Orthopedic Sport Review | Dr Hutaif Sports Medicine Rev -...
14 Apr 2026
83 min read
112 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Sport Review | Dr Hutaif Sports Me...
00:00
Start Quiz
Question 1High Yield
Which treatment regimen for Ewing sarcoma most effectively controls disease?
Explanation
Patients with Ewing sarcoma need chemotherapy to treat micrometastatic disease. Historical outcomes of patients who receive local control alone without chemotherapy are dismal. Chemotherapy alone, however, is not adequate to control local bulky disease. Local control options include radiation therapy or wide surgical resection. Historically, it was believed that surgery should be recommended for expendable bones to minimize morbidity. More recent data support improved outcomes (vs outcomes associated with radiation alone to the primary site of disease) for patients who undergo wide surgical resection; consequently, chemotherapy plus wide surgical resection is the most effective regimen.
RECOMMENDED READINGS
19. [Rodriguez-Galindo C, Spunt SL, Pappo AS. Treatment of Ewing sarcoma family of tumors: current status and outlook for the future. Med Pediatr Oncol. 2003 May;40(5):276-87. Review. Erratum in: Med Pediatr Oncol. 2003 Dec;41(6):594. PubMed PMID: 12652615. ](http://www.ncbi.nlm.nih.gov/pubmed/12652615)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12652615)
20. Bacci G, Toni A, Avella M, Manfrini M, Sudanese A, Ciaroni D, Boriani S, Emiliani E, Campanacci
[M. Long-term results in 144 localized Ewing's sarcoma patients treated with combined therapy. Cancer. 1989 Apr 15;63(8):1477-86. PubMed PMID: 2924256. ](http://www.ncbi.nlm.nih.gov/pubmed/2924256)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2924256)
21. [Maheshwari AV, Cheng EY. Ewing sarcoma family of tumors. J Am Acad Orthop Surg. 2010 Feb;18(2):94-107. Review. PubMed PMID: 20118326. ](http://www.ncbi.nlm.nih.gov/pubmed/20118326)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20118326)
22. Weis L. Ewing’s Sarcoma. In: Simon MA, Springfield D, eds. _Surgery for Bone and Soft Tissue Tumors_. Philadelphia, PA: Lippincott-Raven; 1998:287-298.
23. DuBois SG, Krailo MD, Gebhardt MC, Donaldson SS, Marcus KJ, Dormans J, Shamberger RC, Sailer S, Nicholas RW, Healey JH, Tarbell NJ, Randall RL, Devidas M, Meyer JS, Granowetter L, Womer RB, Bernstein M, Marina N, Grier HE. Comparative evaluation of local control strategies in localized
Ewing sarcoma of bone: a report from the Children's Oncology Group. Cancer. 2015 Feb 1;121(3):467-
[75/. doi: 10.1002/cncr.29065. Epub 2014 Sep 23. PubMed PMID: 25251206. ](http://www.ncbi.nlm.nih.gov/pubmed/25251206)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25251206)
RECOMMENDED READINGS
19. [Rodriguez-Galindo C, Spunt SL, Pappo AS. Treatment of Ewing sarcoma family of tumors: current status and outlook for the future. Med Pediatr Oncol. 2003 May;40(5):276-87. Review. Erratum in: Med Pediatr Oncol. 2003 Dec;41(6):594. PubMed PMID: 12652615. ](http://www.ncbi.nlm.nih.gov/pubmed/12652615)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12652615)
20. Bacci G, Toni A, Avella M, Manfrini M, Sudanese A, Ciaroni D, Boriani S, Emiliani E, Campanacci
[M. Long-term results in 144 localized Ewing's sarcoma patients treated with combined therapy. Cancer. 1989 Apr 15;63(8):1477-86. PubMed PMID: 2924256. ](http://www.ncbi.nlm.nih.gov/pubmed/2924256)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2924256)
21. [Maheshwari AV, Cheng EY. Ewing sarcoma family of tumors. J Am Acad Orthop Surg. 2010 Feb;18(2):94-107. Review. PubMed PMID: 20118326. ](http://www.ncbi.nlm.nih.gov/pubmed/20118326)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20118326)
22. Weis L. Ewing’s Sarcoma. In: Simon MA, Springfield D, eds. _Surgery for Bone and Soft Tissue Tumors_. Philadelphia, PA: Lippincott-Raven; 1998:287-298.
23. DuBois SG, Krailo MD, Gebhardt MC, Donaldson SS, Marcus KJ, Dormans J, Shamberger RC, Sailer S, Nicholas RW, Healey JH, Tarbell NJ, Randall RL, Devidas M, Meyer JS, Granowetter L, Womer RB, Bernstein M, Marina N, Grier HE. Comparative evaluation of local control strategies in localized
Ewing sarcoma of bone: a report from the Children's Oncology Group. Cancer. 2015 Feb 1;121(3):467-
[75/. doi: 10.1002/cncr.29065. Epub 2014 Sep 23. PubMed PMID: 25251206. ](http://www.ncbi.nlm.nih.gov/pubmed/25251206)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25251206)
Question 2High Yield
What is the most common cause of rotator cuff injury in high school athletes?
Explanation
A large number of etiologies of rotator cuff injury have been proposed. Both intrinsic and extrinsic mechanisms have been suggested. In the young athlete the common underlying mechanism is overuse. Contributing factors include increased laxity, anatomic variation in the coracoacromial arch, and altered kinematics.
REFERENCES: Wilkins KE: Shoulder injuries: Epidemiology, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 175-182.
Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannnotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 3-30.
REFERENCES: Wilkins KE: Shoulder injuries: Epidemiology, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 175-182.
Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannnotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 3-30.
Question 3High Yield
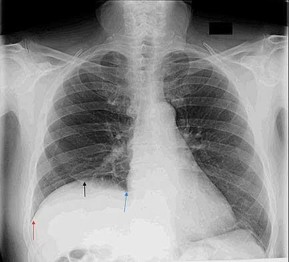
Figure 49 is the chest radiograph of a 47-year-old man who underwent right shoulder arthroscopy under general anesthesia and regional blockade (interscalene). The finding in the radiographic image likely is attributable to which mechanism?
Explanation
Positive end-pressure ventilation can cause alveolar rupture and pneumothorax, not elevation of the hemidiaphragm on the surgical side. The phrenic nerve, which controls the right hemidiaphragm, is not encountered during routine shoulder surgery because it courses medial to the scalene musculature near the midline of the neck. A traction injury is unlikely to cause injury to the phrenic nerve because it is part of the cervical plexus, which is not normally subject to traction during shoulder surgery. Hemidiaphragm paralysis via the phrenic nerve has been reported to occur as often as 100% of the time with use of interscalene regional anesthesia.
RECOMMENDED READINGS
1. [Urmey WF, Talts KH, Sharrock NE. One hundred percent incidence of hemidiaphragmatic paresis associated with interscalene brachial plexus anesthesia as diagnosed by ultrasonography. Anesth Analg. 1991 Apr;72(4):498-503. PubMed PMID: 2006740.](http://www.ncbi.nlm.nih.gov/pubmed/2006740)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2006740)
2. [Lenters TR, Davies J, Matsen FA 3rd. The types and severity of complications associated with interscalene brachial plexus block anesthesia: local and national evidence. J Shoulder Elbow Surg. 2007 Jul-Aug;16(4):379-87. Epub 2007 Apr 19. PubMed PMID: 17448698.](http://www.ncbi.nlm.nih.gov/pubmed/17448698)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17448698)
RECOMMENDED READINGS
1. [Urmey WF, Talts KH, Sharrock NE. One hundred percent incidence of hemidiaphragmatic paresis associated with interscalene brachial plexus anesthesia as diagnosed by ultrasonography. Anesth Analg. 1991 Apr;72(4):498-503. PubMed PMID: 2006740.](http://www.ncbi.nlm.nih.gov/pubmed/2006740)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2006740)
2. [Lenters TR, Davies J, Matsen FA 3rd. The types and severity of complications associated with interscalene brachial plexus block anesthesia: local and national evidence. J Shoulder Elbow Surg. 2007 Jul-Aug;16(4):379-87. Epub 2007 Apr 19. PubMed PMID: 17448698.](http://www.ncbi.nlm.nih.gov/pubmed/17448698)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17448698)
Question 4High Yield
What finding would most likely be present on an AP radiograph of a nondislocated elbow with an anteromedial coronoid fracture?
Explanation
No detailed explanation provided for this question.
Question 5High Yield
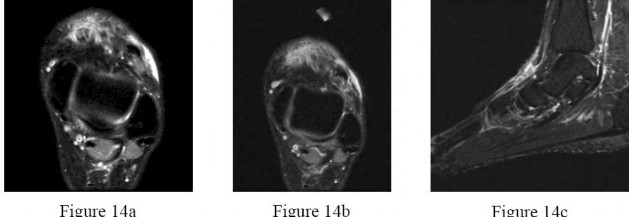
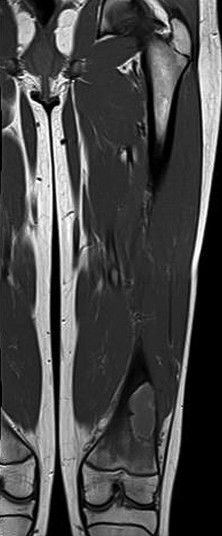
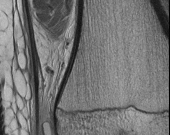
Figures 14a through 14c are the MRI scans of a 37-year-old woman who sustained a traumatic laceration to the anterior aspect of the ankle. The wound was closed in the emergency department. On examination,she has a foot drop and ambulates with a steppage gait. With successful surgical repair, what is the most common long-term residual?
---
---

Explanation
Anterior tendon disruption has been described in association with direct trauma, gout,inflammatory arthritis, local steroid injections, and diabetes. When a
rupture is accurately diagnosed in younger, healthy, active patients, surgical repair has been recommended. Surgical repair results in improved patient satisfaction; however, isokinetic testing has shown decreased dorsiflexion and inversion strength compared with the uninvolved side. Numbness can result from missed superficial nerve laceration. Persistent foot drop and use of an ankle-foot orthosis are more frequently seen in chronic missed injuries or with nonsurgical management.
---
rupture is accurately diagnosed in younger, healthy, active patients, surgical repair has been recommended. Surgical repair results in improved patient satisfaction; however, isokinetic testing has shown decreased dorsiflexion and inversion strength compared with the uninvolved side. Numbness can result from missed superficial nerve laceration. Persistent foot drop and use of an ankle-foot orthosis are more frequently seen in chronic missed injuries or with nonsurgical management.
---
Question 6High Yield
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?
Explanation
The most commonly injured neurovascular structure during an anterior approach for the repair of a distal biceps tendon rupture is the lateral antebrachial cutaneous nerve. This structure is located lateral to the biceps tendon and in a superficial location just deep to the subcutaneous layer. The antecubital vein is medial and superficial with the brachial artery and median nerve also medial to the biceps tendon but deep to the common flexors. The posterior interosseous nerve is deep within the supinator muscle and can be injured in the deep dissection or through the posterior approach when using a two-incision approach.
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Ramsey ML: Distal biceps tendon injuries: Diagnosis and management. J Am Acad Orthop Surg 1999;7:199-207.
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Ramsey ML: Distal biceps tendon injuries: Diagnosis and management. J Am Acad Orthop Surg 1999;7:199-207.
Question 7High Yield
Slide 1 Slide 2 Slide 3
A 44-year-old obese man presents for treatment of acute ankle pain. He does not have a history of trauma or a systemic history of note. His opposite foot has had multiple episodes of acute pain in the past, lasting from 3 to 5 days. On examination, the
ankle is warm, swollen, and exquisitely tender to palpation and any range of motion (Slide1, Slide 2, and Slide 3). C oncerned about the source of pain, you aspirate the joint and send the sample for analysis. You expect to find:
A 44-year-old obese man presents for treatment of acute ankle pain. He does not have a history of trauma or a systemic history of note. His opposite foot has had multiple episodes of acute pain in the past, lasting from 3 to 5 days. On examination, the
ankle is warm, swollen, and exquisitely tender to palpation and any range of motion (Slide1, Slide 2, and Slide 3). C oncerned about the source of pain, you aspirate the joint and send the sample for analysis. You expect to find:
Explanation
This patient most likely has an acute attack of gout. The prior episodes of foot pain and the sudden onset lasting 5 days for each bout is characteristic. The ankle is not a common location for gout (the most frequent site is the hallux metatarsophalangeal joint). The treatment should consist of injection of a corticosteroid into the joint and administration of appropriate oral anti-inflammatory medication.
Question 8High Yield
In surgical correction of the adult acquired flatfoot deformity, a medial translational calcaneal osteotomy is often performed in conjunction with additional soft tissue correction medially. One of the proposed biomechanical effects of the osteotomy associated with improvement in the arch of the foot is:
Explanation
The medial shift of the calcaneus effectively moves the Achilles tendon, thereby increasing the medial torque on the subtalar joint. The valgus deforming force of the Achilles on the heel is neutralized. The plantar fascia is lengthened, not tightened, by the medial shift of the calcaneus.
Question 9High Yield
What nerve is at the highest risk for injury with a percutaneous repair of an Achilles tendon injury?
Explanation
Cadaver and clinical studies have shown that the sural nerve is at the highest risk for injury with a percutaneous repair of the Achilles tendon.
REFERENCE: Hockenbury RT, Johns JC: A biomechanical in vitro comparison of open versus percutaneous repair of tendon Achilles. Foot Ankle 1990;11:67-72.
REFERENCE: Hockenbury RT, Johns JC: A biomechanical in vitro comparison of open versus percutaneous repair of tendon Achilles. Foot Ankle 1990;11:67-72.
Question 10High Yield
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. The patient fails an extensive course of physical therapy and is unable to return to baseball. He and his orthopaedic surgeon elect to proceed with surgery. During a repeat evaluation, he has negative sulcus and Beighton sign findings, and radiographs show 5° of glenoid retroversion. What is the most appropriate surgical plan?
---
---
---
---


Explanation
Posterior shoulder instability is a rare form of instability that often presents with pain rather than feelings of instability. It often occurs in young athletes during activities that put the shoulder in an “at-risk position” (flexion, adduction, internal rotation). Repetitive microtrauma can lead to posterior shoulder instability such as seen in football linemen. Swinging a bat or golf club places the lead arm in a flexed, adducted, and internally rotated position, which can lead to posterior translation of the humeral head that is forcibly reduced in follow-through, as seen in this patient. The glenohumeral joint relies on static and dynamic stabilizers. Static stabilizers help prevent instability at the end ranges of motion when the ligaments are taut. Dynamic stabilizers work to prevent subluxation at midranges of motion, at which the ligaments are lax. The rotator cuff is integral as a dynamic stabilizer of the shoulder. It works through a process called concavity compression. The four muscles of the rotator cuff compress the humeral head into the concavity of the glenoid-labrum. This prevents the humeral head from subluxing during the midranges of motion. Of the four rotator cuff muscles, the subscapularis is most important at preventing posterior subluxation. This patient has posterior instability, and various surgical techniques may be indicated depending on findings. Arthroscopic labral repair is indicated for anterior instability. Arthroscopic posterior labral repair is indicated for this patient because he has a posterior labral tear and posterior instability. If a patient has ligamentous laxity (not seen in this scenario because sulcus and Beighton sign findings would be negative), a posterior capsular shift with rotator interval closure is indicated. If a patient has excessive glenoid retroversion (not seen in this scenario with 5 degrees of retroversion), a posterior opening-wedge osteotomy is appropriate. The most common complication seen after arthroscopic posterior labral repair is stiffness, followed by recurrent instability
and degenerative joint disease.
and degenerative joint disease.
Question 11High Yield
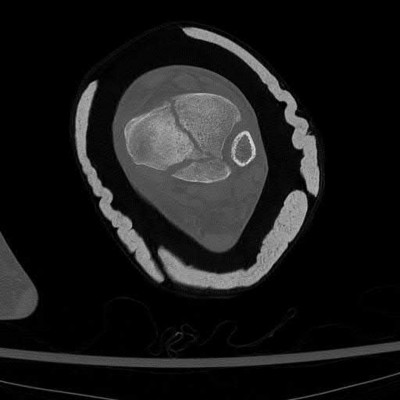
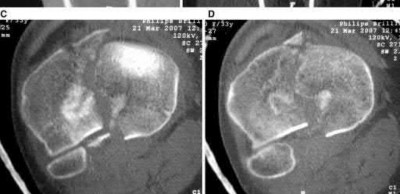
A 35-year-old male presents 6 weeks following open reduction and internal fixation of the injury shown in Figures A and B performed through a sinus tarsi approach. He is a 1/2-pack-per-day smoker and his body mass index (BMI) is 25. He last presented 3 weeks ago at which time his wound appeared healed, and the sutures were removed. Physical therapy was also initiated for gentle range of motion exercises. He reports that his main surgical incision "opened up" a few days ago and has been draining. He denies fevers or chills at this time. On physical exam, he has a small, 1 cm area of wound dehiscence with no exposed hardware. His current radiograph is
shown in Figure C. Which of the following combines the risk factors this patient has for wound dehiscence with the next best step in treatment?
shown in Figure C. Which of the following combines the risk factors this patient has for wound dehiscence with the next best step in treatment?



Explanation
Smoking is a risk factor for wound dehiscence after open reduction and internal fixation (ORIF) of calcaneal fractures. Superficial wound dehiscence should initially be treated with cessation of physical therapy, immobilization, and nonsurgical wound management.
The most common complication associated with ORIF of calcaneus fractures is delayed wound healing. The extensile lateral approach is the most commonly used approach for treating these injuries and has been associated with wound breakdown in nearly 25% of patients. The sinus tarsi approach utilizes a much smaller incision and studies have shown fewer wound healing difficulties. Preoperative risk factors that predispose to wound breakdown include smoking, diabetes, open fractures, high BMI, and closure of the wound in a single layer. In the event of superficial wound breakdown, range of motion exercises should be stopped and a prophylactic course of antibiotics should be started with nonsurgical wound management. If purulence is encountered or the wound is found to be deep, hospitalization with serial debridements and antibiotics is required.
Clare et al. performed a review of how to manage complications of calcaneal fractures. They report that immobilization after wound breakdown should be performed with casting with a window over the wound to allow for wound care and wet-to-dry dressing changes. Once the wound is healed, range-of-motion exercises may be resumed.
Folk et al. performed a review of early wound complications of operative treatment of calcaneus fractures through the lateral extensile approach. They found that smoking, open fractures, and diabetes were risks for a wound complication. They recommend that patients with identifiable risk factors should be counseled of this potential complication.
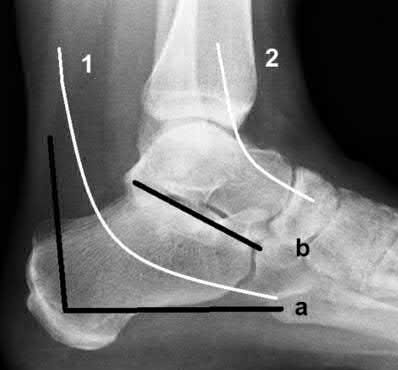
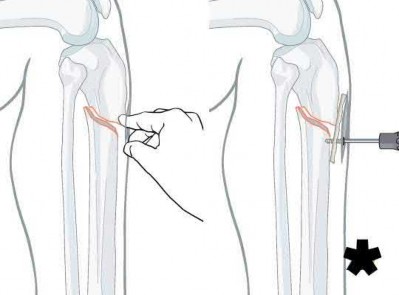
Figure A is a lateral ankle radiograph demonstrating a displaced, intraarticular calcaneal fracture. Figure B is an axial CT image demonstrating the fracture and the sustentaculum tali. Figure C is a lateral ankle radiograph demonstrating fixation of the fracture with a plate and independent screws.
This fixation strategy is utilized along with a sinus tarsi approach. Illustration A is a radiograph illustrating the two approaches used to fix calcaneus fractures. The letter (a) represents the lateral extensile incision while (b) represents the sinus tarsi incision. The number (1) correlates to the location of the sural nerve, while (2) correlates with the superficial peroneal nerve.
Incorrect Answers:
Answer 1: This patient has a normal BMI and irrigation and debridement with removal of hardware is not indicated at this point as the fracture is not healed. Answer 2: The sinus tarsi approach is more forgiving of the soft tissues compared with the lateral extensile approach. Irrigation and debridement with retention of hardware is not indicated at this point.
Answer 3: The sinus tarsi approach is more forgiving of the soft tissues compared with the lateral extensile approach.
Answer 4: The sinus tarsi approach is more forgiving of the soft tissues compared with the lateral extensile approach. Irrigation and debridement with retention of hardware is not indicated at this point.
The most common complication associated with ORIF of calcaneus fractures is delayed wound healing. The extensile lateral approach is the most commonly used approach for treating these injuries and has been associated with wound breakdown in nearly 25% of patients. The sinus tarsi approach utilizes a much smaller incision and studies have shown fewer wound healing difficulties. Preoperative risk factors that predispose to wound breakdown include smoking, diabetes, open fractures, high BMI, and closure of the wound in a single layer. In the event of superficial wound breakdown, range of motion exercises should be stopped and a prophylactic course of antibiotics should be started with nonsurgical wound management. If purulence is encountered or the wound is found to be deep, hospitalization with serial debridements and antibiotics is required.
Clare et al. performed a review of how to manage complications of calcaneal fractures. They report that immobilization after wound breakdown should be performed with casting with a window over the wound to allow for wound care and wet-to-dry dressing changes. Once the wound is healed, range-of-motion exercises may be resumed.
Folk et al. performed a review of early wound complications of operative treatment of calcaneus fractures through the lateral extensile approach. They found that smoking, open fractures, and diabetes were risks for a wound complication. They recommend that patients with identifiable risk factors should be counseled of this potential complication.
Figure A is a lateral ankle radiograph demonstrating a displaced, intraarticular calcaneal fracture. Figure B is an axial CT image demonstrating the fracture and the sustentaculum tali. Figure C is a lateral ankle radiograph demonstrating fixation of the fracture with a plate and independent screws.
This fixation strategy is utilized along with a sinus tarsi approach. Illustration A is a radiograph illustrating the two approaches used to fix calcaneus fractures. The letter (a) represents the lateral extensile incision while (b) represents the sinus tarsi incision. The number (1) correlates to the location of the sural nerve, while (2) correlates with the superficial peroneal nerve.
Incorrect Answers:
Answer 1: This patient has a normal BMI and irrigation and debridement with removal of hardware is not indicated at this point as the fracture is not healed. Answer 2: The sinus tarsi approach is more forgiving of the soft tissues compared with the lateral extensile approach. Irrigation and debridement with retention of hardware is not indicated at this point.
Answer 3: The sinus tarsi approach is more forgiving of the soft tissues compared with the lateral extensile approach.
Answer 4: The sinus tarsi approach is more forgiving of the soft tissues compared with the lateral extensile approach. Irrigation and debridement with retention of hardware is not indicated at this point.
Question 12High Yield
A 24-year-old man who plays golf noted the immediate onset of pain on the ulnar side of his hand and has been unable to swing a club for the past 6 weeks after striking a tree root with his club during his golf swing. Examination reveals full motion of the wrist, diminished grip strength, and tenderness over the hypothenar region. A CT scan of the hand and wrist is shown in Figure 26. Management should consist of
Explanation
Fractures of the hook of the hamate frequently are not identified in the acute phase. Because the fracture can be difficult to see on plain radiographs, the lack of findings can lead to a painful nonunion. A carpal tunnel view may show the fracture, but a CT scan will best detect the injury. Immobilization is the treatment of choice and will result in union in most patients unless the diagnosis is delayed. However, excision of the fragment may be necessary for patients who have nonunion, persistent pain, or ulnar nerve palsy.
REFERENCES: Carroll RE, Lakin JF: Fracture of the hook of the hamate: Acute treatment. J Trauma 1993;34:803-805.
Whalen JL, Bishop AT, Linscheid RL: Nonoperative treatment of acute hamate hook fractures. J Hand Surg Am 1992;17:507-511.
REFERENCES: Carroll RE, Lakin JF: Fracture of the hook of the hamate: Acute treatment. J Trauma 1993;34:803-805.
Whalen JL, Bishop AT, Linscheid RL: Nonoperative treatment of acute hamate hook fractures. J Hand Surg Am 1992;17:507-511.
Question 13High Yield
A healthy 65-year-old woman undergoes anatomic total shoulder arthroplasty to address osteoarthritis (OA). The surgery is uncomplicated. What is the most common indication for future revision?
Explanation
The most common reason for revision surgery following unconstrained shoulder arthroplasty for glenohumeral OA is loosening of the implant. In most studies that distinguish glenoid from humeral loosening, the glenoid component is more frequently affected. Comprehensive systematic reviews have found that radiographic glenoid loosening can comprise nearly 30% to 40% of all complications following shoulder arthroplasty for non-inflammatory arthritis. Infections, periprosthetic fractures, and rotator cuff tears are uncommon. In the population-based study by Matsen and associates, 10% of the revisions were performed for loosening versus 7% for infection and 7% for rotator cuff tearing.
5
5
Question 14High Yield
Where does the blood supply enter the fracture fragment?
Explanation
- Posteriorly_
Question 15High Yield
In addition to physical therapy, what is the best course of treatment at this time?
Explanation
- Ankle-foot orthosis
Question 16High Yield
What is the most appropriate way to communicate instructions to a family when there is a language barrier?










Explanation
Ideally, professional medical interpreters should be used in situations involving language difficulties. Printed instructions are helpful, but, if there is a language barrier, these instructions cannot substitute for conversing and answering questions. Asking the child to translate (no matter how fluent he or she may be) is suboptimal. Nonmedical staff may not be fluent enough to adequately translate medical terms.
Figure 14a
Figure 14b
Figure 14c
Figure 14d
Figure 14e
Figure 15a
Figure 15b
Figure 15c
Figure 15d
---|---|---
Figure 16a
Figure 16b
RESPONSES FOR QUESTIONS 14 THROUGH 16
1. Aspiration, cultures, surgical irrigation and debridement, and intravenous (IV) nafcillin
2. Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
3. Aspiration, cultures, Lyme serology, and oral amoxicillin
4. Biopsy, culture, curettage, bone graft, and possible internal fixation
5. Physical therapy, ibuprofen, and an antinuclear antibody test
Select the most appropriate treatment above to address each clinical scenario below.
Figure 14a
Figure 14b
Figure 14c
Figure 14d
Figure 14e
Figure 15a
Figure 15b
Figure 15c
Figure 15d
---|---|---
Figure 16a
Figure 16b
RESPONSES FOR QUESTIONS 14 THROUGH 16
1. Aspiration, cultures, surgical irrigation and debridement, and intravenous (IV) nafcillin
2. Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
3. Aspiration, cultures, Lyme serology, and oral amoxicillin
4. Biopsy, culture, curettage, bone graft, and possible internal fixation
5. Physical therapy, ibuprofen, and an antinuclear antibody test
Select the most appropriate treatment above to address each clinical scenario below.
Question 17High Yield
The histology of the lesion is shown in Figure 101d. What is the most likely complication after treatment of this lesion?
Explanation
_
_
_**DISCUSSION FOR QUESTIONS 101 THROUGH 103:**_
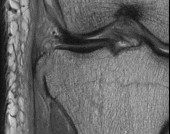
The MRI scans show a well-circumscribed inhomogenous mass at the anterior ankle joint consistent with a diagnosis of pigmented villonodular synovitis (PVNS), not an anatomic variant. An inflammatory mass,such as the pannus of rheumatoid arthritis, would reveal moderate signal intensity with relatively uniform signal throughout. The mass is well encapsulated, respecting tissue boundaries and not showing invasive characteristics as malignancies would. The arthroscopic image is also consistent with the reddish-brown frond-like tissue of PVNS. PVNS of the ankle can be treated arthroscopically. If this mode of treatment is chosen, a tissue sample should be sent to pathology for microscopic analysis; débridement should be performed on the remaining tissue. Removal of the instrumentation without débridement will not provide treatment and will result in disease progression. Tourniquet placement does not provide therapeutic benefit.
Brachytherapy has not been described for the treatment of PVNS of the ankle. The histologic image shows multiple multinucleated giant cells, hemosiderin, and very few mitotic figures – consistent with a diagnosis of PVNS. A common complication of PVNS treatment is local recurrence. Arthrofibrosis and chondrolysis are not seen with proper surgical care of these patients. Because this is not an infectious lesion, disseminated infection after treatment is highly unlikely. PVNS rarely metastasizes.
RESPONSES FOR QUESTIONS 104 THROUGH 106
1. # Toe is fused too straight (plantar flexed)
2. # Toe is fused in too much valgus
3. # Toe is fused in too much dorsiflexion
4. # There is a nonunion of the fusion
5. # Excessive shortening of the first metatarsal during preparation for fusion What is the most likely diagnosis for each patient?
_
_**DISCUSSION FOR QUESTIONS 101 THROUGH 103:**_
The MRI scans show a well-circumscribed inhomogenous mass at the anterior ankle joint consistent with a diagnosis of pigmented villonodular synovitis (PVNS), not an anatomic variant. An inflammatory mass,such as the pannus of rheumatoid arthritis, would reveal moderate signal intensity with relatively uniform signal throughout. The mass is well encapsulated, respecting tissue boundaries and not showing invasive characteristics as malignancies would. The arthroscopic image is also consistent with the reddish-brown frond-like tissue of PVNS. PVNS of the ankle can be treated arthroscopically. If this mode of treatment is chosen, a tissue sample should be sent to pathology for microscopic analysis; débridement should be performed on the remaining tissue. Removal of the instrumentation without débridement will not provide treatment and will result in disease progression. Tourniquet placement does not provide therapeutic benefit.
Brachytherapy has not been described for the treatment of PVNS of the ankle. The histologic image shows multiple multinucleated giant cells, hemosiderin, and very few mitotic figures – consistent with a diagnosis of PVNS. A common complication of PVNS treatment is local recurrence. Arthrofibrosis and chondrolysis are not seen with proper surgical care of these patients. Because this is not an infectious lesion, disseminated infection after treatment is highly unlikely. PVNS rarely metastasizes.
RESPONSES FOR QUESTIONS 104 THROUGH 106
1. # Toe is fused too straight (plantar flexed)
2. # Toe is fused in too much valgus
3. # Toe is fused in too much dorsiflexion
4. # There is a nonunion of the fusion
5. # Excessive shortening of the first metatarsal during preparation for fusion What is the most likely diagnosis for each patient?
Question 18High Yield
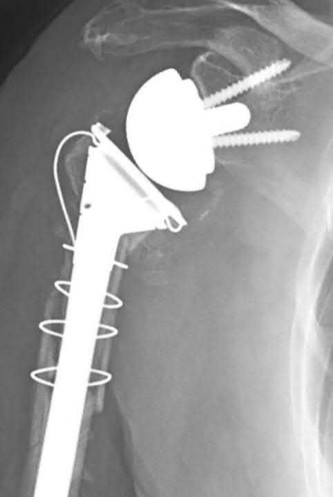
An 80-year-old patient presents 8 months postoperatively with right groin pain. Examination reveals a leg length discrepancy of
1.5cm. Recent radiographs are seen in Figures A and B. What is the most appropriate treatment plan?
1.5cm. Recent radiographs are seen in Figures A and B. What is the most appropriate treatment plan?


Explanation
This patient has atrophic non-union (NU) and varus collapse following cephalomedullary nailing of a subtrochanteric fracture. The ideal treatment involves nail removal, correction of alignment, fracture fixation, and bone grafting. Fixation can be achieved with a nail or plate.
Subtrochanteric fractures can be treated with cephalomedullary nailing or fixed angle plates. Nailing of these fractures is technically challenging because the fracture must be reduced prior to nail passage. Failure to do so leads to varus and procurvatum malreduction.
Bellabarba et al. reviewed plating of femoral nonunions after intramedullary nailing. Of 23 nonunions, 21 healed at an average of 12 weeks. The remaining 2 cases required repeat plating (at 2 and 8 weeks) for hardware breakage because of noncompliance with weightbearing restrictions. They advocate plating because it allows for correction of malalignment and provides a biomechanically superior tension band construct.
Incorrect Answers:
Answer 1:Dynamization is less effective in femoral NU compared with tibial NU. It is suitable for NU of axially stable fractures without significant angular deformity, particularly if statically locked in distraction. It is not suitable in this case because of varus collapse and shortening.
Answer 2: The use of tensioned wire fixators is poorly tolerated in the femur and has a high complication rate.
Answer 3: Reamed exchange nailing is the procedure of choice after IM nailing in the ABSENCE of femoral deformity. It is less effective in this case of varus collapse and shortening. Exchange unreamed nailing is not useful because (1) the new nail follows the same path as the old, making deformity correction impossible, and (2) the new nail cannot be larger than the old nail. A larger implant is only possible following reaming, especially if the isthmus is to be crossed.
Answer 4: Plating around a nail is inadvisable in this case because the existing hardware precludes deformity correction.
Subtrochanteric fractures can be treated with cephalomedullary nailing or fixed angle plates. Nailing of these fractures is technically challenging because the fracture must be reduced prior to nail passage. Failure to do so leads to varus and procurvatum malreduction.
Bellabarba et al. reviewed plating of femoral nonunions after intramedullary nailing. Of 23 nonunions, 21 healed at an average of 12 weeks. The remaining 2 cases required repeat plating (at 2 and 8 weeks) for hardware breakage because of noncompliance with weightbearing restrictions. They advocate plating because it allows for correction of malalignment and provides a biomechanically superior tension band construct.
Incorrect Answers:
Answer 1:Dynamization is less effective in femoral NU compared with tibial NU. It is suitable for NU of axially stable fractures without significant angular deformity, particularly if statically locked in distraction. It is not suitable in this case because of varus collapse and shortening.
Answer 2: The use of tensioned wire fixators is poorly tolerated in the femur and has a high complication rate.
Answer 3: Reamed exchange nailing is the procedure of choice after IM nailing in the ABSENCE of femoral deformity. It is less effective in this case of varus collapse and shortening. Exchange unreamed nailing is not useful because (1) the new nail follows the same path as the old, making deformity correction impossible, and (2) the new nail cannot be larger than the old nail. A larger implant is only possible following reaming, especially if the isthmus is to be crossed.
Answer 4: Plating around a nail is inadvisable in this case because the existing hardware precludes deformity correction.
Question 19High Yield
A 15-year-old boy presented with inability to elevate his right shoulder and flex his elbow. He sustained a fall from an all-terrain vehicle 8 weeks ago. He landed on the right shoulder and twisted his neck. Radiographs of the skull, chest, cervical and thoracic spine, and shoulder were normal. There was no loss of consciousness, chest pain, or breathing difficulties. The patient was observed in the hospital until stable and referred for follow-up in the hand clinic at 4 weeks. An electromyelogram (EMG) was scheduled. C linical examination revealed weakness of deltoid, supraspinatus, infraspinatus, teres minor, biceps, brachialis, brachioradialis, and extensor carpi radialis longus. The remainder of his forearm musculature was preserved and he could
grasp, release, and pinch. Sensations were decreased along the distribution of the axillary nerve. There was 3 cm wasting of his arm and 2 cm of the forearm. Tinelâs sign is positive around the clavicle. Hornerâs signs are absent and his arm lies against the body. The EMG report showed fibrillation potentials in the weak muscles. The patient can now flex his elbow. When asked to demonstrate, he flexes his wrist and pronates his forearm to swing his elbow into flexion.
Diagnosis of the condition is:
grasp, release, and pinch. Sensations were decreased along the distribution of the axillary nerve. There was 3 cm wasting of his arm and 2 cm of the forearm. Tinelâs sign is positive around the clavicle. Hornerâs signs are absent and his arm lies against the body. The EMG report showed fibrillation potentials in the weak muscles. The patient can now flex his elbow. When asked to demonstrate, he flexes his wrist and pronates his forearm to swing his elbow into flexion.
Diagnosis of the condition is:
Explanation
The involved muscles have C 5, C 6 root innervations. Positive Tinelâs sign, functioning rhomboids and serratus anterior, and the absence of Hornerâs syndrome rule out a preganglionic lesion. The EMG finding confirms the clinical finding. Subclinical involvement of any other muscle is not shown. Neuropraxia usually recovers in 6 weeks and EMG shows fibrillation, which is inconsistent with neuropraxia. Brachial plexus neuritis, Parsonage-Turner syndrome, has an acute presentation following a painful episode involving the whole arm. There is significant history of a fall in this case.
Question 20High Yield
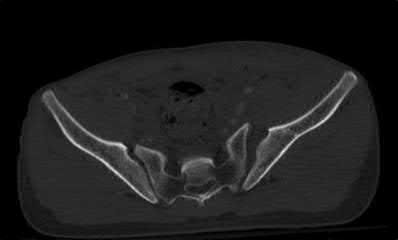
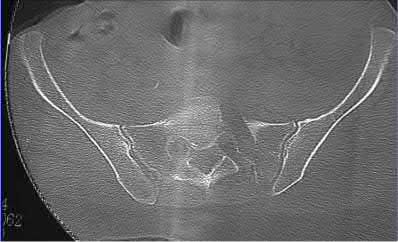
A 24-year-old male sustains the injury seen in Figure A after being thrown from a motorcycle at a high speed. Which of the following fixation methods has been shown to be the most stable fixation construct for this injury?

Explanation
Figure A shows an APC III injury, which is a rotationally and vertically unstable injury, with damage to the anterior ring, pelvic floor, and posterior ligamentous stabilizing structures.
The referenced study by Sagi et al found that biomechanically, a percutaneous iliosacral screw and anterior ring internal fixation was the most stable construct. In addition, he found no biomechanical support for addition of a second iliosacral screw.
The referenced study by Sagi et al found that biomechanically, a percutaneous iliosacral screw and anterior ring internal fixation was the most stable construct. In addition, he found no biomechanical support for addition of a second iliosacral screw.
Question 21High Yield
A 72-year-old man with a previous contralateral ankle fusion, rheumatoid arthritis, and 5 degrees of valgus; he has pursued nonsurgical treatment for 30 years and now has unrelenting pain
Explanation
- Ankle replacement
Question 22High Yield
Figures 1 and 2 are the radiograph and MRI scan of a 16-year-old boy who injured his right knee by a lateral side impact while playing football. The MRI indicates what structure was most likely injured?


Explanation
This is a rupture of the anterolateral ligament complex and a portion of the IT band. This injury is highly correlated with a complete ACL injury. In the MRI, the curvilinear or elliptic bone fragment (Segond fracture) projected parallel to the lateral aspect of the tibial plateau, the lateral capsular sign, is seen. The lateral capsular sign is also associated with ACL tears. Thus, this is an MRI showing a complete ACL _tear._
Question 23High Yield
An erythrocyte sedimentation rate (ESR) of what level is considered a good cutoff for guiding an index of suspicion for infection:
Explanation
With an ESR of 30 mm/hr to 35 mm/hr, sensitivities have been reported from 0.60 to 0.96 and specificities from 0.65 to
1
1
Question 24High Yield
A 52-year-old man who was a former high school pitcher now reports loss of elbow flexion and extension with pain at the extremes of motion. Nonsurgical management has failed to provide relief. Examination reveals movement from 50 degrees to 110 degrees and is painful only at the limits of motion. A radiograph is shown in Figure 12. Treatment should consist of
Explanation
Based on the history, examination, and radiograph, the patient has typical degenerative arthritis of the elbow. This condition is found almost exclusively in men, and there is almost universally a history of repetitive heavy use or overuse of the elbow. Patients report pain at terminal extension and usually have a flexion contracture. Radiographs reveal osteophytes on the coronoid and olecranon and in the coronoid and olecranon fossae. The osteophytes are often associated with loose bodies that sometimes are attached to the soft tissues. Treatment should consist of removal of all loose bodies and impinging osteophytes using open technique or by arthroscopy. The capsular contractures should be released at the same time.
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Morrey BF: Primary degenerative arthritis of the elbow: Treatment by ulnohumeral arthroplasty. J Bone Joint Surg Br 1992;74:409-413.
Redden JF, Stanley D: Arthroscopic fenestration of the olecranon fossa in the treatment of osteoarthritis of the elbow. Arthroscopy 1993;9:14-16.
O’Driscoll SW: Elbow arthritis: Treatment options. J Am Acad Orthop Surg 1993;1:106-116.
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Morrey BF: Primary degenerative arthritis of the elbow: Treatment by ulnohumeral arthroplasty. J Bone Joint Surg Br 1992;74:409-413.
Redden JF, Stanley D: Arthroscopic fenestration of the olecranon fossa in the treatment of osteoarthritis of the elbow. Arthroscopy 1993;9:14-16.
O’Driscoll SW: Elbow arthritis: Treatment options. J Am Acad Orthop Surg 1993;1:106-116.
Question 25High Yield
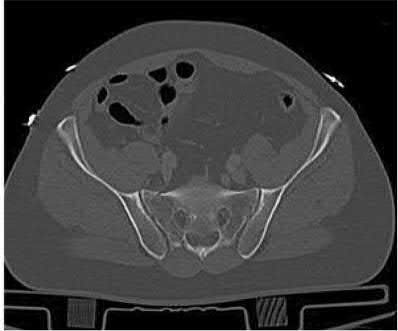
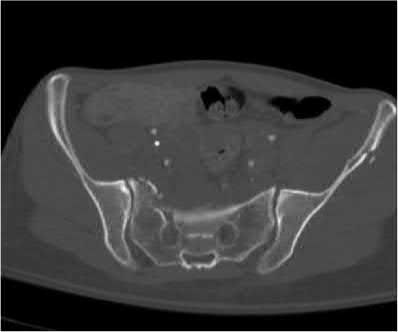
A 40-year-old male laborer sustained a fall from height and has isolated pelvic pain. He is otherwise hemodynamically stable. A radiograph is shown in Figure A. A stress examination under anesthesia does not show any further anterior diastasis or posterior pelvic ring displacement. Computed tomography reveals no asymmetry of the sacroiliac joints. What is the most appropriate management of this injury?

Explanation
This patient sustained an open-book pelvic fracture with a pubic symphysis diastasis of less than 2.5cm. From the Young and Burgess classification, he has anteroposterior compression (AP) type 1 injury. Treatment of this is protected weight-bearing and symptomatic treatment. Stress examination can be utilized in order to ensure that the injury is, in fact, a APC-1 injury, and not a more severe posterior injury that would require operative intervention.
Question 26High Yield
ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2B
ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2B
ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2B










































Explanation
This patient has a posterior knee dislocation with an ischemic limb that does not reverse following reduction. Emergent vascular exploration and reconstruction is indicated.
Knee dislocations are associated with popliteal artery injury in 18-45% of cases and range from intimal tears to complete transection. Amputation rates of 85% have been reported if revascularization is delayed greater than 6 to 8 hours.
Neurologic injury occurs in 15-40% of cases and is most common after posterolateral dislocation. The peroneal nerve is more commonly injured.
Rihn et al. reviewed the acutely dislocated knee. They recommend a vascular consult if pulses are weak, or ABI is compromised. They warn that in arterial injury, pulses, temperature and capillary refill can be normal. If the limb remains ischemic, surgical exploration and revascularization is indicated.
Medina et al. systematically reviewed neurovascular injury after knee dislocation in 862 patients. Vascular injury rate was 18%, and nerve injury rate was 25%. Repair was performed in 80% of vascular injuries, and amputation in 12%. The most vascular injury was seen in KDIIIL injuries (32%) and posterior dislocation (25%).
Figure A is an AP radiograph of a posterior knee dislocation. Figure B is a lateral showing the same injury.
Incorrect Answers:
: The limb remains ischemic. Splinting and observation alone are inappropriate.
Answer 3: External fixation is appropriate for immobilization following reduction, especially for very obese patients (BMI>50) where casting/splinting is not possible, and especially to protect a vascular reconstruction. However, the MOST important next step is vascular exploration to attempt revascularization.
Answers 4 and 5: CT angiography and standard angiography will only serve to delay vascular exploration of the ischemic limb. On-table angiograms will be performed during the surgery, obviating the need for preoperative angiography outside the operating room (OR).
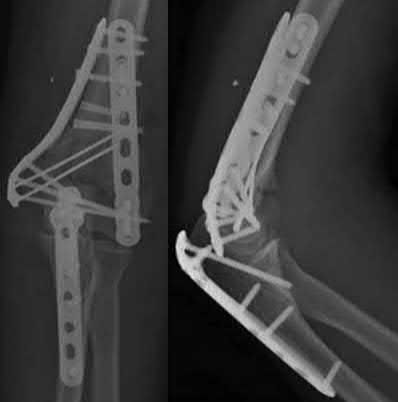
A 51-year-old carpenter presents with a distal humerus nonunion (Figures A and B). After repair of the nonunion, he is lost to follow up for 3 months and then presents to your clinic pain-free and with evidence of fracture union. On examination the elbow arc of motion is 10-80 degrees. Following a brief failed trial of conservative management, you recommend:
1) Open release of the posterior bundle of the MCL and excision of osteophytes
2) Complete open release of the MCL and LCL complexes with radiation for heterotopic ossification prophylaxis
3) Arthroscopic release of the anterior capsule with removal of hardware
4) Removal of hardware and dome osteotomy
5) Functional bracing and recommendation for job retraining
Limited flexion outside a functional range of motion (30-130 degrees) can be quite debilitating, and it is often addressed with open release of the posterior bundle of the MCL and posterior capsule and excision of osteophytes.
A frequent complication of distal humerus fractures is post-traumatic stiffness. This patient has had multiple procedures about the distal humerus, and the question stem implies that he did not complete a structured range of motion protocol following the repair of his nonunion. Beyond a trial of conservative management, there are many techniques described for capsule and soft tissue releases as well as bony resections if heterotopic ossification is present. This patient's severely limited flexion would best be addressed with a release of the posterior bundle of the MCL, and with flexion
A 51-year-old female presents with an acute inability to extend her thumb, four months after she was treated with cast immobilization for a minimally-displaced distal radius fracture. What is the most appropriate treatment at this time?
1) Occupational therapy for strengthening
2) Extensor carpi radialis longus transfer to extensor pollicus longus
3) Extensor pollicis brevis transfer to extensor pollicus longus
4) Extensor indicis proprius transfer to extensor pollicus longus
5) Primary repair of extensor pollicus longus
A rare complication of non-displaced or minimally displaced fractures of the distal radius treated with a cast is a delayed rupture of the extensor pollicis longus (EPL) tendon. The EPL is the primary extensor of the interphalangeal joint of the thumb and also assists with metacarpophalangeal extension.
Extensor indicis proprius transfer to the EPL is the most widely used and reported treatment for this condition.
Magnussen et al. reviewed results of EIP transfer following ruptures of the EPL, with 19/21 good results. None of the cases had any loss of independent index finger extension although index extensor strength reduced to half of that of the contralateral side.
Hove et al. reported a similar satisfaction rate following treatment of 15 patients. In his series of 4,400 distal radius fractures treated over a 5 year period, the incidence of delayed tendon rupture following distal radius fracture was 0.3 percent.
A 25-year-old female is involved in a motor vehicle collision. She presents with the isolated injury seen in Figures A through D. Her leg is swollen but her skin is intact. She has no clinical signs of compartment syndrome. Which of the following treatment options will allow for maintenance of fracture alignment and minimize the risk of soft tissue complications?
1) Closed reduction and long-leg non-weight bearing cast
2) Immediate open reduction of the tibia through an anterolateral approach
3) Percutaneous fixation of the articular surface and intramedullary nailing
4) Definitive uniplanar external fixator
5) Immediate open reduction of the tibia through an anteromedial approach
The patient presents with a closed distal third metaphyseal-diaphyseal distal tibia fracture with simple intra-articular extension. Immediate intramedullary nailing along with percutaneous fixation of the articular component provides appropriate restoration of length, rotation and alignment and minimizes the risk of wound complication.
Displaced distal third tibia fractures may be associated with simple intraarticular extension. Operative treatment of intra-articular distal tibia fractures has historically been performed with open reduction and internal fixation. Early open reduction and plate fixation of pilon fractures has been associated with high rates of infection and wound complication. In select patterns with simple articular extension, percutaneous screw fixation and medullary nailing may provide appropriate reduction with minimal soft-tissue risk.
Marcus et al. evaluated the outcomes of immediate intramedullary nailing and percutaneous fixation of simple intra-articular distal tibia fractures (AO/OTA 43 C1 and C2). The authors found excellent rates of union and alignment, however caution against broad application of this technique until more rigorous randomized studies can be performed.
Sirkin et al. retrospectively evaluated the results of a staged approach to management of intra-articular distal tibia fractures with temporary bridging external fixation followed by open reduction and internal fixation (ORIF). The authors found decreased rates of wound complication and infection compared with prior studies.
Figures A and B demonstrate a distal third tibial shaft fracture with simple intra-articular extension. The axial and coronal CT cuts in Figures C and D further clarify the articular injury. Illustrations A and B demonstrate a comminuted distal third tibial fracture with simple intra-articular extension. Illustrations C and D are fluoroscopic images of the same injury after intramedullary nailing and percutaneous fixation of the articular component.
Incorrect Answers:
Answer 1: Closed reduction and casting of this injury results in increased rates of malalignment
Answers 2 and 5: Immediate open reduction of pilon fractures has historically been associated with high rates of infection and wound complications
Answer 4: This fracture pattern would be difficult to control with a uniplanar fixator. A circular or multiplanar fixator would be a potential treatment option
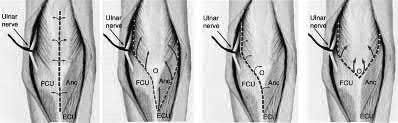
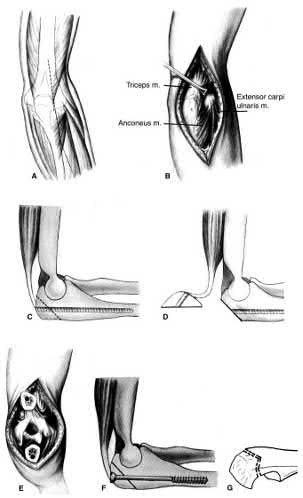
A 24-year-old woman is thrown from her motorcycle and sustains the closed injury shown in Figures A through C. Open reduction and internal fixation is planned. What surgical technique will best allow visualization of the joint surface and allow early range of motion?
1) Bryan-Morrey approach and parallel plating
2) Triceps reflecting anconeus pedicle approach and parallel plating
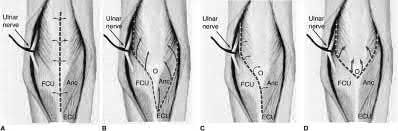
3) Triceps reflecting anconeus pedicle approach and orthogonal plating on the posteromedial and lateral surfaces
4) Olecranon osteotomy and parallel plating
5) Olecranon osteotomy and orthogonal plating on the posteromedial and lateral surfaces
Access to complex intra-articular fractures is best achieved by an olecranon osteotomy (OO). Fixation can be with parallel plating or orthogonal plating.
Bicolumnar fixation of distal humerus fractures should follow the principles outlined by O'Driscoll: Distal fragments should be held by as many screws as possible; every screw in the distal fragments should pass through a plate; each screw should engage as many articular fragments as possible.
Galano et al. review treatment for bicolumnar distal humerus fractures. They note that the olecranon osteotomy, Alonso-Llames triceps sparing and Campbell triceps splitting approaches expose 57%, 46% and 35% of the articular surface, respectively. The OO and paratricipital (triceps sparing)
approaches allow for early ROM. Protected motion is required for the O'Driscoll TRAP and Bryan-Morrey approaches for tendon-to-bone healing.
Coles et al. retrospectively reviewed the OO in fixation of 70 fractures. Osteotomy fixation was with an intramedullary screw and dorsal ulnar wiring, or with a plate. The rate of OO increased with fracture difficulty (from AO type C1-C3). There was 1 delayed union but no nonunions.
Figures A and B show a AO/OTA type C2 intraarticular distal humerus fracture. Figure C is a coronal CT scan showing intraarticular comminution. Illustration A shows fixation of the fracture with bicolumnar plating through an olecranon osteotomy approach. Illustration B shows the various approaches to the distal humerus (left, Campbell triceps splitting; center left, O'Driscoll triceps reflecting anconeus pedicle; center right, Bryan-Morrey approach, leaving the triceps attached laterally to the fasciocutaneous flap, but elevating it off the ulna; right, olecranon osteotomy). Illustration C shows 3 methods of olecranon osteotomy (A and B, Intra-articular transverse; C-F, Extra-articular oblique; G, Intra-articular chevron).
Incorrect Answers:
Answer 1: The Bryan-Morrey approach provides excellent medial exposure, but inadequate lateral exposure. The triceps is lifted subperiosteally, and the anconeus is released subperiosteally. Triceps repair depends on tendon-bone healing.
Answer 2: The O'Driscoll TRAP approach detaches triceps and anconeus from their distal insertions in a V-shaped flap that is reflected proximally. Repair to bone is via drill holes in the ulna. Early mobilization is not recommended.
Answers 3 and 5: Orthogonal plating is performed on the POSTEROLATERAL and MEDIAL surfaces.
A 31-year-old male sustains an isolated handgun injury shown in Figure A. On physical examination, he has a 0.5 cm wound over the anteromedial aspect of his thigh, with no gross contamination of the skin edges. He is neurovascularly intact. The patient has received tetanus prophylaxis and antibiotics in the emergency department.
What would next best step in treatment?
1) External fixation and IV antibiotics for 6 weeks
2) Irrigation and debridement of wound and external fixation for 6 weeks
3) Reamed antegrade or retrograde intramedullary nail
4) Irrigation and debridement of wound, reamed antegrade nail and IV antibiotics for 6 weeks
5) Irrigation and debridement of wound, reamed retrograde nail and IV antibiotics for 6 weeks
This patient has sustained a low-velocity gunshot to the right femoral diaphysis. The next best step in treatment would be insertion of a reamed antegrade or retrograde intramedullary nail. During surgery, the gunshot wound could be closed primarily if it was considered clean, or allowed to heal by secondary intention if it was there was any concern.
Low-velocity gunshot wounds are typically treated as closed fractures, since the risk of osteomyelitis is very low. These are typically bullets from handguns that travel 600 meters per second). The timing and direction (e.g. antegrade or retrograde) of nail insertion has not shown to
affect outcomes.
Cannada et al. reviewed 74 cases of femoral diaphyseal fractures caused by gunshots. All were treated with reamed, retrograde, statically locked intramedullary nailing, without formal irrigation and debridement in the operating room. Outcomes showed low incidence of shortening, angular deformity and infection rate.
Dougherty et al. compared retrograde vs. antegrade intramedullary nailing for the treatment of gunshot diaphyseal femur fractures. No significant differences were found between groups with regards to operative time, blood loss, or radiographic union. They conclude that immediate retrograde or antegrade nailing is safe for the early treatment of gunshot femur fractures.
Figure A shows an AP radiograph of the right femur. There is a gunshot fracture in the proximal femoral shaft with retained bullet fragments. The leg has been placed in temporary traction.
Incorrect Answers:
Answer 1: External fixation would be considered for treatment of femur fractures in damage control orthopaedics.
Answer 2: IV antibiotics for 6 weeks would not be necessary with low velocity gunshot wounds with clean wounds.
Answer 4 and 5: The direction of nail entry does not seem to affect outcomes with these fractures. Irrigation and debridement of wound, as well as IV antibiotics, wound not be necessary, aforementioned.
Figure A shows a radiograph of a 19-year-old male with an isolated shotgun injury. On physical examination, he has a 3 cm wound over the posterolateral aspect of his arm. In addition, he has weakness with wrist and finger extension, but no sensory deficits. The patient has received tetanus prophylaxis and antibiotics in the emergency department. What would be the next best steps in treatment?
1) Urgent open reduction internal fixation and fibular osteoseptocutaneous flap
2) Irrigation and debridement and external fixation
3) Irrigation and debridement, repair of the radial nerve and retrograde intramedullary nail
4) CT scan, urgent open reduction internal fixation and IV antibiotics for 6 weeks
5) Closed reduction, CT scan, immobilization in a coaptation splint
This patient has sustained a shotgun blast to the midshaft humerus. The next best step would be irrigation and debridement, and external fixation of the fracture.
Shotgun injuries are typically treated as open fractures, whereas low-energy gunshot wounds are treated as closed fractures. The initial operative treatment of shotgun wounds should include irrigation and debridement and stabilization with external fixation. The goal of treatment is to stabilize the severe soft-tissue injury and bone loss, as well as to aggressively debride devitalized tissue and gross contamination.
Dougherty et al. reviewed gunshot fractures to the humerus. They report that
peripheral nerve injuries are relatively common with these injuries, with a more common incidence in distal injuries than proximal.
Joshi et al. looked at low velocity gunshot fractures to the humerus. They found that these injuries can be safely treated as closed fractures with local wound care, fracture brace and oral antibiotics. The time to union was similar in the non-operative and open treatment group.
Berick et al. examined the indications for nerve exploration with humerus gunshot fractures. They recommend continued observation of isolated nerve palsies associated with gunshot fractures of the humerus. However, consider early nerve exploration of palsies when associated with a concomitant vascular injury.
Figure A shows a high velocity shotgun fracture to the left humerus with retained buck fragments. Illustration A shows a similar injury stabilized with external fixation.
Incorrect Answers:
Answer 1: Due to the severity of soft tissue injury, external fixation should be considered for initial stabilization. Vascularized fibular grafts has been expanded to an osteoseptocutaneous flap by including a cutaneous flap on the lateral aspect of the lower leg. These are not typically used in the acute setting.
Answer 3: Retrograde intramedullary nail would not be the ideal implant for this injury, acutely.
Answer 4 and 5: There is no indication for a CT scan or prolonged antibiotics. The fracture and soft-tissue injury should be initially stabilized with external fixation. Coaptation splinting will interfere with soft tissue care.
A 34-year-old male sustains the closed injury seen in Figure A as a result of a high-speed motor vehicle collision. What is the most appropriate next step in treatment?
1) Open reduction and internal fixation
2) Spanning external fixation
3) Percutaneous internal fixation
4) Closed reduction and cast placement
5) Ankle arthrodesis
The radiograph shows a comminuted pilon fracture, which is associated with high-energy trauma and significant soft tissue injury. The tested concept here is the importance of avoiding definitive reduction and fixation of this high-energy injury, which has been shown to be associated with an increased risk of wound complications and deep infections (as compared to staged treatment with usage of a spanning external fixator).
Patterson et al. reviewed 23 consecutive patients with comminuted distal tibia fractures. They showed 0% infections or wound-healing problems in their patient population treated with a two-staged protocol. Their protocol involved fibula fixation with an intramedullary implant and application of a medial external fixator to to regain length and restore anatomic alignment. Reevaluation of the limb occurred ten to fourteen days later for definitive fixation.
Sirkin et al. retrospectively reviewed 40 closed and 17 open pilon fractures (AO types 43A-C) that were treated with staged surgical management (avg. time from ext. fix. to formal reconstruction was 14 days (range 4 to 31) They reported 17% post-operative wound complication in the closed group and 11% post-operative wound complication in the open group (Gustilo Type I-III). They suggest the technique was successful in both closed and open pilon fractures.
A 72-year-old woman falls down stairs and sustains the injury shown in Figure A. Additional radiographs are performed in Figure B to help assess the fracture pattern. These additional radiographs represent which of the following?
1) Oblique radiographs
2) In-situ radiographs under anesthesia
3) Traction radiographs
4) Fracture flexion radiographs
5) Fracture extension radiographs
Additional traction radiographs are performed in distal humerus fractures to better understand the fracture configuration.
Traction radiographs help align the fracture fragments for better visualization. This is useful in comminuted fractures where distal fragments are telescoped or flexed on the proximal fragments, making CT scan visualization difficult.
Proper visualization can help determine (1) the approach to the distal humerus, (2) whether to perform ORIF or total elbow arthroplasty (in select patients), (3) whether to add a 3rd plate (lateral column), (4) whether to add tricortical bone graft to augment distal fixation and restore trochlear width.
Doornberg et al. examined whether 3D CT improved fracture characterization. They found that 3D CT improved interobserver and intraobserver reliability for fracture characterization and classification. It also improved intraobserver accuracy for fracture characteristics, but not interobserver accuracy. They concluded that 3D CT is helpful for preoperative planning.
Galano et al. reviewed treatment strategies for bicolumnar distal humerus fractures. They state that 3D CT compensates for oblique scans from formatting in an incorrect plane, and allows for subtraction of the radius/ulna to properly demonstrate articular incongruity, degree of comminution and column involvement.
Figures A and B show a distal humerus fracture without traction (A) and with traction (B) applied. Illustration A shows the same fracture after bicolumnar plating. Illustration B shows the different surgical approaches to the distal humerus (A, Campbell triceps splitting; B, O'Driscoll triceps reflecting anconeus pedicle [TRAP]; C, Bryan-Morrey triceps reflecting; D, olecranon osteotomy)
Incorrect Answers:
Answer 1: These radiographs aren't oblique images.
Answer 2: Radiographs under anesthesia do not add further information unless traction is applied.
Answers 4 and 5: Flexion and extension will further impact and displaced fragments and will not improve alignment.
Mirror therapy is indicated for which of the following clinical conditions?
1) Impaired proprioception after lower extremity injury
2) Two-stage flexor tendon reconstruction
3) Plumbism
4) Anterior cruciate ligament reconstruction
5) Phantom pain
Mirror therapy is a useful technique to improve phantom pain in amputees. Phantom limb pain is a painful sensation that is perceived within a body part that no longer exists.
Under mirror therapy, a patient is allowed to feel the imaginary movement of the removed body part behaving as normal body movement through a mirror. The mirror image of the normal body part helps reorganize and integrate the mismatch between proprioception and visual feedback of the amputated segment.
Tilak et al. performed a randomized controlled trial of 26 patients with phantom limb pain, and found that mirror therapy as well as transcutaneous electrical nerve stimulation both significantly improved pain scores, but no difference was seen between the two groups. They recommend use of both modalities in treatment of phantom limb pain, as they are noninvasive and inexpensive.
Chan et al. reviewed 22 patients utilizing mirror therapy for amputation related phantom limb pain, and found that patients reported a significant decrease in pain when utilizing this treatment modality as compared to covered mirror therapy or mental imagery therapy.
Illustration A shows a patient with an upper extremity amputation using a mirror to perform movements during a mirror therapy session.
Incorrect Answers:
Answer 1: Mirror therapy is not indicated for proprioception training. Answer 2: Mirror therapy is not indicated for flexor tendon injuries. Answer 3: Mirror therapy is not indicated for lead poisoning.
Answer 4: Mirror therapy is not indicated for ACL reconstruction.
A patient presents to the emergency department with the injury seen in Figure A. Which of the following is true about radial nerve palsies associated with isolated humeral shaft fractures after low velocity gunshot wounds?
1) The initial treatment involves debridement, irrigation, nerve exploration, and osteosynthesis.
2) The radial nerve palsy is often a result of neurotmesis.
3) Initial treatment involves splinting and observation for return of neurologic function.
4) Electrophysiologic testing for radial nerve palsies is indicated after 2-3 weeks without improvement.
5) The radial nerve palsy will not resolve regardless of attempted interventions.
When a patient sustains an isolated humeral shaft fracture and radial nerve palsy from a GSW, the initial treatment involves splinting with observation.
The majority of humeral shaft fractures are treated initially with a coaptation splint and then transitioned to a functional brace. Absolute surgical indications for operative management include: open fracture, brachial plexus injury, compartment syndrome, floating elbow, or vascular injury. A radial nerve palsy is not an indication for surgical management of an isolated humeral shaft fracture. Radial nerve injury from a low-velocity GSW is similar to that of blunt force trauma and thus, immediate exploration is not necessary. Instead, nerve function should be observed. Seventy percent of these nerve injuries will resolve spontaneously. Additionally, the patient should receive a short course of antibiotics as any low velocity GSW would be treated.
Guo et al retrospectively reviewed the electrophysiologic data for 40 radial nerve palsies caused by GSWs and blunt trauma. After characterizing the palsies by level of injury, completeness of nerve injury, and other associated nerves injured, they found there to be no difference in any of these variables between GSW induced radial nerve palsies and blunt trauma induced palsies.
Vaidya et al retrospectively reviewed the outcomes of 54 patients with humeral shaft fractures resulting from low velocity GSWs comparing operative and nonoperative treatments. They found that patients receiving non-operative management did well and that 70% of radial nerve palsies in the non-operative treatment group resolved on their own. They recommended non-operative treatment for the majority of isolated humeral shaft fractures resulting from civilian gunshot wounds.
Figure A is a radiograph of a humeral shaft fracture after a GSW. Illustration A is a radiograph of a humeral shaft fracture with a coaptation in place.
Illustration B is an example of a functional brace.
Incorrect answers:
Answer 1: This is the initial treatment for an open humeral shaft fracture associated with an radial nerve palsy.
Answer 2: Radial nerve palsy from a low velocity GSW is usually axonotmesis. Neurotmesis the most common injury in open fractures.
Answer 4:EMG testing is not indicated until 3-4 months of radial nerve palsy with no neural recovery.
Answer 5: Seventy percent of radial nerve palsies will spontaneously resolve
A 76-year-old male community ambulatory presented to clinic complaining of pain in the left groin that has been persistent for the last 8 months. Radiographs obtained from clinic are seen in Figure A. You suspect a femoral neck nonunion and obtain a CT scan which confirmed it. Which of the following statements is true?
1) Total hip arthroplasty will provide patient with the best long term outcomes
2) Valgus malreduction is closely correlated with failure of fixation after reduction and cannulated screw fixation
3) The patient's best outcome would be with an open reduction, bone grafting, and changing to an inverted triangle configuration of screws
4) The most appropriate treatment is a valgus osteotomy to correct malreduction
5) Providing this patient with a hemiarthroplasty increases rates of postoperative dislocation when comparing to total hip arthroplasty
A total hip arthroplasty (THA) after nonunion of a femoral neck fracture would provide the best long term outcomes in a 76-year-old male who is a community ambulator.
After nonunion of a femoral neck fracture, hemiarthroplasty and THA are good salvage option for the physiologically older patients. When deciding between these two options, THA is better for active and cognitively intact patients. THA is also indicated in patients with radiographic evidence of degenerative disease about the acetabulum. Hemiarthroplasty is advocated for patients who are older and less active.
Yang et al. retrospectively investigated the risk factors for nonunion in patients treated with cannulated screws. They reviewed 202 patients who had femoral neck fractures and were treated with internal fixation with cannulated screws. They identified that triangle configuration, displaced fracture, borderline or unacceptable reduction, and increased screw shaft subchondral purchase over the femoral neck were all risk factors for nonunion after internal fixation.
Inverted triangle configuration was found to increase rate of union.
Archibeck et al. retrospectively reviewed the outcomes of 102 THAs after failed internal fixation for a hip fracture (including both femoral neck and intertrochanteric). They concluded that the conversion of failed hip internal fixation has elevated risks compared to a primary THA, however, it may still be successful. The biggest concern for these patients postoperatively are periprosthetic fracture and dislocation.
Figures and Illustrations:
Figure A is an AP pelvic radiograph demonstrating a nonunion of a femoral neck fracture after suboptimal fixation with 3 cannulated screws in a triangle configuration.
Illustration A is an AP radiograph of the left hip in this patient following conversion to THA.
Illustration B is a radiograph demonstrating a valgus osteotomy. Illustration C shows an example of a femoral neck nonunion with varus malreduction.
Incorrect Answers:
Answer 2: Varus reduction is closely correlated with failure in this fixation method.
Answer 3: The patient's best outcome would be with THA.
Answer 4: This would be a good option in a younger patient, but given age and functional capacity, the best option is THA.
Answer 5: Patients with hemiarthroplasty have lower rates of dislocation.
A 22-year-old male cyclist was struck by a car. He complains of right knee pain and swelling, as well as reduced sensation and weakness in his right foot. His leg compartments are soft and not tender. Distal pulses in the extremity are palpable. Radiographs of the knee, as shown in Figures A and B, were taken after a closed reduction maneuver was performed. What would be the next best step in management of this patient?
1) Non-operative managment, but arrange for early follow-up in clinic
2) Intra-compartmental pressure measurements
3) Ankle-brachial index measurements
4) Knee spanning external fixation
5) Open reduction internal fixation
This patient presents with a Schatzker IV tibia plateau fracture with lower extremity neurologic deficits. The next best step would be to investigate for an acute vascular injury with ankle-brachial index measurements.
Fracture-dislocations of the knee must be suspected with all Schatzker type IV injuries as this fracture pattern is usually associated with high energy trauma. Identifying this injury should prompt a thorough assessment of the neurovascular structures across the knee. After closed reduction and emergent immobilization of the knee, ankle brachial indices (ABI) must be immediately performed. If
A 25-year-old woman sustains a fall on an outstretched hand. She complains of elbow pain. Examination reveals tenderness over the lateral elbow and pain on elbow motion. Injury radiographs and CT scans are shown in Figures A and B, respectively. What is the next best step?
1) Splint until swelling subsides, then long-arm cast
2) Excision of fracture fragments
3) Closed reduction and percutaneous pinning
4) Open reduction and internal fixation (ORIF)
5) Radial head replacement
This patient has Mason II radial head fracture. ORIF will give the best results.
Non-/minimally displaced radial head fractures without a block to rotation can be managed nonoperatively. Complete articular fractures with >=3 fragments do better with radial head replacement. Indications for ORIF include large articular surface fragments, > 2 mm of displacement, mechanical block to forearm rotation, or associated fractures or ligament injuries requiring surgery.
Pike et al. retrospectively compared patients undergoing ORIF for isolated radial head fractures with radial fractures associated with other fractures/dislocations. They found no differences in pain/disability and complications or secondary capsular release between groups.
Yoon et al. retrospectively compared isolated partial articular displaced (2-5mm) radial head fractures treated nonoperatively vs ORIF. They found no clinical benefit with ORIF compared to non-operative management. The ORIF
group had more complications. Younger patient age and larger fracture displacement favored operative intervention. Younger patients fared worse.
Figures A and B are radiographs and 3D reformatted CT images showing a displaced partial articular radial head fracture.
Incorrect Answers:
Answer 1: Nonoperative management is indicated for non-/minimally displaced fractures.
Answer 2: Excision is an option for small partial articular fragments = 3 fragments.
When placing an intramedullary nail for closed distal tibia shaft fractures, all of the following methods are described techniques to aid anatomic reduction EXCEPT:
1) Plating of a concomitant fibula fracture
2) Percutaneous placement of reduction foreceps at the fracture site
3) Placing a Poller screw
4) Placing a small-fragment plate at the fracture site
5) Placing syndesmotic fixation
Of the choices above, syndesmotic fixation would not help anatomically reduce these fractures.
Fractures of the distal tibia are challenging fractures to achieve an anatomic reduction. The medullary canals at either end of the tibia are capacious compared to the mid-diaphysis thus inhibiting an endosteal fit. These fractures have a tendency to become mal-aligned unless certain steps are taken to ensure restoration of the length, alignment, and rotation. Using a Poller or blocking screw can function to narrow the space available for the nail to guide the nail or correct deformity. The use of large pointed-reduction forceps or a small frag plate may also be used for provisional fixation. Additionally, plating concomitant fibula fractures may help indirectly restore length and reduce the tibia fracture. Concomitant syndesmotic injuries are not commonly seen and fixation for these is not required unless stress exam clearly demonstrates it.
Casstevens et al. reviewed the surgical management of distal tibia fractures using either plates/screws or intramedullary nails. Current literature shows near equivalence of either technique regarding union and alignment. They recommend treating each fracture on a case-by-case basis with consideration of the soft tissues and fracture pattern when determining fixation choices.
Tejwani et al. reviewed surgical techniques for managing metaphyseal and meta-diaphysial tibia fractures. Advances in tibial nail design have helped tremendously in negotiating these fractures. Though current supporting literature is based mostly on case series, the use of suprapatellar entry intramedullary nails may help avoid the common deformity of procurvatum and valgus seen with proximal tibia fractures.
Egol et al. retrospectively reviewed distal tibial shaft fracture undergoing intramedullary nailing, with and without concomitant fibula fracture plate fixation. They found fractures with fibular fixation maintained better alignment beyond 12 week post-operatively than those without fixation. Given these findings they recommended fibular plating for all distal tibial shaft fractures.
Illustration A shows a fibula fracture that was plated prior to tibia IMN placement. Illustrations B and C show the use of pointed reduction forceps placed percutaneously to reduce the fracture. Illustration D shows the use of a blocking screw (denoted by the arrow) to keep the nail lateralized and the fracture out of valgus. Illustration E shows the use of a plate to reduce the fracture prior to nail placement.
Incorrect Answers:
Answers 1, 2, 3, and 4: All of these have been described in the literature to help aid in reducing these fractures
A 70-year-old woman falls down a flight of stairs and sustains the injury shown in Figures A and B to her dominant upper extremity. She lives alone and has no other medical history. Which of the following surgical options is best to minimize complications for this fracture pattern?
1) Open reduction and internal fixation with a long locking plate
2) Uncemented reverse total shoulder arthroplasty with tuberosity repair
3) Cemented reverse total shoulder arthroplasty without tuberosity repair
4) Cemented reverse total shoulder arthroplasty with tuberosity repair
5) Proximal humeral resection with endoprosthetic replacement
This patient has a complex proximal humerus fracture with metaphyseal comminution and poor bone stock. Cemented reverse total shoulder arthroplasty (rTSA) using a long stem prosthesis and tuberosity repair is indicated.
Proximal humerus fragility fractures are hard to treat because of comminution and poor bone stock. AVN is common with glenohumeral fracture-dislocation. Hemiarthroplasty (and standard total shoulder arthroplasty, TSA) is unreliable because of dependence on tuberosity healing. rTSA is recommended for fractures in patients >70 years with severely comminuted fractures, high likelihood of head AVN, and poor tuberosity bone quality (osteoporosis or comminution).
Bufquin et al. retrospectively reviewed the use of rTSA for treatment of 43 patients with 3- and 4-part proximal humerus fractures. They found satisfactory elevation (97°), ER in abduction (30°), constant scores (44) and modified Constant scores (66%). Complications included calcification (90%), tuberosity displacement (53%) and scapular notching (25%). They concluded that rTSA was a good procedure because it provides pain relief and easier functional recovery in spite of failed tuberosity healing.
Anakwenze et al. systematically reviewed acute proximal humerus fractures. Frequency weighted range of motion was flexion 122°, abduction 97°, ER at neutral 18°. Tuberosity repair yielded higher ER compared to no repair.
Scapular notching was the most common complication (32%). They concluded that rTSA patients tended to be elderly women with 4-part fractures, had good pain control but residual dysfunction.
Jobin et al. reviewed rTSA for management of proximal humerus 3- and 4-part fractures. They note >50% of cases have tuberosity resorption. They recommend repairing the greater tuberosity to restore infraspinatus/teres minor function which improves external rotation strength. Greater tuberosity malunion is not a result of secondary displacement, but rather, from intraoperative malreduction. Lesser tuberosity repair should be performed if there is significant bone loss or intraoperative anterior instability.
Figures A and B are AP radiograph and 3D reformatted CT scan showing comminuted proximal humerus fracture dislocation. Illustration A shows rTSA performed with distal cementation of a long stem prosthesis and cerclage fixation of the proximal shaft and the tuberosity fragments.
Incorrect Answers:
Answer 1: ORIF has potential complications of screw cut out, AVN, fracture collapse, tuberosity resorption and loss of fixation. The risk of AVN (and resultant screw cut out) is high because of comminuted fracture-dislocation. Answer 2: Cementing is indicated because metaphyseal fracture bone loss compromises stem fixation.
Answer 3: Greater tuberosity repair improves external rotation strength. Lesser tuberosity repair adds to anterior stability.
Answer 5: Proximal humeral replacement is only necessary for tumor or unreconstructable fractures. They have poorer outcomes because of loss of rotator cuff function.
A 26-year-old male underwent statically locked intramedullary nail fixation for a comminuted left femur fracture. An early post-
operative computed tomography (CT) scanogram was taken to check rotational alignment, as shown in Figure A. What would be the next best step in the management of this patient?
1) Observation and close follow-up
2) Dynamization of the intramedullary nail
3) Revision surgery, internally rotate distal fragment by 19 degrees
4) Revision surgery, externally rotate distal fragment by 8 degrees
5) Revision surgery, internally rotate proximal fragment by 11 degrees
The CT scanogram shows the operative left femur is 8 degrees externally rotated compared to the native right femur. No correction is required unless malalignment is >15 degrees and symptomatic. Therefore, the most appropriate next step would be to continue with postoperative observation and close follow-up.
The primary purpose of CT scanogram is to measure the angle of rotation of the femoral neck relative to the femoral condyle. To do this, the right and left femurs must be scanned together using a 5mm helical slice scanner at the hip and knee. The first slice should reveal the alignment of the femoral neck, so as to allow for measurement of the femoral neck-to-horizontal (FNH) angle. The second slice should reveal the alignment of the posterior femoral condyles.
This allows measurement of the posterior condyle-to-horizontal (PCH) angle. Finally, to calculate the rotational alignment (RA), the FNH angle and PCH angles are subtracted (e.g., RA = FNH - PCH). Normal RA is usually +5 to +20 degrees, which is also referred to as 5 to 20 degrees of femoral anteversion.
Lindsey et al. reviewed femoral malrotation following intramedullary nail fixation. They showed the incidence of rotational malalignment was ~28%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is ~11-13°. However, they noted that some patients have up to 15° difference in rotation in native limbs.
Therefore 15 degrees and symptomatic.
Which of the following images shows an injury pattern most consistent with a lateral compression type 3 pelvic ring injury?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Figure C is an axial CT scan of a lateral compression type 3 (LC3) pelvic ring injury.
Classically, LC3 injuries demonstrate an ipsilateral lateral compression and a contralateral APC (windswept pelvis) fracture pattern. The most common mechanism of injury in these cases is a rollover MVC or pedestrian vs. auto. LC1 injuries are characterized by an oblique or transverse ramus fracture and ipsilateral anterior sacral ala compression fracture, while LC2 injuries consist of a rami fracture and ipsilateral posterior ilium fracture dislocation (crescent fracture). While LC1 injuries can often initially be managed conservatively with protected weight-bearing and close observation, LC2 and LC3 pelvic ring injuries are almost universally operative.
Pennal et al. discuss a radiologic technique for assessing the forces producing pelvic disruption and its use in logically classifying pelvic injury. Based on this radiologic assessment and along with some biomechanical studies, they propose a classification system involving three major forces producing injury that can also be helpful in the management of these patients.
Young et al. performed a retrospective analysis of the plain radiographs of 142 cases of pelvic fractures and identified four patterns of force that presented with distinctive, recognizable radiographic appearances. They describe a classification system for pelvic fractures based on radiographic and clinical findings that correlates with associated injury to soft-tissue structures and enables the surgeon to begin corrective procedures rapidly.
Incorrect Answers:
Answer 1: This represents a lateral compression type 2 injury. Answer 2: This represents a lateral compression type 1 injury.
Answer 4: This represents an anterior posterior compression type 2 injury. Answer 5: This represents an anterior posterior compression type 3 injury.
For a patient with an unstable pelvic fracture, the amount of blood tranfusions required in the first 24 hours has shown to be most predictive for what variable?
1) Length of hospital stay
2) Association with neurological deficit(s)
3) Length of intensive care stay
4) Cardiac collapse
5) Mortality
Unstable pelvic fractures can be devastating injuries often resulting in significant morbidity and even death.
According to the referenced study by Smith et al, fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased ISS or RTS scores. Deaths were most commonly from exsanguination (24 hours).
Incorrect Answers: Choices 1-4 do not correlate with increased blood transfusions to the extent of Option 5.
A healthy 27 year-old-male is brought into the emergency department after a fall from height. He has a suspected left C8-T1 nerve injury. Which of the following findings would most suggest a root avulsion injury rather than a brachial plexus injury at this level?
1) Reduced radial artery pulse
2) Double break in the ipsilateral superior shoulder suspensory complex
3) Elevated hemidiaphragm
4) Musculocutaneous nerve deficit
5) Drooping of the left eyelid
Drooping of the left eyelid is a presenting feature of Horner's syndrome. Horner's syndrome represents a disruption of the sympathetic chain via C8 and/or T1 root avulsion after trauma.
Brachial plexus injuries are often classified as preganglionic vs. postganglionic injuries. Preganglionic injuries are typically avulsion injuries proximal to the dorsal root ganglion. Clinical features suggestive of lower root avulsion injury include a person falling from height clutching on object to save himself, Horner’s syndrome (drooping of the eyelid (ptosis), pupillary constriction (miosis) and anhidrosis), absence of a Tinel sign or tenderness to percussion in the neck, and a normal histamine test (C8-T1 sympathetic ganglion - intact triple response (redness, wheal, flare)).
Caporrino et al. reviewed 102 patients to assess the best modality (e.g. physical examination, MRI and nerve conduction studies [NCSs]) for diagnosing and localizing brachial plexus injuries. They found the best diagnostic performance with physical examination (sensitivity = 97.8%; specificity = 30.8%) and NCSs (sensitivity = 98.9%; specificity = 23.1%). MRI had inferior performance for all measurements. They conclude that NCSs exhibited superior performance to MRI, and should be considered a more reliable supporting tool after detailed physical examination.
Incorrect Answers:
Answer 1, 2: The superior shoulder suspensory complex (SSSC) is located in close proximity to the brachial plexus. Disruption of the SSSC may affect the local anatomy and cause local brachial plexus or vascular injury.
Answer 3: Elevated hemidiaphragm (Phrenic nerve C3,4,5) may be suggestive an upper brachial plexus root avulsion, e.g. C5, C6 injury.
Answer 4: Musculocutaneous nerve deficiency (C5 deficiency) results in weakness to the biceps.
A 46-year-old competitive cyclist falls while racing and suffers an isolated fracture as seen in Figure A. He is positioned on a fracture table and a closed reduction maneuver is attempted, unsuccessfully.
Which of the following treatment plans is most appropriate?
1) Obtain a CT scan intraoperatively to reassess the quality of reduction
2) Perform additional closed reduction maneuvers until the reduction is adequate for percutaneous fixation
3) As long as the stepoff is less than 7mm in any plane of imaging, it is appropriate to proceed with percutaneous fixation
4) Perform an open reduction and internal fixation using a sliding hip screw
5) Perform an acute total hip arthroplasty through a direct anterior approach since the patient is on the fracture table
When standard closed reduction maneuvers using a traction table are unsuccessful, displaced femoral neck fracture in young adults (10 degrees varus/valgus or anteversion/retroversion) or has
significant displacement (5 mm or more in ANY view) is unacceptable, and an open reduction should be performed. Of course, this can be very difficult to assess in the operating room, where uncalibrated fluoroscopy with difficult to obtain tangential imaging is heavily relied upon to make this assessment.
Accordingly, when the quality of closed reduction is questionable, the best treatment plan is to obtain a better reduction with direct visualization of the femoral neck prior to fixation.
A systematic review of the literature by Pauyo, et al. cites numerous studies showing a higher incidence of osteonecrosis of the femoral head in patients with displaced femoral neck fractures treated with unsatisfactory reductions. Furthermore, performing multiple closed reduction attempts is also associated with a higher risk of osteonecrosis.
Upadhyay et al. performed a randomized controlled trial of 102 patients with femoral neck fractures treated with closed or open reductions, which were randomized. The groups had similar rates of nonunions and osteonecrosis of the femoral head; however, subanalysis revealed a "poor" reduction was the highest predictor of poor outcome, whether the reduction was attempted open or closed. Interestingly, the quality of reduction was more important than the implant used or the timing of surgery (including surgeries performed > 48h after injury).
Figure A shows a pre-operative AP x-ray of the patient's high-energy femoral neck fracture. Illustrations A and B are intraoperative fluoroscopic and postoperative CT scans of this same patient, highlighting that fluoroscopy may "hide" the degree of residual displacement.
Incorrect Answers:
Knee dislocations are associated with popliteal artery injury in 18-45% of cases and range from intimal tears to complete transection. Amputation rates of 85% have been reported if revascularization is delayed greater than 6 to 8 hours.
Neurologic injury occurs in 15-40% of cases and is most common after posterolateral dislocation. The peroneal nerve is more commonly injured.
Rihn et al. reviewed the acutely dislocated knee. They recommend a vascular consult if pulses are weak, or ABI is compromised. They warn that in arterial injury, pulses, temperature and capillary refill can be normal. If the limb remains ischemic, surgical exploration and revascularization is indicated.
Medina et al. systematically reviewed neurovascular injury after knee dislocation in 862 patients. Vascular injury rate was 18%, and nerve injury rate was 25%. Repair was performed in 80% of vascular injuries, and amputation in 12%. The most vascular injury was seen in KDIIIL injuries (32%) and posterior dislocation (25%).
Figure A is an AP radiograph of a posterior knee dislocation. Figure B is a lateral showing the same injury.
Incorrect Answers:
: The limb remains ischemic. Splinting and observation alone are inappropriate.
Answer 3: External fixation is appropriate for immobilization following reduction, especially for very obese patients (BMI>50) where casting/splinting is not possible, and especially to protect a vascular reconstruction. However, the MOST important next step is vascular exploration to attempt revascularization.
Answers 4 and 5: CT angiography and standard angiography will only serve to delay vascular exploration of the ischemic limb. On-table angiograms will be performed during the surgery, obviating the need for preoperative angiography outside the operating room (OR).
A 51-year-old carpenter presents with a distal humerus nonunion (Figures A and B). After repair of the nonunion, he is lost to follow up for 3 months and then presents to your clinic pain-free and with evidence of fracture union. On examination the elbow arc of motion is 10-80 degrees. Following a brief failed trial of conservative management, you recommend:
1) Open release of the posterior bundle of the MCL and excision of osteophytes
2) Complete open release of the MCL and LCL complexes with radiation for heterotopic ossification prophylaxis
3) Arthroscopic release of the anterior capsule with removal of hardware
4) Removal of hardware and dome osteotomy
5) Functional bracing and recommendation for job retraining
Limited flexion outside a functional range of motion (30-130 degrees) can be quite debilitating, and it is often addressed with open release of the posterior bundle of the MCL and posterior capsule and excision of osteophytes.
A frequent complication of distal humerus fractures is post-traumatic stiffness. This patient has had multiple procedures about the distal humerus, and the question stem implies that he did not complete a structured range of motion protocol following the repair of his nonunion. Beyond a trial of conservative management, there are many techniques described for capsule and soft tissue releases as well as bony resections if heterotopic ossification is present. This patient's severely limited flexion would best be addressed with a release of the posterior bundle of the MCL, and with flexion
A 51-year-old female presents with an acute inability to extend her thumb, four months after she was treated with cast immobilization for a minimally-displaced distal radius fracture. What is the most appropriate treatment at this time?
1) Occupational therapy for strengthening
2) Extensor carpi radialis longus transfer to extensor pollicus longus
3) Extensor pollicis brevis transfer to extensor pollicus longus
4) Extensor indicis proprius transfer to extensor pollicus longus
5) Primary repair of extensor pollicus longus
A rare complication of non-displaced or minimally displaced fractures of the distal radius treated with a cast is a delayed rupture of the extensor pollicis longus (EPL) tendon. The EPL is the primary extensor of the interphalangeal joint of the thumb and also assists with metacarpophalangeal extension.
Extensor indicis proprius transfer to the EPL is the most widely used and reported treatment for this condition.
Magnussen et al. reviewed results of EIP transfer following ruptures of the EPL, with 19/21 good results. None of the cases had any loss of independent index finger extension although index extensor strength reduced to half of that of the contralateral side.
Hove et al. reported a similar satisfaction rate following treatment of 15 patients. In his series of 4,400 distal radius fractures treated over a 5 year period, the incidence of delayed tendon rupture following distal radius fracture was 0.3 percent.
A 25-year-old female is involved in a motor vehicle collision. She presents with the isolated injury seen in Figures A through D. Her leg is swollen but her skin is intact. She has no clinical signs of compartment syndrome. Which of the following treatment options will allow for maintenance of fracture alignment and minimize the risk of soft tissue complications?
1) Closed reduction and long-leg non-weight bearing cast
2) Immediate open reduction of the tibia through an anterolateral approach
3) Percutaneous fixation of the articular surface and intramedullary nailing
4) Definitive uniplanar external fixator
5) Immediate open reduction of the tibia through an anteromedial approach
The patient presents with a closed distal third metaphyseal-diaphyseal distal tibia fracture with simple intra-articular extension. Immediate intramedullary nailing along with percutaneous fixation of the articular component provides appropriate restoration of length, rotation and alignment and minimizes the risk of wound complication.
Displaced distal third tibia fractures may be associated with simple intraarticular extension. Operative treatment of intra-articular distal tibia fractures has historically been performed with open reduction and internal fixation. Early open reduction and plate fixation of pilon fractures has been associated with high rates of infection and wound complication. In select patterns with simple articular extension, percutaneous screw fixation and medullary nailing may provide appropriate reduction with minimal soft-tissue risk.
Marcus et al. evaluated the outcomes of immediate intramedullary nailing and percutaneous fixation of simple intra-articular distal tibia fractures (AO/OTA 43 C1 and C2). The authors found excellent rates of union and alignment, however caution against broad application of this technique until more rigorous randomized studies can be performed.
Sirkin et al. retrospectively evaluated the results of a staged approach to management of intra-articular distal tibia fractures with temporary bridging external fixation followed by open reduction and internal fixation (ORIF). The authors found decreased rates of wound complication and infection compared with prior studies.
Figures A and B demonstrate a distal third tibial shaft fracture with simple intra-articular extension. The axial and coronal CT cuts in Figures C and D further clarify the articular injury. Illustrations A and B demonstrate a comminuted distal third tibial fracture with simple intra-articular extension. Illustrations C and D are fluoroscopic images of the same injury after intramedullary nailing and percutaneous fixation of the articular component.
Incorrect Answers:
Answer 1: Closed reduction and casting of this injury results in increased rates of malalignment
Answers 2 and 5: Immediate open reduction of pilon fractures has historically been associated with high rates of infection and wound complications
Answer 4: This fracture pattern would be difficult to control with a uniplanar fixator. A circular or multiplanar fixator would be a potential treatment option
A 24-year-old woman is thrown from her motorcycle and sustains the closed injury shown in Figures A through C. Open reduction and internal fixation is planned. What surgical technique will best allow visualization of the joint surface and allow early range of motion?
1) Bryan-Morrey approach and parallel plating
2) Triceps reflecting anconeus pedicle approach and parallel plating
3) Triceps reflecting anconeus pedicle approach and orthogonal plating on the posteromedial and lateral surfaces
4) Olecranon osteotomy and parallel plating
5) Olecranon osteotomy and orthogonal plating on the posteromedial and lateral surfaces
Access to complex intra-articular fractures is best achieved by an olecranon osteotomy (OO). Fixation can be with parallel plating or orthogonal plating.
Bicolumnar fixation of distal humerus fractures should follow the principles outlined by O'Driscoll: Distal fragments should be held by as many screws as possible; every screw in the distal fragments should pass through a plate; each screw should engage as many articular fragments as possible.
Galano et al. review treatment for bicolumnar distal humerus fractures. They note that the olecranon osteotomy, Alonso-Llames triceps sparing and Campbell triceps splitting approaches expose 57%, 46% and 35% of the articular surface, respectively. The OO and paratricipital (triceps sparing)
approaches allow for early ROM. Protected motion is required for the O'Driscoll TRAP and Bryan-Morrey approaches for tendon-to-bone healing.
Coles et al. retrospectively reviewed the OO in fixation of 70 fractures. Osteotomy fixation was with an intramedullary screw and dorsal ulnar wiring, or with a plate. The rate of OO increased with fracture difficulty (from AO type C1-C3). There was 1 delayed union but no nonunions.
Figures A and B show a AO/OTA type C2 intraarticular distal humerus fracture. Figure C is a coronal CT scan showing intraarticular comminution. Illustration A shows fixation of the fracture with bicolumnar plating through an olecranon osteotomy approach. Illustration B shows the various approaches to the distal humerus (left, Campbell triceps splitting; center left, O'Driscoll triceps reflecting anconeus pedicle; center right, Bryan-Morrey approach, leaving the triceps attached laterally to the fasciocutaneous flap, but elevating it off the ulna; right, olecranon osteotomy). Illustration C shows 3 methods of olecranon osteotomy (A and B, Intra-articular transverse; C-F, Extra-articular oblique; G, Intra-articular chevron).
Incorrect Answers:
Answer 1: The Bryan-Morrey approach provides excellent medial exposure, but inadequate lateral exposure. The triceps is lifted subperiosteally, and the anconeus is released subperiosteally. Triceps repair depends on tendon-bone healing.
Answer 2: The O'Driscoll TRAP approach detaches triceps and anconeus from their distal insertions in a V-shaped flap that is reflected proximally. Repair to bone is via drill holes in the ulna. Early mobilization is not recommended.
Answers 3 and 5: Orthogonal plating is performed on the POSTEROLATERAL and MEDIAL surfaces.
A 31-year-old male sustains an isolated handgun injury shown in Figure A. On physical examination, he has a 0.5 cm wound over the anteromedial aspect of his thigh, with no gross contamination of the skin edges. He is neurovascularly intact. The patient has received tetanus prophylaxis and antibiotics in the emergency department.
What would next best step in treatment?
1) External fixation and IV antibiotics for 6 weeks
2) Irrigation and debridement of wound and external fixation for 6 weeks
3) Reamed antegrade or retrograde intramedullary nail
4) Irrigation and debridement of wound, reamed antegrade nail and IV antibiotics for 6 weeks
5) Irrigation and debridement of wound, reamed retrograde nail and IV antibiotics for 6 weeks
This patient has sustained a low-velocity gunshot to the right femoral diaphysis. The next best step in treatment would be insertion of a reamed antegrade or retrograde intramedullary nail. During surgery, the gunshot wound could be closed primarily if it was considered clean, or allowed to heal by secondary intention if it was there was any concern.
Low-velocity gunshot wounds are typically treated as closed fractures, since the risk of osteomyelitis is very low. These are typically bullets from handguns that travel 600 meters per second). The timing and direction (e.g. antegrade or retrograde) of nail insertion has not shown to
affect outcomes.
Cannada et al. reviewed 74 cases of femoral diaphyseal fractures caused by gunshots. All were treated with reamed, retrograde, statically locked intramedullary nailing, without formal irrigation and debridement in the operating room. Outcomes showed low incidence of shortening, angular deformity and infection rate.
Dougherty et al. compared retrograde vs. antegrade intramedullary nailing for the treatment of gunshot diaphyseal femur fractures. No significant differences were found between groups with regards to operative time, blood loss, or radiographic union. They conclude that immediate retrograde or antegrade nailing is safe for the early treatment of gunshot femur fractures.
Figure A shows an AP radiograph of the right femur. There is a gunshot fracture in the proximal femoral shaft with retained bullet fragments. The leg has been placed in temporary traction.
Incorrect Answers:
Answer 1: External fixation would be considered for treatment of femur fractures in damage control orthopaedics.
Answer 2: IV antibiotics for 6 weeks would not be necessary with low velocity gunshot wounds with clean wounds.
Answer 4 and 5: The direction of nail entry does not seem to affect outcomes with these fractures. Irrigation and debridement of wound, as well as IV antibiotics, wound not be necessary, aforementioned.
Figure A shows a radiograph of a 19-year-old male with an isolated shotgun injury. On physical examination, he has a 3 cm wound over the posterolateral aspect of his arm. In addition, he has weakness with wrist and finger extension, but no sensory deficits. The patient has received tetanus prophylaxis and antibiotics in the emergency department. What would be the next best steps in treatment?
1) Urgent open reduction internal fixation and fibular osteoseptocutaneous flap
2) Irrigation and debridement and external fixation
3) Irrigation and debridement, repair of the radial nerve and retrograde intramedullary nail
4) CT scan, urgent open reduction internal fixation and IV antibiotics for 6 weeks
5) Closed reduction, CT scan, immobilization in a coaptation splint
This patient has sustained a shotgun blast to the midshaft humerus. The next best step would be irrigation and debridement, and external fixation of the fracture.
Shotgun injuries are typically treated as open fractures, whereas low-energy gunshot wounds are treated as closed fractures. The initial operative treatment of shotgun wounds should include irrigation and debridement and stabilization with external fixation. The goal of treatment is to stabilize the severe soft-tissue injury and bone loss, as well as to aggressively debride devitalized tissue and gross contamination.
Dougherty et al. reviewed gunshot fractures to the humerus. They report that
peripheral nerve injuries are relatively common with these injuries, with a more common incidence in distal injuries than proximal.
Joshi et al. looked at low velocity gunshot fractures to the humerus. They found that these injuries can be safely treated as closed fractures with local wound care, fracture brace and oral antibiotics. The time to union was similar in the non-operative and open treatment group.
Berick et al. examined the indications for nerve exploration with humerus gunshot fractures. They recommend continued observation of isolated nerve palsies associated with gunshot fractures of the humerus. However, consider early nerve exploration of palsies when associated with a concomitant vascular injury.
Figure A shows a high velocity shotgun fracture to the left humerus with retained buck fragments. Illustration A shows a similar injury stabilized with external fixation.
Incorrect Answers:
Answer 1: Due to the severity of soft tissue injury, external fixation should be considered for initial stabilization. Vascularized fibular grafts has been expanded to an osteoseptocutaneous flap by including a cutaneous flap on the lateral aspect of the lower leg. These are not typically used in the acute setting.
Answer 3: Retrograde intramedullary nail would not be the ideal implant for this injury, acutely.
Answer 4 and 5: There is no indication for a CT scan or prolonged antibiotics. The fracture and soft-tissue injury should be initially stabilized with external fixation. Coaptation splinting will interfere with soft tissue care.
A 34-year-old male sustains the closed injury seen in Figure A as a result of a high-speed motor vehicle collision. What is the most appropriate next step in treatment?
1) Open reduction and internal fixation
2) Spanning external fixation
3) Percutaneous internal fixation
4) Closed reduction and cast placement
5) Ankle arthrodesis
The radiograph shows a comminuted pilon fracture, which is associated with high-energy trauma and significant soft tissue injury. The tested concept here is the importance of avoiding definitive reduction and fixation of this high-energy injury, which has been shown to be associated with an increased risk of wound complications and deep infections (as compared to staged treatment with usage of a spanning external fixator).
Patterson et al. reviewed 23 consecutive patients with comminuted distal tibia fractures. They showed 0% infections or wound-healing problems in their patient population treated with a two-staged protocol. Their protocol involved fibula fixation with an intramedullary implant and application of a medial external fixator to to regain length and restore anatomic alignment. Reevaluation of the limb occurred ten to fourteen days later for definitive fixation.
Sirkin et al. retrospectively reviewed 40 closed and 17 open pilon fractures (AO types 43A-C) that were treated with staged surgical management (avg. time from ext. fix. to formal reconstruction was 14 days (range 4 to 31) They reported 17% post-operative wound complication in the closed group and 11% post-operative wound complication in the open group (Gustilo Type I-III). They suggest the technique was successful in both closed and open pilon fractures.
A 72-year-old woman falls down stairs and sustains the injury shown in Figure A. Additional radiographs are performed in Figure B to help assess the fracture pattern. These additional radiographs represent which of the following?
1) Oblique radiographs
2) In-situ radiographs under anesthesia
3) Traction radiographs
4) Fracture flexion radiographs
5) Fracture extension radiographs
Additional traction radiographs are performed in distal humerus fractures to better understand the fracture configuration.
Traction radiographs help align the fracture fragments for better visualization. This is useful in comminuted fractures where distal fragments are telescoped or flexed on the proximal fragments, making CT scan visualization difficult.
Proper visualization can help determine (1) the approach to the distal humerus, (2) whether to perform ORIF or total elbow arthroplasty (in select patients), (3) whether to add a 3rd plate (lateral column), (4) whether to add tricortical bone graft to augment distal fixation and restore trochlear width.
Doornberg et al. examined whether 3D CT improved fracture characterization. They found that 3D CT improved interobserver and intraobserver reliability for fracture characterization and classification. It also improved intraobserver accuracy for fracture characteristics, but not interobserver accuracy. They concluded that 3D CT is helpful for preoperative planning.
Galano et al. reviewed treatment strategies for bicolumnar distal humerus fractures. They state that 3D CT compensates for oblique scans from formatting in an incorrect plane, and allows for subtraction of the radius/ulna to properly demonstrate articular incongruity, degree of comminution and column involvement.
Figures A and B show a distal humerus fracture without traction (A) and with traction (B) applied. Illustration A shows the same fracture after bicolumnar plating. Illustration B shows the different surgical approaches to the distal humerus (A, Campbell triceps splitting; B, O'Driscoll triceps reflecting anconeus pedicle [TRAP]; C, Bryan-Morrey triceps reflecting; D, olecranon osteotomy)
Incorrect Answers:
Answer 1: These radiographs aren't oblique images.
Answer 2: Radiographs under anesthesia do not add further information unless traction is applied.
Answers 4 and 5: Flexion and extension will further impact and displaced fragments and will not improve alignment.
Mirror therapy is indicated for which of the following clinical conditions?
1) Impaired proprioception after lower extremity injury
2) Two-stage flexor tendon reconstruction
3) Plumbism
4) Anterior cruciate ligament reconstruction
5) Phantom pain
Mirror therapy is a useful technique to improve phantom pain in amputees. Phantom limb pain is a painful sensation that is perceived within a body part that no longer exists.
Under mirror therapy, a patient is allowed to feel the imaginary movement of the removed body part behaving as normal body movement through a mirror. The mirror image of the normal body part helps reorganize and integrate the mismatch between proprioception and visual feedback of the amputated segment.
Tilak et al. performed a randomized controlled trial of 26 patients with phantom limb pain, and found that mirror therapy as well as transcutaneous electrical nerve stimulation both significantly improved pain scores, but no difference was seen between the two groups. They recommend use of both modalities in treatment of phantom limb pain, as they are noninvasive and inexpensive.
Chan et al. reviewed 22 patients utilizing mirror therapy for amputation related phantom limb pain, and found that patients reported a significant decrease in pain when utilizing this treatment modality as compared to covered mirror therapy or mental imagery therapy.
Illustration A shows a patient with an upper extremity amputation using a mirror to perform movements during a mirror therapy session.
Incorrect Answers:
Answer 1: Mirror therapy is not indicated for proprioception training. Answer 2: Mirror therapy is not indicated for flexor tendon injuries. Answer 3: Mirror therapy is not indicated for lead poisoning.
Answer 4: Mirror therapy is not indicated for ACL reconstruction.
A patient presents to the emergency department with the injury seen in Figure A. Which of the following is true about radial nerve palsies associated with isolated humeral shaft fractures after low velocity gunshot wounds?
1) The initial treatment involves debridement, irrigation, nerve exploration, and osteosynthesis.
2) The radial nerve palsy is often a result of neurotmesis.
3) Initial treatment involves splinting and observation for return of neurologic function.
4) Electrophysiologic testing for radial nerve palsies is indicated after 2-3 weeks without improvement.
5) The radial nerve palsy will not resolve regardless of attempted interventions.
When a patient sustains an isolated humeral shaft fracture and radial nerve palsy from a GSW, the initial treatment involves splinting with observation.
The majority of humeral shaft fractures are treated initially with a coaptation splint and then transitioned to a functional brace. Absolute surgical indications for operative management include: open fracture, brachial plexus injury, compartment syndrome, floating elbow, or vascular injury. A radial nerve palsy is not an indication for surgical management of an isolated humeral shaft fracture. Radial nerve injury from a low-velocity GSW is similar to that of blunt force trauma and thus, immediate exploration is not necessary. Instead, nerve function should be observed. Seventy percent of these nerve injuries will resolve spontaneously. Additionally, the patient should receive a short course of antibiotics as any low velocity GSW would be treated.
Guo et al retrospectively reviewed the electrophysiologic data for 40 radial nerve palsies caused by GSWs and blunt trauma. After characterizing the palsies by level of injury, completeness of nerve injury, and other associated nerves injured, they found there to be no difference in any of these variables between GSW induced radial nerve palsies and blunt trauma induced palsies.
Vaidya et al retrospectively reviewed the outcomes of 54 patients with humeral shaft fractures resulting from low velocity GSWs comparing operative and nonoperative treatments. They found that patients receiving non-operative management did well and that 70% of radial nerve palsies in the non-operative treatment group resolved on their own. They recommended non-operative treatment for the majority of isolated humeral shaft fractures resulting from civilian gunshot wounds.
Figure A is a radiograph of a humeral shaft fracture after a GSW. Illustration A is a radiograph of a humeral shaft fracture with a coaptation in place.
Illustration B is an example of a functional brace.
Incorrect answers:
Answer 1: This is the initial treatment for an open humeral shaft fracture associated with an radial nerve palsy.
Answer 2: Radial nerve palsy from a low velocity GSW is usually axonotmesis. Neurotmesis the most common injury in open fractures.
Answer 4:EMG testing is not indicated until 3-4 months of radial nerve palsy with no neural recovery.
Answer 5: Seventy percent of radial nerve palsies will spontaneously resolve
A 76-year-old male community ambulatory presented to clinic complaining of pain in the left groin that has been persistent for the last 8 months. Radiographs obtained from clinic are seen in Figure A. You suspect a femoral neck nonunion and obtain a CT scan which confirmed it. Which of the following statements is true?
1) Total hip arthroplasty will provide patient with the best long term outcomes
2) Valgus malreduction is closely correlated with failure of fixation after reduction and cannulated screw fixation
3) The patient's best outcome would be with an open reduction, bone grafting, and changing to an inverted triangle configuration of screws
4) The most appropriate treatment is a valgus osteotomy to correct malreduction
5) Providing this patient with a hemiarthroplasty increases rates of postoperative dislocation when comparing to total hip arthroplasty
A total hip arthroplasty (THA) after nonunion of a femoral neck fracture would provide the best long term outcomes in a 76-year-old male who is a community ambulator.
After nonunion of a femoral neck fracture, hemiarthroplasty and THA are good salvage option for the physiologically older patients. When deciding between these two options, THA is better for active and cognitively intact patients. THA is also indicated in patients with radiographic evidence of degenerative disease about the acetabulum. Hemiarthroplasty is advocated for patients who are older and less active.
Yang et al. retrospectively investigated the risk factors for nonunion in patients treated with cannulated screws. They reviewed 202 patients who had femoral neck fractures and were treated with internal fixation with cannulated screws. They identified that triangle configuration, displaced fracture, borderline or unacceptable reduction, and increased screw shaft subchondral purchase over the femoral neck were all risk factors for nonunion after internal fixation.
Inverted triangle configuration was found to increase rate of union.
Archibeck et al. retrospectively reviewed the outcomes of 102 THAs after failed internal fixation for a hip fracture (including both femoral neck and intertrochanteric). They concluded that the conversion of failed hip internal fixation has elevated risks compared to a primary THA, however, it may still be successful. The biggest concern for these patients postoperatively are periprosthetic fracture and dislocation.
Figures and Illustrations:
Figure A is an AP pelvic radiograph demonstrating a nonunion of a femoral neck fracture after suboptimal fixation with 3 cannulated screws in a triangle configuration.
Illustration A is an AP radiograph of the left hip in this patient following conversion to THA.
Illustration B is a radiograph demonstrating a valgus osteotomy. Illustration C shows an example of a femoral neck nonunion with varus malreduction.
Incorrect Answers:
Answer 2: Varus reduction is closely correlated with failure in this fixation method.
Answer 3: The patient's best outcome would be with THA.
Answer 4: This would be a good option in a younger patient, but given age and functional capacity, the best option is THA.
Answer 5: Patients with hemiarthroplasty have lower rates of dislocation.
A 22-year-old male cyclist was struck by a car. He complains of right knee pain and swelling, as well as reduced sensation and weakness in his right foot. His leg compartments are soft and not tender. Distal pulses in the extremity are palpable. Radiographs of the knee, as shown in Figures A and B, were taken after a closed reduction maneuver was performed. What would be the next best step in management of this patient?
1) Non-operative managment, but arrange for early follow-up in clinic
2) Intra-compartmental pressure measurements
3) Ankle-brachial index measurements
4) Knee spanning external fixation
5) Open reduction internal fixation
This patient presents with a Schatzker IV tibia plateau fracture with lower extremity neurologic deficits. The next best step would be to investigate for an acute vascular injury with ankle-brachial index measurements.
Fracture-dislocations of the knee must be suspected with all Schatzker type IV injuries as this fracture pattern is usually associated with high energy trauma. Identifying this injury should prompt a thorough assessment of the neurovascular structures across the knee. After closed reduction and emergent immobilization of the knee, ankle brachial indices (ABI) must be immediately performed. If
A 25-year-old woman sustains a fall on an outstretched hand. She complains of elbow pain. Examination reveals tenderness over the lateral elbow and pain on elbow motion. Injury radiographs and CT scans are shown in Figures A and B, respectively. What is the next best step?
1) Splint until swelling subsides, then long-arm cast
2) Excision of fracture fragments
3) Closed reduction and percutaneous pinning
4) Open reduction and internal fixation (ORIF)
5) Radial head replacement
This patient has Mason II radial head fracture. ORIF will give the best results.
Non-/minimally displaced radial head fractures without a block to rotation can be managed nonoperatively. Complete articular fractures with >=3 fragments do better with radial head replacement. Indications for ORIF include large articular surface fragments, > 2 mm of displacement, mechanical block to forearm rotation, or associated fractures or ligament injuries requiring surgery.
Pike et al. retrospectively compared patients undergoing ORIF for isolated radial head fractures with radial fractures associated with other fractures/dislocations. They found no differences in pain/disability and complications or secondary capsular release between groups.
Yoon et al. retrospectively compared isolated partial articular displaced (2-5mm) radial head fractures treated nonoperatively vs ORIF. They found no clinical benefit with ORIF compared to non-operative management. The ORIF
group had more complications. Younger patient age and larger fracture displacement favored operative intervention. Younger patients fared worse.
Figures A and B are radiographs and 3D reformatted CT images showing a displaced partial articular radial head fracture.
Incorrect Answers:
Answer 1: Nonoperative management is indicated for non-/minimally displaced fractures.
Answer 2: Excision is an option for small partial articular fragments = 3 fragments.
When placing an intramedullary nail for closed distal tibia shaft fractures, all of the following methods are described techniques to aid anatomic reduction EXCEPT:
1) Plating of a concomitant fibula fracture
2) Percutaneous placement of reduction foreceps at the fracture site
3) Placing a Poller screw
4) Placing a small-fragment plate at the fracture site
5) Placing syndesmotic fixation
Of the choices above, syndesmotic fixation would not help anatomically reduce these fractures.
Fractures of the distal tibia are challenging fractures to achieve an anatomic reduction. The medullary canals at either end of the tibia are capacious compared to the mid-diaphysis thus inhibiting an endosteal fit. These fractures have a tendency to become mal-aligned unless certain steps are taken to ensure restoration of the length, alignment, and rotation. Using a Poller or blocking screw can function to narrow the space available for the nail to guide the nail or correct deformity. The use of large pointed-reduction forceps or a small frag plate may also be used for provisional fixation. Additionally, plating concomitant fibula fractures may help indirectly restore length and reduce the tibia fracture. Concomitant syndesmotic injuries are not commonly seen and fixation for these is not required unless stress exam clearly demonstrates it.
Casstevens et al. reviewed the surgical management of distal tibia fractures using either plates/screws or intramedullary nails. Current literature shows near equivalence of either technique regarding union and alignment. They recommend treating each fracture on a case-by-case basis with consideration of the soft tissues and fracture pattern when determining fixation choices.
Tejwani et al. reviewed surgical techniques for managing metaphyseal and meta-diaphysial tibia fractures. Advances in tibial nail design have helped tremendously in negotiating these fractures. Though current supporting literature is based mostly on case series, the use of suprapatellar entry intramedullary nails may help avoid the common deformity of procurvatum and valgus seen with proximal tibia fractures.
Egol et al. retrospectively reviewed distal tibial shaft fracture undergoing intramedullary nailing, with and without concomitant fibula fracture plate fixation. They found fractures with fibular fixation maintained better alignment beyond 12 week post-operatively than those without fixation. Given these findings they recommended fibular plating for all distal tibial shaft fractures.
Illustration A shows a fibula fracture that was plated prior to tibia IMN placement. Illustrations B and C show the use of pointed reduction forceps placed percutaneously to reduce the fracture. Illustration D shows the use of a blocking screw (denoted by the arrow) to keep the nail lateralized and the fracture out of valgus. Illustration E shows the use of a plate to reduce the fracture prior to nail placement.
Incorrect Answers:
Answers 1, 2, 3, and 4: All of these have been described in the literature to help aid in reducing these fractures
A 70-year-old woman falls down a flight of stairs and sustains the injury shown in Figures A and B to her dominant upper extremity. She lives alone and has no other medical history. Which of the following surgical options is best to minimize complications for this fracture pattern?
1) Open reduction and internal fixation with a long locking plate
2) Uncemented reverse total shoulder arthroplasty with tuberosity repair
3) Cemented reverse total shoulder arthroplasty without tuberosity repair
4) Cemented reverse total shoulder arthroplasty with tuberosity repair
5) Proximal humeral resection with endoprosthetic replacement
This patient has a complex proximal humerus fracture with metaphyseal comminution and poor bone stock. Cemented reverse total shoulder arthroplasty (rTSA) using a long stem prosthesis and tuberosity repair is indicated.
Proximal humerus fragility fractures are hard to treat because of comminution and poor bone stock. AVN is common with glenohumeral fracture-dislocation. Hemiarthroplasty (and standard total shoulder arthroplasty, TSA) is unreliable because of dependence on tuberosity healing. rTSA is recommended for fractures in patients >70 years with severely comminuted fractures, high likelihood of head AVN, and poor tuberosity bone quality (osteoporosis or comminution).
Bufquin et al. retrospectively reviewed the use of rTSA for treatment of 43 patients with 3- and 4-part proximal humerus fractures. They found satisfactory elevation (97°), ER in abduction (30°), constant scores (44) and modified Constant scores (66%). Complications included calcification (90%), tuberosity displacement (53%) and scapular notching (25%). They concluded that rTSA was a good procedure because it provides pain relief and easier functional recovery in spite of failed tuberosity healing.
Anakwenze et al. systematically reviewed acute proximal humerus fractures. Frequency weighted range of motion was flexion 122°, abduction 97°, ER at neutral 18°. Tuberosity repair yielded higher ER compared to no repair.
Scapular notching was the most common complication (32%). They concluded that rTSA patients tended to be elderly women with 4-part fractures, had good pain control but residual dysfunction.
Jobin et al. reviewed rTSA for management of proximal humerus 3- and 4-part fractures. They note >50% of cases have tuberosity resorption. They recommend repairing the greater tuberosity to restore infraspinatus/teres minor function which improves external rotation strength. Greater tuberosity malunion is not a result of secondary displacement, but rather, from intraoperative malreduction. Lesser tuberosity repair should be performed if there is significant bone loss or intraoperative anterior instability.
Figures A and B are AP radiograph and 3D reformatted CT scan showing comminuted proximal humerus fracture dislocation. Illustration A shows rTSA performed with distal cementation of a long stem prosthesis and cerclage fixation of the proximal shaft and the tuberosity fragments.
Incorrect Answers:
Answer 1: ORIF has potential complications of screw cut out, AVN, fracture collapse, tuberosity resorption and loss of fixation. The risk of AVN (and resultant screw cut out) is high because of comminuted fracture-dislocation. Answer 2: Cementing is indicated because metaphyseal fracture bone loss compromises stem fixation.
Answer 3: Greater tuberosity repair improves external rotation strength. Lesser tuberosity repair adds to anterior stability.
Answer 5: Proximal humeral replacement is only necessary for tumor or unreconstructable fractures. They have poorer outcomes because of loss of rotator cuff function.
A 26-year-old male underwent statically locked intramedullary nail fixation for a comminuted left femur fracture. An early post-
operative computed tomography (CT) scanogram was taken to check rotational alignment, as shown in Figure A. What would be the next best step in the management of this patient?
1) Observation and close follow-up
2) Dynamization of the intramedullary nail
3) Revision surgery, internally rotate distal fragment by 19 degrees
4) Revision surgery, externally rotate distal fragment by 8 degrees
5) Revision surgery, internally rotate proximal fragment by 11 degrees
The CT scanogram shows the operative left femur is 8 degrees externally rotated compared to the native right femur. No correction is required unless malalignment is >15 degrees and symptomatic. Therefore, the most appropriate next step would be to continue with postoperative observation and close follow-up.
The primary purpose of CT scanogram is to measure the angle of rotation of the femoral neck relative to the femoral condyle. To do this, the right and left femurs must be scanned together using a 5mm helical slice scanner at the hip and knee. The first slice should reveal the alignment of the femoral neck, so as to allow for measurement of the femoral neck-to-horizontal (FNH) angle. The second slice should reveal the alignment of the posterior femoral condyles.
This allows measurement of the posterior condyle-to-horizontal (PCH) angle. Finally, to calculate the rotational alignment (RA), the FNH angle and PCH angles are subtracted (e.g., RA = FNH - PCH). Normal RA is usually +5 to +20 degrees, which is also referred to as 5 to 20 degrees of femoral anteversion.
Lindsey et al. reviewed femoral malrotation following intramedullary nail fixation. They showed the incidence of rotational malalignment was ~28%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is ~11-13°. However, they noted that some patients have up to 15° difference in rotation in native limbs.
Therefore 15 degrees and symptomatic.
Which of the following images shows an injury pattern most consistent with a lateral compression type 3 pelvic ring injury?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Figure C is an axial CT scan of a lateral compression type 3 (LC3) pelvic ring injury.
Classically, LC3 injuries demonstrate an ipsilateral lateral compression and a contralateral APC (windswept pelvis) fracture pattern. The most common mechanism of injury in these cases is a rollover MVC or pedestrian vs. auto. LC1 injuries are characterized by an oblique or transverse ramus fracture and ipsilateral anterior sacral ala compression fracture, while LC2 injuries consist of a rami fracture and ipsilateral posterior ilium fracture dislocation (crescent fracture). While LC1 injuries can often initially be managed conservatively with protected weight-bearing and close observation, LC2 and LC3 pelvic ring injuries are almost universally operative.
Pennal et al. discuss a radiologic technique for assessing the forces producing pelvic disruption and its use in logically classifying pelvic injury. Based on this radiologic assessment and along with some biomechanical studies, they propose a classification system involving three major forces producing injury that can also be helpful in the management of these patients.
Young et al. performed a retrospective analysis of the plain radiographs of 142 cases of pelvic fractures and identified four patterns of force that presented with distinctive, recognizable radiographic appearances. They describe a classification system for pelvic fractures based on radiographic and clinical findings that correlates with associated injury to soft-tissue structures and enables the surgeon to begin corrective procedures rapidly.
Incorrect Answers:
Answer 1: This represents a lateral compression type 2 injury. Answer 2: This represents a lateral compression type 1 injury.
Answer 4: This represents an anterior posterior compression type 2 injury. Answer 5: This represents an anterior posterior compression type 3 injury.
For a patient with an unstable pelvic fracture, the amount of blood tranfusions required in the first 24 hours has shown to be most predictive for what variable?
1) Length of hospital stay
2) Association with neurological deficit(s)
3) Length of intensive care stay
4) Cardiac collapse
5) Mortality
Unstable pelvic fractures can be devastating injuries often resulting in significant morbidity and even death.
According to the referenced study by Smith et al, fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased ISS or RTS scores. Deaths were most commonly from exsanguination (24 hours).
Incorrect Answers: Choices 1-4 do not correlate with increased blood transfusions to the extent of Option 5.
A healthy 27 year-old-male is brought into the emergency department after a fall from height. He has a suspected left C8-T1 nerve injury. Which of the following findings would most suggest a root avulsion injury rather than a brachial plexus injury at this level?
1) Reduced radial artery pulse
2) Double break in the ipsilateral superior shoulder suspensory complex
3) Elevated hemidiaphragm
4) Musculocutaneous nerve deficit
5) Drooping of the left eyelid
Drooping of the left eyelid is a presenting feature of Horner's syndrome. Horner's syndrome represents a disruption of the sympathetic chain via C8 and/or T1 root avulsion after trauma.
Brachial plexus injuries are often classified as preganglionic vs. postganglionic injuries. Preganglionic injuries are typically avulsion injuries proximal to the dorsal root ganglion. Clinical features suggestive of lower root avulsion injury include a person falling from height clutching on object to save himself, Horner’s syndrome (drooping of the eyelid (ptosis), pupillary constriction (miosis) and anhidrosis), absence of a Tinel sign or tenderness to percussion in the neck, and a normal histamine test (C8-T1 sympathetic ganglion - intact triple response (redness, wheal, flare)).
Caporrino et al. reviewed 102 patients to assess the best modality (e.g. physical examination, MRI and nerve conduction studies [NCSs]) for diagnosing and localizing brachial plexus injuries. They found the best diagnostic performance with physical examination (sensitivity = 97.8%; specificity = 30.8%) and NCSs (sensitivity = 98.9%; specificity = 23.1%). MRI had inferior performance for all measurements. They conclude that NCSs exhibited superior performance to MRI, and should be considered a more reliable supporting tool after detailed physical examination.
Incorrect Answers:
Answer 1, 2: The superior shoulder suspensory complex (SSSC) is located in close proximity to the brachial plexus. Disruption of the SSSC may affect the local anatomy and cause local brachial plexus or vascular injury.
Answer 3: Elevated hemidiaphragm (Phrenic nerve C3,4,5) may be suggestive an upper brachial plexus root avulsion, e.g. C5, C6 injury.
Answer 4: Musculocutaneous nerve deficiency (C5 deficiency) results in weakness to the biceps.
A 46-year-old competitive cyclist falls while racing and suffers an isolated fracture as seen in Figure A. He is positioned on a fracture table and a closed reduction maneuver is attempted, unsuccessfully.
Which of the following treatment plans is most appropriate?
1) Obtain a CT scan intraoperatively to reassess the quality of reduction
2) Perform additional closed reduction maneuvers until the reduction is adequate for percutaneous fixation
3) As long as the stepoff is less than 7mm in any plane of imaging, it is appropriate to proceed with percutaneous fixation
4) Perform an open reduction and internal fixation using a sliding hip screw
5) Perform an acute total hip arthroplasty through a direct anterior approach since the patient is on the fracture table
When standard closed reduction maneuvers using a traction table are unsuccessful, displaced femoral neck fracture in young adults (10 degrees varus/valgus or anteversion/retroversion) or has
significant displacement (5 mm or more in ANY view) is unacceptable, and an open reduction should be performed. Of course, this can be very difficult to assess in the operating room, where uncalibrated fluoroscopy with difficult to obtain tangential imaging is heavily relied upon to make this assessment.
Accordingly, when the quality of closed reduction is questionable, the best treatment plan is to obtain a better reduction with direct visualization of the femoral neck prior to fixation.
A systematic review of the literature by Pauyo, et al. cites numerous studies showing a higher incidence of osteonecrosis of the femoral head in patients with displaced femoral neck fractures treated with unsatisfactory reductions. Furthermore, performing multiple closed reduction attempts is also associated with a higher risk of osteonecrosis.
Upadhyay et al. performed a randomized controlled trial of 102 patients with femoral neck fractures treated with closed or open reductions, which were randomized. The groups had similar rates of nonunions and osteonecrosis of the femoral head; however, subanalysis revealed a "poor" reduction was the highest predictor of poor outcome, whether the reduction was attempted open or closed. Interestingly, the quality of reduction was more important than the implant used or the timing of surgery (including surgeries performed > 48h after injury).
Figure A shows a pre-operative AP x-ray of the patient's high-energy femoral neck fracture. Illustrations A and B are intraoperative fluoroscopic and postoperative CT scans of this same patient, highlighting that fluoroscopy may "hide" the degree of residual displacement.
Incorrect Answers:
Question 27High Yield
Four days ago, a 13-year-old boy stubbed his toe on a chair while running barefoot through his home.
He received no treatment at the time. He is now seen at the orthopaedic clinic with the radiograph and clinical photograph shown in Figures 27a and 27b. What is the next step in management?
He received no treatment at the time. He is now seen at the orthopaedic clinic with the radiograph and clinical photograph shown in Figures 27a and 27b. What is the next step in management?
Explanation
The boy has a Seymour’s fracture of the toe. The germinal matrix of the nail bed is trapped in the fracture site; thus this should be considered an open fracture. Ideally, it should be treated with open reduction and internal fixation and use of antibiotics at the time of injury. Because this is a delayed presentation, it is even more important to do a formal open reduction and a good irrigation and debridement, followed by the use of postoperative antibiotics. Because the fracture has been displaced for several days, overall management will be easier if the fracture reduction is maintained with pin fixation.
REFERENCE: Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL. American Academy of Orthopaedic Surgeons, 2008, p 737.
REFERENCE: Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL. American Academy of Orthopaedic Surgeons, 2008, p 737.
Question 28High Yield
Which of the following organisms is most often found in a late (> 3 months) infection of a total hip arthroplasty?

Explanation
DISCUSSION: Staphylococcus epidermidis is the most common organism found in an infected total hip arthroplasty greater than 3 months from the origional surgery. Staphylococcus aureus is more common in acute postoperative infections, and E. coli is associated with infections of the urinary tract. Streptococcus species are less common.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL American Academy of Orthopedic Surgeons, 2006, pp 475-503.
Figure 82
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL American Academy of Orthopedic Surgeons, 2006, pp 475-503.
Figure 82
Question 29High Yield
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
Coleman block testing, performed by placing an elevation under the lateral border of the foot, is used to determine if the forefoot and/or plantar flexed first ray is causing a compensatory varus in the hindfoot. The block is placed under the lateral border of the foot, and therefore does not have any relation to the Achilles tendon and suppleness of the hindfoot.
REFERENCES: Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
REFERENCES: Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 30High Yield
72
Figure 72 is the radiograph of a 58-year-old active woman with progressive medial first MTP joint pain, particularly with shoe wear and increased activity. The patient has no hypermobility.
Figure 72 is the radiograph of a 58-year-old active woman with progressive medial first MTP joint pain, particularly with shoe wear and increased activity. The patient has no hypermobility.

Explanation
- Proximal first metatarsal osteotomy
Question 31High Yield
Figure below shows a cross-table lateral radiograph obtained from a healthy 56-year-old woman with
recurrent hip dislocations 6 months after total hip arthroplasty performed through a posterolateral approach. Each dislocation occurred when she was bending over to put her shoes on or pick something up. She has dislocated four times and has had no pain between dislocations. Abductor strength is 5 out of
5/. The infection work-up is negative. What is the best next step?
recurrent hip dislocations 6 months after total hip arthroplasty performed through a posterolateral approach. Each dislocation occurred when she was bending over to put her shoes on or pick something up. She has dislocated four times and has had no pain between dislocations. Abductor strength is 5 out of
5/. The infection work-up is negative. What is the best next step?

Explanation
The cross-table lateral radiograph shows that the patient has decreased acetabular anteversion. She is likely impinging on her cup in flexion and levering the femoral component posteriorly. Given a well-fixed and well-aligned femoral component and a negative infection work-up, the preferred treatment is to revise the acetabulum with a goal of increasing acetabular anteversion to avoid prosthetic impingement. Conversion to a constrained or elevated rim liner is suboptimal in this setting, because the problem is impingement. Indications for a constrained liner are neuromuscular compromise, abductor deficiency, or instability despite well-fixed and well-placed components. Given her 5 of 5 abductor strength, gluteus
medius repair is not indicated.
medius repair is not indicated.
Question 32High Yield
A 23-year-old soccer player sustains a grade III complete posterior cruciate ligament (PCL) tear after colliding with another player. In reconstructing the PCL, it is optimal to reconstruct the
Explanation
The PCL is a nonisometric structure with nonuniform tension during knee motion, with maximum tension at 90° of flexion. While the posteromedial PCL fibers have been found to be the most isometric, the anterolateral fibers represent the bulk of the ligament. Studies have suggested that anterior placement of the femoral tunnel is superior to placement in an isometric position. The anterolateral bundle tightens as the knee flexes; therefore, it is optimal to tension the graft at 90° of flexion.
REFERENCES: Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Burns WC II, Draganich LF, Pyevich M, Reider B: The effect of femoral tunnel position and graft tensioning technique on posterior laxity of the posterior cruciate ligament-reconstructed knee. Am J Sports Med 1995;23:424-430.
REFERENCES: Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Burns WC II, Draganich LF, Pyevich M, Reider B: The effect of femoral tunnel position and graft tensioning technique on posterior laxity of the posterior cruciate ligament-reconstructed knee. Am J Sports Med 1995;23:424-430.
Question 33High Yield
A 30-year-old male undergoes successful surgical fixation of a displaced talar neck fracture. Which of the following is the most likely long-term complication even after anatomic reduction and stable fixation is achieved?


Explanation
It is important to counsel patients regarding these devastating injuries and their poor prognosis, as osteonecrosis, subtalar and tibiotalar joint degeneration, and talar collapse are not infrequent.
In a series by Lindvall et al, subtalar joint arthritis was reported as more common than osteonecrosis of the talus at 4 year follow-up after fixation. Osteonecrosis of the talus was the next most common complication following surgery.
The referenced article by Vallier et al reported on mid- to long-term follow-up of this patient population. Ten of the twenty-six patients had development of osteonecrosis of the talar body, but only half experienced collapse of the talar dome. All patients with a history of both an open fracture and osteonecrosis experienced collapse. Seventeen of twenty-six patients had posttraumatic arthritis of the tibiotalar joint, and nine of twenty-six had posttraumatic arthritis of the subtalar joint.
Illustrations A and B show a displaced talar neck fracture.
In a series by Lindvall et al, subtalar joint arthritis was reported as more common than osteonecrosis of the talus at 4 year follow-up after fixation. Osteonecrosis of the talus was the next most common complication following surgery.
The referenced article by Vallier et al reported on mid- to long-term follow-up of this patient population. Ten of the twenty-six patients had development of osteonecrosis of the talar body, but only half experienced collapse of the talar dome. All patients with a history of both an open fracture and osteonecrosis experienced collapse. Seventeen of twenty-six patients had posttraumatic arthritis of the tibiotalar joint, and nine of twenty-six had posttraumatic arthritis of the subtalar joint.
Illustrations A and B show a displaced talar neck fracture.
Question 34High Yield
A 14-year-old gymnast misses her dismount off of the uneven bars, hits the mat face first, and loses consciousness for about 15 seconds. She is dazed and confused for several minutes. She does not complain of pain, numbness, or weakness and she is moving all extremities without deficit. The athlete and coach would like to return to competition that day. What is the best next step?
Explanation
The National Collegiate Athletic Association's health and safety guidelines regarding concussion management recommend no return to play on the same day of an injury. In particular, athletes sustaining a concussion should not return to play the same day as their injury. Before resuming exercise, athletes must be asymptomatic or returned to baseline symptoms at rest and have no symptoms with cognitive effort. They must be off of medications that could mask or alter concussion symptoms. Neurocognitive testing can be a helpful tool in determining brain function even after all symptoms of concussion have resolved. With a comparison baseline test, this evaluation, in conjunction with a physician's examination, may reduce risk for second impact syndrome. The athlete's clinical neurologic examination findings (cognitive, cranial nerve, balance testing) must return to baseline before resuming exercise. Research has shown that among youth athletes, it may take longer for tested functions to return to baseline (compared with the recovery rate in adult athletes). Brain MRI scan has no role in evaluating athletes for return to play in this situation.
Question 35High Yield
Figures 1 and 2 are the radiographs of a 25-month-old boy who sustained an isolated right leg injury leaping from the couch. The patient underwent closed manipulation with immediate spica-cast application. One week following the injury, radiographs in the cast reveal just <2 cm of shortening at the fracture. What is the most appropriate next step in treatment?

Explanation
■
Limb-length inequality is one of the most common complications following treatment of femoral shaft fractures in children. In children <10 years-old, some degree of accelerated growth, or overgrowth, may occur in the involved extremity. This typically occurs in the 3 to 24 months following injury.
The average amount of overgrowth is 1.5 to 2 cm, such that leaving a fracture shortened by this amount is acceptable in children undergoing spica-cast immobilization for treatment (typically in children between 6 months and 4 to 5 years-old).
■
Limb-length inequality is one of the most common complications following treatment of femoral shaft fractures in children. In children <10 years-old, some degree of accelerated growth, or overgrowth, may occur in the involved extremity. This typically occurs in the 3 to 24 months following injury.
The average amount of overgrowth is 1.5 to 2 cm, such that leaving a fracture shortened by this amount is acceptable in children undergoing spica-cast immobilization for treatment (typically in children between 6 months and 4 to 5 years-old).
Question 36High Yield
What is the most likely cause of her symptoms?
Explanation
- Rotator cuff tear_
Question 37High Yield
Figure 1 is the axial MRI scan of a 45-year-old brick mason who experienced acute right elbow pain after attempting to lift a wheelbarrow. Examination reveals pain and swelling in the antecubital fossa, weakness with forearm supination, and an abnormal hook test. The surgeon performs an anterior repair with two anchors. Three months after surgery, the patient has appropriate strength and range of motion but reports persistent radiating paresthesias along the radial side of the forearm. What is the best next step in management?
Explanation
This is a classic presentation of an acute traumatic distal biceps tendon rupture. In the dominant extremity of a manual laborer, this injury can result in approximately 40% loss of supination strength. Although not required, an MRI scan can confirm
the diagnosis. In general, a single incision anterior or two incision anterior/ posterior repair can be utilized for surgical intervention with similar success rates. Although the percentage of complications is similar between surgical approaches, the type of complications can vary. Anterior only repairs have a
20
higher risk of traction injury to the lateral antebrachial cutaneous nerve (LABC) secondary to the degree of retraction required for exposure in muscular patients. Posterior repairs have a higher risk for radiographic heterotopic bone formation. Fortunately, most LABC injuries are neuropraxias and resolve with observation, but resolution may take up to 6 months. In this case, ongoing observation is appropriate, with surgical exploration being considered only in chronic cases. Patients should be appropriately counseled about this issue prior to surgery.
the diagnosis. In general, a single incision anterior or two incision anterior/ posterior repair can be utilized for surgical intervention with similar success rates. Although the percentage of complications is similar between surgical approaches, the type of complications can vary. Anterior only repairs have a
20
higher risk of traction injury to the lateral antebrachial cutaneous nerve (LABC) secondary to the degree of retraction required for exposure in muscular patients. Posterior repairs have a higher risk for radiographic heterotopic bone formation. Fortunately, most LABC injuries are neuropraxias and resolve with observation, but resolution may take up to 6 months. In this case, ongoing observation is appropriate, with surgical exploration being considered only in chronic cases. Patients should be appropriately counseled about this issue prior to surgery.
Question 38High Yield
A 53-year-old man sustains a fall while skiing. He experiences immediate pain and deformity in his lower leg just above his ski boot top. Radiographs of his left lower leg are shown in Figures 1 and

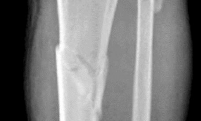




Explanation
The patient has sustained a proximal third tibia and fibula fracture, sometimes referred to as a "boot top" fracture when sustained while alpine skiing. These fractures frequently fall into apex anterior and valgus
angulation as shown in the radiographs. Great care needs to be taken during intramedullary nailing to avoid fixing the fracture in a malreduced position. The use of Poller blocking screws in the posterior and lateral aspects of the proximal fragment can help to avoid this complication (posterior screw prevents flexion deformity while lateral screw prevents valgus deformity). Additional technical pearls include starting with a more lateral entry point for the guidewire, placing a provisional unicortical plate prior to nailing to maintain the reduction, or using a suprapatellar entry nail to allow for fixation with the knee in _a semi-extended position._
angulation as shown in the radiographs. Great care needs to be taken during intramedullary nailing to avoid fixing the fracture in a malreduced position. The use of Poller blocking screws in the posterior and lateral aspects of the proximal fragment can help to avoid this complication (posterior screw prevents flexion deformity while lateral screw prevents valgus deformity). Additional technical pearls include starting with a more lateral entry point for the guidewire, placing a provisional unicortical plate prior to nailing to maintain the reduction, or using a suprapatellar entry nail to allow for fixation with the knee in _a semi-extended position._
Question 39High Yield
Figure 46a is the lateral radiograph of a 54-year-old man who has had a painless soft-tissue mass on his right foot that has been growing slowly for about 1 year. MR sequences are shown in Figures 46b through 46e. A biopsy is performed, and a low-power hematoxylin and eosin photomicrograph is seen in Figure 46f. The most appropriate treatment for this lesion is

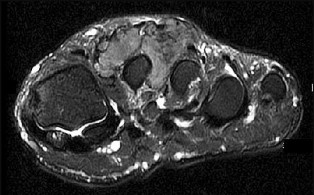
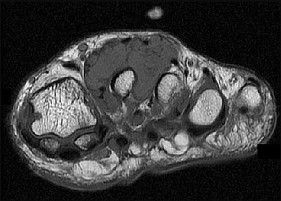
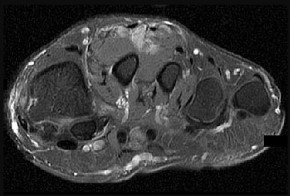
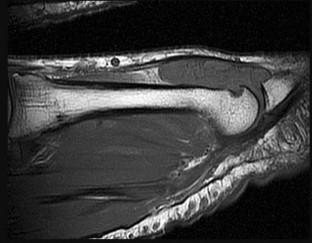
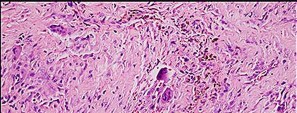
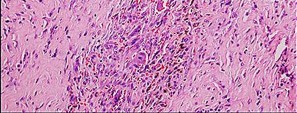
Explanation
This is a giant-cell tumor of the tendon sheath. A solid lesion larger than 1.5 cm in the hand or foot warrants biopsy to rule out malignancy. The 3 most common benign tumors of the foot are ganglion cysts, giant-cell tumors of tendon sheath, and hemangiomas. Radiographs are nonspecific but may reveal extrinsic erosions of bone by a giant-cell tumor of the tendon sheath. MR findings of prominent low-signal intensity (seen with T2 weighting) and “blooming” artifact from the hemosiderin (seen with gradient-echo sequences) are nearly pathognomonic of this diagnosis, as
seen here. Pathology shows hemosiderin-laden macrophages and giant cells as seen in the histology. Uric acid reduction would be indicated for gout and wide local excision for a soft-tissue sarcoma. Observation awaiting mature mineralization would apply to heterotopic ossification.
RECOMMENDED READINGS
29. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis: radiologic-pathologic correlation. Radiographics. 2008 Sep-Oct;28(5):1493-
[518/. doi: 10.1148/rg.285085134. PubMed PMID: 18794322. ](http://www.ncbi.nlm.nih.gov/pubmed/18794322)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18794322)
30. [Ruggieri P, Angelini A, Jorge FD, Maraldi M, Giannini S. Review of foot tumors seen in a university tumor institute. J Foot Ankle Surg. 2014 May-Jun;53(3):282-5. doi: 10.1053/j.jfas.2014.01.015. Review. PubMed PMID: 24751209. ](http://www.ncbi.nlm.nih.gov/pubmed/24751209)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24751209)
seen here. Pathology shows hemosiderin-laden macrophages and giant cells as seen in the histology. Uric acid reduction would be indicated for gout and wide local excision for a soft-tissue sarcoma. Observation awaiting mature mineralization would apply to heterotopic ossification.
RECOMMENDED READINGS
29. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis: radiologic-pathologic correlation. Radiographics. 2008 Sep-Oct;28(5):1493-
[518/. doi: 10.1148/rg.285085134. PubMed PMID: 18794322. ](http://www.ncbi.nlm.nih.gov/pubmed/18794322)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18794322)
30. [Ruggieri P, Angelini A, Jorge FD, Maraldi M, Giannini S. Review of foot tumors seen in a university tumor institute. J Foot Ankle Surg. 2014 May-Jun;53(3):282-5. doi: 10.1053/j.jfas.2014.01.015. Review. PubMed PMID: 24751209. ](http://www.ncbi.nlm.nih.gov/pubmed/24751209)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24751209)
Question 40High Yield
Which of the following conditions is not associated with an increased risk of congenital vertical talus?
Explanation
Patients with cerebral palsy do not have an increased risk of congenital vertical talus, but they may develop an acquired neuromuscular vertical talus.
Patients with myelomeningocele have approximately a 5% to 10% risk of vertical talus, far above that of the general population.
Arthrogryposis is associated with an increased risk of vertical talus.
Nail patella syndrome is associated with an increased risk of vertical talus. Sacral agenesis is associated with an increased risk of vertical talus.
Patients with myelomeningocele have approximately a 5% to 10% risk of vertical talus, far above that of the general population.
Arthrogryposis is associated with an increased risk of vertical talus.
Nail patella syndrome is associated with an increased risk of vertical talus. Sacral agenesis is associated with an increased risk of vertical talus.
Question 41High Yield
Which of the following is true concerning Achilles tendon ruptures:
Explanation
Important points to remember about Achilles tendon ruptures: A. Most common in middle-aged men
B. Often intermittent sports activity
C . Left more than right
D. Often the tendon is abnormal (degenerative) E. Mechanism
1/. Sudden forced plantarflexion
2/. Unexpected dorsiflexion
3/. Violent dorsiflexion of the plantar flexed foot
Factors which may make the patient more prone to rupture: A. Steroids
B. Fluoroquinolones
B. Often intermittent sports activity
C . Left more than right
D. Often the tendon is abnormal (degenerative) E. Mechanism
1/. Sudden forced plantarflexion
2/. Unexpected dorsiflexion
3/. Violent dorsiflexion of the plantar flexed foot
Factors which may make the patient more prone to rupture: A. Steroids
B. Fluoroquinolones
Question 42High Yield
The bony abnormalities in this condition occur mostly in the
Explanation
- tarsal bones.
Question 43High Yield
A collegiate lacrosse player is struck on the head by an opposing player’s stick. She is initially
unresponsive. She regains consciousness within 2 minutes but remains confused and uncooperative, complaining of head and neck pain. This is her second concussion of the calendar year. Initial management should consist of
unresponsive. She regains consciousness within 2 minutes but remains confused and uncooperative, complaining of head and neck pain. This is her second concussion of the calendar year. Initial management should consist of
Explanation
This patient has sustained a significant concussion or minor brain injury. Although all answer options reflect important steps in her management, the initial primary concern in any player who is confused or combative is protection of the cervical spine until formal clearance can be performed. This patient requires immediate immobilization, collar placement, and, ultimately, transportation to a hospital. Cervical immobilization should be achieved before transport, given her complaints of neck pain and inability to provide a reliable examination.
Question 44High Yield
With respect to the clinical photograph shown in Figure 97, what artery provides the most blood supply to the area of the planned incision?
Explanation
The photograph shows the planned incision for an extensile lateral approach to the calcaneus. The lateral calcaneal artery, usually a branch of the peroneal artery, provides blood supply to the majority of the full-thickness flap of an extensile lateral approach. Other branches also contribute,including the lateral malleolar and lateral tarsal arteries, although to a lesser degree.
Question 45High Yield
1224) A 55-year-old male is involved in a motorcycle crash and sustains a closed, right-sided, midshaft femur fracture. This is an isolated injury. He is treated with retrograde femoral nailing, and postoperatively is noted to have 30 degrees of internal rotation of the operative extremity, when compared with his nonsurgical side. Which of the following is the most likely cause of this malrotation deformity?
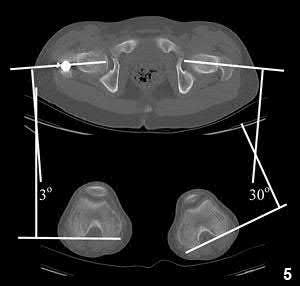
Explanation
Internal rotation of the distal segment of the femur relative to the proximal segment of the femur during nailing can cause a malrotation deformity.
Postsurgical internal malrotation after treatment for a diaphyseal femur fracture typically occurs either via internal rotation of the distal segment relative to the proximal or external rotation of the proximal segment relative to the distal. These clinical findings are consistent with an iatrogenic increase in femoral anteversion.
Dimitriou et al. performed a study to quantify the side-to-side anatomic variation in the proximal femur and the implications for preoperative planning and leg length discrepancy following hip arthroplasty. CT-based 3D femoral models were reconstructed for 122 paired femurs in 61 young healthy subjects with no history of hip pathology. Significant side-to-side differences were found in femoral anteversion, horizontal offset, and femoral head center location.
They concluded that relying on the anatomic landmarks of the contralateral femur during hip arthroplasty may not necessarily result in restoration of native anatomy and leg-length.
Karaman et al. conducted a study which saught to clarify the influence of a femoral rotational malalignment of ≥10° after intramedullary nailing on daily activities. They evaluated twenty-four femoral shaft fracture patients treated with closed antegrade IMN, and determined the presence of malrotation with post-operative CT scans. Ten of the 24 patients had a CT-detected true rotational malalignment of ≥10° compared with the unaffected side, and were noted to have significantly worse functional outcome scores compared with normally rotated femoral shaft patients.
Espinoza et al. present a technique using intraoperative fluoroscopy and the anteversion inherent to the IM nail for obtaining appropriate femoral rotational alignment during surgery. The authors state that their technique reliably sets the femoral anteversion within a normal physiologic range with minimal additional intraoperative steps and without preoperative measurements.
Illustration A shows a CT evaluation of femoral malrotation. The angle on the uninjured side measures 30°, while the malrotated fractured side measures only 3°, indicating a 27° external rotation deformity.
Incorrect Answers:
Answer 1: This would result in external rotation of the femur. Answer 2: This would result in external rotation of the femur. Answer 3: This would result in external rotation of the femur. Answer 4: The contralateral femur would not be affected in this case.
Postsurgical internal malrotation after treatment for a diaphyseal femur fracture typically occurs either via internal rotation of the distal segment relative to the proximal or external rotation of the proximal segment relative to the distal. These clinical findings are consistent with an iatrogenic increase in femoral anteversion.
Dimitriou et al. performed a study to quantify the side-to-side anatomic variation in the proximal femur and the implications for preoperative planning and leg length discrepancy following hip arthroplasty. CT-based 3D femoral models were reconstructed for 122 paired femurs in 61 young healthy subjects with no history of hip pathology. Significant side-to-side differences were found in femoral anteversion, horizontal offset, and femoral head center location.
They concluded that relying on the anatomic landmarks of the contralateral femur during hip arthroplasty may not necessarily result in restoration of native anatomy and leg-length.
Karaman et al. conducted a study which saught to clarify the influence of a femoral rotational malalignment of ≥10° after intramedullary nailing on daily activities. They evaluated twenty-four femoral shaft fracture patients treated with closed antegrade IMN, and determined the presence of malrotation with post-operative CT scans. Ten of the 24 patients had a CT-detected true rotational malalignment of ≥10° compared with the unaffected side, and were noted to have significantly worse functional outcome scores compared with normally rotated femoral shaft patients.
Espinoza et al. present a technique using intraoperative fluoroscopy and the anteversion inherent to the IM nail for obtaining appropriate femoral rotational alignment during surgery. The authors state that their technique reliably sets the femoral anteversion within a normal physiologic range with minimal additional intraoperative steps and without preoperative measurements.
Illustration A shows a CT evaluation of femoral malrotation. The angle on the uninjured side measures 30°, while the malrotated fractured side measures only 3°, indicating a 27° external rotation deformity.
Incorrect Answers:
Answer 1: This would result in external rotation of the femur. Answer 2: This would result in external rotation of the femur. Answer 3: This would result in external rotation of the femur. Answer 4: The contralateral femur would not be affected in this case.
Question 46High Yield
Figures below show the radiographs obtained from a 90-year-old woman who is seen in the emergency
department after a fall from a height. She has right hip and thigh pain and is unable to bear weight. Based on this patient's history and imaging, what is the best next step?
department after a fall from a height. She has right hip and thigh pain and is unable to bear weight. Based on this patient's history and imaging, what is the best next step?
Explanation
Periprosthetic fracture is the third most common reason (after loosening and infection) for revision surgery after total hip arthroplasty (THA). Late periprosthetic fracture risk is 0.4% to 1.1% after primary
THA and 2.1% to 4% after revision THA. Risk factors for periprosthetic fracture include age over 70 years, decreasing bone mass, and loosening of implants and osteolysis. The risk of concomitant infection in the presence of a periprosthetic fracture is 11%, according to Chevillotte and associates. Obtaining presurgical aspiration or intrasurgical tissue for culture is recommended if concomitant infection is suspected.
THA and 2.1% to 4% after revision THA. Risk factors for periprosthetic fracture include age over 70 years, decreasing bone mass, and loosening of implants and osteolysis. The risk of concomitant infection in the presence of a periprosthetic fracture is 11%, according to Chevillotte and associates. Obtaining presurgical aspiration or intrasurgical tissue for culture is recommended if concomitant infection is suspected.
Question 47High Yield
What is the statistical likelihood that this boy could develop a progressive deformity for which surgery would be necessary?
Explanation
- Lower than 5%
Question 48High Yield
What structure attaches at the fracture site shown in Figures 107a and 107b?
Explanation
_**
**_
**_
Question 49High Yield
When performing elbow arthroscopy, it is often necessary to evaluate the posterior compartment. When entering the posterior compartment of the elbow, what are the two safest and most commonly used portals?
Explanation
DISCUSSION: The posterior portal created 3 cm proximal to the tip of the olecranon and the posterior lateral portal created 3 cm proximal from the tip of the olecranon and just lateral to the triceps are the “workhorse” portals of the posterior compartment and although relatively safe, risks exist. The radial nerve proximity averages 4.8 mm (3 to 8 mm) from the posterolateral portal. The central posterior portal close to 20 mm from the ulnar nerve.
REFERENCES: Steinmann SP: Elbow arthroscopy. J Am Society of the Hand 2003 ;3:199-207.
Dodson CC, Nho SJ, Williams RJ III, et al: Elbow Arthroscopy. J Am Acad Orthop Surg 2008:16:574- 585.
DISCUSSION: The posterior portal created 3 cm proximal to the tip of the olecranon and the posterior lateral portal created 3 cm proximal from the tip of the olecranon and just lateral to the triceps are the “workhorse” portals of the posterior compartment and although relatively safe, risks exist. The radial nerve proximity averages 4.8 mm (3 to 8 mm) from the posterolateral portal. The central posterior portal close to 20 mm from the ulnar nerve.
REFERENCES: Steinmann SP: Elbow arthroscopy. J Am Society of the Hand 2003 ;3:199-207.
Dodson CC, Nho SJ, Williams RJ III, et al: Elbow Arthroscopy. J Am Acad Orthop Surg 2008:16:574- 585.
Question 50High Yield
Mallet finger injuries refer to:
Explanation
Mallet finger injuries may be associated with fractures of the bony tuft, fractures of the middle phalanx, flexor tendon injuries, and intrinsic tightness. However, mallet injuries refer to lack of continuity at the DIP joint.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon