 is not a SOP as surgeons are allowed to participate in or consult in meetings that are conducive to the effective exchange of information. The SOP also stipulate that tuition, travel, and modest hospitality (including meals and receptions) are allowed to attend an industry-sponsored non-CME course.
A prospective randomized trial is conducted to test the efficacy of Vitamin C versus placebo in treating patients who develop chronic regional pain syndrome (CRPS) after distal radius fractures. At first follow-up, the rates of CRPS are 1% and 9% in the study and placebo group, respectively. Which statistical test is most appropriate to determine significance?
1) Single factor analysis of variance
2) Chi-square test
3) Student t-test
4) Mann-Whitney rank sum test
5) Wilcoxon rank sum test
In the study provided, we need to determine whether distributions of categorical variables differ from one another. The appropriate study is the chi- square test.
Data can be classified as numerical (continuous) or categorical (proportional). Responses to such questions as "What is your major?" or Do you own a car?" are categorical because they yield data such as "biology" or "no." In contrast, responses to such questions as "How tall are you?" or "What is your G.P.A.?" are numerical. When comparing two independent means from numeric data, a t-test is performed. However, if categorical data is being compared, the chi- square test will determine if the proportions are really different.
Kocher et al. review basic clinical epidemiology and biostatistics relevant to orthopaedic surgery. Amongst other things, they describe that data can be summarized in terms of measures of central tendency, such as mean, median, and mode, and in terms of measures of dispersion, such as range, standard deviation, and percentiles.
Illustration A shows an algorithm for determining which test to use for varying data. Incorrect Answers:
Answer 1: Analysis of variance (ANOVA) is used to compare means of three or more independent groups in which the data are normally distributed.
Answer 3: Student t-test is used for comparing means of continuous data that is normally
distributed.
Answer 4: The Mann-Whitney and Wilcoxon rank sum tests are used for comparing means of non-continuous data.
Answer 5: The Mann-Whitney and Wilcoxon rank sum tests are used for comparing means of non-continuous data.
A 35-year-old patient is involved in a motor vehicle accident and sustains multiple fractures including a closed comminuted proximal meta-diaphyseal tibia fracture. The surgeon is considering bridge plating the fracture using a minimally invasive approach. Which of the following is true regarding bridge plating?
1) A locked plate construct (locked screws) or hybrid construct (locked and non- locked screws) is necessary.
2) Periosteal stripping is performed through two incisions proximal and distal to the fracture.
3) Bridge plating is performed following direct reduction of the fracture.
4) AO Type A diaphyseal fractures are best treated with this technique.
5) Bridge plating with a long working length creates a flexible, axially stable construct.
In bridged plating, only the most proximal and distal screw holes are filled. This creates a flexible, axially stable construct.
Bridge plating is applicable to all long-bone fractures with complex fragmentation and where intramedullary nailing or conventional plate fixation is not suitable. The construct preserves the blood supply to the fracture fragments as the fracture site is undisturbed during the operative procedure. It provides RELATIVE stability, allowing for some motion at the fracture site, leading to callus formation and secondary bone healing. The construct is FLEXIBLE because of increased distance between the 2 screws closest to the fracture (long working length), allowing for stress distribution and permitting more motion at the fracture site. The construct is also AXIALLY STABLE because the plate acts as an extramedullary splint and resists axial compression.
Livani et al. advocate using an anterior or antero-lateral approach for minimally invasive plating of the humerus. They recommend that distal access is obtained first, allowing identification of the lateral antebrachial cutaneous nerve. For distal fractures, they recommend extending the plate down to the lateral column.
Apivatthakakul et al. defined minimally-invasive plate osteosynthesis (MIPO) danger zones from the lateral epicondyle. They found the musculocutaneous nerve averaged 18- 43% of the humeral length, the danger zone for the radial nerve averaged 36-59% of the humeral length, and the most dangerous screws that penetrated or touched the radial nerve lay 47-53% of the humeral length.
Illustration A shows a distal tibia fracture. Illustration B shows radiographs 5 months after bridge plating of this fracture. There is callus formation, characteristic of indirect bone healing.
Answer 1: Locked plates are not necessary for bridge plating. Conventional plate/screws may be used.
Answer 2: Bridge plating through a minimally invasive approach avoids periosteal stripping and the plate lies in a submuscular location. It is especially important where comminution is present and preservation of tenuous
periosteal blood supply is critical.
Answer 3: Bridge plating is usually applied following some form of indirect reduction. Indirect reduction involves manipulating fragments into the correct position without opening the fracture site, thus minimizing damage to the blood supply. The main principle of indirect reduction is distraction.
Answer 4: AO Type A simple diaphyseal fractures are best treated with intramedullary nailing (relative stability) or anatomic reduction and compression plate fixation (absolute stability).
Which of the following components of bone is most responsible for compressive strength?
1) Type I collagen
2) Osteocalcin
3) Proteoglycans
4) Osteonectin
5) Osteopontin
Proteoglycans, in addition to calcium hydroxyapatite [Ca10(PO4)6(OH)2], are most responsible for providing compressive strength.
Bone is composed of both organic and inorganic components. Inorganic components include calcium hydroxyapatite and osteocalcium phosphate. Organic components include collagen, proteoglycans, matrix proteins, cytokines and growth factors. While Type I collagen is responsible for providing the tensile strength of bone, proteoglycans and calcium hydroxyapatite [Ca10(PO4)6(OH)2] are most responsible for providing compressive strength. Proteoglycans contain a core protein with various
numbers of covalently attached side chains of glycosaminoglycans. In addition to providing compressive strength, they are also responsible for binding growth factors and inhibiting mineralization.
Knothe et al. review the osteocyte. They discuss that osteocytes are the most abundant
cells in bone, are actively involved in maintaining the bony matrix, and may act as mechanosensors.
Illustration A shows a proteoglycan aggregate, which can form when individual molecules link onto a chain of hyaluronic acid.
Incorrect Answers:
Answer 1: Type I collagen is responsible for the tensile strength of bone. Answer 2: Osteocalcin is the most abundant non-collagenous protein in the matrix and promotes the mineralization and formation of bone.
Answer 4: Osteonectin is believed to have a role in regulating calcium or organizing mineral in matrix.
Answer 5: Osteopontin is a cell-binding protein.
A prospective, randomized controlled trial of 150 patients undergoing total hip arthroplasty is performed to test whether repair of the capsule during a posterior approach reduces post-operative dislocations in the first three months. The study found no difference in dislocation rate if the capsule was repaired versus not repaired (p =**
**.34). Subsequently, a multicenter follow-up study of 2000 patients showed that repairing the capsule led to a decreased dislocation rate**
**in the first three months (p = .03). Assuming the second study reflects reality, which of the following errors occurred in the first study?
1) Observer bias
2) Type-II error
3) Alpha error
4) Type-I error
5) Confounding error
In this situation, the null hypothesis was accepted when it should have been rejected.
This is a type-II error.
A study can have two types of errors. Type-I errors, or alpha errors, occur when the null hypothesis is rejected when it should have been accepted. The alpha level refers to the probability of a type-I error. By convention, the alpha level of significance is set at 0.05, which means that we accept the finding of a significant association if there is less than a one in twenty chance that the observed association was due to chance alone. Type-II errors, or beta errors, occur when the null hypothesis is accepted when it should be rejected. This
often occurs when studies are underpowered. In the example above, the null hypothesis is that repair of the capsule does not reduce dislocations within the first three months. Since the first study did not show a statistically significant difference, the null hypothesis was accepted. Since a more powered study showed that repair of the capsule does reduce dislocations, the null hypothesis should have been rejected in the initial study (if it was adequately powered).
Fosgate et al. review the importance of sample size calculations when performing research. They state that sample size ensures statistical significance if the subsequent data collection is perfectly consistent with the assumptions made for the sample size calculation (assuming power was set as
50% or greater).
Illustration A shows the difference between type-I and type-II errors. Video V is a lecture discussing statistical definition review of PPV, NPV, sensitivity and specificity.
Incorrect Answers:
Answer 1: Observer bias is when the observer (usually the investigator) influences the results of an experiment as a result of their own bias. Answer 3: Alpha errors are the same as type I error (see below).
Answer 4: A type-I error would reject the null hypothesis when it is true. Answer 5: A confounder is a variable that has associations with both the dependent and independent variables, potentially distorting their relationship. Confounders are not technically considered "errors," but instead are variables
that properly constructed studies attempt to avoid.
**Which of the following is a potential cause of fretting corrosion?**
1) The micromotion at the femoral head-neck junction in a modular total hip replacement
2) A stainless-steel cerclage wire is in contact with a titanium-alloy femoral stem
3) Friction between polyethylene liner and femoral head leading to osteolysis
4) The formation of pits within a stainless-steel plate and the subsequent release of metal ions
5) The formation of an adherent oxide coating on titanium implants
Micromotion at the femoral head-neck junction can lead to fretting corrosion, one of the most common causes of failure of a modular implant.
Modular components give surgeons excellent intraoperative flexibility, but are susceptible to various types of corrosion. While titanium and cobalt-chrome contain a protective surface oxide layer, continued micromotion at the modular junction may disrupt the protective layer leading to fretting corrosion, defined as micromotion at contact sites under load. This may eventually lead to a painful synovitis that necessitates a revision procedure.
Srinivasan et al. review modularity in total hip arthroplasty. Amongst other things, they discuss the modularity of the femoral head/neck junction, describing the morse taper interlocking system that provides both axial and rotational stability.
Illustration A shows an example of corrosion at the head/neck junction of a total hip arthroplasty.
Incorrect Answers:
Answer 2: This is an example of galvanic corrosion, as two dissimilar metals are in contact with each other.
Answer 3: This is an example of adhesive wear.
Answer 4: This is an example of pitting corrosion, or crevice corrosion. Answer 5: This process is called self-passivization, enabling titanium to become corrosion resistant.
Which of the following situations is most likely to decrease sentinel event errors?
1) Physician and nurse training is lengthened by 20%
2) Resident hours are decreased to 55 hours per week
3) An environment is created where all members of the healthcare team feel empowered to express their concerns and beliefs
4) Holding individuals responsible for errors in clinical judgement
5) Physicians and nurses are assigned to a smaller number of patients
Creating an environment where all members of the healthcare team feel empowered to express their beliefs increases communication, the key element in decreasing sentinel events.
Research has shown that 70% of sentinel event errors are caused by improper communication. Specific ways to improve communication include effective clinical handover between shifts and breaking down the "hierarchy" so that all members of the team can discuss their expectations and concerns. Barriers to effective communication include distractions, cultural differences, power distance relationships, time pressures, and lack of organization.
Leonard et al. describe specific clinical experiences in the application of surgical briefings, properties of high reliability perinatal care, the value of critical event training and simulation, and benefits of a standardised communication process in the care of patients transferred from hospitals to skilled nursing facilities. They recommend embedding standardized tools and behaviors to bridge differences in communications styles between clinicians.
Incorrect Answers:
Answer 1: Increasing training time is unlikely to decrease sentinel event errors if effective communication is not established.
Answer 2: Some studies have shown increased error rates with decreased resident physician work hours.
Answer 4: Holding individuals responsible for errors in clinical judgement has not specifically been cited as a way to decrease errors within a healthcare setting.
Answer 5: While this may decrease sentinel event errors, this has not been to be as effective as improvements in communication.
Which of the following side effects is most strongly associated with the use of NSAIDs?
1) Hepatic dysfunction
2) Renal impairment
3) Prolonged QTc
4) Seizures
5) Hematuria
All NSAIDs have the potential to cause serious renal impairment.
NSAIDs work by inhibiting the cyclooxygenase pathway (COX), which is comprised of the COX-1 and COX-2 pathways. The COX-1 pathway is involved in prostaglandin E2– mediated gastric mucosal protection and thromboxane effects on coagulation, while the COX-2 pathway is mainly involved with the modulation of pain and fever without effect on platelet function. While selective COX-2 inhibitors have a decreased side effect profile, all NSAIDS
have the potential to cause renal impairment and their use should be limited in patients with underlying renal disease.
Horlocker et al. review multimodal pain management in the perioperative setting of a total joint arthroplasty. Specifically, they note that NSAIDs should be used cautiously in patients with underlying renal dysfunction who are to undergo a procedure with major blood loss.
Griffin et al. reviewed 1,799 patients hospitalized for acute renal failure. They found that NSAIDs increased the risk of renal failure by 58% and that NSAID use resulted in 25 excess hospital admissions per 10,000 years of use.
Illustration A shows the COX pathways and their inhibition by NSAIDs. Incorrect Answers:
Answers 1, 3, 4, 5: NSAIDs have not been shown to be strongly associated with these side effects.
It is recommended that invasive dental work be completed prior to the initiation of which of the following medications?
1) Glucosamine
2) Cholecalciferol
3) Levothyroxine
4) Teriparatide
5) Bisphosphonates
Bisphosphonate therapy combined with invasive dental work increases the risk for development osteonecrosis of the jaw.
Bisphosphonates are a class of drugs that prevent bone mass loss by inhibiting osteoclast resorption. They are used in the treatment of vertebral compression fractures, non- vertebral fragility fractures, osteogenesis imperfecta, multiple myeloma, and avascular necrosis. Because bisphosphonates have been associated with osteonecrosis of the jaw, it is suggested that all invasive
dental work be completed prior to initiation of treatment.
Pazianas et al. (2011) review the safety profile of bisphosphonates. Specifically, they cite gastrointestinal discomfort, atypical femur fractures, osteonecrosis of the jaw, ocular inflammation, and musculoskeletal pain as common side effects. They state there is limited evidence surrounding
bisphosphonate's association with esophageal cancer and atrial fibrillation.
Pazianas et al. (2007) reviewed 11 publications that reported 26 cases of osteonecrosis of the jaw following initiation of bisphosphonate treatment. Age
>60 years, female sex, and previous invasive dental treatment were the most common characteristics of those who developed ONJ.
Illustration A shows the various bisphosphonates and their mechanisms of action. Illustration B shows an example of osteonecrosis of the jaw, a side effect that has been linked to bisphonphonate treatment.
Incorrect Answers:
Answer 1: Glucosamine is a dietary supplement used in the management of osteoarthritis. It is not contraindicated prior to dental work.
Answer 2: Cholecalciferol is Vitamin D3. Toxicity and side effects are rare with Vitamin D therapy.
Answer 3: Levothyroxine is used in the treatment of hypothyroidism. It is not contraindicated prior to dental work.
Answer 4: Teriparatide (Forteo) has been used in the treatment of osteonecrosis of the jaw caused by bisphosphonates.
Figures A and B show radiographs of a 24-year-old female with a soccer injury. A physical examination reveals an isolated, closed injury with no clinical features of neurovascular injury or compartment syndrome. She has been consented to be treated with intramedullary nail fixation. A pre-operative note by the anaesthesiology team makes reference to the patients fair skin and natural red-hair color. How will this information affect the post-operative management of this patient?
1) Longer duration of anticoagulation due to increased risk of DVT
2) Avoiding anticoagulation medications due to increased risk of bleeding
3) Require higher dosages of post-operative analgesia
4) Longer period of non-weight bearing on surgical limb
5) Avoiding opioids due to higher risk of unrecognized allergies
Female patients with natural red-hair may require higher dosages of post- operative analgesia compared to other hair types.
Melanocortin-1-receptor (MC1R) is one of the key proteins involved in hair color and skin tone. Mutations of the MC1R alleles can render this protein non- functional, which results in a phenotype of red-hair and fair skin. Mutations of the MC1R have shown to modulate the pain response and opioid efficacy in these patients. Women are more commonly affected and often require more anaesthetic and higher dosages of opioid to achieve comparable MAC level and pain-relief, respectively, as women with other hair types.
Liem et al. showed that a greater concentration of induction and maintenance agents (sevoflurane and desflurane, respectively) were required to sustain comparable MAC levels in red-haired patients as dark haired patients.
Fillingim et al. reviewed the affect of gender, sex and pain. They concluded there is a biopsychosocial element of pain that is perceived differently by men and women. In terms of postoperative and procedural pain, the outcome might be more severe in women than men.
Delaney et al. looked at the involvement of the melanocortin-1 receptor in acute pain in mice. They found that while the MC1R is better known as a gene involved in mammalian hair colour, it was shown to be involved in the pain pathway of inflammatory but not neuropathic origin. Mutations of MC1R showed increased tolerance to noxious pain stimulus in mice.
Figures A and B are AP and lateral radiographs of a left tibia. There is a low energy, distal third shaft fracture with no cortical apposition on the AP view.
Incorrect Answers:
Answer 1,2: Mutations in the Melanocortin-1-receptor (MC1R) has not shown to affect the coagulation pathway, with no increased risk of bleeding or clotting.
Answer 4: Mutations in the Melanocortin-1-receptor (MC1R) does not affect fracture fixation or weight-bearing status post-operatively
Answer 5: There is not a higher risk of opioid allergy in these patients.
Which of the following medications used for thromboprophylaxis following orthoapedic surgery is a direct inhibitor of factor Xa?
1) Dextran
2) Rivaroxaban (Xarelto)
3) Coumadin
4) Fondaparinux (Arixtra)
5) Aspirin
Rivaroxaban (Xarelto), an oral anticoagulant, is a direct inhibitor of factor Xa.
Rivaroxaban (Xarelto) is a member of a new class of oral, direct (antithrombin- independent) factor Xa inhibitors, which restrict thrombin generation both in vitro and in vivo. Inhibition of Factor Xa interrupts the intrinsic and extrinsic pathway of the blood coagulation cascade, inhibiting both thrombin formation and development of thrombi.
Eriksson et al. compare rivaroxaban to enoxaparin for the prevention of symptomatic venous embolism following total hip arthroplasty. Major venous thromboembolism occurred in 4 of 1686 patients (0.2%) in the rivaroxaban group and in 33 of 1678 patients (2.0%) in the enoxaparin group. Additionally, major bleeding events were similar between the two groups.
Illustration A shows the mechanisms of action of various agents used for thromboprophylaxis.
Incorrect Answers:
Answer 1: The antithrombotic effect of dextran is mediated through its binding of erythrocytes, platelets, and vascular endothelium, increasing their electronegativity and thus reducing erythrocyte aggregation and platelet adhesiveness. Dextrans also reduce factor VIII-Ag Von Willebrand factor, thereby decreasing platelet function.
Answer 3: Coumadin inhibits vitamin K 2,3-epoxide reductase, thereby limiting the production of vitamin K-dependent clotting factors (II, VII, IX, X) as well
as Protein C and Protein S.
Answer 4: Fondaparinux is an indirect inhibitor of factor Xa, not direct.
Answer 5: Aspirin inhibits the production of prostaglandins and thromboxanes.
The origin of bovine derived grafts is particularly important to which of the following religious groups?
1) Christianity
2) Islam
3) Hinduism
4) Buddhism
5) Judaism
The origin of bovine-derived surgical implants should be discussed in further detail with patients ascribing to Hinduism.
Patients come from a variety of religious backgrounds. Depending on a patient’s religion, the origin of surgical implants may have implications for their use. In Hinduism, bovine animals are considered sacred. Use of cow by- products is considered purifying in nature. Subsequently, the origin of bovine derived implants should be discussed with patients ascribing to Hinduism.
Easterbrook et al. evaluated the utility of porcine and bovine surgical implants amongst those of Jewish, Muslim and Hindu faiths. Hindu religious leaders, who were surveyed, did not approve of the use of bovine surgical implants.
Enoch et al. evaluated the acceptability of biological products amongst various religious groups. The Hindu religious leaders were found to not have an objection to the use of biological implants derived from cows.
Illustration A shows a clinical photo of a fetal bovine derived dermal substitute. Incorrect Answers:
Answers 1, 2, 4, 5: While the origin of implants should be discussed with all patients prior to use, bovine derived implants may have specific implications with Hindu patients. Use of porcine-implants should be discussed with patients who are of Jewish and Muslim faiths.
Immunological testing of anti-cyclic citrullinated peptide antibodies (anti- CCP) is most commonly used for the diagnosis and prognosis of which immunological condition?
1) Ankylosis spondylitis
2) Rheumatoid arthritis
3) Psoriatic arthritis
4) Systemic lupus erythematosus
5) Reiter's syndrome
Anti-cyclic citrullinated peptide antibodies (anti-CCP) are commonly used as a marker for the diagnosis and prognosis of rheumatoid arthritis (RA).
Immunological studies are commonly performed to investigate cases of suspected rheumatoid arthritis. Rheumatoid factor has historically been used as a primary marker for RA. However, in more recent years, the use of anti- CCP antibodies has shown to be as sensitive as, and more specific than, rheumatoid factor (RF) in early and fully established disease. In general, anti-
CCP assays equate to a sensitivity of 50-75% and a specificity of 90-95%. High levels of anti-CCP have been shown to be indicative of a more erosive disease process and may be detected before the onset of arthritis.
Gardner and Kadel reviewed the laboratory studies most commonly used in rhuematologic diseases. Standard ordering for clinically suspected RA include Rf, anti- CCP, ESR/CRP as well as other markers of autoimmune diseases such as antinuclear antibodies, anticardiolipin antibodies and lupus anticoagulant, HLA-B27, and uric acid levels.
Illustration A shows the sensitivity and specificity of anti-CCP vs. RF in a variety of autoimmune diseases.
Incorrect Answers:
Answers 1,3-5: Anti-CCP is not routinely used to diagnose and monitor these conditions.
Vitamin C has been shown to decrease the likelihood of which of the following complications following surgery on the foot and ankle in non-diabetic patients?
1) Nonunion
2) Complex Regional Pain Syndrome, type II
3) Malunion
4) Complex Regional Pain Syndrome, type I
5) Wound infection
Vitamin C has been shown to decrease the likelihood of developing complex regional pain syndrome (CRPS), type 1, when given post-operatively to patients undergoing foot and ankle and wrist surgery.
CRPS is a frequent post-operative complication, with rates varying from 10-
37%. Type I CRPS does not have an identifiable nerve lesion, while type II has an identifiable nerve lesion. Multiple studies have shown that vitamin C decreases rates of CRPS following distal radius fractures, and more recently, the same has been shown following foot and ankle surgery. While the exact mechanism of CRPS is unknown, vitamin C has been shown to reduce lipid peroxidation, scavenge hydroxyl radicals, protect the capillary endothelium, and inhibit vascular permeability. All of these characteristics of vitamin C may play a role in modulating the pain pathway.
Zollinger et al. perform a double-blind, prospective, multicenter trial where
416 patients with 427 wrist fractures were randomly allocated to treatment with placebo or treatment with 200, 500, or 1500 mg of vitamin C daily for fifty days. The prevalence of complex regional pain syndrome was 2.4% in the vitamin C group and 10.1% in the placebo group.
Besse et al. compare two groups of patients undergoing surgery on the foot and ankle to determine the effect of vitamin C on the development of CRPS, type I. CRPS type I occurred in 18 cases (9.6%) in the group not given vitamin C, and 4 cases (1.7%) in the group given vitamin C.
Illustration A shows an example of a limb affected by CRPS. Note the increased swelling, a common physical exam finding in patients afflicted with the disease.
Incorrect Answers:
Answers 1, 2, 3, 5: Vitamin C has not been shown to decrease the incidence of these conditions.
A 25-year-old Spanish speaking male presents to the emergency department 6 hours after sustaining the injury seen in Figure A. He is grossly intoxicated and screaming in pain. Physical examination reveals a closed injury with overlying muscular compartments that are extremely firm to palpation. After sedating the patient, measurements of the intracompartmental pressures were all found to be**
**> 75mmHg. His wife is Spanish speaking and expected to arrive to the hospital in 2-3 hours with a relative to help with translation. No medical translator is**
**available. You attempt to outline the risk and benefits of surgery to the patient, but the he repeatedly interrupts you and yells out ,"No surgery!". An English-Spanish speaking friend is with the patient and says that he has known the patient for over 2 years and will help with any decision making. What would be the next most appropriate step in the management of this patient?
1) Delay surgery to monitor the patient for impending compartment syndrome
2) Proceed with surgery with urgent fasciotomy after documenting the necessity of treatment without consent
3) Delay the surgery until the wife arrives and able to give informed consent with the aid of a translator
4) Proceed with surgery for urgent fasciotomy after obtaining informed consent from the patients friend
5) Respect the patients autonomy and reassess the patient in the morning when he demonstrates capacity to accurately comprehend the proposed treatment
This patient is presenting with compartment syndrome of the right tibia. In a situation of required surgery for limb threatening injury without available legal consent the surgeon should confirm and document the necessity of care with a fellow colleague.
Physicians are responsible for whether a patient is able to reasonably understand their medical condition and the nature of any proposed medical procedure, including the risks, benefits, and available alternatives. If the patient lacks this capacity, disclosure imposed by the doctrine of informed
consent are excused because irreparable harm that may result from the physician’s hesitation to provide treatment. Detailed documentation is also important. In addition, the attending physician should contact the Risk Management Dept at the hospital for support prior to surgical intervention or have a medical translator involved to ensure information is being translated properly.
Katz et al. reviewed the medical decision making process of Hispanic people. They showed that Hispanic people are more likely to permit their physician to take the predominant role in making health decisions compared to Non- Hispanic people.
Figure A shows a comminuted tibia and fibula fracture. Incorrect Answers
Answer 1: This patient has confirmed compartmental syndrome. Surgical delay would be negligent.
Answer 3: Delay until his wife arrives would be necessary in non-life or-limb threatening conditions. In this case however, surgical delay could result in significant harm to the patient and therefore, the doctrine of informed consent can be excused.
Answer 4: Consent can only be given by a friend that has pre-existing notice of the patients views in the setting of emergencies and only when the dedicated decision maker is not available. The patients friend does not have enduring power of attorney and has not been appointed as a formal substitute decision-maker.
Answer 5: The patient does not demonstrate capacity to make an informed decision about his health. Therefore the views of his autonomy cannot be formulated.
A Spanish speaking child sustained the injury seen in Figure A after a fall at school. He was casted in the emergency department without the assistance of an interpreter and advised to return to see an orthopaedic surgeon in 1 week. However, the family returns to the emergency department with the child 3 months later, still in the cast. What is the most likely reason the child did not attend the recommended orthopaedic follow-up visit.?
1) The child is a victim of neglect
2) The child had no symptoms of pain
3) He was allowed to return to school wearing the cast
4) Concerns of cost
5) Follow-up instructions were not effectively communicated
The most likely reason the child did not attend the recommended orthopaedic follow-up visit was a language barrier preventing effective communication of the intended follow-up instructions.
Communication skills and cultural competence is a key element in good orthopaedic care. Poor communication can often lead to devastating outcomes. In this example, poor communication resulted in this patient being lost to
follow-up. Language barriers must be accommodated and alternative methods of communication must be utilized.
Levinson et al. examined how patients present their medical issues in clinical encounters and how physicians respond to these clues in routine primary care and surgical settings. They showed that good communication relies mostly on the physicians ability to identify patient clues within the clinical encounter.
Poor communication between the physician tended to delay clinical visits, poor follow-up and unsatisfactory outcomes.
Figure A is an AP radiograph of the elbow in a skeletally immature patient. Figure B is a lateral radiograph of the elbow with a posterior fat pad sign, suggestive of an occult fracture.
Incorrect Answers:
Answer 1,2,3,4: The most likely reason for loss to follow-up in this scenario is miscommunication regarding follow-up.
A 25-year-old female presents to the emergency room within increasing left shoulder pain after walking into a door 5 months ago. She previously sustained a femoral fracture 2 years ago after tripping on a rug. Relevant skeletal survey radiographs and tissue biopsy results are shown in Figures A through D. Laboratory investigations show normal glomerular filtration rate and creatinine clearance. Dual energy x-ray absorptiometry (DEXA) scan shows T-score of -1.4 and**
**-1.2 at the hip and lumbar spine, respectively. Which of the following laboratory values in Figure E most likely reflects this patient's condition?
1) A
2) B
3) C
4) D
5) E
This patient has primary hyperparathyroidism. Laboratory investigations are likely to show elevated serum intact parathyroid hormone (PTH), alkaline phosphatase (ALP) and ionized serum calcium, and low serum phosphate.
Primary hyperparathyroidism is most commonly caused by a single adenoma (80-90%). Besides the signs and symptoms of hypercalcemia, patients present
with calcification of menisci and articular cartilage, erosions in hand bones, "salt and pepper skull", and brown tumors (osteoclastomas), which appear as lytic regions expanding the cortex and causing pathological fractures, so named because of hemosiderin deposition.
Singhal et al. reviewed primary hyperparathyroidism. They advocate routine serum calcium levels for patients with pathologic fractures. If this is elevated, total and ionized calcium and intact PTH levels should be obtained. They feel that surgery for orthopaedic stabilization and parathyroidectomy should be performed simultaneously for better outcome.
Mankin et al. reviewed metabolic bone disease. They suggest that patients with mild disease with normal calcium levels do not require treatment. For patients with high calcium levels, treatment should include maintenance of fluid balance, localization and removal of the adenoma, bony stabilization, and medications (calcitonin, estrogen, bisphosphonates, and calcimimetics such as cinacalcet).
Figure A is an AP radiograph showing a lytic expansile lesion with pathological fracture in metadiaphyseal region of left humerus with similar lesion in the
fifth posterior rib. Figure B is an AP radiograph showing a lytic expansile lesion in the third metacarpal of the right hand and the fifth metacarpal of the left hand. Figure C is a low power micrograph of a brown tumor demonstrating a central zone of bone resorption, and filling with fibroblastic tissue, with a peripheral rim of osteoid production. Figure D is a high power micrograph of a brown tumor. In areas of bone resorption, there are numerous osteoclast-like giant cells amidst a fibrous stroma. This is unlike a true giant cell tumor, which lacks a fibrogenic stroma.
Incorrect Answers:
Answer 2: Elevated PTH and ALP, and low serum calcium and high serum phosphate are characteristic of secondary hyperparathyroidism. This occurs in chronic renal disease, where there is overproduction of PTH because of hyperphosphatemia, hypocalcemia,
and impaired 1,25-dihydroxyvitamin D production by the diseased kidneys. This patient has normal renal function. Answer 3: Elevated PTH, ALP, serum calcium and phosphate occur in tertiary hyperparathyroidism. This again occurs in chronic renal disease after prolonged chronic secondary hyperparathyroidism or after renal transplantation, where the parathyroid glands become autonomous and PTH levels do not normalize. This patient has normal renal function.
Answer 4: Normal PTH, low ALP and high serum calcium and phosphate occur in hypophosphatasia. The defect lies in tissue-nonspecific isoenzyme of alkaline phosphatase (TNSALP) and urine phosphoethanolamine levels are
elevated.
Answer 5: Low PTH, normal ALP, low serum calcium and high serum phosphate levels suggest hypoparathyroidism.
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
Question 3High Yield
The patient returns 4 years later; now he is a 17-year-old boy who has anterior knee pain with jumping and kneeling (Figure 28). The pain is located at the tibial tubercle. There is soft-tissue swelling and tenderness to palpation over the tubercle. He is able to do a straight-leg raise and there is no effusion, but the pain prevents him from playing basketball. Initial treatment should include

Explanation
- nonsurgical treatment with ice, nonsteroidal anti-inflammatory drugs (NSAIDs,) physical therapy for stretching, and an unloading brace._
Question 4High Yield
The risk of nerve injury following revision total hip arthroplasty (THA) is approximately:
Explanation
Following primary THA, the incidence of nerve palsy is reported to be approximately 1.3%, but may be as high as 5.2% for primary THA performed for developmental dysplasia or dislocation. For revision surgery, the incidence may be as high as
7.60%
7.60%
Question 5High Yield
The fracture seen in Figures A and B is most likely to occur in which of the following growth plate zones?



Explanation
**
Physeal fractures typically occur through the zone of provisional calcification. Answers 3-5 are all part of the hypertrophic zone which is labeled "D" on the histologic illustration A. Illustration B shows the relationship of the physeal zones to the epiphysis and metaphysis of a growing bone. However, the stress concentration is greatest in the sub-layer where there is a transition from the soft cartilagenous physis to the harder calcific metaphysis.
As discussed in the review by Ballock and O'Keefe, the growth plate is a remarkable portion of the skeleton that requires precise coordination between multiple endocrine, paracrine, and autocrine signaling systems. While fractures can occur in any portion of the growth plate, the zone of provisional calcification is the most common.
Physeal fractures typically occur through the zone of provisional calcification. Answers 3-5 are all part of the hypertrophic zone which is labeled "D" on the histologic illustration A. Illustration B shows the relationship of the physeal zones to the epiphysis and metaphysis of a growing bone. However, the stress concentration is greatest in the sub-layer where there is a transition from the soft cartilagenous physis to the harder calcific metaphysis.
As discussed in the review by Ballock and O'Keefe, the growth plate is a remarkable portion of the skeleton that requires precise coordination between multiple endocrine, paracrine, and autocrine signaling systems. While fractures can occur in any portion of the growth plate, the zone of provisional calcification is the most common.
Question 6High Yield
When comparing the failure load of an evenly tensioned four-stranded hamstring tendon anterior cruciate ligament autograft to a 10-mm bone-patellar tendon-bone autograft, the hamstring graft will fail at a tension
Explanation
The failure load of an evenly tensioned four-stranded hamstring tendon autograft has been reported to be 4,500 Newtons. The failure load of a 10-mm patellar tendon autograft has been estimated at 2,600 Newtons. The intact anterior cruciate ligament failure load has been calculated at 1,725 Newtons.
REFERENCES: Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA: Arthroscopic reconstruction of the anterior cruciate ligament: A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 1999;27:448-454.
Hamner DL, Brown CH Jr, Steiner ME, et al: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Noyes FR, Butler DL, Grood ES, et al: Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J Bone Joint Surg Am 1984;66:344-352.
REFERENCES: Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA: Arthroscopic reconstruction of the anterior cruciate ligament: A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 1999;27:448-454.
Hamner DL, Brown CH Jr, Steiner ME, et al: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Noyes FR, Butler DL, Grood ES, et al: Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J Bone Joint Surg Am 1984;66:344-352.
Question 7High Yield
Figure 1 is the clinical photograph of a 65-year-old right-hand dominant man who has finger contracture and stiffness. He experiences minimal pain but has severe functional limitations and elects for treatment with injectable collagenase _Clostridium histolyticum_. What types of collagen will be affected by this injection?
---
---

Explanation
Type II collagen is the predominant type found in articular cartilage. Type IV collagen is the predominant type found in the basement membranes of neurovascular structures. Collagenase _Clostridium_ __histolyticum__ _injection targets type I and type III collagen._
Question 8High Yield
A functional nerve transfer involves
Explanation
Nerve transfer can provide some function to a functionless nerve. Typically, nerve transfer includes intrafascicular dissection; cutting of a functioning nerve fascicle; and suturing the
released, functioning nerve fascicle to a nonfunctioning nerve branch. A common application of nerve transfer in the upper extremity involves attachment of a functioning motor fascicle of the ulnar nerve to the nonfunctioning musculocutaneous branch to the biceps muscle to restore active elbow flexion in patients with nerve root avulsion brachial plexus injuries. Motor nerves can be transferred to other motor nerves, and sensory nerves can be transferred to other sensory nerves. Treatment of acute nerve gaps with nerve grafting, conduits, or nerve growth factors does not describe nerve transfer. Although implanting neuromas into neighboring muscle tissue can decrease symptoms related to the neuroma, this does not describe a nerve transfer, and a neuroma cannot reinnervate a muscle.
RECOMMENDED READINGS
10. Tung TH, Mackinnon SE. Nerve transfers: indications, techniques, and outcomes. J Hand Surg Am. 2010 Feb;35(2):332-41. doi: 10.1016/j.jhsa.2009.12.002. Review. PubMed PMID: 20141906.
11. Dodds SD. Peripheral Nervous System. In Boyer MI, ed. AAOS Comprehensive Orthopaedic Review. Vol 1. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:113-126.
released, functioning nerve fascicle to a nonfunctioning nerve branch. A common application of nerve transfer in the upper extremity involves attachment of a functioning motor fascicle of the ulnar nerve to the nonfunctioning musculocutaneous branch to the biceps muscle to restore active elbow flexion in patients with nerve root avulsion brachial plexus injuries. Motor nerves can be transferred to other motor nerves, and sensory nerves can be transferred to other sensory nerves. Treatment of acute nerve gaps with nerve grafting, conduits, or nerve growth factors does not describe nerve transfer. Although implanting neuromas into neighboring muscle tissue can decrease symptoms related to the neuroma, this does not describe a nerve transfer, and a neuroma cannot reinnervate a muscle.
RECOMMENDED READINGS
10. Tung TH, Mackinnon SE. Nerve transfers: indications, techniques, and outcomes. J Hand Surg Am. 2010 Feb;35(2):332-41. doi: 10.1016/j.jhsa.2009.12.002. Review. PubMed PMID: 20141906.
11. Dodds SD. Peripheral Nervous System. In Boyer MI, ed. AAOS Comprehensive Orthopaedic Review. Vol 1. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:113-126.
Question 9High Yield
Figures 75a and 75b are the radiographs after attempted reduction of an injury in a 9-year-old girl. Which anatomic structure is most likely to be interposed?


Explanation
The injury shown is a flexion-type supracondylar humerus fracture. The most commonly interposed anatomic structure is the ulnar nerve. The brachialis muscle is often interposed in extension-type fractures, as are the median nerve and radial artery. The radial nerve is at risk for entrapment in a humeral shaft fracture or distal third humeral fracture.
Figure 76
CLINICAL SITUATION FOR QUESTIONS 76 THROUGH 80
Figure 76 is the clinical photograph of an infant with foot deformities.
Figure 76
CLINICAL SITUATION FOR QUESTIONS 76 THROUGH 80
Figure 76 is the clinical photograph of an infant with foot deformities.
Question 10High Yield
A 59-year-old man reports moderate shoulder pain and very restricted range of motion after undergoing humeral arthroplasty for osteoarthritis 1 year ago. An AP radiograph is shown in Figure 32. Management should now consist of
Explanation
The radiograph reveals that an insufficient amount of the proximal humerus was excised in the index procedure, resulting in malalignment of the humeral component, overstuffing of the glenohumeral joint, and glenoid arthritis. It is unlikely that physical therapy or soft-tissue releases alone will be adequate. Revision of the humeral component, recutting of the proximal humerus to allow a more anatomic alignment of the humeral component, appropriate soft-tissue releases, and glenoid arthroplasty will offer the best chance of improvement in this difficult situation.
REFERENCES: Neer CS II, Kirby RM: Revision of humeral head and total shoulder arthroplasties. Clin Orthop 1982;170:189-195.
Petersen SA, Hawkins RJ: Revision of failed total shoulder arthroplasty. Orthop Clin North Am 1998;29:519-533.
REFERENCES: Neer CS II, Kirby RM: Revision of humeral head and total shoulder arthroplasties. Clin Orthop 1982;170:189-195.
Petersen SA, Hawkins RJ: Revision of failed total shoulder arthroplasty. Orthop Clin North Am 1998;29:519-533.
Question 11High Yield
After placing a type I mallet finger in a splint at the initial visit, next follow-up should be:
Explanation
After placement of the splint, the patient should follow-up in the next week to make sure the finger is still maintained in full extension. Loosening of the splint will occur as swelling decreases.
Question 12High Yield
What is the major difference in outcome following open reduction and internal fixation (ORIF) of the tibial plafond at 2 to 5 days versus 10 to 20 days?
Explanation
Long-term outcomes following tibial plafond fractures treated with ORIF are satisfactory in most patients despite a high incidence of posttraumatic osteoarthritis. If ORIF is delayed until 10 to 20 days following injury, the major difference in outcomes is fewer complications associated with wound healing. Ankle strength, pain, range of motion, and the development of arthritis are equal regardless of the time until fixation.
REFERENCES: Sirkin M, Sanders R, DePasquale T, et al: A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 1999;13:78-84.
Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
REFERENCES: Sirkin M, Sanders R, DePasquale T, et al: A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 1999;13:78-84.
Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 13High Yield
1240) Which of the following factors is associated with the highest rate of nonunion of a midshaft clavicle fracture?

Explanation
The risk of nonunion in patients sustaining middle 1/3 clavicle fractures is increased in female patients.
Clavicle fractures are often secondary to direct blows to the lateral aspect of the shoulder. Physical examination is important to ascertain the status of the
skin and neurovascular structures to help guide treatment management. Although most non-displaced middle 1/3 clavicle fractures may be treated successfully with conservative measures, the risk for non-union (1-5%) increases with increasing comminution, female gender, shortening greater than 2 cm and an advanced age of the patient.
Robinson et al. reviewed 581 patients treated non-operatively for midshaft clavicle fractures. A nonunion rate of 4.5 % was identified at 24 weeks after the injury. They identified four factors that contributed to non-union, including: female gender, lack of cortical apposition, comminution of the fracture fragments and advancing age.
Zlowdzki et al. reviewed 2144 clavicle fracture cases in a comprehensive meta-analysis. They report displacement as the highest risk factor for nonunion (15.1%) in nonoperatively treated clavicle fractures, and simple slings were favored over figure of 8 braces. They also report an 86% reduction in the nonunion rate when operative fixation is chosen over nonoperative treatment for displaced clavicle fractures.
Illustration A shows the presence of a non-union of a midshaft clavicle fracture. A video is provided that reviews management of clavicle injuries.
Incorrect Answers
Answers 1, 3: Older patients and comminution of the fracture were found to be risk factors for non-union in midshaft clavicle injuries
Answers 4, 5: Neither of these are associated with an increased risk of nonunion in midshaft clavicular fractures.
Clavicle fractures are often secondary to direct blows to the lateral aspect of the shoulder. Physical examination is important to ascertain the status of the
skin and neurovascular structures to help guide treatment management. Although most non-displaced middle 1/3 clavicle fractures may be treated successfully with conservative measures, the risk for non-union (1-5%) increases with increasing comminution, female gender, shortening greater than 2 cm and an advanced age of the patient.
Robinson et al. reviewed 581 patients treated non-operatively for midshaft clavicle fractures. A nonunion rate of 4.5 % was identified at 24 weeks after the injury. They identified four factors that contributed to non-union, including: female gender, lack of cortical apposition, comminution of the fracture fragments and advancing age.
Zlowdzki et al. reviewed 2144 clavicle fracture cases in a comprehensive meta-analysis. They report displacement as the highest risk factor for nonunion (15.1%) in nonoperatively treated clavicle fractures, and simple slings were favored over figure of 8 braces. They also report an 86% reduction in the nonunion rate when operative fixation is chosen over nonoperative treatment for displaced clavicle fractures.
Illustration A shows the presence of a non-union of a midshaft clavicle fracture. A video is provided that reviews management of clavicle injuries.
Incorrect Answers
Answers 1, 3: Older patients and comminution of the fracture were found to be risk factors for non-union in midshaft clavicle injuries
Answers 4, 5: Neither of these are associated with an increased risk of nonunion in midshaft clavicular fractures.
Question 14High Yield
A 55-year-old man with a 4-part proximal humerus fracture with intra-articular comminution and a large greater tuberosity fragment
Explanation
- Hemiarthroplasty_
Question 15High Yield
Videos 1 and 2 are the coronal plane MRI scan and arthroscopic evaluation of a 48-year-old woman with 2 weeks of posterior knee pain after feeling a “pop” in the knee while climbing stairs. Physical examination reveals passive range of motion of +5° to 120°, with pain limiting her in terminal extension. Failure of surgical repair of the injured structure is most associated with
Explanation
The MRI scan and surgical video are showing an example of a posterior medial meniscal root tear/avulsion. Many studies have shown successful treatment of these tears with repair using various techniques and minimal progression to osteoarthritis (OA). Most studies exclude patients with high BMI. Brophy and associates demonstrated in their series that high BMI was associated with higher rates of clinical OA and need for subsequent surgery.
Multiple studies in the literature demonstrate good results with a variety of techniques. A valgus alignment in this setting would be considered protective, as opposed to a varus alignment >5°, which has also been associated with worse outcomes. The vascularity of the meniscus is consistently poor throughout most of its volume, including the root, and is not considered to be significantly different from person to person and should affect all root repairs equally.
Multiple studies in the literature demonstrate good results with a variety of techniques. A valgus alignment in this setting would be considered protective, as opposed to a varus alignment >5°, which has also been associated with worse outcomes. The vascularity of the meniscus is consistently poor throughout most of its volume, including the root, and is not considered to be significantly different from person to person and should affect all root repairs equally.
Question 16High Yield
Haversian bone is composed of vascular channels surrounded circumferentially by lamellar bone. Which of the following terms is used to describe the unit of bone composed of a neurovascular channel surrounded by a cell-permeated layer of bone matrix:
Explanation
The osteon is a unique arrangement of bone cells and matrix surrounding a blood vessel. The osteon is an irregular branching, anastomosing cylinder composed of a centrally placed neurovascular canal surrounded by cell-permeated layers of bone matrix.
The bone remodeling unit refers to the cutting cone of leading osteoclasts and following osteoblasts.
Plexiform bone is a structural type of bone found in large animals where rapid bone growth occurs. There are alternating layers of lamellar and woven bone.
Volkman canals are the channels connecting different osteons or Haversian units.
Canaliculi are small channels through which the cell processes of the osteocytes connect to each other. Correct Answer: Osteon
The bone remodeling unit refers to the cutting cone of leading osteoclasts and following osteoblasts.
Plexiform bone is a structural type of bone found in large animals where rapid bone growth occurs. There are alternating layers of lamellar and woven bone.
Volkman canals are the channels connecting different osteons or Haversian units.
Canaliculi are small channels through which the cell processes of the osteocytes connect to each other. Correct Answer: Osteon
Question 17High Yield
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. This patient elects nonsurgical treatment and later experiences persistent instability. Examination reveals an asymmetric Dial test finding and a varus thrust during ambulation. Which osteotomy and correction appropriately addresses this chronic instability pattern?
---
---

Explanation
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, one major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading. The scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used.
Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Question 18High Yield
Which of the following has been associated with an increased likelihood of stress shielding after cementless total hip arthroplasty?
Explanation
DISCUSSION: Although stress shielding has not been associated with adverse clinical outcomes to date, it is a commonly observed process after cementless total hip arthroplasty. Factors that increase the magnitude of stress shielding include the use of distally fixed cobalt-chrome stems, particularly in patients with osteoporosis. Large diameter femoral components (larger than 18 mm in diameter) have also been associated with an increased prevalence of stress shielding.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 345-368.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 345-368.
Question 19High Yield
In addition to her planned primary procedure, how can the surgeon best improve this patient's lumbar lordosis?
Explanation
- Use of an interbody strut at L5-S1
Question 20High Yield
A 4-year-old girl sustains an isolated spiral femoral fracture after falling from her tricycle. Management should consist of
Explanation
Immediate spica casting is ideal for younger children with uncomplicated femoral fractures that are the result of relatively low-energy injury. Surgical stabilization of pediatric femoral fractures is most commonly performed in children who are older than age 6 years or in children with other factors associated with their femoral fracture, such as concomitant head injury, open fracture, floating knee, severe comminution, or vascular injury.
REFERENCES: Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659.
Sponseller PD: Surgical management of pediatric femoral fractures. Instr Course Lect 2002;51:361-365.
Wright JG: The treatment of femoral shaft fractures in children: A systematic overview and critical appraisal of the literature. Can J Surg 2000;43:180-189.
Levy J, Ward WT: Pediatric femur fractures: An overview of treatment. Orthopedics 1993;16:183-190.
REFERENCES: Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659.
Sponseller PD: Surgical management of pediatric femoral fractures. Instr Course Lect 2002;51:361-365.
Wright JG: The treatment of femoral shaft fractures in children: A systematic overview and critical appraisal of the literature. Can J Surg 2000;43:180-189.
Levy J, Ward WT: Pediatric femur fractures: An overview of treatment. Orthopedics 1993;16:183-190.
Question 21High Yield
Anterior approach


Explanation
The nerve most commonly injured in the posterior approach to the hip is the sciatic nerve. Overall injury prevalence is 1% to 2%. This nerve is more commonly injured in cases of hip dysplasia with excessive leg lengthening. The superior gluteal nerve is at highest risk with the direct lateral approach to the hip. This nerve courses in the gluteus medius muscle and is
at risk when splitting the muscle 5 cm proximal to the greater trochanter. The lateral femoral 73
cutaneous nerve is commonly damaged with anterior total hip replacement surgery. Neuropraxia has been reported in 81% of patients. The inferior gluteal nerve travels from the greater sciatic notch and enters the gluteus maximus muscle. It is at risk when the posterior approach to the hip is used.
RECOMMENDED READINGS
1. Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia.
PA: Lippincott Williams & Wilkins; 2003:365-453.
2. [DeHart MM, Riley LH Jr. Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg. 1999 Mar-Apr;7(2):101-11. Review. PubMed PMID: 10217818. ](http://www.ncbi.nlm.nih.gov/pubmed/10217818)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/10217818)[ at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10217818)
3. Goulding K, Beaulé PE, Kim PR, Fazekas A. Incidence of lateral femoral cutaneous nerve neuropraxia after anterior approach hip arthroplasty. Clin Orthop Relat Res. 2010 Sep;468(9):2397-404. doi: 10.1007/s11999-010-1406-5. PubMed PMID:
[20532717.](http://www.ncbi.nlm.nih.gov/pubmed/20532717)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20532717)
Figures 87a and 87b are sagittal and coronal MR images of the affected elbow of a 36-year-old man who has a history of painful mechanical symptoms in his dominant arm when extending his elbow in full supination. What is the most likely cause of his painful snapping?
A
B
1. Lacertus fibrosis contracture
2. Intra-articular loose bodies 74
3. Olecranon fossa impingement
4. Radiocapitellar plica
PREFERRED RESPONSE: 4- Radiocapitellar plica
DISCUSSION
The MRI studies show a radiocapitellar plica. This anomalous structure has been associated with symptomatic snapping. Lacertus fibrosis contracture will not cause painful snapping. An intra-articular pathology such as loose bodies is not present on these imaging studies. Olecranon fossa impingement causes posterior pain in extension and is not shown in the images.
RECOMMENDED READINGS
1. [Antuna SA, O'Driscoll SW. Snapping plicae associated with radiocapitellar chondromalacia. Arthroscopy. 2001 May;17(5):491-5. PubMed 11337715. ](http://www.ncbi.nlm.nih.gov/pubmed/11337715)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/11337715)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11337715)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11337715)
2. [Ruch DS, Papadonikolakis A, Campolattaro RM. The posterolateral plica: a cause of refractory lateral elbow pain. J Shoulder Elbow Surg. 2006 May-Jun;15(3):367-70. PubMed PMID: 16679240. ](http://www.ncbi.nlm.nih.gov/pubmed/16679240)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16679240)
at risk when splitting the muscle 5 cm proximal to the greater trochanter. The lateral femoral 73
cutaneous nerve is commonly damaged with anterior total hip replacement surgery. Neuropraxia has been reported in 81% of patients. The inferior gluteal nerve travels from the greater sciatic notch and enters the gluteus maximus muscle. It is at risk when the posterior approach to the hip is used.
RECOMMENDED READINGS
1. Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia.
PA: Lippincott Williams & Wilkins; 2003:365-453.
2. [DeHart MM, Riley LH Jr. Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg. 1999 Mar-Apr;7(2):101-11. Review. PubMed PMID: 10217818. ](http://www.ncbi.nlm.nih.gov/pubmed/10217818)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/10217818)[ at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10217818)
3. Goulding K, Beaulé PE, Kim PR, Fazekas A. Incidence of lateral femoral cutaneous nerve neuropraxia after anterior approach hip arthroplasty. Clin Orthop Relat Res. 2010 Sep;468(9):2397-404. doi: 10.1007/s11999-010-1406-5. PubMed PMID:
[20532717.](http://www.ncbi.nlm.nih.gov/pubmed/20532717)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20532717)
Figures 87a and 87b are sagittal and coronal MR images of the affected elbow of a 36-year-old man who has a history of painful mechanical symptoms in his dominant arm when extending his elbow in full supination. What is the most likely cause of his painful snapping?
A
B
1. Lacertus fibrosis contracture
2. Intra-articular loose bodies 74
3. Olecranon fossa impingement
4. Radiocapitellar plica
PREFERRED RESPONSE: 4- Radiocapitellar plica
DISCUSSION
The MRI studies show a radiocapitellar plica. This anomalous structure has been associated with symptomatic snapping. Lacertus fibrosis contracture will not cause painful snapping. An intra-articular pathology such as loose bodies is not present on these imaging studies. Olecranon fossa impingement causes posterior pain in extension and is not shown in the images.
RECOMMENDED READINGS
1. [Antuna SA, O'Driscoll SW. Snapping plicae associated with radiocapitellar chondromalacia. Arthroscopy. 2001 May;17(5):491-5. PubMed 11337715. ](http://www.ncbi.nlm.nih.gov/pubmed/11337715)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/11337715)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11337715)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11337715)
2. [Ruch DS, Papadonikolakis A, Campolattaro RM. The posterolateral plica: a cause of refractory lateral elbow pain. J Shoulder Elbow Surg. 2006 May-Jun;15(3):367-70. PubMed PMID: 16679240. ](http://www.ncbi.nlm.nih.gov/pubmed/16679240)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16679240)
Question 22High Yield
Figure 1 shows the radiograph obtained from a 54-year-old woman with rheumatoid arthritis who has thumb pain and dysfunction. Nonsurgical treatment, including splinting, oral NSAIDs, activity modification, and steroid injections, has failed. What is the most appropriate surgical intervention?
---
---

Explanation
Various options exist to treat thumb CMC arthritis: trapezial resection alone, trapezial resection with ligament suspensionplasty or tendon interposition, trapezial resection with both ligament suspensionplasty and tendon interposition, CMC fusion, and CMC replacement. MCP hyperextension can develop in long-standing CMC arthritis, contributing to CMC instability as well as thumb pain and weakness. In patients with concomitant MCP hyperextension that exceeds 30°,
correction of the deformity of the MCP joint must also be addressed and can be done with MCP capsulodesis, extensor pollicis brevis tendon transfer, or MCP fusion. Fusion of both the thumb CMC and MP joints is not recommended as this would result in marked stiffness and dysfunction.
correction of the deformity of the MCP joint must also be addressed and can be done with MCP capsulodesis, extensor pollicis brevis tendon transfer, or MCP fusion. Fusion of both the thumb CMC and MP joints is not recommended as this would result in marked stiffness and dysfunction.
Question 23High Yield
A 20-year-old man sustained an injury to his arm during a tug-of-war contest. An MRI scan is shown in Figure 18. What is the most likely diagnosis?
Explanation
The MRI scan reveals a transection of the biceps muscle. The underlying brachialis is intact. This injury can occur as a result of a cord wrapped around the upper arm. Care should be taken to ensure that there is no concurrent vascular injury. A posterior subcutaneous lipoma appears as a well-encapsulated mass on T2-weighted images.
REFERENCES: Heckman JD, Levine MI: Traumatic closed transection of the biceps brachii in the military parachutist. J Bone Joint Surg Am 1978;60:369-372.
Mellen PF: Parachute static line injury with vascular compromise. Mil Med 1989;154:364-365.
REFERENCES: Heckman JD, Levine MI: Traumatic closed transection of the biceps brachii in the military parachutist. J Bone Joint Surg Am 1978;60:369-372.
Mellen PF: Parachute static line injury with vascular compromise. Mil Med 1989;154:364-365.
Question 24High Yield
Figures 45a and 45b are the radiographs of a previously asymptomatic 10-year-old girl who fell off of her bike. Treatment of this lesion should consist of


Explanation
Nonossifying fibroma of bone is a common entity and consists of a solitary eccentric, lytic expanded lesion in the metaphysis of a long bone. Clinically, nonossifying fibromas are asymptomatic and are usually an incidental finding on radiograph. These lesions normally regress spontaneously.
RECOMMENDED READINGS
27. [Mankin HJ, Trahan CA, Fondren G, Mankin CJ. Non-ossifying fibroma, fibrous cortical defect and Jaffe-Campanacci syndrome: a biologic and clinical review. Chir Organi Mov. 2009 May;93(1):1-7. doi: 10.1007/s12306-009-0016-4. Epub 2009 Apr 29. Review. PubMed PMID: 19711155. ](http://www.ncbi.nlm.nih.gov/pubmed/19711155)[View](http://www.ncbi.nlm.nih.gov/pubmed/19711155)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19711155)
28. [Smith SE, Kransdorf MJ. Primary musculoskeletal tumors of fibrous origin. Semin Musculoskelet Radiol. 2000;4(1):73-88. Review. PubMed PMID: 11061693. ](http://www.ncbi.nlm.nih.gov/pubmed/11061693)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11061693)
RECOMMENDED READINGS
27. [Mankin HJ, Trahan CA, Fondren G, Mankin CJ. Non-ossifying fibroma, fibrous cortical defect and Jaffe-Campanacci syndrome: a biologic and clinical review. Chir Organi Mov. 2009 May;93(1):1-7. doi: 10.1007/s12306-009-0016-4. Epub 2009 Apr 29. Review. PubMed PMID: 19711155. ](http://www.ncbi.nlm.nih.gov/pubmed/19711155)[View](http://www.ncbi.nlm.nih.gov/pubmed/19711155)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19711155)
28. [Smith SE, Kransdorf MJ. Primary musculoskeletal tumors of fibrous origin. Semin Musculoskelet Radiol. 2000;4(1):73-88. Review. PubMed PMID: 11061693. ](http://www.ncbi.nlm.nih.gov/pubmed/11061693)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11061693)
Question 25High Yield
Figure 78 is the radiograph of a 20-year-old male college basketball player who sustained the injury shown. Which treatment most likely will allow quickest return to play?

Explanation
Proximal diaphyseal/metadiaphyseal fifth metatarsal fractures have long been recognized as injuries that can be slow to heal, posing substantial risk for nonunion. Although there are treatment options, most authors believe that aggressive surgical treatment is most appropriate for patients who are active, especially athletes, because healing time can be shortened with surgery.
RECOMMENDED READINGS
24. [Portland G, Kelikian A, Kodros S. Acute surgical management of Jones' fractures. Foot Ankle Int. 2003 Nov;24(11):829-33. PubMed PMID: 14655886.](http://www.ncbi.nlm.nih.gov/pubmed/14655886)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14655886)
25. [Fernández Fairen M, Guillen J, Busto JM, Roura J. Fractures of the fifth metatarsal in basketball players. Knee Surg Sports Traumatol Arthrosc. 1999;7(6):373-7. ](http://www.ncbi.nlm.nih.gov/pubmed/10639656)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10639656)
RECOMMENDED READINGS
24. [Portland G, Kelikian A, Kodros S. Acute surgical management of Jones' fractures. Foot Ankle Int. 2003 Nov;24(11):829-33. PubMed PMID: 14655886.](http://www.ncbi.nlm.nih.gov/pubmed/14655886)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14655886)
25. [Fernández Fairen M, Guillen J, Busto JM, Roura J. Fractures of the fifth metatarsal in basketball players. Knee Surg Sports Traumatol Arthrosc. 1999;7(6):373-7. ](http://www.ncbi.nlm.nih.gov/pubmed/10639656)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10639656)
Question 26High Yield
A 45-year-old man has a draining sinus and recurrent infection of his right total knee arthroplasty. He has
had two prior revision surgeries after the primary procedure and three other surgeries before his initial replacement, including a proximal tibial osteotomy and subsequent hardware removal. On clinical examination, he has a draining sinus in the mid portion of his surgical scar and a range of motion of 5° to
85°. AP and lateral radiographs of the right knee are shown in Figures below. During surgery, the femoral component is found to be grossly loose, but the tibial component is well fixed. What is the most appropriate extensile approach that would provide adequate exposure and aid in tibial component extraction?
had two prior revision surgeries after the primary procedure and three other surgeries before his initial replacement, including a proximal tibial osteotomy and subsequent hardware removal. On clinical examination, he has a draining sinus in the mid portion of his surgical scar and a range of motion of 5° to
85°. AP and lateral radiographs of the right knee are shown in Figures below. During surgery, the femoral component is found to be grossly loose, but the tibial component is well fixed. What is the most appropriate extensile approach that would provide adequate exposure and aid in tibial component extraction?

Explanation
Extended tibial tubercle osteotomy is an extensile approach to revision total knee arthroplasty that affords excellent exposure and can facilitate removal of tibial sleeves and cones. This patient has had multiple surgeries, including a proximal tibial osteotomy, as well as poor range of motion, patella baja, and a well- fixed metaphyseal sleeve component. Classically, an extended tibial tubercle osteotomy provides outstanding exposure for component removal in the setting of prior high tibial osteotomy and patella baja. For this patient, it is important to recognize the patella baja on the radiographs, as well as the tibial sleeve. In many of these cases the osteotomy provides access to the sleeve to help with extraction, because the stem will not pull through the sleeve or detach from the tray to allow visualization of the sleeve. The extended medial parapatellar approach is just a long medial approach that typically yields good exposure
but would not help with the patella baja or extraction of the tibial sleeve. The quadriceps snip would give good exposure to the knee but would not aid in tibial component removal. Lastly, the medial epicondyle osteotomy could help with exposure and tensioning of the medial complex of the knee but would not help
with tibial component extraction.
but would not help with the patella baja or extraction of the tibial sleeve. The quadriceps snip would give good exposure to the knee but would not aid in tibial component removal. Lastly, the medial epicondyle osteotomy could help with exposure and tensioning of the medial complex of the knee but would not help
with tibial component extraction.
Question 27High Yield
A
B
C
Figures 62a through 62c are the MR images and CT scan of a 65-year-old man with a history of diabetes mellitus, hypertension, and smoking. He has a 6-week history of increasing midback pain, lower extremity pain, and weakness. What is the most likely diagnosis, and how should this diagnosis be confirmed?
B
C
Figures 62a through 62c are the MR images and CT scan of a 65-year-old man with a history of diabetes mellitus, hypertension, and smoking. He has a 6-week history of increasing midback pain, lower extremity pain, and weakness. What is the most likely diagnosis, and how should this diagnosis be confirmed?
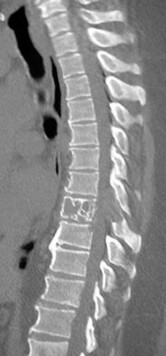

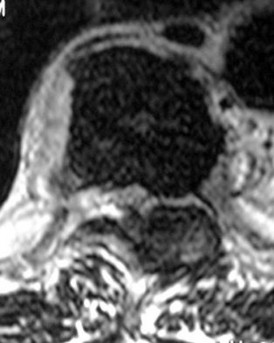
Explanation
The sagittal T2-weighted and axial T2-weighted images show a lesion within the T8 vertebral body that involves the posterior elements. There is an associated epidural component that results in compression of the spinal cord. The sagittal reconstructed CT image shows a lytic lesion within the T8 vertebral body. This pattern of vertebral body involvement with preservation
of the adjacent disks and endplates in a 65-year-old patient is most compatible with a diagnosis of a tumor. The most likely tumor is a metastatic lesion. A CT-guided biopsy will confirm this diagnosis. Although thoracic tuberculosis does not typically cross the disk space, the lack of an anterior soft-tissue component decreases the likelihood of this diagnosis.
RECOMMENDED READINGS
[Khanna AJ, Shindle MK, Wasserman BA, Gokaslan ZL, Gonzales RA, Buchowski JM, Riley LH 3rd. Use of magnetic resonance imaging in differentiating compartmental location of spinal tumors. Am J Orthop (Belle Mead NJ). 2005 Oct;34(10):472-6. Review. PubMed PMID: 16304794. ](http://www.ncbi.nlm.nih.gov/pubmed/16304794)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16304794)
[White AP, Kwon BK, Lindskog DM, Friedlaender GE, Grauer JN. Metastatic disease of the spine. J Am Acad Orthop Surg. 2006 Oct;14(11):587-98. Review. PubMed PMID: 17030592. ](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[View](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17030592)
of the adjacent disks and endplates in a 65-year-old patient is most compatible with a diagnosis of a tumor. The most likely tumor is a metastatic lesion. A CT-guided biopsy will confirm this diagnosis. Although thoracic tuberculosis does not typically cross the disk space, the lack of an anterior soft-tissue component decreases the likelihood of this diagnosis.
RECOMMENDED READINGS
[Khanna AJ, Shindle MK, Wasserman BA, Gokaslan ZL, Gonzales RA, Buchowski JM, Riley LH 3rd. Use of magnetic resonance imaging in differentiating compartmental location of spinal tumors. Am J Orthop (Belle Mead NJ). 2005 Oct;34(10):472-6. Review. PubMed PMID: 16304794. ](http://www.ncbi.nlm.nih.gov/pubmed/16304794)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16304794)
[White AP, Kwon BK, Lindskog DM, Friedlaender GE, Grauer JN. Metastatic disease of the spine. J Am Acad Orthop Surg. 2006 Oct;14(11):587-98. Review. PubMed PMID: 17030592. ](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[View](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17030592)
Question 28High Yield
A 40-year-old male laborer sustained a fall from height and has isolated pelvic pain. He is otherwise hemodynamically stable. A radiograph is shown in Figure A. A stress examination under anesthesia does not show any further anterior diastasis or posterior pelvic ring displacement. Computed tomography reveals no asymmetry of the sacroiliac joints. What is the most appropriate management of this injury?

Explanation
This patient sustained an open-book pelvic fracture with a pubic symphysis diastasis of less than 2.5cm. From the Young and Burgess classification, he has anteroposterior compression (AP) type 1 injury. Treatment of this is protected weight-bearing and symptomatic treatment. Stress examination can be utilized in order to ensure that the injury is, in fact, a APC-1 injury, and not a more severe posterior injury that would require operative intervention.
Question 29High Yield
When compared with individuals with diffuse idiopathic scoliosis (DISH), patients with ankylosing spondylitis have which of the following rates of neurologic injury, treatment complications, and mortality?
Explanation
All patients with hyperostotic conditions of the spine are at a high risk of neurologic injury following even minor trauma. However, several studies have shown that patients with ankylosing spondylitis have higher rates of neurologic injury and complications related to treatment compared with individuals with DISH. A recent meta-analysis was unable to show a significantly increased risk of mortality for patients with ankylosing spondylitis relative to those with DISH (3-month mortality estimated at 17% to 20%).
Question 30High Yield
The radiographs and CT scan seen in Figures 28a through 28d reveal what type of acetabular fracture pattern?
Explanation
The AP, obturator oblique, and iliac oblique views of the pelvis reveal a fracture that disrupts the iliopectineal and ilioischial lines, indicating a fracture that involves both anterior and posterior columns. However, it does not have the other features of anterior or posterior column fracture patterns. A displaced posterior wall fracture is also present, best seen on the obturator oblique view. The anterior to posterior directed fracture line on the CT scan indicates a transverse fracture; therefore, the patient has a transverse with posterior wall fracture pattern. A T-type fracture would be similar but would have a break into the obturator ring.
REFERENCES: Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
REFERENCES: Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 31High Yield
In rotator cuff tear arthropathy with pseudoparalysis, forward elevation of the humerus away from the body is prohibited because of
Explanation
DISCUSSION
The rotator cuff serves as a humeral head compressor that stabilizes the humeral head in the glenoid concavity so that the deltoid can convert a vertical force into abduction and forward elevation. The deltoid functions normally in patients with chronic rotator cuff arthropathy, so no atony is present. Glenoid concavity can be lost over time, but this is not the primary mechanism for failure of elevation. The biceps tendon does not serve as a humeral head compressor and does not prevent proximal migration of the shoulder when it is present.
DISCUSSION
The rotator cuff serves as a humeral head compressor that stabilizes the humeral head in the glenoid concavity so that the deltoid can convert a vertical force into abduction and forward elevation. The deltoid functions normally in patients with chronic rotator cuff arthropathy, so no atony is present. Glenoid concavity can be lost over time, but this is not the primary mechanism for failure of elevation. The biceps tendon does not serve as a humeral head compressor and does not prevent proximal migration of the shoulder when it is present.
Question 32High Yield
A 51-year-old male 2-pack per day smoker presents with a hyperkeratotic light brown plaque on the dorsum of his left ring finger that has been present for 7 years. It measures 14 mm by 13 mm. Initially, it responded to topical wart treatments, but has failed to do so recently so he sought evaluation by a dermatologist who biopsied the lesion. The results revealed squamous cell carcinoma (SCC) in situ, and he was referred for further surgical management. He has no other skin lesions, no history of SCC and no axillary lymphadenopathy. What is the next step in management?
Explanation
SCC in situ is a low-grade malignancy that typically presents as painless lesions on areas of high sun exposure such as the dorsum of the hand and fingers. The recommended treatment for lesions smaller than 100 mm is wide excision with 4 mm margins to a depth 1 layer below the tumor, along with any adjacent area of induration. Sentinel lymph node biopsy is typically not indicated in the setting of a low-grade tumor such as this one and in the absence of axillary lymphadenopathy.
Question 33High Yield
38A
B
Three months later this patient has continued swelling and giving-way episodes. Figures 38a and 38b are his stress radiographs. This study indicates laxity in which ligament?
B
Three months later this patient has continued swelling and giving-way episodes. Figures 38a and 38b are his stress radiographs. This study indicates laxity in which ligament?


Explanation
- Anterior talofibular
Question 34High Yield
A 50-year-old woman presents with pain in the second toe. She describes this as burning and notes swelling of the toe for the past month. Upon examination, there appears to be instability of the toe with a positive dorsal subluxation stress test. The anatomic structure which is responsible for this patientâs symptoms is:
Explanation
This patient describes swelling of the toe, which is not associated with an interdigital neuroma. The pain, swelling, and clinical findings suggest a rupture of the plantar plate with early instability and second metatarsophalangeal synovitis.
Question 35High Yield
A 56-year-old man underwent right total shoulder arthroplasty 2 months ago. Recently while reaching with his shoulder in a flexed and adducted position, he noted shoulder pain and afterwards he could not externally rotate his arm. An axillary radiograph is shown in Figure 30. What is the most likely cause of this problem?
Explanation
Anteversion of the humeral component may result in anterior instability of the component. Posterior instability after total shoulder arthroplasty is usually the result of some combination of the following factors: untreated anterior soft-tissue contractures, excessive posterior capsular laxity, and excessive retroversion of the humeral and/or glenoid components.
REFERENCES: Cofield RH, Edgerton BC: Total shoulder arthroplasty: Complications and revision surgery. Instr Course Lect 1990;39:449-462.
Wirth MA, Rockwood CA Jr: Complications of total shoulder replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
69. A 70-year-old man seen in the emergency department has had left shoulder pain and a fever of 101.5 degrees F (38.6 degrees C) for the past 3 days. He denies any history of trauma. Examination reveals tenderness anterosuperiorly and at the posterior glenohumeral joint line. He has very limited range of motion (passive and active). Laboratory studies show a WBC count of 12,000/mm3 and an erythrocyte sedimentation rate of 48 mm/h. Initial management should consist of
1- an oral cephalosporin antibiotic and discharge home.
2- IV oxacillin and gentamicin.
3- arthroscopic drainage of the glenohumeral joint.
4- open irrigation and drainage of the glenohumeral joint.
5- aspiration of the glenohumeral joint and subacromial space with Gram stain and culture of the fluid.
PREFERRED RESPONSE: 5
DISCUSSION: It appears that the patient has septic arthritis of the glenohumeral joint; therefore, initial management should consist of aspiration of the glenohumeral joint and subacromial space separately, followed by Gram stain and culture of the fluid. Based on the findings, broad-spectrum IV antibiotics should be started. If the diagnosis of septic arthritis is confirmed, then arthroscopic or open surgical drainage usually is indicated.
REFERENCES: Sawyer JR, Esterhai JL Jr: Shoulder infections, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997.
Leslie BM, Harris JM, Driscoll D: Septic arthritis of the shoulder in adults. J Bone Joint Surg Am 1989;71:1516-1522.
REFERENCES: Cofield RH, Edgerton BC: Total shoulder arthroplasty: Complications and revision surgery. Instr Course Lect 1990;39:449-462.
Wirth MA, Rockwood CA Jr: Complications of total shoulder replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
69. A 70-year-old man seen in the emergency department has had left shoulder pain and a fever of 101.5 degrees F (38.6 degrees C) for the past 3 days. He denies any history of trauma. Examination reveals tenderness anterosuperiorly and at the posterior glenohumeral joint line. He has very limited range of motion (passive and active). Laboratory studies show a WBC count of 12,000/mm3 and an erythrocyte sedimentation rate of 48 mm/h. Initial management should consist of
1- an oral cephalosporin antibiotic and discharge home.
2- IV oxacillin and gentamicin.
3- arthroscopic drainage of the glenohumeral joint.
4- open irrigation and drainage of the glenohumeral joint.
5- aspiration of the glenohumeral joint and subacromial space with Gram stain and culture of the fluid.
PREFERRED RESPONSE: 5
DISCUSSION: It appears that the patient has septic arthritis of the glenohumeral joint; therefore, initial management should consist of aspiration of the glenohumeral joint and subacromial space separately, followed by Gram stain and culture of the fluid. Based on the findings, broad-spectrum IV antibiotics should be started. If the diagnosis of septic arthritis is confirmed, then arthroscopic or open surgical drainage usually is indicated.
REFERENCES: Sawyer JR, Esterhai JL Jr: Shoulder infections, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997.
Leslie BM, Harris JM, Driscoll D: Septic arthritis of the shoulder in adults. J Bone Joint Surg Am 1989;71:1516-1522.
Question 36High Yield
A 14-year-old girl with a history of aortic root dilation and FBN1 gene mutation and arachnodactyly presents with a thoracolumbar curve of 55°. When compared with patients with adolescent idiopathic scoliosis, the expected outcome with posterior spinal fusion and instrumentation of this patient's scoliosis would be (a) higher
Explanation
■
Marfan syndrome is an autosomal dominant disorder caused by a defect in the FBN1 gene encoding fibrillin1. The main orthopaedic feature of Marfan syndrome is overgrowth of the long bones and related tall stature, chest deformities (pectus carinatum or excavatum), arachnodactyly, protrusio acetabuli, flatfeet, scoliosis and dural ectasia.
Scoliosis in Marfan patients tends to progress rapidly, be less responsive to bracing, and have more revisions and complications as a result of higher rates of cerebrospinal fluid leaks, fixation failure, spine fracture, distal degeneration, proximal add on, and dural ectasia. Fixation failure is likely attributable to osteopenia, dysplastic pedicles, and dysplastic lamina. Dural ectasia, or enlargement of the dural sac, is a highly specific diagnostic feature of Marfan syndrome and is present in more than two-thirds of patients. As the dural sac balloons, it may erode the surrounding bone, which already is weakened by the genetic mutation. These changes pose a challenge to surgical fixation and create a high likelihood of fracture and dural injury. Although some studies report higher blood loss and longer surgical times than in patients with adolescent idiopathic scoliosis, other studies dispute this. Neurological complication and pseudoarthrosis rates have been similar between these two groups of patients.
Marfan syndrome is an autosomal dominant disorder caused by a defect in the FBN1 gene encoding fibrillin1. The main orthopaedic feature of Marfan syndrome is overgrowth of the long bones and related tall stature, chest deformities (pectus carinatum or excavatum), arachnodactyly, protrusio acetabuli, flatfeet, scoliosis and dural ectasia.
Scoliosis in Marfan patients tends to progress rapidly, be less responsive to bracing, and have more revisions and complications as a result of higher rates of cerebrospinal fluid leaks, fixation failure, spine fracture, distal degeneration, proximal add on, and dural ectasia. Fixation failure is likely attributable to osteopenia, dysplastic pedicles, and dysplastic lamina. Dural ectasia, or enlargement of the dural sac, is a highly specific diagnostic feature of Marfan syndrome and is present in more than two-thirds of patients. As the dural sac balloons, it may erode the surrounding bone, which already is weakened by the genetic mutation. These changes pose a challenge to surgical fixation and create a high likelihood of fracture and dural injury. Although some studies report higher blood loss and longer surgical times than in patients with adolescent idiopathic scoliosis, other studies dispute this. Neurological complication and pseudoarthrosis rates have been similar between these two groups of patients.
Question 37High Yield
1237) Which of the following is an indication for surgical treatment of an acute humeral shaft fracture?
Explanation
Humeral shaft fractures can be managed nonoperatively due to a high union rate with infrequent complications. Certain situations, however, favor operative osteosynthesis: failure of closed reduction, associated articular injury, vascular or brachial plexus injuries, associated ipsilateral forearm fractures, segmental fractures, and pathologic fractures. Open fractures should be irrigated and debrided if necessary with subsequent external or internal fixation. Polytrauma patients with multiple extremity or multi-system injuries may also be considered for operative stabilization. A relative indication also may be the transverse or short oblique fracture in an active patient since these fracture patterns are more prone to delayed union. An acute radial nerve palsy associated with a humeral shaft fracture is not an indication for surgery.
Question 38High Yield
What is the most common organism implicated in periprosthetic infection of the shoulder?
Explanation
C acnes is the most common organism recovered in prosthetic shoulder infections (33%), Coagulase-negative Staphylococcus is second (21%), Methicillin-sensitive S aureus (13%), and S epidermidis (10%). MRSA accounts for 5% and Enterococcus species, 1.5%.
54
54
Question 39High Yield
Figure 97 is the clinical photograph of a 74-year-old man 6 months after undergoing an acute anterior inferior shoulder dislocation. The patient notes weakness in shoulder flexion, abduction, and extension. This clinical picture represents damage to a nerve that courses

Explanation
The axillary nerve supplies innervation to the deltoid muscle; this image shows atrophy of this muscle. It arises from the posterior cord of the brachial plexus, coursing on the anterior surface of the subscapularis and then traveling inferior to the glenohumeral joint capsule and coursing from posterior to anterior on the deep surface of the deltoid muscle. Deltoid atrophy
can mimic infraspinatus atrophy as shown in the image, but the latter would not cause the
84
physical symptoms or lateral and anterior atrophy.
Response 1 describes the course of the suprascapular nerve. Damage to this nerve causes loss of abduction and external rotation strength as well as dull, aching superior shoulder pain. Response 2 describes the course of the spinal accessory nerve. Damage to this nerve causes trapezius atrophy, depressed shoulder girdle, lateral scapular winging, scapular dyskinesis, trapezius weakness, and limited active shoulder abduction. Response 3 describes the course of the long thoracic nerve. The superficial location and the length of this nerve are thought to predispose it to injury. Damage to this nerve causes weakness of the serratus anterior which results in a depressed shoulder girdle, medial scapular winging, scapular dyskinesis, and weakened forward flexion.
RECOMMENDED READINGS
1. [Uz A, Apaydin N, Bozkurt M, Elhan A. The anatomic branch pattern of the axillary nerve. J Shoulder Elbow Surg. 2007 Mar-Apr;16(2):240-4. Epub 2006 Nov 9. PubMed PMID: 17097311.](http://www.ncbi.nlm.nih.gov/pubmed/17097311)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17097311)
2. [Piasecki DP, Romeo AA, Bach BR Jr, Nicholson GP. Suprascapular neuropathy. J Am Acad Orthop Surg. 2009 Nov;17(11):665-76. Review. PubMed PMID: 19880677. ](http://www.ncbi.nlm.nih.gov/pubmed/19880677)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19880677)
can mimic infraspinatus atrophy as shown in the image, but the latter would not cause the
84
physical symptoms or lateral and anterior atrophy.
Response 1 describes the course of the suprascapular nerve. Damage to this nerve causes loss of abduction and external rotation strength as well as dull, aching superior shoulder pain. Response 2 describes the course of the spinal accessory nerve. Damage to this nerve causes trapezius atrophy, depressed shoulder girdle, lateral scapular winging, scapular dyskinesis, trapezius weakness, and limited active shoulder abduction. Response 3 describes the course of the long thoracic nerve. The superficial location and the length of this nerve are thought to predispose it to injury. Damage to this nerve causes weakness of the serratus anterior which results in a depressed shoulder girdle, medial scapular winging, scapular dyskinesis, and weakened forward flexion.
RECOMMENDED READINGS
1. [Uz A, Apaydin N, Bozkurt M, Elhan A. The anatomic branch pattern of the axillary nerve. J Shoulder Elbow Surg. 2007 Mar-Apr;16(2):240-4. Epub 2006 Nov 9. PubMed PMID: 17097311.](http://www.ncbi.nlm.nih.gov/pubmed/17097311)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17097311)
2. [Piasecki DP, Romeo AA, Bach BR Jr, Nicholson GP. Suprascapular neuropathy. J Am Acad Orthop Surg. 2009 Nov;17(11):665-76. Review. PubMed PMID: 19880677. ](http://www.ncbi.nlm.nih.gov/pubmed/19880677)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19880677)
Question 40High Yield
A 30-year-old woman complains of medial knee pain 15 years after a meniscectomy. Radiographs show her affected knee to be 8° varus while her contralateral knee shows 3° varus. What is the goal of performing a high tibial osteotomy (HTO) on this patient?
Explanation
Varus and valgus deformities are contributing factors for unilateral osteoarthritis. Leg alignment is a driving force in the management of weight distribution in the knee, and the HTO is biomechanically designed to realign the weight-bearing line (WBL) in the coronal plane. HTO shifts load in the tibial plateau away from the arthritic compartment toward the healthy compartment. Reducing tibiofemoral load and decreasing thrust moment arms in the affected compartment of the knee joint lessens pain and slows progression of osteoarthritis.
Question 41High Yield
Which of the following is most frequently associated with heterotopic ossification about the shoulder?
Explanation
Multiple attempts at closed reduction, delayed surgery for proximal humeral fractures, and associated closed head injury all have been associated with a higher incidence of heterotopic ossification.
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, p 291.
Neer CS: Displaced proximal humerus fractures: Part II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, p 291.
Neer CS: Displaced proximal humerus fractures: Part II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
Question 42High Yield
Which of the following factors has been shown to increase the risk of peroneal tendon pathology in patients who have undergone posterior plating of lateral malleolar fractures?

Explanation
Low plate positioning with a prominent screw head in the most distal hole of the plate was shown to be correlated with peroneal tendon lesions. Distal plate placement in the absence of prominent screws was not associated with tendon lesions. Trimmed plates, locked plates, and uncontoured plates have not been shown to increase the risk of peroneal tendon pathology.
---
---
Question 43High Yield
Advantages of plain film radiograph in diagnosis and treatment of femoral acetabular impingement do NOT include:
Explanation
Plain film radiographs can successfully detect cam and pincer impingement and cartilage space narrowing, as well as allow quantified measurement of femoral head coverage. A magnetiCresonance arthrogram is necessary, however, to successfully visualize labral pathology.
Question 44High Yield
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
The pectoralis major tendon inserts lateral to the biceps tendon, which runs in the bicipital groove. The primary vascular supply of the articular surface of the humeral head is derived from the anterior circumflex humeral artery, which continues into the arcuate artery once it enters the bone. The entry point is on the anterolateral aspect of the humerus just medial to the greater tuberosity within the bicipital groove. To avoid compromising circulation, the blade plate should be placed lateral to the bicipital groove and pectoralis major tendon insertion.
REFERENCES: Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Gerber C, Schneeberger AG: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
REFERENCES: Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Gerber C, Schneeberger AG: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 45High Yield
..A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
Explanation
- Proximal avulsion of the lateral ulnar collateral ligament
Question 46High Yield
What is the most likely diagnosis based on the MRI findings shown in Figures 87a and 87b?
Explanation
DISCUSSION: The MRI scans reveal increased signal in the medial facet of the patella and the anterior aspect of the lateral femoral condyle. This pattern is typically seen in patients with acute patellar dislocations. In patients with ACL tears, the bone bruise of the lateral femoral condyle is usually seen in the central portion at the sulcus terminalis and the posterior half of the lateral tibial plateau and is not usually seen in the patella. This pattern of bone bruising is not seen with patellar tendon ruptures, LCL tears, and PCL tears.
REFERENCES: Elias DA, White LM, Fithian DA: Acute lateral patellar dislocation at MR imaging: Injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology 2002;225:736-743.
Virolainen H, Visuri T, Kuusela T: Acute dislocation of the patella: MR findings. Radiology 1993;189:243-246.
REFERENCES: Elias DA, White LM, Fithian DA: Acute lateral patellar dislocation at MR imaging: Injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology 2002;225:736-743.
Virolainen H, Visuri T, Kuusela T: Acute dislocation of the patella: MR findings. Radiology 1993;189:243-246.
Question 47High Yield
A 28-year-old construction worker with a body mass index (BMI) of 31 sustained a Weber C fracture 3 years ago. An open reduction and internal fixation was performed, but he developed degenerative changes in the ankle as seen in Figure 13. Management consisting of bracing, shoe modifications, and other modalities has failed to provide relief. He is symptomatic enough that he wants definitive treatment. What is the best treatment option at this time?

Explanation
Ankle fusion will provide the most reliable
pain relief and function for this young manual laboror. At his young age and with a BMI of 31, both total joint
---
arthroplasty and allograft replacement are controversial. An interpositional graft could be
an option, but there is not enough evidence in the literature to recommend it at this time. The radiographs show degenerative changes that are too far advanced for an arthroscopic ankle débridement to be of any benefit.
pain relief and function for this young manual laboror. At his young age and with a BMI of 31, both total joint
---
arthroplasty and allograft replacement are controversial. An interpositional graft could be
an option, but there is not enough evidence in the literature to recommend it at this time. The radiographs show degenerative changes that are too far advanced for an arthroscopic ankle débridement to be of any benefit.
Question 48High Yield
1253) A 69-year-old female sustains the injuries seen in Figures A and
B. This injury is best classified as which of the following?
B. This injury is best classified as which of the following?



Explanation
The radiographs and CT scan images show a depressed lateral tibial plateau fracture, which is correctly classified as a Schatzker III tibial plateau fracture. This fracture typically occurs as the result of the femoral condyle directly impacting the articular surface in older patients with osteopenia.
The referenced article by Bennett et al reviews the associated soft tissue injury with tibial plateau fractures. They found a 56% frequency of associated soft tissue injuries overall, with MCL injured in 20%, the LCL in 3% , the menisci in 20%, the peroneal nerve in 3%, and the anterior cruciate ligaments in 10%.
Schatzker type IV and type II fracture patterns were associated with the highest frequency of soft tissue injuries.
The referenced article by Bennett et al reviews the associated soft tissue injury with tibial plateau fractures. They found a 56% frequency of associated soft tissue injuries overall, with MCL injured in 20%, the LCL in 3% , the menisci in 20%, the peroneal nerve in 3%, and the anterior cruciate ligaments in 10%.
Schatzker type IV and type II fracture patterns were associated with the highest frequency of soft tissue injuries.
Question 49High Yield
A 16-year-old football player reports the acute onset of pain in his left foot. An AP radiograph is shown in Figure
8/. What treatment is most likely to result in successful healing for this injury?
8/. What treatment is most likely to result in successful healing for this injury?
Explanation
Fractures in this region of the fifth metatarsal have been shown to be prone to delayed union and
nonunion and therefore are most reliably managed with internal fixation. Bone grafting is generally not required.
REFERENCES: Herrera-Soto JA, Scherb M, Duffy MF, et al: Fractures of the fifth metatarsal in children and adolescents. J Pediatr Orthop 2007;27:427-431.
Fetzer GB, Wright RW: Metatarsal shaft fractures and fractures of the proximal fifth metatarsal. Clin Sports Med 2006;25:139-150.
nonunion and therefore are most reliably managed with internal fixation. Bone grafting is generally not required.
REFERENCES: Herrera-Soto JA, Scherb M, Duffy MF, et al: Fractures of the fifth metatarsal in children and adolescents. J Pediatr Orthop 2007;27:427-431.
Fetzer GB, Wright RW: Metatarsal shaft fractures and fractures of the proximal fifth metatarsal. Clin Sports Med 2006;25:139-150.
Question 50High Yield
A 14-year-old girl has a head-on-head collision while playing basketball. She had no loss of consciousness but had persistent headaches for 2 weeks. The patient is now back to school and has no headaches. What is the best next step?
Explanation
Mild traumatic brain injury is common in the adolescent child. Neuropsychological examination is widely used but, in this case, the patient is asymptomatic and has no baseline testing. There is a limited role for MRI in the recovery process of concussions. Furthermore, higher levels of physical/cognitive activity should be avoided due to their potential to increase total recovery time. In this scenario, a graduated return to activity is most appropriate thus, the next appropriate step is to start light aerobic activity.
2
2
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon