Comprehensive Orthopedic Review | Dr Hutaif General Ort -...
14 Apr 2026
86 min read
94 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Comprehensive Orthopedic Review | Dr Hutaif G...
00:00
Start Quiz
Question 1High Yield
A 45-year-old woman with grade II adult-acquired flatfoot deformity has pain on the lateral side of her foot just distal to the tip of the fibula. Which component of a comprehensive flatfoot reconstruction most likely will address the deformity responsible for this pain?
Explanation
Patients develop lateral ankle pain with progression of adult-acquired flatfoot deformity. This is associated with increased hindfoot valgus deformity. Calcaneal fibular impingement has been considered the primary cause of this pain. Studies demonstrate that arthrosis of the posterior facet of the subtalar joint strongly correlates with lateral pain in adult-acquired flatfoot deformity. Both conditions are related to hindfoot valgus deformity. Although lateral column lengthening is a powerful tool for correction of flatfoot deformity, its effect on hindfoot deformity is less defined. Lateral column lengthening provides better correction of the longitudinal arch of the midfoot and realignment of the medial column than other osteotomies. A medializing calcaneal osteotomy has a significant linear effect on hindfoot valgus alignment. Spring ligament reconstruction and medial cuneiform opening-wedge osteotomies have less effect on hindfoot alignment than the medial calcaneal slide.
RECOMMENDED READINGS
Ellis SJ, Deyer T, Williams BR, Yu JC, Lehto S, Maderazo A, Pavlov H, Deland JT. Assessment of lateral hindfoot pain in acquired flatfoot deformity using weightbearing multiplanar imaging. Foot Ankle Int. 2010 May;31(5):361-71. doi: 10.3113/FAI.2010.0361. PubMed PMID:
[20460061/. ](http://www.ncbi.nlm.nih.gov/pubmed/20460061)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20460061)
[Chan JY, Williams BR, Nair P, Young E, Sofka C, Deland JT, Ellis SJ. The contribution of medializing calcaneal osteotomy on hindfoot alignment in the reconstruction of the stage II adult acquired flatfoot deformity. Foot Ankle Int.2013 Feb;34(2):159-66.doi: 10.1177/ 1071100712460225. Epub 2013 Jan 10. PubMed PMID: 23413053. ](http://www.ncbi.nlm.nih.gov/pubmed/23413053)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23413053)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23413053)
RECOMMENDED READINGS
Ellis SJ, Deyer T, Williams BR, Yu JC, Lehto S, Maderazo A, Pavlov H, Deland JT. Assessment of lateral hindfoot pain in acquired flatfoot deformity using weightbearing multiplanar imaging. Foot Ankle Int. 2010 May;31(5):361-71. doi: 10.3113/FAI.2010.0361. PubMed PMID:
[20460061/. ](http://www.ncbi.nlm.nih.gov/pubmed/20460061)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20460061)
[Chan JY, Williams BR, Nair P, Young E, Sofka C, Deland JT, Ellis SJ. The contribution of medializing calcaneal osteotomy on hindfoot alignment in the reconstruction of the stage II adult acquired flatfoot deformity. Foot Ankle Int.2013 Feb;34(2):159-66.doi: 10.1177/ 1071100712460225. Epub 2013 Jan 10. PubMed PMID: 23413053. ](http://www.ncbi.nlm.nih.gov/pubmed/23413053)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23413053)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23413053)
Question 2High Yield
Human calcium absorption occurs in the
Explanation
Dietary calcium is absorbed in the small intestine. This absorption is stimulated by 1,25 dihydroxyvitamin D3. Correct Answer: Small intestine
Question 3High Yield
What is the primary concern regarding resolution of this fracture?
Explanation
- Blood supply to this area
Question 4High Yield
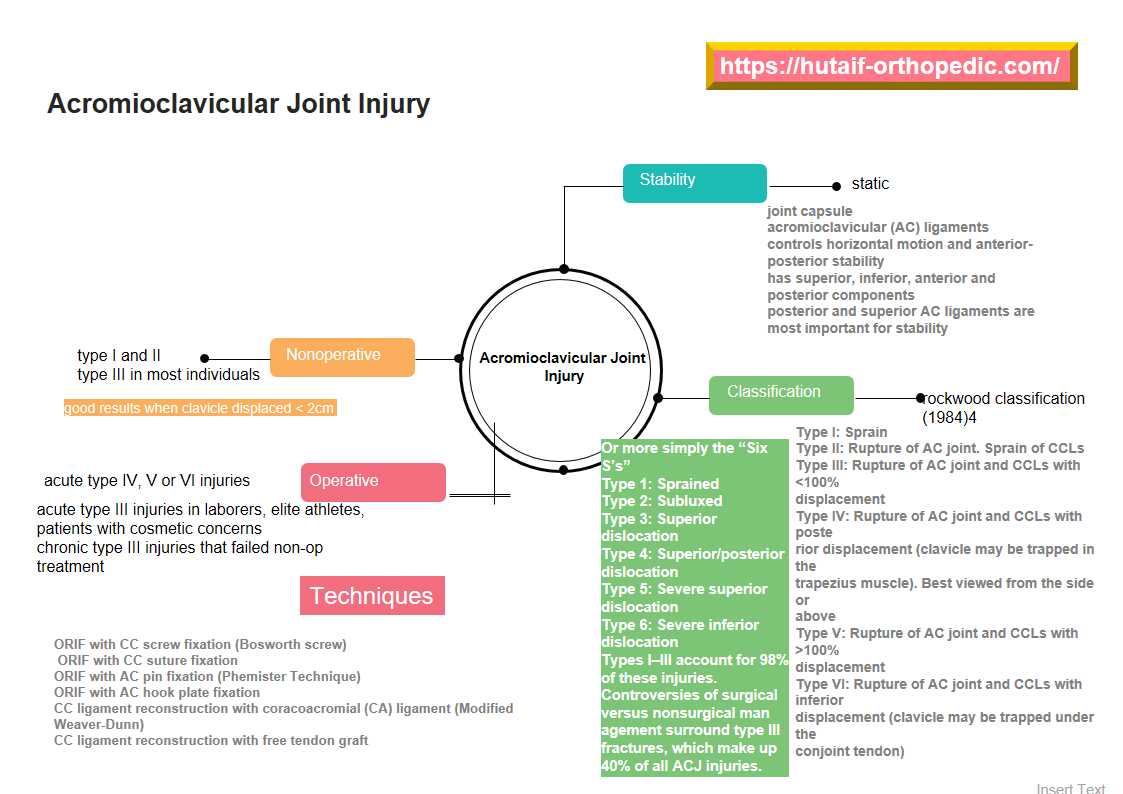
Which of the following techniques after surgical stabilization of patella fractures has the highest risk of hardware migration?




Explanation
Fixation of patella fractures with a tension-band construct consisting of K-wires that are only bent proximally has the highest risk of undergoing hardware migration (Figure A).
There are many techniques described in operative fixation of patella fractures. Historically, tension band wiring has been the most commonly utilized fixation strategy. The classic technique consists of 2 K-wires and a figure of eight cerclage wiring with bending of the wires proximally. This has been associated with a risk of hardware migration and subsequently high incidence of hardware removal. Though migration of hardware may certainly be associated with other fixation strategies, it is the highest for tension band wiring with K-wires.
Eggink et al. performed a study to evaluate the clinical and radiological results of internal fixation of patella fractures, comparing tension band wiring with the proximal wire bent and both the proximal and distal wires bent. Of 60 patients, they found migration of the K-wires in 3 patients. All of these migrations occurred in the group with the proximally bent wires. They recommend bending of K-wires both proximally and distally to avoid this potential complication.
Smith et al. performed a study to identify and review early complications in the operative treatment of patella fractures. They used modified tension band wire fixation in forty-nine fractures, whereas two fractures were treated with tension band wires threaded through cannulated screws. They found that 22% of patients treated with tension band wiring had fracture displacement within the early postoperative period and 9 patients required hardware removal. They conclude that the incidence of early complications in patients treated with tension band wiring is higher than previously reported.
Figure A is an AP radiograph of the knee demonstrating fixation with a tension band wiring technique utilizing K-wires that are only bent proximally. Figure B is an AP radiograph of the knee demonstrating fixation with an anteriorly based plate. Figure C is a lateral radiograph of the knee demonstrating fixation with multiple small plates. Figure D is a lateral radiograph of the knee demonstrating fixation with cannulated screws and a cerclage wire. Figure E is a radiograph demonstrating fixation with a tension band wiring technique utilizing K-wires that are bent both proximally and distally.
Incorrect Answers:
Answers 2, 3, 4, & 5: These fixation strategies have not been associated with hardware migration.
There are many techniques described in operative fixation of patella fractures. Historically, tension band wiring has been the most commonly utilized fixation strategy. The classic technique consists of 2 K-wires and a figure of eight cerclage wiring with bending of the wires proximally. This has been associated with a risk of hardware migration and subsequently high incidence of hardware removal. Though migration of hardware may certainly be associated with other fixation strategies, it is the highest for tension band wiring with K-wires.
Eggink et al. performed a study to evaluate the clinical and radiological results of internal fixation of patella fractures, comparing tension band wiring with the proximal wire bent and both the proximal and distal wires bent. Of 60 patients, they found migration of the K-wires in 3 patients. All of these migrations occurred in the group with the proximally bent wires. They recommend bending of K-wires both proximally and distally to avoid this potential complication.
Smith et al. performed a study to identify and review early complications in the operative treatment of patella fractures. They used modified tension band wire fixation in forty-nine fractures, whereas two fractures were treated with tension band wires threaded through cannulated screws. They found that 22% of patients treated with tension band wiring had fracture displacement within the early postoperative period and 9 patients required hardware removal. They conclude that the incidence of early complications in patients treated with tension band wiring is higher than previously reported.
Figure A is an AP radiograph of the knee demonstrating fixation with a tension band wiring technique utilizing K-wires that are only bent proximally. Figure B is an AP radiograph of the knee demonstrating fixation with an anteriorly based plate. Figure C is a lateral radiograph of the knee demonstrating fixation with multiple small plates. Figure D is a lateral radiograph of the knee demonstrating fixation with cannulated screws and a cerclage wire. Figure E is a radiograph demonstrating fixation with a tension band wiring technique utilizing K-wires that are bent both proximally and distally.
Incorrect Answers:
Answers 2, 3, 4, & 5: These fixation strategies have not been associated with hardware migration.
Question 5High Yield
A 62-year-old woman has advanced osteoarthritis of the knee that has been refractory to nonsurgical treatment. She wishes to discuss total knee arthroplasty. She reports a lifelong history of intolerance to most jewelry and is concerned about having an allergic reaction to the metallic knee implant.Hypersensitivity to metal implants is usually classified as what type of Gell-Coombs reaction?
Explanation
Most “metal allergy” is classified as type IV, or delayed-type hypersensitivity response, which is a cellmediated response. Types I, II, and III are not generally associated with metal hypersensitivity responses.Type I reactions are typically anaphylaxis. Type II reactions are antibody mediated, such as seen in Grave’s disease or hemolytic anemia. Type III reactions are immune complex diseases such as serum sickness or systemic lupus erythematosus.
Question 6High Yield
This image represents the end stage of an uncompensated rotator cuff tear.
Explanation
Axillary lateral and anteroposterior (AP) images of the right shoulder (Figures 59c and 59d) reveal osteoarthrosis of the glenohumeral joint, which typically is not associated with significant rotator cuff pathology. An examination often shows limitations in range of motion, crepitance, and pain with motion. An AP radiographic image of the right shoulder (Figure 59b) reveals proximal humeral migration, which normally correlates with rotator cuff tear size. Tears extending into the infraspinatus tendon are associated with more humeral migration than is seen with isolated supraspinatus tears. Presenting complaints are usually of pain and weakness. Examination findings include subacromial crepitance and weakness during rotator cuff testing. Rarely, this may be associated with pseudoparalysis in large uncompensated rotator cuff tears. The CT image of the right shoulder (Figure 59a) shows superior migration of the humerus with respect to the glenoid surface and end-stage
degenerative changes at the glenohumeral joint. These changes are classified as rotator cuff arthropathy. Pain and weakness are common, as is the presence of pseudoparalysis and limited range of motion.
RECOMMENDED READINGS
1. [Kelly JD Jr, Norris TR. Decision making in glenohumeral arthroplasty. J Arthroplasty. 2003 Jan;18(1):75-82. Review. PubMed PMID: 12555187. ](http://www.ncbi.nlm.nih.gov/pubmed/12555187)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12555187)
2. Keener JD, Wei AS, Kim HM, Steger-May K, Yamaguchi K. Proximal humeral migration in shoulders with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am. 2009 Jun;91(6):1405-13. doi: 10.2106/JBJS.H.00854. PubMed PMID:
[19487518/. ](http://www.ncbi.nlm.nih.gov/pubmed/19487518)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19487518)
3. [Neer CS 2nd, Craig EV, Fukuda H. Cuff-tear arthropathy. J Bone Joint Surg Am. 1983 Dec;65(9):1232-44. PubMed PMID: 6654936. ](http://www.ncbi.nlm.nih.gov/pubmed/6654936)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/6654936)
degenerative changes at the glenohumeral joint. These changes are classified as rotator cuff arthropathy. Pain and weakness are common, as is the presence of pseudoparalysis and limited range of motion.
RECOMMENDED READINGS
1. [Kelly JD Jr, Norris TR. Decision making in glenohumeral arthroplasty. J Arthroplasty. 2003 Jan;18(1):75-82. Review. PubMed PMID: 12555187. ](http://www.ncbi.nlm.nih.gov/pubmed/12555187)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12555187)
2. Keener JD, Wei AS, Kim HM, Steger-May K, Yamaguchi K. Proximal humeral migration in shoulders with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am. 2009 Jun;91(6):1405-13. doi: 10.2106/JBJS.H.00854. PubMed PMID:
[19487518/. ](http://www.ncbi.nlm.nih.gov/pubmed/19487518)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19487518)
3. [Neer CS 2nd, Craig EV, Fukuda H. Cuff-tear arthropathy. J Bone Joint Surg Am. 1983 Dec;65(9):1232-44. PubMed PMID: 6654936. ](http://www.ncbi.nlm.nih.gov/pubmed/6654936)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/6654936)
Question 7High Yield
Figures 1 and 2 are the CT and MR spine images of an 82-year-old man who has a history of ankylosing spondylitis falls onto his back. He has no neurologic deficits upon examination in the emergency department. What is the most appropriate next step?

Explanation
■
Spinal fractures in patients with ankylosing spondylitis are unstable and generally necessitate surgical intervention. In a patient with a spinal fracture in the setting of ankylosing spondylitis, posterior instrumented fusion is an appropriate surgical procedure. Treatment with a thoracolumbar orthosis is not an option for patients with extension distraction injuries in the setting of an ankylosed spine because of risk for displacement. Similarly, simply checking upright radiographs is generally not advocated. Laminectomy alone is inappropriate for this patient because there is no cord compression and neurologic symptoms are absent. Stabilization is the treatment goal.
Spinal fractures in patients with ankylosing spondylitis are unstable and generally necessitate surgical intervention. In a patient with a spinal fracture in the setting of ankylosing spondylitis, posterior instrumented fusion is an appropriate surgical procedure. Treatment with a thoracolumbar orthosis is not an option for patients with extension distraction injuries in the setting of an ankylosed spine because of risk for displacement. Similarly, simply checking upright radiographs is generally not advocated. Laminectomy alone is inappropriate for this patient because there is no cord compression and neurologic symptoms are absent. Stabilization is the treatment goal.
Question 8High Yield
A 12-year-old boy reports knee discomfort after prolonged strenuous activities. He denies knee swelling or catching and has no pain with activities of daily living. A radiograph is shown in Figure 4. Prognosis for the pathology shown is most
influenced by
influenced by
Explanation
While many factors play a role in the outcome of osteochondritis dissecans, ample evidence has shown that the prognosis is most influenced by the growth status of the plates. If the growth plates are open, the chance of a successful outcome is significantly greater than if they are closed.
REFERENCES: Federico DJ, Lynch JK, Jokl P: Osteochondritis dissecans of the knee: A historical review of etiology and treatment. Arthroscopy 1990;6:190-197.
Linden B: Osteochondritis dissecans of the femoral condyles: A long-term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
REFERENCES: Federico DJ, Lynch JK, Jokl P: Osteochondritis dissecans of the knee: A historical review of etiology and treatment. Arthroscopy 1990;6:190-197.
Linden B: Osteochondritis dissecans of the femoral condyles: A long-term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
Question 9High Yield
The fracture seen in Figure 1 is most likely associated with injury to what ligamentous structure?
Explanation
The radiograph shows an extra-articular distal clavicle fracture lateral to the clavicular attachment point of the coracoclavicular ligaments (conoid and trapezoid). However, unlike a scenario featuring a typical Neer type I fracture, the interval between coracoid and clavicle is clearly widened, and there is marked fracture displacement. This signifies disruption to the coracoclavicular ligaments. The inferior glenohumeral ligament is important to glenohumeral joint stability, but has no effect on the relationship between clavicle and scapula. The AC ligaments are thickenings of the AC joint capsule. They have been shown to be responsible for 90% of anteroposterior stability of the AC joint. The coracoclavicular ligaments are responsible for 77% of stability for superior translation (as in this case). The coracoacromial ligament connects two parts of the scapula (coracoid and acromion) and is part of the arch that supports the rotator cuff.
Question 10High Yield
Augmentation of a Broström repair with the mobilized lateral portion of the extensor retinaculum (Gould
modification) is expected to produce
modification) is expected to produce
Explanation
Multiple biomechanical studies have investigated the contribution of the Gould modification with the Broström anatomic repair for chronic ankle instability. No studies to date have demonstrated a statistically significant difference in initial ankle stability with inclusion of the Gould modification or augmentation of the repair with a mobilized lateral portion of the extensor retinaculum. No clear association exists between the Broström-Gould repair technique and risk for nerve injury, postsurgical range of motion, or incidence of osteoarthritis on long-term follow-up.
Question 11High Yield
A 75-year-old man presents with complaints of shoulder pain, bruising, and weakness following a fall onto his outstretched hand. He underwent an uncomplicated anatomic total shoulder arthroplasty 5 years prior with good range of motion and strength. His current radiographs are shown in Figures 1 and
Explanation
The patient's radiographs demonstrate humeral head elevation and anterior translation, suggesting a massive traumatic rotator cuff tear. In this setting, a rotator cuff repair is unlikely to be successful, and a revision to reverse total shoulder arthroplasty is indicated. A latissimus dorsi transfer can address only a portion of the patient's rotator cuff deficiency. Physical therapy may result in some degree of improvement, but this cannot address the joint instability and malalignment. If the shoulder remains in its current position, progressive glenoid loosening would be expected due to the “rocking horse” phenomenon resulting in eccentric glenoid edge loading. Shields and Wiater compared conversion of an anatomic total shoulder to a reverse total shoulder for rotator cuff deficiency with primary reverse total shoulder arthroplasty and found similar American Shoulder and Elbow Surgeons Standardized Shoulder Assessment and visual analog scale pain scores at 2-year follow-up.
Question 12High Yield
A 40-year-old woman with no history of back problems has a symptomatic L4-5 disk herniation with an L5 radiculopathy that has failed to respond to 12 weeks of nonsurgical management. In the preoperative discussion, the surgeon advises the patient that the chance of recurrence of the herniation after successful diskectomy is what percent?
Explanation
DISCUSSION: The incidence of recurrent disk herniation after a successful diskectomy is approximately 5% to 10%. Indications for surgical diskectomy for a recurrence are the same as for a primary diskectomy.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 685-698.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 127-139.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 685-698.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 127-139.
Question 13High Yield
Figures 4a through 4j
A B 4
D C .
E
F G H
5
I J
A B 4
D C .
E
F G H
5
I J









Explanation
- Normal foot
Question 14High Yield
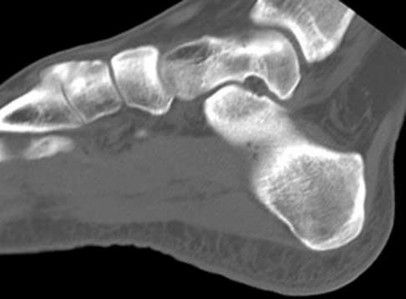
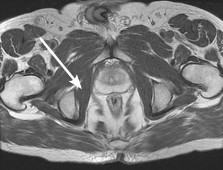
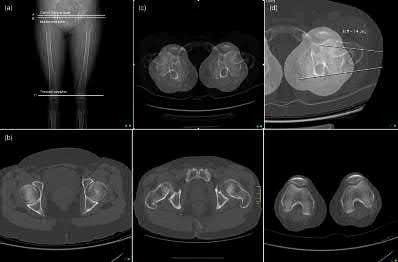
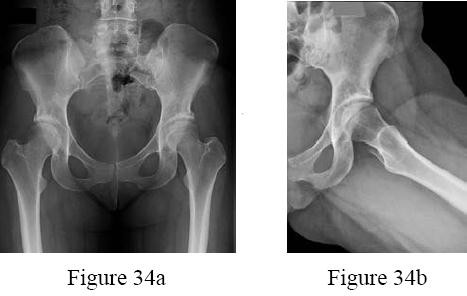
Figure 12a shows a cross section of the pelvis at the level of the greater trochanters. What structure is marked with the arrow? ](http://www.orthobullets.com/anatomy/10075/obturator-internus)
Explanation
No detailed explanation provided for this question.
Question 15High Yield
Figure 90 is the radiograph of this patient 5 months later when he returned for his preseason football physical. He is asymptomatic. What is the best next step?










Explanation
This patient has a closed midshaft clavicle fracture with significant displacement that has healed and remodeled nicely with nonsurgical treatment. Functional disability or nonunion after nonsurgical treatment of clavicle fractures in adolescents is rare. Schulz and associates showed no differences in pain, strength, range of motion, or subjective outcome scores between injured and uninjured limbs treated nonsurgically to address displaced, shortened midshaft clavicle fractures in adolescents. Bae and associates demonstrated that clavicle fracture malunions in adolescents do not cause loss of motion or strength.
Figure 91a
Figure 91b
Figure 92
Figure 93
Figure 94a
Figure 94b
Figure 94c
Figure 95a
Figure 95b
Figure 96
RESPONSES FOR QUESTIONS 91 THROUGH 96
1. Chromosome 17 mutation
2. MYH3 mutation
3. Embryonic vascular interruption
4. Infantile vascular interruption
5. Chromosome 11 mutation
6. Sporadic inheritance
Select the appropriate etiology listed above for each pictured syndrome.
Figure 91a
Figure 91b
Figure 92
Figure 93
Figure 94a
Figure 94b
Figure 94c
Figure 95a
Figure 95b
Figure 96
RESPONSES FOR QUESTIONS 91 THROUGH 96
1. Chromosome 17 mutation
2. MYH3 mutation
3. Embryonic vascular interruption
4. Infantile vascular interruption
5. Chromosome 11 mutation
6. Sporadic inheritance
Select the appropriate etiology listed above for each pictured syndrome.
Question 16High Yield
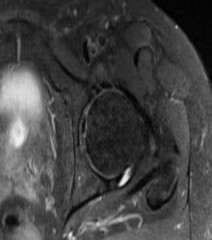
A 15-year-old girl has had 4 months of right hip and groin pain. Upon examination, she has 25° of internal rotation with the hip flexed, which causes pain on the right side. Her left side shows 20° of internal rotation but no significant pain. Plain radiographs show that the patient has no dysplasia and an alpha angle of 68° on the right side and 70° on the left side. She has not undergone any formal treatment to date. What is the best course of initial management?
Explanation
■
Recent studies have shown success in conservative management for adolescent patients with femoroacetabular impingement syndrome. In a patient who has had symptoms for 4 months with no trial of physical therapy, this is the best step. In addition, even though the radiographic and range-of-motion parameters are more profound in the nonpainful hip, multiple authors have documented the presence of FAI morphology in asymptomatic patients, and the role of prophylactic surgery has not been elucidated. In addition, there are recent concerns about retained gadolinium, and its promise in imaging is starting to decline in elective type procedures.
Recent studies have shown success in conservative management for adolescent patients with femoroacetabular impingement syndrome. In a patient who has had symptoms for 4 months with no trial of physical therapy, this is the best step. In addition, even though the radiographic and range-of-motion parameters are more profound in the nonpainful hip, multiple authors have documented the presence of FAI morphology in asymptomatic patients, and the role of prophylactic surgery has not been elucidated. In addition, there are recent concerns about retained gadolinium, and its promise in imaging is starting to decline in elective type procedures.
Question 17High Yield
Which of the following mutations occurs in patients with diastrophic dysplasia:
Explanation
One should remember the important mutations that occur in musculoskeletal conditions: FGFR3 mutation: Achondroplasia
Type IX collagen mutation: Multiple epiphyseal dysplasia (MED)
WISP3 mutation: Spondyloepiphyseal dysplasia with progressive osteoarthropathy
Type II collagen mutation: Stickler syndrome
Sulfate transporter gene mutation: Diastrophic dysplasia
Fibrillin gene mutation: Marfanâs syndrome
Type V collagen mutation: Ehlers-Danlos syndrome
Type I collagen mutation: Osteogenesis imperfecta
C orrect Answer: Sulfate transporter gene mutation
Type IX collagen mutation: Multiple epiphyseal dysplasia (MED)
WISP3 mutation: Spondyloepiphyseal dysplasia with progressive osteoarthropathy
Type II collagen mutation: Stickler syndrome
Sulfate transporter gene mutation: Diastrophic dysplasia
Fibrillin gene mutation: Marfanâs syndrome
Type V collagen mutation: Ehlers-Danlos syndrome
Type I collagen mutation: Osteogenesis imperfecta
C orrect Answer: Sulfate transporter gene mutation
Question 18High Yield
An 82-year-old woman presents for treatment of a painful second toe deformity. The toe is subluxated at the metatarsophalangeal (MP) joint, and a fixed claw toe deformity is present. Despite severe hallux valgus, and the hallux under riding the second toe, the hallux and bunion are not symptomatic. The procedure that will ideally correct this deformity is:
Explanation
This elderly patient has a symptomatic second toe deformity only, and surgery to the hallux should be avoided if possible. This is a common clinical problem, and although patients do not readily accept amputation of the toe, it is the preferred procedure because it does not involve reconstruction of the hallux. C orrection of the second toe without amputation will not work unless the hallux deformity is addressed.
Question 19High Yield
A 70-year-old woman has a 3-year history of gradually increasing diffuse and global right knee pain. Her
main issues are difficulty with stairs, stiffness with prolonged sitting, and swelling. She has taken NSAIDs and has received intra-articular steroid injections, all with decreasing efficacy. Her right knee examination reveals a range of motion of 15° to 80° with a fixed deformity to varus and valgus stress. Her symptoms are no longer manageable nonsurgically. Radiographs reveal a 30-degree mechanical axis deformity. When using the measured resection technique during total knee arthroplasty (TKA), the best way to avoid femoral malrotation is to reference the
main issues are difficulty with stairs, stiffness with prolonged sitting, and swelling. She has taken NSAIDs and has received intra-articular steroid injections, all with decreasing efficacy. Her right knee examination reveals a range of motion of 15° to 80° with a fixed deformity to varus and valgus stress. Her symptoms are no longer manageable nonsurgically. Radiographs reveal a 30-degree mechanical axis deformity. When using the measured resection technique during total knee arthroplasty (TKA), the best way to avoid femoral malrotation is to reference the
Explanation
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point, can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking
or instability, which is a common complication associated with primary TKA.
or instability, which is a common complication associated with primary TKA.
Question 20High Yield
A 45-year-old man who underwent an open capsulolabral stabilization procedure
15 years ago now reports pain and has no external rotation on the affected side. Nonsurgical management has failed to provide relief. Examination reveals external rotation to -5 degrees compared with 50 degrees of external rotation on the contralateral side. Radiographs show a small inferior osteophyte and minimal posterior glenoid wear. Which of the following procedures will offer the best chance of restoring motion, decreasing pain, and preserving the native joint?
15 years ago now reports pain and has no external rotation on the affected side. Nonsurgical management has failed to provide relief. Examination reveals external rotation to -5 degrees compared with 50 degrees of external rotation on the contralateral side. Radiographs show a small inferior osteophyte and minimal posterior glenoid wear. Which of the following procedures will offer the best chance of restoring motion, decreasing pain, and preserving the native joint?
Explanation
Loss of external rotation following stabilization procedures can result in progressive degenerative joint disease. A tight anterior capsule results in posterior humeral translation and progressive posterior glenoid wear. Patients with early degenerative joint disease and pain can be treated with anterior release to restore more normal glenohumeral biomechanics. This procedure not only improves function but also decreases pain in most patients. Closed manipulation at 15 years after surgery is unlikely to be successful and carries the risk of complications. Acromioplasty, posterior release, and removal of osteophytes do not address the pathology. Arthroscopic releases are favored for intra-articular procedures that have addressed the pathology of instability. Open releases are recommended for nonanatomic extra-articular repairs that include subscapularis tightening procedures.
REFERENCES: MacDonald PB, Hawkins RJ, Fowler PJ, et al: Release of the subscapularis for internal rotation contracture and pain after anterior repair for recurrent anterior dislocation of the shoulder. J Bone Joint Surg Am 1992;74:734-737.
Warner JJ, Allen AA, Marks PH, et al: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
REFERENCES: MacDonald PB, Hawkins RJ, Fowler PJ, et al: Release of the subscapularis for internal rotation contracture and pain after anterior repair for recurrent anterior dislocation of the shoulder. J Bone Joint Surg Am 1992;74:734-737.
Warner JJ, Allen AA, Marks PH, et al: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
Question 21High Yield
1229) A young male patient underwent intramedullary nail fixation for a diaphyseal femur fracture. A post-operative CT scanogram is performed to assess rotational alignment between the surgical and non-surgical femur. Which of the following measurement(s) are considered acceptable differences in regards to femoral rotational
malreduction after intramedullary nail fixation as compared to the uninjured femur?
malreduction after intramedullary nail fixation as compared to the uninjured femur?
Explanation
The maximum acceptable difference in rotational malreduction between the surgical and contralateral legs for femoral version is 15°. Therefore, answers 1 and 2 are correct.
Normal femoral neck anteversion is approximately 11-13°, with a normal range between 5-20°. The variation within the same patients can also be up to 15° difference between limbs. Current literature has shown that this 15° difference is well tolerated by patients, including when this has occured as a result of rotational malreduction following intramedullary nail fixation for a diaphyseal femur fracture.
Ayalon et al. aimed to compare the difference in femoral version (DFV) after intramedullary nailing performed by a trauma-trained and non-trauma trained surgeon. The mean post-operative DFV was 8.7° in these patients, compared to 10.7° in those treated by surgeons of other subspecialties. Post-operative version or percentage of DFV >15° did not significantly differ between these two groups.
Omar et al. studied the utility of pre-operative 'virtual reduction' of bilateral femoral fractures that were initially stabilized with external fixation. After external fixation, the mean rotational difference between both legs was 15.0°
± 10.2°. Following virtual reduction, the mean rotational difference between both legs was 2.1° ± 1.2°, after intramedullary nailing, compared to 6.1° ±
2.8° without the pre-operative tool.
Illustration A shows the typical CT scanogram cuts used to measure femoral version. Note, femoral version is obtained by measuring an angle between a line along the femoral neck and another line along the posterior condylar axis.
Incorrect Answers:
Answers 1-5: More than 15° difference in version between femurs is considered the upper limit for acceptable reduction.
Normal femoral neck anteversion is approximately 11-13°, with a normal range between 5-20°. The variation within the same patients can also be up to 15° difference between limbs. Current literature has shown that this 15° difference is well tolerated by patients, including when this has occured as a result of rotational malreduction following intramedullary nail fixation for a diaphyseal femur fracture.
Ayalon et al. aimed to compare the difference in femoral version (DFV) after intramedullary nailing performed by a trauma-trained and non-trauma trained surgeon. The mean post-operative DFV was 8.7° in these patients, compared to 10.7° in those treated by surgeons of other subspecialties. Post-operative version or percentage of DFV >15° did not significantly differ between these two groups.
Omar et al. studied the utility of pre-operative 'virtual reduction' of bilateral femoral fractures that were initially stabilized with external fixation. After external fixation, the mean rotational difference between both legs was 15.0°
± 10.2°. Following virtual reduction, the mean rotational difference between both legs was 2.1° ± 1.2°, after intramedullary nailing, compared to 6.1° ±
2.8° without the pre-operative tool.
Illustration A shows the typical CT scanogram cuts used to measure femoral version. Note, femoral version is obtained by measuring an angle between a line along the femoral neck and another line along the posterior condylar axis.
Incorrect Answers:
Answers 1-5: More than 15° difference in version between femurs is considered the upper limit for acceptable reduction.
Question 22High Yield
The injury pattern shown in the CT image in Figure 26 is most commonly associated with which mechanism?

Explanation
Posterior shoulder dislocations are most commonly the result of seizures and electrical shock. Collision athletic events, postpolio syndrome, and traction injury are rarely associated with posterior shoulder dislocations. The bony defect caused by impaction of the anterior superior humeral head on the posterior glenoid has been referred to as a “reverse Hill-Sachs lesion.”
RECOMMENDED READINGS
1. McLaughlin HL: Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;64:1584-1590.
2. [Kowalsky MS, Levine WN. Traumatic posterior glenohumeral dislocation: classification, pathoanatomy, diagnosis, and treatment. Orthop Clin North Am. 2008 Oct;39(4):519-33, viii. doi: 10.1016/j.ocl.2008.05.008. Review. PubMed PMID: 18803981.](http://www.ncbi.nlm.nih.gov/pubmed/18803981)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18803981)
RECOMMENDED READINGS
1. McLaughlin HL: Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;64:1584-1590.
2. [Kowalsky MS, Levine WN. Traumatic posterior glenohumeral dislocation: classification, pathoanatomy, diagnosis, and treatment. Orthop Clin North Am. 2008 Oct;39(4):519-33, viii. doi: 10.1016/j.ocl.2008.05.008. Review. PubMed PMID: 18803981.](http://www.ncbi.nlm.nih.gov/pubmed/18803981)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18803981)
Question 23High Yield
A 17-year-old pitcher reports pain over the medial aspect of the elbow that occurs during the acceleration phase of throwing, and it prevents him from throwing at the velocity needed to be competitive. What structure is most likely injured in this patient?


Explanation
DISCUSSION: The anterior bundle of the ulnar collateral ligament of the elbow is the primary constraint to valgus force of the elbow. In pitchers and in overhead athletes, injury to this portion of the ligament results in valgus instability. Reconstruction of the anterior band of the ulnar collateral ligament is necessary in many elite athletic throwers to allow them to return to this competitive activity.
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Cain EL, Dugas JR, Wolf RS, et al: Elbow injuries in throwing athletes: A current concepts review. Am J Sports Med 2003;31:621-635.
Rettig AC, Sherrill C, Snead DS, et al: Nonoperative treatment of ulnar collateral ligament injuries in
throwing athletes. Am J Sports Med 2001 ;29:15-17.
/
Figure 55a Question 55
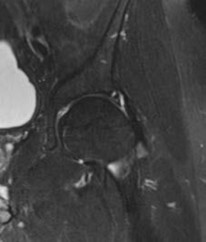
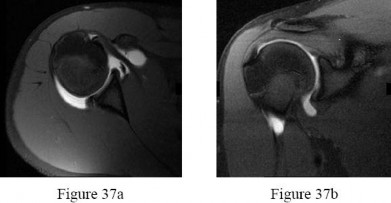
A 22-year-old male basketball player has had knee pain for the past 3 months. He denies any history of trauma. He has symptoms of catching but no locking. He has rested for 2 weeks but symptoms returned when he resumed sporting activities. Tr and T2-weighted MRI scans are shown in Figures 55a and 55b. What is the most likely diagnosis?
1. #### Locked lateral meniscus tear
2. #### Anterior cruciate ligament tear
3. #### Ganglion cyst of the anterior cruciate ligament
4. #### Synovial osteochondromatosis
5. #### Pigmented villonodular synovitis PREFERRED RESPONSE: 3
DISCUSSION: The MRI scans show a cystic structure within the anterior cruciate ligament. It is fluid filled as seen on the T2 sequence. Ganglion cysts of the cruciate ligaments are rare. The most common presentation is pain with occasional loss of motion. Instability is not a chief complaint and often there is no evidence of laxity on examination. If nonsurgical management fails, arthroscopic debridement of the cyst is the accepted method of treatment.
REFERENCES: Liu SH, Osti L, Mirzayan R: Ganglion cysts of the anterior cruciate ligament: A case report and review of the literature. Arthroscopy 1994; 10:110-112.
Parish EN, Dixon P, Cross MJ: Ganglion cysts of the anterior cruciate ligament: A series of 15 cases. Arthroscopy 2005;21:445-447.
Figure 56
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Cain EL, Dugas JR, Wolf RS, et al: Elbow injuries in throwing athletes: A current concepts review. Am J Sports Med 2003;31:621-635.
Rettig AC, Sherrill C, Snead DS, et al: Nonoperative treatment of ulnar collateral ligament injuries in
throwing athletes. Am J Sports Med 2001 ;29:15-17.
/
Figure 55a Question 55
A 22-year-old male basketball player has had knee pain for the past 3 months. He denies any history of trauma. He has symptoms of catching but no locking. He has rested for 2 weeks but symptoms returned when he resumed sporting activities. Tr and T2-weighted MRI scans are shown in Figures 55a and 55b. What is the most likely diagnosis?
1. #### Locked lateral meniscus tear
2. #### Anterior cruciate ligament tear
3. #### Ganglion cyst of the anterior cruciate ligament
4. #### Synovial osteochondromatosis
5. #### Pigmented villonodular synovitis PREFERRED RESPONSE: 3
DISCUSSION: The MRI scans show a cystic structure within the anterior cruciate ligament. It is fluid filled as seen on the T2 sequence. Ganglion cysts of the cruciate ligaments are rare. The most common presentation is pain with occasional loss of motion. Instability is not a chief complaint and often there is no evidence of laxity on examination. If nonsurgical management fails, arthroscopic debridement of the cyst is the accepted method of treatment.
REFERENCES: Liu SH, Osti L, Mirzayan R: Ganglion cysts of the anterior cruciate ligament: A case report and review of the literature. Arthroscopy 1994; 10:110-112.
Parish EN, Dixon P, Cross MJ: Ganglion cysts of the anterior cruciate ligament: A series of 15 cases. Arthroscopy 2005;21:445-447.
Figure 56
Question 24High Yield
Which of the following is considered a critical element in surgically correcting posttraumatic elbow flexion contractures in adolescents:
Explanation
Bae and Waters have shown that adolescents with significant posttraumatic elbow flexion contractures can gain an average of 54Â
° of motion with surgical release. They believe postoperative physical therapy and continuous passive motion are considered critical to success of surgical release. Lengthening of the biceps or triceps is not recommended. Measures to prevent postoperative heterotopic ossification did not influence the outcome.
° of motion with surgical release. They believe postoperative physical therapy and continuous passive motion are considered critical to success of surgical release. Lengthening of the biceps or triceps is not recommended. Measures to prevent postoperative heterotopic ossification did not influence the outcome.
Question 25High Yield
If surgery is chosen, what is the optimum procedure?
Explanation
- Costotransversectomy with posterior instrumentation
Question 26High Yield
Figures 11a and 11b show the AP and lateral radiographs of a 32-year-old patient on hemodialysis who has increasing elbow pain and a visibly growing mass over the extensor surface. Figure 11c shows the photomicrograph of the biopsy specimen. What is the most likely diagnosis?
Explanation
The radiographic findings are classic for tumoral calcinosis; they are not consistent with myositis ossificans, fungal granuloma, or hemochromatosis. The condition typically appears as large aggregations of dense calcified lobules confined to the surrounding soft tissues. Hyperphosphatemia is a fundamental factor in many patients with this condition. Tumoral calcinosis also occurs in the setting of chronic renal failure when mineral homeostasis is not controlled. The histologic appearance is essentially a foreign body granuloma reaction. Multilocular cysts with purplish amorphous material are surrounded by thick connective tissue capsules. The fibrous walls contain numerous foreign body giant cells. Surgical excision is indicated if the tumor causes discomfort or interferes with function.
REFERENCES: Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Boskey AL, Vigorita VJ, Sencer O, Stuchin SA, Lane JM: Chemical, microscopic, and ultrastructural characterization of the mineral deposits in tumoral calcinosis. Clin Orthop 1983;178:258-269.
REFERENCES: Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Boskey AL, Vigorita VJ, Sencer O, Stuchin SA, Lane JM: Chemical, microscopic, and ultrastructural characterization of the mineral deposits in tumoral calcinosis. Clin Orthop 1983;178:258-269.
Question 27High Yield
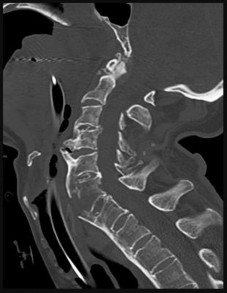
Figure 46 is the CT scan of a 50-year-old man who is brought to the emergency department after a fall. He has a complete C5 neurological injury. What is the root cause of his fracture?
Explanation
This patient has a fracture dislocation through the body of C6. Because the spine is ankylosed, it is rigid and prone to injury even in the setting of low-energy incidents. This patient has ankylosing spondylitis because the anterior longitudinal ligament is ossified. Ankylosing spondylosis is a seronegative spondyloarthropathy with sacroiliac joint involvement most commonly. It has a male predilection of 3:1. In the spine, it is characterized by diffuse syndesmotic ankylosis resulting in a “bamboo spine.”
This patient also has degenerative changes found at C3-4, C4-5, but the ankylosing of the spine is the main reason for the higher fracture risk. DISH (Forestier disease) is a noninflammatory
spondyloarthropathy characterized by flowing ossifications and bone proliferations at sites of tendinous and ligamentous insertion.
RECOMMENDED READINGS
7. [El Tecle NE, Abode-Iyamah KO, Hitchon PW, Dahdaleh NS. Management of spinal fractures in patients with ankylosing spondylitis. Clin Neurol Neurosurg. 2015 Dec;139:177-82. doi: 10.1016/j.clineuro.2015.10.014. Epub 2015 Oct 23. Review. PubMed PMID: 26513429. ](http://www.ncbi.nlm.nih.gov/pubmed/26513429)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/26513429)[ ](http://www.ncbi.nlm.nih.gov/pubmed/26513429)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26513429)
8. [Lukasiewicz AM, Bohl DD, Varthi AG, Basques BA, Webb ML, Samuel AM, Grauer JN. Spinal Fracture in Patients With Ankylosing Spondylitis: Cohort Definition, Distribution of Injuries, and Hospital Outcomes. Spine (Phila Pa 1976). 2016 Feb;41(3):191-6. doi: 10.1097/BRS.0000000000001190. PubMed PMID: 26579959. ](http://www.ncbi.nlm.nih.gov/pubmed/26579959)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26579959)
This patient also has degenerative changes found at C3-4, C4-5, but the ankylosing of the spine is the main reason for the higher fracture risk. DISH (Forestier disease) is a noninflammatory
spondyloarthropathy characterized by flowing ossifications and bone proliferations at sites of tendinous and ligamentous insertion.
RECOMMENDED READINGS
7. [El Tecle NE, Abode-Iyamah KO, Hitchon PW, Dahdaleh NS. Management of spinal fractures in patients with ankylosing spondylitis. Clin Neurol Neurosurg. 2015 Dec;139:177-82. doi: 10.1016/j.clineuro.2015.10.014. Epub 2015 Oct 23. Review. PubMed PMID: 26513429. ](http://www.ncbi.nlm.nih.gov/pubmed/26513429)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/26513429)[ ](http://www.ncbi.nlm.nih.gov/pubmed/26513429)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26513429)
8. [Lukasiewicz AM, Bohl DD, Varthi AG, Basques BA, Webb ML, Samuel AM, Grauer JN. Spinal Fracture in Patients With Ankylosing Spondylitis: Cohort Definition, Distribution of Injuries, and Hospital Outcomes. Spine (Phila Pa 1976). 2016 Feb;41(3):191-6. doi: 10.1097/BRS.0000000000001190. PubMed PMID: 26579959. ](http://www.ncbi.nlm.nih.gov/pubmed/26579959)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26579959)
Question 28High Yield
Recommendations for sports activity should include
Explanation
- avoidance of contact or collision sports.
Question 29High Yield
A 28-year-old woman is having low back pain that wakes her up at night. A CT scan reveals a lytic lesion in the fifth lumbar vertebrae shown in Figure

Explanation
■
The patient has a giant cell tumor. Surgery remains the standard of care; however, the monoclonal antibody against RANKL has been shown to be effective in preventing tumor progression, and it is an effective nonsurgical option. Radiation is not recommended, as this is a benign tumor and the patient is young. En bloc resection has been shown to be effective, but the patient is hoping to avoid surgery. Bisphosphonates are not an effective treatment for giant cell tumors.
The patient has a giant cell tumor. Surgery remains the standard of care; however, the monoclonal antibody against RANKL has been shown to be effective in preventing tumor progression, and it is an effective nonsurgical option. Radiation is not recommended, as this is a benign tumor and the patient is young. En bloc resection has been shown to be effective, but the patient is hoping to avoid surgery. Bisphosphonates are not an effective treatment for giant cell tumors.
Question 30High Yield
Figure 53 shows the radiograph of a 48-year-old man who has a left side periprosthetic femoral fracture around the femoral stem of a previous revision hip arthroplasty. What is the most appropriate treatment?

Explanation
DISCUSSION: In type B3 fractures, the proximal femur is so deficient that it cannot be treated with open reduction and internal fixation or support a new femoral component. In younger patients, the femur can be reconstructed with allograft prosthesis composite to restore bone stock. Removal of the distal stem with trephines would compromise fixation with cement. Elderly and low-demand patients can be treated more simply with a cemented segmental replacement prosthesis, such as that used for tumor reconstruction.
REFERENCES: Parvizi J, Tarity TD, Slenker N, et al: Proximal femoral replacement in patients with non- neoplastic conditions. J Bone Joint Surg Am 2007;89:1036-1043.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Lee SR, Bostrom MP: Periprosthetic fractures of the femur after total hip arthroplasty. Instr Course Lect 2004;53:111-118.
Figure 54
DISCUSSION: In type B3 fractures, the proximal femur is so deficient that it cannot be treated with open reduction and internal fixation or support a new femoral component. In younger patients, the femur can be reconstructed with allograft prosthesis composite to restore bone stock. Removal of the distal stem with trephines would compromise fixation with cement. Elderly and low-demand patients can be treated more simply with a cemented segmental replacement prosthesis, such as that used for tumor reconstruction.
REFERENCES: Parvizi J, Tarity TD, Slenker N, et al: Proximal femoral replacement in patients with non- neoplastic conditions. J Bone Joint Surg Am 2007;89:1036-1043.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Lee SR, Bostrom MP: Periprosthetic fractures of the femur after total hip arthroplasty. Instr Course Lect 2004;53:111-118.
Figure 54
Question 31High Yield
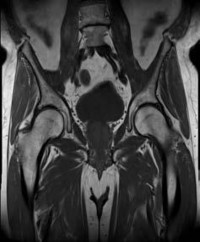
Figure 1 is the radiograph of a 15-year-old boy with scoliosis. He has back pain and spinal asymmetry. Examination reveals a spinal curvature without cutaneous manifestations. Neurological examination reveals a normal motor and sensory examination, normal deep tendon reflexes, present superficial abdominal reflexes, and negative Babinski sign. His MRI scans are shown in Figures 2 and

Explanation
■
The MRI scans reveal a spinal cord with a noted central spinal canal syrinx. The patient has a normal neurological examination. There is no evidence of Chiari malformation or tethered spinal cord. Thus, for this patient, a neurosurgical evaluation is not required nor is a cerebral spinal fluid shunt. As the deformity has progressed past 50° in a skeletally immature teenager, brace treatment is no longer appropriate, and surgical correction of the scoliosis is the most appropriate treatment.
The MRI scans reveal a spinal cord with a noted central spinal canal syrinx. The patient has a normal neurological examination. There is no evidence of Chiari malformation or tethered spinal cord. Thus, for this patient, a neurosurgical evaluation is not required nor is a cerebral spinal fluid shunt. As the deformity has progressed past 50° in a skeletally immature teenager, brace treatment is no longer appropriate, and surgical correction of the scoliosis is the most appropriate treatment.
Question 32High Yield
Which of the following statements regarding ganglions is false:
Explanation
Transillumination is a hallmark of ganglions. Because of the location from which ganglia arise and the dissection performed during resection, a decrease in range of motion can be seen postoperatively. Needle aspiration is diagnostic and can be therapeutic, however, recurrence rates as high as 95% have been reported. Volar ganglia can often be intimately associated with the radial artery. Ganglia may often be multilobulated.
Question 33High Yield
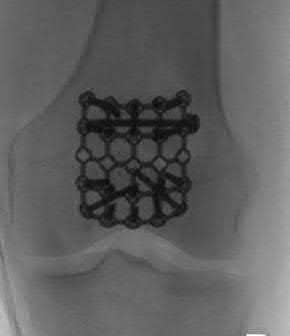
Figures 1 and 2 are the clinical photographs of a 2-month-old infant with a foot deformity. The parents have been doing stretching exercises at home with some improvement in foot position. What is the most appropriate course of treatment?

Explanation
■
The figures reveal a calcaneovalgus foot deformity with an associated posterior medial bow of the tibia. The foot deformity occurs quite commonly and is most likely related to intrauterine positioning. Calcaneovalgus foot deformity frequently will spontaneously correct. However, occasionally the deformity may be more severe and require either stretching exercises or even serial casting. With this particular deformity, it is most important to differentiate it from a congenital vertical talus. The congenital vertical talus has hindfoot equinus associated with it, while a calcaneovalgus foot deformity has a hindfoot that dorsiflexes normally. Because the deformity has improved, it does not require treatment with serial casting or a brace.
Although the foot deformity may do well, posterior medial bowing of the tibia is associated with leg length discrepancy (LLD), which may vary in severity. Typically, surgical intervention for leg length equalization is required. For this reason, the child should be seen on a routine basis to assess correction of the deformity, as well as document the LLD. Initial radiographs should be obtained at this visit to make the diagnosis and document the deformity. Over time, the deformity may improve so that it is not as clinically apparent; however, the LLD will persist.
■
The figures reveal a calcaneovalgus foot deformity with an associated posterior medial bow of the tibia. The foot deformity occurs quite commonly and is most likely related to intrauterine positioning. Calcaneovalgus foot deformity frequently will spontaneously correct. However, occasionally the deformity may be more severe and require either stretching exercises or even serial casting. With this particular deformity, it is most important to differentiate it from a congenital vertical talus. The congenital vertical talus has hindfoot equinus associated with it, while a calcaneovalgus foot deformity has a hindfoot that dorsiflexes normally. Because the deformity has improved, it does not require treatment with serial casting or a brace.
Although the foot deformity may do well, posterior medial bowing of the tibia is associated with leg length discrepancy (LLD), which may vary in severity. Typically, surgical intervention for leg length equalization is required. For this reason, the child should be seen on a routine basis to assess correction of the deformity, as well as document the LLD. Initial radiographs should be obtained at this visit to make the diagnosis and document the deformity. Over time, the deformity may improve so that it is not as clinically apparent; however, the LLD will persist.
Question 34High Yield
A 55-year-old man was injured when a large piece of sheet metal lacerated his medial elbow while working at a factory. He underwent primary repair of the lacerated structures shown in Figures 1 and 2 on the day of injury. In addition to this surgical treatment, what nerve transfer procedure should be considered during this primary operative intervention to improve his functional recovery?
---
---
---
---



Explanation
In adults, the repair of high ulnar nerve injuries typically yields incomplete motor recovery and disappointing functional results despite early surgical intervention and careful surgical technique. Early transfer of the terminal branch of the AIN to the deep ulnar motor fascicle can rapidly reinnervate distal targets and potentially preserve motor end plate function in the intrinsic musculature of the hand because of the proximity of the nerve transfer to the target muscle. Sensory deficits due to an ulnar nerve injury
can be restored through a transfer of median sensory fascicles to the distal ulna sensory fascicles. This procedure typically would not be considered at the time of the original surgery, because sensory recovery is more likely than motor recovery in the setting of a high ulnar nerve injury. For radial nerve injuries, wrist extension can be restored through an FDS branch of the median nerve transfer to the ECRB branch of the radial nerve. The FCU fascicle of the ulnar nerve can be transferred to the biceps branch of the _musculocutaneous nerve to restore elbow flexion and supination._
can be restored through a transfer of median sensory fascicles to the distal ulna sensory fascicles. This procedure typically would not be considered at the time of the original surgery, because sensory recovery is more likely than motor recovery in the setting of a high ulnar nerve injury. For radial nerve injuries, wrist extension can be restored through an FDS branch of the median nerve transfer to the ECRB branch of the radial nerve. The FCU fascicle of the ulnar nerve can be transferred to the biceps branch of the _musculocutaneous nerve to restore elbow flexion and supination._
Question 35High Yield
A prospective, randomized study of the use of intravenous bisphosphonate therapy following a hip fracture (control = no bisphosphonate; study group = annual zoledronic acid) would most likely yield the following outcome:
Explanation
A large prospective, randomized study showed a reduction in vertebral and nonvertebral fractures when patients were treated with intravenous (IV) zoledronic acid within 90 days of a hip fracture, followed up with annual treatment.
Important points to remember about this study:
Study: Zoledronic acid (5 mg, IV) within 90 days of hip fracture and then annually (1,000 patients in each group) New fractures: 8.6% vs 13.9% (absolute risk reduction, 5.3%; relative risk reduction, 35%)
New fractures
  o   Vertebral: 1.7% vs 3.8% (P = .02)
  o   Nonvertebral: 7.6% vs 10.7% (P = .03)
  o   Hip: 2.0% vs 3.5% (relative risk 30%, not significant)   o   Divergence of fracture-free survival at 12 months BMD
  o   12 month: 2.6% vs -1.0%   o   24 month: 4.7% vs -0.7%   o   36 month: 5.5% vs -0.9% Death
  o   Hazard ratio: -0.72 (0.56 to 0.93 C I, P = .01) Adverse advents
  o   Pyrexia: 8.7% vs 3.1%   o   Myalgia: 4.9% vs 2.7%
  o   Bone pain: 3.2% vs 1.0%
C orrect Answer: Decrease in new fractures; survival advantage
Important points to remember about this study:
Study: Zoledronic acid (5 mg, IV) within 90 days of hip fracture and then annually (1,000 patients in each group) New fractures: 8.6% vs 13.9% (absolute risk reduction, 5.3%; relative risk reduction, 35%)
New fractures
  o   Vertebral: 1.7% vs 3.8% (P = .02)
  o   Nonvertebral: 7.6% vs 10.7% (P = .03)
  o   Hip: 2.0% vs 3.5% (relative risk 30%, not significant)   o   Divergence of fracture-free survival at 12 months BMD
  o   12 month: 2.6% vs -1.0%   o   24 month: 4.7% vs -0.7%   o   36 month: 5.5% vs -0.9% Death
  o   Hazard ratio: -0.72 (0.56 to 0.93 C I, P = .01) Adverse advents
  o   Pyrexia: 8.7% vs 3.1%   o   Myalgia: 4.9% vs 2.7%
  o   Bone pain: 3.2% vs 1.0%
C orrect Answer: Decrease in new fractures; survival advantage
Question 36High Yield
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less
than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include
than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include
Explanation
With a severe injury to the upper extremity, the best opportunity for achieving a good functional result for a floating elbow is immediate debridement of the open fracture, followed by internal fixation of the fractures. The ability to do this depends on the patient’s physiologic status. In this patient, the procedure is acceptable because she has normal vital signs and no chest or abdominal injuries, and normal physiologic parameters (base excess and lactate) show adequate peripheral perfusion. The surgical approaches will be determined by the associated injury patterns and open wounds. In this patient, the humerus was debrided and stabilized through a posterior approach as was the medial condyle fracture. The ulna was fixed through an extension of the posterior incision and the radius through a separate dorsal approach.
REFERENCES: Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
REFERENCES: Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Question 37High Yield
A 8-year-old girl sustained a Gustilo-Anderson grade III open tibia fracture 1 week ago and underwent two debridements with definitive fracture fixation. She now has a soft-tissue defect that measures 7 cm
× 7 cm on the distal third leg that is a 3 centimeters proximal to the ankle. There is exposed bone on the medial aspect of her leg. A Negative pressure wound therapy (NPWT) device was applied to her leg. All of the following are benefits of the NPWT EXCEPT:
× 7 cm on the distal third leg that is a 3 centimeters proximal to the ankle. There is exposed bone on the medial aspect of her leg. A Negative pressure wound therapy (NPWT) device was applied to her leg. All of the following are benefits of the NPWT EXCEPT:
Explanation
Due to the limited soft tissue coverage of the medial aspect of the distal third of the tibia, full-thickness wound in this region often requires free-flap coverage. However, NWPT is typically applied first, as this has been shown to contribute to all of the above benefits with the exception of decreased wound angiogenesis.
NPWT has a number or purported beneits, including stimulation of angiogenesis, reduction of local edema, increased blood flow at the wound bed, and increased granulation tissue in the wound. These affects accelerate wound healing and may reduce the need for complex wound coverage. NPT has become increasingly popular as a temporizing measure for complex wound management and can enable outpatient treatment.
Caniano et al. reviewed 51 pediatric patients who underwent NPWT using the Vacuum Assisted Closure (VAC) device to aid in soft tissue closure. Nine of these patients had extremity wounds, for which a VAC was applied as a bridge to either a skin graft or a free flap. The VAC was applied intraoperatively, and patients then followed up as an outpatient with dressing changes performed three times weekly. The authors found that NPWT was safe, cost-effective to complex wound care, and permitted outpatien management.
Mooney et al. reviewed 27 patients with complex extremity wounds managed with NPWT. They found that all wounds, whether acute or with prior failed soft tissue procedure, eventually healed with NPWT and without additional complex coverage procedures. The authors noted that patients developed robust granulation tissue, even over exposed bone, tendon, joint, and hardware, which could then be covered with a split thickness graft or allowed to heal by
secondary intention. They concluded that NPWT may decrease need for complex microvascular tissue transfer.
Incorrect Answers:
Answer 1: NPWT decreases the likelihood of complex secondary soft tissue reconstruction.
Answer 2: NPWT often permits outpatient management of complex wounds. Answer 3: NPWT reduces edema to the wound bed.
Answer 4. NPWT stimulates of granulation tissue and prepares the wound for STSG or free flap.
NPWT has a number or purported beneits, including stimulation of angiogenesis, reduction of local edema, increased blood flow at the wound bed, and increased granulation tissue in the wound. These affects accelerate wound healing and may reduce the need for complex wound coverage. NPT has become increasingly popular as a temporizing measure for complex wound management and can enable outpatient treatment.
Caniano et al. reviewed 51 pediatric patients who underwent NPWT using the Vacuum Assisted Closure (VAC) device to aid in soft tissue closure. Nine of these patients had extremity wounds, for which a VAC was applied as a bridge to either a skin graft or a free flap. The VAC was applied intraoperatively, and patients then followed up as an outpatient with dressing changes performed three times weekly. The authors found that NPWT was safe, cost-effective to complex wound care, and permitted outpatien management.
Mooney et al. reviewed 27 patients with complex extremity wounds managed with NPWT. They found that all wounds, whether acute or with prior failed soft tissue procedure, eventually healed with NPWT and without additional complex coverage procedures. The authors noted that patients developed robust granulation tissue, even over exposed bone, tendon, joint, and hardware, which could then be covered with a split thickness graft or allowed to heal by
secondary intention. They concluded that NPWT may decrease need for complex microvascular tissue transfer.
Incorrect Answers:
Answer 1: NPWT decreases the likelihood of complex secondary soft tissue reconstruction.
Answer 2: NPWT often permits outpatient management of complex wounds. Answer 3: NPWT reduces edema to the wound bed.
Answer 4. NPWT stimulates of granulation tissue and prepares the wound for STSG or free flap.
Question 38High Yield
A patient sustained the injuries shown in the radiographs and clinical photograph seen in Figures 10a through 10c. The neurovascular examination is normal. The first step in emergent management of the extremity injuries should consist of
Explanation
The figures show an open tibial fracture, a femoral shaft fracture, and femoral head dislocation. The most urgent treatment is reduction of the femoral head, as timing to reduction has been correlated with preventing osteonecrosis. After reduction of the femoral head, the next priority is wound management, followed by stabilization of the femoral and tibial fractures with either splinting, traction, or external fixation.
REFERENCES: Sahin V, Karakas ES, Aksu S, et al: Traumatic dislocation and fracture-dislocation of the hip: A long-term follow-up study. J Trauma 2003;54:520-529.
Moed BR, WillsonCarr SE, Watson JT: Results of operative treatment of fractures of the posterior wall of the acetabulum. J Bone Joint Surg Am 2002;84:752-758.
REFERENCES: Sahin V, Karakas ES, Aksu S, et al: Traumatic dislocation and fracture-dislocation of the hip: A long-term follow-up study. J Trauma 2003;54:520-529.
Moed BR, WillsonCarr SE, Watson JT: Results of operative treatment of fractures of the posterior wall of the acetabulum. J Bone Joint Surg Am 2002;84:752-758.
Question 39High Yield
The most common extraskeletal manifestation of this disease is
Explanation
- café au lait macules._
Question 40High Yield
Quadriceps tendonitis
_Please select the most likely diagnosis listed above for each clinical situation._
-A 26-year-old weightlifter had increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication, corticosteroid injections, and rest failed to alleviate his symptoms. He underwent an arthroscopic distal clavicle resection with excision of the distal 8 mm of clavicle (Mumford procedure). Three months after surgery, he reported popping by his clavicle and mild pain. His clavicle demonstrated mild posterior instability on examination without any obvious deformity on his radiographs. What structures were compromised during his excision?
_Please select the most likely diagnosis listed above for each clinical situation._
-A 26-year-old weightlifter had increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication, corticosteroid injections, and rest failed to alleviate his symptoms. He underwent an arthroscopic distal clavicle resection with excision of the distal 8 mm of clavicle (Mumford procedure). Three months after surgery, he reported popping by his clavicle and mild pain. His clavicle demonstrated mild posterior instability on examination without any obvious deformity on his radiographs. What structures were compromised during his excision?











Explanation
--The patient is provided with a medial unloader brace that provides substantial pain relief and he is able to work while wearing the brace. After 4 months he returns to work and says that while the brace enable him to work, it is uncomfortable. Consequently, his symptoms return when he is not wearing the brace and he is requesting a surgical intervention for his problem. What is the most appropriate surgical treatment?
1) Valgus-producing high tibial osteotomy (VPHTO)
2) Repeat knee arthroscopy
3) Total knee arthroplasty (TKA)
4) Medial meniscus transplant
--The patient is offered a VPHTO. What aspect of his history will determine the most appropriate VPHTO technique?
1) Prior arthroscopy
2) Current smoking history
3) BMI of 22
4) Age of 40
FOR QUESTIONS 13 THROUGH 16_
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. An ultrasound can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario.
Because the patient has a correctable deformity (gaps 3 mm with valgus stress) and his symptoms are localized to the involved compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgicalplanning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient.A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation,examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result,current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 is an indication for HTO but does not influence technique.
-When reconstructing the anterior cruciate ligament (ACL), what is the most common source of potential autograft failure?
1) Graft choice
2) Tunnel position
3) Tibial fixation
4) Femoral fixation
_CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 20_
A 25-year-old healthy woman injured her left knee while playing professional soccer. She has never injured this knee before. Examination 2 days after the injury occurred reveals the following: a moderate effusion, a positive Lachman test result, and mild lateral tenderness. Range of motion is between 20 degrees and 70 degrees. Radiographs reveal no fracture. An MRI scan reveals a complete rupture of the anterior cruciate ligament (ACL), an effusion, and bone bruises of the lateral femoral condyle and lateral tibial plateau. No meniscal tear is seen. The patient would like to continue playing at the professional level.
--What is the next treatment step?
1) Immobilization of the knee for 6 weeks, followed by rehabilitation and delayed ACL reconstruction
2) Immediate ACL reconstruction
3) Immediate rehabilitation for 6 months followed by ACL reconstruction if the patient is unstable in a brace
4) Immediate rehabilitation with delayed ACL reconstruction (when the athlete obtains full knee range of motion)
-What is this patient’s risk for developing osteoarthritis (OA) of the knee?
1) There is no risk for development of knee OA after reconstruction of the ligament.
2) There is no risk for development of knee OA after a double-bundle ACL reconstruction.
3) There is no evidence that ACL reconstruction reduces the incidence of knee OA.
4) There is 100% likelihood that she will develop knee OA after single-bundle ACL reconstruction.
-The patient asks if something about her anatomy has resulted in this injury. ACL anatomy differs between men and women in what manner?
1) There is no significant difference in ACL anatomy between men and women.
2) A woman’s ACL has a smaller cross-sectional area.
3) The cross-sectional area of a woman’s ACL is larger.
4) The intercondylar notch is wider in women than in men.
FOR QUESTIONS 18 THROUGH 20_
This patient has the clinical findings of an ACL rupture that is confirmed on MRI scan. She is a professional athlete and would like to return to her sport. Immediate ACL reconstruction in the setting of a knee with limited motion carries an increased risk for postsurgical stiffness. Delayed surgery after the patient regains range of motion is the preferred response. It has been shown that a woman’s ACL is smaller in the cross-sectional area.
-Figure 21 is the radiograph of a 31-year-old man who had left shoulder pain after a fall during a snow boarding jump. Residual displacement of 5 mm after closed reduction is most likely to result in which of the following?
1) Nonunion
2) Osteonecrosis
3) Altered rotator cuff mechanics
4) Normal shoulder function
-What strategy has proven most effective in preventing transmission of methicillin-resistant Staphylococcus aureus among teammates?
1) Separate players with infections in a separate locker room or changing area.
2) Treat teammates of the infected player with prophylactic antibiotics.
3) Cover any skin lesions with occlusive dressing during sporting activity.
4) Ban players with infections from any team event.
-Figure 23 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain?
1) Forward elevation in the scapular plane
2) External rotation and abduction
3) Flexion, adduction, and internal rotation
4) Flexion and abduction
_**CLINICAL SITUATION FOR QUESTIONS 24 AND 25**_
During the third quarter of a high school football game, a 16-year-old running back gets tackled and limps off the field. During the initial sideline evaluation, he has tenderness on the right iliac crest. He is a little dizzy, has a headache, and tells you, “I need to get back in the game to help the team score before halftime.”
-How can this scenario be managed most effectively?
1) Initiate rest, ice the iliac crest, and return to play when he is not limping.
2) Initiate rest, ice the iliac crest, and return to play after 20 minutes.
3) Keep the player on the sideline, perform a cognitive evaluation, and repeat the physical assessment.
4) Keep the player out of the game and send him emergently to the hospital for imaging.
-Sideline examination of this patient showed no cervical pain or tenderness; motor and sensory function were normal; and his pupils were equal, round, and reactive. He was alert and oriented to the score of game, time on the clock, and current quarter of play. His iliac crest had mild tenderness but no swelling or crepitus. The player states that he has a slight headache and is no longer dizzy. What is the most appropriate treatment?
1) Return him to the game and observe his play closely.
2) Do not return to the game and do not allow play for the remainder of the season.
3) Do not return to the game and begin a graduated return-to-play protocol for future games.
4) Perform a sideline noncontact exercise testing examination and return him to the game if he is asymptomatic.
FOR QUESTIONS 24 AND 25_
Although this player limps off the field, the fact that he felt dizzy, had a headache, and did not initially recognize that he was playing in the third quarter indicates that he sustained a concussion. The player should be kept out of the game until a cognitive examination and repeat physical assessment is completed.Even if his physical symptoms have resolved, a certain period of time has expired, or he states that he is“ready,” he should not be returned to play prior to this assessment. Sending the patient to an emergency department should be considered only after this assessment and appropriate initial sideline treatment is initiated. The Consensus Statement on Concussion in Sport recommends that no athlete with concussion symptoms be returned to same-day play. This patient still has a slight headache, but even if this resolved he should not return to the game. Adolescents and high school athletes may have neurophysiological deficits that may not be evident on the sideline, or they may have a delayed onset of symptoms. A graduated return to play for future games is recommended.
_CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29_
A 32-year-old woman has a 2-year history of progressively worsening right groin pain that is exacerbated by activity. She reports no traumatic injury and an extensive work-up by her gynecologist has ruled out an intrapelvic source of her pain. The patient is a recreational athlete and exercises regularly in the gym.The pain is preventing her from performing these activities. She reports no catching or locking symptoms.Her examination reveals a physically fit female (BMI of 20) with limited right hip range of motion. She has no tenderness to palpation around the hip. While lying supine and bringing her hip into progressive flexion with internal rotation and adduction, her groin pain is reproduced. She has normal limb lengths and demonstrates weakness secondary to pain with hip flexion on the affected side.
-What is the most likely cause of this patient’s groin pain?
1) Femoroacetabular impingement (FAI)
2) Osteoarthritis of the sacroiliac joint
3) Intra-articular loose body
4) Trochanteric bursitis
-The patient is enrolled in physical therapy for 6 weeks with little improvement of her hip symptoms.What is the next most appropriate diagnostic test to determine the presence of an associated acetabular labral tear in this patient?
1) Diagnostic arthroscopy of the hip
2) MRI scan of the hip
3) MRI arthrogram of the hip
4) Ultrasound of the hip
-The study obtained in confirms the presence of an anterosuperior acetabular labral tear and pincer morphology of the acetabulum. What is the most likely location of a chondral injury associated with these findings?
1) Posteroinferior acetabulum
2) Posterosuperior acetabulum
3) Femoral head above the fovea
4) Femoral head below the fovea
-The patient experienced little improvement with activity modification and physical therapy. An intraarticular corticosteroid injection provides excellent but short-lived pain control. She requests surgical treatment for her hip and she is counseled regarding arthroscopy and consent is obtained. Intraoperatively,a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. What treatment is most appropriate considering these findings?
1) Suture anchor repair of the labral tear and no bony resection
2) Suture anchor repair of the labral tear and bony resection of the pincer lesion
3) Debridement of the labral tear and bony resection of the pincer lesion
4) Debridement of the labral tear with no bony resection of the pincer lesion
FOR QUESTIONS 26 THROUGH 29_
The clinical scenario, examination, and MRI scans are consistent with a pincer-type FAI. The decreased range of motion is secondary to the pain produced by the continued abutment of the femoral head against the anterosuperior acetabulum. Flexing the hip while internally rotating and adducting the leg recreates this contact and is typically painful. No clinical signs suggest sacroiliac joint arthritis, an intra-articular loose body, or trochanteric bursitis, although these are all diagnoses that should be considered in a patient with a painful hip. The most sensitive and specific study to detect an acetabular labral tear is an MRI arthrogram of the hip. This study should be obtained in this patient to evaluate the labrum as well as the status of the articular cartilage. An MRI scan without intra-articular contrast is not as sensitive as an arthrogram. An ultrasound can provide a dynamic assessment of the hip and help in the setting of a snapping hip; however, this study is not reliable to determine the presence of a labral tear. In the setting of pincer FAI, the forced leverage of the anterosuperior femoral head upon the anterior acetabulum results in abnormal forces against the posteroinferior acetabulum. This continued force can lead to a chondral lesion in this location know as a “counter-coup” injury. Chondral lesions of the femoral head are rare in the setting of pincer FAI. The posterosuperior quadrant does not experience increased force and rarely sustains chondral injuries. The patient is a young, active individual with no pre-existing degenerative changes, so repair of the tear with bony resection of the pincer lesion is the most appropriate treatment.A capsulolabral detachment should be repaired because these tears can heal and the labrum functions as a seal, preventing egress of synovial fluid from the joint space. If the pincer lesion is not resected, the patient will continue to experience abnormal contact and the repair will likely fail. There is no evidence that the patient has a cam impingement, and recontouring of the femoral head/neck junction is not appropriate. Simple debridement should be reserved for intrasubstance tears of the labrum, which would not be expected to heal with repair.
_**CLINICAL SITUATION FOR QUESTIONS 30 THROUGH 32**_
Figures 30a and 30b are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he
believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg.
-What examination findings are most consistent with the pathology seen in the radiographs?
1) Pain with resisted hip flexion
2) Pain with a half sit-up, plus tenderness at the pubic ramus
3) Pain with a combination of hip flexion, adduction, and internal rotation
4) Tenderness to palpation at the greater trochanter
-What is the most likely diagnosis for the source of this patient’s pain?
1) Cam-type femoroacetabular impingement
2) Pincer-type femoroacetabular impingement
3) Hip flexor strain
4) Athletic pubalgia
-Images from an MRI scan of this patient’s left hip are shown in Figure 30c through 30e. What is the most likely cause of his acute pain?
1) Significant cartilage loss on the acetabulum
2) Labral tear
3) Femoral neck stress fracture
4) Tendonopathy of the rectus femoris
FOR QUESTIONS 30 THROUGH 32_
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement.Surgical treatment for cam impingement can be effective for symptomatic patients. Even among highlevel athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable to those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment.Byrd and Jones described 5 patients who developed transient neurapraxias that resolved uneventfully.The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a periacetabular osteotomy can develop a more retroverted acetabulum as well.
-A 25-year-old recreational soccer player has recurrent shoulder dislocations. He first dislocated his shoulder playing football in high school, was treated in a sling for 6 weeks, and returned to play for the remainder of the season. He did well until 2 years later when he reinjured the shoulder. He says that his shoulder dislocates with little injury and always “feels loose.” Examination reveals anterior instability and an MR arthrogram reveals an anterior-inferior labral tear and surgical treatment is recommended. He inquires about the benefits of arthroscopic vs open procedure. Which of the following statements reflects an advantage associated with arthroscopic procedures compared to open stabilization?
1) Range of motion might be slightly better after an arthroscopic procedure.
2) Rate of recurrent instability is lower after an arthroscopic procedure.
3) Rates of return to work are higher after an arthroscopic procedure.
4) Rates of return to sports are higher after an arthroscopic procedure.
-Figures 34a and 34b are the radiographs of a 38-year-old woman who had increasing left hip pain with activity. She noted no lower back or buttock pain and no pain along her lateral thigh. The pain usually only bothers her with running and cycling.
Nonsteroidal anti-inflammatory drugs helped initially but are not relieving her pain now. Examination with the patient supine reveals pain with internal and external rotation of her hip
with her hip and knee in an extended position. With her hip flexed to 90 degrees, she has internal rotation only to neutral, but full external rotation. What is the most likely diagnosis?
1) Cam-type femoroacetabular impingement
2) Pincer-type femoroacetabular impingement
3) Intra-articular loose body
4) Snapping psoas tendon
-A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman with a soft endpoint, varus laxity at 30 degrees, and a positive dial test at 30 degrees that dissipates at 90 degrees of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome?
1) Hamstring autograft
2) Revision ACL reconstruction and posterior cruciate ligament (PCL) reconstruction
3) Revision ACL reconstruction and posteromedial corner reconstruction
4) Revision ACL reconstruction and posterolateral corner reconstruction
-A 49-year-old man is seeking a second opinion for continued knee pain and swelling. He went to his primary doctor for swelling “on top of his knee,” and he says his doctor drained some clear fluid. He noted that his condition improved for about 1 week before the swelling returned. He now has increasing pain and redness around his kneecap.
Examination reveals significant swelling of his prepatellar bursa,with erythema over the bursa that extends to the surrounding skin. His temperature in the office is 101.7°F. What is the next step in treatment for this patient?
1) Initiate oral antibiotics for 7 days.
2) Reaspirate the bursa and inject a corticosteroid.
3) Recommend padding the patella for kneeling and ice.
4) Perform an open bursectomy and start intravenous antibiotics.
_CLINICAL SITUATION FOR QUESTIONS 37 AND 38_
An 18-year-old right-hand-dominant college freshman who is a third baseman has pain in his right shoulder after using his outstretched right arm for support while diving to catch a low line drive. He describes pivoting on his right hand and arm while reaching out to make the catch with his left-hand glove. He had pain in his shoulder but was able to finish the game with some pain while throwing. Five days later, he experiences popping pain deep in his shoulder that has improved since the injury but continued to be bothersome deep in the shoulder with higher-velocity throwing. Examination demonstrated decreased internal rotation, posterior pain with cross-body adduction and posteriorly directed force, and full rotator cuff strength. Radiograph findings were normal. After 6 weeks of physical therapy (PT), his range of motion has improved but he continues to experience deep pain with therapy. Examination shows symmetric range of motion and posterior pain with the jerk test and Kim test. His rotator cuff is strong.Figure 37a Figure 37b
-What is the next step in treatment?
1) Continued PT
2) Subacromial injection
3) CT scan
4) MRI arthrogram
-T1-weighted, fat-saturated MRI scans are shown in Figures 37a and 37b. What is the next step intreatment?
1) Open reduction internal fixation (ORIF)
2) Rotator cuff repair
3) Labrum repair
4) Chondroplasty
FOR QUESTIONS 37 AND 38_
Examination findings of posterior glenohumeral tenderness, decreased internal rotation, and reproduction of symptoms with a posterior stress test indicate a posterior shoulder injury or instability. The jerk test,with the patient seated, positions the arm in forward flexion and internal rotation with elbow flexion. One hand of the examiner is placed on the patient’s distal clavicle and scapular spine and the other hand grasps the elbow. The arm is jerked posteriorly while the shoulder girdle is jerked anteriorly, which creates pain as the posteriorly subluxated humeral head relocates into the glenoid fossa. During the Kim test, the patient is seated with the arm in 90 degrees of abduction. While the arm is elevated 45 degrees diagonally (forward flexion and adduction), the examiner applies an axial load to the elbow and a downward and posterior force to the upper arm. A positive result causes a sudden onset of posterior shoulder pain. A positive jerk test combined with a positive Kim test has a 97% sensitivity for posterior instability. After extensive PT, the patient continues to have examination findings consistent with posterior shoulder injury or instability, so an MRI scan or MRI arthrography would be helpful to assess for any pathology.A subacromial injection is not indicated by this examination, which shows a strong rotator cuff and no demonstrated bursal-sided symptoms. A CT scan can be helpful in scenarios involving bony pathology,but an MRI is indicated at this stage in the evaluation of soft tissue. Although continuing PT may help to abate symptoms, the patient was continuing to have symptoms with PT. The MRI arthrogram shows a complex posterior labrum tear at the inferior to mid glenoid with separation of labrum from the glenoid. Because the examination findings are consistent with the MRI findings and nonsurgical treatment has failed to resolve symptoms, the next step is to recommend surgical treatment with labrum debridement and/or repair. No examination or MRI findings indicate a need for injection, rotator cuff repair, ORIF, or chondroplasty unless incidental intrasurgical findings are found.
A high school athlete sustained a noncontact injury to his right knee. He says that during a football game he felt a pop and his leg gave way. He attempted to continue to play but was unable secondary to pain.Five days after the injury, radiographs of his right knee do not reveal any abnormalities. On examination,he has an effusion on the injured side and no joint line tenderness. His range of motion is full extension to 110 degrees of flexion. At 20 degrees of flexion, he has increased anterior translation compared to the contralateral, uninjured left side. At 90 degrees of flexion, the tibia does not translate posteriorly. As his knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a“clunk” within the knee. What is the most likely biomechanical basis for the “clunk”?
1) In extension, the medial tibial plateau is subluxated; as an internal rotation/valgus force is applied in conjunction with flexion, the medial tibial plateau reduces.
2) In extension, the medial tibial plateau is reduced; as an internal rotation/valgus force is applied in conjunction with flexion, the medial tibial plateau subluxates.
3) In extension, the lateral tibial plateau is reduced; as an internal rotation/valgus force is applied in conjunction with flexion, the lateral plateau subluxates.
4) In extension, the lateral tibial plateau is subluxated; as an internal rotation/valgus force is applied in conjunction with flexion, the lateral plateau reduces.
_**CLINICAL SITUATION FOR QUESTIONS 40 THROUGH 42**_
A 9-year-old boy was injured while playing soccer. His examination revealed painful range of motion between 5 degrees and 75 degrees. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality.
-What is the next diagnostic step?
1) Repeat radiographs while the patient is weight bearing
2) Ultrasound of the lower extremity and calf
3) Stress radiographs
4) CT scan
-What is the most likely area of injury?
1) Femoral attachment of the medial collateral ligament
2) Tibial attachment of the medial collateral ligament
3) Hypertrophic zone of the growth plate
4) Proliferative zone of the growth plate
FOR QUESTIONS 40 THROUGH 42_
This patient likely has a physeal injury to the distal femoral physis. Stress radiographs or an MRI scan will most reliably reveal this diagnosis. The growth plate, when injured, is most commonly fractured through the hypertrophic zone of cartilage, its weakest point. This patient is optimally treated in a cylindrical or long-leg cast. Younger patients can be treated with a hip spica with a leg extension.
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
1) Psoriasis
2) Tinea corporis
3) Herpes simplex virus
4) Community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA)
_CLINICAL SITUATION FOR QUESTIONS 44 AND 45_
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
-Range of motion of the knee is between 0 degrees and 70 degrees. What is the most appropriate treatment option?
1) Nonweight-bearing activity with crutches
2) Microfracture of the chondral defect
3) Immediate anterior cruciate ligament (ACL) reconstruction
4) Delayed ACL reconstruction
-The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports,and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation,patients who follow an early accelerated rehabilitation protocol experience
1) increased laxity.
2) no differences in long-term results.
3) increased risk for graft failure.
4) lower Knee Injury and Osteoarthritis Outcome Scores (KOOS).
FOR QUESTIONS 44 AND 45_
The Lachman test is the most sensitive examination for acute ACL injuries. ACL injury rates are higher in women than in men. This likely is attributable to anatomic differences (smaller notches, smaller ligaments, and different landing biomechanics). Lateral meniscal tears are more common than medial tears. The anterior drawer test is accentuated with 30 degrees of external rotation of the tibia. The MRI scan shows bone bruises consistent with an ACL tear. It is also always necessary to examine other structures of the knee in patients with ACL tears. All ligaments of the affected knee should be assessed.Lateral meniscal tears are frequently associated with ACL tears. Medial meniscal tears and posterolateral corner deficiency are also possible. Randomized clinical trials comparing an early accelerated vs nonaccelerated rehabilitation have demonstrated no significant differences in long-term results. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
-Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease that is characterized by
1) onset most often by age 30.
2) a temporary state of neuronal and axonal derangement.
3) manifestations of affect such as apathy, irritability, and suicidal ideation.
4) absence of gross pathological brain changes upon autopsy.
-In the shoulder position of 90-degree forward flexion and internal rotation, what is the most important static stabilizer of the glenohumeral joint?
1) Rotator interval
2) Infraspinatus
3) Anterior band of the inferior glenohumeral ligament
4) Posterior band of the inferior glenohumeral ligament
_**CLINICAL SITUATION FOR QUESTIONS 48 AND 49**_
A 17-year-old high school wrestler sustains an abrasion over the posterior aspect of his right elbow during a match. During the next few days the abrasion becomes erythematous and he is placed on oral cephalexin 500 mg four times per day. The erythema extends proximally despite the antibiotic regimen. The patient is afebrile, there is no fluid collection associated with the lesion, and his elbow joint is not involved.
-What is the most appropriate treatment?
1) Switch to oral trimethoprim-sulfamethoxazole double-strength twice per day for 10 to 14 days
2) Switch to oral ciprofloxacin 500 mg twice per day for 10 to 14 days
3) Begin cefazolin 1 gram intravenously (IV) every 8 hours for 7 to 10 days
4) Irrigation and debridement with empiric IV antibiotic coverage
-Assuming that the lesion can be covered appropriately and there is no drainage from the lesion, when should the patient be allowed to safely return to wrestling?
1) When the absence of pain is reported by the wrestler for 3 consecutive days
2) When 72 hours of antibiotics have been administered and there is no extension of the lesion for 48 hours
3) When laboratory values are within defined limits and the patient remains afebrile for 3 days
4) When the lesion has decreased in size by 50%
FOR QUESTIONS 48 AND 49_
This patient has cellulitis, which is typically caused by group A Streptococcus or Staphylococcus. The patient’s lack of improvement with first-line antibiotics is concerning for methicillin-resistant Staphylococcus aureus (MRSA) infection. MRSA cellulitis is becoming more prevalent in young athletes,and a high index of suspicion is required to provide appropriate intervention during this
aggressive disease process. The diagnosis is typically made clinically without the use of cultures. Oral trimethoprimsulfamethoxazole (a sulfonamide-class drug) double strength twice daily for 10 to 14 days or doxycycline (a tetracycline-class drug) 100 mg twice daily for 10 to 14 days are recommended for first-line treatment of suspected MRSA cellulitis. There is no indication to proceed with irrigation and debridement; however, if the patient develops a soft-tissue abscess or the underlying joint becomes involved, this would be an appropriate intervention. Switching the athlete to an IV cephalosporin (cefazolin) is not likely to be effective against the presumed resistant bacteria.
Ciprofloxacin (a fluoroquinolone-class drug) is effective against many bacteria, but not MRSA. The current recommendation for wrestlers with cellulitis is that return to competition be allowed after 72 hours of antibiotic treatment if there has been no extension of the cellulitis for 48 hours, the lesion can be covered, and there is no drainage from the lesion. The other responses are not current recommendations for return to competition.
-A 19-year-old linebacker underwent a coracoid transfer procedure for recurrent anterior glenohumeral instability. At his 1-week postsurgical check-up, his incision is doing well; however, he reports numbness over the lateral aspect of his forearm. What nerve may have been injured during his surgery?
1) Axillary
2) Median
3) Musculocutaneous
4) Radial
-What is the most important genetic element that distinguishes community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) from hospital-acquired MRSA?
1) Beta-lactamase
2) Penicillin-binding protein 2a
3) Panton-Valentine leukocidin (PVL)
4) Staphylococcus cassette chromosome (SCCmec) type I
_CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 54_
A 13-year-old baseball player fell while rounding second base 2 days ago. He said it felt like his knee buckled when he turned toward third base. He could not finish the game, but was able to bear weight with a limp. He has had no previous knee injuries, but now complains of pain in his right knee. Initial examination demonstrated an effusion, tenderness at the proximal medial collateral region and medial patellofemoral retinaculum, decreased range of motion, and patella apprehension. He was otherwise ligamentously stable. No other noteworthy physical findings were found.
-What is the next treatment step?
1) Radiographs
2) Arthroscopy
3) MRI scan
4) Duplex ultrasound
-What do the radiographs shown in Figures 52a and 52b reveal?
1) Medial femoral chondyle physeal widening
2) Osseous or osteochondral loose fragment
3) Osgood-Schlatter disease
4) Patella nondisplaced fracture
-Figures 52c and 52d show the proton density fat-saturated MRI scans. Treatment at this stage includes arthroscopy and
1) early functional rehabilitation.
2) proximal realignment alone.
3) attempted internal fixation.
4) medial collateral ligament (MCL) repair.
FOR QUESTIONS 52 THROUGH 54_
This patient’s examination indicates a patellar or peripatellar knee injury. Initial evaluation with radiographs will assess for fracture, subluxation, or osteochondral injury. Examination findings did not demonstrate a need for emergent surgery, an MRI scan, or an ultrasound, so radiographs are the initial diagnostic imaging choice. Radiographs show an osseous or osteochondral loose fragment.
There is no evidence of obvious nondisplaced fracture or physeal changes. In suspected patella dislocation or subluxation with loose fragment seen on radiographs, an MRI scan is indicated. Lateral release alone is seldom indicated in a knee that was normal before injury. Acute proximal realignment has not been shown to alter long-term outcomes for first-time dislocators. The examination and MRI scan did not indicate a need for MCL repair. Closed reduction of the osteochondral fragment would not be indicated or appropriate for this injury. Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed.
-While obtaining informed consent for a lateral closing-wedge osteotomy, what complication should be discussed with the patient as exclusive to this procedure and not encountered in medial opening-wedge osteotomy?
1) Compartment syndrome
2) Plate breakage
3) Neurologic injury
4) Proximal tibiofibular joint disruption
_**CLINICAL SITUATION FOR QUESTIONS 56 THROUGH 58**_
Figure 56 is the MRI scan of a 15-year-old girl who had left knee pain after sustaining a noncontact twisting injury while playing soccer. She reported severe pain initially that has since improved. On examination, she had a large knee effusion with lateral joint line tenderness. Range of motion is from 5 degrees of extension to 70 degrees of flexion. She wishes to return to sports at her preinjury level of activity.
-What examination test is most likely to reveal abnormal findings?
1) Pivot shift test
2) Quadriceps active test
3) Patellar apprehension test
4) External rotation recurvatum test
-What is the most appropriate treatment?
1) Delayed ligament reconstruction
2) Physical therapy and functional bracing
3) Immediate ligament repair
4) Immediate ligament reconstruction
-What is the most likely mechanism of injury?
1) External rotation
2) Posterior translation
3) Hyperextension and varus
4) Anterior translation and internal rotation
FOR QUESTIONS 56 THROUGH 58_
The MRI scan shows a bone bruise of the lateral femoral condyle and lateral tibial plateau. This injury pattern is commonly associated with anterior cruciate ligament (ACL) rupture and an abnormal pivot shift test result. Treatment of an ACL tear in a high-demand athlete should consist of ligament reconstruction.In this patient, surgery should be delayed until she regains full range of motion to minimize risk for arthrofibrosis after surgery. Recent analysis has shown that the noncontact mechanism is more consistent with anterior translation, affecting both the medial and lateral compartments. The bone bruise in the lateral femoral condyle occurs more anterior than that of the medial femoral condyle, suggesting that internal rotation has occurred. The external rotation recurvatum test assesses for posterolateral corner injury, and a positive quadriceps active test is consistent with posterior cruciate ligament rupture. An abnormal patellar apprehension test result is suggestive of patellar instability. Nonsurgical treatment is unlikely to result in sufficient stability if this patient returns to sports at her preinjury level of activity.Primary ACL repair is associated with high failure rates. Although the precise mechanism of injury varies,injuries can be broadly classified into contact and noncontact injuries. Noncontact injuries occur with the knee in slight flexion, valgus, and internal rotation, and contact injuries typically involve a lateralside impact producing a valgus force to the knee. The valgus component of noncontact injuries has been thought to cause mainly lateral compartment bone bruising. Posterior translation is the most common mechanism of posterior cruciate ligament rupture, and hyperextension and varus is associated with posterolateral corner injury.
-A 12-year-old boy who plays multiple sports has had insidious-onset heel pain while running for 4 months. On examination, he had ankle dorsiflexion of 5 degrees. The squeeze test result was positive and the Thompson test result was negative. He has no pain with forced ankle plantar flexion. What is the most likely diagnosis?
1) Achilles rupture
2) Gastrocnemius strain
3) Calcaneal apophysitis
4) Os trigonum syndrome
_CLINICAL SITUATION FOR QUESTIONS 60 AND 61_
A 15-year-old boy has had shoulder pain for 4 weeks during the middle of baseball season. The patient says his pain is “all over my shoulder.” Examination reveals tenderness to palpation over the anterolateral aspect of the shoulder. Internal and external rotation range of motion is restricted.
Radiographs show metaphyseal sclerosis.
-What is the most significant risk factor for the development of little leaguer’s shoulder in this scenario?
1) Recent increase in the number of pitches
2) Gender (male)
3) Glenohumeral internal rotation deficit
4) Genetic factors
-This boy’s parents are eager to get him back on the field as soon as possible. What is the most appropriate treatment option?
1) Screw fixation of the epiphysis
2) Arthroscopic debridement
3) A shut-down period until the boy is asymptomatic, and gradual return to pitching via a throwing program
4) An intra-articular cortisone injection
FOR QUESTIONS 60 AND 61_
Although a recent increase in the number of pitches may have contributed to this patient’s development of little leaguer’s shoulder, the most significant overall factor is age. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress, and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Genetic factors and gender have not been studied in association with little leaguer’s shoulder. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms.Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to baseline pitching is implemented until the patient is back to baseline. This protocol has a long-term success rate exceeding 90%.
-is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal.What is the main function of the structure delineated by the black asterisks?
1) Resist anterior translation during knee flexion
2) Resist posterior translation during knee flexion
3) Resist rotatory loads during knee flexion
4) Resist rotatory loads during knee extension
-A 25-year-old wrestler has been experiencing increasing left knee pain since his last professional cage fight. He complains of both pain and instability on the medial side of his left knee. Examination reveals a grade 3 Lachman and pseudolaxity with valgus stress. Dial test findings are normal. Radiographs show medial degenerative changes and 5 degrees of varus alignment. What is the most appropriate treatment?
1) Rehabilitation with vibration-platform weight-bearing squats
2) Anterior cruciate ligament (ACL) reconstruction with autograft bone-tendon-bone
3) High-tibial osteotomy (HTO)
4) HTO plus ACL reconstruction at the same time
-What is an example of cognitive rest after concussion?
1) Playing chess
2) Increasing reading
3) Working online
4) Limiting video games
_**CLINICAL SITUATION FOR QUESTIONS 65 THROUGH 67**_
Figure 65 is the radiograph of a 24-year-old man who had left knee pain after sustaining a twisting injury while playing Ultimate Frisbee. On examination, he had a large effusion with tenderness over the lateral joint line. Pivot shift testing results were positive. Prone dial testing results at 30 degrees and 90 degrees were negative. An MRI scan shows a tear of the anterior cruciate ligament (ACL).
-Based on the radiograph, the attachment for which structure has been disrupted?
1) Iliotibial band
2) Popliteus tendon
3) Lateral meniscus
4) Lateral capsular ligament
-Compared with a transtibial technique, what effect will drilling the femoral tunnel through the anteromedial portal have?
1) Produces a longer femoral tunnel
2) Improves visualization while drilling
3) Should be performed at 90 degrees of knee flexion
4) Allows for independent access to the anatomic femoral insertion
-The patient requests anatomic double-bundle ACL reconstruction. Compared with transtibial singlebundle ACL reconstruction, anatomic double-bundle ACL reconstruction is more likely to
1) restore improved knee kinematics.
2) allow for earlier return to sports.
3) result in better clinical outcomes scores.
4) be associated with lower surgery cost.
FOR QUESTIONS 65 THROUGH 67
The radiograph shows a Segond fracture, an avulsion fracture involving the lateral capsular ligament.
This radiographic finding has been associated with ACL rupture in 75% to 100% of cases. Drilling the femoral tunnel through the anteromedial portal allows for independent access to the native femoral attachment. Fiber orientation is more oblique than with a transtibial technique and more closely resembles that of the native ligament. Double-bundle reconstruction attempts to duplicate native ACL anatomy.Biomechanical studies have shown that double-bundle reconstruction more
closely reproduces normal knee kinematics; however, this technique does not offer a clear advantage in terms of clinical outcomes.The iliotibial band inserts onto Gerdy’s tubercle. The popliteus tendon originates from the lateral femoral condyle. The lateral meniscus attaches near the intercondylar eminence at the anterior and posterior meniscal roots. Recent advances in ACL reconstruction focus on restoring the native ACL anatomy.Studies have determined that a knee flexion angle of 110 degrees is optimal to avoid blowout of the back wall and injury to the lateral structures while drilling.
Femoral tunnel length is typically shorter than with a transtibial approach and decreases with higher-flexion angles. Double-bundle reconstruction is associated with higher surgical costs because of the need for additional fixation and, in the case of allograft reconstruction, a second graft.
-A 42-year-old man has increasing pain and, to a lesser extent, some occasional left knee instability.Several years earlier he sustained a noncontact twisting injury to his knee. He had some initial soreness and pain but was able to resume his normal activities while avoiding sports. On examination, the patient has medial joint line pain, a grade 2+ Lachman, and a slight varus thrust. His radiographs reveal mild-tomoderate medial compartment osteoarthritis with varus alignment. What surgical treatment strategy likely will alleviate his pain?
1) Distal femoral osteotomy
2) Unicompartmental knee replacement
3) High tibial osteotomy (HTO), lateral closing wedge
4) HTO, medial opening wedge with decreased tibial slope
_**RESPONSES FOR QUESTIONS 69 THROUGH 71**_
1) Valgus-producing high tibial osteotomy (VPHTO)
2) Repeat knee arthroscopy
3) Total knee arthroplasty (TKA)
4) Medial meniscus transplant
--The patient is offered a VPHTO. What aspect of his history will determine the most appropriate VPHTO technique?
1) Prior arthroscopy
2) Current smoking history
3) BMI of 22
4) Age of 40
FOR QUESTIONS 13 THROUGH 16_
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. An ultrasound can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario.
Because the patient has a correctable deformity (gaps 3 mm with valgus stress) and his symptoms are localized to the involved compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgicalplanning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient.A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation,examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result,current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 is an indication for HTO but does not influence technique.
-When reconstructing the anterior cruciate ligament (ACL), what is the most common source of potential autograft failure?
1) Graft choice
2) Tunnel position
3) Tibial fixation
4) Femoral fixation
_CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 20_
A 25-year-old healthy woman injured her left knee while playing professional soccer. She has never injured this knee before. Examination 2 days after the injury occurred reveals the following: a moderate effusion, a positive Lachman test result, and mild lateral tenderness. Range of motion is between 20 degrees and 70 degrees. Radiographs reveal no fracture. An MRI scan reveals a complete rupture of the anterior cruciate ligament (ACL), an effusion, and bone bruises of the lateral femoral condyle and lateral tibial plateau. No meniscal tear is seen. The patient would like to continue playing at the professional level.
--What is the next treatment step?
1) Immobilization of the knee for 6 weeks, followed by rehabilitation and delayed ACL reconstruction
2) Immediate ACL reconstruction
3) Immediate rehabilitation for 6 months followed by ACL reconstruction if the patient is unstable in a brace
4) Immediate rehabilitation with delayed ACL reconstruction (when the athlete obtains full knee range of motion)
-What is this patient’s risk for developing osteoarthritis (OA) of the knee?
1) There is no risk for development of knee OA after reconstruction of the ligament.
2) There is no risk for development of knee OA after a double-bundle ACL reconstruction.
3) There is no evidence that ACL reconstruction reduces the incidence of knee OA.
4) There is 100% likelihood that she will develop knee OA after single-bundle ACL reconstruction.
-The patient asks if something about her anatomy has resulted in this injury. ACL anatomy differs between men and women in what manner?
1) There is no significant difference in ACL anatomy between men and women.
2) A woman’s ACL has a smaller cross-sectional area.
3) The cross-sectional area of a woman’s ACL is larger.
4) The intercondylar notch is wider in women than in men.
FOR QUESTIONS 18 THROUGH 20_
This patient has the clinical findings of an ACL rupture that is confirmed on MRI scan. She is a professional athlete and would like to return to her sport. Immediate ACL reconstruction in the setting of a knee with limited motion carries an increased risk for postsurgical stiffness. Delayed surgery after the patient regains range of motion is the preferred response. It has been shown that a woman’s ACL is smaller in the cross-sectional area.
-Figure 21 is the radiograph of a 31-year-old man who had left shoulder pain after a fall during a snow boarding jump. Residual displacement of 5 mm after closed reduction is most likely to result in which of the following?
1) Nonunion
2) Osteonecrosis
3) Altered rotator cuff mechanics
4) Normal shoulder function
-What strategy has proven most effective in preventing transmission of methicillin-resistant Staphylococcus aureus among teammates?
1) Separate players with infections in a separate locker room or changing area.
2) Treat teammates of the infected player with prophylactic antibiotics.
3) Cover any skin lesions with occlusive dressing during sporting activity.
4) Ban players with infections from any team event.
-Figure 23 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain?
1) Forward elevation in the scapular plane
2) External rotation and abduction
3) Flexion, adduction, and internal rotation
4) Flexion and abduction
_**CLINICAL SITUATION FOR QUESTIONS 24 AND 25**_
During the third quarter of a high school football game, a 16-year-old running back gets tackled and limps off the field. During the initial sideline evaluation, he has tenderness on the right iliac crest. He is a little dizzy, has a headache, and tells you, “I need to get back in the game to help the team score before halftime.”
-How can this scenario be managed most effectively?
1) Initiate rest, ice the iliac crest, and return to play when he is not limping.
2) Initiate rest, ice the iliac crest, and return to play after 20 minutes.
3) Keep the player on the sideline, perform a cognitive evaluation, and repeat the physical assessment.
4) Keep the player out of the game and send him emergently to the hospital for imaging.
-Sideline examination of this patient showed no cervical pain or tenderness; motor and sensory function were normal; and his pupils were equal, round, and reactive. He was alert and oriented to the score of game, time on the clock, and current quarter of play. His iliac crest had mild tenderness but no swelling or crepitus. The player states that he has a slight headache and is no longer dizzy. What is the most appropriate treatment?
1) Return him to the game and observe his play closely.
2) Do not return to the game and do not allow play for the remainder of the season.
3) Do not return to the game and begin a graduated return-to-play protocol for future games.
4) Perform a sideline noncontact exercise testing examination and return him to the game if he is asymptomatic.
FOR QUESTIONS 24 AND 25_
Although this player limps off the field, the fact that he felt dizzy, had a headache, and did not initially recognize that he was playing in the third quarter indicates that he sustained a concussion. The player should be kept out of the game until a cognitive examination and repeat physical assessment is completed.Even if his physical symptoms have resolved, a certain period of time has expired, or he states that he is“ready,” he should not be returned to play prior to this assessment. Sending the patient to an emergency department should be considered only after this assessment and appropriate initial sideline treatment is initiated. The Consensus Statement on Concussion in Sport recommends that no athlete with concussion symptoms be returned to same-day play. This patient still has a slight headache, but even if this resolved he should not return to the game. Adolescents and high school athletes may have neurophysiological deficits that may not be evident on the sideline, or they may have a delayed onset of symptoms. A graduated return to play for future games is recommended.
_CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29_
A 32-year-old woman has a 2-year history of progressively worsening right groin pain that is exacerbated by activity. She reports no traumatic injury and an extensive work-up by her gynecologist has ruled out an intrapelvic source of her pain. The patient is a recreational athlete and exercises regularly in the gym.The pain is preventing her from performing these activities. She reports no catching or locking symptoms.Her examination reveals a physically fit female (BMI of 20) with limited right hip range of motion. She has no tenderness to palpation around the hip. While lying supine and bringing her hip into progressive flexion with internal rotation and adduction, her groin pain is reproduced. She has normal limb lengths and demonstrates weakness secondary to pain with hip flexion on the affected side.
-What is the most likely cause of this patient’s groin pain?
1) Femoroacetabular impingement (FAI)
2) Osteoarthritis of the sacroiliac joint
3) Intra-articular loose body
4) Trochanteric bursitis
-The patient is enrolled in physical therapy for 6 weeks with little improvement of her hip symptoms.What is the next most appropriate diagnostic test to determine the presence of an associated acetabular labral tear in this patient?
1) Diagnostic arthroscopy of the hip
2) MRI scan of the hip
3) MRI arthrogram of the hip
4) Ultrasound of the hip
-The study obtained in confirms the presence of an anterosuperior acetabular labral tear and pincer morphology of the acetabulum. What is the most likely location of a chondral injury associated with these findings?
1) Posteroinferior acetabulum
2) Posterosuperior acetabulum
3) Femoral head above the fovea
4) Femoral head below the fovea
-The patient experienced little improvement with activity modification and physical therapy. An intraarticular corticosteroid injection provides excellent but short-lived pain control. She requests surgical treatment for her hip and she is counseled regarding arthroscopy and consent is obtained. Intraoperatively,a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. What treatment is most appropriate considering these findings?
1) Suture anchor repair of the labral tear and no bony resection
2) Suture anchor repair of the labral tear and bony resection of the pincer lesion
3) Debridement of the labral tear and bony resection of the pincer lesion
4) Debridement of the labral tear with no bony resection of the pincer lesion
FOR QUESTIONS 26 THROUGH 29_
The clinical scenario, examination, and MRI scans are consistent with a pincer-type FAI. The decreased range of motion is secondary to the pain produced by the continued abutment of the femoral head against the anterosuperior acetabulum. Flexing the hip while internally rotating and adducting the leg recreates this contact and is typically painful. No clinical signs suggest sacroiliac joint arthritis, an intra-articular loose body, or trochanteric bursitis, although these are all diagnoses that should be considered in a patient with a painful hip. The most sensitive and specific study to detect an acetabular labral tear is an MRI arthrogram of the hip. This study should be obtained in this patient to evaluate the labrum as well as the status of the articular cartilage. An MRI scan without intra-articular contrast is not as sensitive as an arthrogram. An ultrasound can provide a dynamic assessment of the hip and help in the setting of a snapping hip; however, this study is not reliable to determine the presence of a labral tear. In the setting of pincer FAI, the forced leverage of the anterosuperior femoral head upon the anterior acetabulum results in abnormal forces against the posteroinferior acetabulum. This continued force can lead to a chondral lesion in this location know as a “counter-coup” injury. Chondral lesions of the femoral head are rare in the setting of pincer FAI. The posterosuperior quadrant does not experience increased force and rarely sustains chondral injuries. The patient is a young, active individual with no pre-existing degenerative changes, so repair of the tear with bony resection of the pincer lesion is the most appropriate treatment.A capsulolabral detachment should be repaired because these tears can heal and the labrum functions as a seal, preventing egress of synovial fluid from the joint space. If the pincer lesion is not resected, the patient will continue to experience abnormal contact and the repair will likely fail. There is no evidence that the patient has a cam impingement, and recontouring of the femoral head/neck junction is not appropriate. Simple debridement should be reserved for intrasubstance tears of the labrum, which would not be expected to heal with repair.
_**CLINICAL SITUATION FOR QUESTIONS 30 THROUGH 32**_
Figures 30a and 30b are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he
believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg.
-What examination findings are most consistent with the pathology seen in the radiographs?
1) Pain with resisted hip flexion
2) Pain with a half sit-up, plus tenderness at the pubic ramus
3) Pain with a combination of hip flexion, adduction, and internal rotation
4) Tenderness to palpation at the greater trochanter
-What is the most likely diagnosis for the source of this patient’s pain?
1) Cam-type femoroacetabular impingement
2) Pincer-type femoroacetabular impingement
3) Hip flexor strain
4) Athletic pubalgia
-Images from an MRI scan of this patient’s left hip are shown in Figure 30c through 30e. What is the most likely cause of his acute pain?
1) Significant cartilage loss on the acetabulum
2) Labral tear
3) Femoral neck stress fracture
4) Tendonopathy of the rectus femoris
FOR QUESTIONS 30 THROUGH 32_
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement.Surgical treatment for cam impingement can be effective for symptomatic patients. Even among highlevel athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable to those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment.Byrd and Jones described 5 patients who developed transient neurapraxias that resolved uneventfully.The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a periacetabular osteotomy can develop a more retroverted acetabulum as well.
-A 25-year-old recreational soccer player has recurrent shoulder dislocations. He first dislocated his shoulder playing football in high school, was treated in a sling for 6 weeks, and returned to play for the remainder of the season. He did well until 2 years later when he reinjured the shoulder. He says that his shoulder dislocates with little injury and always “feels loose.” Examination reveals anterior instability and an MR arthrogram reveals an anterior-inferior labral tear and surgical treatment is recommended. He inquires about the benefits of arthroscopic vs open procedure. Which of the following statements reflects an advantage associated with arthroscopic procedures compared to open stabilization?
1) Range of motion might be slightly better after an arthroscopic procedure.
2) Rate of recurrent instability is lower after an arthroscopic procedure.
3) Rates of return to work are higher after an arthroscopic procedure.
4) Rates of return to sports are higher after an arthroscopic procedure.
-Figures 34a and 34b are the radiographs of a 38-year-old woman who had increasing left hip pain with activity. She noted no lower back or buttock pain and no pain along her lateral thigh. The pain usually only bothers her with running and cycling.
Nonsteroidal anti-inflammatory drugs helped initially but are not relieving her pain now. Examination with the patient supine reveals pain with internal and external rotation of her hip
with her hip and knee in an extended position. With her hip flexed to 90 degrees, she has internal rotation only to neutral, but full external rotation. What is the most likely diagnosis?
1) Cam-type femoroacetabular impingement
2) Pincer-type femoroacetabular impingement
3) Intra-articular loose body
4) Snapping psoas tendon
-A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman with a soft endpoint, varus laxity at 30 degrees, and a positive dial test at 30 degrees that dissipates at 90 degrees of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome?
1) Hamstring autograft
2) Revision ACL reconstruction and posterior cruciate ligament (PCL) reconstruction
3) Revision ACL reconstruction and posteromedial corner reconstruction
4) Revision ACL reconstruction and posterolateral corner reconstruction
-A 49-year-old man is seeking a second opinion for continued knee pain and swelling. He went to his primary doctor for swelling “on top of his knee,” and he says his doctor drained some clear fluid. He noted that his condition improved for about 1 week before the swelling returned. He now has increasing pain and redness around his kneecap.
Examination reveals significant swelling of his prepatellar bursa,with erythema over the bursa that extends to the surrounding skin. His temperature in the office is 101.7°F. What is the next step in treatment for this patient?
1) Initiate oral antibiotics for 7 days.
2) Reaspirate the bursa and inject a corticosteroid.
3) Recommend padding the patella for kneeling and ice.
4) Perform an open bursectomy and start intravenous antibiotics.
_CLINICAL SITUATION FOR QUESTIONS 37 AND 38_
An 18-year-old right-hand-dominant college freshman who is a third baseman has pain in his right shoulder after using his outstretched right arm for support while diving to catch a low line drive. He describes pivoting on his right hand and arm while reaching out to make the catch with his left-hand glove. He had pain in his shoulder but was able to finish the game with some pain while throwing. Five days later, he experiences popping pain deep in his shoulder that has improved since the injury but continued to be bothersome deep in the shoulder with higher-velocity throwing. Examination demonstrated decreased internal rotation, posterior pain with cross-body adduction and posteriorly directed force, and full rotator cuff strength. Radiograph findings were normal. After 6 weeks of physical therapy (PT), his range of motion has improved but he continues to experience deep pain with therapy. Examination shows symmetric range of motion and posterior pain with the jerk test and Kim test. His rotator cuff is strong.Figure 37a Figure 37b
-What is the next step in treatment?
1) Continued PT
2) Subacromial injection
3) CT scan
4) MRI arthrogram
-T1-weighted, fat-saturated MRI scans are shown in Figures 37a and 37b. What is the next step intreatment?
1) Open reduction internal fixation (ORIF)
2) Rotator cuff repair
3) Labrum repair
4) Chondroplasty
FOR QUESTIONS 37 AND 38_
Examination findings of posterior glenohumeral tenderness, decreased internal rotation, and reproduction of symptoms with a posterior stress test indicate a posterior shoulder injury or instability. The jerk test,with the patient seated, positions the arm in forward flexion and internal rotation with elbow flexion. One hand of the examiner is placed on the patient’s distal clavicle and scapular spine and the other hand grasps the elbow. The arm is jerked posteriorly while the shoulder girdle is jerked anteriorly, which creates pain as the posteriorly subluxated humeral head relocates into the glenoid fossa. During the Kim test, the patient is seated with the arm in 90 degrees of abduction. While the arm is elevated 45 degrees diagonally (forward flexion and adduction), the examiner applies an axial load to the elbow and a downward and posterior force to the upper arm. A positive result causes a sudden onset of posterior shoulder pain. A positive jerk test combined with a positive Kim test has a 97% sensitivity for posterior instability. After extensive PT, the patient continues to have examination findings consistent with posterior shoulder injury or instability, so an MRI scan or MRI arthrography would be helpful to assess for any pathology.A subacromial injection is not indicated by this examination, which shows a strong rotator cuff and no demonstrated bursal-sided symptoms. A CT scan can be helpful in scenarios involving bony pathology,but an MRI is indicated at this stage in the evaluation of soft tissue. Although continuing PT may help to abate symptoms, the patient was continuing to have symptoms with PT. The MRI arthrogram shows a complex posterior labrum tear at the inferior to mid glenoid with separation of labrum from the glenoid. Because the examination findings are consistent with the MRI findings and nonsurgical treatment has failed to resolve symptoms, the next step is to recommend surgical treatment with labrum debridement and/or repair. No examination or MRI findings indicate a need for injection, rotator cuff repair, ORIF, or chondroplasty unless incidental intrasurgical findings are found.
A high school athlete sustained a noncontact injury to his right knee. He says that during a football game he felt a pop and his leg gave way. He attempted to continue to play but was unable secondary to pain.Five days after the injury, radiographs of his right knee do not reveal any abnormalities. On examination,he has an effusion on the injured side and no joint line tenderness. His range of motion is full extension to 110 degrees of flexion. At 20 degrees of flexion, he has increased anterior translation compared to the contralateral, uninjured left side. At 90 degrees of flexion, the tibia does not translate posteriorly. As his knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a“clunk” within the knee. What is the most likely biomechanical basis for the “clunk”?
1) In extension, the medial tibial plateau is subluxated; as an internal rotation/valgus force is applied in conjunction with flexion, the medial tibial plateau reduces.
2) In extension, the medial tibial plateau is reduced; as an internal rotation/valgus force is applied in conjunction with flexion, the medial tibial plateau subluxates.
3) In extension, the lateral tibial plateau is reduced; as an internal rotation/valgus force is applied in conjunction with flexion, the lateral plateau subluxates.
4) In extension, the lateral tibial plateau is subluxated; as an internal rotation/valgus force is applied in conjunction with flexion, the lateral plateau reduces.
_**CLINICAL SITUATION FOR QUESTIONS 40 THROUGH 42**_
A 9-year-old boy was injured while playing soccer. His examination revealed painful range of motion between 5 degrees and 75 degrees. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality.
-What is the next diagnostic step?
1) Repeat radiographs while the patient is weight bearing
2) Ultrasound of the lower extremity and calf
3) Stress radiographs
4) CT scan
-What is the most likely area of injury?
1) Femoral attachment of the medial collateral ligament
2) Tibial attachment of the medial collateral ligament
3) Hypertrophic zone of the growth plate
4) Proliferative zone of the growth plate
FOR QUESTIONS 40 THROUGH 42_
This patient likely has a physeal injury to the distal femoral physis. Stress radiographs or an MRI scan will most reliably reveal this diagnosis. The growth plate, when injured, is most commonly fractured through the hypertrophic zone of cartilage, its weakest point. This patient is optimally treated in a cylindrical or long-leg cast. Younger patients can be treated with a hip spica with a leg extension.
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
1) Psoriasis
2) Tinea corporis
3) Herpes simplex virus
4) Community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA)
_CLINICAL SITUATION FOR QUESTIONS 44 AND 45_
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
-Range of motion of the knee is between 0 degrees and 70 degrees. What is the most appropriate treatment option?
1) Nonweight-bearing activity with crutches
2) Microfracture of the chondral defect
3) Immediate anterior cruciate ligament (ACL) reconstruction
4) Delayed ACL reconstruction
-The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports,and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation,patients who follow an early accelerated rehabilitation protocol experience
1) increased laxity.
2) no differences in long-term results.
3) increased risk for graft failure.
4) lower Knee Injury and Osteoarthritis Outcome Scores (KOOS).
FOR QUESTIONS 44 AND 45_
The Lachman test is the most sensitive examination for acute ACL injuries. ACL injury rates are higher in women than in men. This likely is attributable to anatomic differences (smaller notches, smaller ligaments, and different landing biomechanics). Lateral meniscal tears are more common than medial tears. The anterior drawer test is accentuated with 30 degrees of external rotation of the tibia. The MRI scan shows bone bruises consistent with an ACL tear. It is also always necessary to examine other structures of the knee in patients with ACL tears. All ligaments of the affected knee should be assessed.Lateral meniscal tears are frequently associated with ACL tears. Medial meniscal tears and posterolateral corner deficiency are also possible. Randomized clinical trials comparing an early accelerated vs nonaccelerated rehabilitation have demonstrated no significant differences in long-term results. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
-Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease that is characterized by
1) onset most often by age 30.
2) a temporary state of neuronal and axonal derangement.
3) manifestations of affect such as apathy, irritability, and suicidal ideation.
4) absence of gross pathological brain changes upon autopsy.
-In the shoulder position of 90-degree forward flexion and internal rotation, what is the most important static stabilizer of the glenohumeral joint?
1) Rotator interval
2) Infraspinatus
3) Anterior band of the inferior glenohumeral ligament
4) Posterior band of the inferior glenohumeral ligament
_**CLINICAL SITUATION FOR QUESTIONS 48 AND 49**_
A 17-year-old high school wrestler sustains an abrasion over the posterior aspect of his right elbow during a match. During the next few days the abrasion becomes erythematous and he is placed on oral cephalexin 500 mg four times per day. The erythema extends proximally despite the antibiotic regimen. The patient is afebrile, there is no fluid collection associated with the lesion, and his elbow joint is not involved.
-What is the most appropriate treatment?
1) Switch to oral trimethoprim-sulfamethoxazole double-strength twice per day for 10 to 14 days
2) Switch to oral ciprofloxacin 500 mg twice per day for 10 to 14 days
3) Begin cefazolin 1 gram intravenously (IV) every 8 hours for 7 to 10 days
4) Irrigation and debridement with empiric IV antibiotic coverage
-Assuming that the lesion can be covered appropriately and there is no drainage from the lesion, when should the patient be allowed to safely return to wrestling?
1) When the absence of pain is reported by the wrestler for 3 consecutive days
2) When 72 hours of antibiotics have been administered and there is no extension of the lesion for 48 hours
3) When laboratory values are within defined limits and the patient remains afebrile for 3 days
4) When the lesion has decreased in size by 50%
FOR QUESTIONS 48 AND 49_
This patient has cellulitis, which is typically caused by group A Streptococcus or Staphylococcus. The patient’s lack of improvement with first-line antibiotics is concerning for methicillin-resistant Staphylococcus aureus (MRSA) infection. MRSA cellulitis is becoming more prevalent in young athletes,and a high index of suspicion is required to provide appropriate intervention during this
aggressive disease process. The diagnosis is typically made clinically without the use of cultures. Oral trimethoprimsulfamethoxazole (a sulfonamide-class drug) double strength twice daily for 10 to 14 days or doxycycline (a tetracycline-class drug) 100 mg twice daily for 10 to 14 days are recommended for first-line treatment of suspected MRSA cellulitis. There is no indication to proceed with irrigation and debridement; however, if the patient develops a soft-tissue abscess or the underlying joint becomes involved, this would be an appropriate intervention. Switching the athlete to an IV cephalosporin (cefazolin) is not likely to be effective against the presumed resistant bacteria.
Ciprofloxacin (a fluoroquinolone-class drug) is effective against many bacteria, but not MRSA. The current recommendation for wrestlers with cellulitis is that return to competition be allowed after 72 hours of antibiotic treatment if there has been no extension of the cellulitis for 48 hours, the lesion can be covered, and there is no drainage from the lesion. The other responses are not current recommendations for return to competition.
-A 19-year-old linebacker underwent a coracoid transfer procedure for recurrent anterior glenohumeral instability. At his 1-week postsurgical check-up, his incision is doing well; however, he reports numbness over the lateral aspect of his forearm. What nerve may have been injured during his surgery?
1) Axillary
2) Median
3) Musculocutaneous
4) Radial
-What is the most important genetic element that distinguishes community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) from hospital-acquired MRSA?
1) Beta-lactamase
2) Penicillin-binding protein 2a
3) Panton-Valentine leukocidin (PVL)
4) Staphylococcus cassette chromosome (SCCmec) type I
_CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 54_
A 13-year-old baseball player fell while rounding second base 2 days ago. He said it felt like his knee buckled when he turned toward third base. He could not finish the game, but was able to bear weight with a limp. He has had no previous knee injuries, but now complains of pain in his right knee. Initial examination demonstrated an effusion, tenderness at the proximal medial collateral region and medial patellofemoral retinaculum, decreased range of motion, and patella apprehension. He was otherwise ligamentously stable. No other noteworthy physical findings were found.
-What is the next treatment step?
1) Radiographs
2) Arthroscopy
3) MRI scan
4) Duplex ultrasound
-What do the radiographs shown in Figures 52a and 52b reveal?
1) Medial femoral chondyle physeal widening
2) Osseous or osteochondral loose fragment
3) Osgood-Schlatter disease
4) Patella nondisplaced fracture
-Figures 52c and 52d show the proton density fat-saturated MRI scans. Treatment at this stage includes arthroscopy and
1) early functional rehabilitation.
2) proximal realignment alone.
3) attempted internal fixation.
4) medial collateral ligament (MCL) repair.
FOR QUESTIONS 52 THROUGH 54_
This patient’s examination indicates a patellar or peripatellar knee injury. Initial evaluation with radiographs will assess for fracture, subluxation, or osteochondral injury. Examination findings did not demonstrate a need for emergent surgery, an MRI scan, or an ultrasound, so radiographs are the initial diagnostic imaging choice. Radiographs show an osseous or osteochondral loose fragment.
There is no evidence of obvious nondisplaced fracture or physeal changes. In suspected patella dislocation or subluxation with loose fragment seen on radiographs, an MRI scan is indicated. Lateral release alone is seldom indicated in a knee that was normal before injury. Acute proximal realignment has not been shown to alter long-term outcomes for first-time dislocators. The examination and MRI scan did not indicate a need for MCL repair. Closed reduction of the osteochondral fragment would not be indicated or appropriate for this injury. Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed.
-While obtaining informed consent for a lateral closing-wedge osteotomy, what complication should be discussed with the patient as exclusive to this procedure and not encountered in medial opening-wedge osteotomy?
1) Compartment syndrome
2) Plate breakage
3) Neurologic injury
4) Proximal tibiofibular joint disruption
_**CLINICAL SITUATION FOR QUESTIONS 56 THROUGH 58**_
Figure 56 is the MRI scan of a 15-year-old girl who had left knee pain after sustaining a noncontact twisting injury while playing soccer. She reported severe pain initially that has since improved. On examination, she had a large knee effusion with lateral joint line tenderness. Range of motion is from 5 degrees of extension to 70 degrees of flexion. She wishes to return to sports at her preinjury level of activity.
-What examination test is most likely to reveal abnormal findings?
1) Pivot shift test
2) Quadriceps active test
3) Patellar apprehension test
4) External rotation recurvatum test
-What is the most appropriate treatment?
1) Delayed ligament reconstruction
2) Physical therapy and functional bracing
3) Immediate ligament repair
4) Immediate ligament reconstruction
-What is the most likely mechanism of injury?
1) External rotation
2) Posterior translation
3) Hyperextension and varus
4) Anterior translation and internal rotation
FOR QUESTIONS 56 THROUGH 58_
The MRI scan shows a bone bruise of the lateral femoral condyle and lateral tibial plateau. This injury pattern is commonly associated with anterior cruciate ligament (ACL) rupture and an abnormal pivot shift test result. Treatment of an ACL tear in a high-demand athlete should consist of ligament reconstruction.In this patient, surgery should be delayed until she regains full range of motion to minimize risk for arthrofibrosis after surgery. Recent analysis has shown that the noncontact mechanism is more consistent with anterior translation, affecting both the medial and lateral compartments. The bone bruise in the lateral femoral condyle occurs more anterior than that of the medial femoral condyle, suggesting that internal rotation has occurred. The external rotation recurvatum test assesses for posterolateral corner injury, and a positive quadriceps active test is consistent with posterior cruciate ligament rupture. An abnormal patellar apprehension test result is suggestive of patellar instability. Nonsurgical treatment is unlikely to result in sufficient stability if this patient returns to sports at her preinjury level of activity.Primary ACL repair is associated with high failure rates. Although the precise mechanism of injury varies,injuries can be broadly classified into contact and noncontact injuries. Noncontact injuries occur with the knee in slight flexion, valgus, and internal rotation, and contact injuries typically involve a lateralside impact producing a valgus force to the knee. The valgus component of noncontact injuries has been thought to cause mainly lateral compartment bone bruising. Posterior translation is the most common mechanism of posterior cruciate ligament rupture, and hyperextension and varus is associated with posterolateral corner injury.
-A 12-year-old boy who plays multiple sports has had insidious-onset heel pain while running for 4 months. On examination, he had ankle dorsiflexion of 5 degrees. The squeeze test result was positive and the Thompson test result was negative. He has no pain with forced ankle plantar flexion. What is the most likely diagnosis?
1) Achilles rupture
2) Gastrocnemius strain
3) Calcaneal apophysitis
4) Os trigonum syndrome
_CLINICAL SITUATION FOR QUESTIONS 60 AND 61_
A 15-year-old boy has had shoulder pain for 4 weeks during the middle of baseball season. The patient says his pain is “all over my shoulder.” Examination reveals tenderness to palpation over the anterolateral aspect of the shoulder. Internal and external rotation range of motion is restricted.
Radiographs show metaphyseal sclerosis.
-What is the most significant risk factor for the development of little leaguer’s shoulder in this scenario?
1) Recent increase in the number of pitches
2) Gender (male)
3) Glenohumeral internal rotation deficit
4) Genetic factors
-This boy’s parents are eager to get him back on the field as soon as possible. What is the most appropriate treatment option?
1) Screw fixation of the epiphysis
2) Arthroscopic debridement
3) A shut-down period until the boy is asymptomatic, and gradual return to pitching via a throwing program
4) An intra-articular cortisone injection
FOR QUESTIONS 60 AND 61_
Although a recent increase in the number of pitches may have contributed to this patient’s development of little leaguer’s shoulder, the most significant overall factor is age. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress, and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Genetic factors and gender have not been studied in association with little leaguer’s shoulder. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms.Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to baseline pitching is implemented until the patient is back to baseline. This protocol has a long-term success rate exceeding 90%.
-is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal.What is the main function of the structure delineated by the black asterisks?
1) Resist anterior translation during knee flexion
2) Resist posterior translation during knee flexion
3) Resist rotatory loads during knee flexion
4) Resist rotatory loads during knee extension
-A 25-year-old wrestler has been experiencing increasing left knee pain since his last professional cage fight. He complains of both pain and instability on the medial side of his left knee. Examination reveals a grade 3 Lachman and pseudolaxity with valgus stress. Dial test findings are normal. Radiographs show medial degenerative changes and 5 degrees of varus alignment. What is the most appropriate treatment?
1) Rehabilitation with vibration-platform weight-bearing squats
2) Anterior cruciate ligament (ACL) reconstruction with autograft bone-tendon-bone
3) High-tibial osteotomy (HTO)
4) HTO plus ACL reconstruction at the same time
-What is an example of cognitive rest after concussion?
1) Playing chess
2) Increasing reading
3) Working online
4) Limiting video games
_**CLINICAL SITUATION FOR QUESTIONS 65 THROUGH 67**_
Figure 65 is the radiograph of a 24-year-old man who had left knee pain after sustaining a twisting injury while playing Ultimate Frisbee. On examination, he had a large effusion with tenderness over the lateral joint line. Pivot shift testing results were positive. Prone dial testing results at 30 degrees and 90 degrees were negative. An MRI scan shows a tear of the anterior cruciate ligament (ACL).
-Based on the radiograph, the attachment for which structure has been disrupted?
1) Iliotibial band
2) Popliteus tendon
3) Lateral meniscus
4) Lateral capsular ligament
-Compared with a transtibial technique, what effect will drilling the femoral tunnel through the anteromedial portal have?
1) Produces a longer femoral tunnel
2) Improves visualization while drilling
3) Should be performed at 90 degrees of knee flexion
4) Allows for independent access to the anatomic femoral insertion
-The patient requests anatomic double-bundle ACL reconstruction. Compared with transtibial singlebundle ACL reconstruction, anatomic double-bundle ACL reconstruction is more likely to
1) restore improved knee kinematics.
2) allow for earlier return to sports.
3) result in better clinical outcomes scores.
4) be associated with lower surgery cost.
FOR QUESTIONS 65 THROUGH 67
The radiograph shows a Segond fracture, an avulsion fracture involving the lateral capsular ligament.
This radiographic finding has been associated with ACL rupture in 75% to 100% of cases. Drilling the femoral tunnel through the anteromedial portal allows for independent access to the native femoral attachment. Fiber orientation is more oblique than with a transtibial technique and more closely resembles that of the native ligament. Double-bundle reconstruction attempts to duplicate native ACL anatomy.Biomechanical studies have shown that double-bundle reconstruction more
closely reproduces normal knee kinematics; however, this technique does not offer a clear advantage in terms of clinical outcomes.The iliotibial band inserts onto Gerdy’s tubercle. The popliteus tendon originates from the lateral femoral condyle. The lateral meniscus attaches near the intercondylar eminence at the anterior and posterior meniscal roots. Recent advances in ACL reconstruction focus on restoring the native ACL anatomy.Studies have determined that a knee flexion angle of 110 degrees is optimal to avoid blowout of the back wall and injury to the lateral structures while drilling.
Femoral tunnel length is typically shorter than with a transtibial approach and decreases with higher-flexion angles. Double-bundle reconstruction is associated with higher surgical costs because of the need for additional fixation and, in the case of allograft reconstruction, a second graft.
-A 42-year-old man has increasing pain and, to a lesser extent, some occasional left knee instability.Several years earlier he sustained a noncontact twisting injury to his knee. He had some initial soreness and pain but was able to resume his normal activities while avoiding sports. On examination, the patient has medial joint line pain, a grade 2+ Lachman, and a slight varus thrust. His radiographs reveal mild-tomoderate medial compartment osteoarthritis with varus alignment. What surgical treatment strategy likely will alleviate his pain?
1) Distal femoral osteotomy
2) Unicompartmental knee replacement
3) High tibial osteotomy (HTO), lateral closing wedge
4) HTO, medial opening wedge with decreased tibial slope
_**RESPONSES FOR QUESTIONS 69 THROUGH 71**_
Question 41High Yield
Slide 1
This patient presents for treatment of a painful hallux varus deformity following correction of hallux valgus deformity (Slide). All of the following procedures may be acceptable surgical alternatives for correction of deformity with the exception of:
This patient presents for treatment of a painful hallux varus deformity following correction of hallux valgus deformity (Slide). All of the following procedures may be acceptable surgical alternatives for correction of deformity with the exception of:
Explanation
The extensor hallucis longus or the extensor hallucis brevis (rarely the abductor hallucis) may be used as a tendon transfer for correction. Arthrodesis of the hallux interphalangeal joint may be performed for correction of a fixed claw deformity of the interphalangeal joint, usually in conjunction with a tendon transfer. Arthrodesis of the metatarsophalangeal joint is a reasonable alternative provided there is no fixed deformity of the interphalangeal joint present and when arthritis or fixed deformity of the metatarsophalangeal joint is present.
Question 42High Yield
Slide 1
A 17-year-old patient presents for evaluation and treatment of pain in the back of her ankle. She is a ballet dancer and has noticed that for the past year, she is unable to assume the pointe position without pain. Upon clinical examination she has full range of motion, excellent strength, normal toe function, and pain with pressure in the posterior ankle. The cause of her pain is:
A 17-year-old patient presents for evaluation and treatment of pain in the back of her ankle. She is a ballet dancer and has noticed that for the past year, she is unable to assume the pointe position without pain. Upon clinical examination she has full range of motion, excellent strength, normal toe function, and pain with pressure in the posterior ankle. The cause of her pain is:
Explanation
Posterior ankle impingement is common in ballet dancers. When in the pointe position, maximum plantar flexion of the ankle is present, and pain may occur from impingement in the posterior ankle. Flexor hallucis tendonitis may cause posterior ankle pain, but there is no evidence for this condition here.
Question 43High Yield
Figures 1 and 2 are the radiographs of a 10-year-old boy who came to the emergency department after sustaining a basketball injury. He has a large effusion and increased translation on Lachman’s examination. What is the most appropriate management of this injury?

Explanation
■
The imaging shows a displaced tibial spine avulsion. Non-displaced or minimally displaced fractures can be treated with long leg casting in extension, but displaced fractures require either open or arthroscopically assisted reduction and internal fixation with either screws or a suture construct. Although late knee instability is reported, an attempt at fracture fixation is recommended rather than acutely undergoing ACL reconstruction.
■
The imaging shows a displaced tibial spine avulsion. Non-displaced or minimally displaced fractures can be treated with long leg casting in extension, but displaced fractures require either open or arthroscopically assisted reduction and internal fixation with either screws or a suture construct. Although late knee instability is reported, an attempt at fracture fixation is recommended rather than acutely undergoing ACL reconstruction.
Question 44High Yield
Which of the following is the major blood supply to the heel pad?
Explanation
No detailed explanation provided for this question.
Question 45High Yield
A 32-year-old woman with a history of diabetes presents with a 1-month history of painless swelling in the foot. The foot is swollen, warm, and erythema is present in the midfoot. She has no fever and her blood sugars are normal. Radiographs demonstrate the presence of fracture and dislocation of the tarsometatarsal joint. There are no new periosteal bone formations, and complete dorsal dislocation of the metatarsals on the cuneiforms is noted. The ideal treatment is:
Explanation
If there is a contraindication to performing surgery, nonoperative methods of treatment for an acute C harcot neuroarthropathy may be acceptable. This patientâs midfoot is dislocated and is likely to result in a worsening deformity over time, with ulceration and infection possible. Open reduction with internal fixation has not proven sufficient in patients presenting with the symptoms indicated in the scenario. Arthrodesis is most likely to yield a satisfactory outcome.
Question 46High Yield
A 12-year-old girl is seen after tripping and twisting her ankle earlier in the morning. She had immediate pain and swelling and was unable to bear weight. Radiographs are shown in Figures 80a through 80c.
Appropriate treatment should consist of which of the following?
Appropriate treatment should consist of which of the following?
Explanation
Salter Harris III and IV fractures of the medial malleolus often contain a large cartilaginous portion, larger than the apparent ossified fragment seen on radiographs. Consequently, articular incongruity is common. As such, open reduction and internal fixation is often required. Growth disturbance and angular deformity are also common complications of Salter Harris III and IV fractures of the distal tibia.
REFERENCES: Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659.
Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment. J Am Acad Orthop Surg 2001;9:268-278.
REFERENCES: Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659.
Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment. J Am Acad Orthop Surg 2001;9:268-278.
Question 47High Yield
A 20-year-old woman sustained the closed injury shown in Figures 49a and 49b in a motor vehicle accident. Examination reveals that this is an isolated injury; however, she has a complete radial nerve palsy. Management should consist of
Explanation
Lacerated radial nerves are associated with open humeral fractures. All open humeral fractures with radial nerve palsy should be managed with radial nerve exploration and skeletal stabilization. Closed humeral fractures with associated radial nerve palsy usually have an intact nerve with neurapraxia. Most of these patients recover without surgical treatment. If the patient has multiple injuries, skeletal stabilization may be indicated to improve mobilization. For an isolated closed humeral fracture with a radial nerve palsy, the treatment of choice is splinting for 1 to 2 weeks, followed by a humeral fracture brace.
REFERENCES: Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high-energy humeral shaft fractures. J Hand Surg Am 2004;29:144-147.
Foster RJ, Swiontkowski MF, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
REFERENCES: Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high-energy humeral shaft fractures. J Hand Surg Am 2004;29:144-147.
Foster RJ, Swiontkowski MF, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
Question 48High Yield
A 42-year-old woman has persistent thumb pain that she notes is worse with opening jars and turning her car key. Opponens splinting provides some relief, but she is poorly tolerant of the splint. Finkelstein’s test is negative, and a carpometacarpal grind test is positive. The radiographs shown in Figures 48a and 48b reveal minimal degenerative changes at the first carpometacarpal joint. What is the best course of action?
Explanation
The woman has early basilar thumb arthritis. An extension osteotomy will redirect the force to the dorsal, more uninvolved portion of the first carpometacarpal joint and has been reported to alleviate pain in these patients. Arthrodesis is usually reserved for young, typically male laborers. Thermal shrinkage and denervation are considered experimental at this time. Interposition arthroplasty is typically used for more advanced stages of arthritis.
REFERENCES: Tomaino MM: Treatment of Eaton stage I trapeziometacarpal disease with thumb metacarpal extension osteotomy. J Hand Surg Am 2000;25:1100-1106.
Pellegrini VD Jr, Parentis M, Judkins A, et al: Extension metacarpal osteotomy in the treatment of trapeziometacarpal osteoarthritis: A biomechanical study. J Hand Surg Am 1996;21:16-23.
Tomaino MM, Pellegrini VD, Burton RI: Arthroplasty of the basal joint of the thumb: Long-term follow-up after ligament reconstruction with tendon interposition. J Bone Joint Surg Am 1995;77:346-355.
REFERENCES: Tomaino MM: Treatment of Eaton stage I trapeziometacarpal disease with thumb metacarpal extension osteotomy. J Hand Surg Am 2000;25:1100-1106.
Pellegrini VD Jr, Parentis M, Judkins A, et al: Extension metacarpal osteotomy in the treatment of trapeziometacarpal osteoarthritis: A biomechanical study. J Hand Surg Am 1996;21:16-23.
Tomaino MM, Pellegrini VD, Burton RI: Arthroplasty of the basal joint of the thumb: Long-term follow-up after ligament reconstruction with tendon interposition. J Bone Joint Surg Am 1995;77:346-355.
Question 49High Yield
A 32-year-old man who works as a laborer has had left trapezius wasting and lateral scapular winging after injuring his shoulder when a cargo box fell onto his neck 8 months ago. He now reports posterior shoulder pain and fatigue, and he has difficulty shrugging his shoulder. Examination reveals marked scapular winging, impingement signs, and an asymmetrical appearance when the patient attempts a shoulder shrug. Primary scapular-trapezius winging is the result of damage to the
Explanation
The patient has primary scapular-trapezius winging. This condition can be caused by blunt trauma to the relatively superficial spinal accessory nerve that is located in the floor of the posterior cervical triangle in the subcutaneous tissue. Other causes of injury include penetrating trauma, traction, or surgical injury. With trapezius winging, the shoulder appears depressed and laterally translated because of an unopposed serratus anterior. This contrasts with primary serratus anterior winging, which is caused by injury to the long thoracic nerve. In this condition, the scapula assumes a position of superior elevation and medial translation, and the inferior angle is rotated medially. The thoracodorsal nerve supplies the latissimus dorsi and is not involved in primary scapular winging.
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Wright TA: Accessory spinal nerve injury. Clin Orthop 1975;108:15-18.
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Wright TA: Accessory spinal nerve injury. Clin Orthop 1975;108:15-18.
Question 50High Yield
Epiphysiodesis for macrodactyly should be performed at the following location:
Explanation
Treatment by epiphysiodesis for macrodactyly is ineffective if only single phalanges are treated. Therefore, treatment of the proximal phalanx, distal phalanx, or the middle phalanx alone is incorrect. The author prefers to perform epiphysiodesis only on the proximal and distal phalanges. The middle phalanx is not treated to preserve motion at the proximal interphalangeal joint.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon