Orthopedic On Review | Dr Hutaif General Orthopedics Re -...
14 Apr 2026
50 min read
93 Views

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic On Review | Dr Hutaif General Orth...
00:00
Start Quiz
Question 1High Yield
Aneurysmal bone cyst of the spine is most likely in this age group:
Explanation
The most common age is the second decade; the mean age is 13 years old.
Question 2High Yield
A 75-year-old man sustains an anterior dislocation of his reverse total shoulder arthroplasty. What activity places the arm in the position most commonly associated with reverse total shoulder dislocation?
Explanation
DISCUSSION
Proper soft-tissue tension is critical to prevent instability of a reverse total shoulder implanted with the deltopectoral approach; dislocation of the prosthesis is exceedingly rare if the superior approach is employed. The arm position implicated in reverse total shoulder instability is extension, adduction, and internal rotation,
such as pushing out of a chair. The other positions described do not involve extension of the shoulder.
DISCUSSION
Proper soft-tissue tension is critical to prevent instability of a reverse total shoulder implanted with the deltopectoral approach; dislocation of the prosthesis is exceedingly rare if the superior approach is employed. The arm position implicated in reverse total shoulder instability is extension, adduction, and internal rotation,
such as pushing out of a chair. The other positions described do not involve extension of the shoulder.
Question 3High Yield
The structure at highest risk for injury in total hip arthroplasty (THA) is the:
Explanation
The external iliaCartery and vein are immobile and lie close to the pelvis, and thus are at high risk for injury in THA. The external iliaCvein lies within 7 mm of the anterior column of the pelvis at the anterior inferior iliaCspine and within 4 mm at the acetabula dome. The external iliaCartery is at less risk due to its thicker intima and increased distance from the bone. The external iliaCartery lies within 10 mm of the bone at the anterior inferior iliaCspine and within 7 mm at the acetabular dome. The common femoral artery lies anterior and medial to the hip capsule. Only the iliopsoas lies between the vessel and capsule at this point. The femoral vein lies medial to the artery and is not likely to be injured. The obturator vessels are also at risk, lying fixed within 1 mm of the bony surface at the quadrilateral surface, with their only protection being the interposition of the obturator internus muscle
Question 4High Yield
A 17-year-old high school football player sustains a neck injury in a game. During the initial on-field
assessment, the team physician removes the player’s helmet, and the athlete is log-rolled to the supine position while the physician manually stabilizes his cervical spine. An examination demonstrates tenderness to palpation over the cervical spine and neurologic deficits in bilateral upper and lower extremities. Shoulder pads prohibit proper placement of a hard cervical collar, and the athlete is immobilized on a spine board and transported to the emergency department via ambulance. Comprehensive evaluation in the emergency department reveals a bilateral facet dislocation of C5 on C6. The on-field intervention most likely to cause a neurologic injury is
assessment, the team physician removes the player’s helmet, and the athlete is log-rolled to the supine position while the physician manually stabilizes his cervical spine. An examination demonstrates tenderness to palpation over the cervical spine and neurologic deficits in bilateral upper and lower extremities. Shoulder pads prohibit proper placement of a hard cervical collar, and the athlete is immobilized on a spine board and transported to the emergency department via ambulance. Comprehensive evaluation in the emergency department reveals a bilateral facet dislocation of C5 on C6. The on-field intervention most likely to cause a neurologic injury is
Explanation
Complete immobilization of the cervical spine is critical for athletes with a suspected cervical spine or spinal cord injury. The spinal cord in the subaxial spine is especially sensitive to motion, and removal of protective gear such as the helmet and shoulder pads presents an unacceptable risk for progressive neurologic injury in the setting of a potentially unstable cervical spine injury. Removal of the face mask alone is typically performed to improve access to an athlete's airway. Protective equipment often prevents
proper placement of a hard cervical collar, and the spine board offers a variety of options for safe cervical spine immobilization of helmeted athletes without a hard cervical collar. The log-roll and lift-and-slide techniques allow for the safe transfer of an athlete to a spine board while maintaining appropriate manual stabilization of the cervical spine.
proper placement of a hard cervical collar, and the spine board offers a variety of options for safe cervical spine immobilization of helmeted athletes without a hard cervical collar. The log-roll and lift-and-slide techniques allow for the safe transfer of an athlete to a spine board while maintaining appropriate manual stabilization of the cervical spine.
Question 5High Yield
Surveillance for growth arrest resulting from this injury should continue for how long after injury?
Explanation
Lateral condyle fractures in skeletally immature patients are uncommon. This is a displaced and rotated lateral condyle fracture. Although closed reduction could be attempted, these fractures are notoriously difficult to reduce even with an open approach.
The blood supply to the lateral condyle fragment enters posterolaterally. Disruption of the blood supply may lead to osteonecrosis of the capitellum, so great care should be taken during open approaches to the elbow in skeletally immature patients, especially during lateral condyle open reduction and internal fixation.
Treatment of lateral condyle fractures in skeletally immature patients may be fraught with danger. The most common complication is persistent stiffness.
Growth arrest is a surprisingly rare complication, considering the fracture usually involves the capitellar physis, and reduction of the physis is often radiographically imperfect even with open reduction. However, this may be an underrecognized complication because arrest of the capitellar physis may not be evident until 1 to 3 years postinjury—beyond the time at which some surgeons or patients believe follow-up is necessary. Growth arrest has been reported with smooth wire fixation and lag screw fixation. The average time to radiographic union of a lateral condyle fracture is 6 weeks.
RECOMMENDED READINGS
10. [Cardona JI, Riddle E, Kumar SJ. Displaced fractures of the lateral humeral condyle: criteria for implant removal. J Pediatr Orthop. 2002 Mar-Apr;22(2):194-7. PubMed PMID: 11856929. ](http://www.ncbi.nlm.nih.gov/pubmed/11856929)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/11856929)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11856929)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11856929)
11. [Stein BE, Ramji AF, Hassanzadeh H, Wohlgemut JM, Ain MC, Sponseller PD. Cannulated Lag Screw Fixation of Displaced Lateral Humeral Condyle Fractures Is Associated With Lower Rates of Open Reduction and Infection Than Pin Fixation. J Pediatr Orthop. 2015 Jul 17. [Epub ahead of print] PubMed PMID: 26192878. ](http://www.ncbi.nlm.nih.gov/pubmed/26192878)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26192878)
12. [Das De S, Bae DS, Waters PM. Displaced humeral lateral condyle fractures in children: should we bury the pins? J Pediatr Orthop. 2012 Sep;32(6):573-8. doi: 10.1097/BPO.0b013e318263a25f. PubMed PMID: 22892618. ](http://www.ncbi.nlm.nih.gov/pubmed/22892618)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22892618)
13. [Cates RA, Mehlman CT. Growth arrest of the capitellar physis after displaced lateral condyle fractures in children. J Pediatr Orthop. 2012 Dec;32(8):e57-62. doi: 10.1097/BPO.0b013e31826bb0d5. PubMed PMID: 23147632. ](http://www.ncbi.nlm.nih.gov/pubmed/23147632)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23147632)
The blood supply to the lateral condyle fragment enters posterolaterally. Disruption of the blood supply may lead to osteonecrosis of the capitellum, so great care should be taken during open approaches to the elbow in skeletally immature patients, especially during lateral condyle open reduction and internal fixation.
Treatment of lateral condyle fractures in skeletally immature patients may be fraught with danger. The most common complication is persistent stiffness.
Growth arrest is a surprisingly rare complication, considering the fracture usually involves the capitellar physis, and reduction of the physis is often radiographically imperfect even with open reduction. However, this may be an underrecognized complication because arrest of the capitellar physis may not be evident until 1 to 3 years postinjury—beyond the time at which some surgeons or patients believe follow-up is necessary. Growth arrest has been reported with smooth wire fixation and lag screw fixation. The average time to radiographic union of a lateral condyle fracture is 6 weeks.
RECOMMENDED READINGS
10. [Cardona JI, Riddle E, Kumar SJ. Displaced fractures of the lateral humeral condyle: criteria for implant removal. J Pediatr Orthop. 2002 Mar-Apr;22(2):194-7. PubMed PMID: 11856929. ](http://www.ncbi.nlm.nih.gov/pubmed/11856929)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/11856929)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11856929)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11856929)
11. [Stein BE, Ramji AF, Hassanzadeh H, Wohlgemut JM, Ain MC, Sponseller PD. Cannulated Lag Screw Fixation of Displaced Lateral Humeral Condyle Fractures Is Associated With Lower Rates of Open Reduction and Infection Than Pin Fixation. J Pediatr Orthop. 2015 Jul 17. [Epub ahead of print] PubMed PMID: 26192878. ](http://www.ncbi.nlm.nih.gov/pubmed/26192878)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26192878)
12. [Das De S, Bae DS, Waters PM. Displaced humeral lateral condyle fractures in children: should we bury the pins? J Pediatr Orthop. 2012 Sep;32(6):573-8. doi: 10.1097/BPO.0b013e318263a25f. PubMed PMID: 22892618. ](http://www.ncbi.nlm.nih.gov/pubmed/22892618)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22892618)
13. [Cates RA, Mehlman CT. Growth arrest of the capitellar physis after displaced lateral condyle fractures in children. J Pediatr Orthop. 2012 Dec;32(8):e57-62. doi: 10.1097/BPO.0b013e31826bb0d5. PubMed PMID: 23147632. ](http://www.ncbi.nlm.nih.gov/pubmed/23147632)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23147632)
Question 6High Yield
Following application of topical lidocaine, copious arterial bleeding is noted from the region of 1 neurovascular bundle, and the digit remains cool and pale. What is the best next step?
Explanation
Figure 52
Used with permission from Benson LS, Williams CS, Kahle M. Dupuytren’s contracture. J Am Acad Surg. 1998
Jan-Feb;6(1):24-35. Review
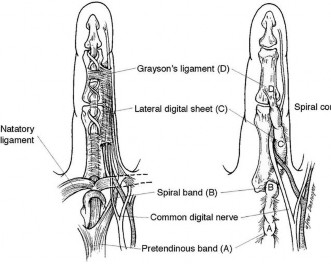
The spiral cord seen in Dupuytren disease arises from the confluence of abnormal fascial thickening of the spiral bands, lateral digital sheet, and Grayson’s ligament. The orientation of these contributing structures results in a continuous band of fibrous tissue spiraling around the neurovascular bundle. As the developing spiral cord contractures from distal to proximal, the cord itself becomes increasingly linear and shorter, causing displacement of the neurovascular bundle both centrally and superficially. This displacement of the neurovascular bundle brings it closer to the skin and midline, making it more vulnerable to surgical trauma.
Studies have demonstrated a high association between a PIP joint flexion contracture and a spiral cord (Figure 52). Spiral cords are also seen in association with a soft, fleshy mass between the proximal digital flexion crease and distal palmar crease in the interdigital space referred to as an interdigital soft-tissue mass. This represents displacement of normal subcutaneous tissues by contracture of the diseased fascia associated with the spiral cord. Dupuytren diathesis, MCP joint contracture, and the presence of knuckle pads are not indicative of a spiral cord.
A complication following surgical treatment of Dupuytren contracture is trauma to the neurovascular bundle. This can be a consequence of blunt or sharp trauma. In the case of traumatic stretch injury from retraction, vasospasm may develop. The treatment of vasospasm includes flexion, warming the digit, and application of topical medication to treat vasospasm. Allowing the newly extended digit to flex is an important first step, particularly in the case of chronic and severe PIP joint contractures. In these cases, the vessel may have shortened over time, and full extension may cause intimal trauma and secondary vasospasm. Cold is also a stimulus for reactive vasospasm, so warming the digit with warm saline irrigation can be helpful. Finally, topically applied lidocaine (without vasoconstrictive additives) can help diminish vasospasm and lead to digital reperfusion. Phentolamine is useful in cases of prolonged vasospasm secondary to administration of anesthetics containing epinephrine. Streptokinase is a thrombolytic agent that may be useful in treatment of embolic or thrombotic vascular disease. Systemic heparin is useful for digital vessel repair but should not be necessary to treat simple vasospasm.
Copious bleeding in the region of the neurovascular bundle following palmar fasciectomy is an indication of potential arterial trauma. In the setting of arterial laceration, direct repair is necessary, particularly when the digit is dysvascular. This means that both digital vessels are involved or that the intact vessel is insufficient to adequately perfuse the digit. During surgery, the vessels can be directly visualized, and arteriography is unlikely to add additional information of value. Streptokinase is not indicated in this situation because it is useful for thrombolysis rather than vascular repair. Ligation of a traumatized digital artery might be appropriate for a digit that is otherwise well perfused; however, this is not appropriate in the setting of a dysvascular digit. Direct suture of the arterial laceration or segmental grafting necessary to restore adequate digital perfusion in this scenario.
RECOMMENDED READINGS
1. [Rayan GM. Dupuytren disease: Anatomy, pathology, presentation, and treatment. J Bone Joint Surg Am. 2007 Jan;89(1):189-98. Review. PubMed PMID: 17256226. ](http://www.ncbi.nlm.nih.gov/pubmed/17256226)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17256226)
2. [Watson HK, Paul H Jr. Pathologic anatomy. Hand Clin. 1991 Nov;7(4):661-8. Review. PubMed PMID: 1769988. ](http://www.ncbi.nlm.nih.gov/pubmed/1769988)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1769988)
3. [Jones NF, Huang JI. Emergency microsurgical revascularization for critical ischemia during surgery for Dupuytren's contracture: a case report. J Hand Surg Am. 2001 Nov;26(6):1125-8. PubMed PMID: 11721263. ](http://www.ncbi.nlm.nih.gov/pubmed/11721263)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11721263)
Used with permission from Benson LS, Williams CS, Kahle M. Dupuytren’s contracture. J Am Acad Surg. 1998
Jan-Feb;6(1):24-35. Review
The spiral cord seen in Dupuytren disease arises from the confluence of abnormal fascial thickening of the spiral bands, lateral digital sheet, and Grayson’s ligament. The orientation of these contributing structures results in a continuous band of fibrous tissue spiraling around the neurovascular bundle. As the developing spiral cord contractures from distal to proximal, the cord itself becomes increasingly linear and shorter, causing displacement of the neurovascular bundle both centrally and superficially. This displacement of the neurovascular bundle brings it closer to the skin and midline, making it more vulnerable to surgical trauma.
Studies have demonstrated a high association between a PIP joint flexion contracture and a spiral cord (Figure 52). Spiral cords are also seen in association with a soft, fleshy mass between the proximal digital flexion crease and distal palmar crease in the interdigital space referred to as an interdigital soft-tissue mass. This represents displacement of normal subcutaneous tissues by contracture of the diseased fascia associated with the spiral cord. Dupuytren diathesis, MCP joint contracture, and the presence of knuckle pads are not indicative of a spiral cord.
A complication following surgical treatment of Dupuytren contracture is trauma to the neurovascular bundle. This can be a consequence of blunt or sharp trauma. In the case of traumatic stretch injury from retraction, vasospasm may develop. The treatment of vasospasm includes flexion, warming the digit, and application of topical medication to treat vasospasm. Allowing the newly extended digit to flex is an important first step, particularly in the case of chronic and severe PIP joint contractures. In these cases, the vessel may have shortened over time, and full extension may cause intimal trauma and secondary vasospasm. Cold is also a stimulus for reactive vasospasm, so warming the digit with warm saline irrigation can be helpful. Finally, topically applied lidocaine (without vasoconstrictive additives) can help diminish vasospasm and lead to digital reperfusion. Phentolamine is useful in cases of prolonged vasospasm secondary to administration of anesthetics containing epinephrine. Streptokinase is a thrombolytic agent that may be useful in treatment of embolic or thrombotic vascular disease. Systemic heparin is useful for digital vessel repair but should not be necessary to treat simple vasospasm.
Copious bleeding in the region of the neurovascular bundle following palmar fasciectomy is an indication of potential arterial trauma. In the setting of arterial laceration, direct repair is necessary, particularly when the digit is dysvascular. This means that both digital vessels are involved or that the intact vessel is insufficient to adequately perfuse the digit. During surgery, the vessels can be directly visualized, and arteriography is unlikely to add additional information of value. Streptokinase is not indicated in this situation because it is useful for thrombolysis rather than vascular repair. Ligation of a traumatized digital artery might be appropriate for a digit that is otherwise well perfused; however, this is not appropriate in the setting of a dysvascular digit. Direct suture of the arterial laceration or segmental grafting necessary to restore adequate digital perfusion in this scenario.
RECOMMENDED READINGS
1. [Rayan GM. Dupuytren disease: Anatomy, pathology, presentation, and treatment. J Bone Joint Surg Am. 2007 Jan;89(1):189-98. Review. PubMed PMID: 17256226. ](http://www.ncbi.nlm.nih.gov/pubmed/17256226)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17256226)
2. [Watson HK, Paul H Jr. Pathologic anatomy. Hand Clin. 1991 Nov;7(4):661-8. Review. PubMed PMID: 1769988. ](http://www.ncbi.nlm.nih.gov/pubmed/1769988)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1769988)
3. [Jones NF, Huang JI. Emergency microsurgical revascularization for critical ischemia during surgery for Dupuytren's contracture: a case report. J Hand Surg Am. 2001 Nov;26(6):1125-8. PubMed PMID: 11721263. ](http://www.ncbi.nlm.nih.gov/pubmed/11721263)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11721263)
Question 7High Yield
A 16-year-old high school football player has anterior shoulder pain after tackling an opponent with his arm in abduction and external rotation.
Explanation
- Anterior shoulder subluxation_
Question 8High Yield
If aspiration findings are negative or equivocal, the diagnosis can be established with
Explanation
- arthroscopy._
Question 9High Yield
In medical malpractice cases against spine surgeons, what factor is associated with a judgement for the plaintiff?
Explanation
■
Medical litigation is common in spine surgery. In a study evaluating “spine surgery” related legal cases from 1988 to 2015, 234 cases met the inclusion criteria. Diagnostic delay cases were significantly associated with plaintiff verdict or settlement. Therapeutic delay cases were also associated with plaintiff verdict or settlement. Catastrophic complications resulted in larger payouts (6.1 million) as compared with noncatastrophic complications (2.9 million). There is no association between specialty (neurosurgery or orthopaedic spine surgery), patient age/sex, and case outcome or award.
Medical litigation is common in spine surgery. In a study evaluating “spine surgery” related legal cases from 1988 to 2015, 234 cases met the inclusion criteria. Diagnostic delay cases were significantly associated with plaintiff verdict or settlement. Therapeutic delay cases were also associated with plaintiff verdict or settlement. Catastrophic complications resulted in larger payouts (6.1 million) as compared with noncatastrophic complications (2.9 million). There is no association between specialty (neurosurgery or orthopaedic spine surgery), patient age/sex, and case outcome or award.
Question 10High Yield
Despite adequate medical management, the patient continues to experience leg pain that interferes with even the lowest demands of daily living. You recommend prophylactic intramedullary nailing of the tibia with interlocking screws. Prior to the surgery, you should recommend
Explanation
- an endocrinology consultation._
Question 11High Yield
What is the most common complication following distal biceps tendon repair?
Explanation
The distal biceps tendon is commonly torn with an eccentric contraction of the biceps when the elbow is taken into extension. Patients treated nonsurgically will note loss of at least 50% supination strength and may develop discomfort with resistive activities. The video shows the squeeze test to evaluate the integrity of the biceps tendon. The test is similar to the Thompson test in the evaluation of an Achilles tendon rupture. The distal arm is squeezed with the elbow flexed 60 to 80 degrees and the forearm pronated. By shortening the musculotendinous unit, the intact biceps tendon will lead to forearm supination. If the biceps is torn, the forearm will not supinate as shown in the video. The maneuver is performed with the elbow in flexion to minimize tension on the brachialis muscle and isolate the biceps. Ruland and associates evaluated 25 patients with suspected distal biceps ruptures and correctly diagnosed all but 1 false-positive result that involved a partial tear. The lacertus fibrosus is not evaluated with this maneuver.
When considering a repair, a 1- or 2-incision technique may be performed. Chavan and associates performed a systematic review comparing the 2 techniques and reported similar complication rates. The 2-incision technique was associated with more instances of significant loss of forearm rotation and more unsatisfactory clinical results. The 1-incision technique is associated with a higher incidence of lateral antebrachial cutaneous neuropathy likely attributable to retraction. The biceps insertion is a thin semilunar area on the posterior/ulnar aspect of the radial tuberosity centered at approximately 30 degrees anterior to the lateral/coronal plane with the arm fully supinated. Forthman and associates used CT scan to asses 30 cadaveric specimens and noted that the biceps tuberosity orientation would prohibit an anatomic repair in 35% of arms for which the 1-incision technique was used.
Mazzocca and associates reported the highest load to failure of the Endobutton (440 newton (N)) compared to fixation with suture anchor (381 N), Wartenberg syndrome (310 N), and an interference screw (232 N). Greenberg and associates noted greater load to failure for the Endobutton (584 N) compared to suture anchor (254 N) and transosseous tunnel (178 N) constructs. Spang and associates reported comparable strength of the Endobutton repair when compared to suture anchors. Fifty N of force is required to hold the elbow flexed at 90 degrees against gravity, which is well below the strength of the repairs studied.
Neuropraxia of the lateral antebrachial cutaneous nerve branch is the most common complication associated with distal biceps repair, with a reported incidence as high as 40%. The nerve branch lies between the biceps and brachialis as it crosses the surgical field in the antecubital fossa. The neuropathy may be related to aggressive retraction, particularly when using the 1-incision technique, and often resolves with time. Cain and associates reported minor complications were common (but major complications uncommon) following distal biceps repair. Reported complications are lateral antebrachial cutaneous paresthesia (26%), radial sensory nerve paresthesia (6%), posterior interosseous nerve injury (4%), and rerupture (2%).
RECOMMENDED READINGS
1. Ruland RT, Dunbar RP, Bowen JD. The biceps squeeze test for diagnosis of distal biceps tendon ruptures. Clin Orthop Relat Res. 2005 Aug;(437):128-31. PubMed PMID: 16056039.
2. Forthman CL, Zimmerman RM, Sullivan MJ, Gabel GT. Cross-sectional anatomy of the bicipital tuberosity and biceps brachii tendon insertion: relevance to anatomic tendon repair. J Shoulder Elbow Surg. 2008 May-Jun;17(3):522-6. doi: 10.1016/j.jse.2007.11.002. Epub 2008 Mar 6. PubMed PMID: 18325797.
3. Chavan PR, Duquin TR, Bisson LJ. Repair of the ruptured distal biceps tendon: a systematic review. Am J Sports Med. 2008 Aug;36(8):1618-24. doi: 10.1177/0363546508321482. Review. PubMed PMID: 18658024.
4. Mazzocca AD, Burton KJ, Romeo AA, Santangelo S, Adams DA, Arciero RA. Biomechanical evaluation of 4 techniques of distal biceps brachii tendon repair. Am J Sports Med. 2007 Feb;35(2):252-
8/. Epub 2006 Dec 27. PubMed PMID: 17192318.
5. Cain RA, Nydick JA, Stein MI, Williams BD, Polikandriotis JA, Hess AV. Complications following distal biceps repair. J Hand Surg Am. 2012 Oct;37(10):2112-7. doi: 10.1016/j.jhsa.2012.06.022. Epub 2012 Aug 30. PubMed PMID: 22938802.
6. Greenberg JA, Fernandez JJ, Wang T, Turner C. EndoButton-assisted repair of distal biceps tendon ruptures. J Shoulder Elbow Surg. 2003 Sep-Oct;12(5):484-90. Erratum in: J Shoulder Elbow Surg. 2005 Mar-Apr;14(2):231. PubMed PMID: 14564273.
7. Spang JT, Weinhold PS, Karas SG. A biomechanical comparison of EndoButton versus suture anchor repair of distal biceps tendon injuries. J Shoulder Elbow Surg. 2006 Jul-Aug;15(4):509-14. PubMed PMID: 16831659.
When considering a repair, a 1- or 2-incision technique may be performed. Chavan and associates performed a systematic review comparing the 2 techniques and reported similar complication rates. The 2-incision technique was associated with more instances of significant loss of forearm rotation and more unsatisfactory clinical results. The 1-incision technique is associated with a higher incidence of lateral antebrachial cutaneous neuropathy likely attributable to retraction. The biceps insertion is a thin semilunar area on the posterior/ulnar aspect of the radial tuberosity centered at approximately 30 degrees anterior to the lateral/coronal plane with the arm fully supinated. Forthman and associates used CT scan to asses 30 cadaveric specimens and noted that the biceps tuberosity orientation would prohibit an anatomic repair in 35% of arms for which the 1-incision technique was used.
Mazzocca and associates reported the highest load to failure of the Endobutton (440 newton (N)) compared to fixation with suture anchor (381 N), Wartenberg syndrome (310 N), and an interference screw (232 N). Greenberg and associates noted greater load to failure for the Endobutton (584 N) compared to suture anchor (254 N) and transosseous tunnel (178 N) constructs. Spang and associates reported comparable strength of the Endobutton repair when compared to suture anchors. Fifty N of force is required to hold the elbow flexed at 90 degrees against gravity, which is well below the strength of the repairs studied.
Neuropraxia of the lateral antebrachial cutaneous nerve branch is the most common complication associated with distal biceps repair, with a reported incidence as high as 40%. The nerve branch lies between the biceps and brachialis as it crosses the surgical field in the antecubital fossa. The neuropathy may be related to aggressive retraction, particularly when using the 1-incision technique, and often resolves with time. Cain and associates reported minor complications were common (but major complications uncommon) following distal biceps repair. Reported complications are lateral antebrachial cutaneous paresthesia (26%), radial sensory nerve paresthesia (6%), posterior interosseous nerve injury (4%), and rerupture (2%).
RECOMMENDED READINGS
1. Ruland RT, Dunbar RP, Bowen JD. The biceps squeeze test for diagnosis of distal biceps tendon ruptures. Clin Orthop Relat Res. 2005 Aug;(437):128-31. PubMed PMID: 16056039.
2. Forthman CL, Zimmerman RM, Sullivan MJ, Gabel GT. Cross-sectional anatomy of the bicipital tuberosity and biceps brachii tendon insertion: relevance to anatomic tendon repair. J Shoulder Elbow Surg. 2008 May-Jun;17(3):522-6. doi: 10.1016/j.jse.2007.11.002. Epub 2008 Mar 6. PubMed PMID: 18325797.
3. Chavan PR, Duquin TR, Bisson LJ. Repair of the ruptured distal biceps tendon: a systematic review. Am J Sports Med. 2008 Aug;36(8):1618-24. doi: 10.1177/0363546508321482. Review. PubMed PMID: 18658024.
4. Mazzocca AD, Burton KJ, Romeo AA, Santangelo S, Adams DA, Arciero RA. Biomechanical evaluation of 4 techniques of distal biceps brachii tendon repair. Am J Sports Med. 2007 Feb;35(2):252-
8/. Epub 2006 Dec 27. PubMed PMID: 17192318.
5. Cain RA, Nydick JA, Stein MI, Williams BD, Polikandriotis JA, Hess AV. Complications following distal biceps repair. J Hand Surg Am. 2012 Oct;37(10):2112-7. doi: 10.1016/j.jhsa.2012.06.022. Epub 2012 Aug 30. PubMed PMID: 22938802.
6. Greenberg JA, Fernandez JJ, Wang T, Turner C. EndoButton-assisted repair of distal biceps tendon ruptures. J Shoulder Elbow Surg. 2003 Sep-Oct;12(5):484-90. Erratum in: J Shoulder Elbow Surg. 2005 Mar-Apr;14(2):231. PubMed PMID: 14564273.
7. Spang JT, Weinhold PS, Karas SG. A biomechanical comparison of EndoButton versus suture anchor repair of distal biceps tendon injuries. J Shoulder Elbow Surg. 2006 Jul-Aug;15(4):509-14. PubMed PMID: 16831659.
Question 12High Yield
After direct lateral (transpsoas) interbody fusion surgery at L3-4, a patient reports numbness in the scrotum, and ipsilateral anterior thigh pain develops. What is the most likely cause?
Explanation
■
The genitofemoral nerve is at risk at almost any level in the lateral transpsoas approach. The nerve provides sensory innervation to the anterior thigh and scrotum/labia. The ilioinguinal nerve provides sensory innervation to the mons pubis or labia in women and the upper scrotum in men. The femoral nerve is responsible for sensation to the anterior and medial aspects of the thigh, leg, and medial foot. It also provides innervation to knee extensor muscles. Prolonged decubitus positioning, especially with jackknife hyperextension, can cause stretching of the femoral nerve and transient weakness of the ipsilateral quadriceps.
The genitofemoral nerve is at risk at almost any level in the lateral transpsoas approach. The nerve provides sensory innervation to the anterior thigh and scrotum/labia. The ilioinguinal nerve provides sensory innervation to the mons pubis or labia in women and the upper scrotum in men. The femoral nerve is responsible for sensation to the anterior and medial aspects of the thigh, leg, and medial foot. It also provides innervation to knee extensor muscles. Prolonged decubitus positioning, especially with jackknife hyperextension, can cause stretching of the femoral nerve and transient weakness of the ipsilateral quadriceps.
Question 13High Yield
In the study design for evaluating the effectiveness of total hip replacement, the endpoint can be only:
Explanation
In the study design, it is paramount that a universal, well-defined endpoint is chosen. In the well-established Scandinavian Hip Registries, this endpoint is revision total hip arthroplasty. Whether this endpoint is sensitive enough is debatable. For more in- depth studies, several other endpoints, such as pain or postoperative functional level, may also be used
Question 14High Yield
Contraindications to high tibial osteotomy include:
Explanation
Lateral compartment narrowing, lateral tibial subluxation of more than 1 cm, medial compartment bone loss of more than 3 mm, and ligament instability are contraindications to high tibial osteotomy
Question 15High Yield
..Figure 33 is the radiograph of a 27-year-old bicyclist who crashes. He has an isolated and closed injury. He is neurovascularly intact in the upper extremity. The lateral fragment is displaced inferiorly by

Explanation
- gravity.
Question 16High Yield
A 13-year-old girl was riding on an all-terrain vehicle when the driver struck a tree. She sustained the injury shown in Figures 45a through 45d. This injury is best described as what type of acetabular fracture pattern?
Explanation
The fracture is a both-column fracture in the Judet/Letournel classification and a C3 in the AO classification. There is extension into the sacroiliac joint along the pelvic brim and comminution along the posterior column above the sciatic notch. Both the anterior and posterior columns are separately broken and displaced. However, the defining feature of a both-column pattern, as seen in this patient, is that all articular fragments are on fracture fragments and no joint surface is left intact to the axial skeleton above. The use of three-dimensional images makes it easier to view the location of the fracture fragments and the amount and direction
of displacement.
REFERENCES: Helfet DL, Beck M, Gautier E, et al: Surgical techniques for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 533-603.
Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
of displacement.
REFERENCES: Helfet DL, Beck M, Gautier E, et al: Surgical techniques for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 533-603.
Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 17High Yield
1222) Which of the following fluoroscopic views is used to assess
intra-articular screw penetration during volar fixation of a distal radius fracture?
intra-articular screw penetration during volar fixation of a distal radius fracture?


Explanation
Due to radial inclination, a true lateral view of the wrist will not show whether screws from a volar plate are intra-articular; a 23° elevated lateral view is needed to adequately assess this.
The amount of elevation will depend on the degree to which the surgeon restores radial inclination; for example, if the surgeon only restores 15° of radial inclination, then the surgeon would only have to elevate the wrist 15° from a true lateral in order to have the radiographic beam point down the joint line. Failure to diagnose intra-articular screws intraoperatively can lead to degenerative changes.
Tweet et al. performed a survey of orthopedic surgeons regarding their preferred method of visualizing screw placement during wrist fixation. The majority of surgeons reported that they obtain multiple views, including AP/PA wrist views, a 23° lateral inclination view, and a true lateral view. They also performed a cadaveric study looking at different x-ray views and screw penetration. They reported that live rotational fluoroscopy provided the highest sensitivity (93%) and specificity (96%) for the detection of intra-articular screw penetration.
Patel et al. evaluated the ability of surgeons at different levels to critically assess distal radius fixation and screw placement. They found that supplementation with a 23° lateral view increased accuracy and confidence in all position, specialty, and experience groups. Confidence scores were significantly higher following the evaluation of three views versus two views. Residents exhibited the greatest improvements in accuracy and confidence. For first-phase (standard view) assessments, accuracy scores were significantly better for attendings with less than 10 years of post-fellowship experience than those with more.
Illustration A is a non-elevated lateral of the wrist, while illustration B is a 23° elevated lateral radiograph. Illustration C is an example of a skyline view, which assesses for screws penetrating the dorsal cortex.
Incorrect Answers:
Answer 1: The dorsal skyline view shows dorsal screw length and is useful to
check for long distal screws.
Answers 2 and 3: The AP and PA wrist views do not show intra-articular screw penetration due to the volar tilt and concavity of the joint.
Answer 5: A 45° oblique lateral view does not visualize the joint as this angle does not match the radial inclination.
The amount of elevation will depend on the degree to which the surgeon restores radial inclination; for example, if the surgeon only restores 15° of radial inclination, then the surgeon would only have to elevate the wrist 15° from a true lateral in order to have the radiographic beam point down the joint line. Failure to diagnose intra-articular screws intraoperatively can lead to degenerative changes.
Tweet et al. performed a survey of orthopedic surgeons regarding their preferred method of visualizing screw placement during wrist fixation. The majority of surgeons reported that they obtain multiple views, including AP/PA wrist views, a 23° lateral inclination view, and a true lateral view. They also performed a cadaveric study looking at different x-ray views and screw penetration. They reported that live rotational fluoroscopy provided the highest sensitivity (93%) and specificity (96%) for the detection of intra-articular screw penetration.
Patel et al. evaluated the ability of surgeons at different levels to critically assess distal radius fixation and screw placement. They found that supplementation with a 23° lateral view increased accuracy and confidence in all position, specialty, and experience groups. Confidence scores were significantly higher following the evaluation of three views versus two views. Residents exhibited the greatest improvements in accuracy and confidence. For first-phase (standard view) assessments, accuracy scores were significantly better for attendings with less than 10 years of post-fellowship experience than those with more.
Illustration A is a non-elevated lateral of the wrist, while illustration B is a 23° elevated lateral radiograph. Illustration C is an example of a skyline view, which assesses for screws penetrating the dorsal cortex.
Incorrect Answers:
Answer 1: The dorsal skyline view shows dorsal screw length and is useful to
check for long distal screws.
Answers 2 and 3: The AP and PA wrist views do not show intra-articular screw penetration due to the volar tilt and concavity of the joint.
Answer 5: A 45° oblique lateral view does not visualize the joint as this angle does not match the radial inclination.
Question 18High Yield
A 7-month-old girl is newly seen for a dislocation of the left hip. The newborn exam was unremarkable; there was no history of trauma or evidence of spasticity. Recommended treatment includes:
Explanation
An exam under anesthesia and arthrogram should be performed. C losed reduction must be performed if the hip reduces with a medial dye pool less than 4 mm and a safe zone greater than 20°.
The Pavlik harness is not strong enough to hold an infant older than 4 to 6 months. Open reduction is reserved for hips that do not reduce by closed means.
A Salter osteotomy is only indicated if the hip is still unstable after an open reduction.
The Pavlik harness is not strong enough to hold an infant older than 4 to 6 months. Open reduction is reserved for hips that do not reduce by closed means.
A Salter osteotomy is only indicated if the hip is still unstable after an open reduction.
Question 19High Yield
Glucose control assessment is best achieved by ordering which blood test?
Explanation
- Hemoglobin A1C
Question 20High Yield
Which of the following zones of the physis is involved in Salter Harris Type I and II fractures:
Explanation
Salter Harris Type I and II fractures occur through the zone of provisional calcification or through the hypertrophiCzone. The reserve and proliferative zone remain intact and growth can proceed normal after healing of the fracture
Question 21High Yield
What nerve is at greatest risk of harm from the portal shown in Figure 36?
Explanation
The figure shows the anterolateral portal for elbow arthroscopy, and injury to the radial nerve has been reported in conjunction with this portal site. Studies have shown that closer proximity to the radial nerve is associated with more distal portal sites. The lateral and posterior antebrachial cutaneous nerves are both at less risk of injury. The ulnar and median nerves are both fairly remote to this location.
REFERENCES: Field LD, Altchek DW, Warren RF, O’Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Papilion JD, Neff RS, Shall LM: Compression neuropathy of the radial nerve as a complication of elbow arthroscopy: A case report and review of the literature. Arthroscopy 1988;4:284-286.
Poehling GG, Whipple TL, Sisco L, Goldman B: Elbow arthroscopy: A new technique. Arthroscopy 1989;5:222-224.
REFERENCES: Field LD, Altchek DW, Warren RF, O’Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Papilion JD, Neff RS, Shall LM: Compression neuropathy of the radial nerve as a complication of elbow arthroscopy: A case report and review of the literature. Arthroscopy 1988;4:284-286.
Poehling GG, Whipple TL, Sisco L, Goldman B: Elbow arthroscopy: A new technique. Arthroscopy 1989;5:222-224.
Question 22High Yield
An 8-year-old girl with a history of Down syndrome is being evaluated to participate in gym activities. She is otherwise doing well and has appropriate motor developmental milestones. Her neurological exam is normal and cervical spine AP, lateral, flexion and extension radiographs reveal an atlanto-dens interval (ADI) of 7 mm, and normal occipitoatlantal mobility. What is the most appropriate recommendation?
Explanation
■
Down syndrome, with an incidence of 1 in 660 live births, remains the most common human malformation pattern. Individuals with Down syndrome have an increased incidence of congenital heart disease, ophthalmologic disorders, gastrointestinal disorders, thyroid disease, and leukemia.
Musculoskeletal problems commonly occur in Down syndrome and include patellofemoral and hip instability, bunions, severe flatfoot, and instability of cervical spine, which could result in cord compromise and neurological impairment or death.
Increased ADI in the Down syndrome population has not been directly correlated with a concomitant increase in neurologic compromise. The radiographs of the cervical spine in the Down syndrome population must be evaluated by standards specific to that population, and not by traditional standards derived from the radiographs of the cervical spine in the general population. Radiographic evaluation of the cervical spine in the young athlete with Down syndrome is only one component of the preparticipation screening and must be correlated with a pertinent history of physical activity and a detailed physical exam.
When a Down patient presents with an ADI >10 mm and evidence of spinal cord compression, there is little disagreement about the need for surgical intervention. When the ADI is between 4.5 mm and 10 mm in a patient with no decrease in physical activities and no abnormal neurological finding, this may represent hypermobility rather than instability in the Down syndrome population. With an ADI between 4.5 mm and 10 mm, athletes with Down syndrome may participate in most activities but have been advised to avoid high-risk sports such as diving and football.
Down syndrome, with an incidence of 1 in 660 live births, remains the most common human malformation pattern. Individuals with Down syndrome have an increased incidence of congenital heart disease, ophthalmologic disorders, gastrointestinal disorders, thyroid disease, and leukemia.
Musculoskeletal problems commonly occur in Down syndrome and include patellofemoral and hip instability, bunions, severe flatfoot, and instability of cervical spine, which could result in cord compromise and neurological impairment or death.
Increased ADI in the Down syndrome population has not been directly correlated with a concomitant increase in neurologic compromise. The radiographs of the cervical spine in the Down syndrome population must be evaluated by standards specific to that population, and not by traditional standards derived from the radiographs of the cervical spine in the general population. Radiographic evaluation of the cervical spine in the young athlete with Down syndrome is only one component of the preparticipation screening and must be correlated with a pertinent history of physical activity and a detailed physical exam.
When a Down patient presents with an ADI >10 mm and evidence of spinal cord compression, there is little disagreement about the need for surgical intervention. When the ADI is between 4.5 mm and 10 mm in a patient with no decrease in physical activities and no abnormal neurological finding, this may represent hypermobility rather than instability in the Down syndrome population. With an ADI between 4.5 mm and 10 mm, athletes with Down syndrome may participate in most activities but have been advised to avoid high-risk sports such as diving and football.
Question 23High Yield
Figure 19 is an anteroposterior pelvis radiograph of a 60-year-old woman who has a 4-month history of right hip pain. She has a
medical history of lupus and has used
21
prednisone in the past, but not currently.
Her pain is persistent despite use of over-the-counter pain medications and activity modifications. What is the most appropriate treatment at this point?
medical history of lupus and has used
21
prednisone in the past, but not currently.
Her pain is persistent despite use of over-the-counter pain medications and activity modifications. What is the most appropriate treatment at this point?

Explanation
This scenario describes osteonecrosis of the hip, likely attributable to chronic corticosteroid use. Her radiographs show bilateral hip involvement with whole-head involvement and collapse of the femoral head. Observation, protected weight bearing, and bisphosphonates have been advocated during the precollapse stage, but, considering the advanced
involvement of the femoral heads, these treatments are not indicated. Hip arthroplasty is the most reliable treatment option at this point to resolve her symptoms. Total hip resurfacing is not indicated for multiple reasons, including poor bone stock from corticosteroid use and her age. Large-head involvement and concerns about metal-on-metal articulation in someone with potential for renal impairment (such as a patient with lupus) also are contraindications to total hip resurfacing. Total hip arthroplasty will offer the best chance for success.
RECOMMENDED READINGS
1. Mont M, Bezwasa H. Osteonecrosis: Strategies for treatment. In: Callaghan JJ, Rosenberg AG, Rubash HE, eds. The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:477-499.
2. [Lieberman JR, Berry DJ, Mont MA, Aaron RK, Callaghan JJ, Rajadhyaksha AD, Urbaniak JR. Osteonecrosis of the hip: management in the 21st century. Instr Course Lect. 2003;52:337-55. Review. PubMed PMID: 12690862.](http://www.ncbi.nlm.nih.gov/pubmed/12690862)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690862)
involvement of the femoral heads, these treatments are not indicated. Hip arthroplasty is the most reliable treatment option at this point to resolve her symptoms. Total hip resurfacing is not indicated for multiple reasons, including poor bone stock from corticosteroid use and her age. Large-head involvement and concerns about metal-on-metal articulation in someone with potential for renal impairment (such as a patient with lupus) also are contraindications to total hip resurfacing. Total hip arthroplasty will offer the best chance for success.
RECOMMENDED READINGS
1. Mont M, Bezwasa H. Osteonecrosis: Strategies for treatment. In: Callaghan JJ, Rosenberg AG, Rubash HE, eds. The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:477-499.
2. [Lieberman JR, Berry DJ, Mont MA, Aaron RK, Callaghan JJ, Rajadhyaksha AD, Urbaniak JR. Osteonecrosis of the hip: management in the 21st century. Instr Course Lect. 2003;52:337-55. Review. PubMed PMID: 12690862.](http://www.ncbi.nlm.nih.gov/pubmed/12690862)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690862)
Question 24High Yield
Figures 1 through 4 are the AP and lateral radiographs and MR images of a 12-year-old postmenarchal girl who injured her right knee playing basketball 2 weeks ago. She developed significant swelling and pain and was unable to bear weight. How should the family be counseled regarding expectations and outcomes following this injury?

Explanation
■
Historically, anterior cruciate ligament (ACL) injuries in skeletally immature patients were treated nonsurgically with bracing, physical therapy, and activity modification because of concerns about risk to the physis during ACL reconstruction. Current evidence suggests that patients treated surgically have less knee instability, higher rates of return to activity, higher functional scores, and lower rates of subsequent meniscal tear. One of the most common complications encountered after ACL reconstruction in this patient population is secondary injury of the same or the contralateral knee, which has been found to be >5 times greater than that of healthy controls. Nearly 30% of athletes in one cohort sustained a second ACL injury within 24 months of return to sport, with approximately one-third of these injuries occurring in the ipsilateral knee and twothirds occurring in the contralateral knee. Thus, although most young athletes are able to return to sports after reconstruction of their ACL, they have a significantly higher risk of secondary ACL injury (ipsilateral or contralateral) compared with the adult population.
■
Historically, anterior cruciate ligament (ACL) injuries in skeletally immature patients were treated nonsurgically with bracing, physical therapy, and activity modification because of concerns about risk to the physis during ACL reconstruction. Current evidence suggests that patients treated surgically have less knee instability, higher rates of return to activity, higher functional scores, and lower rates of subsequent meniscal tear. One of the most common complications encountered after ACL reconstruction in this patient population is secondary injury of the same or the contralateral knee, which has been found to be >5 times greater than that of healthy controls. Nearly 30% of athletes in one cohort sustained a second ACL injury within 24 months of return to sport, with approximately one-third of these injuries occurring in the ipsilateral knee and twothirds occurring in the contralateral knee. Thus, although most young athletes are able to return to sports after reconstruction of their ACL, they have a significantly higher risk of secondary ACL injury (ipsilateral or contralateral) compared with the adult population.
Question 25High Yield
Which of the following features is associated with type 2 osteoporosis:
Explanation
Type 1 osteoporosis is the most common form of osteoporosis and is found in women during postmenopausal years. Type 1 osteoporosis is related to estrogen deficiency rather than a problem in calcium intake or absorption.
Features of type 1 osteoporosis include:
Female to male ratio is 6:1
High turnover osteoporosis
Bone loss rate of 2% to 3% per year for 6 to 10 years following menopause
Trabecular bone is most affected
Related to estrogen deficiency rather than calcium intake
Type 2 osteoporosis, also called senile or involutional osteoporosis, is a low turnover osteoporosis and principally occurs in patients older than 75 years of age.
Features of type 2 osteoporosis include: Female to male ratio is 2:1
Patients older than 75 years of age
Low turnover osteoporosis
Trabecular and cortical bone affected
Associated with hip fractures
Related to a lifelong deficiency of calcium
Features of type 1 osteoporosis include:
Female to male ratio is 6:1
High turnover osteoporosis
Bone loss rate of 2% to 3% per year for 6 to 10 years following menopause
Trabecular bone is most affected
Related to estrogen deficiency rather than calcium intake
Type 2 osteoporosis, also called senile or involutional osteoporosis, is a low turnover osteoporosis and principally occurs in patients older than 75 years of age.
Features of type 2 osteoporosis include: Female to male ratio is 2:1
Patients older than 75 years of age
Low turnover osteoporosis
Trabecular and cortical bone affected
Associated with hip fractures
Related to a lifelong deficiency of calcium
Question 26High Yield
A 4-year-old boy has had an isolated painful limp for the past month. He is diagnosed with Legg-Calve- Perthes disease (LCPD) that involves nearly all of his capital femoral epiphysis. Which of the following best describes his prognosis?

Explanation
DISCUSSION: This young child with total head involvement LCPD is at some risk of a poor outcome due to the extent of his disease. Most children of this age will recover well with a good outcome. He is more likely to end up with a spherical femoral head than an older child with the same extent of involvement.
REFERENCES: Schoenecker PL, Stone JW, Capelli AM: Legg-Perthes disease in children under 6 years old. Orthop Rev 1993;22:201-208.
Rosenfeld SB, Herring JA, Chao JC: Legg-Calve-Perthes disease: A review of cases with onset before six years of age. J Bone Joint Surg Am 2007;89:2712-2722.
Figure 78
REFERENCES: Schoenecker PL, Stone JW, Capelli AM: Legg-Perthes disease in children under 6 years old. Orthop Rev 1993;22:201-208.
Rosenfeld SB, Herring JA, Chao JC: Legg-Calve-Perthes disease: A review of cases with onset before six years of age. J Bone Joint Surg Am 2007;89:2712-2722.
Figure 78
Question 27High Yield
A 28-year-old man is thrown from his motorcycle and sustains the closed injury seen in Figure A. The limb remains neurovascularly intact. What is the most appropriate initial treatment of this injury?

Explanation
Figure A shows a significantly displaced, high-energy proximal tibia fracture with intra-articular extension. Appropriate initial treatment includes application of a spanning external fixation device with fasciotomy if needed.
The referenced article by Egol et al noted a low rate of wound infection, improved access to soft tissues, prevention of further articular damage, and osseous stabilization. They reported the downside being residual knee stiffness.
The referenced article by Egol et al noted a low rate of wound infection, improved access to soft tissues, prevention of further articular damage, and osseous stabilization. They reported the downside being residual knee stiffness.
Question 28High Yield
Which of the following is the rate-limiting step in the production of biologically active Vitamin D:
Explanation
The addition of a second hydroxyl group at the 1 position to 25 hydroxy vitamin D3 is the rate-limiting step in the formation of the active from of vitamin D3. Impaired renal function is common in older individuals
Question 29High Yield
C ardinal signs of evenomation include all of the following except:
Explanation
The cardinal signs of evenomation appear between 10 minutes and 4 hours after a person is bitten. The signs include fang marks, pain, swelling, and local necrosis. C yanosis is not considered a cardinal sign of evenomation.
Question 30High Yield
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?**
Explanation
Internal impingement of the shoulder is now a well-recognized cause of shoulder pain in the throwing athlete. First described by Walch and associates, it involves contact of the rotator cuff and labrum in the maximally externally rotated and abducted shoulder, such as in the late cocking phase of the throwing motion. Schickendantz and associates have shown this contact to be physiologic in most patients and becoming pathologic with repetitive overhead activity.
REFERENCES: Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
McFarland EG, Hsu CY, Neira C, O’Neil O: Internal impingement of the shoulder: A clinical and arthroscopic analysis. J Shoulder Elbow Surg 1999;8:458-460.
REFERENCES: Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
McFarland EG, Hsu CY, Neira C, O’Neil O: Internal impingement of the shoulder: A clinical and arthroscopic analysis. J Shoulder Elbow Surg 1999;8:458-460.
Question 31High Yield
A newborn girl is noted to have decreased movement in the right upper extremity. She was large (10 lbs) at birth and was delivered vaginally with shoulder dystocia. She does not have elbow flexion, external shoulder rotation, or abduction. She has had weak finger flexion for 3 months. At 4-months-old, she regains the ability to flex her elbow. Recommended treatment includes:
Explanation
C onservative therapy is predicted to bring a good result because biceps are returning at four months of age. However, stretching of the shoulder is indicated to maintain a range of external rotation and abduction.
Magnetic resonance imaging is only indicated if there is a need to consider microvascular repair.
Tendon transfers are performed later (at several years of age), if shoulder abduction and external rotation are significantly limited.
Microvascular repair is mainly considered in patients who do not have return of biceps function by five months.
Open reduction is indicated later (if the shoulder joint is subluxated or severely contracted) after motor recovery has reached a plateau.
Magnetic resonance imaging is only indicated if there is a need to consider microvascular repair.
Tendon transfers are performed later (at several years of age), if shoulder abduction and external rotation are significantly limited.
Microvascular repair is mainly considered in patients who do not have return of biceps function by five months.
Open reduction is indicated later (if the shoulder joint is subluxated or severely contracted) after motor recovery has reached a plateau.
Question 32High Yield
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by
Explanation
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by the use of a direct lateral approach to the ankle. The superficial peroneal nerve and its branches exit the fascial hiatus approximately 9 cm to 10 cm proximal to the tip of the distal fibula with a range of 4 cm to 13 cm, and their course is typically anterior to the midlateral plane of the fibula. However, small branches may course across the surgical plane directly laterally. A posterior-lateral approach diminishes the risk of injury to the superficial peroneal nerve and its branches; however, by moving farther posterior, the sural nerve and its branches may be at increased risk. Cast immobilization may injure the cutaneous nerves about the ankle; however, the risks are greater with surgical intervention. A medial or anterior-medial approach to the ankle will not injure the superficial peroneal nerve at the ankle level.
REFERENCES: Redfern DJ, Sauve PS, Sakellariou A: Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771-774.
Miller SD: Ankle fractures, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1341-1366.
REFERENCES: Redfern DJ, Sauve PS, Sakellariou A: Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771-774.
Miller SD: Ankle fractures, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1341-1366.
Question 33High Yield
Which ligament is most important in maintaining stability of the scapholunate joint?


Explanation
Scapholunate instability frequently develops as a consequence of blunt trauma to the wrist and is associated with significant clinical morbidity. The ligamentous anatomy and kinematics of the
carpus are complex and have been the focus of much clinical and biomechanical research. Multiple ligamentous structures contribute to the structure and function of the scapholunate articulation.
The wrist can be viewed as a 3-tiered structure with the forearm bones and carpometacarpal segments separated by the intercalated proximal row. The link between the distal and proximal carpal rows depends in large part on the scapholunate articulation. Instability of this articulation leads to altered kinematics and clinical symptomatology.
Multiple ligaments contribute to scapholunate joint integrity. They can be divided into intrinsic and extrinsic groups. The scapholunate interosseous ligament (SLIL) is described as intrinsic and is a C-shaped ligamentous structure that can be divided into 3 parts for descriptive purposes. The dorsal component is the thickest, with an average thickness of 3 mm and is approximately 5 mm in proximal-distal dimension. It attaches the proximal pole of the scaphoid to the dorsal aspect of the lunate. The proximal component has variable thickness and is composed largely of fibrocartilage. The volar component averages only 1 mm in thickness and 5 mm in proximal-distal dimension. It merges with the radioscapholunate ligament proximally and with the radioscaphocapitate (RSC) ligament distally. The other stabilizers are referred to as extrinsic because they connect the scaphoid and lunate to the radius and other carpal bones. Several ligaments at the palmar aspect of the carpus contribute to scapholunate stability. The RSC ligament runs from the radial styloid to the scaphoid fossa. The long radiolunate ligament (LRL) extends from the volar radius to the volar lunate. The radioscapholunate ligament (RSL) attaches the volar distal radius to the volar aspect of the SLIL. The scaphotrapezial ligament (ST) attaches the distal pole of the scaphoid to the trapezium.
Other extrinsic ligaments contributing to scapholunate stability are found at the dorsal aspect of the carpus. The dorsal radiocarpal ligament (DRC) originates from the dorsal distal radius and inserts onto the dorsum of the lunate, triquetrum, and lunotriquetral interosseous ligament. The dorsal intercarpal ligament (DIC) attaches to the dorsum of the triquetrum and extends radially, past the lunate, to insert on the dorsal distal pole of the scaphoid.
Although the exact contribution of each ligament to scapholunate stability is not fully understood, some interesting observations have been made. The SLIL appears to be the primary stabilizing structure. Sectioning the SLIL alone, without disturbing the extrinsic stabilizers, leads to substantial widening of the scapholunate interval and altered motion patterns of both the scaphoid and lunate. Sectioning the RSC and ST ligaments with an intact SLIL does not significantly alter scaphoid or lunate kinematics with respect to motion in the flexion-extension and radial-ulnar planes. Similarly, sectioning of the ST and DIC ligaments by another study group demonstrated no alterations in scapholunate motion, whereas DRC sectioning led to only modest ulnar deviation of the lunate. Although many ligaments contribute to the stability of the scapholunate joint, the SLIL appears to be the primary stabilizer. The most robust and functionally important part of the SLIL appears to be the dorsal component. The role of the secondary stabilizers is significant, and more work is necessary to fully understand their contributions.
RECOMMENDED READINGS
1. [Rajan PV, Day CS. Scapholunate Interosseous Ligament Anatomy and Biomechanics. J Hand Surg Am. 2015 Aug;40(8):1692-702. doi: 10.1016/j.jhsa.2015.03.032. Epub 2015 Jul 1. Review. PubMed PMID: 26143029.](http://www.ncbi.nlm.nih.gov/pubmed/26143029)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26143029)
2. Drewniany JJ, Palmer AK, Flatt AE. The scaphotrapezial ligament complex: an anatomic and biomechanical study. J Hand Surg Am. 1985 Jul;10(4):492-8. PubMed PMID: 4020059.
3. Short WH, Werner FW, Green JK, Masaoka S. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: Part II. J Hand Surg Am. 2005 Jan;30(1):24-34. PubMed PMID: 15680552.
4. Short WH, Werner FW, Green JK, Sutton LG, Brutus JP. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: part III. J Hand Surg Am. 2007 Mar;32(3):297-309.
**
carpus are complex and have been the focus of much clinical and biomechanical research. Multiple ligamentous structures contribute to the structure and function of the scapholunate articulation.
The wrist can be viewed as a 3-tiered structure with the forearm bones and carpometacarpal segments separated by the intercalated proximal row. The link between the distal and proximal carpal rows depends in large part on the scapholunate articulation. Instability of this articulation leads to altered kinematics and clinical symptomatology.
Multiple ligaments contribute to scapholunate joint integrity. They can be divided into intrinsic and extrinsic groups. The scapholunate interosseous ligament (SLIL) is described as intrinsic and is a C-shaped ligamentous structure that can be divided into 3 parts for descriptive purposes. The dorsal component is the thickest, with an average thickness of 3 mm and is approximately 5 mm in proximal-distal dimension. It attaches the proximal pole of the scaphoid to the dorsal aspect of the lunate. The proximal component has variable thickness and is composed largely of fibrocartilage. The volar component averages only 1 mm in thickness and 5 mm in proximal-distal dimension. It merges with the radioscapholunate ligament proximally and with the radioscaphocapitate (RSC) ligament distally. The other stabilizers are referred to as extrinsic because they connect the scaphoid and lunate to the radius and other carpal bones. Several ligaments at the palmar aspect of the carpus contribute to scapholunate stability. The RSC ligament runs from the radial styloid to the scaphoid fossa. The long radiolunate ligament (LRL) extends from the volar radius to the volar lunate. The radioscapholunate ligament (RSL) attaches the volar distal radius to the volar aspect of the SLIL. The scaphotrapezial ligament (ST) attaches the distal pole of the scaphoid to the trapezium.
Other extrinsic ligaments contributing to scapholunate stability are found at the dorsal aspect of the carpus. The dorsal radiocarpal ligament (DRC) originates from the dorsal distal radius and inserts onto the dorsum of the lunate, triquetrum, and lunotriquetral interosseous ligament. The dorsal intercarpal ligament (DIC) attaches to the dorsum of the triquetrum and extends radially, past the lunate, to insert on the dorsal distal pole of the scaphoid.
Although the exact contribution of each ligament to scapholunate stability is not fully understood, some interesting observations have been made. The SLIL appears to be the primary stabilizing structure. Sectioning the SLIL alone, without disturbing the extrinsic stabilizers, leads to substantial widening of the scapholunate interval and altered motion patterns of both the scaphoid and lunate. Sectioning the RSC and ST ligaments with an intact SLIL does not significantly alter scaphoid or lunate kinematics with respect to motion in the flexion-extension and radial-ulnar planes. Similarly, sectioning of the ST and DIC ligaments by another study group demonstrated no alterations in scapholunate motion, whereas DRC sectioning led to only modest ulnar deviation of the lunate. Although many ligaments contribute to the stability of the scapholunate joint, the SLIL appears to be the primary stabilizer. The most robust and functionally important part of the SLIL appears to be the dorsal component. The role of the secondary stabilizers is significant, and more work is necessary to fully understand their contributions.
RECOMMENDED READINGS
1. [Rajan PV, Day CS. Scapholunate Interosseous Ligament Anatomy and Biomechanics. J Hand Surg Am. 2015 Aug;40(8):1692-702. doi: 10.1016/j.jhsa.2015.03.032. Epub 2015 Jul 1. Review. PubMed PMID: 26143029.](http://www.ncbi.nlm.nih.gov/pubmed/26143029)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26143029)
2. Drewniany JJ, Palmer AK, Flatt AE. The scaphotrapezial ligament complex: an anatomic and biomechanical study. J Hand Surg Am. 1985 Jul;10(4):492-8. PubMed PMID: 4020059.
3. Short WH, Werner FW, Green JK, Masaoka S. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: Part II. J Hand Surg Am. 2005 Jan;30(1):24-34. PubMed PMID: 15680552.
4. Short WH, Werner FW, Green JK, Sutton LG, Brutus JP. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: part III. J Hand Surg Am. 2007 Mar;32(3):297-309.
**
Question 34High Yield
What is the incidence of malignant transformation for the lesion shown in Figures 24a and 24b?







Explanation
The lesion shown is an osteochondroma of the distal femur. In the vast majority of cases these are benign lesions, but malignant transformation to chondrosarcoma can occur in approximately 1% of solitary lesions. The malignant transformation rate can be as high as 25% to 30% among those with multiple hereditary exostosis. For solitary lesions, degeneration to chondrosarcoma occurs more commonly in sessile lesions, as opposed to those that are pedunculated, and in lesions that are located in the pelvis. Tumors typically become painful with malignant degeneration. Usually, if chondrosarcoma develops, it is a low-grade tumor.
RECOMMENDED READINGS
16. [T Scharschmidt, J Mayerson. Chrondrosarcoma. Orthopaedic Knowledge Online Journal. November 2010. ](http://www.aaos.org/OKOJ/vol8/issue10/ONC021/)http://www.aaos.org/OKOJ/vol8/issue10/ONC021/ Accessed May 2, 2016.
17. [Marco RA, Gitelis S, Brebach GT, Healey JH. Cartilage tumors: evaluation and treatment. J Am Acad Orthop Surg. 2000 Sep-Oct;8(5):292-304. Review. PubMed PMID: 11029557. ](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11029557)
RECOMMENDED READINGS
16. [T Scharschmidt, J Mayerson. Chrondrosarcoma. Orthopaedic Knowledge Online Journal. November 2010. ](http://www.aaos.org/OKOJ/vol8/issue10/ONC021/)http://www.aaos.org/OKOJ/vol8/issue10/ONC021/ Accessed May 2, 2016.
17. [Marco RA, Gitelis S, Brebach GT, Healey JH. Cartilage tumors: evaluation and treatment. J Am Acad Orthop Surg. 2000 Sep-Oct;8(5):292-304. Review. PubMed PMID: 11029557. ](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11029557)
Question 35High Yield
The vessel seen in the clinical photographs shown in Figures 50a and 50b (1,2 intercompartmental supraretinacular artery) is being dissected to be used as a source of vascularized bone graft for a patient who is scheduled to undergo internal fixation of a scaphoid nonunion. This vessel is a branch of what artery?
Explanation
The 1,2 intercompartmental supraretinacular artery is a branch of the radial artery. The vessel provides a reliable source of vascularized bone graft with an adequate pedicle length for use in scaphoid nonunions.
REFERENCES: Sheetz KK, Bishop AT, Berger RA: The arterial blood supply of the distal radius and ulna and its potential use in vascularized pedicled bone grafts. J Hand Surg 1995;20:902-914.
Steinmann SP, Bishop AT, Berger RA: Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg
2002;27:391-401.
REFERENCES: Sheetz KK, Bishop AT, Berger RA: The arterial blood supply of the distal radius and ulna and its potential use in vascularized pedicled bone grafts. J Hand Surg 1995;20:902-914.
Steinmann SP, Bishop AT, Berger RA: Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg
2002;27:391-401.
Question 36High Yield
Corticosteroids decrease bone mass through which of the following mechanisms:
Explanation
Corticosteroids decrease overall protein synthesis. In the intestines, corticosteroids decrease calcium-binding proteins, hence decreasing the absorption of calcium.
Corticosteroids:
Decrease overall protein synthesis
Increase calcium excretion in the kidney
Inhibit bone formation and absorption at high doses
With the above changes, a state of secondary hyperparathyroidism exists. Correct Answer: Inhibiting calcium absorption in the intestines
Corticosteroids:
Decrease overall protein synthesis
Increase calcium excretion in the kidney
Inhibit bone formation and absorption at high doses
With the above changes, a state of secondary hyperparathyroidism exists. Correct Answer: Inhibiting calcium absorption in the intestines
Question 37High Yield
A 38-year-old woman who tripped and fell on her outstretched arm reports pain with movement. Examination reveals swelling. AP and lateral radiographs are shown in Figures 43a and 43b. Management should consist of
Explanation
The patient has a type I (Hahn-Steinthal) capitellar fracture that is best seen on the lateral radiograph. If a fracture fragment is seen proximal to the radial head, a capitellar fracture is the most likely injury because radial head fractures do not migrate proximally. The fragment is large enough for fixation. Excision is the preferred treatment for small shear osteochondral type II (Kocher-Lorenz) capitellar fractures. Closed reduction usually is not successful because of rotation of the displaced fragment.
REFERENCES: Mehdian H, McKee M: Management of proximal and distal humerus fractures. Orthop Clin North Am 2000;31:115-127.
Ring D, Jupiter J, Gulotta L: Articular fractures of the distal part of the humerus. J Bone Joint Surg Am 2003;85:232-238.
REFERENCES: Mehdian H, McKee M: Management of proximal and distal humerus fractures. Orthop Clin North Am 2000;31:115-127.
Ring D, Jupiter J, Gulotta L: Articular fractures of the distal part of the humerus. J Bone Joint Surg Am 2003;85:232-238.
Question 38High Yield
A 21-year-old pitcher reports shoulder pain with hard throwing. He notes that the pain occurs in the early acceleration phase of his throw. Given his history, what structures are at greatest risk for injury?
Explanation
Internal impingement in the thrower’s shoulder occurs in the abducted, externally rotated position as described by Walch and associates. The injury is thought to occur from repetitive contact between the posterosuperior portion of the labrum and glenoid against the articular side of the rotator cuff and greater tuberosity.
REFERENCES: Paley KJ, Jobe FW, Pink MM, et al: Arthroscopic findings in the overhand throwing athlete: Evidence for posterior internal impingement of the rotator cuff. Arthroscopy 2000;16:35-40.
Jazrawi LM, McCluskey GM III, Andrews JR: Superior labral anterior and posterior lesions and internal impingement in the overhead athlete. Instr Course Lect 2003;52:43-63.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg
1992;1:238-245.
REFERENCES: Paley KJ, Jobe FW, Pink MM, et al: Arthroscopic findings in the overhand throwing athlete: Evidence for posterior internal impingement of the rotator cuff. Arthroscopy 2000;16:35-40.
Jazrawi LM, McCluskey GM III, Andrews JR: Superior labral anterior and posterior lesions and internal impingement in the overhead athlete. Instr Course Lect 2003;52:43-63.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg
1992;1:238-245.
Question 39High Yield
Which of the following statements is true concerning atlanto-occipital dislocations in children:
Explanation
Pediatric atlanto-occipital dislocation is increasing in frequency due to improved emergency care. Although the injuries are sometimes fatal and are often accompanied by severe spinal cord injury, this is not always the case. Although the dens-basion distance should be less than 10 mm and the power ratio should be less than 1 in normals, these are not always abnormal in children with such injuries. C linical and radiographic correlation, with computer tomography or magnetic resonance imaging if needed, are called for to maximize diagnosis.
Question 40High Yield
Which of the following resist articular cartilage compression and fluid flow:
Explanation
Type II collagen fibers resist tensile and shear deformation forces in the articular cartilage.
In contrast, the glycosaminoglycan aggregates resist articular cartilage compression and fluid flow.
In contrast, the glycosaminoglycan aggregates resist articular cartilage compression and fluid flow.
Question 41High Yield
A 72-year-old man with a previous contralateral ankle fusion, rheumatoid arthritis, and 5 degrees of valgus; he has pursued nonsurgical treatment for 30 years and now has unrelenting pain
Explanation
- Ankle replacement
Question 42High Yield
A 40-year-old male laborer with an acute left shoulder injury (Figures 94a and 94b).


Explanation
- Open reduction and internal fixation (ORIF)_
Question 43High Yield
Initial treatment for De Quervain disease involves:
Explanation
Initial treatment for De Quervain tenosynovitis involves rest and splinting with steroid injection into the first dorsal compartment. The splint should be worn as much as possible for 3 to 4 weeks. The extensor carpi radialis brevis has been implicated in lateral epicondulitis. The extensor pollicis longus can be a source of pain as it wraps over the wrist extensor giving the classic symptoms of intersection syndrome between the second and third dorsal compartments. Surgical release is only indicated in persistent cases that have failed conservative management. In 20% to 30% of cases, the first compartment is divided by longitudinal septations into two distinct tunnels. C are must be taken to identify and release both of these tunnels, as well as any multiple tendinous slips, when performing a surgical release.
Question 44High Yield
**A prospective outcome study is performed at a single institution to analyze the potential differences in treating intertrochanteric hip fractures with a plate/screw device versus an intramedullary device. No specific randomization is performed because an equal number of surgeons have p
Scientific References
- for the use of one of these devices and they are allowed to continue their preferred method. Hip- specific and general health-related outcome measures are used, an excellent follow-up rate of 85% of the patients at 2 years is accomplished, and there appears to be results that favor the intramedullary device but the confidence intervals are wide. This study would be considered to carry what level of evidence?**
Explanation
**
This is a prospective comparative study but is not randomized or blinded and
is therefore a Level II therapeutic study. To qualify as Level I, it would need to be a high- quality randomized trial with narrow confidence intervals regardless of a significant difference or no difference in outcomes. Level III would be
case-control studies or retrospective comparisons. Level IV is case series and Level V is expert opinion.
This is a prospective comparative study but is not randomized or blinded and
is therefore a Level II therapeutic study. To qualify as Level I, it would need to be a high- quality randomized trial with narrow confidence intervals regardless of a significant difference or no difference in outcomes. Level III would be
case-control studies or retrospective comparisons. Level IV is case series and Level V is expert opinion.
Question 45High Yield
A 72-year-old woman with diabetes mellitus has right hand numbness. Provocative test findings are consistent with carpal tunnel syndrome, and electrodiagnostic study (EDS) findings show prolonged median motor and sensory distal latencies with low-amplitude thenar compound muscle action potential. Poor prognosis is most associated with which factor?
Explanation
Although carpal tunnel syndrome remains a clinical diagnosis, EDS findings have become important tools. Moderate disease is defined as abnormal median sensory distal latency and prolonged median motor distal latency. Severe disease is defined as prolonged median motor and sensory distal latencies witheither absent sensory nerve action potential or mixed nerve action potential or low-amplitude or absent thenar compound muscle action potential. Although female gender and diabetes are considered risk factors, there is little association with postsurgical outcome. Severe disease as confirmed by EDS is the factor most _strongly associated with poor recovery after surgery._
Question 46High Yield
The histology of the lesion is shown in Figure 101d. What is the most likely complication after treatment of this lesion?
Explanation
_
_
_**DISCUSSION FOR QUESTIONS 101 THROUGH 103:**_
The MRI scans show a well-circumscribed inhomogenous mass at the anterior ankle joint consistent with a diagnosis of pigmented villonodular synovitis (PVNS), not an anatomic variant. An inflammatory mass,such as the pannus of rheumatoid arthritis, would reveal moderate signal intensity with relatively uniform signal throughout. The mass is well encapsulated, respecting tissue boundaries and not showing invasive characteristics as malignancies would. The arthroscopic image is also consistent with the reddish-brown frond-like tissue of PVNS. PVNS of the ankle can be treated arthroscopically. If this mode of treatment is chosen, a tissue sample should be sent to pathology for microscopic analysis; débridement should be performed on the remaining tissue. Removal of the instrumentation without débridement will not provide treatment and will result in disease progression. Tourniquet placement does not provide therapeutic benefit.
Brachytherapy has not been described for the treatment of PVNS of the ankle. The histologic image shows multiple multinucleated giant cells, hemosiderin, and very few mitotic figures – consistent with a diagnosis of PVNS. A common complication of PVNS treatment is local recurrence. Arthrofibrosis and chondrolysis are not seen with proper surgical care of these patients. Because this is not an infectious lesion, disseminated infection after treatment is highly unlikely. PVNS rarely metastasizes.
RESPONSES FOR QUESTIONS 104 THROUGH 106
1. # Toe is fused too straight (plantar flexed)
2. # Toe is fused in too much valgus
3. # Toe is fused in too much dorsiflexion
4. # There is a nonunion of the fusion
5. # Excessive shortening of the first metatarsal during preparation for fusion What is the most likely diagnosis for each patient?
_
_**DISCUSSION FOR QUESTIONS 101 THROUGH 103:**_
The MRI scans show a well-circumscribed inhomogenous mass at the anterior ankle joint consistent with a diagnosis of pigmented villonodular synovitis (PVNS), not an anatomic variant. An inflammatory mass,such as the pannus of rheumatoid arthritis, would reveal moderate signal intensity with relatively uniform signal throughout. The mass is well encapsulated, respecting tissue boundaries and not showing invasive characteristics as malignancies would. The arthroscopic image is also consistent with the reddish-brown frond-like tissue of PVNS. PVNS of the ankle can be treated arthroscopically. If this mode of treatment is chosen, a tissue sample should be sent to pathology for microscopic analysis; débridement should be performed on the remaining tissue. Removal of the instrumentation without débridement will not provide treatment and will result in disease progression. Tourniquet placement does not provide therapeutic benefit.
Brachytherapy has not been described for the treatment of PVNS of the ankle. The histologic image shows multiple multinucleated giant cells, hemosiderin, and very few mitotic figures – consistent with a diagnosis of PVNS. A common complication of PVNS treatment is local recurrence. Arthrofibrosis and chondrolysis are not seen with proper surgical care of these patients. Because this is not an infectious lesion, disseminated infection after treatment is highly unlikely. PVNS rarely metastasizes.
RESPONSES FOR QUESTIONS 104 THROUGH 106
1. # Toe is fused too straight (plantar flexed)
2. # Toe is fused in too much valgus
3. # Toe is fused in too much dorsiflexion
4. # There is a nonunion of the fusion
5. # Excessive shortening of the first metatarsal during preparation for fusion What is the most likely diagnosis for each patient?
Question 47High Yield
Figures 1 through 5 are the radiographs and MRI scans of an 80-year-old woman who had a total hip arthroplasty (THA) 10 years ago and recently experienced an episode of dislocation that was reduced. She currently has no pain, but has a limp and moderate apprehension. Her erythrocyte sedimentation rate is 32 and C-reactive protein is 34. Her cobalt level is 32.8 ug/L (normal <1ug/L) and chromium level 14 ug/L (normal < 5ug/L). The hip aspiration is negative. What is the most appropriate treatment? 35
Explanation
36
The patient has a metal-on-metal articulation with pseudotumor, causing instability and destruction of the abductors. Although inflammatory markers are elevated, this may occur with adverse local soft-tissue reaction, and aspiration may be necessary to rule out infection. Conversion to a polyethylene articulation is necessary to prevent ongoing damage. The MRI scan reveals compromise of abductors by the pseudotumor, but sparing of the gluteus maximus.This facilitates abductor reconstruction to address the limp and improve stability.
The patient has a metal-on-metal articulation with pseudotumor, causing instability and destruction of the abductors. Although inflammatory markers are elevated, this may occur with adverse local soft-tissue reaction, and aspiration may be necessary to rule out infection. Conversion to a polyethylene articulation is necessary to prevent ongoing damage. The MRI scan reveals compromise of abductors by the pseudotumor, but sparing of the gluteus maximus.This facilitates abductor reconstruction to address the limp and improve stability.
Question 48High Yield
Iontophoresis has been effectively used in all of the following EXC EPT:
Explanation
Iontophoresis is effective in soft tissue conditions such as rotator cuff bursitis and lateral epicondylitis.
Question 49High Yield
Figure 18a shows the initial lateral radiograph of a 6-year-old girl who sustained a fracture in a motor vehicle accident and was treated in a cast 1 year ago. She now has the valgus deformity seen in Figure 18b. Treatment should consist of
Explanation
Proximal tibial metaphyseal fractures may result in late genu valgum as a result of asymmetric growth of the proximal tibia. These patients are best treated with observation because the deformity is likely to remodel. Osteotomy is not indicated and potentially will lead to recurrence. Stapling of the medial tibial physis is appropriate in patients who have a severe and progressive deformity.
REFERENCES: Cozen L: Knock-knee deformity in children: Congenital and acquired. Clin Orthop 1990;258:191-203.
Jackson DW, Cozen L: Genu valgum as a complication of proximal tibial metaphyseal fractures in children. J Bone Joint Surg Am 1971;53:1571-1578.
Brammar TJ, Rooker GD: Remodeling of valgus deformity secondary to proximal metaphyseal fracture of the tibia. Injury 1998;29:558-560.
Ogden JA, Ogden DA, Pugh L, et al: Tibia valga after proximal metaphyseal fractures in childhood: A normal biologic response. J Pediatr Orthop 1995;15:489-494.
Salter RB, Best TN: Pathogenesis of progressive valgus deformity following fractures of the proximal metaphyseal region of the tibia in young children. Instr Course Lect 1992;41:409-411.
REFERENCES: Cozen L: Knock-knee deformity in children: Congenital and acquired. Clin Orthop 1990;258:191-203.
Jackson DW, Cozen L: Genu valgum as a complication of proximal tibial metaphyseal fractures in children. J Bone Joint Surg Am 1971;53:1571-1578.
Brammar TJ, Rooker GD: Remodeling of valgus deformity secondary to proximal metaphyseal fracture of the tibia. Injury 1998;29:558-560.
Ogden JA, Ogden DA, Pugh L, et al: Tibia valga after proximal metaphyseal fractures in childhood: A normal biologic response. J Pediatr Orthop 1995;15:489-494.
Salter RB, Best TN: Pathogenesis of progressive valgus deformity following fractures of the proximal metaphyseal region of the tibia in young children. Instr Course Lect 1992;41:409-411.
Question 50High Yield
-are the radiographs of a 58-year-old right-hand dominant woman who fell from a standing height directly onto her left shoulder and now reports left shoulder pain and is unable to elevate her arm. She has a normal sensory examination. The patient refuses any type of surgical intervention.What factor will have the greatest impact on her outcome at 1 year?

Explanation
No detailed explanation provided for this question.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon