Ortho Free Review | Dr Hutaif General Orthopedics Revie -...
14 Apr 2026
57 min read
77 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Ortho Free Review | Dr Hutaif General Orthope...
00:00
Start Quiz
Question 1High Yield
During shoulder motion with the elbow controlled in a brace, electromyographic studies of the supraspinatus show significant activity with all range-of-motion testing. Concurrent electromyographic studies of the long head of the biceps will most
likely show
likely show
Explanation
During electromyographic studies, the long head of the biceps has been shown to have little activity throughout a wide range of shoulder motion as long as the elbow is immobilized. The supraspinatus is active throughout the range of shoulder motion. Rotator cuff tears do not influence biceps activity as long as the elbow is controlled.
REFERENCES: Yamaguchi K, Riew KD, Galutz LM, et al: Biceps activity during shoulder motion: An electromyographic analysis. Clin Orthop 1997;336:122-129.
Levy AS, Kelly BT, Lintner SA, et al: Function of the long head of the biceps at the shoulder: Electromyographic analysis. J Shoulder Elbow Surg 2001;10:250-255.
REFERENCES: Yamaguchi K, Riew KD, Galutz LM, et al: Biceps activity during shoulder motion: An electromyographic analysis. Clin Orthop 1997;336:122-129.
Levy AS, Kelly BT, Lintner SA, et al: Function of the long head of the biceps at the shoulder: Electromyographic analysis. J Shoulder Elbow Surg 2001;10:250-255.
Question 2High Yield
What is the preferred imaging modality to determine the glenoid wear pattern in a patient with rheumatoid arthritis:
Explanation
A computed tomography scan provides important information in regard to the version of the glenoid, wear pattern, amount of wear, glenohumeral subluxation, as well as desired entry point
Question 3High Yield
Figures 20a and 20b are the radiographs of a 56-year-old woman who runs a horse farm. She has a 2-year history of increasing ankle pain and swelling without previous treatment. Which treatment is most appropriate at this time?


Explanation
This patient has end-stage ankle arthritis. A short course of NSAIDs may provide pain and inflammation relief. Bracing with either an ankle-foot orthosis or Arizona brace can reduce pain by offloading the ankle joint. Ankle fusion is a reliable procedure for treatment of end-stage ankle arthritis and is especially recommended for active people after it is determined that nonsurgical measures no longer provide adequate relief. Arthroscopic debridement and cheilectomy may be indicated for bony impingement and mild arthritis with little articular cartilage loss. The long-term results of ankle distraction arthroplasty are not yet well defined but likewise would be reserved for scenarios in which nonsurgical measures no longer provide adequate relief. The patient must be able to wear a thin-wire external fixator for 3 months.
RECOMMENDED READINGS
Abidi NA, Neufeld SK, Brage ME, Reese KA, Sabharwal S, Paley, D. Ankle arthritis. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:159-193.
Saltzman CL: Ankle arthritis, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle. Philadelphia, PA, Mosby Elsevier, 2007, vol 1, pp 929-932.
RECOMMENDED READINGS
Abidi NA, Neufeld SK, Brage ME, Reese KA, Sabharwal S, Paley, D. Ankle arthritis. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:159-193.
Saltzman CL: Ankle arthritis, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle. Philadelphia, PA, Mosby Elsevier, 2007, vol 1, pp 929-932.
Question 4High Yield
A 42-year-old woman sustains a closed posterior elbow dislocation. A closed reduction is performed, and the elbow appears stable under fluoroscopic examination through a full arc of motion. Initial treatment should consist of
Explanation
This is a simple (no associated fracture) elbow dislocation. Such dislocations can be treated with closed reduction followed by mobilization after 5 to 7 days to avoid stiffness, provided the elbow is stable through a full arc of motion at the time of reduction. If the elbow is unstable but has a short arc of stability, then using a hinged brace in the stable arc may be considered. It may be necessary to splint the elbow in pronation if the medial collateral ligament (MCL) is intact and the lateral collateral ligament (LCL) is disrupted, or in supination if the LCL is intact but the MCL disrupted. Surgical repair of the LCL and MCL may be required only if the elbow does not have a stable arc at the time of reduction. If the elbow remains unstable after repair, then application of a hinged external fixator may be considered.
45
45
Question 5High Yield
A 61-year-old right-hand dominant woman falls down the stairs, resulting in a left anteroinferior shoulder dislocation and non- comminuted greater tuberosity fracture. A closed glenohumeral reduction with intravenous sedation is performed in the emergency department. After reduction, the greater tuberosity fragment remains displaced by 2 mm. What is the most appropriate treatment?
Explanation
Greater tuberosity fractures and rotator cuff tears associated with a traumatic dislocation are more commonly seen in women >60 years. Greater tuberosity fractures that are displaced <5 mm in the general population and <3 mm in laborers and professional athletes can be treated successfully without surgery. Early passive range of motion is important to avoid stiffness.
3
3
Question 6High Yield
..A 25-year-old man is planning to have an elbow contracture release. His elbow range of motion is 40 degrees to 90 degrees of flexion. He has no heterotopic ossification. His ring and small fingers become numb as his elbow approaches his flexion endpoint. There is no evidence of instability of the ulna-humeral or radioulnar joints. To achieve the best possible outcome, the surgeon should
Explanation
- decompress the ulnar nerve.
Question 7High Yield
Optimal treatment for a symptomatic ganglion is:
Explanation
Surgical excision of a symptomatic ganglion, with removal of the entire ganglion stalk and a portion of the joint capsule at its base, reliably relieves pain and has a low recurrence rate (approximately 5%). C losed rupture, while potentially effective, has a recurrence rate of approximately 50%. Ganglions are prone to recur after aspiration, although 3 serial aspirations of a ganglion have been shown to reduce the recurrence rate to about 15%. The addition of corticosteroids to aspiration treatment has not been shown to provide any additional benefit. While observation of painless ganglions is certainly acceptable treatment given their benign prognosis, it is not considered the optimal course for a symptomatic lesion.
Question 8High Yield
Figure 1 is the radiograph of a 13-year-old right-hand dominant male baseball pitcher who presents with new onset right shoulder pain. Over the past month, he has participated in several tournaments. He was unable to complete his most recent game secondary to continued pain while throwing. Examination reveals a healthy, adolescent male in no apparent distress. Range-of-motion examination of the bilateral shoulders is symmetric with mild pain at the end points of motion. He reports pain on palpation over the lateral aspect of his deltoid. What pathologic process is most likely responsible for this patient's pain?
Explanation
48
The clinical vignette describes a 13-year-old boy with Little Leaguers’ shoulder. This is an injury to the proximal humerus growth plate specifically involving the hypertrophic zone of the physis. This condition is considered a Salter-Harris 1 injury to the proximal humerus physis and most commonly affects male throwing athletes ages 11 to 16. The proximal humerus growth plate closes between the ages of 18 to 21. The mechanism of injury involves microtrauma to the growth plate from exposure to excessive rotational torque and distraction forces during the late cocking; early acceleration and deceleration phases of throwing, respectively. High pitch counts have been implicated as risk factors for injury. The diagnosis is frequently made clinically; however, radiographs of the shoulder may reveal widening of the proximal humeral physis in comparison with the contralateral side. Treatment includes cessation of throwing for 3 to 6 months. The patient should be asymptomatic prior to return to a throwing program. Physical therapy and a program of guided return to throwing that enforces proper pitching mechanics can be helpful during a return to play. Following established pitch counts and allowing for appropriate rest before throwing can help to prevent future recurrence.
The clinical vignette describes a 13-year-old boy with Little Leaguers’ shoulder. This is an injury to the proximal humerus growth plate specifically involving the hypertrophic zone of the physis. This condition is considered a Salter-Harris 1 injury to the proximal humerus physis and most commonly affects male throwing athletes ages 11 to 16. The proximal humerus growth plate closes between the ages of 18 to 21. The mechanism of injury involves microtrauma to the growth plate from exposure to excessive rotational torque and distraction forces during the late cocking; early acceleration and deceleration phases of throwing, respectively. High pitch counts have been implicated as risk factors for injury. The diagnosis is frequently made clinically; however, radiographs of the shoulder may reveal widening of the proximal humeral physis in comparison with the contralateral side. Treatment includes cessation of throwing for 3 to 6 months. The patient should be asymptomatic prior to return to a throwing program. Physical therapy and a program of guided return to throwing that enforces proper pitching mechanics can be helpful during a return to play. Following established pitch counts and allowing for appropriate rest before throwing can help to prevent future recurrence.
Question 9High Yield
According to the MRI scan shown in Figure 1, which pathologic finding is expected to be encountered during arthroscopy?
Explanation
images show a flap tear of the medial meniscus (Figure 2), anterior cruciate ligament tear (Figure 3), and a full thickness articular cartilage defect (Figure 5). Other less likely causes of a double PCL sign include intermeniscal ligament, meniscofemoral ligaments, loose bodies, osteophytes, and fracture fragments.
13
13
Question 10High Yield
An 18-year-old man was in a motor vehicle accident and sustained a closed head injury, right displaced scapular body and glenoid fractures, a right proximal humeral fracture, fractures of ribs one through three, facial fractures, and bilateral pubic rami fractures with minimal displacement. He has a systolic blood pressure of 80/40 mm Hg despite fluid resuscitation. A radiograph is shown in Figure 17. Spiral CT does not identify any thoracic or abdominal injuries. What is the next most appropriate step in management?
Explanation
The patient has sustained high-energy upper extremity and chest injuries. He continues to remain hemodynamically unstable with no obvious thoracic or abdominal injury responsible for bleeding. The pelvic fracture is unlikely to be causing significant bleeding. A scapulothoracic dissociation and possible disruption of one of the great vessels of the upper extremity should be considered. Evaluation of peripheral pulses or blood pressure indices bilaterally in the upper extremities is a simple way to evaluate the need for further work-up. If there is any discrepancy or further concern, angiography of the involved extremity is necessary.
REFERENCES: Althausen PL, Lee MA, Finkemeier CG: Scapulothoracic dissociation: Diagnosis and treatment. Clin Orthop 2003;416:237-244.
Witz M, Korzets Z, Lehmann J: Traumatic scapulothoracic dissociation. J Cardiovasc Surg 2000;41:927-929.
REFERENCES: Althausen PL, Lee MA, Finkemeier CG: Scapulothoracic dissociation: Diagnosis and treatment. Clin Orthop 2003;416:237-244.
Witz M, Korzets Z, Lehmann J: Traumatic scapulothoracic dissociation. J Cardiovasc Surg 2000;41:927-929.
Question 11High Yield
Which of the following findings is likely to be pathologic in a thin, well-conditioned endurance athlete?
Explanation
Left ventricular hypertrophy by voltage is a nonspecific diagnosis, especially in athletes with an asthenic body habitus. High vagal tone in endurance athletes may result in first degree or even type I second degree (ie, Wenckebach) AV block in endurance athletes. High vagal tone results in resting sinus bradycardia in many trained athletes. A I-II/IV systolic ejection murmur is occasionally found in healthy athletes; however, when the murmur increases in intensity with maneuvers that decrease ventricular filling, such as standing or the Valsalva maneuver, dynamic obstruction that is the result of hypertrophic obstructive cardiomyopathy should be suspected. Nonspecific STT wave changes in the lateral leads on ECG are not uncommon in highly trained athletes; thus, they are nonspecific for ischemic heart disease.
REFERENCES: Pelliccia A, Maron BJ, Culasso F, DiPaolo FM, et al: Clinical significance of abnormal electrocardiographic patterns in trained athletes. Circulation 2000;102:278-284.
Maron BJ, Thompson PD, Puffer JC, McGrew CA: Cardiovascular preparticipation screening of competitive athletes: A statement for health professionals from the Sudden Death Committee (Clinical Cardiology) and Congenital Cardiac Defects Committee (Cardiovascular Disease in the Young), American Heart Association. Circulation 1996;94:850-856.
REFERENCES: Pelliccia A, Maron BJ, Culasso F, DiPaolo FM, et al: Clinical significance of abnormal electrocardiographic patterns in trained athletes. Circulation 2000;102:278-284.
Maron BJ, Thompson PD, Puffer JC, McGrew CA: Cardiovascular preparticipation screening of competitive athletes: A statement for health professionals from the Sudden Death Committee (Clinical Cardiology) and Congenital Cardiac Defects Committee (Cardiovascular Disease in the Young), American Heart Association. Circulation 1996;94:850-856.
Question 12High Yield
During revision total knee arthroplasty (TKA), there is significant laxity in 90° of flexion and 10° short of full extension. Correcting the gap imbalance is best achieved by
Explanation
When performing revision TKA, the management of gap imbalance and joint line is of critical importance. The flexion gap is generally driven by femoral component size; increasing femoral component size by tightening the flexion gap and downsizing the femoral component size increases the flexion gap. Resecting more distal femur will open up the extension gap; augmenting the femur distally will tighten up the extension gap. Resecting more tibia affects both flexion and extension gaps equally.
Question 13High Yield
Which of the following symptoms are most commonly associated with piriformis syndrome?
Explanation
Piriformis syndrome is best characterized by localized posterior hip pain and radicular symptoms in the sciatic distribution because of compression of the piriformis muscle on the sciatic nerve. Weakness in hip extension is not a characteristic finding, nor is pain with hip abduction or flexion. Hypesthesia of the lateral thigh would be more characteristic of a lesion of the lateral femoral cutaneous nerve. Radiating medial thigh pain would suggest hip joint pathology or upper lumbar nerve root irritation. Weakness in internal rotation is not a characteristic feature, and hypesthesia of the perineum would suggest possible involvement of the pudendal nerve.
REFERENCES: Byrd JWT: Thigh, hip, and pelvis, in Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy, ed 2. Philadelphia, PA, WB Saunders, 2002,
pp 114-139.
Levin SM: Piriformis syndrome. Orthopedics 2000;23:183-184.
REFERENCES: Byrd JWT: Thigh, hip, and pelvis, in Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy, ed 2. Philadelphia, PA, WB Saunders, 2002,
pp 114-139.
Levin SM: Piriformis syndrome. Orthopedics 2000;23:183-184.
Question 14High Yield
When compared to patients who undergo endoprosthetic reconstruction, patients who undergo rotationplasty are more likely to
Explanation
Debate exists regarding the prognostic significance of pathologic fractures with respect to both overall survival and local recurrence, with most older studies indicating that fracture increases these risks and more recent research suggesting that risks are not increased as much as previously believed. This patient’s fracture is minimally displaced and amenable to cast immobilization. Healing of osteosarcoma pathologic femur fractures treated with casting and neoadjuvant chemotherapy has been well documented. Acute amputation was historically the standard treatment and remains an option for markedly displaced fractures with severe contamination. However, this scenario remains amenable to limb salvage. Spanning external fixation is suboptimal because the femoral canal will be breached proximally, creating a potential site of infection or a fracture stress riser if a stemmed endoprosthesis is to be used. Immediate limb-sparing resection is not advised because there will be higher risk for contamination from the acute hematoma, which will likely resolve with casting and chemotherapy.
The MRI series reveals extensive contamination of the knee joint by fracture hematoma. Such contamination precludes the more commonly performed intra-articular resection. Extra-articular resection, although technically feasible, is more difficult and frequently less functional than intra-articular resection. The MRI reveals that the sciatic nerve and its branches are distant from the fracture hematoma and tumor. Femoral fixation is not challenging in this patient because the tumor is quite distal. Soft-tissue coverage should be adequate because no subcutaneous contamination is shown on MRI.
Rotationplasty is a reasonable alternative to extra-articular resection and amputation among adults. Only the major nerves need to be free of tumor because even contaminated vessels can be resected with subsequent anastomosis after rotation and shortening. Vascular compromise is the most common cause of early limb loss after rotationplasty because both anastomosed and rotated vessels are at risk for thrombosis. Local recurrence is typically a later complication. Wound infections and fixation failures may occur but rarely result in acute limb loss.
Patients who undergo rotationplasty function at a level comparable to those who undergo below-knee amputation. High-impact activities are not discouraged for patients who undergo rotationplasty because there are no concerns about prosthetic wear or loosening. Psychosocial and occupational impairment are not worse among patients who undergo rotationplasty vs other forms of reconstruction. Revision surgery is less common with rotationplasty because there are fewer late infections, and concerns about prosthetic wear and loosening are eliminated.
RECOMMENDED READINGS
70. Salunke AA, Chen Y, Tan JH, Chen X, Khin LW, Puhaindran ME. Does a pathological fracture affect the prognosis in patients with osteosarcoma of the extremities? a systematic review and meta-analysis.
Bone Joint J. 2014 Oct;96-B(10):1396-403. doi: 10.1302/0301-620X.96B10.34370. Review. PubMed
[PMID: 25274928 ](http://www.ncbi.nlm.nih.gov/pubmed/25274928)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25274928)
71. [Scully SP, Ghert MA, Zurakowski D, Thompson RC, Gebhardt MC. Pathologic fracture in osteosarcoma : prognostic importance and treatment implications. J Bone Joint Surg Am. 2002 Jan;84-A(1):49-57. Erratum in: J Bone Joint Surg Am 2002 Apr;84-A(4):622. ](http://www.ncbi.nlm.nih.gov/pubmed/11792779)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11792779)
72. [Zwolak P, Kühnel SP, Fuchs B. Extraarticular knee resection for sarcomas with preservation of the extensor mechanism: surgical technique and review of cases. Clin Orthop Relat Res. 2011 Jan;469(1):251-6. doi: 10.1007/s11999-010-1359-8. Epub 2010 Apr 24. ](http://www.ncbi.nlm.nih.gov/pubmed/20419485)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20419485)
73. Sawamura C, Hornicek FJ, Gebhardt MC. Complications and risk factors for failure of rotationplasty: review of 25 patients. Clin Orthop Relat Res. 2008 Jun;466(6):1302-8. doi: 10.1007/s11999-008-0231-
[6/. Epub 2008 Apr 11. PubMed PMID: 18404295.](http://www.ncbi.nlm.nih.gov/pubmed/18404295)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18404295)
74. [Agarwal M, Puri A, Anchan C, Shah M, Jambhekar N. Rotationplasty for bone tumors: is there still a role? Clin Orthop Relat Res. 2007 Jun;459:76-81. PubMed PMID: 17414168.](http://www.ncbi.nlm.nih.gov/pubmed/17414168)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/17414168)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17414168)
75. [Teall T, Barrera M, Barr R, Silva M, Greenberg M. Psychological resilience in adolescent and young adult survivors of lower extremity bone tumors. Pediatr Blood Cancer. 2013 Jul;60(7):1223-30. doi: 10.1002/pbc.24441. Epub 2012 Dec 19. PubMed PMID: 23255460.](http://www.ncbi.nlm.nih.gov/pubmed/23255460)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23255460)
76. [Hillmann A, Weist R, Fromme A, Völker K, Rosenbaum D. Sports activities and endurance capacity of bone tumor patients after rotationplasty. Arch Phys Med Rehabil. 2007 Jul;88(7):885-90. PubMed PMID: 17601469. ](http://www.ncbi.nlm.nih.gov/pubmed/17601469)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17601469)
The MRI series reveals extensive contamination of the knee joint by fracture hematoma. Such contamination precludes the more commonly performed intra-articular resection. Extra-articular resection, although technically feasible, is more difficult and frequently less functional than intra-articular resection. The MRI reveals that the sciatic nerve and its branches are distant from the fracture hematoma and tumor. Femoral fixation is not challenging in this patient because the tumor is quite distal. Soft-tissue coverage should be adequate because no subcutaneous contamination is shown on MRI.
Rotationplasty is a reasonable alternative to extra-articular resection and amputation among adults. Only the major nerves need to be free of tumor because even contaminated vessels can be resected with subsequent anastomosis after rotation and shortening. Vascular compromise is the most common cause of early limb loss after rotationplasty because both anastomosed and rotated vessels are at risk for thrombosis. Local recurrence is typically a later complication. Wound infections and fixation failures may occur but rarely result in acute limb loss.
Patients who undergo rotationplasty function at a level comparable to those who undergo below-knee amputation. High-impact activities are not discouraged for patients who undergo rotationplasty because there are no concerns about prosthetic wear or loosening. Psychosocial and occupational impairment are not worse among patients who undergo rotationplasty vs other forms of reconstruction. Revision surgery is less common with rotationplasty because there are fewer late infections, and concerns about prosthetic wear and loosening are eliminated.
RECOMMENDED READINGS
70. Salunke AA, Chen Y, Tan JH, Chen X, Khin LW, Puhaindran ME. Does a pathological fracture affect the prognosis in patients with osteosarcoma of the extremities? a systematic review and meta-analysis.
Bone Joint J. 2014 Oct;96-B(10):1396-403. doi: 10.1302/0301-620X.96B10.34370. Review. PubMed
[PMID: 25274928 ](http://www.ncbi.nlm.nih.gov/pubmed/25274928)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25274928)
71. [Scully SP, Ghert MA, Zurakowski D, Thompson RC, Gebhardt MC. Pathologic fracture in osteosarcoma : prognostic importance and treatment implications. J Bone Joint Surg Am. 2002 Jan;84-A(1):49-57. Erratum in: J Bone Joint Surg Am 2002 Apr;84-A(4):622. ](http://www.ncbi.nlm.nih.gov/pubmed/11792779)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11792779)
72. [Zwolak P, Kühnel SP, Fuchs B. Extraarticular knee resection for sarcomas with preservation of the extensor mechanism: surgical technique and review of cases. Clin Orthop Relat Res. 2011 Jan;469(1):251-6. doi: 10.1007/s11999-010-1359-8. Epub 2010 Apr 24. ](http://www.ncbi.nlm.nih.gov/pubmed/20419485)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20419485)
73. Sawamura C, Hornicek FJ, Gebhardt MC. Complications and risk factors for failure of rotationplasty: review of 25 patients. Clin Orthop Relat Res. 2008 Jun;466(6):1302-8. doi: 10.1007/s11999-008-0231-
[6/. Epub 2008 Apr 11. PubMed PMID: 18404295.](http://www.ncbi.nlm.nih.gov/pubmed/18404295)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18404295)
74. [Agarwal M, Puri A, Anchan C, Shah M, Jambhekar N. Rotationplasty for bone tumors: is there still a role? Clin Orthop Relat Res. 2007 Jun;459:76-81. PubMed PMID: 17414168.](http://www.ncbi.nlm.nih.gov/pubmed/17414168)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/17414168)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17414168)
75. [Teall T, Barrera M, Barr R, Silva M, Greenberg M. Psychological resilience in adolescent and young adult survivors of lower extremity bone tumors. Pediatr Blood Cancer. 2013 Jul;60(7):1223-30. doi: 10.1002/pbc.24441. Epub 2012 Dec 19. PubMed PMID: 23255460.](http://www.ncbi.nlm.nih.gov/pubmed/23255460)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23255460)
76. [Hillmann A, Weist R, Fromme A, Völker K, Rosenbaum D. Sports activities and endurance capacity of bone tumor patients after rotationplasty. Arch Phys Med Rehabil. 2007 Jul;88(7):885-90. PubMed PMID: 17601469. ](http://www.ncbi.nlm.nih.gov/pubmed/17601469)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17601469)
Question 15High Yield
Figures 1 through 3 are the radiographs of a 68-year-old woman with progressive shoulder pain. She has failed all nonoperative modalities and now presents with refractory shoulder pain at night and with any attempted shoulder motion. She lacks the ability to forward elevate or abduct her shoulder >45°. What is the best treatment option?
37
37
Explanation
The patient has cuff tear arthropathy associated with significant pain and poor function. At age 68, a reverse total shoulder arthroplasty is the most reliable option to address her complaints. Arthroscopic debridement with superior capsular reconstruction would be a consideration in a younger patient with an irreparable posterosuperior rotator cuff tear, little to no glenohumeral arthritis, and little to no humeral head elevation. Total shoulder arthroplasty would have a high rate of glenoid component failure and limited function, regardless of the type of glenoid component utilized. Clinical outcomes of reverse total shoulder arthroplasty are superior to hemiarthroplasty in the setting of cuff tear arthropathy.
38
38
Question 16High Yield
Figures 31a and 31b are the radiographs of a 5-year-old boy with an elbow injury.

Explanation
Figure 26 shows lucent areas of both femoral condyles. This may represent a variation of ossification, in which case this boy’s knee pain is coincidental. Another possibility is atypical osteochondritis dissecans. An MRI will distinguish between the 2 entities and will guide treatment.
Figures 27a and 27b show healing rib and distal tibia fractures. These fractures likely are attributable to child abuse. A plain radiographic skeletal survey is sufficient for orthopaedic needs.
A triplane fracture of the distal tibia is revealed in Figure 28. A CT scan will quantify displacement and identify fracture fragments for planning of screw trajectories if open reduction and internal fixation is indicated (displacement > 2 mm).
In Figure 29, the linear lucency of the capitellum indicates an early osteochondritis dissecans. An MRI will allow staging of the lesion.
Figure 30 shows that the left radius and ulna do not align with the humerus; this is the likely result of a transphyseal fracture of the distal humerus. An arthrogram will outline the unossified distal humerus and allow for reduction. For an unstable neonate, this likely can be performed in the NICU.
Figures 31a and 31b reveal a widely displaced lateral condyle fracture for which open reduction and internal fixation is required. No advanced imaging is necessary.
Figure 32
Figures 27a and 27b show healing rib and distal tibia fractures. These fractures likely are attributable to child abuse. A plain radiographic skeletal survey is sufficient for orthopaedic needs.
A triplane fracture of the distal tibia is revealed in Figure 28. A CT scan will quantify displacement and identify fracture fragments for planning of screw trajectories if open reduction and internal fixation is indicated (displacement > 2 mm).
In Figure 29, the linear lucency of the capitellum indicates an early osteochondritis dissecans. An MRI will allow staging of the lesion.
Figure 30 shows that the left radius and ulna do not align with the humerus; this is the likely result of a transphyseal fracture of the distal humerus. An arthrogram will outline the unossified distal humerus and allow for reduction. For an unstable neonate, this likely can be performed in the NICU.
Figures 31a and 31b reveal a widely displaced lateral condyle fracture for which open reduction and internal fixation is required. No advanced imaging is necessary.
Figure 32
Question 17High Yield
A 13-year-old boy has a mild deformity of the left sternoclavicular joint after being involved in a rollover accident while riding an all-terrain vehicle. Examination in the emergency department reveals that he is hemodynamically stable, and his neurovascular examination is normal. The CT scan shown in Figure 22 was obtained because radiographs were inconclusive. Management should consist of
Explanation
The CT scan reveals a completely displaced physeal fracture of the medial clavicle with marked posterior displacement of the distal fragment. This fracture pattern is associated with potential injury to the vascular structures of the mediastinum. Reduction should be performed for this fracture and generally can be done closed with shoulder retraction and upward pull on the clavicle with a towel clip. Once reduced, the fracture is relatively stable and typically will heal in good position. Reduction should be performed in the operating room in the event that a vascular injury is detected once compression is removed from the clavicle. Open reduction may be necessary if closed reduction is not possible; however, pinning or ligament reconstruction usually is not necessary.
REFERENCES: Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, p 581.
Wirth MA, Rockwood CA Jr: Acute and chronic traumatic injuries of the sternoclavicular joint. J Am Acad Orthop Surg 1996;4:268-278.
REFERENCES: Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, p 581.
Wirth MA, Rockwood CA Jr: Acute and chronic traumatic injuries of the sternoclavicular joint. J Am Acad Orthop Surg 1996;4:268-278.
Question 18High Yield
If aspiration findings are negative or equivocal, the diagnosis can be established with
Explanation
- arthroscopy._
Question 19High Yield
A 25-year-old man sustains a left brachial plexus injury from a fall while rock climbing. Examination reveals poor intrinsic function of the hand, ptosis, and miosis. He is able to abduct and forward flex his shoulder with full strength. This combination of physical findings is most suggestive of what pattern of nerve injury?
Explanation
A preganglionic lesion occurs proximal to the spinal foramen, whereas a postganglionic lesion occurs distal to the spinal foramen in the root, trunk, division, cord, or branches of the brachial plexus. The Horner sign, which is characterized by miosis, ptosis, anhydrosis, and enophthalmos, results from an injury to the sympathetic ganglion, which lies in close proximity to the T1 root level. The presence of a Horner sign is highly suggestive of a T1 preganglionic injury. Other physical examination indicators of a preganglionic injury include atrophy of the parascapular muscles (injury to the dorsal rami of the cervical spinal nerve roots), winged scapula (injury to the long thoracic nerve) and hemidiaphragmatic paralysis (phrenic nerve injury). The lack of intrinsic hand function in this patient is also suggestive of an injury at the level of C8-T1. Preservation of shoulder abduction and forward flexion would not typically be seen with an injury to the C5-C6 roots or the upper trunk.
Question 20High Yield
All of the following developmental anomalies are associated with ulnar club hand except:
Explanation
Atrial septal defects are developmental abnormalities present in patients with radial club hand or Holt-Oram syndrome.
Question 21High Yield
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient
is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. Radiographs of the player’s right ankle confirm there are no fractures. With a lateral talar tilt test result of 19°, which additional structure is most likely damaged?
is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. Radiographs of the player’s right ankle confirm there are no fractures. With a lateral talar tilt test result of 19°, which additional structure is most likely damaged?
Explanation
The anterior drawer test is performed with the ankle in 10° of plantar flexion, which results in the greatest amount of translation. The test investigates the integrity of the anterior talofibular ligament with a key distance of translation being 8 to 10 mm. While the patient is sitting and has her knees flexed over the edge of a table or bench, the physician uses one hand to stabilize the distal leg and with the other hand applies an anterior force to the heel in an attempt to gap the talus anteriorly from under the tibia. The
anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization _and a guided rehabilitation program that emphasizes proprioceptive stability._
anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization _and a guided rehabilitation program that emphasizes proprioceptive stability._
Question 22High Yield
Figure 1 is the radiograph of a 50-year old woman with lateral-sided left knee pain. She noticed the pain over the last few months and has had no new injury. She had a microfracture performed of her lateral femoral condyle 5 years ago. What is the likely cause of the finding noted on her radiograph?
---
---


Explanation
The radiograph reveals bony overgrowth of the microfracture site on the lateral femoral condyle. This occurs from violation of the subchondral plate during aggressive removal of the calcified cartilage layer during the microfracture. It is important during a microfracture to attempt to have a contained lesion and remove the calcified cartilage layer down to the subchondral plate, but avoid aggressively penetrating the _plate._
Question 23High Yield
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. If the patient chooses surgical reconstruction, he should be advised that, when compared with a transtibial technique, the tibial inlay technique has been shown to provide
---
---

Explanation
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, one major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading. The scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be
appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for _vascular injury._
appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for _vascular injury._
Question 24High Yield
Meleneyâs infection is caused by:
Explanation
Aerobic hemolytic staphylococci and microaerophyllic non-hemolytic streptococci synergistically act to produce Meleneyâs infection. Meleney's infection is a gangrenous infection that often results after a small injury. The infection is characterized by significant, rapid swelling with gangrenous changes.
Question 25High Yield
A 5-year-old girl sustained a nondisplaced fracture of the proximal tibial metaphysis, which was treated with a long leg cast and which healed uneventfully. Clinical examination and the image seen in Figure 1 reveals a deformity at 1 year postinjury. The most appropriate management at this time would be

Explanation
■
Development of proximal tibial valgus is an uncommon, but well-documented, complication of proximal tibial metaphyseal fractures in children. There are multiple theories as to the origin, but the exact etiolgy is unknown. Management with a guide-growth procedure is rarely required, because most patients ultimately achieve spontaneous correction.
■
Development of proximal tibial valgus is an uncommon, but well-documented, complication of proximal tibial metaphyseal fractures in children. There are multiple theories as to the origin, but the exact etiolgy is unknown. Management with a guide-growth procedure is rarely required, because most patients ultimately achieve spontaneous correction.
Question 26High Yield
A 50-year-old electrician who is right-hand dominant has had right shoulder pain and stiffness after sustaining an electric shock 2 months ago. An AP radiograph obtained at the time of injury was considered negative, and the patient was diagnosed with a shoulder sprain. The patient now reports continued shoulder pain and restricted motion. AP and axillary radiographs and a CT scan are shown in Figures 41a through 41c. Management should consist of
Explanation
Open reduction and transfer of the subscapularis and lesser tuberosity into the humeral head defect is the treatment of choice for chronic posterior dislocations in which the articular defect consists of 20% to 40% of the articular surfaces. Closed reduction can be used if the dislocation is recognized early and the articular defect is less than 20% of the articular surface. Humeral arthroplasty is reserved for patients with an articular defect that is greater than 45% to 50% of the head.
REFERENCES: Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Checchia SL, Santos PD, Miyazaki AN: Surgical treatment of acute and chronic posterior fracture-dislocation of the shoulder. J Shoulder Elbow Surg 1998;7:53-65.
REFERENCES: Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Checchia SL, Santos PD, Miyazaki AN: Surgical treatment of acute and chronic posterior fracture-dislocation of the shoulder. J Shoulder Elbow Surg 1998;7:53-65.
Question 27High Yield
What is the chief mechanism of action of parathyroid hormone (PTH) in the treatment of patients with osteoporosis?
Explanation
■
Recombinant human PTH benefits patients with osteoporosis by stimulating osteoblastic bone formation and reducing osteoblastic apoptosis. Treatment reduces vertebral fractures by 65%. PTH analogs act similarly and reduce vertebral fractures by 47%. Bisphosphonates reduce the resorptive activity of osteoclasts and cause a dissociation of bone formation and resorption that favors bone formation and reduce vertebral fractures by 50% to 70%. Selective estrogen receptor modulators inhibit bone resorption and reduce vertebral fractures by 35%. Humanized monoclonal antibodies inhibit osteoclast formation and reduce vertebral fractures by 68%.
Recombinant human PTH benefits patients with osteoporosis by stimulating osteoblastic bone formation and reducing osteoblastic apoptosis. Treatment reduces vertebral fractures by 65%. PTH analogs act similarly and reduce vertebral fractures by 47%. Bisphosphonates reduce the resorptive activity of osteoclasts and cause a dissociation of bone formation and resorption that favors bone formation and reduce vertebral fractures by 50% to 70%. Selective estrogen receptor modulators inhibit bone resorption and reduce vertebral fractures by 35%. Humanized monoclonal antibodies inhibit osteoclast formation and reduce vertebral fractures by 68%.
Question 28High Yield
Slide 1
A 43-year-old construction worker sustained a work-related injury to his foot 7 months ago. He was initially treated with cast immobilization and limited weight bearing. He has lateral foot pain and inability to walk comfortably. He has limited walking endurance. Upon examination, pain is present laterally along the course of the peroneal tendons, and no motion of the subtalar joint is present. The recommendation is:
A 43-year-old construction worker sustained a work-related injury to his foot 7 months ago. He was initially treated with cast immobilization and limited weight bearing. He has lateral foot pain and inability to walk comfortably. He has limited walking endurance. Upon examination, pain is present laterally along the course of the peroneal tendons, and no motion of the subtalar joint is present. The recommendation is:
Explanation
A worker who sustains a calcaneus fracture must be returned to the work force as soon as possible. Although these alternatives for treatment may be considered in the patient with limited activity and low demands, the longer the time from injury to salvage surgery with arthrodesis, the less likely it is that the injured worker will ever return to gainful employment. Therefore, subtalar arthrodesis should be performed.
Question 29High Yield
When using antibiotic-laden polymethylmethacrylate (PMMA) to treat osteomyelitis, vancomycin and tobramycin are heat stable and have not produced systemic toxicity at various levels. Which dose is closest to the highest recommended concentration for each drug?

Explanation
Vancomycin and tobramycin do not produce systemic toxicity in doses as high as 10.5 grams of vancomycin and 12.5 grams of tobramycin per 40 mg of PMMA.
RECOMMENDED READINGS
10. [Hake ME, Young H, Hak DJ, Stahel PF, Hammerberg EM, Mauffrey C. Local antibiotic therapy strategies in orthopaedic trauma: Practical tips and tricks and review of the literature. Injury. 2015 Aug;46(8):1447-56. doi: 10.1016/j.injury.2015.05.008. Epub 2015 May 14. Review. PubMed PMID: 26007616. ](http://www.ncbi.nlm.nih.gov/pubmed/26007616)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26007616)
11. [Springer BD, Lee GC, Osmon D, Haidukewych GJ, Hanssen AD, Jacofsky DJ. Systemic safety of high-dose antibiotic-loaded cement spacers after resection of an infected total knee arthroplasty. Clin Orthop Relat Res. 2004 Oct;(427):47-51. PubMed PMID: 15552135. ](http://www.ncbi.nlm.nih.gov/pubmed/15552135)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15552135)
CLINICAL SITUATION FOR QUESTIONS 84 THROUGH 86
Figure 84 is the noncontrast MR image obtained at 2 weeks postinjury for a 52-year-old man who was injured after falling from a ladder. His arm is caught in an abducted, externally rotated
position. There is no sense of dislocation. Initial radiograph findings are normal. The radiologic review reads “Probable superior labral anterior to posterior (SLAP) tear.”
RECOMMENDED READINGS
10. [Hake ME, Young H, Hak DJ, Stahel PF, Hammerberg EM, Mauffrey C. Local antibiotic therapy strategies in orthopaedic trauma: Practical tips and tricks and review of the literature. Injury. 2015 Aug;46(8):1447-56. doi: 10.1016/j.injury.2015.05.008. Epub 2015 May 14. Review. PubMed PMID: 26007616. ](http://www.ncbi.nlm.nih.gov/pubmed/26007616)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26007616)
11. [Springer BD, Lee GC, Osmon D, Haidukewych GJ, Hanssen AD, Jacofsky DJ. Systemic safety of high-dose antibiotic-loaded cement spacers after resection of an infected total knee arthroplasty. Clin Orthop Relat Res. 2004 Oct;(427):47-51. PubMed PMID: 15552135. ](http://www.ncbi.nlm.nih.gov/pubmed/15552135)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15552135)
CLINICAL SITUATION FOR QUESTIONS 84 THROUGH 86
Figure 84 is the noncontrast MR image obtained at 2 weeks postinjury for a 52-year-old man who was injured after falling from a ladder. His arm is caught in an abducted, externally rotated
position. There is no sense of dislocation. Initial radiograph findings are normal. The radiologic review reads “Probable superior labral anterior to posterior (SLAP) tear.”
Question 30High Yield
A 45-year-old distance runner has a hyaluronic acid injection to his knee because of degenerative arthritis. He immediately develops a severe rash and a systemic hypersensitivity reaction. This patient most likely is also allergic to which of the following?
Explanation
DISCUSSION: Preparations of hyaluronic acid can be divided into low and high molecular weight compounds. Contraindications to intra-articular hyaluronic acid include joint or skin infection, overlying skin disease, and allergies to chicken or egg products if using a preparation derived from rooster comb.
REFERENCES: Gloyscen DN, Gillespie MJ, Schenek RC: The effects of medication in sports injuries, in DeLee JC, Drez D Jr, Miller MD (eds): Orthopedic Sports Medicine: Principles and Practice, ed 2.
Philadelphia, PA, WB Saunders, 2003, vol 1, pp 121-124.
Schenck RC Jr: New approaches to the treatment of osteoarthritis: Oral glucosamine and chondroitin sulfate. Instr Course Lect 2000;49:491-494.
DISCUSSION: Preparations of hyaluronic acid can be divided into low and high molecular weight compounds. Contraindications to intra-articular hyaluronic acid include joint or skin infection, overlying skin disease, and allergies to chicken or egg products if using a preparation derived from rooster comb.
REFERENCES: Gloyscen DN, Gillespie MJ, Schenek RC: The effects of medication in sports injuries, in DeLee JC, Drez D Jr, Miller MD (eds): Orthopedic Sports Medicine: Principles and Practice, ed 2.
Philadelphia, PA, WB Saunders, 2003, vol 1, pp 121-124.
Schenck RC Jr: New approaches to the treatment of osteoarthritis: Oral glucosamine and chondroitin sulfate. Instr Course Lect 2000;49:491-494.
Question 31High Yield
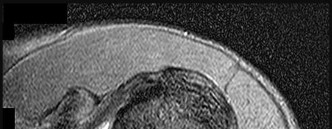
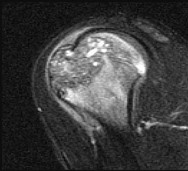
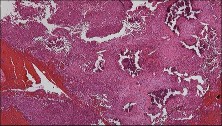
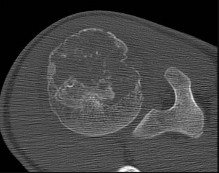
Figures 48a through 48e are the MR image, radiograph, CT scan, and biopsy specimens of a 14-year-old boy with right shoulder pain without antecedent trauma. What is the most likely diagnosis?


Explanation
Imaging reveals a destructive mineralized lesion of the epiphysis and metaphysis in a skeletally immature patient. Epiphyseal lesions include chondroblastoma in skeletally immature patients and giant-cell tumors in skeletally mature patients. The histology confirms the diagnosis with the presence of multinucleated giant cells, “chicken-wire” calcifications, and chondroid islands. Chondrosarcoma would look histologically more aggressive than this and is unusual in children. Unicameral bone cysts do not have mineralization and are typically confined to the metaphysis radiologically. Eosinophilic granuloma can mimic many different lesions radiographically and can occasionally be found in the epiphysis of children, but the histology does not demonstrate classic Langerhans cells.
RECOMMENDED READINGS
34. Wold LE, Unni KK, Sim FH, Sundaram M, Adler C-P, eds. _Atlas of Orthopedic Pathology_. 2nd edition. Philadelphia PA: Saunders; 2003:232:237.
35. [De Mattos CB, Angsanuntsukh C, Arkader A, Dormans JP. Chondroblastoma and chondromyxoid fibroma. J Am Acad Orthop Surg. 2013 Apr;21(4):225-33. doi: 10.5435/JAAOS-21-04-225. Review. PubMed PMID: 23545728.](http://www.ncbi.nlm.nih.gov/pubmed/23545728)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23545728)
CLINICAL SITUATION FOR QUESTIONS 49 AND 50
Figure 49 is the radiograph of a 22-year-old woman with pain and snapping about the knee. Her husband does not have this condition.
RECOMMENDED READINGS
34. Wold LE, Unni KK, Sim FH, Sundaram M, Adler C-P, eds. _Atlas of Orthopedic Pathology_. 2nd edition. Philadelphia PA: Saunders; 2003:232:237.
35. [De Mattos CB, Angsanuntsukh C, Arkader A, Dormans JP. Chondroblastoma and chondromyxoid fibroma. J Am Acad Orthop Surg. 2013 Apr;21(4):225-33. doi: 10.5435/JAAOS-21-04-225. Review. PubMed PMID: 23545728.](http://www.ncbi.nlm.nih.gov/pubmed/23545728)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23545728)
CLINICAL SITUATION FOR QUESTIONS 49 AND 50
Figure 49 is the radiograph of a 22-year-old woman with pain and snapping about the knee. Her husband does not have this condition.
Question 32High Yield
A 31-year-old male sustains an ipsilateral displaced transverse acetabular fracture, pubic rami fractures, and a sacroiliac joint dislocation. What structure should be reduced and stabilized first?
Explanation
In an ipsilateral unstable pelvic ring and acetabular fractures, the pelvic ring injury must be initially stabilized in order to reduce the acetabular fracture to a stable base.
The referenced article by Matta reviewed 259 patients with acetabular fractures treated within 21 days of injury and found that the hip joint can be preserved and post-traumatic osteoarthrosis can be avoided if an anatomical reduction is achieved.
The referenced article by Matta reviewed 259 patients with acetabular fractures treated within 21 days of injury and found that the hip joint can be preserved and post-traumatic osteoarthrosis can be avoided if an anatomical reduction is achieved.
Question 33High Yield
When elevating the arm, the ratio of scapulothoracic to glenohumeral motion over the total range of motion is best described as
Explanation
The ratio of scapulothoracic to glenohumeral motion with elevation has been shown to vary depending on what portion of elevation is examined, how much load is on the arm, and the technique used to measure increments of elevation. However, almost every study shows that the ratio of scapulothoracic to glenohumeral motion is 1:2 for the contributions over a full range of elevation to 170 degrees. In the first 30 degrees of elevation, there is significant variability in the ratio, and there may be significant variability up to around 60 degrees.
REFERENCES: Inman VT, Saunders JR, Abbott LC: Observations of the function of the shoulder joint. Clin Orthop 1996;330:3-12.
Freedman L, Munro RH: Abduction of the arm in the scapular plane: Scapular and glenohumeral movements. J Bone Joint Surg Am 1966;18:1503.
REFERENCES: Inman VT, Saunders JR, Abbott LC: Observations of the function of the shoulder joint. Clin Orthop 1996;330:3-12.
Freedman L, Munro RH: Abduction of the arm in the scapular plane: Scapular and glenohumeral movements. J Bone Joint Surg Am 1966;18:1503.
Question 34High Yield
The principle of homologous recombination in gene therapy is used to:
Explanation
Novel approaches to treating genetiCdiseases involve gene repair or replacement rather than gene supplementation. One such approach is based on the principle of homologous recombination (replacement of a defective gene by a normal gene)
Question 35High Yield
A newborn male child has a left foot deformity as shown in Figures 54a and 54b. The family history and birth history are unremarkable. The child is healthy and thriving, and examination of the spine, hips, and neurologic system reveals normal findings. What is the best treatment for the foot deformity?
Explanation
DISCUSSION: The foot shows all the classic signs of a clubfoot with hindfoot equinus, heel varus, supination, and forefoot adduction. The Ponseti method is now well recognized as the best treatment for idiopathic clubfoot. It calls for manipulation of the clubfoot on a weekly basis with the application of long leg cast to slowly achieve correction. A percutaneous heel cord tenotomy is often required, followed by an additional 3-week period of casting and eventual use of a foot abduction orthosis. AFO night splints will not achieve any correction. Anterior tibial tendon transfer is sometimes performed for a clubfoot with recurrence or if there is supination in the swing phase of gait. Short leg casts are not sufficient to achieve full correction of a clubfoot.
REFERENCES: Herzenberg JE, Radler C, Bor N: Ponseti versus traditional methods of casting for idiopathic clubfoot. J Pediatr Orthop 2002;22:517-521.
Morcuende JA, Dolan LA, Dietz FR, et al: Radical reduction in the rate of extensive corrective surgery for clubfoot using the Ponseti method. Pediatrics 2004; 113:376-380.
REFERENCES: Herzenberg JE, Radler C, Bor N: Ponseti versus traditional methods of casting for idiopathic clubfoot. J Pediatr Orthop 2002;22:517-521.
Morcuende JA, Dolan LA, Dietz FR, et al: Radical reduction in the rate of extensive corrective surgery for clubfoot using the Ponseti method. Pediatrics 2004; 113:376-380.
Question 36High Yield
Figures 1 and 2 show the clinical photograph and ultrasonography image obtained from an 8-month-old boy who has a 2-month history of a well-circumscribed mass in the palm, just proximal to the palmar digital crease of the index finger. The mass has not changed in size and does not seem to cause pain. What is the best next step in treatment?
---
---
---
---



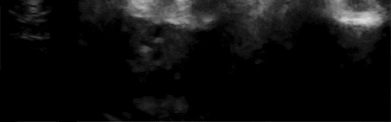
Explanation
The history, clinical photograph, and ultrasonography evaluation point to a diagnosis of ganglion cyst. The likelihood of resolution of ganglion cysts without intervention in pediatric patients ranges from 66-79%. Therefore the most appropriate treatment at this time is observation. Because the diagnosis is confirmed with the information provided, excisional biopsy and further imaging are not necessary.
Question 37High Yield
A 45-year-old postmenopausal smoker with a body mass index (BMI) of 22 has had severe knee pain for the past year. The pain has been progressing and the patient is now only able to perform activities of daily living. Knee radiographs reveal medial compartment osteoarthritis without any involvement of the patellofemoral joint or the lateral compartment. What is the contraindication for a high tibial osteotomy (HTO) in this patient?
Explanation
The principal contraindications to valgus-producing HTO include (1) lateral compartment degenerative joint disease, (2) loss of a significant portion of the lateral meniscus, (3) symptomatic patellofemoral degenerative joint disease,
(4) nonconcordant pain (ie, patellofemoral pain with medial compartment osteoarthritis), (5) smoking, (6) patient unwillingness to accept the anticipated cosmetic appearance of the desired amount of angular correction, and (7) inflammatory arthritis.
(4) nonconcordant pain (ie, patellofemoral pain with medial compartment osteoarthritis), (5) smoking, (6) patient unwillingness to accept the anticipated cosmetic appearance of the desired amount of angular correction, and (7) inflammatory arthritis.
Question 38High Yield
A 42-year-old patient has had painful inferior subluxation of the glenohumeral joint following a recent cerebrovascular accident (CVA). Figure 34 shows the AP radiograph of the shoulder. Management should consist of**
Explanation
Following a CVA and with the resumption of upright posture, downward subluxation of the glenohumeral joint may occur. Although usually painless, some patients may report pain secondary to stretching of the brachial plexus. This is the result of flaccid paralysis of the deltoid muscle, and it will persist until some motor tone or spasticity returns to the shoulder girdle musculature. Early sling support and range-of-motion exercises to prevent contracture will provide the best relief. Surgical procedures are not indicated.
REFERENCES: Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
McCollough NC III: Orthopaedic evaluation and treatment of the stroke patient. Instr Course Lect 1975;24:45-55.
REFERENCES: Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
McCollough NC III: Orthopaedic evaluation and treatment of the stroke patient. Instr Course Lect 1975;24:45-55.
Question 39High Yield
Figure 1
A 63-year-old woman who underwent attempted correction of a hallux valgus deformity 3 years previously presents to the office. She has pain in the hallux from dorsal abutment of the hallux on the shoe. There is no pain in the lesser toes or metatarsals. The recommended procedure to alleviate the irritation of the hallux is:
A 63-year-old woman who underwent attempted correction of a hallux valgus deformity 3 years previously presents to the office. She has pain in the hallux from dorsal abutment of the hallux on the shoe. There is no pain in the lesser toes or metatarsals. The recommended procedure to alleviate the irritation of the hallux is:
Explanation
This patient had previously undergone resection arthroplasty (Keller) for correction. A common complication of this procedure is a cock-up toe deformity due to insufficiency of the short flexors. This can be corrected with lengthening of the extensor hallucis. If the latter procedure fails, then an arthrodesis can be performed.
Question 40High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic instability best assessed intra-operatively?
---
---
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic instability best assessed intra-operatively?
---
---


Explanation
The radiographs reveal a trimalleolar ankle fracture dislocation with an associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
5. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
6. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
7. Maximizes the surface area for ankle joint loading
8. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
5. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
6. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
7. Maximizes the surface area for ankle joint loading
8. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
Question 41High Yield
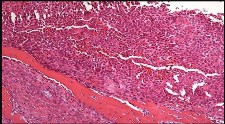
What is the neoplastic cell of origin for this tumor?
Explanation
Tenosynovial giant-cell tumors are widely known as pigmented villonodular synovitis (PVNS), although this term is misleading because this tumor type is a clonal neoplasm and does not involve an inflammatory process. It often is shown to have a t(1:2)(p13q37) karyotype resulting in CSF1-COL6A3 gene fusion. There are various amounts of mononuclear cells, osteoclastlike giant cells, foamy histiocytes, hemosiderophages, and chronic inflammatory cells. Local recurrences are common, but CSF1R inhibitors are being investigated in studies involving local control improvement and disease regression.
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
1. [Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. ](http://www.ncbi.nlm.nih.gov/pubmed/21823110)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21823110)
2. Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. _Enzinger & Weiss’s Soft Tissue Tumors_. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
3. [Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/27267143)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/27267143)
4. [Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. ](http://www.ncbi.nlm.nih.gov/pubmed/26222558)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26222558)
5. [Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.](http://www.ncbi.nlm.nih.gov/pubmed/24898549)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24898549)
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
1. [Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. ](http://www.ncbi.nlm.nih.gov/pubmed/21823110)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21823110)
2. Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. _Enzinger & Weiss’s Soft Tissue Tumors_. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
3. [Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/27267143)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/27267143)
4. [Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. ](http://www.ncbi.nlm.nih.gov/pubmed/26222558)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26222558)
5. [Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.](http://www.ncbi.nlm.nih.gov/pubmed/24898549)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24898549)
Question 42High Yield
Which of the following tendons is the primary antagonist of the posterior tibialis tendon?
Explanation
The primary action of the posterior tibialis tendon is inversion of the foot; secondarily, it plantar flexes the ankle. The anterior tibialis tendon also inverts the foot and only partially antagonizes the posterior tibialis tendon. The primary action of the peroneus longus is plantar flexion of the first ray. It secondarily everts the posterior tibialis tendon. The action of the flexor digitorum longus tendon is synergistic with the posterior tibialis tendon. The primary action of the peroneus brevis tendon is eversion; therefore, it is the primary antagonist of the posterior tibialis tendon.
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 550-551.
Mann RA: Biomechanics of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 2-36.
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 550-551.
Mann RA: Biomechanics of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 2-36.
Question 43High Yield
A 35-year-old man has substantial pain at the base of his dominant right thumb. Orthosis use, anti-inflammatory medication, and corticosteroid injections have failed to improve his symptoms. Which condition is a contraindication to the surgery shown in the radiograph (Figure 38)?

Explanation
There are multiple surgical options for treatment of symptomatic thumb carpometacarpal (CMC) joint arthritis, including trapeziectomy with or without suspensionplasty and with or without tendon interposition, prosthetic replacement, or arthrodesis. However, for a young manual laborer, a more robust solution is required so he can withstand the rigors of occupational activities. Arthrodesis of the CMC joint provides good pain relief but a relatively high nonunion rate (8%-21%). Presence of STT arthritis is a contraindication to CMC fusion because the STT joint will undergo increased stresses following CMC fusion, which will cause early failure of the surgical intervention. Bilateral thumb CMC fusions can be performed, and bilateral disease is not a contraindication to this procedure. Concomitant wrist arthritis does not preclude CMC fusion because this can be addressed with scaphoid excision and partial wrist fusion, which is not compromised by CMC fusion. Lack of MCP joint hyperextension does not preclude CMC fusion; substantial MCP hyperextension should be addressed at the time of arthroplasty for CMC arthritis with MCP fusion or volar capsulodesis.
RECOMMENDED READINGS
25. [Rizzo M, Moran SL, Shin AY. Long-term outcomes of trapeziometacarpal arthrodesis in the management of trapeziometacarpal arthritis. J Hand Surg Am. 2009 Jan; 34(1):20-6. doi: 10.1016/j.jhsa.2008.09.022. PubMed PMID: 19121726.](http://www.ncbi.nlm.nih.gov/pubmed/19121726)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19121726)
26. [Goldfarb CA, Stern PJ. Indications and techniques for thumb carpometacarpal arthrodesis. Tech Hand Up Extrem Surg. 2002 Dec;6(4):178-84. PubMed PMID: 16520598. ](http://www.ncbi.nlm.nih.gov/pubmed/16520598)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16520598)
RECOMMENDED READINGS
25. [Rizzo M, Moran SL, Shin AY. Long-term outcomes of trapeziometacarpal arthrodesis in the management of trapeziometacarpal arthritis. J Hand Surg Am. 2009 Jan; 34(1):20-6. doi: 10.1016/j.jhsa.2008.09.022. PubMed PMID: 19121726.](http://www.ncbi.nlm.nih.gov/pubmed/19121726)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19121726)
26. [Goldfarb CA, Stern PJ. Indications and techniques for thumb carpometacarpal arthrodesis. Tech Hand Up Extrem Surg. 2002 Dec;6(4):178-84. PubMed PMID: 16520598. ](http://www.ncbi.nlm.nih.gov/pubmed/16520598)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16520598)
Question 44High Yield
Figures 42a through 42d are the radiograph, CT scans, and biopsy specimen of a 38-year-old man who arrived at the emergency department with urinary retention. He has no other symptoms. What is the most appropriate treatment for this lesion?

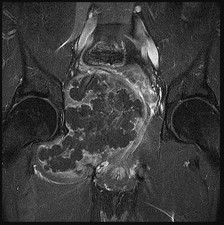
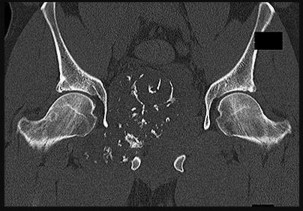
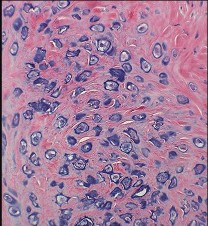
Explanation
These images reveal a chondrosarcoma. On radiograph, chondrosarcoma is a fusiform, lucent defect with scalloping of the inner cortex and periosteal reaction. Extension into the soft tissue may be present, as well as punctate or stippled calcification of the cartilage matrix. Histologically, chondrosarcoma is differentiated from benign cartilage tumors by enlarged plump nuclei, multiple cells per lacunae, binucleated cells, and hyperchromic nuclear pleomorphism. Treatment of most chondrosarcomas is surgery only because adjuvant treatments are not effective.
RECOMMENDED READINGS
17. [Weber KL, Pring ME, Sim FH. Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res. 2002 Apr;(397):19-28. PubMed PMID: 11953591. ](http://www.ncbi.nlm.nih.gov/pubmed/11953591)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11953591)
18. [Rajani R, Gibbs CP. Treatment of Bone Tumors. Surg Pathol Clin. 2012 Mar 1;5(1):301-318. PubMed PMID: 22328909. ](http://www.ncbi.nlm.nih.gov/pubmed/22328909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22328909)
RECOMMENDED READINGS
17. [Weber KL, Pring ME, Sim FH. Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res. 2002 Apr;(397):19-28. PubMed PMID: 11953591. ](http://www.ncbi.nlm.nih.gov/pubmed/11953591)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11953591)
18. [Rajani R, Gibbs CP. Treatment of Bone Tumors. Surg Pathol Clin. 2012 Mar 1;5(1):301-318. PubMed PMID: 22328909. ](http://www.ncbi.nlm.nih.gov/pubmed/22328909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22328909)
Question 45High Yield
Which ligament is most important in maintaining stability of the scapholunate joint?


Explanation
Scapholunate instability frequently develops as a consequence of blunt trauma to the wrist and is associated with significant clinical morbidity. The ligamentous anatomy and kinematics of the
carpus are complex and have been the focus of much clinical and biomechanical research. Multiple ligamentous structures contribute to the structure and function of the scapholunate articulation.
The wrist can be viewed as a 3-tiered structure with the forearm bones and carpometacarpal segments separated by the intercalated proximal row. The link between the distal and proximal carpal rows depends in large part on the scapholunate articulation. Instability of this articulation leads to altered kinematics and clinical symptomatology.
Multiple ligaments contribute to scapholunate joint integrity. They can be divided into intrinsic and extrinsic groups. The scapholunate interosseous ligament (SLIL) is described as intrinsic and is a C-shaped ligamentous structure that can be divided into 3 parts for descriptive purposes. The dorsal component is the thickest, with an average thickness of 3 mm and is approximately 5 mm in proximal-distal dimension. It attaches the proximal pole of the scaphoid to the dorsal aspect of the lunate. The proximal component has variable thickness and is composed largely of fibrocartilage. The volar component averages only 1 mm in thickness and 5 mm in proximal-distal dimension. It merges with the radioscapholunate ligament proximally and with the radioscaphocapitate (RSC) ligament distally. The other stabilizers are referred to as extrinsic because they connect the scaphoid and lunate to the radius and other carpal bones. Several ligaments at the palmar aspect of the carpus contribute to scapholunate stability. The RSC ligament runs from the radial styloid to the scaphoid fossa. The long radiolunate ligament (LRL) extends from the volar radius to the volar lunate. The radioscapholunate ligament (RSL) attaches the volar distal radius to the volar aspect of the SLIL. The scaphotrapezial ligament (ST) attaches the distal pole of the scaphoid to the trapezium.
Other extrinsic ligaments contributing to scapholunate stability are found at the dorsal aspect of the carpus. The dorsal radiocarpal ligament (DRC) originates from the dorsal distal radius and inserts onto the dorsum of the lunate, triquetrum, and lunotriquetral interosseous ligament. The dorsal intercarpal ligament (DIC) attaches to the dorsum of the triquetrum and extends radially, past the lunate, to insert on the dorsal distal pole of the scaphoid.
Although the exact contribution of each ligament to scapholunate stability is not fully understood, some interesting observations have been made. The SLIL appears to be the primary stabilizing structure. Sectioning the SLIL alone, without disturbing the extrinsic stabilizers, leads to substantial widening of the scapholunate interval and altered motion patterns of both the scaphoid and lunate. Sectioning the RSC and ST ligaments with an intact SLIL does not significantly alter scaphoid or lunate kinematics with respect to motion in the flexion-extension and radial-ulnar planes. Similarly, sectioning of the ST and DIC ligaments by another study group demonstrated no alterations in scapholunate motion, whereas DRC sectioning led to only modest ulnar deviation of the lunate. Although many ligaments contribute to the stability of the scapholunate joint, the SLIL appears to be the primary stabilizer. The most robust and functionally important part of the SLIL appears to be the dorsal component. The role of the secondary stabilizers is significant, and more work is necessary to fully understand their contributions.
RECOMMENDED READINGS
1. [Rajan PV, Day CS. Scapholunate Interosseous Ligament Anatomy and Biomechanics. J Hand Surg Am. 2015 Aug;40(8):1692-702. doi: 10.1016/j.jhsa.2015.03.032. Epub 2015 Jul 1. Review. PubMed PMID: 26143029.](http://www.ncbi.nlm.nih.gov/pubmed/26143029)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26143029)
2. Drewniany JJ, Palmer AK, Flatt AE. The scaphotrapezial ligament complex: an anatomic and biomechanical study. J Hand Surg Am. 1985 Jul;10(4):492-8. PubMed PMID: 4020059.
3. Short WH, Werner FW, Green JK, Masaoka S. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: Part II. J Hand Surg Am. 2005 Jan;30(1):24-34. PubMed PMID: 15680552.
4. Short WH, Werner FW, Green JK, Sutton LG, Brutus JP. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: part III. J Hand Surg Am. 2007 Mar;32(3):297-309.
**
carpus are complex and have been the focus of much clinical and biomechanical research. Multiple ligamentous structures contribute to the structure and function of the scapholunate articulation.
The wrist can be viewed as a 3-tiered structure with the forearm bones and carpometacarpal segments separated by the intercalated proximal row. The link between the distal and proximal carpal rows depends in large part on the scapholunate articulation. Instability of this articulation leads to altered kinematics and clinical symptomatology.
Multiple ligaments contribute to scapholunate joint integrity. They can be divided into intrinsic and extrinsic groups. The scapholunate interosseous ligament (SLIL) is described as intrinsic and is a C-shaped ligamentous structure that can be divided into 3 parts for descriptive purposes. The dorsal component is the thickest, with an average thickness of 3 mm and is approximately 5 mm in proximal-distal dimension. It attaches the proximal pole of the scaphoid to the dorsal aspect of the lunate. The proximal component has variable thickness and is composed largely of fibrocartilage. The volar component averages only 1 mm in thickness and 5 mm in proximal-distal dimension. It merges with the radioscapholunate ligament proximally and with the radioscaphocapitate (RSC) ligament distally. The other stabilizers are referred to as extrinsic because they connect the scaphoid and lunate to the radius and other carpal bones. Several ligaments at the palmar aspect of the carpus contribute to scapholunate stability. The RSC ligament runs from the radial styloid to the scaphoid fossa. The long radiolunate ligament (LRL) extends from the volar radius to the volar lunate. The radioscapholunate ligament (RSL) attaches the volar distal radius to the volar aspect of the SLIL. The scaphotrapezial ligament (ST) attaches the distal pole of the scaphoid to the trapezium.
Other extrinsic ligaments contributing to scapholunate stability are found at the dorsal aspect of the carpus. The dorsal radiocarpal ligament (DRC) originates from the dorsal distal radius and inserts onto the dorsum of the lunate, triquetrum, and lunotriquetral interosseous ligament. The dorsal intercarpal ligament (DIC) attaches to the dorsum of the triquetrum and extends radially, past the lunate, to insert on the dorsal distal pole of the scaphoid.
Although the exact contribution of each ligament to scapholunate stability is not fully understood, some interesting observations have been made. The SLIL appears to be the primary stabilizing structure. Sectioning the SLIL alone, without disturbing the extrinsic stabilizers, leads to substantial widening of the scapholunate interval and altered motion patterns of both the scaphoid and lunate. Sectioning the RSC and ST ligaments with an intact SLIL does not significantly alter scaphoid or lunate kinematics with respect to motion in the flexion-extension and radial-ulnar planes. Similarly, sectioning of the ST and DIC ligaments by another study group demonstrated no alterations in scapholunate motion, whereas DRC sectioning led to only modest ulnar deviation of the lunate. Although many ligaments contribute to the stability of the scapholunate joint, the SLIL appears to be the primary stabilizer. The most robust and functionally important part of the SLIL appears to be the dorsal component. The role of the secondary stabilizers is significant, and more work is necessary to fully understand their contributions.
RECOMMENDED READINGS
1. [Rajan PV, Day CS. Scapholunate Interosseous Ligament Anatomy and Biomechanics. J Hand Surg Am. 2015 Aug;40(8):1692-702. doi: 10.1016/j.jhsa.2015.03.032. Epub 2015 Jul 1. Review. PubMed PMID: 26143029.](http://www.ncbi.nlm.nih.gov/pubmed/26143029)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26143029)
2. Drewniany JJ, Palmer AK, Flatt AE. The scaphotrapezial ligament complex: an anatomic and biomechanical study. J Hand Surg Am. 1985 Jul;10(4):492-8. PubMed PMID: 4020059.
3. Short WH, Werner FW, Green JK, Masaoka S. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: Part II. J Hand Surg Am. 2005 Jan;30(1):24-34. PubMed PMID: 15680552.
4. Short WH, Werner FW, Green JK, Sutton LG, Brutus JP. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: part III. J Hand Surg Am. 2007 Mar;32(3):297-309.
**
Question 46High Yield
A 65-year-old man with ankylosing spondylitis has a fall from a standing height. He previously had minimal range of motion in his cervical spine, but now notices he is better able to extend his head. He is seen in the emergency department and released with a soft collar for use as needed.
Explanation
- Fracture displacement or subluxation leading to neurologic injury
Question 47High Yield
A 65-year-old woman with diabetes has fever and erythema 2 weeks after undergoing instrumented spinal fusion.
Explanation
- Postoperative deep surgical site infection
Question 48High Yield
A 35-year-old man sustained a Lisfranc dislocation 2 years ago. He was treated with standard open reduction and fixation. At 4 months, the screws were removed. He now has increasing pain and discomfort. A current radiograph is shown in Figure 85. What is the best treatment option?

Explanation
The most reliable treatment will be a reduction and fusion of the medial three TMT joints.There is adequate proof in the literature that fusion of all five TMT joints should be avoided because the fusion rate as well as functional outcome is inferior with fusion of all five joints compared with fusion of the medial three TMT joints and preservation of mobility in the 4-5 TMT joints. There is too much deformity and arthritis to warrant a revision open reduction and internal fixation. An interpositional graft is not proven to help in this situation because it neither corrects the deformity nor aids in stability.
---
---
Question 49High Yield
A 57-year-old man has a bone lesion that was identified on radiograph and MR imaging (Figures 17a and 17b) that were taken to evaluate anterior knee pain. An examination reveals a positive patellar apprehension test finding. The patient brings his imaging findings to his appointment, and you learn that an image-guided core needle biopsy was performed based upon the radiologist’s interpretation of the imaging. The core needle biopsy pathology interpretation text reads, “a low-
grade cartilage consistent with either enchondroma or low-grade chondrosarcoma. Clinical and imaging correlation is recommended.” What is the best next step?
grade cartilage consistent with either enchondroma or low-grade chondrosarcoma. Clinical and imaging correlation is recommended.” What is the best next step?

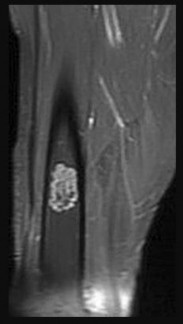


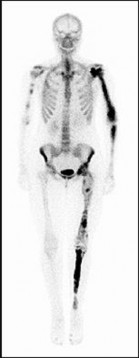
Explanation
Low-grade cartilage lesions are among the few diagnoses for which proceeding to definitive surgical treatment without a definitive histologic diagnosis is appropriate. Extended curettage with adjuvants is an acceptable treatment option for both enchondroma and low-grade chondrosarcoma of the extremities; as such, it is appropriate to proceed to definitive treatment when these are the only diagnoses in the differential. There is no consensus regarding the number and type of adjuvants used in intralesional curettage. There is also lack of consensus regarding how to reconstruct the resultant defect, with some favoring cement and others favoring bone grafting. A wide resection with intercalary resection is not indicated. Most commonly, serial radiologic studies are recommended to ensure no change occurs over time when the lesion is found incidentally, as in this patient.
The t(9;22) translocation occurs in extraskeletal myxoid chondrosarcoma, which is not a consideration for this patient based upon location, imaging, and the biopsy interpretation. Repeat core needle biopsy is not indicated because the value of core needle biopsy in general for low-grade cartilage lesions is questionable in light of sampling error concerns and the inability of expert pathologists to reliably distinguish between enchondroma and low-grade chondrosarcoma. Many orthopaedic oncologists favor proceeding directly to curettage with adjuvants without any biopsy
when the imaging is classic for a low-grade cartilage tumor without any evidence of dedifferentiation. Enchondromas are frequently positron emission tomography (PET) avid, and PET is not used to distinguish enchondroma from low-grade chondrosarcoma.
RECOMMENDED READINGS
30. [Hickey M, Farrokhyar F, Deheshi B, Turcotte R, Ghert M. A systematic review and meta-analysis of intralesional versus wide resection for intramedullary grade I chondrosarcoma of the extremities. Ann Surg Oncol. 2011 Jun;18(6):1705-9. doi: 10.1245/s10434-010-1532-z. Epub 2011 Jan 22. Review. PubMed PMID: 21258968. ](http://www.ncbi.nlm.nih.gov/pubmed/21258968)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21258968)
31. [Meftah M, Schult P, Henshaw RM. Long-term results of intralesional curettage and cryosurgery for treatment of low-grade chondrosarcoma. J Bone Joint Surg Am. 2013 Aug 7;95(15):1358-64. doi: 10.2106/JBJS.L.00442. PubMed PMID: 23925739. ](http://www.ncbi.nlm.nih.gov/pubmed/23925739)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23925739)
32. [Skeletal Lesions Interobserver Correlation among Expert Diagnosticians (SLICED) Study Group. Reliability of histopathologic and radiologic grading of cartilaginous neoplasms in long bones. J Bone Joint Surg Am. 2007 Oct;89(10):2113-23. PubMed PMID: 17908885. ](http://www.ncbi.nlm.nih.gov/pubmed/17908885)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17908885)
33. Jesus-Garcia R, Osawa A, Filippi RZ, Viola DC, Korukian M, de Carvalho Campos Neto G, Wagner
[J. Is PET-CT an accurate method for the differential diagnosis between chondroma and chondrosarcoma? Springerplus. 2016 Feb 29;5:236. doi: 10.1186/s40064-016-1782-8. eCollection 2016. PubMed PMID: 27026930. ](http://www.ncbi.nlm.nih.gov/pubmed/27026930)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/27026930)
CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 21
Figures 18a through 18c are the radiographs and bone scan of a 23-year-old woman.
The t(9;22) translocation occurs in extraskeletal myxoid chondrosarcoma, which is not a consideration for this patient based upon location, imaging, and the biopsy interpretation. Repeat core needle biopsy is not indicated because the value of core needle biopsy in general for low-grade cartilage lesions is questionable in light of sampling error concerns and the inability of expert pathologists to reliably distinguish between enchondroma and low-grade chondrosarcoma. Many orthopaedic oncologists favor proceeding directly to curettage with adjuvants without any biopsy
when the imaging is classic for a low-grade cartilage tumor without any evidence of dedifferentiation. Enchondromas are frequently positron emission tomography (PET) avid, and PET is not used to distinguish enchondroma from low-grade chondrosarcoma.
RECOMMENDED READINGS
30. [Hickey M, Farrokhyar F, Deheshi B, Turcotte R, Ghert M. A systematic review and meta-analysis of intralesional versus wide resection for intramedullary grade I chondrosarcoma of the extremities. Ann Surg Oncol. 2011 Jun;18(6):1705-9. doi: 10.1245/s10434-010-1532-z. Epub 2011 Jan 22. Review. PubMed PMID: 21258968. ](http://www.ncbi.nlm.nih.gov/pubmed/21258968)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21258968)
31. [Meftah M, Schult P, Henshaw RM. Long-term results of intralesional curettage and cryosurgery for treatment of low-grade chondrosarcoma. J Bone Joint Surg Am. 2013 Aug 7;95(15):1358-64. doi: 10.2106/JBJS.L.00442. PubMed PMID: 23925739. ](http://www.ncbi.nlm.nih.gov/pubmed/23925739)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23925739)
32. [Skeletal Lesions Interobserver Correlation among Expert Diagnosticians (SLICED) Study Group. Reliability of histopathologic and radiologic grading of cartilaginous neoplasms in long bones. J Bone Joint Surg Am. 2007 Oct;89(10):2113-23. PubMed PMID: 17908885. ](http://www.ncbi.nlm.nih.gov/pubmed/17908885)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17908885)
33. Jesus-Garcia R, Osawa A, Filippi RZ, Viola DC, Korukian M, de Carvalho Campos Neto G, Wagner
[J. Is PET-CT an accurate method for the differential diagnosis between chondroma and chondrosarcoma? Springerplus. 2016 Feb 29;5:236. doi: 10.1186/s40064-016-1782-8. eCollection 2016. PubMed PMID: 27026930. ](http://www.ncbi.nlm.nih.gov/pubmed/27026930)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/27026930)
CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 21
Figures 18a through 18c are the radiographs and bone scan of a 23-year-old woman.
Question 50High Yield
Estrogen deficiency results in which of the following:
Explanation
Estrogen deficiency results in increased bone resorption. An increase in IL-6 expression stimulates osteoclasts to resorb bone.
An increase in M-CSF and RANKL results in increased osteoclastiCactivity. OPG decreases osteoclastiCactivity as a decoy inhibitor of RANK
An increase in M-CSF and RANKL results in increased osteoclastiCactivity. OPG decreases osteoclastiCactivity as a decoy inhibitor of RANK
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon