Arab Board Orthopedic B Review | Dr Hutaif General Orth -...
14 Apr 2026
60 min read
135 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Arab Board Orthopedic B Review | Dr Hutaif Ge...
00:00
Start Quiz
Question 1High Yield
A 54-year-old woman presents with a 1-year history of medial foot and ankle pain. She does not recall an episode of trauma, and she has had no change in her daily living activities. Her foot is changing shape; it is flatter than the opposite foot. On clinical examination she has a unilateral flatfoot deformity, an inability to perform a single heel rise, and weak inversion strength. The subtalar joint is flexible. Following an initial period of support of the foot, surgery is recommended. The ideal procedure is:
Explanation
This patient has a rupture of the posterior tibial tendon. Repair of the tendon will not work because there is a degenerative elongation of the tendon that will not heal. Because the foot is flexible, arthrodesis is not necessary. Flexor digitorum longus transfer with calcaneal osteotomy is a reliable procedure for treatment of Stage II posterior tibial tendon insufficiency.
Question 2High Yield
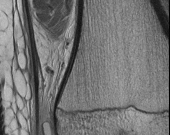
Figures 1 and 2 are the MRI scans of a 21-year-old swimmer who has had pain in the lateral shoulder for 6 months. It is worse while swimming and with reaching overhead. Twelve weeks of physical therapy and a single corticosteroid injection have failed to improve her symptoms. What is the best next step?
18
18
Explanation
In the MRI scans, the patient has a high-grade tear of the undersurface of the superior rotator cuff. This is known as a partial articular-sided tendon avulsion lesion. This is often seen in overhead athletes and is associated with internal impingement. Given the length of symptoms, failure to respond to nonsurgical treatment, and the high-grade nature of the tear in a young patient, an arthroscopic repair should be performed. The available images do not demonstrate evidence of SLAP tear, Bankart lesion, or suprascapular nerve compression.
Question 3High Yield
A 17-year-old male football player is seen 1 week after developing symptoms of infectious mononucleosis in the middle of the season. Examination reveals evidence of splenomegaly. He and his parents want to know if he can play in a game the following day. What is the most appropriate recommendation?

Explanation
DISCUSSION: Infectious mononucleosis (IMN) is a self-limiting viral (Epstein-Barr virus) infection that affects mostly adolescents. One of the clinical findings in IMN is splenomegaly. Unfortunately, the splenomegaly is palpable only 50% of the time. The risk for spontaneous splenic rupture is highest 3 weeks after the onset of symptoms. Thus, most clinicians recommend return to contact sports after 4 weeks from the onset of symptoms. This patient presented 1 week after the onset of symptoms, so he can return to play in 3-4 weeks from the time he was examined. The athlete should be afebrile, well hydrated, and asymptomatic. Airway obstruction is usually not of concern. Disease transmission to teammates is possible in the acute phases.
REFERENCES: Waninger KD, Harcke HT: Determination of safe return to play for athletes recovering from infectious mononucleosis: A review of the literature. Clin J Sport Med 2005; 15:410-416.
Auwaerter PG: Infectious mononucleosis: Return to play. Clin Sports Med 2004;23:485-497.
Figure 17
REFERENCES: Waninger KD, Harcke HT: Determination of safe return to play for athletes recovering from infectious mononucleosis: A review of the literature. Clin J Sport Med 2005; 15:410-416.
Auwaerter PG: Infectious mononucleosis: Return to play. Clin Sports Med 2004;23:485-497.
Figure 17
Question 4High Yield
Figures 17a and 17b show the radiographs of a 32-year-old professional athlete who sustained an injury to the first metatarsal. A view of the opposite noninjured side is shown in Figure 17c. Management of the fracture should consist of
Explanation
Parameters for first metatarsal fracture management are different than for shaft fractures of the central second, third, and fourth metatarsals. The first metatarsal carries a greater load and if malunited, can create transfer lesions by virtue of uneven weight distribution; therefore, nonsurgical management is not indicated for this patient. Percutaneous pinning is not as likely to result in an anatomic reduction as open reduction and internal fixation. As his livelihood depends on an expeditious return to function, the choice of open reduction and internal fixation allows for earlier motion and rehabilitation.
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 64-65.
Shereff MJ: Compartment syndromes of the foot. Instr Course Lect 1990;39:127-132.
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 64-65.
Shereff MJ: Compartment syndromes of the foot. Instr Course Lect 1990;39:127-132.
Question 5High Yield
What is the average time to radiographic union of this fracture?
Explanation
- 6 weeks_
Question 6High Yield
Pediatric flexor tendon injuries of the upper extremity differ from adult flexor tendon injuries in which of the following ways?
Explanation
DISCUSSION: Pediatric flexor tendon injuries have several remarkable distinctions from those in adults. Delayed presentation is more common in children, at times requiring staged flexor tendon reconstruction. Three to four weeks of postoperative immobilization following acute repair is recommended in children as opposed to early motion protocols used in adults. Temporary paralytic agents (botulinum toxin type A) have also been shown to facilitate the rehabilitation phase of flexor tendon care in very young children.
REFERENCE: Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of
Orthopaedic Surgeons, 2008, p 675.
REFERENCE: Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of
Orthopaedic Surgeons, 2008, p 675.
Question 7High Yield
A 32-year-old female sustained a bimalleolar ankle fracture and was treated with open reduction and internal fixation four months ago. A radiograph of her ankle is shown in Figure A. Recommended management should consist of?

Explanation
This patient requires revision open reduction and internal fixation of her syndesmosis as post-operative radiographs demonstrate a severely malaligned ankle with obvious syndesmosis widening and fibular shortening.
Malalignment following ankle fracture fixation can alter the anatomical axis of the joint, articular congruency, and normal load distribution. This predisposes the patient to the development of chronic pain, functional impairment, and finally early post-traumatic ankle arthritis.
Marti et al. retrospectively reviewed the outcomes of 31 patients with malunited ankle fractures who underwent reconstructive osteotomies. The authors found that reconstruction resulted in good or excellent results in the majority of patients. They also note that minor post-traumatic arthritis was not a contraindication to reconstruction.
Ramsey et al. evaluated 23 cadaveric ankles using a carbon black transference technique to determine the contact area in the dissected tibiotalar articulations, with the talus in neutral position and displaced one, two, four, and six millimeters laterally. They found that 1 mm of lateral talar displacement resulted in a 42% decrease in tibiotalar contact area.
Figure A is a x-ray demonstrating severe malalignment of a bimalleolar ankle fracture following fixation of the fibula and medial malleolus. There is obvious shortening of the fibula and lateral shift and valgus tilt of the talus associated with a disrupted syndesmosis.
Incorrect Answers:
Answer 1 & 2: Physical therapy and short leg bracing are not indicated at this point as the anatomical malalignment needs to first be addressed via revision surgery.
Answer 4: The addition of a syndesmosis screw will not successfully reduce the syndesmosis as it has been chronically malreduced and will require open reduction and debridement prior to syndesmosis screw fixation.
Answer 5: Open medial ankle ligament reconstruction is insufficient in isolation to provide mechanical stability to the ankle fractures with syndesmosis disruption.
Malalignment following ankle fracture fixation can alter the anatomical axis of the joint, articular congruency, and normal load distribution. This predisposes the patient to the development of chronic pain, functional impairment, and finally early post-traumatic ankle arthritis.
Marti et al. retrospectively reviewed the outcomes of 31 patients with malunited ankle fractures who underwent reconstructive osteotomies. The authors found that reconstruction resulted in good or excellent results in the majority of patients. They also note that minor post-traumatic arthritis was not a contraindication to reconstruction.
Ramsey et al. evaluated 23 cadaveric ankles using a carbon black transference technique to determine the contact area in the dissected tibiotalar articulations, with the talus in neutral position and displaced one, two, four, and six millimeters laterally. They found that 1 mm of lateral talar displacement resulted in a 42% decrease in tibiotalar contact area.
Figure A is a x-ray demonstrating severe malalignment of a bimalleolar ankle fracture following fixation of the fibula and medial malleolus. There is obvious shortening of the fibula and lateral shift and valgus tilt of the talus associated with a disrupted syndesmosis.
Incorrect Answers:
Answer 1 & 2: Physical therapy and short leg bracing are not indicated at this point as the anatomical malalignment needs to first be addressed via revision surgery.
Answer 4: The addition of a syndesmosis screw will not successfully reduce the syndesmosis as it has been chronically malreduced and will require open reduction and debridement prior to syndesmosis screw fixation.
Answer 5: Open medial ankle ligament reconstruction is insufficient in isolation to provide mechanical stability to the ankle fractures with syndesmosis disruption.
Question 8High Yield
A 75-year-old man has persistent radial sided hand and wrist pain. Radiographs demonstrate severe scaphotrapezial trapezoidal arthritis. His basal joint is unaffected. His pain has failed to improve with bracing, activity modification, and image-guided corticosteroid injection. He has elected surgical treatment. What longterm complication can arise from a distal scaphoid resection?
Explanation
Resection of the distal pole of the scaphoid eliminates the arthritic contact at the scaphotrapeziotrapezoid joint; however, it functionally shortens the scaphoid. Theoretically, the lunate is at equilibrium between the extension moment of the capitate and the triquetrum and the flexion moment of the scaphoid. Shortening the scaphoid allows the extension moment of the triquetrum to predominate, pulling the lunate into extension and creating a DISI deformity. Concomitant capsulodesis or interposition is recommended _by some authors to prevent this complication._
Question 9High Yield
Figures 1 and 2 are the clinical photograph and radiograph of a newborn who is seen for evaluation of his feet. A rigid rocker bottom foot is present with dorsal foot crease. The most appropriate next step in management is

Explanation
■
Congenital vertical talus is a rare condition in which the navicular is dorsally dislocated on the talus. There is also hindfoot equinus and valgus, resulting in the rocker bottom appearance. Fifty percent of cases are associated with other conditions (arthrogryposis, chromosomal abnormalities, skeletal dysplasia, myelomeningocele). Once the diagnosis is confirmed, usually on a plantar flexion lateral radiograph (the first MT does not align with the first metatarsal), treatment with serial casting described by Dobbs and associates is instituted. Once the talus lines up with the first metatarsal, surgical reduction of the talonavicular joint with pinning and Achilles tenotomy are done to correct the deformity.
■
Congenital vertical talus is a rare condition in which the navicular is dorsally dislocated on the talus. There is also hindfoot equinus and valgus, resulting in the rocker bottom appearance. Fifty percent of cases are associated with other conditions (arthrogryposis, chromosomal abnormalities, skeletal dysplasia, myelomeningocele). Once the diagnosis is confirmed, usually on a plantar flexion lateral radiograph (the first MT does not align with the first metatarsal), treatment with serial casting described by Dobbs and associates is instituted. Once the talus lines up with the first metatarsal, surgical reduction of the talonavicular joint with pinning and Achilles tenotomy are done to correct the deformity.
Question 10High Yield
A 12-year-old boy with achondroplasia has a gradual 40° thoracolumbar kyphosis. He is unable to walk more than two blocks. Magnetic resonance imaging reveals spinal stenosis, and the patient is scheduled to undergo posterior decompression from T12- S1. In addition to this procedure, you recommend:
Explanation
Extensive posterior decompression poses a high risk of postoperative increase in kyphosis because of both the patientâs age and pre-existing kyphosis.
Observation would not be a good idea because the risk is already known to be high.
Neither a brace nor an uninstrumented fusion would prevent the deformity from developing. C orpectomy is not indicated because the kyphosis is not focal.
Posterior instrumented fusion at the time of decompression is indicated.
Observation would not be a good idea because the risk is already known to be high.
Neither a brace nor an uninstrumented fusion would prevent the deformity from developing. C orpectomy is not indicated because the kyphosis is not focal.
Posterior instrumented fusion at the time of decompression is indicated.
Question 11High Yield
The addition of oblique lumbar radiographs has been shown to
Explanation
- provide no significant benefit.
Question 12High Yield
Figure 33 is the preoperative photograph of the patient's forefoot with the heel taken out of valgus. Which procedure will best address this forefoot deformity (which cannot be passively corrected by the examiner)?
33
33


Explanation
The most common cause of acquired adult flatfoot deformity (AAFD) is dysfunction of the posterior tibial tendon. Tearing of the calcaneonavicular (spring) ligament and gastrocnemius contracture results from longer-standing attenuation of the posterior tibial tendon. Tarsal coalitions typically cause rigid flatfoot deformity. The calcaneonavicular ligament comprises superomedial and inferomedial bands. More than 70% of patients with AAFD have tearing of the superomedial band. Tearing of the inferior band is seen less commonly. Deltoid ligament insufficiency can be seen in long-standing valgus foot deformity. Initial treatment should start with ankle-foot orthosis bracing and physical therapy.
The radiographs reveal loss of arch, significant uncoverage of the talar head by the navicular, and lack of significant arthritis. Fusion procedures are not indicated considering the patient's flexible deformity and the absence of hindfoot arthritis. Realignment osteotomy must be combined with flexor digitorum longus tendon transfer to successfully alleviate this patient's symptoms. Lateral column lengthening will correct the forefoot abduction and talonavicular subluxation. A medial sliding osteotomy can achieve additional correction and decompress subfibular impingement. A dorsal opening plantar flexion (Cotton) osteotomy of the medial cuneiform is an adjunct procedure that is needed to balance the foot in cases of residual forefoot varus, as seen in the clinical photograph.
RECOMMENDED READINGS
Pinney SJ, Lin SS. Current concept review: acquired adult flatfoot deformity. [Foot Ankle Int. 2006 Jan;27(1):66-75. Review. PubMed PMID: 16442033. ](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16442033)
[Bluman EM, Title CI, Myerson MS. Posterior tibial tendon rupture: a refined classification system. Foot Ankle Clin. 2007 Jun;12(2):233-49, v. Review. PubMed PMID: 17561198. ](http://www.ncbi.nlm.nih.gov/pubmed/17561198)[View](http://www.ncbi.nlm.nih.gov/pubmed/17561198)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17561198)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17561198)
Haddad SL, Mann RA. Flatfoot deformity in adults. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:1007-1085.
The radiographs reveal loss of arch, significant uncoverage of the talar head by the navicular, and lack of significant arthritis. Fusion procedures are not indicated considering the patient's flexible deformity and the absence of hindfoot arthritis. Realignment osteotomy must be combined with flexor digitorum longus tendon transfer to successfully alleviate this patient's symptoms. Lateral column lengthening will correct the forefoot abduction and talonavicular subluxation. A medial sliding osteotomy can achieve additional correction and decompress subfibular impingement. A dorsal opening plantar flexion (Cotton) osteotomy of the medial cuneiform is an adjunct procedure that is needed to balance the foot in cases of residual forefoot varus, as seen in the clinical photograph.
RECOMMENDED READINGS
Pinney SJ, Lin SS. Current concept review: acquired adult flatfoot deformity. [Foot Ankle Int. 2006 Jan;27(1):66-75. Review. PubMed PMID: 16442033. ](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16442033)
[Bluman EM, Title CI, Myerson MS. Posterior tibial tendon rupture: a refined classification system. Foot Ankle Clin. 2007 Jun;12(2):233-49, v. Review. PubMed PMID: 17561198. ](http://www.ncbi.nlm.nih.gov/pubmed/17561198)[View](http://www.ncbi.nlm.nih.gov/pubmed/17561198)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17561198)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17561198)
Haddad SL, Mann RA. Flatfoot deformity in adults. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:1007-1085.
Question 13High Yield
A 69-year-old patient with diabetes has had acute-onset back pain and difficulty with ambulation for several hours. Evaluation reveals a temperature of 38.3°C, a white blood cell (WBC) count of 14000/µL (reference range [rr], 4500-11000/µL), C-reactive protein (CRP) level of 120 mg/L (rr, 0.08-3.1 mg/L), erythrocyte sedimentation rate of 130 mm/h (rr, 0-20 mm/h), normal rectal examination findings, and normal sensation to light touch. Motor function testing of the lower extremities reveals 3/5 ankle dorsiflexion and 4/5 plantar flexion strength bilaterally. An MR image reveals a large epidural abscess from L1-5. What is the most appropriate treatment at this time?


Explanation
Epidural abscess is a serious and potentially disastrous condition. Although medical management is effective in some situations, surgical decompression is considered urgent with the presence of a neurological deficit. Medical management can be considered in the case of a neurologically intact patient, particularly when the microorganism has been identified. If medical management is chosen, careful observation and serial examination for neurologic deterioration is required. Surgical decompression is indicated if a patient's neurologic status worsens or if medical management failure is noted. Additionally, diabetes, a CRP level higher than 115 mg/L, WBC higher than 12500/µL , and bacteremia have proven predictive of medical treatment failure. This patient would be a better candidate for urgent surgical decompression and subsequent IV antibiotics than for medical management.
RECOMMENDED READINGS
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683/. ](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
CLINICAL SITUATION FOR QUESTIONS 96 AND 97
Figures 96a and 96b are the CT scans of a 32-year-old man who was thrown from his motorcycle. He has humeral shaft and femoral shaft fractures. A secondary survey reveals substantial tenderness to his lower thoracic spine. He is awake and alert and his movement is limited by pain secondary to the extremity fractures. He is otherwise neurologically intact.
A B
RECOMMENDED READINGS
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683/. ](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
CLINICAL SITUATION FOR QUESTIONS 96 AND 97
Figures 96a and 96b are the CT scans of a 32-year-old man who was thrown from his motorcycle. He has humeral shaft and femoral shaft fractures. A secondary survey reveals substantial tenderness to his lower thoracic spine. He is awake and alert and his movement is limited by pain secondary to the extremity fractures. He is otherwise neurologically intact.
A B
Question 14High Yield
A 41-year-old female postal worker reports a 9-month history of left groin and lateral hip pain. She denies pain in the right hip. Her social history reveals that she smokes and drinks on average five alcoholic beverages per week. Her body mass index (BMI) is 26. Radiographs are shown in Figures 31a through 31c and coronal and axial MRI scans are shown in Figures 3 Id and 31e, respectively. What is the most important factor that will determine if her right hip will become symptomatic?

Explanation
DISCUSSION: Several factors have been examined as potentially predictive of progression in the patient with an asymptomatic osteonecrotic lesion of the femoral head. While the presence of ongoing risk factors, lesion location, lesion stage, age, gender, and BMI have all been suspected as important, the size of the lesion, particularly when over one third of the size of the femoral head, is a significant risk factor for progression.
REFERENCES: Nam KW, Kim YL, Yoo JJ, et al: Fate of untreated asymptomatic osteonecrosis of the femoral head. J Bone Joint Surg Am 2008;90:477-484.
Hungerford DS, Jones LC: Asymptomatic osteonecrosis: Should it be treated? Clin Orthop Relat Res 2004;429:124-130.
Figure 32a Figure 32b Figure 32c Figure 32d
REFERENCES: Nam KW, Kim YL, Yoo JJ, et al: Fate of untreated asymptomatic osteonecrosis of the femoral head. J Bone Joint Surg Am 2008;90:477-484.
Hungerford DS, Jones LC: Asymptomatic osteonecrosis: Should it be treated? Clin Orthop Relat Res 2004;429:124-130.
Figure 32a Figure 32b Figure 32c Figure 32d
Question 15High Yield
Figures 1 and 2 are the radiographs of a 13-year-old girl who stumbled off a porch. Damage to which artery is implicated in the development of compartment syndrome in this patient?

Explanation
■
The anterior tibial recurrent artery branches from the anterior tibial artery as it pierces the intermuscular septum and courses proximally near the lateral aspect of the tibial tubercle. This places it at risk for injury with tibial tubercle fractures and can contribute to an isolated anterior compartment syndrome. The other listed arteries are not typically injured in this fracture pattern.
■
The anterior tibial recurrent artery branches from the anterior tibial artery as it pierces the intermuscular septum and courses proximally near the lateral aspect of the tibial tubercle. This places it at risk for injury with tibial tubercle fractures and can contribute to an isolated anterior compartment syndrome. The other listed arteries are not typically injured in this fracture pattern.
Question 16High Yield
Which of the following describes the inheritance pattern of Gaucher's disease:
Explanation
Structural defects are usually transmitted by an autosomal-dominant pattern. In contrast, with metabolic or enzyme deficiencies, the condition is usually transmitted in an autosomal-recessive pattern.
Remember the major autosomal-recessive conditions: Sickle cell disease
Osteogenesis imperfecta (Types II, III)
Hypophosphatasia Homocystinuria Gaucher's disease
Remember the major autosomal-recessive conditions: Sickle cell disease
Osteogenesis imperfecta (Types II, III)
Hypophosphatasia Homocystinuria Gaucher's disease
Question 17High Yield
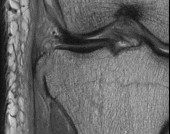
Figures 10a through 10c are the radiographs and MR image of a 65-year-old woman with rheumatoid arthritis who has posterior headaches, hand and gait clumsiness, and dizziness. What is the most likely diagnosis?



Explanation
Rheumatoid arthritis is a chronic inflammatory synovitis. The neck is a common site of involvement, after hands and feet. Fortunately, radiographic evidence of instability does not equal neurological deficits. The 3 most common cervical presentations are atlantoaxial subluxation, basilar invagination, and subaxial subluxation. Atlantoaxial subluxation is attributable to an incompetent transverse ligament or erosion of the dens. It is demonstrated by a widened anterior atlantodental interval. Basilar invagination is attributable to cranial settling with the tip of the dens pressing on the spinal cord or midbrain. Subaxial subluxation is attributable to the destabilization of the facet joints.
Basilar invagination symptoms can include posterior headaches, cervical myelopathy, dizziness, and sudden death from compression of the medulla oblongata. In this scenario, there is no subaxial or atlantoaxial subluxation or rheumatoid plaque.
RECOMMENDED READINGS
17. [Fujiwara K, Owaki H, Fujimoto M, Yonenobu K, Ochi T. A long-term follow-up study of cervical lesions in rheumatoid arthritis. J Spinal Disord. 2000 Dec;13(6):519-26. PubMed PMID: 11132984. ](http://www.ncbi.nlm.nih.gov/pubmed/11132984)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11132984)
18. Boden SD, Dodge LD, Bohlman HH, Rechtine GR. Rheumatoid arthritis of the cervical spine. A longterm analysis with predictors of paralysis and recovery. J Bone Joint Surg Am. 1993 Sep;75(9):1282-
[97/. PubMed PMID: 8408150. ](http://www.ncbi.nlm.nih.gov/pubmed/8408150)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8408150)
19. [Riew KD, Hilibrand AS, Palumbo MA, Sethi N, Bohlman HH. Diagnosing basilar invagination in the rheumatoid patient. The reliability of radiographic criteria. J Bone Joint Surg Am. 2001 Feb;83-A(2):194-200. PubMed PMID: 11216680. ](http://www.ncbi.nlm.nih.gov/pubmed/11216680)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11216680)
Basilar invagination symptoms can include posterior headaches, cervical myelopathy, dizziness, and sudden death from compression of the medulla oblongata. In this scenario, there is no subaxial or atlantoaxial subluxation or rheumatoid plaque.
RECOMMENDED READINGS
17. [Fujiwara K, Owaki H, Fujimoto M, Yonenobu K, Ochi T. A long-term follow-up study of cervical lesions in rheumatoid arthritis. J Spinal Disord. 2000 Dec;13(6):519-26. PubMed PMID: 11132984. ](http://www.ncbi.nlm.nih.gov/pubmed/11132984)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11132984)
18. Boden SD, Dodge LD, Bohlman HH, Rechtine GR. Rheumatoid arthritis of the cervical spine. A longterm analysis with predictors of paralysis and recovery. J Bone Joint Surg Am. 1993 Sep;75(9):1282-
[97/. PubMed PMID: 8408150. ](http://www.ncbi.nlm.nih.gov/pubmed/8408150)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8408150)
19. [Riew KD, Hilibrand AS, Palumbo MA, Sethi N, Bohlman HH. Diagnosing basilar invagination in the rheumatoid patient. The reliability of radiographic criteria. J Bone Joint Surg Am. 2001 Feb;83-A(2):194-200. PubMed PMID: 11216680. ](http://www.ncbi.nlm.nih.gov/pubmed/11216680)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11216680)
Question 18High Yield
Figure 90
Explanation
- Anterior interosseous nerve (AIN) palsy**
Question 19High Yield
The following skeletal feature helps to establish a diagnostic level of major skeletal involvement in Marfan syndrome:
Explanation
Pectus carinatum has a high diagnostic value for Marfan syndrome.
Hyperextension of the knees is not common in patients with Marfan syndrome. This skeletal feature is seen in many other conditions; therefore, it has low diagnostic specificity.
Atlantoaxial subluxation is rare in Marfan syndrome, but is common in some of the skeletal dysplasias.
Although patients with Marfan syndrome are generally tall, height is too nonspecific to be a helpful diagnostic criterion. Kyphosis is not a skeletal diagnostic criterion.
Hyperextension of the knees is not common in patients with Marfan syndrome. This skeletal feature is seen in many other conditions; therefore, it has low diagnostic specificity.
Atlantoaxial subluxation is rare in Marfan syndrome, but is common in some of the skeletal dysplasias.
Although patients with Marfan syndrome are generally tall, height is too nonspecific to be a helpful diagnostic criterion. Kyphosis is not a skeletal diagnostic criterion.
Question 20High Yield
What patient factor is predictive of better outcomes for surgical management of a displaced calcaneal fracture compared to nonsurgical management?
Explanation
A recent randomized trial of surgical versus nonsurgical management of calcaneal fractures showed that patients who were on workers’ compensation did poorly with surgical care. These patients had less favorable outcomes regardless of their initial management. Factors such as age, smoking, and vasculopathies compromise skin healing, leading to greater surgical risks. The best results were obtained in patients who are younger than age 40 years, have unilateral injuries and are injured during noncompensable activities. Women tend to do better with surgery than men.
REFERENCES: Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
REFERENCES: Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Question 21High Yield
Which of the following noncollagenous proteins aid in regulating the maturation of bone mineral crystals:
Explanation
Bone sialoproteins are important in the initiation of mineralization of collagen. They promote apatite nucleation and growth of the crystals. Osteocalcin (bone Gla protein) is important for mineral proliferation and maturation.
Note the role of promoters and inhibitors: Apatite nucleation and growth Promoters
Type I collagen Bone sialoprotein Matrix vesicles Phosphoproteins Proteolipids Biglycan
Inhibitors
Large proteoglycans Pyrophosphate Adenosine triphosphate Citrate
Mineral proliferation
Regulators
Osteocalcin Phosphoproteins Proteoglycans
Note the role of promoters and inhibitors: Apatite nucleation and growth Promoters
Type I collagen Bone sialoprotein Matrix vesicles Phosphoproteins Proteolipids Biglycan
Inhibitors
Large proteoglycans Pyrophosphate Adenosine triphosphate Citrate
Mineral proliferation
Regulators
Osteocalcin Phosphoproteins Proteoglycans
Question 22High Yield
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of
Explanation
Results of treatment of subscapularis rupture are best when immediate repair is performed. When the cause of the anterior instability is the result of rupture of the subscapularis tendon and the component position is acceptable, revising the position of the component is unnecessary. Restoring the coracoacromial arch and subacromial decompression are related to superior instability and rotator cuff pathology, respectively, and would not correct the instability caused by subscapularis rupture.
REFERENCES: Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
REFERENCES: Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 23High Yield
Which of the following is true regarding brace treatment for Scheuermann kyphosis:
Explanation
Brace treatment is effective for Scheuermann kyphosis. Unlike idiopathic scoliosis, permanent improvement of the deformity is the goal.
The Milwaukee brace is often indicated.
Brace treatment is ineffective for curves over 74°. The brace should be worn until skeletal maturity.
The Milwaukee brace is often indicated.
Brace treatment is ineffective for curves over 74°. The brace should be worn until skeletal maturity.
Question 24High Yield
Dexamethasone is a steroid. Long term use can result in osteoporosis.
A 20-year-old male sustains bilateral humeral shaft fractures and bilateral femoral shaft fractures from a motor vehicle collision. While awaiting surgery, the patient suddenly becomes tachycardic,
hypoxemic and experiences mental status changes; physical exam demonstrates multiple petechiae in his bilateral axilla. CT angiography is ordered and is negative for pulmonary embolus. What is the most likely diagnosis?
A 20-year-old male sustains bilateral humeral shaft fractures and bilateral femoral shaft fractures from a motor vehicle collision. While awaiting surgery, the patient suddenly becomes tachycardic,
hypoxemic and experiences mental status changes; physical exam demonstrates multiple petechiae in his bilateral axilla. CT angiography is ordered and is negative for pulmonary embolus. What is the most likely diagnosis?






Explanation
Strain is defined as the change in length/original length (L) and is created by a deformation of a material from an applied force.
The mechanical environment at the fracture site has a major influence on fracture healing. Granulation tissue can withstand higher strain, which stabilizes the mechanical environment and forms a scaffold on which cartilage and bone eventually form; this occurs after strain decreases incrementally. Optimal healing, however, depends on duration, rate, timing and type of mechanical influence. Bone is formed by osteoblasts that are adapted to the very low strains of over 1% change in length. Osteoblast synthesis and proliferation is stimulated at uniaxial strain of between 0.3% and 2.8%. It is known that limited inter-fragmentary movement of 0.2 mm to 1 mm is optimal for fracture
healing, resulting in promotion of callus and increase in rigidity. Excessive movement, on the other hand, prolongs fracture healing. Researchers have identified that tissue strain of 2% is suitable for primary
bone healing and secondary bone healing takes place at tissue strain of 2-
10%. Strain of 10-100% results in fibrous tissue formation and 100% strain to non-union. This is known as Perren's theory.
Stokes published a review article on the effects of stress on bone healing and growth, and notes the importance of the 'Hueter-Volkmann Law' (growth is retarded by increased mechanical compression, and accelerated by reduced loading in comparison with normal values) in bone growth. Stokes also notes that sustained compression of physiological magnitude inhibits growth by 40%
or more, while distraction increases growth rate by a much smaller amount.
Illustration A shows an example of a stress-strain curve, with several key definitions labeled on the diagram.
Incorrect Answers:
: This is the elastic limit or yield point.
Answer 3: The time-dependent deformations caused by creep and shrinkage have an Answer effect on the stiffness or modulus of an object.
Answer 4: This is the definition of force density. Answer 5: This is the definition of stress.
Which of the following materials is most susceptible to galvanic corrosion?
1) Titanium
2) Zirconia
3) Polyethylene
4) Cobalt-chromium
5) Alumina
Of the materials listed, cobalt-chromium is the only material that is most susceptible to galvanic corrosion. Galvanic corrosion is defined as intense localized electrochemical attack between two metal components exposed to
corrosive environments.
Incorrect Answers:
Answer 1: Titanium has less galvanic corrosion than cobalt-chromium alloys because it chemically protects itself by a reaction called self-passivation, which is the formation of a protective surface oxide.
Answer 2 & 5: Zirconia and alumina are both ceramics, and are immune to metallic galvanic corrosion.
Answer 3: Polyethylene is a plastic polymer which is also immune to metallic galvanic corrosion.
The sclerotome of the somites develops into what mature anatomical structure?
1) Autonomic nervous system
2) Dorsal muscles
3) Ventral muscles
4) Appendicular skeleton
5) Axial skeleton
The somites are mesodermal in origin; somites eventually form dermis (dermatome), skeletal muscle (myotome), sclerotome or cartilage, tendons, and endothelial cells. The sclerotome of the somites develops into the axial skeleton. The neural crest forms the peripheral nervous system, the lateral plate mesoderm becomes the dermis, and the dorsal myotome (epimere) becomes the dorsal muscles.
Illustration A depicts the sclerotome of the somites development into the vertebra. The nucleus pulposus forms from the notochord and the annulus fibrosus forms from the sclerotome.
All of the following antibiotics function by interfering with cell wall synthesis EXCEPT
1) Cefazolin
2) Penicillin G
3) Vancomycin
4) Imipenem
5) Gentamicin
Cephalosporins (cefazolin), penicillins, vancomycin, and imipenem function by interfering with cell wall synthesis. Gentamicin, an aminoglycoside, functions by inhibiting ribosomes and protein synthesis and does not affect cell wall synthesis.
The reference by Mader et al. is an instructional course lecture that reviews
the different mechanisms of antibiotics and their indications in musculoskeletal infections. Illustration A is a table showing common mechanisms of antibiotics.
What is the most common radiographic finding in reflex sympathetic dystrophy (RSD) or complex regional pain syndrome of the knee?
1) patella baja
2) patella alta
3) patella osteopenia
4) generalized osteopenia
5) supracondylar stress fracture
Reflex Sympathetic Dystrophy (RSD) of the knee is different than that of the upper extremity. Pain out of proportion to the initial injury is the hallmark symptom. Other features include vasomotor disturbances, delayed functional recovery and various associated trophic changes. The JAAOS article by Cooper et al states that patellar osteopenia "is the most common radiographic finding". However, they go on to state that the most reliable diagnostic test is symptom relief after sympathetic blockade. The JBJS article by Cooper et al treated 14 patients with RSD of the knee with epidural blocks for 4 days. Eleven patients had complete resolution of their symptoms, and pain that was out of proportion to the severity of the injury was the most consistent finding. Katz et al reviewed 36 patients with RSD primarily affecting the knee. They found that injuries or operation about the patellofemoral joint triggered its onset in 64% of patients.
Tumor necrosis factor receptor 1 is involved in which of the following cellular events?
1) Replication
2) Agenesis
3) Apoptosis
4) Senescence
5) Ectopy
Apoptosis is defined as a sequence of events leading to programmed cell death. A cell undergoing apoptosis goes through a series of signaling events in which the cell disposes of itself in a neat and orderly manner. This is in contrast to cell lysis where the cell is destroyed, releasing its contents (including harmful enzymes) and DNA material which is toxic to neighboring cells.
Ashkenazi et al present a review of apoptosis, including the biochemical mechanism behind the programming. They note that the death receptors Fas and tumor necrosis factor receptor 1 (TNFR1) trigger apoptosis upon engagement by their cognate death ligands.
Illustration A shows a diagram of apoptosis, including the cellular mechanisms.
The Stark II regulations limit which of the following activities for physicians who accept Medicare and/or Medicaid insurance payments?
1) Direct use of implant manufacturer financial support for non-CME courses
2) Use of in-office durable medical equipment for patient care
3) Physician office space rental at fair market value prices
4) Direct physician employment by a hospital system
5) Referral of patients to entities in which the physician has a financial relationship
On Jan. 3, 2001, the United States Department of Health and Human Services (HHS) released the first phase of its long-anticipated final regulations addressing self-referrals by physicians. These regulations clarify self-referral prohibitions under section 1877 of the Social Security Act, often referred to as the "Stark law," which bar physicians from making referrals to entities in which the physician has a financial relationship, and for which no statutory exception applies. Stark II presently provides for civil money penalties not to exceed
$100,000 for each "arrangement or scheme" that a person knows or should know has a principal purpose to violate the statute. Additionally, the government may withhold payments for prohibited referrals or seek to recoup past payments.
Which of the following statements best describes a plasmid?
1) An extrachromosomal, circular piece of DNA that replicates independently of host DNA
2) An extrachromosomal, linear piece of RNA which replicates independently of host DNA
3) A protein which promotes transcription of DNA to RNA
4) A gene which leads to cancerous cell transformation
5) A gene which suppresses cancerous cell transformation
A plasmid is an extrachromosomal circular piece of DNA that replicates independently of host DNA.
In nature, plasmids frequently carry genes that may benefit the survival of the organism, such as antibiotic resistance genes. Artificially, plasmids are frequently used as vectors to introduce genes into a cell and change genetic expression. This has potential therapeutic benefits for the treatment of
arthritis and bone healing.
Whalen et al. discuss various methods for transferring therapeutic genes into an arthritic joint. These include gene transfer through a vector inserted directly into a joint, and indirect transfer where synovial cells are isolated and genetically modified using vectors, then transplanted back into the joint.
Lieberman et al. present a review discussing the potential future benefits of gene transfer in bone healing, spine fusion, and articular cartilage repair.
Illustration A shows a visual representation of a plasmid. Note how the plasmid is extrachromosomal and the structure is identical to that of the host DNA. Video V is an educational video that gives an overview on plasmids.
Incorrect Answers:
Answer 2: A plasmid is a small piece of DNA, not RNA. Answer 3: This defines a trancription factor.
Answer 4: This defines an oncogene.
Answer 5: This defines a tumor suppressor gene.
An 18-year-old female soccer player sustains a non-contact deceleration injury while making a sharp pivot to strike the ball. She hears a loud pop in her knee, is unable to bear weight initially following the injury, and develops an immediate knee effusion. The structure most likely injured in this athlete exhibits all of the following biomechanical properties EXCEPT:
1) Viscoelasticity
2) Creep
3) Isotropism
4) Stress relaxation
5) Nonlinear elasticity
The clinical presentation is consistent for an ACL tear. The ACL has the biomechanical properties of viscoelasticity, creep, stress relaxation, and nonlinear elasticity. It does NOT demonstrate isotropism. Isotropic materials such as metals exhibit the same mechanical properties in all directions.
All ligaments and tendons are anisotropic and exhibit different mechanical properties depending on the direction of the applied load. Ligaments are viscoelastic indicating they exhibit a time-dependent mechanical behavior. Thus, the relationship between stress and strain is not constant but depends on the time of displacement or load. One characteristic of viscoelasticity is creep, whereby there is an increasing deformation under constant load. Viscoelastic materials also exhibit stress relaxation whereby stress will be reduced or will relax under a constant deformation. Ligaments also demonstrate nonlinear elasticity (see illustration paragraph below).
Screen et al. studied viscoelasticity within isolated tendon fascicles. Their results provide further evidence of the complex anisotropic and viscoelastic nature of tendons. They conclude proteoglycans play an important functional role in controlling the viscoelastic behaviour and the mechanisms of strain transfer within tendon.
Illustration A demonstrates, nonlinear elasticity, which is another characteristic of ligaments. The toe region (labeled A in Illustration A) represents "un- crimping" of the crimp in the collagen fibrils. Since it is easier to stretch out
the crimp of the collagen fibrils, this part of the stress strain curve (the "toe region") shows a relatively low stiffness. As the collagen fibrils become uncrimped, the collagen fibril backbone itself is being stretched (labeled B in Illustration A), which gives rise to a stiffer material. As individual fibrils within the ligament or tendon begin to fail damage accumulates, stiffness is reduced and the ligament/tendons begins to fail (labeled C in Illustration A).
All of the following are desired goals of improved diversity and cultural competence in orthopaedics EXCEPT:
1) Understand cultural differences so that patient-physician relationships are enhanced
2) Reduce disparities in healthcare
3) Establishment of quotas for minority and female medical students
4) Access to orthopaedic care is optimized
5) Better serve the nation's diverse population
There are no plans to create quotas in the residency match selection process. The referenced article by White is a symposium on the need for diversity within orthopaedic surgery.
The AAOS has established goals for diversity in an effort to enhance the patient and physician relationship, eliminate disparities in healthcare, and optimize access to orthopaedic care. The AAOS The Diversity Committee endeavors to significantly improve minority and female access to the orthopaedic profession and more information can be found at the referenced academy website (www3.aaos.org/about/diversity/cul_recr.cfm)
What is the most important factor when choosing an optimal lower limb prosthesis for an adult patient?
1) Prosthesis cost
2) Patient comorbidities
3) Patient functional status
4) Patient gender
5) Patient age
The most important factor when choosing an optimal lower limb prosthesis for an adult patient is the current and potential functional requirements of the patient.
Pinzur reviewed 90 patients treated with lower extremity amputations for peripheral vascular insufficiency and found the current and potential functional status of the patient were more important than any other factor in creating the best lower limb prosthesis for the patient.
A 28-year-old marathon runner has a knee MRI done to evaluate medial sided knee pain. No meniscus tear is identified, but the**
**articular cartilage of the femoral condyles is noted to be twice as thick as normal values. What is the most likely cause of this finding?
1) Osteoarthritis
2) Undiagnosed osteopetrosis
3) Synovial cytokine sensitization due to excess running
4) Extra-articular hydrostatic pressure changes
5) Chondrocyte modulation via mechanotransduction
Chondrocyte modulation via mechanotransduction secondary to excess load is a known cause for alterations in the cellular structure of articular cartilage. Specifically, chondrocyte metabolism responds to both mechanical (mechanical load, hydrostatic pressure change) and chemical stimuli (growth factors, cytokines). It is known that articular cartilage remodels quickly following alterations of mechanical stimuli to the tissue in vivo, and can change its metabolic activities in vitro. As such, generalized thickening of articular cartilage in a marathon runner is most likely secondary to the increased mechanotransduction from repeated load.
Incorrect answers:
Strain is defined as the change in length/original length (L) and is created by a deformation of a material from an applied force.
The mechanical environment at the fracture site has a major influence on fracture healing. Granulation tissue can withstand higher strain, which stabilizes the mechanical environment and forms a scaffold on which cartilage and bone eventually form; this occurs after strain decreases incrementally. Optimal healing, however, depends on duration, rate, timing and type of mechanical influence. Bone is formed by osteoblasts that are adapted to the very low strains of over 1% change in length. Osteoblast synthesis and proliferation is stimulated at uniaxial strain of between 0.3% and 2.8%. It is known that limited inter-fragmentary movement of 0.2 mm to 1 mm is optimal for fracture
healing, resulting in promotion of callus and increase in rigidity. Excessive movement, on the other hand, prolongs fracture healing. Researchers have identified that tissue strain of 2% is suitable for primary
bone healing and secondary bone healing takes place at tissue strain of 2-
10%. Strain of 10-100% results in fibrous tissue formation and 100% strain to non-union. This is known as Perren's theory.
Stokes published a review article on the effects of stress on bone healing and growth, and notes the importance of the 'Hueter-Volkmann Law' (growth is retarded by increased mechanical compression, and accelerated by reduced loading in comparison with normal values) in bone growth. Stokes also notes that sustained compression of physiological magnitude inhibits growth by 40%
or more, while distraction increases growth rate by a much smaller amount.
Illustration A shows an example of a stress-strain curve, with several key definitions labeled on the diagram.
Incorrect Answers:
: This is the elastic limit or yield point.
Answer 3: The time-dependent deformations caused by creep and shrinkage have an Answer effect on the stiffness or modulus of an object.
Answer 4: This is the definition of force density. Answer 5: This is the definition of stress.
Which of the following materials is most susceptible to galvanic corrosion?
1) Titanium
2) Zirconia
3) Polyethylene
4) Cobalt-chromium
5) Alumina
Of the materials listed, cobalt-chromium is the only material that is most susceptible to galvanic corrosion. Galvanic corrosion is defined as intense localized electrochemical attack between two metal components exposed to
corrosive environments.
Incorrect Answers:
Answer 1: Titanium has less galvanic corrosion than cobalt-chromium alloys because it chemically protects itself by a reaction called self-passivation, which is the formation of a protective surface oxide.
Answer 2 & 5: Zirconia and alumina are both ceramics, and are immune to metallic galvanic corrosion.
Answer 3: Polyethylene is a plastic polymer which is also immune to metallic galvanic corrosion.
The sclerotome of the somites develops into what mature anatomical structure?
1) Autonomic nervous system
2) Dorsal muscles
3) Ventral muscles
4) Appendicular skeleton
5) Axial skeleton
The somites are mesodermal in origin; somites eventually form dermis (dermatome), skeletal muscle (myotome), sclerotome or cartilage, tendons, and endothelial cells. The sclerotome of the somites develops into the axial skeleton. The neural crest forms the peripheral nervous system, the lateral plate mesoderm becomes the dermis, and the dorsal myotome (epimere) becomes the dorsal muscles.
Illustration A depicts the sclerotome of the somites development into the vertebra. The nucleus pulposus forms from the notochord and the annulus fibrosus forms from the sclerotome.
All of the following antibiotics function by interfering with cell wall synthesis EXCEPT
1) Cefazolin
2) Penicillin G
3) Vancomycin
4) Imipenem
5) Gentamicin
Cephalosporins (cefazolin), penicillins, vancomycin, and imipenem function by interfering with cell wall synthesis. Gentamicin, an aminoglycoside, functions by inhibiting ribosomes and protein synthesis and does not affect cell wall synthesis.
The reference by Mader et al. is an instructional course lecture that reviews
the different mechanisms of antibiotics and their indications in musculoskeletal infections. Illustration A is a table showing common mechanisms of antibiotics.
What is the most common radiographic finding in reflex sympathetic dystrophy (RSD) or complex regional pain syndrome of the knee?
1) patella baja
2) patella alta
3) patella osteopenia
4) generalized osteopenia
5) supracondylar stress fracture
Reflex Sympathetic Dystrophy (RSD) of the knee is different than that of the upper extremity. Pain out of proportion to the initial injury is the hallmark symptom. Other features include vasomotor disturbances, delayed functional recovery and various associated trophic changes. The JAAOS article by Cooper et al states that patellar osteopenia "is the most common radiographic finding". However, they go on to state that the most reliable diagnostic test is symptom relief after sympathetic blockade. The JBJS article by Cooper et al treated 14 patients with RSD of the knee with epidural blocks for 4 days. Eleven patients had complete resolution of their symptoms, and pain that was out of proportion to the severity of the injury was the most consistent finding. Katz et al reviewed 36 patients with RSD primarily affecting the knee. They found that injuries or operation about the patellofemoral joint triggered its onset in 64% of patients.
Tumor necrosis factor receptor 1 is involved in which of the following cellular events?
1) Replication
2) Agenesis
3) Apoptosis
4) Senescence
5) Ectopy
Apoptosis is defined as a sequence of events leading to programmed cell death. A cell undergoing apoptosis goes through a series of signaling events in which the cell disposes of itself in a neat and orderly manner. This is in contrast to cell lysis where the cell is destroyed, releasing its contents (including harmful enzymes) and DNA material which is toxic to neighboring cells.
Ashkenazi et al present a review of apoptosis, including the biochemical mechanism behind the programming. They note that the death receptors Fas and tumor necrosis factor receptor 1 (TNFR1) trigger apoptosis upon engagement by their cognate death ligands.
Illustration A shows a diagram of apoptosis, including the cellular mechanisms.
The Stark II regulations limit which of the following activities for physicians who accept Medicare and/or Medicaid insurance payments?
1) Direct use of implant manufacturer financial support for non-CME courses
2) Use of in-office durable medical equipment for patient care
3) Physician office space rental at fair market value prices
4) Direct physician employment by a hospital system
5) Referral of patients to entities in which the physician has a financial relationship
On Jan. 3, 2001, the United States Department of Health and Human Services (HHS) released the first phase of its long-anticipated final regulations addressing self-referrals by physicians. These regulations clarify self-referral prohibitions under section 1877 of the Social Security Act, often referred to as the "Stark law," which bar physicians from making referrals to entities in which the physician has a financial relationship, and for which no statutory exception applies. Stark II presently provides for civil money penalties not to exceed
$100,000 for each "arrangement or scheme" that a person knows or should know has a principal purpose to violate the statute. Additionally, the government may withhold payments for prohibited referrals or seek to recoup past payments.
Which of the following statements best describes a plasmid?
1) An extrachromosomal, circular piece of DNA that replicates independently of host DNA
2) An extrachromosomal, linear piece of RNA which replicates independently of host DNA
3) A protein which promotes transcription of DNA to RNA
4) A gene which leads to cancerous cell transformation
5) A gene which suppresses cancerous cell transformation
A plasmid is an extrachromosomal circular piece of DNA that replicates independently of host DNA.
In nature, plasmids frequently carry genes that may benefit the survival of the organism, such as antibiotic resistance genes. Artificially, plasmids are frequently used as vectors to introduce genes into a cell and change genetic expression. This has potential therapeutic benefits for the treatment of
arthritis and bone healing.
Whalen et al. discuss various methods for transferring therapeutic genes into an arthritic joint. These include gene transfer through a vector inserted directly into a joint, and indirect transfer where synovial cells are isolated and genetically modified using vectors, then transplanted back into the joint.
Lieberman et al. present a review discussing the potential future benefits of gene transfer in bone healing, spine fusion, and articular cartilage repair.
Illustration A shows a visual representation of a plasmid. Note how the plasmid is extrachromosomal and the structure is identical to that of the host DNA. Video V is an educational video that gives an overview on plasmids.
Incorrect Answers:
Answer 2: A plasmid is a small piece of DNA, not RNA. Answer 3: This defines a trancription factor.
Answer 4: This defines an oncogene.
Answer 5: This defines a tumor suppressor gene.
An 18-year-old female soccer player sustains a non-contact deceleration injury while making a sharp pivot to strike the ball. She hears a loud pop in her knee, is unable to bear weight initially following the injury, and develops an immediate knee effusion. The structure most likely injured in this athlete exhibits all of the following biomechanical properties EXCEPT:
1) Viscoelasticity
2) Creep
3) Isotropism
4) Stress relaxation
5) Nonlinear elasticity
The clinical presentation is consistent for an ACL tear. The ACL has the biomechanical properties of viscoelasticity, creep, stress relaxation, and nonlinear elasticity. It does NOT demonstrate isotropism. Isotropic materials such as metals exhibit the same mechanical properties in all directions.
All ligaments and tendons are anisotropic and exhibit different mechanical properties depending on the direction of the applied load. Ligaments are viscoelastic indicating they exhibit a time-dependent mechanical behavior. Thus, the relationship between stress and strain is not constant but depends on the time of displacement or load. One characteristic of viscoelasticity is creep, whereby there is an increasing deformation under constant load. Viscoelastic materials also exhibit stress relaxation whereby stress will be reduced or will relax under a constant deformation. Ligaments also demonstrate nonlinear elasticity (see illustration paragraph below).
Screen et al. studied viscoelasticity within isolated tendon fascicles. Their results provide further evidence of the complex anisotropic and viscoelastic nature of tendons. They conclude proteoglycans play an important functional role in controlling the viscoelastic behaviour and the mechanisms of strain transfer within tendon.
Illustration A demonstrates, nonlinear elasticity, which is another characteristic of ligaments. The toe region (labeled A in Illustration A) represents "un- crimping" of the crimp in the collagen fibrils. Since it is easier to stretch out
the crimp of the collagen fibrils, this part of the stress strain curve (the "toe region") shows a relatively low stiffness. As the collagen fibrils become uncrimped, the collagen fibril backbone itself is being stretched (labeled B in Illustration A), which gives rise to a stiffer material. As individual fibrils within the ligament or tendon begin to fail damage accumulates, stiffness is reduced and the ligament/tendons begins to fail (labeled C in Illustration A).
All of the following are desired goals of improved diversity and cultural competence in orthopaedics EXCEPT:
1) Understand cultural differences so that patient-physician relationships are enhanced
2) Reduce disparities in healthcare
3) Establishment of quotas for minority and female medical students
4) Access to orthopaedic care is optimized
5) Better serve the nation's diverse population
There are no plans to create quotas in the residency match selection process. The referenced article by White is a symposium on the need for diversity within orthopaedic surgery.
The AAOS has established goals for diversity in an effort to enhance the patient and physician relationship, eliminate disparities in healthcare, and optimize access to orthopaedic care. The AAOS The Diversity Committee endeavors to significantly improve minority and female access to the orthopaedic profession and more information can be found at the referenced academy website (www3.aaos.org/about/diversity/cul_recr.cfm)
What is the most important factor when choosing an optimal lower limb prosthesis for an adult patient?
1) Prosthesis cost
2) Patient comorbidities
3) Patient functional status
4) Patient gender
5) Patient age
The most important factor when choosing an optimal lower limb prosthesis for an adult patient is the current and potential functional requirements of the patient.
Pinzur reviewed 90 patients treated with lower extremity amputations for peripheral vascular insufficiency and found the current and potential functional status of the patient were more important than any other factor in creating the best lower limb prosthesis for the patient.
A 28-year-old marathon runner has a knee MRI done to evaluate medial sided knee pain. No meniscus tear is identified, but the**
**articular cartilage of the femoral condyles is noted to be twice as thick as normal values. What is the most likely cause of this finding?
1) Osteoarthritis
2) Undiagnosed osteopetrosis
3) Synovial cytokine sensitization due to excess running
4) Extra-articular hydrostatic pressure changes
5) Chondrocyte modulation via mechanotransduction
Chondrocyte modulation via mechanotransduction secondary to excess load is a known cause for alterations in the cellular structure of articular cartilage. Specifically, chondrocyte metabolism responds to both mechanical (mechanical load, hydrostatic pressure change) and chemical stimuli (growth factors, cytokines). It is known that articular cartilage remodels quickly following alterations of mechanical stimuli to the tissue in vivo, and can change its metabolic activities in vitro. As such, generalized thickening of articular cartilage in a marathon runner is most likely secondary to the increased mechanotransduction from repeated load.
Incorrect answers:
Question 25High Yield
Which distal biceps repair technique has the highest load to failure in vitro?
Explanation
- Suspensory cortical button (Endobutton)_
Question 26High Yield
An 18-year-old high school football player exits the field after making a tackle on the opening kickoff. He reports “feeling out of it” and states that he has a headache. He does not recall any loss of consciousness and has no amnesia. He is unable to list the months of the year in reverse order on questioning. He does not return to the game and feels normal at the completion of the game. What is the most sensitive test in assessing deficits after mild traumatic brain injury?

Explanation
DISCUSSION: Most imaging studies in mild traumatic brain injury will be normal. Neuropsychologic testing is the most sensitive test in assessing mild deficits after traumatic brain injury. Sideline assessment is important but less sensitive in assessing deficits. The precise role of neuropsychologic testing in determining return to play has not been fully defined.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 37-38.
62 • American Academy of Orthopaedic Surgeons
Maroon JC, Lovell MR, Norwig J, et al: Cerebral concussion in athletics: Evaluation and neuropsychological testing. Neurosurgery 2000;47:659-672.
Figure 79
DISCUSSION: Most imaging studies in mild traumatic brain injury will be normal. Neuropsychologic testing is the most sensitive test in assessing mild deficits after traumatic brain injury. Sideline assessment is important but less sensitive in assessing deficits. The precise role of neuropsychologic testing in determining return to play has not been fully defined.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 37-38.
62 • American Academy of Orthopaedic Surgeons
Maroon JC, Lovell MR, Norwig J, et al: Cerebral concussion in athletics: Evaluation and neuropsychological testing. Neurosurgery 2000;47:659-672.
Figure 79
Question 27High Yield
A 6-year-old child suffers a displaced fracture of the distal humerus in the supracondylar region. Neurologic and vascular exams are normal. The surgeon decides to reduce and pin the fracture. Which of the following risks increases if the procedure is delayed more than 8 hours?
Explanation
A retrospective comparison study has shown no increase of risks in delayed treatment of supracondylar fractures.
Question 28High Yield
If surgery is chosen, what is the optimum procedure?
Explanation
- Costotransversectomy with posterior instrumentation
Question 29High Yield
-How is the fracture pattern shown in Figures 76a through 76c best classified?

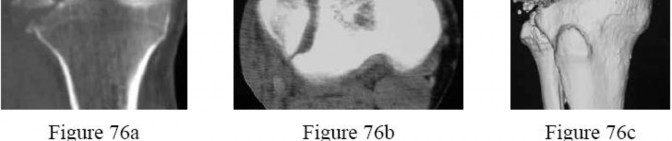
Explanation
No detailed explanation provided for this question.
Question 30High Yield
When conducted at near physiologic strain rates, tensile studies of the inferior glenohumeral ligament (IGHL) have shown that the
Explanation
Tensile testing of the inferior glenohumeral ligament at near physiologic strain rates has shown that the anterior band of the IGHL has the greatest stiffness of the three ligament regions and the glenoid insertion site shows greater strain than the ligament midsubstance.
REFERENCES: Bigliani LU, Pollock RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Ticker JB, Bigliani LU, Soslowsky LJ, Pawluk RJ, Flatow EL, Mow VC: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
REFERENCES: Bigliani LU, Pollock RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Ticker JB, Bigliani LU, Soslowsky LJ, Pawluk RJ, Flatow EL, Mow VC: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Question 31High Yield
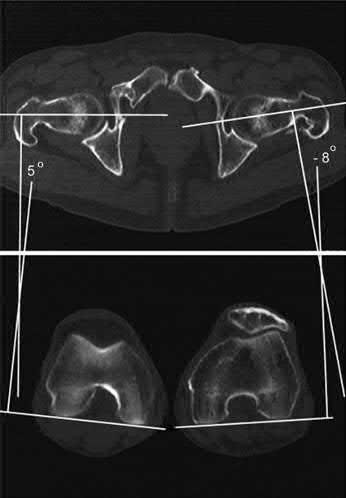
A radiologist uses CT scans to perform research on rotational malalignment of femoral shaft fractures treated with intramedullary nailing. He determines the angle between a line drawn tangential to the femoral condyles and a line drawn through the axis of the femoral neck. He does this for both the injured and uninjured sides. In Figure A, what malalignment is present for the injured left side compared with the uninjured right side?
Explanation
There is external malrotation of 13°.
Rotational malalignment arises after closed intramedullary nailing because anatomical reduction is achieved indirectly, resulting in less rotational control
compared with plate fixation. Rotational malalignment can be expressed as a difference in femoral anteversion between the injured and uninjured legs.
Jaarsma et al. reviewed rotational malalignment of femur fractures. They found that clinical assessment is inaccurate compared with CT measurement (±21°). Using CT measurement, they found the incidence of significant (=>15°) malrotation after IM nailing to be 20-30%. External malrotational leads to more symptoms than internal malrotation. Larger angles of malrotation (>15°) are more symptomatic. Complications of malrotation include degenerative arthritis of the hip and knee.
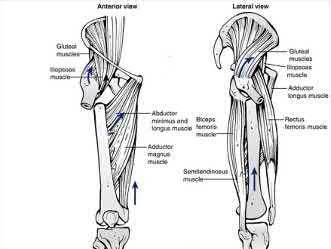
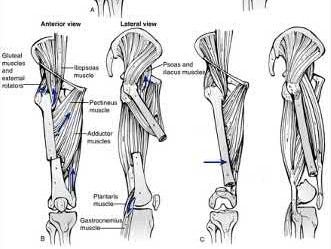
Figure A shows change in internal rotation of -8°-5°= -13°, giving 13° of external malrotation. Illustration A shows muscular attachments that contribute to rotational malalignment. In proximal fractures, the proximal fragment rotates externally (action of the glutei, iliopsoas and hip external rotators), producing internal malrotation. In distal fractures, the distal fragment rotates externally (action of the plantaris and lateral gastrocnemius), producing external malrotation.
Incorrect Answers:
Answers 1, 3, 4, 5: CT-torsion measurements show external malrotation of
13°.
Rotational malalignment arises after closed intramedullary nailing because anatomical reduction is achieved indirectly, resulting in less rotational control
compared with plate fixation. Rotational malalignment can be expressed as a difference in femoral anteversion between the injured and uninjured legs.
Jaarsma et al. reviewed rotational malalignment of femur fractures. They found that clinical assessment is inaccurate compared with CT measurement (±21°). Using CT measurement, they found the incidence of significant (=>15°) malrotation after IM nailing to be 20-30%. External malrotational leads to more symptoms than internal malrotation. Larger angles of malrotation (>15°) are more symptomatic. Complications of malrotation include degenerative arthritis of the hip and knee.
Figure A shows change in internal rotation of -8°-5°= -13°, giving 13° of external malrotation. Illustration A shows muscular attachments that contribute to rotational malalignment. In proximal fractures, the proximal fragment rotates externally (action of the glutei, iliopsoas and hip external rotators), producing internal malrotation. In distal fractures, the distal fragment rotates externally (action of the plantaris and lateral gastrocnemius), producing external malrotation.
Incorrect Answers:
Answers 1, 3, 4, 5: CT-torsion measurements show external malrotation of
13°.
Question 32High Yield
When performing an arthroscopic Bankart repair in the lateral decubitus position, a surgeon notes a patulous capsule and a very lax anterior band of the inferior glenohumeral ligament. The surgeon decides that in addition to simply repairing the torn labrum, a capsular shift should be performed. The surgeon instructs the fellow assisting to take a “nice, big bite” of the capsule in this region to tighten the capsule upon repair. Which postoperative complication is most likely a result of this maneuver?
Explanation
The axillary nerve is at most risk in this area of the glenohumeral joint as it passes adjacent to and just inferior to the 6 o’clock position. Although performing capsular shifts within and up to 1 cm from the glenoid rim is generally considered safe, taking large amounts of capsule (>1 cm) in this region in an effort to tighten the capsule can inadvertently damage the nerve as it crosses there.
The musculocutaneous nerve does not cross in this region, although it can be injured during dissection around the coracoid, such as in arthroscopic Latarjet procedures. The musculocutaneous nerve branches to the lateral cutaneous nerve and provides sensory innervation to the lateral aspect of the forearm.
70
The suprascapular nerve crosses superior and posterior to the glenoid and is at greatest risk during transglenoid screw placement in the anteroposterior directions. The suprascapular nerve innervates the supraspinatus and the infraspinatus. The radial nerve courses behind the humeral shaft and can be damaged during bicortical fixation in the anterior to posterior direction in this region. A radial nerve palsy would result in wrist extension weakness.
The musculocutaneous nerve does not cross in this region, although it can be injured during dissection around the coracoid, such as in arthroscopic Latarjet procedures. The musculocutaneous nerve branches to the lateral cutaneous nerve and provides sensory innervation to the lateral aspect of the forearm.
70
The suprascapular nerve crosses superior and posterior to the glenoid and is at greatest risk during transglenoid screw placement in the anteroposterior directions. The suprascapular nerve innervates the supraspinatus and the infraspinatus. The radial nerve courses behind the humeral shaft and can be damaged during bicortical fixation in the anterior to posterior direction in this region. A radial nerve palsy would result in wrist extension weakness.
Question 33High Yield
Figures 1 and 2 are the radiograph and MRI scan of a 16-year-old boy who injured his right knee by a lateral side impact while playing football. The MRI indicates what structure was most likely injured?


Explanation
This is a rupture of the anterolateral ligament complex and a portion of the IT band. This injury is highly correlated with a complete ACL injury. In the MRI, the curvilinear or elliptic bone fragment (Segond fracture) projected parallel to the lateral aspect of the tibial plateau, the lateral capsular sign, is seen. The lateral capsular sign is also associated with ACL tears. Thus, this is an MRI showing a complete ACL _tear._
Question 34High Yield
A 27-year-old male competitive soccer player reports a 1-year history of pain in the adductor region that has prevented him from playing. Examination reveals tenderness about the adductor attachment to the pelvis, and pain at the same site with resisted contraction of the adductors. There is no tenderness over the hip joint and no signs of a sports hernia. Radiographs are normal. MRI does not show any evidence of enthesopathy. What is the next best step in management?
Explanation
DISCUSSION: Schilders and associates reported their results of treating adductor-related groin pain in competitive athletes. They reported that a single corticosteroid injection into the pubic cleft can be expected to provide at least 1 year of relief of adductor-related groin pain in a competitive athlete with normal findings on MRI. In contrast, when there is evidence of enthesopathy on MRI in this competitive- athlete population, these injections are not therapeutic and are associated with a high likelihood of recurrence of symptoms. Hip arthroscopy is generally reserved for intra-articular problems. Percutaneous adductor tenotomy is not indicated for this condition. A bone scan is unlikely to provide any useful information for clinical decision-making. Rheumatology consultation is also not indicated in the absence of any evidence of inflammatory arthropathy.
REFERENCES: Schilders E, Bismil Q, Robinson P, et al: Adductor-related groin pain in competitive athletes: Role of adductor enthesis, magnetic resonance imaging, and entheseal pubic cleft injections. J Bone Joint Surg Am 2007;89:2173-2178.
Robinson P, Barron DA, Parsons W, et al: Adductor-related groin pain in athletes: Correlation of MR imaging with clinical findings. Skelet Radiol 2004;33:451-457.
DISCUSSION: Schilders and associates reported their results of treating adductor-related groin pain in competitive athletes. They reported that a single corticosteroid injection into the pubic cleft can be expected to provide at least 1 year of relief of adductor-related groin pain in a competitive athlete with normal findings on MRI. In contrast, when there is evidence of enthesopathy on MRI in this competitive- athlete population, these injections are not therapeutic and are associated with a high likelihood of recurrence of symptoms. Hip arthroscopy is generally reserved for intra-articular problems. Percutaneous adductor tenotomy is not indicated for this condition. A bone scan is unlikely to provide any useful information for clinical decision-making. Rheumatology consultation is also not indicated in the absence of any evidence of inflammatory arthropathy.
REFERENCES: Schilders E, Bismil Q, Robinson P, et al: Adductor-related groin pain in competitive athletes: Role of adductor enthesis, magnetic resonance imaging, and entheseal pubic cleft injections. J Bone Joint Surg Am 2007;89:2173-2178.
Robinson P, Barron DA, Parsons W, et al: Adductor-related groin pain in athletes: Correlation of MR imaging with clinical findings. Skelet Radiol 2004;33:451-457.
Question 35High Yield
Which of the following is the function of fibroblast growth factor receptor 3 (FGFR3):
Explanation
Fibroblast growth factor receptor 3 regulates bone growth by limiting enchondral ossification. The other responses refer to:
C artilage oligomeric matrix protein (C OMP): C artilage cell proliferation and migration (through calcium-dependent proteoglycan binding)
Diastrophic dysplasia sulfate transporter gene (DTDST): Transport of sulfate into cells; needed for proteoglycan production
Fibrillin (FBN1): Formation of structural glycoprotein (fibrillin) for elastin-containing micro-fibrils
Neurofibromin (NF-1) - tumor suppressor gene to control cell growth and differentiation; negatively regulates the gene RAS
o RAS causes cell proliferation
C orrect Answer: Regulates bone growth by limiting enchondral ossification
C artilage oligomeric matrix protein (C OMP): C artilage cell proliferation and migration (through calcium-dependent proteoglycan binding)
Diastrophic dysplasia sulfate transporter gene (DTDST): Transport of sulfate into cells; needed for proteoglycan production
Fibrillin (FBN1): Formation of structural glycoprotein (fibrillin) for elastin-containing micro-fibrils
Neurofibromin (NF-1) - tumor suppressor gene to control cell growth and differentiation; negatively regulates the gene RAS
o RAS causes cell proliferation
C orrect Answer: Regulates bone growth by limiting enchondral ossification
Question 36High Yield
A 14-year-old boy is seen for back pain. Radiographic evaluation reveals a grade III isthmic spondylolisthesis. What measurement is most useful in predicting the likelihood of progression?

Explanation
DISCUSSION: Slip angle has been shown to be highly predictive of the risk for increased slippage in patients with spondylolisthesis. None of the other radiographic parameters listed has been shown to be predictive of the risk for increased slippage.
REFERENCES: Huang RP, Bohlman HH, Thompson GH, et al: Predictive value of pelvic incidence in progression of spondylolisthesis. Spine 2003;28:2381-2385.
Mac-Thiong JM, Wang Z, de Guise JA, et al: Postural model of sagittal spino-pelvic alignment and its relevance for lumbosacral developmental spondylolisthesis. Spine 2008;33:2316-2325.
**2010 Pediatric Orthopaedic Examination Answer Book • 23**
Figure 22a Figure 22b
REFERENCES: Huang RP, Bohlman HH, Thompson GH, et al: Predictive value of pelvic incidence in progression of spondylolisthesis. Spine 2003;28:2381-2385.
Mac-Thiong JM, Wang Z, de Guise JA, et al: Postural model of sagittal spino-pelvic alignment and its relevance for lumbosacral developmental spondylolisthesis. Spine 2008;33:2316-2325.
**2010 Pediatric Orthopaedic Examination Answer Book • 23**
Figure 22a Figure 22b
Question 37High Yield
A 55-year-old woman develops posttraumatic arthritis in the elbow following a distal humerus fracture. What is the most likely mid-term (5-
10 years after surgery) complication following semiconstrained total elbow arthroplasty (TEA)?
10 years after surgery) complication following semiconstrained total elbow arthroplasty (TEA)?
Explanation
TEA has been described for posttraumatic arthritis of the elbow and typically involves a young patient population with multiple previous operations on the affected elbow. Morrey and Schneeberger found aseptic component loosening to be uncommon (<10% of patients) and usually occurring >10 years after surgery. Prosthetic fracture, usually of the ulnar component, is also a late-term finding. Infection is the most common mode of early failure but usually occurs within the first 5 years and has an overall rate of approximately 5%. Bushing wear has been reported as the most common cause of mechanical TEA failure in this population at intermediate-term follow-up.
Question 38High Yield
A 90-year-old female slips and falls at home. She is a community ambulator and has no medical problems. She reports right hip pain at this time. Injury radiographs are shown in Figures A & B. Delay of more than 48 hours may result in:



Explanation
Figures A & B demonstrate a right, unstable intertrochanteric femur fracture. Surgical stabilization within 48 hours improves short-term and 30-day mortality.
Hip fractures are common and mortality rates vary. In the elderly, mortality rates may reach 10% at 1-month, 20% at 4-months, and 30% at 1-year. Time to surgery has found to be a decisive factor. A pre-operative delay may lead to an increase in mortality and adversely influence other clinical outcomes.
Clinical guidelines recommend immediate operative stabilization, given the patient is medically fit for surgery.
Nyholm et al. performed a retrospective study of the Danish Fracture Database to investigate whether a surgical delay increases 30-day and 90-day mortality rates for patients with proximal femoral fractures. The 30-day and 90-day mortalities were 10.8% and 17.4%, respectively. The risk of 30-day mortality increased with increasing time intervals of more than 12 hours, 24 hours, and more than 48 hours. 90-day mortality increased with a surgical delay of more than 24 hours. They conclude that rapid surgical treatment should be performed by attending orthopaedic surgeons.
Moja et al. performed a meta-analysis and meta-regression to assess the relationship between surgical delay and mortality in elderly patients with a hip fracture. They analyzed 35 independent studies with 191,873 patients and 34,448 deaths. The majority of studies had a cut-off of 48 hours. They report that early hip surgery was associated with a lower risk of death and pressure sores. They conclude that early hip fracture surgery appears to provide a survival benefit compared to later intervention.
Rodriguez-Fernandez et al. performed a study examining 2 groups with hip fractures. The first group was studied retrospectively and had an average delay of surgical treatment of more than 1-week while the second group was studied prospectively, and had surgical treatment within 48 hours. They found a larger number of complications in the group with a delay in surgical treatment. They conclude that elderly patients with hip fractures should be treated as soon as their medical condition permits.
Figures A and B are the AP and lateral radiographs demonstrating a right, unstable intertrochanteric femur fracture. Illustration A is an intertrochanteric femur fracture, stabilized with a cephalomedullary nail.
Incorrect Answers:
Answer 1: A surgical delay of greater than 48 hours has not been found to increase intraoperative time when patients get to surgery.
Answer 3: A surgical delay of greater than 48 hours has been shown to increase the rate of postoperative pneumonia.
Answer 4: A surgical delay of greater than 48 hours has not been associated with higher rates of blood transfusion.
Answer 5: A surgical delay of greater than 48 hours has not been associated with an increased risk of post-operative infection.
Hip fractures are common and mortality rates vary. In the elderly, mortality rates may reach 10% at 1-month, 20% at 4-months, and 30% at 1-year. Time to surgery has found to be a decisive factor. A pre-operative delay may lead to an increase in mortality and adversely influence other clinical outcomes.
Clinical guidelines recommend immediate operative stabilization, given the patient is medically fit for surgery.
Nyholm et al. performed a retrospective study of the Danish Fracture Database to investigate whether a surgical delay increases 30-day and 90-day mortality rates for patients with proximal femoral fractures. The 30-day and 90-day mortalities were 10.8% and 17.4%, respectively. The risk of 30-day mortality increased with increasing time intervals of more than 12 hours, 24 hours, and more than 48 hours. 90-day mortality increased with a surgical delay of more than 24 hours. They conclude that rapid surgical treatment should be performed by attending orthopaedic surgeons.
Moja et al. performed a meta-analysis and meta-regression to assess the relationship between surgical delay and mortality in elderly patients with a hip fracture. They analyzed 35 independent studies with 191,873 patients and 34,448 deaths. The majority of studies had a cut-off of 48 hours. They report that early hip surgery was associated with a lower risk of death and pressure sores. They conclude that early hip fracture surgery appears to provide a survival benefit compared to later intervention.
Rodriguez-Fernandez et al. performed a study examining 2 groups with hip fractures. The first group was studied retrospectively and had an average delay of surgical treatment of more than 1-week while the second group was studied prospectively, and had surgical treatment within 48 hours. They found a larger number of complications in the group with a delay in surgical treatment. They conclude that elderly patients with hip fractures should be treated as soon as their medical condition permits.
Figures A and B are the AP and lateral radiographs demonstrating a right, unstable intertrochanteric femur fracture. Illustration A is an intertrochanteric femur fracture, stabilized with a cephalomedullary nail.
Incorrect Answers:
Answer 1: A surgical delay of greater than 48 hours has not been found to increase intraoperative time when patients get to surgery.
Answer 3: A surgical delay of greater than 48 hours has been shown to increase the rate of postoperative pneumonia.
Answer 4: A surgical delay of greater than 48 hours has not been associated with higher rates of blood transfusion.
Answer 5: A surgical delay of greater than 48 hours has not been associated with an increased risk of post-operative infection.
Question 39High Yield
A 38-year-old man sustains a terrible triad injury consisting of an elbow dislocation, comminuted and displaced radial head fracture, and a type I coronoid fracture. Intraoperative findings after radial head replacement and lateral collateral ligament complex repair reveal persistent instability consisting of medial opening on valgus stress and posteromedial subluxation of the ulnohumeral and radiocapitellar joints. What is the best next step?
Explanation
Terrible triad injuries of the elbow are common, and the management of type I coronoid tip fractures remains controversial. Type I coronoid fractures result in only small changes in elbow kinematics that have been shown to be uncorrected with suture repair. A type I coronoid tip fracture is not amenable to buttress plate fixation. The radial collateral ligament is a component of the lateral collateral ligament complex and has already been repaired. The persistent medial laxity and posteromedial joint subluxation noted is indicative of ongoing instability. The next step would be repair or reconstruction of the medial collateral ligament, which will normally correct the medial instability. Articulated versus static external fixation can be considered if the joint remains unstable despite repair/reconstruction of the damaged stabilizing structures.
53
53
Question 40High Yield
Figures 1 and 2 are the radiographs of a 37-year-old left-hand dominant man with left elbow pain and stiffness. He has a history of elbow dislocation as a child but denies any recent injuries. He has an arc of motion of 105° and stable ligaments. He describes crepitus and locking during elbow range of motion. He is an avid Crossfit athlete, intending to return to this activity and improve his range of motion. What is the best treatment?
Explanation
14
This is a young, high-demand patient with early posttraumatic arthritis of the elbow. A debridement and capsular release has the ability to address his mechanical symptoms, improve his range of motion, and not result in any post- operative functional restrictions. While this may be a temporizing procedure in this patient, it will allow him to return to weight bearing recreational activities in the near term, which is his goal. A TEA would not be indicated based on the patient's age, his degree of arthritis, and his desire to remain active post- operatively. A radial head replacement would not address the patient's ulnohumeral arthritis. Similarly, an ulnohumeral distraction interposition arthroplasty would not address the patient's radiocapitellar arthritis. Both procedures would also require adjustments to his recreational activities post- operatively to prevent progressive failure of the reconstruction.
This is a young, high-demand patient with early posttraumatic arthritis of the elbow. A debridement and capsular release has the ability to address his mechanical symptoms, improve his range of motion, and not result in any post- operative functional restrictions. While this may be a temporizing procedure in this patient, it will allow him to return to weight bearing recreational activities in the near term, which is his goal. A TEA would not be indicated based on the patient's age, his degree of arthritis, and his desire to remain active post- operatively. A radial head replacement would not address the patient's ulnohumeral arthritis. Similarly, an ulnohumeral distraction interposition arthroplasty would not address the patient's radiocapitellar arthritis. Both procedures would also require adjustments to his recreational activities post- operatively to prevent progressive failure of the reconstruction.
Question 41High Yield
A 58-year-old man with a 50-year history of osteomyelitis of the left tibia has a painful ulceration of the anterior lower limb. Figure 1 is the clinical photograph of the wound, which had purulent discharge and an unpleasant odor. Figures 2 and 3 are radiographs of the left tibia. A biopsy reveals malignant degeneration. What are the most likely findings?
---
---
---
---



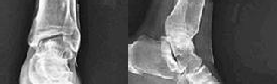
Explanation
Squamous cell carcinoma is the most common type of malignant tumor deriving from chronic osteomyelitis. The most frequently affected site is the tibia, followed by the femur. When the neoplasm invades the bone, there is either osteolytic erosion or a pathological fracture. Diagnosis is confirmed by biopsy at all suspicious wound sites. The malignant transformation most often results in squamous cell carcinoma and much more rarely in fibrosarcoma, osteosarcoma, reticulosarcoma, malignant fibrous histiocytoma or angiosarcoma. Many experts accept amputation as the best treatment option for carcinomatous transformation of chronic bone infections.
Question 42High Yield
A 16-year-old female gymnast reports a 2-month history of back pain since falling off the parallel bars, and she has been unable to return to gymnastics. She has no numbness or tingling. Examination reveals lower back tenderness, some paravertebral muscle spasm, range of motion of the lumbosacral spine is 20 degrees of flexion and 20 degrees of extension, and an equivocal straight leg raise. Lumbosacral spine radiographs demonstrate Schomorl’s nodes but no evidence of spondylolisthesis. What is the next best step in management?
Explanation
DISCUSSION: Injuries to the anterior and middle column in gymnasts occur but are far less common than posterior column injuries such as spondylolysis and spondylolisthesis. The data on injuries to the anterior and middle columns are more limited. Long-term gymnastics exercise is associated with disk degeneration and other anterior and middle column abnormalities as reported by Katz and Scerpella. They identified a series of anterior and middle column abnormalities, including vertebral compression fractures, Schmorl’s nodes, disk degeneration, and disk herniation in young competitive female gymnasts with back pain. Therefore, the differential diagnosis of back pain in these athletes should include abnormalities of the anterior and middle column. Although diagnostic imaging should begin with radiographs, MRI is the best way to diagnosis these abnormalities. A bone scan is more useful for imaging bony abnormalities of the posterior elements. Flexion-extension radiographs are not indicated in this patient. Treatment such as physical therapy or a lumbosacral corset should not be initiated prior to a complete work-up.
REFERENCES: Katz DA, Scerpella TA: Anterior and middle column thoracolumbar spine injuries in young female gymnasts: Report of seven cases and review of the literature. Am J Sports Med 2003;31:611-616.
Tertti M, Paajanen H, Kujala UM, et al: Disc degeneration in young gymnasts: A magnetic resonance imaging study. Am J Sports Med 1990;18:206-208.
REFERENCES: Katz DA, Scerpella TA: Anterior and middle column thoracolumbar spine injuries in young female gymnasts: Report of seven cases and review of the literature. Am J Sports Med 2003;31:611-616.
Tertti M, Paajanen H, Kujala UM, et al: Disc degeneration in young gymnasts: A magnetic resonance imaging study. Am J Sports Med 1990;18:206-208.
Question 43High Yield
A 16-year-old swimmer has right shoulder pain with activity. She describes the continued sensation that her shoulder is "loose." She has been in physical therapy for 7 months to work on strengthening the muscles around her shoulder and scapula. She denies being able to voluntarily dislocate her shoulder. Upon examination, you can feel the humeral head slide over the glenoid rim both anteriorly and posteriorly with the load and shift test. She has a grade III sulcus sign. What is the most appropriate next step?
Explanation
Nonsurgical treatment with activity modification and physical therapy is generally considered the first-line approach for young athletes with multidirectional instability (MDI) of the shoulder. Physical therapy focuses on exercises to strengthen the scapular stabilizers and rotator cuff muscles and restore scapulohumeral rhythm. Although a definitive length of time to assess physical therapy failure is not known, many surgeons believe that a patient with MDI should undergo at least 6 months of physical therapy and activity
36
modification before considering surgery. Although an open inferior capsular shift has historically been considered the gold standard for surgical treatment for MDI, studies have shown good success rates for arthroscopic capsulorrhaphy. Arthroscopy can allow a surgeon to assess all intra-articular structures and address a patient’s particular problem based on arthroscopic findings.
36
modification before considering surgery. Although an open inferior capsular shift has historically been considered the gold standard for surgical treatment for MDI, studies have shown good success rates for arthroscopic capsulorrhaphy. Arthroscopy can allow a surgeon to assess all intra-articular structures and address a patient’s particular problem based on arthroscopic findings.
Question 44High Yield
What is the most likely diagnosis based on the MRI findings shown in Figures 87a and 87b?
Explanation
DISCUSSION: The MRI scans reveal increased signal in the medial facet of the patella and the anterior aspect of the lateral femoral condyle. This pattern is typically seen in patients with acute patellar dislocations. In patients with ACL tears, the bone bruise of the lateral femoral condyle is usually seen in the central portion at the sulcus terminalis and the posterior half of the lateral tibial plateau and is not usually seen in the patella. This pattern of bone bruising is not seen with patellar tendon ruptures, LCL tears, and PCL tears.
REFERENCES: Elias DA, White LM, Fithian DA: Acute lateral patellar dislocation at MR imaging: Injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology 2002;225:736-743.
Virolainen H, Visuri T, Kuusela T: Acute dislocation of the patella: MR findings. Radiology 1993;189:243-246.
REFERENCES: Elias DA, White LM, Fithian DA: Acute lateral patellar dislocation at MR imaging: Injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology 2002;225:736-743.
Virolainen H, Visuri T, Kuusela T: Acute dislocation of the patella: MR findings. Radiology 1993;189:243-246.
Question 45High Yield
Of the following variables, which has the strongest influence on external fixator stiffness?
Explanation
**
Whereas all of the factors will have an impact on frame rigidity and stability, the single biggest factor is the pin diameter because it has an exponential effect.
Whereas all of the factors will have an impact on frame rigidity and stability, the single biggest factor is the pin diameter because it has an exponential effect.
Question 46High Yield
A 12-year-old patient with osteogenic sarcoma metastatic to the spine is noted to have new onset of weakness of both lower extremities. Magnetic resonance imaging shows a mass expanding posteriorly and encroaching on the spinal cord. The recommended initial step is:
Explanation
Radiation therapy combined with steroids should be tried first to try to halt progression of the tumor. Unfortunately, the prognosis for this child is extremely poor.
Increasing the dose of chemotherapy is not likely to work because the metastasis has already progressed despite initial treatment.
Surgical resection must be tried if radiation does not produce improvement. Steroids are an adjunct to treatment but not sufficient alone.
The patient is likely to have progressive paraparesis and loss of bowel function. In order to improve the quality of life remaining, surgical resection should be offered to the patient.
Increasing the dose of chemotherapy is not likely to work because the metastasis has already progressed despite initial treatment.
Surgical resection must be tried if radiation does not produce improvement. Steroids are an adjunct to treatment but not sufficient alone.
The patient is likely to have progressive paraparesis and loss of bowel function. In order to improve the quality of life remaining, surgical resection should be offered to the patient.
Question 47High Yield
A 23-year-old woman has had a 3-year history of snapping and pain in her left hip. She notes that the snapping started while marathon training and is only problematic about 15 minutes into a run. Examination is consistent with a negative Stinchfield, negative logroll, negative flexion abduction/external rotation test (FABER) of the hip; however, she has a positive Ober test as she has difficulty adducting her hip across the midline in the lateral decubitus position. Management consisting of nonsteroidal antiinflammatory drugs and stretching has failed to improve her snapping. What is the most reliable surgical treatment?
Explanation
DISCUSSION: The patient has external-type snapping hip (coxa saltans). It is not uncommon for patients to have a very long duration of symptoms that limit running or other sporting activities, and commonly affects the downward leg (usually the left leg when running on the left side of the road). The snapping causes a profound bursitis at the greater trochanter, and occasionally corticosteroid injections may be helpful. Her physical examination does not suggest an intra-articular process, and is not consistent with an internal-type snapping hip, usually caused by the iliopsoas tendon as it moves over the iliopectineal eminence. Stretching is the mainstay of treatment, as testing with a positive Ober signifies a tight iliotibial band as the thigh has difficulty crossing the midline with adduction. Various iliotibial band lengthening procedures have been described, including a Z-plasty near the proximal origin of the iliotibial band. Release at Gerdy’s tubercle has not been described.
REFERENCES: Provencher MT, Hofmeister EP, Muldoon MP: The surgical treatment of external coxa saltans (the snapping hip) by Z-plasty of the iliotibial band. Am J Sports Med 2004;32:470-476.
Faraj A A, Moulton A, Sirivastava VM: Snapping iliotibial band: Report of ten cases and review of the literature. Acta Orthop Belg 2001;67:19-23.
Brignall CG, Stainsby GD: The snapping hip: Treatment by Z-plasty. J Bone Joint Surg Br 1991 ;73:253-
254.
REFERENCES: Provencher MT, Hofmeister EP, Muldoon MP: The surgical treatment of external coxa saltans (the snapping hip) by Z-plasty of the iliotibial band. Am J Sports Med 2004;32:470-476.
Faraj A A, Moulton A, Sirivastava VM: Snapping iliotibial band: Report of ten cases and review of the literature. Acta Orthop Belg 2001;67:19-23.
Brignall CG, Stainsby GD: The snapping hip: Treatment by Z-plasty. J Bone Joint Surg Br 1991 ;73:253-
254.
Question 48High Yield
The pathology of the lesion shown in Figures 1 and 2 reveal what cellular pattern?
---
---
---
---
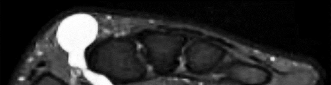
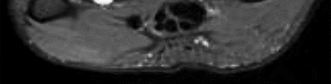
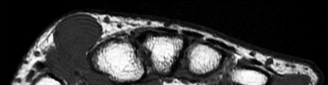
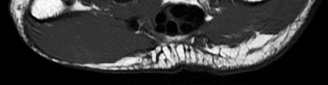
Explanation
No detailed explanation provided for this question.
Question 49High Yield
A patient with a displaced and comminuted fracture of the radial head and neck also has pain and swelling about the ipsilateral distal radioulnar joint. Which treatment option may exacerbate the wrist disorder?
Explanation
This scenario describes a forearm-axial instability pattern, which must be recognized before pursuing treatment. Fracture or dislocation of the lateral elbow compartment (radial head/capitellum) associated with ipsilateral distal radioulnar joint derangement is a form of radioulnar dissociation commonly known as Essex-Lopresti fracture dislocation. Radial head excision sets off a chain of events, and delayed diagnosis can result in considerable morbidity following these injuries. Excision of the radial head allows proximal migration of the radius, causing potential problems at both the elbow and wrist. After such proximal migration has occurred, there is no reliable method of forearm reconstruction.
There are a number of treatments for this condition. Salvage of the radial head by open reduction and internal fixation is preferable if possible. However, in cases of marked comminution, radial metallic head implant arthroplasty is an acceptable substitute. The need for soft-tissue repair or pin stabilization of the distal radioulnar joint has not been defined, although some form of forearm immobilization is necessary to allow healing of the injured interosseous membrane.
RECOMMENDED READINGS
81. Trousdale RT, Amadio PC, Cooney WP, Morrey BF. Radio-ulnar dissociation. A review of twenty cases. J Bone Joint Surg Am. 1992 Dec;74(10):1486-97. PubMed PMID: 1469008.
82. Edwards GS Jr, Jupiter JB. Radial head fractures with acute distal radioulnar dislocation. Essex-Lopresti revisited. Clin Orthop Relat Res. 1988 Sep;(234):61-9. PubMed PMID: 3409602.
There are a number of treatments for this condition. Salvage of the radial head by open reduction and internal fixation is preferable if possible. However, in cases of marked comminution, radial metallic head implant arthroplasty is an acceptable substitute. The need for soft-tissue repair or pin stabilization of the distal radioulnar joint has not been defined, although some form of forearm immobilization is necessary to allow healing of the injured interosseous membrane.
RECOMMENDED READINGS
81. Trousdale RT, Amadio PC, Cooney WP, Morrey BF. Radio-ulnar dissociation. A review of twenty cases. J Bone Joint Surg Am. 1992 Dec;74(10):1486-97. PubMed PMID: 1469008.
82. Edwards GS Jr, Jupiter JB. Radial head fractures with acute distal radioulnar dislocation. Essex-Lopresti revisited. Clin Orthop Relat Res. 1988 Sep;(234):61-9. PubMed PMID: 3409602.
Question 50High Yield
A 68-year-old woman reports pain and sensations of instability following a primary total knee arthroplasty 18 months ago. A preoperative radiograph is shown in Figure 39a and postoperative AP and patellar view
radiographs are shown in Figures 39b and 39c. A CT scan shows that the femoral component is internally rotated 8 degrees and the tibial component is internally rotated 4 degrees. Management should include which of the following?
radiographs are shown in Figures 39b and 39c. A CT scan shows that the femoral component is internally rotated 8 degrees and the tibial component is internally rotated 4 degrees. Management should include which of the following?
Explanation
The patient had a valgus knee preoperatively and in these patients, care must be taken to avoid internal rotation of the femoral component that can lead to patellar instability. At the present time she has a completely dislocated patella, evidence of coronal instability on her AP radiograph, and internally rotated femoral and tibial components; therefore, management should consist of revision of both of her components to place them in appropriate external rotation.
REFERENCES: Malo M, Vince KG: The unstable patella after total knee arthroplasty: Etiology, prevention, and management. J Am Acad Orthop Surg 2003; 11:364-371.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 123-145. Question 40
The term “paradoxical motion,” used to describe knee kinematics, is best described by which of the following definitions?
1. The patella does not roll forward into the trochlear groove during knee extension.
2. The tibia rolls back on the femur during knee extension.
3. The tibiofemoral contact point moves anteriorly during knee flexion.
4. The posterior cruciate ligament rolls posteriorly with respect to the anterior cruciate ligament during knee extension.
5. The femur rolls back on the tibia during knee flexion.
PREFERRED RESPONSE: 3
DISCUSSION: The term “rollback” describes the posterior movement of the tibiofemoral contact point with knee motion from extension to flexion. Therefore, with “paradoxical rollback” this contact point moves anteriorly. “Paradoxical rollback” is a term used to connote the inability of the anterior cruciate- deficient, posterior cruciate-retaining total knee prosthesis to create normal posterior femoral rollback with knee flexion.
REFERENCES: Dennis DA, Komistek RD, Mahfouz MR: In vivo fluoroscopic analysis of fixed-bearing total knee replacements. Clin Orthop Relat Res 2003;410:114-130.
Incavo SJ, Mullins ER, Coughlin KM, et al: Tibiofemoral kinematic analysis after total knee arthroplasty.
J Arthroplasty 2004;19:906-910.
REFERENCES: Malo M, Vince KG: The unstable patella after total knee arthroplasty: Etiology, prevention, and management. J Am Acad Orthop Surg 2003; 11:364-371.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 123-145. Question 40
The term “paradoxical motion,” used to describe knee kinematics, is best described by which of the following definitions?
1. The patella does not roll forward into the trochlear groove during knee extension.
2. The tibia rolls back on the femur during knee extension.
3. The tibiofemoral contact point moves anteriorly during knee flexion.
4. The posterior cruciate ligament rolls posteriorly with respect to the anterior cruciate ligament during knee extension.
5. The femur rolls back on the tibia during knee flexion.
PREFERRED RESPONSE: 3
DISCUSSION: The term “rollback” describes the posterior movement of the tibiofemoral contact point with knee motion from extension to flexion. Therefore, with “paradoxical rollback” this contact point moves anteriorly. “Paradoxical rollback” is a term used to connote the inability of the anterior cruciate- deficient, posterior cruciate-retaining total knee prosthesis to create normal posterior femoral rollback with knee flexion.
REFERENCES: Dennis DA, Komistek RD, Mahfouz MR: In vivo fluoroscopic analysis of fixed-bearing total knee replacements. Clin Orthop Relat Res 2003;410:114-130.
Incavo SJ, Mullins ER, Coughlin KM, et al: Tibiofemoral kinematic analysis after total knee arthroplasty.
J Arthroplasty 2004;19:906-910.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon