Ortho Free Review | Dr Hutaif General Orthopedics Revie -...
14 Apr 2026
48 min read
113 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Ortho Free Review | Dr Hutaif General Orthope...
00:00
Start Quiz
Question 1High Yield
Figure 30 is the radiograph of a newborn admitted to the neonatal intensive care unit (NICU) with a swollen elbow following a difficult birth.
Explanation
- Arthrogram
Question 2High Yield
A 28-year-old man is subjected to a blast and sustains the fragmentary injury shown in the plain radiographs in Figures 99a and 99b. He lacks distal radial nerve function. His wounds have associated soft-tissue damage, although they do not appear grossly contaminated, and tissue loss would not prevent either primary or delayed closure. Which surgical plan is associated with the lowest rate of revision surgery and complications?


Explanation
Two indications for nerve exploration are open fractures and high-velocity injuries. Nerve exploration under these circumstances can improve outcomes. Intramedullary fixation is associated with higher revision surgery and complication rates vs open reduction and internal fixation. Nonsurgical treatment in the setting of a high-energy injury is associated with a higher nonunion rate.
RECOMMENDED READINGS
10. [Heineman DJ, Poolman RW, Nork SE, Ponsen KJ, Bhandari M. Plate fixation or intramedullary fixation of humeral shaft fractures. Acta Orthop. 2010 Apr;81(2):216-23. doi: 10.3109/17453671003635884. Review. Erratum in: Acta Orthop. 2010 Oct;81(5):647. PubMed PMID: 20170424. ](http://www.ncbi.nlm.nih.gov/pubmed/20170424)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20170424)
11. [Bishop J, Ring D. Management of radial nerve palsy associated with humeral shaft fracture: a decision analysis model. J Hand Surg Am. 2009 Jul-Aug;34(6):991-6.e1. doi: 10.1016/j.jhsa.2008.12.029. Epub 2009 Apr 10. PubMed PMID: 19361935. ](http://www.ncbi.nlm.nih.gov/pubmed/19361935)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19361935)
RECOMMENDED READINGS
10. [Heineman DJ, Poolman RW, Nork SE, Ponsen KJ, Bhandari M. Plate fixation or intramedullary fixation of humeral shaft fractures. Acta Orthop. 2010 Apr;81(2):216-23. doi: 10.3109/17453671003635884. Review. Erratum in: Acta Orthop. 2010 Oct;81(5):647. PubMed PMID: 20170424. ](http://www.ncbi.nlm.nih.gov/pubmed/20170424)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20170424)
11. [Bishop J, Ring D. Management of radial nerve palsy associated with humeral shaft fracture: a decision analysis model. J Hand Surg Am. 2009 Jul-Aug;34(6):991-6.e1. doi: 10.1016/j.jhsa.2008.12.029. Epub 2009 Apr 10. PubMed PMID: 19361935. ](http://www.ncbi.nlm.nih.gov/pubmed/19361935)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19361935)
Question 3High Yield
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?
Explanation
The most commonly injured neurovascular structure during an anterior approach for the repair of a distal biceps tendon rupture is the lateral antebrachial cutaneous nerve. This structure is located lateral to the biceps tendon and in a superficial location just deep to the subcutaneous layer. The antecubital vein is medial and superficial with the brachial artery and median nerve also medial to the biceps tendon but deep to the common flexors. The posterior interosseous nerve is deep within the supinator muscle and can be injured in the deep dissection or through the posterior approach when using a two-incision approach.
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Ramsey ML: Distal biceps tendon injuries: Diagnosis and management. J Am Acad Orthop Surg 1999;7:199-207.
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Ramsey ML: Distal biceps tendon injuries: Diagnosis and management. J Am Acad Orthop Surg 1999;7:199-207.
Question 4High Yield
A 66-year-old woman presents with pain and a worsening deformity of her right knee after a total knee arthroplasty (TKA) 5 years ago. She has a complete work-up and is diagnosed with aseptic loosening of the tibia. She is 5’6” in height and 185 pounds. Her preoperative nasal screening shows she is negative for methicillin-resistant Staphylococcus aureus. Based on laxity on physical examination and bone loss, she was indicated for a full revision procedure. She has no known drug allergies and her past medical history is significant for osteoarthritis, hypertension and hypercholesterolemia. The patient undergoes an uncomplicated revision TKA with intraoperative testing confirming aseptic loosening. Based on the patient’s history, what is the most appropriate antibiotic prophylaxis for this patient?
Explanation
89
Historically, cefazolin has been used as a common prophylactic antibiotic for total hip arthroplasty (THA) and TKA. Traditionally, a 1-gram dose was given to patients; however, this has more recently evolved to weight-based dosing. Recommended dosing is currently 1 gram if less than 60 kg, 2 grams if between 60 kg to 120 kg and 3 grams if weighing >120 kg. Rondon and associates recently showed that underdosed patients, a situation that commonly occurs, are at higher risk for periprosthetic joint infection. Our patient falls between 60 kg to 120 kg and should receive 2-gram dosing. As she is not allergic to penicillin or cephalosporins, clindamycin is not an appropriate choice. Further, recent studies have shown no benefit in extended antibiotic use in cases of aseptic revision THA or TKA. This makes the dosing of <24 hours the most appropriate option.
Historically, cefazolin has been used as a common prophylactic antibiotic for total hip arthroplasty (THA) and TKA. Traditionally, a 1-gram dose was given to patients; however, this has more recently evolved to weight-based dosing. Recommended dosing is currently 1 gram if less than 60 kg, 2 grams if between 60 kg to 120 kg and 3 grams if weighing >120 kg. Rondon and associates recently showed that underdosed patients, a situation that commonly occurs, are at higher risk for periprosthetic joint infection. Our patient falls between 60 kg to 120 kg and should receive 2-gram dosing. As she is not allergic to penicillin or cephalosporins, clindamycin is not an appropriate choice. Further, recent studies have shown no benefit in extended antibiotic use in cases of aseptic revision THA or TKA. This makes the dosing of <24 hours the most appropriate option.
Question 5High Yield
A 67-year-old woman has a painful, arthritic proximal interphalangeal (PIP) joint, and nonsurgical measures have failed to improve the pain. What implant and joint replacement approach combination has been demonstrated to have the lowest rate of revision surgery?
Explanation
A recent systematic review compared silicone replacement, pyrocarbon replacement, and surface replacement arthroplasty for PIP arthritis. Silicone arthroplasty through a volar approach showed the greatest gains in arc of motion and had the lowest rate of revision surgeries. The rates of revision surgeries from low to high for each type of arthroplasty were 6% for silicone volar, 10% for silicone lateral, 11%
Surface replacement arthroplasty through a volar
for silicone dorsal, 18% for surface replacement dorsal, and 37% for surface replacement volar. Revision surgeries include implant replacement (to silicone or maintaining the surface replacement), arthrodesis, explantation, amputation, and other procedures.
approach showed the highest revision rate, the worst gain in arc of motion, and the greatest extension lag. However, substantial pain relief and higher satisfaction still were reported after surface replacement arthroplasty, regardless of the complications.
Surface replacement arthroplasty through a volar
for silicone dorsal, 18% for surface replacement dorsal, and 37% for surface replacement volar. Revision surgeries include implant replacement (to silicone or maintaining the surface replacement), arthrodesis, explantation, amputation, and other procedures.
approach showed the highest revision rate, the worst gain in arc of motion, and the greatest extension lag. However, substantial pain relief and higher satisfaction still were reported after surface replacement arthroplasty, regardless of the complications.
Question 6High Yield
..The best initial treatment would entail
Explanation
- isointense signal to the rotator cuff. PREFERRED RESPONSE: 1- calcium carbonate apatite.
PREFERRED RESPONSE: 1- physical therapy and nonsteroidal anti-inflammatory medications.
PREFERRED RESPONSE: 1- physical therapy and nonsteroidal anti-inflammatory medications.
Question 7High Yield
Which of the following statements is true concerning atlanto-occipital dislocations in children:
Explanation
Pediatric atlanto-occipital dislocation is increasing in frequency due to improved emergency care. Although the injuries are sometimes fatal and are often accompanied by severe spinal cord injury, this is not always the case. Although the dens-basion distance should be less than 10 mm and the power ratio should be less than 1 in normals, these are not always abnormal in children with such injuries. C linical and radiographic correlation, with computer tomography or magnetic resonance imaging if needed, are called for to maximize diagnosis.
Question 8High Yield
Enchondral ossification is responsible for mineralization in all of the following conditions except:
Explanation
Enchondral bone formation or ossification is bone formation on a cartilage model. Enchondral bone formation occurs in embryoniClong bone development, epiphyseal secondary center of ossification formation, callus formation during fracture healing, degenerating cartilage of osteoarthritis, calcifying cartilage tumors, and bone formed with use of demineralized bone matrix.
Intramembranous bone formation occurs in flat bone development (pelvis, clavicle, skull bones), bone formation during distraction osteogenesis, and perichondrial bone formation
Intramembranous bone formation occurs in flat bone development (pelvis, clavicle, skull bones), bone formation during distraction osteogenesis, and perichondrial bone formation
Question 9High Yield
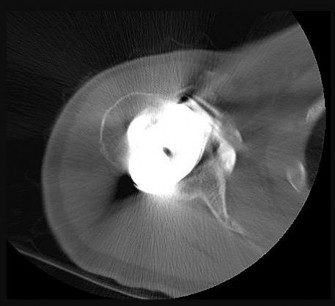
A 72-year-old woman underwent a primary total hip arthroplasty 14 months ago. She states that the hip has now dislocated four times when rising from a low chair, requiring closed reduction. A radiograph is shown in Figure 3a and a CT scan of her pelvis is shown in Figure 3b. What is the most reliable method for rectifying her instability?
Explanation
DISCUSSION: The radiograph shows well-fixed components without evidence of loosening. The CT scan shows severe retroversion of the acetabular component. Revision of the component into the correct amount of anteversion
will most reliably rectify the instability in the face of severe component malposition.
REFERENCES: Parvizi J, Picinic E, Sharkey PF: Revision total hip arthroplasty for instability: Surgical techniques and principles. J Bone Joint Surg Am 2008;90:1134-1142.
DeWal H, Su E, DiCesare PE: Instability following total hip arthroplasty. Am J Orthop 2003;32:377-382. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
DISCUSSION: The radiograph shows well-fixed components without evidence of loosening. The CT scan shows severe retroversion of the acetabular component. Revision of the component into the correct amount of anteversion
will most reliably rectify the instability in the face of severe component malposition.
REFERENCES: Parvizi J, Picinic E, Sharkey PF: Revision total hip arthroplasty for instability: Surgical techniques and principles. J Bone Joint Surg Am 2008;90:1134-1142.
DeWal H, Su E, DiCesare PE: Instability following total hip arthroplasty. Am J Orthop 2003;32:377-382. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Question 10High Yield
A surgeon recommends an interscalene regional block to a patient undergoing shoulder arthroscopy. When asked about potential complications, which of the following is most likely to occur?
Explanation
**
Sensory neuropathy is the most common complication seen with interscalene regional block.
Sensory neuropathy is the most common complication seen with interscalene regional block.
Question 11High Yield
Which of the following is true concerning the genetics of arthritis:
Explanation
One should remember the genetic findings in patients with osteoarthritis: Siblings have a 27% risk compared to spouses
Twice as common in monozygotic twins compared to dizygotic twins Precocious osteoarthritis is associated with type V collagen mutation Does not occur universally in aging hip joints
Distal interphalangeal joint arthritis linked to a region of chromosome 2q
C orrect Answer: Siblings have a 27% risk compared to spouses
Twice as common in monozygotic twins compared to dizygotic twins Precocious osteoarthritis is associated with type V collagen mutation Does not occur universally in aging hip joints
Distal interphalangeal joint arthritis linked to a region of chromosome 2q
C orrect Answer: Siblings have a 27% risk compared to spouses
Question 12High Yield
A 7-year-old girl with a known diagnosis of neurofibromatosis has neck pain and deformity. She has been wearing a soft cervical collar for the past 2 months with mild relief of her symptoms. An MRI scan shows several small neurofibromas on the left side of the cervical spine near the foramina at C6 and 7. A lateral cervical spine radiograph is shown in Figure 34. What is the most appropriate management?

Explanation
**32 • American Academy of Orthopaedic Surgeons**
DISCUSSION: With a diagnosis of neurofibromatosis and severe kyphosis, anterior and posterior treatment is needed to achieve correction and fusion. In situ fusion has a high failure rate with the kyphotic deformity and even with traction, correction of the kyphosis is not expected. Anterior treatment alone may achieve correction, but in neurofibromatosis only circumferential treatment has been shown to provide long-term stability.
REFERENCES: Crawford AH, Schorry EK: Neurofibromatosis update. J Pediatr Orthop 2006;26:4I3- 423. MehJman CT, Al-Sayyad MJ, Crawford AH: Effectiveness of spinal release and halo-femoral traction in the management of severe spinal deformity. J Pediatr Orthop 2004;24:667-673.
Figure 35
**32 • American Academy of Orthopaedic Surgeons**
DISCUSSION: With a diagnosis of neurofibromatosis and severe kyphosis, anterior and posterior treatment is needed to achieve correction and fusion. In situ fusion has a high failure rate with the kyphotic deformity and even with traction, correction of the kyphosis is not expected. Anterior treatment alone may achieve correction, but in neurofibromatosis only circumferential treatment has been shown to provide long-term stability.
REFERENCES: Crawford AH, Schorry EK: Neurofibromatosis update. J Pediatr Orthop 2006;26:4I3- 423. MehJman CT, Al-Sayyad MJ, Crawford AH: Effectiveness of spinal release and halo-femoral traction in the management of severe spinal deformity. J Pediatr Orthop 2004;24:667-673.
Figure 35
Question 13High Yield
The asterisks on Figures 98a through 98c represent which anatomic structure?
A
B
C
A
B
C



Explanation
The popliteus muscle arises from the posteromedial part of the tibia, and the tendon continues to attach to the lateral femoral condyle. The tendon is an intra-articular, extra synovial structure coursing through the popliteus hiatus, then deep to the fibular collateral ligament before inserting in the anterior portion of the popliteal sulcus.
RECOMMENDED READINGS
1. Clarke HD, Scott WN, Insall JN, et al. Anatomy. In: Insall JN, Scott WN, eds. Surgery of the Knee. Vol 1. 4th ed. Philadelphia, PA: Churchill Livingstone; 2006:3-66.
2. Miller TT: Magnetic resonance imaging of the knee. In: Insall JN, Scott WN, eds. Surgery of the Knee. Vol 1. 4th ed. Philadelphia, PA: Churchill Livingstone; 2006:201-224.
RECOMMENDED READINGS
1. Clarke HD, Scott WN, Insall JN, et al. Anatomy. In: Insall JN, Scott WN, eds. Surgery of the Knee. Vol 1. 4th ed. Philadelphia, PA: Churchill Livingstone; 2006:3-66.
2. Miller TT: Magnetic resonance imaging of the knee. In: Insall JN, Scott WN, eds. Surgery of the Knee. Vol 1. 4th ed. Philadelphia, PA: Churchill Livingstone; 2006:201-224.
Question 14High Yield
Prescribing touch (10 to 15 kg) weight-bearing would be most appropriate in the following scenario?
Explanation
Touch weight bearing (10 to 15 kg) regimens have shown to minimize joint reaction forces across the hip. This weight bearing restriction should be considered in patients who have undergone open reduction internal fixation of transtectal transverse posterior wall fractures.
The definition of touch weight bearing (also known as touch-down weight bearing) is ill-defined in the literature. Published data suggest touch weight bearing to be 10 to 15 kg of load applied to ground by the affected limb or less than 20% of body weight. In contrast, partial weight bearing is reported as 20 to 25 kg or 30% to 50% of body weight. Joint reaction forces across the hip
have been shown to be lowest with touch weight-bearing. In this scenario, the foot should be flat against the ground so the flexor and extensor musculature that cross the hip are relaxed. With non-weight bearing restrictions, the musculature across the hip will be contracted, which increases contact pressures and joint reaction forces.
Rubin et al. looked at the validity of touch weight-bearing and partial weight bearing regimens. They found that most patients overload the limb up to 50% more than the target weight prescribed.
Lewis et al. showed that maintaining non-weight-bearing position of the involved leg produces increased compressive forces across the hip joint due to activation of the hip flexors compared to restricted weight-bearing.
Incorrect Answers:
Answer 1: Acute grade II lower ankle sprain can be managed with immediate full weight bearing as tolerated.
Answer 2: Partial lateral meniscectomy for an incomplete radial tear can be managed with immediate full weight bearing as tolerated.
Answer 3: Multifragmentary calcaneus fracture open reduction internal fixation should be managed initially with non-weight bearing.
Answer 4: Uncomplicated cemented hemiarthroplasty for hip fracture can be managed with immediate full weight bearing as tolerated.
The definition of touch weight bearing (also known as touch-down weight bearing) is ill-defined in the literature. Published data suggest touch weight bearing to be 10 to 15 kg of load applied to ground by the affected limb or less than 20% of body weight. In contrast, partial weight bearing is reported as 20 to 25 kg or 30% to 50% of body weight. Joint reaction forces across the hip
have been shown to be lowest with touch weight-bearing. In this scenario, the foot should be flat against the ground so the flexor and extensor musculature that cross the hip are relaxed. With non-weight bearing restrictions, the musculature across the hip will be contracted, which increases contact pressures and joint reaction forces.
Rubin et al. looked at the validity of touch weight-bearing and partial weight bearing regimens. They found that most patients overload the limb up to 50% more than the target weight prescribed.
Lewis et al. showed that maintaining non-weight-bearing position of the involved leg produces increased compressive forces across the hip joint due to activation of the hip flexors compared to restricted weight-bearing.
Incorrect Answers:
Answer 1: Acute grade II lower ankle sprain can be managed with immediate full weight bearing as tolerated.
Answer 2: Partial lateral meniscectomy for an incomplete radial tear can be managed with immediate full weight bearing as tolerated.
Answer 3: Multifragmentary calcaneus fracture open reduction internal fixation should be managed initially with non-weight bearing.
Answer 4: Uncomplicated cemented hemiarthroplasty for hip fracture can be managed with immediate full weight bearing as tolerated.
Question 15High Yield
A high collagen concentration and a low proteoglycan concentration is found in which of the following zones of articular cartilage:
Explanation
The superficial zone has a number of important characteristics: Thinnest articular cartilage layer
Two layers:
Most superficial – fine collagen fibrils (lamina splendens)
Deep layer – flattened fibroblast-like chondrocytes (parallel to joint surface) Forms a cartilage skin
Important chemical properties:
High collagen and low proteoglycan concentration
Fibronectin and water concentrations are highest in this zone
Great tensile stiffness and strength
Seals off the cartilage from the immune system
Two layers:
Most superficial – fine collagen fibrils (lamina splendens)
Deep layer – flattened fibroblast-like chondrocytes (parallel to joint surface) Forms a cartilage skin
Important chemical properties:
High collagen and low proteoglycan concentration
Fibronectin and water concentrations are highest in this zone
Great tensile stiffness and strength
Seals off the cartilage from the immune system
Question 16High Yield
When evaluating a patient with a lumbar burst fracture, the integrity of the posterior ligamentous complex must be evaluated. Which of the following is a complete and accurate list of the components of the posterior ligamentous complex?
Explanation
No detailed explanation provided for this question.
Question 17High Yield
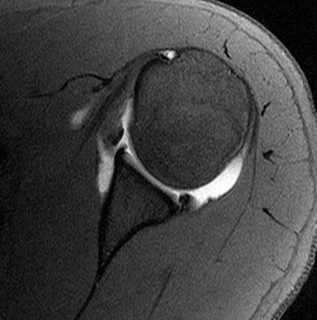
A 39-year-old man has anterior shoulder pain after landing on his abducted left shoulder while playing softball. Examination reveals a stable glenohumeral joint, pain on passive external rotation of greater than 25 degrees, and pain and weakness on belly press (Napoleon’s) test. An MRI scan is shown in Figure 32. To provide maximum pain relief and return of function, management should include
Explanation
The examination and MRI scan confirm a subscapularis rupture and dislocation of the long head of the biceps tendon. The greatest return of function will result from repair of the subscapularis and tenodesis of the biceps tendon. Physical therapy alone will result in inadequate healing of the subscapularis and will not address the biceps tendon. While biceps tenotomy is an option, it will not provide the same level of pain relief and return of function as a tenodesis in a young, active man. There is no evidence for a supraspinatus tear.
REFERENCES: Deutsch A, Altchek DW, Veltri DM, Potter HG, Warren RF: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
REFERENCES: Deutsch A, Altchek DW, Veltri DM, Potter HG, Warren RF: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 18High Yield
A 35-year-old patient sustains a left calcaneus fracture. Which of the following fractures has the highest risk of post-traumatic arthritis?
Explanation
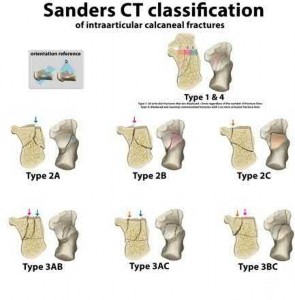
The patient most likely to require late subtalar fusion for post-traumatic arthritis is a male patient with a Sanders Type III fracture treated with ORIF.
The Sanders classification system seems to remain prognostic for injury severity. It has been shown that greater articular injury is associated with greater risk of arthritis, irrespective of patient gender and occupation. In current reviews, type III fractures are 6.5 times more likely to develop PTA and 4 times more likely to require an ST fusion than Sanders type II fractures. Post-traumatic arthritis of the subtalar joint is a common complication.
Successful salvage can be achieved with a subtalar arthrodesis.
Howard et al reported on complications following management of displaced intra-articular calcaneal fractures. 469 patients were randomized into ORIF and non-operative groups. ORIF patients were more likely to develop complications (overall 25% vs 18% of non-op) with fractures of increasing severity (Sanders IV) developing more complications regardless of management strategy.
Sanders et al. reviewed the operative treatment of displaced intra-articular calcaneal fractures. Based on the results of this comparative analysis, the Sanders classification remains prognostic; after a minimum of 10 years, type III fractures were 4 times more likely to need a fusion than type II fractures.
Illustration A shows the Sanders classification. Incorrect Answers:
Answers 1,3-5: Functional outcomes and arthritis will be determined by the
amount of cartilage damage. This is directly correlated with initial injury, fracture pattern (Sanders) and reduction techniques. Worker compensation are associated with worse functional outcome scores, not post-traumatic arthritis.
The Sanders classification system seems to remain prognostic for injury severity. It has been shown that greater articular injury is associated with greater risk of arthritis, irrespective of patient gender and occupation. In current reviews, type III fractures are 6.5 times more likely to develop PTA and 4 times more likely to require an ST fusion than Sanders type II fractures. Post-traumatic arthritis of the subtalar joint is a common complication.
Successful salvage can be achieved with a subtalar arthrodesis.
Howard et al reported on complications following management of displaced intra-articular calcaneal fractures. 469 patients were randomized into ORIF and non-operative groups. ORIF patients were more likely to develop complications (overall 25% vs 18% of non-op) with fractures of increasing severity (Sanders IV) developing more complications regardless of management strategy.
Sanders et al. reviewed the operative treatment of displaced intra-articular calcaneal fractures. Based on the results of this comparative analysis, the Sanders classification remains prognostic; after a minimum of 10 years, type III fractures were 4 times more likely to need a fusion than type II fractures.
Illustration A shows the Sanders classification. Incorrect Answers:
Answers 1,3-5: Functional outcomes and arthritis will be determined by the
amount of cartilage damage. This is directly correlated with initial injury, fracture pattern (Sanders) and reduction techniques. Worker compensation are associated with worse functional outcome scores, not post-traumatic arthritis.
Question 19High Yield
A 40-year-old male who sustained an open pilon fracture 2 weeks ago is scheduled for a below-the-knee amputation (BKA). What laboratory value is the best predictor for wound healing?
Explanation
Based on the choices above, the most important predictor of wound healing is the serum albumin level.
Wound healing is based on several factors, which include the vascular status, the immune status, and the nutritional status of the patient. Some important clinical findings include an ankle brachial index (ABI) > 0.45, a total lymphocyte count > 1500/mm3 and a serum albumin > 3.0 g/dL.
Kay et al. discuss the importance of the nutritional status in wound healing after lower extremity amputation procedures. They found eleven of 25 patients who were malnourished sustained either local or systemic complications postoperatively. They recommend that patients should undergo nutritional screening prior to elective lower extremity amputations, to help optimize their wound healing.
Incorrect Answers
Answer 2: While total protein is a marker of nutritional status, it is not as sensitive as the serum albumin for wound healing potential.
Answers 3, 4, 5: Calcium levels, C-reactive protein and ESR are not markers of wound healing
Wound healing is based on several factors, which include the vascular status, the immune status, and the nutritional status of the patient. Some important clinical findings include an ankle brachial index (ABI) > 0.45, a total lymphocyte count > 1500/mm3 and a serum albumin > 3.0 g/dL.
Kay et al. discuss the importance of the nutritional status in wound healing after lower extremity amputation procedures. They found eleven of 25 patients who were malnourished sustained either local or systemic complications postoperatively. They recommend that patients should undergo nutritional screening prior to elective lower extremity amputations, to help optimize their wound healing.
Incorrect Answers
Answer 2: While total protein is a marker of nutritional status, it is not as sensitive as the serum albumin for wound healing potential.
Answers 3, 4, 5: Calcium levels, C-reactive protein and ESR are not markers of wound healing
Question 20High Yield
Which of the following statements best describes the instantaneous axis of rotation (IAR) for thefunctional spinal unit?
Explanation
The instantaneous axis of rotation is the axis about which each vertebral segment rotates,but is theoretical depending on how it is defined, and varies depending on multiple factors. It is not a fixed point but can move depending on the position of the spine, and it is affected by degenerative conditions,fractures, injuries, and other anatomic changes of the spine. There are three axes of movement with 6 degrees of freedom (rotation and translation movements about each axis).
Question 21High Yield
A 15-year-old girl reports popping and clicking at the sternoclavicular joint and an intermittent asymmetrical prominence of the medial head of the clavicle. She denies any history of trauma or other symptoms. Management should consist of
Explanation
Atraumatic subluxation or dislocation of the sternoclavicular joint typically occurs in individuals with generalized ligamentous laxity. It is generally not painful, has no long-term sequelae, and needs no treatment. In fact, it is more likely to be painful following surgery than if managed nonsurgically.
REFERENCES: Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998,
p 583.
REFERENCES: Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998,
p 583.
Question 22High Yield
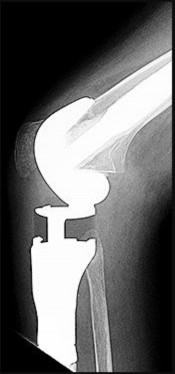
Figure 94 shows the lateral radiograph of an 80-year-old woman who is an independent ambulator and has a supracondylar periprosthetic fracture around the knee. What is the most appropriate management for this patient?
Explanation
DISCUSSION: A supracondylar femoral periprosthetic fracture that is a reducible or an irreducible fracture with poor distal bone stock and in the vicinity of loose or malpositioned components (type III) is very difficult to treat. One of the treatment options for patients with a loose femoral component and poor bone stock is the use of distal femoral replacement. The distal femoral replacement can be performed with relative ease, expediency, and is best suited for elderly or sedentary patients.
REFERENCES: Kassab M, Zalzal P, Azores GM, et al: Management of periprosthetic femoral fractures after total knee arthroplasty using a distal femoral allograft. J Arthroplasty 2004;19:361-368.
Kim KI, Egol KA, Hozack WJ, et al: Periprosthetic fractures after total knee arthroplasties. Clin Orthop Relat Res
2006;446:167-175.
REFERENCES: Kassab M, Zalzal P, Azores GM, et al: Management of periprosthetic femoral fractures after total knee arthroplasty using a distal femoral allograft. J Arthroplasty 2004;19:361-368.
Kim KI, Egol KA, Hozack WJ, et al: Periprosthetic fractures after total knee arthroplasties. Clin Orthop Relat Res
2006;446:167-175.
Question 23High Yield
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Explanation
Malunion of the talus is a devastating complication that leads to malpositioning of the foot and subsequent arthrosis of the subtalar joint complex. This is considered an avoidable complication in that accurate surgical reduction will minimize its development. Posttraumatic arthritis of the subtalar joint, osteonecrosis of the talus, posttraumatic arthritis of the ankle joint, and complex regional pain syndrome all may develop as a result of the initial traumatic event and may not be avoidable despite anatomic reduction.
REFERENCES: Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its affects on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
REFERENCES: Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its affects on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
Question 24High Yield
Which of the following tumors is considered highly vascular?
Explanation
Preoperative embolization is often used for highly vascular lesions such as renal andthyroid metastases.
Question 25High Yield
During what phase of the throwing motion is the highest torque measured across the glenohumeral joint?
Explanation
Electromyography is used to evaluate muscular firing patterns about the shoulder during the throwing sequence. The rotator cuff muscles and biceps are relatively inactive during the acceleration phase, whereas the pectoralis major, serratus anterior, latissimus dorsi, and subscapularis show highest activity. By contrast, deceleration is accomplished by the rotator cuff musculature and the larger trunk muscles acting in concert to slow down the arm. It is during this phase of follow through that the highest torque is measured secondary to eccentric muscle contraction.
REFERENCES: Jobe FW, Moynes DR, Tibone JE, Perry J: An EMG analysis of the shoulder in pitching: A second report. Am J Sports Med 1984;12:218-220.
Pappas AM, Zawacki RM, Sulliva TJ: Biomechanics of baseball pitching: A preliminary report. Am J Sports Med 1985;13:216-222.
Altcheck DW, Dines DM: Shoulder injuries in the throwing athlete. J Am Acad Orthop Surg 1995;3:159-165.
REFERENCES: Jobe FW, Moynes DR, Tibone JE, Perry J: An EMG analysis of the shoulder in pitching: A second report. Am J Sports Med 1984;12:218-220.
Pappas AM, Zawacki RM, Sulliva TJ: Biomechanics of baseball pitching: A preliminary report. Am J Sports Med 1985;13:216-222.
Altcheck DW, Dines DM: Shoulder injuries in the throwing athlete. J Am Acad Orthop Surg 1995;3:159-165.
Question 26High Yield
Figure 1 is the radiograph of a 50-year old woman with lateral-sided left knee pain. She noticed the pain over the last few months and has had no new injury. She had a microfracture performed of her lateral femoral condyle 5 years ago. What is the likely cause of the finding noted on her radiograph?
---
---


Explanation
The radiograph reveals bony overgrowth of the microfracture site on the lateral femoral condyle. This occurs from violation of the subchondral plate during aggressive removal of the calcified cartilage layer during the microfracture. It is important during a microfracture to attempt to have a contained lesion and remove the calcified cartilage layer down to the subchondral plate, but avoid aggressively penetrating the _plate._
Question 27High Yield
A 78-year-old athletic woman has a history of severe back pain without antecedent trauma. She was in the emergency department 2 days ago with a T12 compression fracture. A dual x-ray absorptiometry (DEXA) scan performed earlier this year revealed a T-score of -2.8. Her condition may be attributable to
Explanation
The diagnosis is severe osteoporosis because this patient's T-score is lower than -2.5 on DEXA scan and her fragility fracture involves the T12 vertebra. Osteoporosis may be associated with polymorphisms of the COL1A1 gene. EXT1 is associated with multiple hereditary exostoses, and translocation X:18 is associated with synovial sarcoma. The gene p53 is associated with Li-Fraumeni syndrome and osteosarcoma.
RECOMMENDED READINGS
Masoodi TA, Alsaif MA, Al Shammari SA, Alhamdan AA. Evaluation and identification of damaged single nucleotide polymorphisms in COL1A1 gene involved in osteoporosis. Arch Med Sci. 2013 Oct 31;9(5):899-905. doi: 10.5114/aoms.2012.28598. Epub 2012 May 13.
[PubMed PMID: 24273577. ? ](http://www.ncbi.nlm.nih.gov/pubmed/%2024273577)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2024273577)
[Kurt-Sirin O, Yilmaz-Aydogan H, Uyar M, Seyhan MF, Isbir T, Can A. Combined effects of collagen type I alpha1 (COL1A1) Sp1 polymorphism and osteoporosis risk factors on bone mineral density in Turkish postmenopausal women. Gene. 2014 May 1;540(2):226-31. doi: 10.1016/j.gene.2014.02.028. Epub 2014 Feb 22. PubMed PMID: 24566004. ? ](http://www.ncbi.nlm.nih.gov/pubmed/24566004)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/24566004)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24566004)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24566004)
RECOMMENDED READINGS
Masoodi TA, Alsaif MA, Al Shammari SA, Alhamdan AA. Evaluation and identification of damaged single nucleotide polymorphisms in COL1A1 gene involved in osteoporosis. Arch Med Sci. 2013 Oct 31;9(5):899-905. doi: 10.5114/aoms.2012.28598. Epub 2012 May 13.
[PubMed PMID: 24273577. ? ](http://www.ncbi.nlm.nih.gov/pubmed/%2024273577)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2024273577)
[Kurt-Sirin O, Yilmaz-Aydogan H, Uyar M, Seyhan MF, Isbir T, Can A. Combined effects of collagen type I alpha1 (COL1A1) Sp1 polymorphism and osteoporosis risk factors on bone mineral density in Turkish postmenopausal women. Gene. 2014 May 1;540(2):226-31. doi: 10.1016/j.gene.2014.02.028. Epub 2014 Feb 22. PubMed PMID: 24566004. ? ](http://www.ncbi.nlm.nih.gov/pubmed/24566004)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/24566004)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24566004)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24566004)
Question 28High Yield
After performing an uneventful partial palmar fasciectomy for Dupuytren contracture of the palm and ring finger, a general postsurgical pain medication prescription should include how many narcotic pills?
Explanation
After the designation of pain as the fifth vital sign, opioid analgesic use has steadily increased. Many surgeons routinely prescribe 30 or more pills after elective hand surgery. However, studies show that patients generally use fewer than 30 pills. Patients who underwent bone procedures used 14 pills, and those undergoing soft-tissue procedures used 9 pills. Education and decision aids may help physicians size prescriptions appropriately to avoid overmedication. Patients undergoing small soft-tissue surgeries such as trigger releases should not need narcotics. Those undergoing small-joint surgeries, carpal tunnel releases, and Dupuytren fasciectomy may benefit from a prescription of 10 pills. More extensive surgery, such as open fracture treatment, may justify more pills, but prescriptions should not exceed 40 tablets _under typical circumstances._
Question 29High Yield
A 55-year-old man experiences right shoulder pain 2 years after undergoing hemiarthroplasty for osteoarthritis. His laboratory values indicate normal C-reactive protein, erythrocyte sedimentation rate, and white blood cell count levels. He undergoes a shoulder aspiration and culture and an arthroscopic biopsy; all findings are negative. Belly-press and bear-hug test results are normal (Figures 92a and 92b).

Explanation
- Anatomic total shoulder arthroplasty (TSA)_
Question 30High Yield
A 52-year-old man who weighs 325 lb is wheelchair-bound from severe degenerative arthritis of the left hip. Twenty-four hours after cementless total hip arthroplasty, he develops shortness of breath and evaluation shows a saddle pulmonary embolus. The patient is started on enoxaparin sodium at 150 mg every 12 hours. Two days later, the patient’s hematocrit is 20% despite four units of transfused packed cells, and he now has developed a complete sciatic nerve palsy. What is the best course of action?
Explanation
DISCUSSION: The purpose of this question is to draw attention to the early risks of therapeutic anticoagulation that will be instituted by an intensivist or pulmonologist to treat a life-threatening pulmonary embolus. The temporary vena cava filter is a recent innovation but will effectively reduce the risk of further pulmonary emboli. This requires reversal of anticoagulation for safe insertion of the filter and creates a safe situation for additional surgical solutions. Sciatic nerve compromise was caused by the expanding hematoma in this patient, which could be mitigated by exploration both to assess the nerve and to remove a large hematoma that presents its own long- term risks.
REFERENCES: Della Valle CJ, Steiger DJ, Di Cesare PE: Thromboembolism after hip and knee arthroplasty: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:327-336.
Weil Y, Mattan Y, Goldman V, et al: Sciatic nerve palsy due to hematoma after thrombolysis therapy for acute pulmonary embolism after total hip arthroplasty. J Arthroplasty 2006;21:456-459.
American Academy of Orthopaedic Surgeons Guideline on the Prevention of Symptomatic Pulmonary Embolism in Patients Undergoing Total Hip or Knee Arthroplasty, [www.aaos.org/research/guidelines/](http://www.aaos.org/research/guidelines/) PEguide.asp
DISCUSSION: The purpose of this question is to draw attention to the early risks of therapeutic anticoagulation that will be instituted by an intensivist or pulmonologist to treat a life-threatening pulmonary embolus. The temporary vena cava filter is a recent innovation but will effectively reduce the risk of further pulmonary emboli. This requires reversal of anticoagulation for safe insertion of the filter and creates a safe situation for additional surgical solutions. Sciatic nerve compromise was caused by the expanding hematoma in this patient, which could be mitigated by exploration both to assess the nerve and to remove a large hematoma that presents its own long- term risks.
REFERENCES: Della Valle CJ, Steiger DJ, Di Cesare PE: Thromboembolism after hip and knee arthroplasty: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:327-336.
Weil Y, Mattan Y, Goldman V, et al: Sciatic nerve palsy due to hematoma after thrombolysis therapy for acute pulmonary embolism after total hip arthroplasty. J Arthroplasty 2006;21:456-459.
American Academy of Orthopaedic Surgeons Guideline on the Prevention of Symptomatic Pulmonary Embolism in Patients Undergoing Total Hip or Knee Arthroplasty, [www.aaos.org/research/guidelines/](http://www.aaos.org/research/guidelines/) PEguide.asp
Question 31High Yield
Figures 92a and 92b are the reconstruction radiographs of a 16-year-old boy with a high-grade conventional osteosarcoma of his right proximal tibia. He has completed neoadjuvant
chemotherapy. Wide resection, endoprosthetic proximal tibia replacement, a medial gastrocnemius flap, and a split-thickness skin graft were performed. The preferred postsurgical knee rehabilitation regimen is
chemotherapy. Wide resection, endoprosthetic proximal tibia replacement, a medial gastrocnemius flap, and a split-thickness skin graft were performed. The preferred postsurgical knee rehabilitation regimen is

Explanation
This patient underwent resection of the patellar tendon insertion onto the proximal tibia. The residual tendon is sutured to the prosthesis with augmentation of the repair by the medial gastrocnemius flap. Immobilization for 6 weeks in full extension is preferred to permit healing of the tendon repair and prevent patella alta with associated extensor lag. Cast, splint, or brace are all acceptable options for the initial immobilization. Risk for knee stiffness with such immobilization is low because all of the distal knee ligamentous and capsular attachments are transected with resection. Two weeks of immobilization may be adequate for flap and skin graft healing, but this amount of time is inadequate for patellar tendon healing. Continuous passive motion vs therapist-
directed range of motion has not been rigorously compared for proximal tibia replacement. Responses 1 and 2 include early motion.
RECOMMENDED READINGS
89. [Eckardt JJ, Matthews JG 2nd, Eilber FR. Endoprosthetic reconstruction after bone tumor resections of the proximal tibia. Orthop Clin North Am. 1991 Jan;22(1):149-60. PubMed PMID: 1992431. ](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[View](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[ ](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1992431)
90. [Jentzsch T, Erschbamer M, Seeli F, Fuchs B. Extensor function after medial gastrocnemius flap reconstruction of the proximal tibia. Clin Orthop Relat Res. 2013 Jul;471(7):2333-9. doi: 10.1007/s11999-013-2851-8. Epub 2013 Feb 20. PubMed PMID: 23423620. ](http://www.ncbi.nlm.nih.gov/pubmed/23423620)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/23423620)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23423620)
91. [Mavrogenis AF, Pala E, Angelini A, Ferraro A, Ruggieri P. Proximal tibial resections and reconstructions: clinical outcome of 225 patients. J Surg Oncol. 2013 Mar;107(4):335-42. doi: 10.1002/jso.23216. Epub 2012 Jul 17. PubMed PMID: 22806768. ](http://www.ncbi.nlm.nih.gov/pubmed/22806768)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22806768)
directed range of motion has not been rigorously compared for proximal tibia replacement. Responses 1 and 2 include early motion.
RECOMMENDED READINGS
89. [Eckardt JJ, Matthews JG 2nd, Eilber FR. Endoprosthetic reconstruction after bone tumor resections of the proximal tibia. Orthop Clin North Am. 1991 Jan;22(1):149-60. PubMed PMID: 1992431. ](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[View](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[ ](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1992431)
90. [Jentzsch T, Erschbamer M, Seeli F, Fuchs B. Extensor function after medial gastrocnemius flap reconstruction of the proximal tibia. Clin Orthop Relat Res. 2013 Jul;471(7):2333-9. doi: 10.1007/s11999-013-2851-8. Epub 2013 Feb 20. PubMed PMID: 23423620. ](http://www.ncbi.nlm.nih.gov/pubmed/23423620)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/23423620)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23423620)
91. [Mavrogenis AF, Pala E, Angelini A, Ferraro A, Ruggieri P. Proximal tibial resections and reconstructions: clinical outcome of 225 patients. J Surg Oncol. 2013 Mar;107(4):335-42. doi: 10.1002/jso.23216. Epub 2012 Jul 17. PubMed PMID: 22806768. ](http://www.ncbi.nlm.nih.gov/pubmed/22806768)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22806768)
Question 32High Yield
Figures 66a and 66b are the clinical photographs of an 86-year-old man with a high-grade undifferentiated pleomorphic sarcoma of the right thigh. He is pictured during preparations for wide surgical excision. What is a favorable prognostic factor?


Explanation
Improved survival is found in patients with soft-tissue sarcoma involving the extremities (appendicular) rather than the torso (axial) or head and neck. Although the superficial location above the fascia is associated with improved survival, malignant ulceration or fungation is an independent risk factor for poor outcome. Areas of extensive necrosis are routinely found in high-
grade undifferentiated pleomorphic sarcomas and do not suggest a favorable prognosis. Local inflammatory reactions to malignant ulceration do not improve survival.
RECOMMENDED READINGS
28. [Potter BK, Adams SC, Qadir R, Pitcher JD, Temple HT. Fungating soft-tissue sarcomas. Treatment implications and prognostic importance of malignant ulceration. J Bone Joint Surg Am. 2009 Mar 1;91(3):567-74. doi: 10.2106/JBJS.H.00071. PubMed PMID: 19255216. ](http://www.ncbi.nlm.nih.gov/pubmed/19255216)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19255216)
29. [Brennan MF, Antonescu CR, Moraco N, Singer S. Lessons learned from the study of 10,000 patients with soft tissue sarcoma. Ann Surg. 2014 Sep;260(3):416-21; discussion 421-2. doi: 10.1097/SLA.0000000000000869. PubMed PMID: 25115417. ](http://www.ncbi.nlm.nih.gov/pubmed/25115417)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25115417)
grade undifferentiated pleomorphic sarcomas and do not suggest a favorable prognosis. Local inflammatory reactions to malignant ulceration do not improve survival.
RECOMMENDED READINGS
28. [Potter BK, Adams SC, Qadir R, Pitcher JD, Temple HT. Fungating soft-tissue sarcomas. Treatment implications and prognostic importance of malignant ulceration. J Bone Joint Surg Am. 2009 Mar 1;91(3):567-74. doi: 10.2106/JBJS.H.00071. PubMed PMID: 19255216. ](http://www.ncbi.nlm.nih.gov/pubmed/19255216)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19255216)
29. [Brennan MF, Antonescu CR, Moraco N, Singer S. Lessons learned from the study of 10,000 patients with soft tissue sarcoma. Ann Surg. 2014 Sep;260(3):416-21; discussion 421-2. doi: 10.1097/SLA.0000000000000869. PubMed PMID: 25115417. ](http://www.ncbi.nlm.nih.gov/pubmed/25115417)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25115417)
Question 33High Yield
The major blood supply to the cruciate ligaments arises from which of the
following structures?
following structures?
Explanation
The major blood supply to the cruciate ligaments arises from the ligamentous branches of the middle genicular artery. Few terminal branches of the inferior genicular artery contribute to the blood supply. The synovial plexus and sheath covering the cruciate ligaments are also supplied by branches of the middle genicular artery. The blood supply to the cruciate ligaments is predominately of soft-tissue origin. There is no significant osseous vascular contribution to the ligaments.
REFERENCES: Arnoczky SP: Anatomy of the anterior cruciate ligament. Clin Orthop 1983;172:19-25.
Arnoczsky SP: Blood supply to the anterior cruciate ligament and supporting structures. Orthop Clin North Am 1985;16:15-28.
REFERENCES: Arnoczky SP: Anatomy of the anterior cruciate ligament. Clin Orthop 1983;172:19-25.
Arnoczsky SP: Blood supply to the anterior cruciate ligament and supporting structures. Orthop Clin North Am 1985;16:15-28.
Question 34High Yield
Atraumatic neuropathy of the suprascapular nerve usually occurs at what
anatomic location?
anatomic location?
Explanation
The suprascapular nerve passes through the suprascapular notch and the spinoglenoid notch before innervating the infraspinatus muscle. At both locations, the suprascapular nerve is prone to nerve compression, which often results from a ganglion cyst. The other anatomic locations are not associated with suprascapular nerve impingement.
REFERENCES: Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Post M, Mayer J: Suprascapular nerve entrapment: Diagnosis and treatment. Clin Orthop 1987;223:126-136.
REFERENCES: Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Post M, Mayer J: Suprascapular nerve entrapment: Diagnosis and treatment. Clin Orthop 1987;223:126-136.
Question 35High Yield
Primary treatment of thoracic outlet syndrome should include:
Explanation
Initial treatment of thoracic outlet syndrome is non-operative. Aggravating activities are modified and shoulder girdle strengthening is initiated. Surgery is considered for patients who have failed conservative therapy and suffer intractable pain, and for those who have significant neurologic or vascular deficits. Operative procedures must be tailored to the presumed pathological anatomy; there is no single best procedure.
Question 36High Yield
After making a tackle, a football player is found prone and unconscious without spontaneous respirations. Initial management should consist of
Explanation
The on-field evaluation and management of a seriously injured athlete requires that health care teams have a game plan in place and proper equipment that is readily available. The initial step, which consists of stabilizing the head and neck by manually holding them in a neutral position, is then followed by assessment of breathing, pulses, and level of consciousness. If the athlete is breathing, management should consist of mouth guard removal and airway maintenance. If the athlete is not breathing, the face mask should be removed, with the chin strap left in place. The airway must be established, followed by initiation of assisted breathing. CPR is instituted only when breathing and circulation are compromised. In the unconscious athlete or if a cervical spine injury is suspected, the helmet must not be removed until the athlete has been transported to an appropriate facility and the cervical spine has been completely evaluated.
Scientific References
- : McSwain NE, Garnelli, RL: Helmet removal from injured patients. Bull of Am Coll Surg 1997;82:42-44.
Vegso JJ: Field evaluation and management of head and neck injuries. Post Grad Adv Sport Med 1987;10:2-10.
Question 37High Yield
In the evaluation of somatosensory-evoked potential waveforms for intraoperative neuromonitoring for spinal surgery, the minimum criteria for determining potentially significant changes include
Explanation
The established criteria for interpreting a significant change are 50% decrease in signal amplitude, 10% latency increase, and/or a complete loss of potential. Intraoperative spinal cord monitoring during spinal surgery generally consists of a combination of monitoring modalities.Somatosensory-evoked potentials in combination with intraoperative electromyography can provide adequate coverage of sensory and motor components of spinal cord and nerve root function. Significant changes in evoked potential waveform characteristics can reflect dysfunction of the ascending somatosensory system.
Question 38High Yield
Figure 1 is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal. What is the main function of the structure delineated by the black asterisks?
---
---

Explanation
The structure shown is the posterolateral bundle of the anterior cruciate ligament (ACL). This bundle is optimally positioned in the knee to resist rotatory forces during terminal knee extension. "Resist anterior translation during knee flexion" best describes the anteromedial bundle. "Resist rotatory loads during knee flexion" is unlikely because the posterolateral bundle is tightest during knee extension. The posterior cruciate ligament, not the ACL, functions to resist posterior translation.
Question 39High Yield
Figures 1 through 5 are the radiograph, MRI scan, and clinical photograph of a 9-year-old boy who has a new wound of the posteromedial heel without recent injury or fevers. He has a 2-month history of heel pain and has been treated for calcaneal apophysitis with a walking boot. Complete blood count, CRP level, and ESR are normal. What is the best next step?

Explanation
■
This patient has chronic calcaneal osteomyelitis. Pediatric calcaneal osteomyelitis may follow an indolent course with a delay in diagnosis. Given the draining wound, chronic radiographic changes; and MRI evidence of abscess, operative biopsy and debridement is the next step. Iliac crest aspiration may be appropriate if leukemia is suspected based upon the complete blood count. A bone scan or skeletal survey may be a consideration if the biopsy is consistent with malignancy or if the patient has poorly localized symptoms.
■
This patient has chronic calcaneal osteomyelitis. Pediatric calcaneal osteomyelitis may follow an indolent course with a delay in diagnosis. Given the draining wound, chronic radiographic changes; and MRI evidence of abscess, operative biopsy and debridement is the next step. Iliac crest aspiration may be appropriate if leukemia is suspected based upon the complete blood count. A bone scan or skeletal survey may be a consideration if the biopsy is consistent with malignancy or if the patient has poorly localized symptoms.
Question 40High Yield
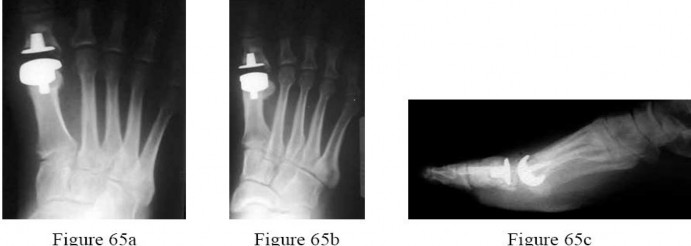
Figures 65a through 65c are the weight-bearing radiographs of a 42-year-old male manual laborer who has a 6-month history of persistent great toe swelling and pain after undergoing a total joint Arthroplasty for hallux rigidus 9 months ago. He denies postoperative wound complications, recent fevers, chills, or other constitutional signs; however, he has never been able to ambulate without pain since his return to work. Examination reveals moderate diffuse swelling, but no fluctuance or drainage.
Range of motion includes 25° of dorsiflexion. Laboratory studies show an erythrocyte sedimentation rate of 18 mm/h and a c-reactive protein level of <0.7 mg/L. What is the most likely source of his symptoms?
---
Range of motion includes 25° of dorsiflexion. Laboratory studies show an erythrocyte sedimentation rate of 18 mm/h and a c-reactive protein level of <0.7 mg/L. What is the most likely source of his symptoms?
---
Explanation
The patient has developed mechanical failure as evidenced by the lucency surrounding the proximal phalanx component. His pain has correlated with his return to work as a manual laborer.Although septic arthritis is a possibility, it is less likely based on the normal laboratory studies and lack of infectious signs. Periprosthetic fracture is unlikely because of the lack of a traumatic event or a sudden change in symptoms rather than a persistent inability to progress his activities. A transfer lesion from metatarsal shortening would result in pain from mechanical overload at areas adjacent to the first
metatarsal. Aseptic loosening from polyethylene debris would imply that the implant has previously been stable and well-fixed, and subsequently loosened over an extended period of time.
metatarsal. Aseptic loosening from polyethylene debris would imply that the implant has previously been stable and well-fixed, and subsequently loosened over an extended period of time.
Question 41High Yield
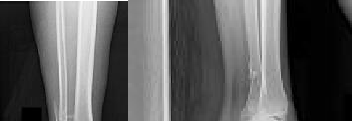
An 80-year-old patient presents 8 months postoperatively with right groin pain. Examination reveals a leg length discrepancy of
1.5cm. Recent radiographs are seen in Figures A and B. What is the most appropriate treatment plan?
1.5cm. Recent radiographs are seen in Figures A and B. What is the most appropriate treatment plan?


Explanation
This patient has atrophic non-union (NU) and varus collapse following cephalomedullary nailing of a subtrochanteric fracture. The ideal treatment involves nail removal, correction of alignment, fracture fixation, and bone grafting. Fixation can be achieved with a nail or plate.
Subtrochanteric fractures can be treated with cephalomedullary nailing or fixed angle plates. Nailing of these fractures is technically challenging because the fracture must be reduced prior to nail passage. Failure to do so leads to varus and procurvatum malreduction.
Bellabarba et al. reviewed plating of femoral nonunions after intramedullary nailing. Of 23 nonunions, 21 healed at an average of 12 weeks. The remaining 2 cases required repeat plating (at 2 and 8 weeks) for hardware breakage because of noncompliance with weightbearing restrictions. They advocate plating because it allows for correction of malalignment and provides a biomechanically superior tension band construct.
Incorrect Answers:
Answer 1:Dynamization is less effective in femoral NU compared with tibial NU. It is suitable for NU of axially stable fractures without significant angular deformity, particularly if statically locked in distraction. It is not suitable in this case because of varus collapse and shortening.
Answer 2: The use of tensioned wire fixators is poorly tolerated in the femur and has a high complication rate.
Answer 3: Reamed exchange nailing is the procedure of choice after IM nailing in the ABSENCE of femoral deformity. It is less effective in this case of varus collapse and shortening. Exchange unreamed nailing is not useful because (1) the new nail follows the same path as the old, making deformity correction impossible, and (2) the new nail cannot be larger than the old nail. A larger implant is only possible following reaming, especially if the isthmus is to be crossed.
Answer 4: Plating around a nail is inadvisable in this case because the existing hardware precludes deformity correction.
Subtrochanteric fractures can be treated with cephalomedullary nailing or fixed angle plates. Nailing of these fractures is technically challenging because the fracture must be reduced prior to nail passage. Failure to do so leads to varus and procurvatum malreduction.
Bellabarba et al. reviewed plating of femoral nonunions after intramedullary nailing. Of 23 nonunions, 21 healed at an average of 12 weeks. The remaining 2 cases required repeat plating (at 2 and 8 weeks) for hardware breakage because of noncompliance with weightbearing restrictions. They advocate plating because it allows for correction of malalignment and provides a biomechanically superior tension band construct.
Incorrect Answers:
Answer 1:Dynamization is less effective in femoral NU compared with tibial NU. It is suitable for NU of axially stable fractures without significant angular deformity, particularly if statically locked in distraction. It is not suitable in this case because of varus collapse and shortening.
Answer 2: The use of tensioned wire fixators is poorly tolerated in the femur and has a high complication rate.
Answer 3: Reamed exchange nailing is the procedure of choice after IM nailing in the ABSENCE of femoral deformity. It is less effective in this case of varus collapse and shortening. Exchange unreamed nailing is not useful because (1) the new nail follows the same path as the old, making deformity correction impossible, and (2) the new nail cannot be larger than the old nail. A larger implant is only possible following reaming, especially if the isthmus is to be crossed.
Answer 4: Plating around a nail is inadvisable in this case because the existing hardware precludes deformity correction.
Question 42High Yield
A 56-year-old man has a painful flatfoot deformity. Attempts at orthotic support and bracing of the foot have not been
successful. On examination, the forefoot is abducted, the heel is fixed in valgus, and the subtalar joint is rigid. The operation that is most likely to correct the foot deformity is:
successful. On examination, the forefoot is abducted, the heel is fixed in valgus, and the subtalar joint is rigid. The operation that is most likely to correct the foot deformity is:
Explanation
By history and physical examination, this patient has a Stage III flatfoot deformity. Due to the rigidity, only an arthrodesis will correct this abnormality. Although a transverse tarsal arthrodesis (C hopartâs arthrodesis) may adequately correct the deformity, a triple arthrodesis will correct all of the components including heel valgus, forefoot abduction, and midfoot pronation.
Question 43High Yield
Stemless shoulder arthroplasty prostheses have recently been suggested as an alternative to traditional stemmed replacement. Advantages of the stemless surgical technique would include
Explanation
55
Glenoid exposure, while better than with surface replacements, is not improved over traditional stemmed replacements. Metaphyseal comminution would make it unlikely that a stemless implant could be used in most four-part fractures. Stemless replacement does have the unique advantage of allowing placement of a prosthesis in the setting of a proximal humerus malunion without the need for an osteotomy, as the prosthesis is not constrained by the position of the stem. While early results are encouraging, there is no long-term data to suggest that survivorship is increased with stemless arthroplasty.
Glenoid exposure, while better than with surface replacements, is not improved over traditional stemmed replacements. Metaphyseal comminution would make it unlikely that a stemless implant could be used in most four-part fractures. Stemless replacement does have the unique advantage of allowing placement of a prosthesis in the setting of a proximal humerus malunion without the need for an osteotomy, as the prosthesis is not constrained by the position of the stem. While early results are encouraging, there is no long-term data to suggest that survivorship is increased with stemless arthroplasty.
Question 44High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Anatomic reduction and stabilization of the posterior malleolus fracture component
---
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Anatomic reduction and stabilization of the posterior malleolus fracture component
---

Explanation
The radiographs reveal a trimalleolar ankle fracture dislocation with an
associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior
malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
17. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
18. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
19. Maximizes the surface area for ankle joint loading
20. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior
malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
17. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
18. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
19. Maximizes the surface area for ankle joint loading
20. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
Question 45High Yield
Slide 1
A 54-year-old woman presents for treatment of an ulcer (Slide). She has diabetes, no protective sensation, and slight deformity of the foot. There is no inflammation of the foot and no purulent drainage. Slight serous oozing is present daily. Initial evaluation and treatment should consist of:
A 54-year-old woman presents for treatment of an ulcer (Slide). She has diabetes, no protective sensation, and slight deformity of the foot. There is no inflammation of the foot and no purulent drainage. Slight serous oozing is present daily. Initial evaluation and treatment should consist of:
Explanation
Ambulatory treatment for a patient with diabetes is always the preferable treatment. In this patient, there is no evidence of infection. Unless drainage is purulent and the ulcer is in contact with bone, there should be minimal concern for infection. Reconstruction of a C harcot deformity of the midfoot is only indicated following repeated failure of nonoperative treatments.
Question 46High Yield
Figures 1 and 2 are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg. What examination findings are most consistent with the pathology seen in the radiographs?




Explanation
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater
trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement. Surgical treatment for cam impingement can be effective for symptomatic patients. Even among high-level athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable with those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment. Byrd and Jones described five patients who developed transient neurapraxias that resolved uneventfully. The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a _periacetabular osteotomy can develop a more retroverted acetabulum as well._
trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement. Surgical treatment for cam impingement can be effective for symptomatic patients. Even among high-level athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable with those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment. Byrd and Jones described five patients who developed transient neurapraxias that resolved uneventfully. The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a _periacetabular osteotomy can develop a more retroverted acetabulum as well._
Question 47High Yield
The mean amount of growth height occurring in each vertbra per year during later childhood and early adolescence is:
Explanation
The mean growth is 0.7 mm per vertebra per year. This measurement is averaged across all of the thoracic and lumbar vertebrae.
Question 48High Yield
A 22-year-old woman has had progressive upper extremity weakness for the past several years. History reveals no pain in her neck or shoulders. Examination reveals scapular winging of both shoulders and weakness in external rotation. She can abduct to only 120 degrees bilaterally, and there is mild supraspinatus weakness. She is otherwise neurologically intact with normal sensation and reflexes; however, she has difficulty whistling. A clinical photograph is shown in Figure 14. What is the most likely diagnosis?
Explanation
Progressive weakness is a common sign with a large differential diagnosis. Nerve, muscle, and joint problems should be excluded when a patient has diffuse weakness and atrophy. Fascioscapulohumeral dystrophy is a rare disease characterized by facial muscle weakness and proximal shoulder muscle weakness. The weakness is usually bilateral, and scapular winging is common. If the scapular winging becomes pronounced, elevation of the shoulder can be affected. In severe cases, scapulothoracic fusion or pectoralis muscle transfer to the scapula may be indicated. Duchenne muscular dystrophy is typically severe and progressive. The other diagnoses are not compatible with the history or the physical findings.
REFERENCES: Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Bunch WH, Siegel IM: Scapulothoracic arthrodesis in fascioscapulohumeral muscular dystrophy: Review of seventeen procedures with three to twenty-one-year follow-up. J Bone Joint Surg Am 1993;75:372-376.
REFERENCES: Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Bunch WH, Siegel IM: Scapulothoracic arthrodesis in fascioscapulohumeral muscular dystrophy: Review of seventeen procedures with three to twenty-one-year follow-up. J Bone Joint Surg Am 1993;75:372-376.
Question 49High Yield
Augmentation of a Broström repair with the mobilized lateral portion of the extensor retinaculum (Gould
modification) is expected to produce
modification) is expected to produce
Explanation
Multiple biomechanical studies have investigated the contribution of the Gould modification with the Broström anatomic repair for chronic ankle instability. No studies to date have demonstrated a statistically significant difference in initial ankle stability with inclusion of the Gould modification or augmentation of the repair with a mobilized lateral portion of the extensor retinaculum. No clear association exists between the Broström-Gould repair technique and risk for nerve injury, postsurgical range of motion, or incidence of osteoarthritis on long-term follow-up.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon