Approaches Orthopedic B Review | Dr Hutaif General Orth -...
14 Apr 2026
64 min read
113 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Approaches Orthopedic B Review | Dr Hutaif Ge...
00:00
Start Quiz
Question 1High Yield
Surgeons can improve the biomechanical stability of a zone II flexor tendon suture repair by
Explanation
Biomechanical stability of zone II flexor tendon repairs can be improved by increasing the suture spread distance at the repair site (near-far), increasing the number of strands at the repair site, increasing the caliber of the suture, using sutures that lock the tendon, and adding an epitendinous repair circumferentially around the tendon. Although maintaining the flexor tendon pulleys and initiating early active motion benefits the functional outcome, these steps do not impact the biomechanical stability of the flexor tendon repair. However, they add more biomechanical stress on the repair site.
RECOMMENDED READINGS
29. [Barrie KA, Wolfe SW, Shean C, Shenbagamurthi D, Slade JF 3rd, Panjabi MM. A biomechanical comparison of multistrand flexor tendon repairs using an in situ testing model. J Hand Surg Am. 2000 May;25(3):499-506. PubMed PMID: 10811755. ](http://www.ncbi.nlm.nih.gov/pubmed/10811755)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10811755)
30. [Lee SK, Goldstein RY, Zingman A, Terranova C, Nasser P, Hausman MR. The effects of core suture purchase on the biomechanical characteristics of a multistrand locking flexor tendon repair: a cadaveric study. J Hand Surg Am. 2010 Jul;35(7):1165-71. doi: 10.1016/j.jhsa.2010.04.003. Epub 2010 Jun 11. PubMed PMID: 20541326. ](http://www.ncbi.nlm.nih.gov/pubmed/%2020541326)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2020541326)
31. Miller B, Dodds SD, deMars A, Zagoreas N, Waitayawinyu T, Trumble TE. Flexor tendon repairs: the impact of fiberwire on grasping and locking core sutures. J Hand Surg Am. 2007 May-Jun;32(5):591-
[6/. PubMed PMID: 17481994. ](http://www.ncbi.nlm.nih.gov/pubmed/17481994)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17481994)
32. [Boyer MI, Strickland JW, Engles D, Sachar K, Leversedge FJ. Flexor tendon repair and rehabilitation: state of the art in 2002. Instr Course Lect. 2003;52:137-61. Review. PubMed PMID: 12690845. ](http://www.ncbi.nlm.nih.gov/pubmed/12690845)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690845)
RECOMMENDED READINGS
29. [Barrie KA, Wolfe SW, Shean C, Shenbagamurthi D, Slade JF 3rd, Panjabi MM. A biomechanical comparison of multistrand flexor tendon repairs using an in situ testing model. J Hand Surg Am. 2000 May;25(3):499-506. PubMed PMID: 10811755. ](http://www.ncbi.nlm.nih.gov/pubmed/10811755)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10811755)
30. [Lee SK, Goldstein RY, Zingman A, Terranova C, Nasser P, Hausman MR. The effects of core suture purchase on the biomechanical characteristics of a multistrand locking flexor tendon repair: a cadaveric study. J Hand Surg Am. 2010 Jul;35(7):1165-71. doi: 10.1016/j.jhsa.2010.04.003. Epub 2010 Jun 11. PubMed PMID: 20541326. ](http://www.ncbi.nlm.nih.gov/pubmed/%2020541326)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2020541326)
31. Miller B, Dodds SD, deMars A, Zagoreas N, Waitayawinyu T, Trumble TE. Flexor tendon repairs: the impact of fiberwire on grasping and locking core sutures. J Hand Surg Am. 2007 May-Jun;32(5):591-
[6/. PubMed PMID: 17481994. ](http://www.ncbi.nlm.nih.gov/pubmed/17481994)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17481994)
32. [Boyer MI, Strickland JW, Engles D, Sachar K, Leversedge FJ. Flexor tendon repair and rehabilitation: state of the art in 2002. Instr Course Lect. 2003;52:137-61. Review. PubMed PMID: 12690845. ](http://www.ncbi.nlm.nih.gov/pubmed/12690845)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690845)
Question 2High Yield
The most common cause of damage to femoral vessels is:
Explanation
Damage to the femoral vessels is most commonly due to aberrant retractor placement. Care should be taken to ensure that the retractor tip is placed directly on bone, and that the iliopsoas is not interposed between the retractor tip and bone. Extruded cement, acetabular cup migration, and capsule dissection have also been implicated in damage to the femoral vessels
Question 3High Yield
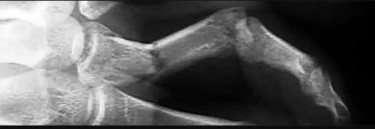
Assuming that the fracture shown in this radiograph (Figure 79) is aligned on the anteroposterior radiograph and heals in this position, secondary to fracture malalignment, there will be loss of active
Explanation
This is a transverse proximal phalanx fracture with apex volar angulation. The fracture displaces into an apex volar angulated position under the pull of the central slip on the distal fragment and the interossei insertions at the base of proximal phalanx. Although it is possible to lose motion in flexion or extension of the MP or PIP joints, the biomechanics will not allow full extension of the PIP joint. If allowed to heal in apex palmar malunion, the predicted corresponding extensor lags are for a 10-degree lag at 16 degrees of angular deformity, a 24-degree lag at 27 degrees of deformity, and a 66-degree lag at 46 degrees of deformity. These fractures usually can be treated with closed reduction with or without percutaneous pinning. With surgical treatment, there may be loss of motion both at the MP and PIP joints.
RECOMMENDED READINGS
60. Henry MH. Fractures of the proximal phalanx and metacarpals in the hand: preferred methods of stabilization. J Am Acad Orthop Surg. 2008 Oct;16(10):586-95. Review. PubMed PMID: 18832602.
61. Faruqui S, Stern PJ, Kiefhaber TR. Percutaneous pinning of fractures in the proximal third of the proximal phalanx: complications and outcomes. J Hand Surg Am. 2012 Jul;37(7):1342-8. doi: 10.1016/j.jhsa.2012.04.019. PubMed PMID: 22721457.
RECOMMENDED READINGS
60. Henry MH. Fractures of the proximal phalanx and metacarpals in the hand: preferred methods of stabilization. J Am Acad Orthop Surg. 2008 Oct;16(10):586-95. Review. PubMed PMID: 18832602.
61. Faruqui S, Stern PJ, Kiefhaber TR. Percutaneous pinning of fractures in the proximal third of the proximal phalanx: complications and outcomes. J Hand Surg Am. 2012 Jul;37(7):1342-8. doi: 10.1016/j.jhsa.2012.04.019. PubMed PMID: 22721457.
Question 4High Yield
**ORTHOPEDIC MCQS OB 20 BASIC7**
700. What method of spinal fixation requires the largest force to disrupt the bone-implant interface?
700. What method of spinal fixation requires the largest force to disrupt the bone-implant interface?
Explanation
concerning available
alternatives as well as the consequences of no treatment must also ensue. The explanation must be made in simple lay terms. 3) The participant must have the mental competency to comprehend the information. 4) There should be reasonable steps to ascertain that the subject understands all aspects of the discussion. 5) The subject actually makes a decision regarding participation.
708. What molecules have been shown to promote fibrosis during muscle injury?
1. Insulin growth factor 1 (IGF-1)
2. Basic fibroblast growth factor (bFGF)
3. Transforming growth factor beta 1 (TGF-ß1)
4. Bone morphogenetic protein
CORRECT answer: 3
A muscle's response to injury can be divided into 4 phases: necrosis, inflammation, repair, and fibrosis. Necrosis involves the degeneration of the muscle fibrils and death. The inflammatory cells then phagocytose the debris and secrete cytokines that promote vascularity. Muscle regeneration does not occur until phagocytic cells remove the debris. Consequently, anti- inflammatory drugs may have negative effects on muscle healing by inhibiting macrophage-induced phagocytosis. Muscle fibrosis occurs at the same time as muscle regeneration and has been shown to involve TGF-ß1. IGF-1 and bFGF are important trophic factors in muscle regeneration. Bone morphogenetic protein has several functions including bone and cartilage regeneration.
709. A surgeon decides to report outcomes for a new surgical procedure that he has performed on 10 patients who have a rare type of arthritis. He provides data on the functional and subjective patient outcomes. This type of study design is best described as a
1. case series.
2. case-control study.
3. cohort study.
4. randomized clinical trial.
CORRECT answer: 1
The type of study design in which a series of cases is presented with outcomes (without a control population or comparison group) is known as a case series. This type of study design, although frequently seen in orthopaedic literature, provides the lowest level of evidence. There is no control group and the population is usually poorly defined. This type of study can be helpful as a starting point for further analysis. A randomized trial provides the highest level of evidence in medical research, featuring a comparison group and
randomized (and usually blinded) placement of subjects into study groups. In case-control studies, cases are compared to a control group. The control group has not
been randomized, but may be a naturally occurring group of subjects who
have not had the same exposure or intervention as the case group. A cohort study can be retrospective or prospective and usually looks at a large group of people over time to assess exposures and incidence of disease.
710. What effect does intermittent administration of parathyroid hormone have on bone?
1. Anabolic
2. Catabolic
3. No effect
4. Decreased quantity
5. Decreased quality
CORRECT answer: 1
Treatment of osteoporosis centers on increasing bone mass by direct anabolic effect and/or inhibiting osteoclastic absorption. Bisphosphonates, selective estrogen receptor modulators, and calcitonin act to decrease bone resorption by inhibiting osteoclasts.
Parathyroid hormone causes both bone formation and resorption, depending on frequency of dosing. Osteoblasts are primary targets for PTH. Once activated, they secrete RANKL and IL-6, which causes osteoclast proliferation/maturation, leading to increased bone resorption. Because of this coupled remodeling process, several observations have been made:
1)intermittent PTH injections increase bone mass, 2) continous infusion lead to bone resorption, and 3) dosing should not continue past 2 yrs. Thus, intermittent parathyroid hormone is anabolic to bone and is used as a treatment of osteoporosis (forteo).
721. What dominant intracellular proteins become directly phosphorylated as a result of bone morphogenetic protein (BMP) binding to its receptors?
1. Myc
2. SMADs
3. Beta-catenin (ß-catenin)
4. Adenylate cyclase
CORRECT answer: 2
BMP proteins, which are part of the larger transforming growth factor-beta super family, bind to serine/threonine receptors on the cell surface. This binding causes phosphorylation of SMAD proteins, which in turn forms a complex that enters the nucleus and initiates the transcription of several genes involved in osteoblastic differentiation. Adenylate cyclase is
a transmembrane protein that acts intracellularly to activate the G protein pathways. Myc is a proto-oncogene that encodes for a transcription factor involved in numerous cell- activation pathways, but is not directly phosphorylated by BMP receptor.
ß-catenin is an intracellular molecule that plays a key role in the Wnt signaling pathway. This pathway is also involved in osteoblastic differentiation, but differs in target proteins within the cell.
722. A 45-year-old previously healthy woman has experienced weakness and fatigability for 2 months. She states she feels best in the morning, but tires easily with exertion. If she sits and rests her strength improves, but she easily tires with each activity. When her fatigue is most severe, she has double vision. Physical examination is**
**positive for ptosis with upward gaze after 20 seconds. When she holds her arms out straight she shows good initial strength, but rapidly decreasing strength with time. What is the pathologic cause of her muscle weakness?
1. Ig antibodies at the neuromuscular (NM) junction
2. Decreased release of acetylcholine at the NM junction
3. Decrease in myelin sheath of axonal nerves with loss of NM junction
4. Absence of dystrophin with excess calcium at sarcolemma
CORRECT answer: 1
The patient has myasthenia gravis, which has its onset in middle age and causes progressive weakness because of the loss of acetylcholine receptors secondary to autoimmune antibodies at the NM junction. Rest periods allow uptake of acetylcholine and initial strength, but easy fatigability. Treatment is aimed at immunomodulation; acetyl cholinesterase inhibitors often coupled with thymectomy can control symptoms.
Decreased release of acetylcholine at the NM junction is the effect of a nondepolarizing drug or toxin botulinum. Patients with muscular dystrophy lack dystrophin that acts at the sarcolemma to regulate calcium channels, and onset of this condition occurs at a younger age. The decrease in myelin indicates Charcot-Marie-Tooth disease and is
often seen with long axon degeneration, such as in the feet and lower legs.
723. You are studying a single continuous variable after administration of a defined treatment intervention. Your statistician informs you the data are not normally distributed. What is the best test to analyze the data?
1. Analysis of variance (ANOVA)
2. Regression analysis
3. Student t test
4. Mann-Whitney U test
CORRECT answer: 4
The Mann-Whitney U test is used when data are nonparametric, meaning either not normally distributed or variances are not equal among groups. Both the Student t test and ANOVA are used with parametric, normally distributed data. A regression analysis is a
statistical model that allows for control of potentially confounding variables. It is used to assess the relationship between a dependent variable and (usually) multiple independent variables.
724. Which of the following is the mechanism of action of aspirin?
1. Inhibition of vitamin K-dependent carboxylation
2. Inhibition of factor Xa through antithrombin binding
3. Binding of cyclooxygenase (COX)-1 and COX-2
4. Direct thrombin inhibition
5. Glycoprotein IIIb agonist binding
CORRECT answer: 3**
Aspirin works by the irreversible binding of cycloxygenase (COX). This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect. In addition, there is a decrease in the level of prostaglandin production due to the COX-1 binding.
Aspirin's effects and respective mechanisms of action vary with dose:
Low doses (typically 75 to 81 mg/day) are sufficient to irreversibly acetylate serine 530 of cyclooxygenase (COX)-1. This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect.
alternatives as well as the consequences of no treatment must also ensue. The explanation must be made in simple lay terms. 3) The participant must have the mental competency to comprehend the information. 4) There should be reasonable steps to ascertain that the subject understands all aspects of the discussion. 5) The subject actually makes a decision regarding participation.
708. What molecules have been shown to promote fibrosis during muscle injury?
1. Insulin growth factor 1 (IGF-1)
2. Basic fibroblast growth factor (bFGF)
3. Transforming growth factor beta 1 (TGF-ß1)
4. Bone morphogenetic protein
CORRECT answer: 3
A muscle's response to injury can be divided into 4 phases: necrosis, inflammation, repair, and fibrosis. Necrosis involves the degeneration of the muscle fibrils and death. The inflammatory cells then phagocytose the debris and secrete cytokines that promote vascularity. Muscle regeneration does not occur until phagocytic cells remove the debris. Consequently, anti- inflammatory drugs may have negative effects on muscle healing by inhibiting macrophage-induced phagocytosis. Muscle fibrosis occurs at the same time as muscle regeneration and has been shown to involve TGF-ß1. IGF-1 and bFGF are important trophic factors in muscle regeneration. Bone morphogenetic protein has several functions including bone and cartilage regeneration.
709. A surgeon decides to report outcomes for a new surgical procedure that he has performed on 10 patients who have a rare type of arthritis. He provides data on the functional and subjective patient outcomes. This type of study design is best described as a
1. case series.
2. case-control study.
3. cohort study.
4. randomized clinical trial.
CORRECT answer: 1
The type of study design in which a series of cases is presented with outcomes (without a control population or comparison group) is known as a case series. This type of study design, although frequently seen in orthopaedic literature, provides the lowest level of evidence. There is no control group and the population is usually poorly defined. This type of study can be helpful as a starting point for further analysis. A randomized trial provides the highest level of evidence in medical research, featuring a comparison group and
randomized (and usually blinded) placement of subjects into study groups. In case-control studies, cases are compared to a control group. The control group has not
been randomized, but may be a naturally occurring group of subjects who
have not had the same exposure or intervention as the case group. A cohort study can be retrospective or prospective and usually looks at a large group of people over time to assess exposures and incidence of disease.
710. What effect does intermittent administration of parathyroid hormone have on bone?
1. Anabolic
2. Catabolic
3. No effect
4. Decreased quantity
5. Decreased quality
CORRECT answer: 1
Treatment of osteoporosis centers on increasing bone mass by direct anabolic effect and/or inhibiting osteoclastic absorption. Bisphosphonates, selective estrogen receptor modulators, and calcitonin act to decrease bone resorption by inhibiting osteoclasts.
Parathyroid hormone causes both bone formation and resorption, depending on frequency of dosing. Osteoblasts are primary targets for PTH. Once activated, they secrete RANKL and IL-6, which causes osteoclast proliferation/maturation, leading to increased bone resorption. Because of this coupled remodeling process, several observations have been made:
1)intermittent PTH injections increase bone mass, 2) continous infusion lead to bone resorption, and 3) dosing should not continue past 2 yrs. Thus, intermittent parathyroid hormone is anabolic to bone and is used as a treatment of osteoporosis (forteo).
721. What dominant intracellular proteins become directly phosphorylated as a result of bone morphogenetic protein (BMP) binding to its receptors?
1. Myc
2. SMADs
3. Beta-catenin (ß-catenin)
4. Adenylate cyclase
CORRECT answer: 2
BMP proteins, which are part of the larger transforming growth factor-beta super family, bind to serine/threonine receptors on the cell surface. This binding causes phosphorylation of SMAD proteins, which in turn forms a complex that enters the nucleus and initiates the transcription of several genes involved in osteoblastic differentiation. Adenylate cyclase is
a transmembrane protein that acts intracellularly to activate the G protein pathways. Myc is a proto-oncogene that encodes for a transcription factor involved in numerous cell- activation pathways, but is not directly phosphorylated by BMP receptor.
ß-catenin is an intracellular molecule that plays a key role in the Wnt signaling pathway. This pathway is also involved in osteoblastic differentiation, but differs in target proteins within the cell.
722. A 45-year-old previously healthy woman has experienced weakness and fatigability for 2 months. She states she feels best in the morning, but tires easily with exertion. If she sits and rests her strength improves, but she easily tires with each activity. When her fatigue is most severe, she has double vision. Physical examination is**
**positive for ptosis with upward gaze after 20 seconds. When she holds her arms out straight she shows good initial strength, but rapidly decreasing strength with time. What is the pathologic cause of her muscle weakness?
1. Ig antibodies at the neuromuscular (NM) junction
2. Decreased release of acetylcholine at the NM junction
3. Decrease in myelin sheath of axonal nerves with loss of NM junction
4. Absence of dystrophin with excess calcium at sarcolemma
CORRECT answer: 1
The patient has myasthenia gravis, which has its onset in middle age and causes progressive weakness because of the loss of acetylcholine receptors secondary to autoimmune antibodies at the NM junction. Rest periods allow uptake of acetylcholine and initial strength, but easy fatigability. Treatment is aimed at immunomodulation; acetyl cholinesterase inhibitors often coupled with thymectomy can control symptoms.
Decreased release of acetylcholine at the NM junction is the effect of a nondepolarizing drug or toxin botulinum. Patients with muscular dystrophy lack dystrophin that acts at the sarcolemma to regulate calcium channels, and onset of this condition occurs at a younger age. The decrease in myelin indicates Charcot-Marie-Tooth disease and is
often seen with long axon degeneration, such as in the feet and lower legs.
723. You are studying a single continuous variable after administration of a defined treatment intervention. Your statistician informs you the data are not normally distributed. What is the best test to analyze the data?
1. Analysis of variance (ANOVA)
2. Regression analysis
3. Student t test
4. Mann-Whitney U test
CORRECT answer: 4
The Mann-Whitney U test is used when data are nonparametric, meaning either not normally distributed or variances are not equal among groups. Both the Student t test and ANOVA are used with parametric, normally distributed data. A regression analysis is a
statistical model that allows for control of potentially confounding variables. It is used to assess the relationship between a dependent variable and (usually) multiple independent variables.
724. Which of the following is the mechanism of action of aspirin?
1. Inhibition of vitamin K-dependent carboxylation
2. Inhibition of factor Xa through antithrombin binding
3. Binding of cyclooxygenase (COX)-1 and COX-2
4. Direct thrombin inhibition
5. Glycoprotein IIIb agonist binding
CORRECT answer: 3**
Aspirin works by the irreversible binding of cycloxygenase (COX). This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect. In addition, there is a decrease in the level of prostaglandin production due to the COX-1 binding.
Aspirin's effects and respective mechanisms of action vary with dose:
Low doses (typically 75 to 81 mg/day) are sufficient to irreversibly acetylate serine 530 of cyclooxygenase (COX)-1. This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect.
Question 5High Yield
A 12-year-old girl is referred because of a positive school scoliosis screen. She has a curve of 16° from T5 to T12, convex to the right. She incidentally also complains of mild back pain over the region of the curve several times per month. Neurologic examination is normal. Recommended treatment includes:
Explanation
Home exercises and re-examination in follow-up is the most appropriate treatment in view of lack of any worrisome features. If this child had severe pain or significant night pain, then further imaging studies would be warranted.
The magnetic resonance imaging is not indicated in this situation. The bone scan has a low likelihood of being positive.
Bracing is not indicated for the curve or the pain.
C omputer tomography is unlikely to demonstrate any pathology.
The magnetic resonance imaging is not indicated in this situation. The bone scan has a low likelihood of being positive.
Bracing is not indicated for the curve or the pain.
C omputer tomography is unlikely to demonstrate any pathology.
Question 6High Yield
What is the most commonly reported complication following elbow arthroscopy?
Explanation
The complication rate following elbow arthroscopy is reported at 5%. The most commonly reported complication is transient neurapraxia, with nerve transection remaining an unfortunate and rare event. While infection remains the most common serious complication, it is uncommon (0.8%). Synovial cutaneous fistula and compartment syndrome, while reported, are the least frequent complications of elbow arthroscopy.
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of elbow arthroscopy.
J Bone Joint Surg Am 2001;83:25-34.
Morrey BF: Elbow complication, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 519-522.
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of elbow arthroscopy.
J Bone Joint Surg Am 2001;83:25-34.
Morrey BF: Elbow complication, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 519-522.
Question 7High Yield
1222) Which of the following fluoroscopic views is used to assess
intra-articular screw penetration during volar fixation of a distal radius fracture?
intra-articular screw penetration during volar fixation of a distal radius fracture?


Explanation
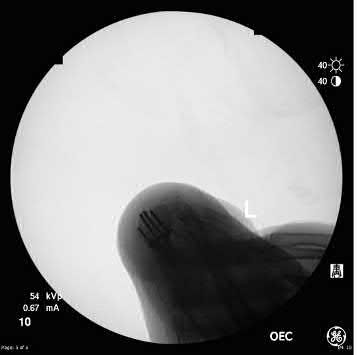
Due to radial inclination, a true lateral view of the wrist will not show whether screws from a volar plate are intra-articular; a 23° elevated lateral view is needed to adequately assess this.
The amount of elevation will depend on the degree to which the surgeon restores radial inclination; for example, if the surgeon only restores 15° of radial inclination, then the surgeon would only have to elevate the wrist 15° from a true lateral in order to have the radiographic beam point down the joint line. Failure to diagnose intra-articular screws intraoperatively can lead to degenerative changes.
Tweet et al. performed a survey of orthopedic surgeons regarding their preferred method of visualizing screw placement during wrist fixation. The majority of surgeons reported that they obtain multiple views, including AP/PA wrist views, a 23° lateral inclination view, and a true lateral view. They also performed a cadaveric study looking at different x-ray views and screw penetration. They reported that live rotational fluoroscopy provided the highest sensitivity (93%) and specificity (96%) for the detection of intra-articular screw penetration.
Patel et al. evaluated the ability of surgeons at different levels to critically assess distal radius fixation and screw placement. They found that supplementation with a 23° lateral view increased accuracy and confidence in all position, specialty, and experience groups. Confidence scores were significantly higher following the evaluation of three views versus two views. Residents exhibited the greatest improvements in accuracy and confidence. For first-phase (standard view) assessments, accuracy scores were significantly better for attendings with less than 10 years of post-fellowship experience than those with more.
Illustration A is a non-elevated lateral of the wrist, while illustration B is a 23° elevated lateral radiograph. Illustration C is an example of a skyline view, which assesses for screws penetrating the dorsal cortex.
Incorrect Answers:
Answer 1: The dorsal skyline view shows dorsal screw length and is useful to
check for long distal screws.
Answers 2 and 3: The AP and PA wrist views do not show intra-articular screw penetration due to the volar tilt and concavity of the joint.
Answer 5: A 45° oblique lateral view does not visualize the joint as this angle does not match the radial inclination.
The amount of elevation will depend on the degree to which the surgeon restores radial inclination; for example, if the surgeon only restores 15° of radial inclination, then the surgeon would only have to elevate the wrist 15° from a true lateral in order to have the radiographic beam point down the joint line. Failure to diagnose intra-articular screws intraoperatively can lead to degenerative changes.
Tweet et al. performed a survey of orthopedic surgeons regarding their preferred method of visualizing screw placement during wrist fixation. The majority of surgeons reported that they obtain multiple views, including AP/PA wrist views, a 23° lateral inclination view, and a true lateral view. They also performed a cadaveric study looking at different x-ray views and screw penetration. They reported that live rotational fluoroscopy provided the highest sensitivity (93%) and specificity (96%) for the detection of intra-articular screw penetration.
Patel et al. evaluated the ability of surgeons at different levels to critically assess distal radius fixation and screw placement. They found that supplementation with a 23° lateral view increased accuracy and confidence in all position, specialty, and experience groups. Confidence scores were significantly higher following the evaluation of three views versus two views. Residents exhibited the greatest improvements in accuracy and confidence. For first-phase (standard view) assessments, accuracy scores were significantly better for attendings with less than 10 years of post-fellowship experience than those with more.
Illustration A is a non-elevated lateral of the wrist, while illustration B is a 23° elevated lateral radiograph. Illustration C is an example of a skyline view, which assesses for screws penetrating the dorsal cortex.
Incorrect Answers:
Answer 1: The dorsal skyline view shows dorsal screw length and is useful to
check for long distal screws.
Answers 2 and 3: The AP and PA wrist views do not show intra-articular screw penetration due to the volar tilt and concavity of the joint.
Answer 5: A 45° oblique lateral view does not visualize the joint as this angle does not match the radial inclination.
Question 8High Yield
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by
Explanation
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by the use of a direct lateral approach to the ankle. The superficial peroneal nerve and its branches exit the fascial hiatus approximately 9 cm to 10 cm proximal to the tip of the distal fibula with a range of 4 cm to 13 cm, and their course is typically anterior to the midlateral plane of the fibula. However, small branches may course across the surgical plane directly laterally. A posterior-lateral approach diminishes the risk of injury to the superficial peroneal nerve and its branches; however, by moving farther posterior, the sural nerve and its branches may be at increased risk. Cast immobilization may injure the cutaneous nerves about the ankle; however, the risks are greater with surgical intervention. A medial or anterior-medial approach to the ankle will not injure the superficial peroneal nerve at the ankle level.
REFERENCES: Redfern DJ, Sauve PS, Sakellariou A: Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771-774.
Miller SD: Ankle fractures, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1341-1366.
REFERENCES: Redfern DJ, Sauve PS, Sakellariou A: Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771-774.
Miller SD: Ankle fractures, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1341-1366.
Question 9High Yield
1235) Which of the following pelvic injury types has the highest reported mortality rate?


Explanation
Anterior posterior compression (APC) injuries have the highest mortality rates of the fracture patterns listed.
APC injuries have high rates of concomitant thoracic and abdominal visceral injuries leading to the highest rates of mortality among pelvic fractures. Lateral compression (LC) fractures have particularly high incidences of associated brain and head injury with lower mortality than APC injuries. Overall, as the grade of pelvic ring injury increases the rates of associated injuries increases, regardless of exact mechanism of injury. The overall mortality rate for any pelvic trauma is roughly 15%, with APC III mortality around 37%, and overall
APC mortality rates around 26%. LC of any grade has an estimated mortality around 13%. Vertical shear and CMI have estimated mortality of 25% and 17.1%, respectively. The lowest mortality rates are following acetabular fractures with estimates around 1.5%.
Dalal et al retrospectively reviewed 340 trauma patients with pelvic injuries to analyze organ injury, resuscitative requirements, and outcomes. They found the highest mortality rates were in APC III and that more severe APC injuries had greater organ damage and mortality. They conclude that the mechanical force type and classification of injury are predictors of organ injury pattern, resuscitation needs, and mortality.
Eastridge et al reviewed 1,014 injured pedestrians for pelvic injuries, associated injuries, and relationship of treatments to outcomes. They found the highest mortality rates were associated with APC III and LC III injuries patterns at 50%. They conclude that pelvic fractures are a sign of significant energy imparted on the body and severity of associated injuries lead to the high rates of morbidity and mortality.
Illustration A and B show an APC III and LC III injury, respectively. Incorrect Answers:
Answer 2, 3, 4, and 5: LC III, acetabular fracture, vertical shear, and combined
mechanism injuries all have lower mortality rates than APC injuries.
APC injuries have high rates of concomitant thoracic and abdominal visceral injuries leading to the highest rates of mortality among pelvic fractures. Lateral compression (LC) fractures have particularly high incidences of associated brain and head injury with lower mortality than APC injuries. Overall, as the grade of pelvic ring injury increases the rates of associated injuries increases, regardless of exact mechanism of injury. The overall mortality rate for any pelvic trauma is roughly 15%, with APC III mortality around 37%, and overall
APC mortality rates around 26%. LC of any grade has an estimated mortality around 13%. Vertical shear and CMI have estimated mortality of 25% and 17.1%, respectively. The lowest mortality rates are following acetabular fractures with estimates around 1.5%.
Dalal et al retrospectively reviewed 340 trauma patients with pelvic injuries to analyze organ injury, resuscitative requirements, and outcomes. They found the highest mortality rates were in APC III and that more severe APC injuries had greater organ damage and mortality. They conclude that the mechanical force type and classification of injury are predictors of organ injury pattern, resuscitation needs, and mortality.
Eastridge et al reviewed 1,014 injured pedestrians for pelvic injuries, associated injuries, and relationship of treatments to outcomes. They found the highest mortality rates were associated with APC III and LC III injuries patterns at 50%. They conclude that pelvic fractures are a sign of significant energy imparted on the body and severity of associated injuries lead to the high rates of morbidity and mortality.
Illustration A and B show an APC III and LC III injury, respectively. Incorrect Answers:
Answer 2, 3, 4, and 5: LC III, acetabular fracture, vertical shear, and combined
mechanism injuries all have lower mortality rates than APC injuries.
Question 10High Yield
A patient has sustained the injury shown in the MRI scan in Figure

Explanation
■
The MRI cervical spine scan reveals a C4-C5 traumatic anterolisthesis with severe spinal stenosis. There is evidence of spinal cord swelling and myelomalacia at this level. A physical examination is provided. The ASIA scale provides grading of severity of a spinal cord injury.
The grading incorporates strength and motor function based on the spinal level.
ASIA A is a complete spinal cord injury with no motor or sensory function. ASIA B is an incomplete spinal cord injury with no motor function below the spinal level of injury and sacral sparing of sensation. ASIA C is an incomplete spinal cord injury with motor function <3 of 5 in more than half of the muscles below the spinal level of injury. ASIA D is an incomplete spinal cord injury with motor function >3 of 5 in at least half of the muscles below the spinal level of injury. ASIA E is normal sensation and motor function.
The MRI cervical spine scan reveals a C4-C5 traumatic anterolisthesis with severe spinal stenosis. There is evidence of spinal cord swelling and myelomalacia at this level. A physical examination is provided. The ASIA scale provides grading of severity of a spinal cord injury.
The grading incorporates strength and motor function based on the spinal level.
ASIA A is a complete spinal cord injury with no motor or sensory function. ASIA B is an incomplete spinal cord injury with no motor function below the spinal level of injury and sacral sparing of sensation. ASIA C is an incomplete spinal cord injury with motor function <3 of 5 in more than half of the muscles below the spinal level of injury. ASIA D is an incomplete spinal cord injury with motor function >3 of 5 in at least half of the muscles below the spinal level of injury. ASIA E is normal sensation and motor function.
Question 11High Yield
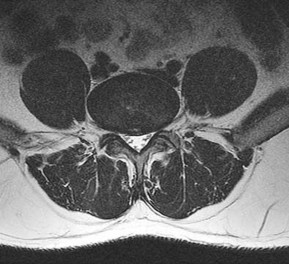
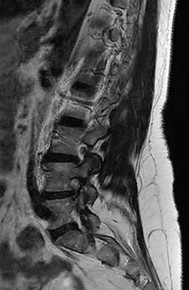
A 50-year-old woman undergoes an L4-S1 laminectomy and noninstrumented fusion for degenerative spondylolisthesis.
Explanation
Complications are numerous in adult spinal deformity surgery. Many complications are related to the patient's sagittal balance following surgery and recognition of the potential to develop sagittal imbalance or flat-back syndrome following spinal fusion. The quality of bone density is important in spinal instrumented fusions, especially among older patients. Patients with osteopenia or osteoporosis have a higher incidence of proximal-level screw cut-out through the vertebral body into the cephalad disk space.
Proximal junctional kyphosis is common in longer instrumented fusions, especially when instrumented to the sacrum/pelvis; when the spine is fixed in a "flat" or hypolordotic position; when the thoracic spine is hyperkyphotic (ie, Scheuermann kyphosis); when the end instrumented vertebrae is kyphotic; or when the sagittal plumb line (measured from C7) is more than 4 cm forward of the posterior corner of the sacrum.
Sagittal imbalance is a common complication when the spine is instrumented in a hypolordotic position. This can occur with degenerative conditions that necessitate multilevel fusions or fusions to sacrum without recognition of the degree of lordosis the patient should have. Pelvic incidence (PI) is a spinopelvic measurement that is a constant that measures an angle from the hips to the midpoint of the sacral end plate. PI correlates to the amount of lumbar lordosis that a patient would typically have in an upright position (+/-10 degrees). If a patient has significant sagittal imbalance, he or she will have a forward lean and lack the ability to extend the spine to stand upright. In an attempt to stand upright, the patient may bend his or her knees or hips in a crouched position. When extending their knees, they again lean forward.
Pseudarthrosis is common with noninstrumented fusions. Deep surgical-site infections are uncommon but can be major complications that are difficult to treat, necessitating formal irrigation and debridement and long-term antibiotics. Patients with diabetes have a higher incidence of infection.
RECOMMENDED READINGS
Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005 Sep 15;30(18):2024-
[9/. PubMed PMID: 16166889.](http://www.ncbi.nlm.nih.gov/pubmed/16166889)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16166889)
[Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. Sagittal thoracic decompensation following long adult lumbar spinal instrumentation and fusion to L5 or S1: causes, prevalence, and risk factor analysis. Spine (Phila Pa 1976). 2006 Sep 15;31(20):2359-66. PubMed PMID: 16985465.](http://www.ncbi.nlm.nih.gov/pubmed/16985465)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16985465)
Proximal junctional kyphosis is common in longer instrumented fusions, especially when instrumented to the sacrum/pelvis; when the spine is fixed in a "flat" or hypolordotic position; when the thoracic spine is hyperkyphotic (ie, Scheuermann kyphosis); when the end instrumented vertebrae is kyphotic; or when the sagittal plumb line (measured from C7) is more than 4 cm forward of the posterior corner of the sacrum.
Sagittal imbalance is a common complication when the spine is instrumented in a hypolordotic position. This can occur with degenerative conditions that necessitate multilevel fusions or fusions to sacrum without recognition of the degree of lordosis the patient should have. Pelvic incidence (PI) is a spinopelvic measurement that is a constant that measures an angle from the hips to the midpoint of the sacral end plate. PI correlates to the amount of lumbar lordosis that a patient would typically have in an upright position (+/-10 degrees). If a patient has significant sagittal imbalance, he or she will have a forward lean and lack the ability to extend the spine to stand upright. In an attempt to stand upright, the patient may bend his or her knees or hips in a crouched position. When extending their knees, they again lean forward.
Pseudarthrosis is common with noninstrumented fusions. Deep surgical-site infections are uncommon but can be major complications that are difficult to treat, necessitating formal irrigation and debridement and long-term antibiotics. Patients with diabetes have a higher incidence of infection.
RECOMMENDED READINGS
Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005 Sep 15;30(18):2024-
[9/. PubMed PMID: 16166889.](http://www.ncbi.nlm.nih.gov/pubmed/16166889)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16166889)
[Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. Sagittal thoracic decompensation following long adult lumbar spinal instrumentation and fusion to L5 or S1: causes, prevalence, and risk factor analysis. Spine (Phila Pa 1976). 2006 Sep 15;31(20):2359-66. PubMed PMID: 16985465.](http://www.ncbi.nlm.nih.gov/pubmed/16985465)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16985465)
Question 12High Yield
A 68-year-old woman underwent an uncemented medial/lateral tapered femoral placement during a total
hip arthroplasty. The orthopaedic surgeon noticed a nondisplaced vertical fracture in the calcar region of the femoral neck during final implant insertion. What is the most appropriate treatment?
hip arthroplasty. The orthopaedic surgeon noticed a nondisplaced vertical fracture in the calcar region of the femoral neck during final implant insertion. What is the most appropriate treatment?
Explanation
The recognized treatment for a proximal periprosthetic fracture is to first identify the extent and then optimize the correction of the fracture. Several studies indicate that proximal cerclage wiring is adequate to create "barrel hoop" stability of the proximal femur. Braided cables offer superior stability compared with twisted wires or Luque wires. Finally, the appropriate postoperative treatment is protected
weight bearing for 6 weeks, with periodic radiographs taken at 2-week intervals. Other options such as
cementing the femoral stem and using a revision arthroplasty device are indicated for unstable fractures.
weight bearing for 6 weeks, with periodic radiographs taken at 2-week intervals. Other options such as
cementing the femoral stem and using a revision arthroplasty device are indicated for unstable fractures.
Question 13High Yield
A 34-year-old man underwent a transtibial amputation as the result of a work-related injury. The amputation was performed at the inferior level of the tibial tubercle. The residual limb has a soft-tissue envelope composed of gastrocnemius muscle that is used as soft-tissue cushioning for the distal tibia. Despite undergoing several prosthetic fittings, he continues to report pain and instability. Examination reveals that the prosthesis appears to fit well with no apparent pressure points or areas of skin breakdown. He is not willing to have any further surgery. Which of the following modifications will most likely provide relief?
Explanation
While transtibial amputees can be fitted with a prosthesis with a residual limb as short as 5 cm, or with retention of the insertion of the patellar tendon, this patient has an unstable gait because of the limited ability of the prosthetic socket to maintain a snug and stable fit. While cumbersome and bulky, double metal uprights and a corset is the only predictable method of gaining stability. The other methods attempt to add an element of stability; however, they are unlikely to be successful.
REFERENCES: Bowker JH, Goldberg B, Poonekar PD: Transtibial amputation: Surgical procedures and postsurgical management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 429-452.
Kapp S, Cummings D: Transtibial amputation: Prosthetic management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 453-478.
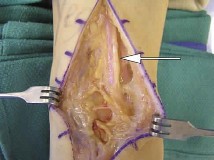
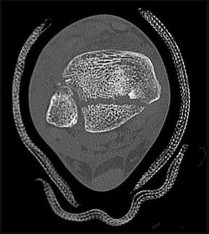
85. A 30-year-old man has had intermittent swelling of his right ankle for the past 6 months. He denies any history of trauma. Radiographs reveal osteolytic changes on both sides of the joint. An axial CT scan and a T2-weighted MRI scan are shown in Figures 40a and 40b. He undergoes surgical excision. An intraoperative photograph and a biopsy specimen are shown in Figures 40c and 40d. What is the most likely diagnosis?
1- Synovial sarcoma
2- Infection
3- Pigmented villonodular synovitis
4- Malignant fibrous histiocytoma
5- Synovial chondromatosis
PREFERRED RESPONSE: 3
DISCUSSION: Pigmented villonodular synovitis often presents with intermittent swelling and minimal pain. It often occurs around joints but may be found around tendon sheaths and bursal linings. Periarticular erosions involving both sides of joints are typical, and multiple joint involvement has been described. Portions of low-signal intensity on T1/- and T2-weighted images are characteristic of hemosiderin-laden processes. High-signal content is suggestive of high water content. The combination of low-signal intensity areas in intra-articular lesions with or without osseous destruction is diagnostic of pigmented villonodular synovitis. Aspiration reveals bloody or brownish fluid. The treatment of choice is synovectomy performed arthroscopically or open. Recurrence is common.
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Simon M, Springfield D: Surgery for the Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 36.
REFERENCES: Bowker JH, Goldberg B, Poonekar PD: Transtibial amputation: Surgical procedures and postsurgical management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 429-452.
Kapp S, Cummings D: Transtibial amputation: Prosthetic management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 453-478.
85. A 30-year-old man has had intermittent swelling of his right ankle for the past 6 months. He denies any history of trauma. Radiographs reveal osteolytic changes on both sides of the joint. An axial CT scan and a T2-weighted MRI scan are shown in Figures 40a and 40b. He undergoes surgical excision. An intraoperative photograph and a biopsy specimen are shown in Figures 40c and 40d. What is the most likely diagnosis?
1- Synovial sarcoma
2- Infection
3- Pigmented villonodular synovitis
4- Malignant fibrous histiocytoma
5- Synovial chondromatosis
PREFERRED RESPONSE: 3
DISCUSSION: Pigmented villonodular synovitis often presents with intermittent swelling and minimal pain. It often occurs around joints but may be found around tendon sheaths and bursal linings. Periarticular erosions involving both sides of joints are typical, and multiple joint involvement has been described. Portions of low-signal intensity on T1/- and T2-weighted images are characteristic of hemosiderin-laden processes. High-signal content is suggestive of high water content. The combination of low-signal intensity areas in intra-articular lesions with or without osseous destruction is diagnostic of pigmented villonodular synovitis. Aspiration reveals bloody or brownish fluid. The treatment of choice is synovectomy performed arthroscopically or open. Recurrence is common.
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Simon M, Springfield D: Surgery for the Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 36.
Question 14High Yield
The family is curious about the likelihood that the condition could worsen. What is the main risk factor for progression of this condition?
Explanation
- Age
Question 15High Yield
Figures 1 through 3 show the radiographs obtained from an 86-year-old- woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
73
73
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 16High Yield
A patient with degenerative osteoarthritis of the sternoclavicular (SC) joint reports constant pain, discomfort, and marked prominence and instability of the SC joint following medial clavicle resection. Which of the following procedures is most likely to produce these signs and symptoms?**
Explanation
Medial clavicle excision alone can be associated with postoperative instability of the clavicle. The clavicle should be stabilized to the first rib by reconstructing the costoclavicular ligament if it is torn or if the resection is lateral to its clavicular insertion. Therefore, care must be taken to resect only that part of the clavicle that is medial to the costoclavicular ligament. Adequate protection for vital structures that lie posterior to the medial end of the clavicle must be provided.
REFERENCES: Bremner RA: Nonarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 583-586.
REFERENCES: Bremner RA: Nonarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 583-586.
Question 17High Yield
Which structures are often encountered and may need to be mobilized in the surgical treatment of the injury shown in Figure 59?
Explanation
_
The CT scan shows a large posterior malleolar fracture that necessitates open reduction and internal fixation. The best approach to this fragment is posterolateral to the ankle, which necessitates an incision over the posterolateral ankle roughly halfway between the fibula and the Achilles tendon. In that interval, the sural nerve runs with the lesser saphenous vein, both of which often need to be mobilized.
The greater saphenous vein and the saphenous nerve run along the medial aspect of the ankle. The superficial peroneal nerve is anterolateral at this level.
RECOMMENDED READINGS
8. [Jowett AJ, Sheikh FT, Carare RO, Goodwin MI. Location of the sural nerve during posterolateral approach to the ankle. Foot Ankle Int. 2010 Oct;31(10):880-3. doi: 10.3113/FAI.2010.0880. PubMed PMID: 20964966.](http://www.ncbi.nlm.nih.gov/pubmed/20964966)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20964966)
9. Franzone JM, Vosseller JT. Posterolateral approach for open reduction and internal fixation of a posterior malleolus fracture--hinging on an intact PITFL to disimpact the tibial plafond: a technical note. Foot Ankle Int. 2013 Aug;34(8):1177-81. doi: 10.1177/1071100713481455. Epub 2013 Mar 12.
[PubMed PMID: 23481092. ](http://www.ncbi.nlm.nih.gov/pubmed/23481092)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23481092)
The CT scan shows a large posterior malleolar fracture that necessitates open reduction and internal fixation. The best approach to this fragment is posterolateral to the ankle, which necessitates an incision over the posterolateral ankle roughly halfway between the fibula and the Achilles tendon. In that interval, the sural nerve runs with the lesser saphenous vein, both of which often need to be mobilized.
The greater saphenous vein and the saphenous nerve run along the medial aspect of the ankle. The superficial peroneal nerve is anterolateral at this level.
RECOMMENDED READINGS
8. [Jowett AJ, Sheikh FT, Carare RO, Goodwin MI. Location of the sural nerve during posterolateral approach to the ankle. Foot Ankle Int. 2010 Oct;31(10):880-3. doi: 10.3113/FAI.2010.0880. PubMed PMID: 20964966.](http://www.ncbi.nlm.nih.gov/pubmed/20964966)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20964966)
9. Franzone JM, Vosseller JT. Posterolateral approach for open reduction and internal fixation of a posterior malleolus fracture--hinging on an intact PITFL to disimpact the tibial plafond: a technical note. Foot Ankle Int. 2013 Aug;34(8):1177-81. doi: 10.1177/1071100713481455. Epub 2013 Mar 12.
[PubMed PMID: 23481092. ](http://www.ncbi.nlm.nih.gov/pubmed/23481092)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23481092)
Question 18High Yield
A 16-year-old high school football player who sustained an acute forceful dorsiflexion ankle injury reported that he felt a pop and then noted immediate swelling over the lateral malleolus. Examination 24 hours later reveals moderate swelling and tenderness along the lateral malleolus. The external rotation, squeeze, anterior drawer, and talar tilt tests are negative. Subluxation of the peroneal tendons is palpable over the peroneal groove of the fibula. Radiographs reveal a small cortical avulsion off the distal rim of the fibula. The stress views show no instability. Initial management for this injury should include
Explanation
The patient has an acute peroneal tendon dislocation. The evaluation for syndesmotic injury and lateral ankle instability is negative. The cortical avulsion off the distal tip of the lateral malleolus, a rim fracture, is characteristic of peroneal tendon dislocations. The sensation of apprehension or frank subluxation of the peroneal tendons with active dorsiflexion of the foot while the foot is held in plantar flexion confirms the diagnosis. Based on these findings, initial management should consist of cast immobilization and protected weight bearing. If a recurrent or chronic condition develops, surgery is the most reliable treatment option.
REFERENCES: Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Marti R: Dislocation of the peroneal tendons. Am J Sports Med 1977;5:19-22.
REFERENCES: Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Marti R: Dislocation of the peroneal tendons. Am J Sports Med 1977;5:19-22.
Question 19High Yield
In an acute closed boutonniere injury, what is the most appropriate splinting technique for the proximal interphalangeal joint?
Explanation
Rupture of the central slip of the extensor mechanism and a varying degree of lateral band volar migration are the pathologic entities in an acute boutonniere injury. Splinting the proximal interphalangeal joint in full extension allows reapproximation of the central slip to the base of the middle phalanx. Distal interphalangeal joint flexion is permitted to allow movement of the lateral bands distally and dorsally, preventing contracture.
REFERENCES: Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
Lovet WL, McCalla MA: Management and rehabilitation of extensor tendon injuries. Orthop Clin North Am 1983;14:811-826.
REFERENCES: Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
Lovet WL, McCalla MA: Management and rehabilitation of extensor tendon injuries. Orthop Clin North Am 1983;14:811-826.
Question 20High Yield
A 21-year-old collegiate female cross-country athlete reports right hip pain that begins about 12 miles into a run, followed by pain resolution when she discontinues running. However, each time she tries to resume a running program, she experiences recurrence of pain deep in the anterior groin. A plain radiograph and MRI scan are shown in Figures 8a and 8b. Management should consist of
Explanation
The history is consistent with a stress fracture. Findings on the plain radiograph are marginal, but the MRI scan shows evidence of stress reaction in the medial neck of the femur (compression side). A lesion on the compression side is not normally at risk for displacement and usually can be managed nonsurgically. A bone scan would further identify the lesion but is not necessary. A skeletal survey and chest radiograph are used in staging a tumor. Radioisotope injection and guided biopsy are sometimes used for osteoid osteomas.
REFERENCES: Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Lynch SA, Renstrom PA: Groin injuries in sport: Treatment strategies. Sports Med 1999;28:137-144.
REFERENCES: Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Lynch SA, Renstrom PA: Groin injuries in sport: Treatment strategies. Sports Med 1999;28:137-144.
Question 21High Yield
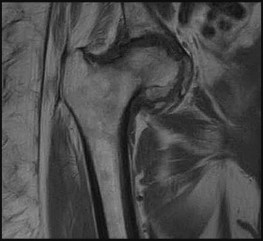
Figure 66
Explanation
Figure 61 reveals transient osteoporosis of the left hip. This is a T1-weighted image of the pelvis with generalized low-intensity signal of the bone marrow in the left femoral head. A T2-weighted
image would show high-intensity signal in a similar distribution. These changes signify an increase in bone marrow edema. On occasion, a subchondral insufficiency fracture is seen, but collapse of the femoral head should not occur with transient osteoporosis of the hip. It is seen most commonly in healthy middle-age men and in women during the third trimester of pregnancy. Hip pain is the most common symptom, and this typically lasts 6 to 8 months. Complete resolution of symptoms without long-term sequelae is the rule with few exceptions.
Figure 62 shows chondrosarcoma of the pelvis. This is a T1-weighted image that reveals a large soft-tissue mass of low-signal intensity, signifying destruction of the left acetabulum with medial protrusion of the left femoral head into the pelvis. These tumors occur typically in adults and are usually located in the proximal femur, ilium, or the periacetabular regions.
Figure 63 shows a superior acetabular labral tear. This is a T2-weighted image of the left hip after administration of intra-articular contrast. The distension of the joint with contrast shows the separation of the superior labrum from the bony acetabular rim.
Figure 64 shows end-stage osteonecrosis of the left femoral head. This is a T1-weighted image of the left hip with low-intensity signal, signifying bone marrow edema and femoral head collapse. There is a bandlike low signal intensity line that is characteristically seen on T1-weighted images. This represents the zone of demarcation between the viable and necrotic bone. The most common risk factors for osteonecrosis are heavy alcohol intake and chronic glucocorticoid use.
Figure 65 shows a T1-weighted image of a dysplastic right hip. A shallow acetabulum is present with approximately 40% uncoverage of the right femoral head. A shallow fovea on the femoral head and a hyperplastic superior labrum also are seen.
Figure 66 shows a T1-weighted image of a nondisplaced right femoral neck fracture. The fracture line is seen in the subcapital region of the femoral neck, and there is low-signal intensity signifying surrounding bone edema. Plain radiographs are negative in 8% of femoral neck fractures, and MRI has been shown to be 99% sensitive.
RECOMMENDED READINGS
1. [Korompilias AV, Karantanas AH, Lykissas MG, Beris AE. Transient osteoporosis. J Am Acad Orthop Surg. 2008 Aug;16(8):480-9. Review. PubMed PMID: 18664637. ](http://www.ncbi.nlm.nih.gov/pubmed/18664637)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18664637)
2. [Hartley KG, Damon BM, Patterson GT, Long JH, Holt GE. MRI techniques: a review and update for the orthopaedic surgeon. J Am Acad Orthop Surg. 2012 Dec;20(12):775-87. doi: 10.5435/JAAOS-20-12-775. Review. PubMed PMID: 23203937. ](http://www.ncbi.nlm.nih.gov/pubmed/23203937)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23203937)
3. Potter HG, Sou IT. Magnetic resonance imaging. In: Callaghan JJ, Rosenberg AG, Rubash HE, eds. _The Adult Hip_. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:409-422.
image would show high-intensity signal in a similar distribution. These changes signify an increase in bone marrow edema. On occasion, a subchondral insufficiency fracture is seen, but collapse of the femoral head should not occur with transient osteoporosis of the hip. It is seen most commonly in healthy middle-age men and in women during the third trimester of pregnancy. Hip pain is the most common symptom, and this typically lasts 6 to 8 months. Complete resolution of symptoms without long-term sequelae is the rule with few exceptions.
Figure 62 shows chondrosarcoma of the pelvis. This is a T1-weighted image that reveals a large soft-tissue mass of low-signal intensity, signifying destruction of the left acetabulum with medial protrusion of the left femoral head into the pelvis. These tumors occur typically in adults and are usually located in the proximal femur, ilium, or the periacetabular regions.
Figure 63 shows a superior acetabular labral tear. This is a T2-weighted image of the left hip after administration of intra-articular contrast. The distension of the joint with contrast shows the separation of the superior labrum from the bony acetabular rim.
Figure 64 shows end-stage osteonecrosis of the left femoral head. This is a T1-weighted image of the left hip with low-intensity signal, signifying bone marrow edema and femoral head collapse. There is a bandlike low signal intensity line that is characteristically seen on T1-weighted images. This represents the zone of demarcation between the viable and necrotic bone. The most common risk factors for osteonecrosis are heavy alcohol intake and chronic glucocorticoid use.
Figure 65 shows a T1-weighted image of a dysplastic right hip. A shallow acetabulum is present with approximately 40% uncoverage of the right femoral head. A shallow fovea on the femoral head and a hyperplastic superior labrum also are seen.
Figure 66 shows a T1-weighted image of a nondisplaced right femoral neck fracture. The fracture line is seen in the subcapital region of the femoral neck, and there is low-signal intensity signifying surrounding bone edema. Plain radiographs are negative in 8% of femoral neck fractures, and MRI has been shown to be 99% sensitive.
RECOMMENDED READINGS
1. [Korompilias AV, Karantanas AH, Lykissas MG, Beris AE. Transient osteoporosis. J Am Acad Orthop Surg. 2008 Aug;16(8):480-9. Review. PubMed PMID: 18664637. ](http://www.ncbi.nlm.nih.gov/pubmed/18664637)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18664637)
2. [Hartley KG, Damon BM, Patterson GT, Long JH, Holt GE. MRI techniques: a review and update for the orthopaedic surgeon. J Am Acad Orthop Surg. 2012 Dec;20(12):775-87. doi: 10.5435/JAAOS-20-12-775. Review. PubMed PMID: 23203937. ](http://www.ncbi.nlm.nih.gov/pubmed/23203937)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23203937)
3. Potter HG, Sou IT. Magnetic resonance imaging. In: Callaghan JJ, Rosenberg AG, Rubash HE, eds. _The Adult Hip_. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:409-422.
Question 22High Yield
64
What is the optimal biomechanical screw placement position to treat a waist-level scaphoid fracture?
What is the optimal biomechanical screw placement position to treat a waist-level scaphoid fracture?






Explanation
Dodds and associates looked at short (compared to long) scaphoid screws placed down the central axis in cadavers. A long screw placed along the central axis was significantly more stable when tested in all planes of motion about the wrist. McCallister and associates examined central placement and eccentric placement in a cadaver model. Central positioning produced 43% more stiffness and 113% more load (P < .01).
RECOMMENDED READINGS
1. [Bedi A, Jebson PJ, Hayden RJ, Jacobson JA, Martus JE. Internal fixation of acute, nondisplaced scaphoid waist fractures via a limited dorsal approach: an assessment of radiographic and functional outcomes. J Hand Surg Am. 2007 Mar;32(3):326-33. PubMed PMID: 17336838.](http://www.ncbi.nlm.nih.gov/pubmed/17336838)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17336838)
2. [Dodds SD, Panjabi MM, Slade JF 3rd. Screw fixation of scaphoid fractures: a biomechanical assessment of screw length and screw augmentation. J Hand Surg Am. 2006 Mar;31(3):405-13. PubMed PMID: 16516734. ](http://www.ncbi.nlm.nih.gov/pubmed/16516734)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16516734)
3. [McCallister WV, Knight J, Kaliappan R, Trumble TE. Central placement of the screw in simulated fractures of the scaphoid waist: a biomechanical study. J Bone Joint Surg Am.2003 Jan;85-A(1):72-7.PubMed: 12533575.](http://www.ncbi.nlm.nih.gov/pubmed/12533575)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12533575)
RESPONSES FOR QUESTIONS 72 THROUGH 75
The figures listed above depict the scenarios described below. Please match the appropriate scenarios and figures.
65
A B
C
D
E F
66
G H
RECOMMENDED READINGS
1. [Bedi A, Jebson PJ, Hayden RJ, Jacobson JA, Martus JE. Internal fixation of acute, nondisplaced scaphoid waist fractures via a limited dorsal approach: an assessment of radiographic and functional outcomes. J Hand Surg Am. 2007 Mar;32(3):326-33. PubMed PMID: 17336838.](http://www.ncbi.nlm.nih.gov/pubmed/17336838)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17336838)
2. [Dodds SD, Panjabi MM, Slade JF 3rd. Screw fixation of scaphoid fractures: a biomechanical assessment of screw length and screw augmentation. J Hand Surg Am. 2006 Mar;31(3):405-13. PubMed PMID: 16516734. ](http://www.ncbi.nlm.nih.gov/pubmed/16516734)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16516734)
3. [McCallister WV, Knight J, Kaliappan R, Trumble TE. Central placement of the screw in simulated fractures of the scaphoid waist: a biomechanical study. J Bone Joint Surg Am.2003 Jan;85-A(1):72-7.PubMed: 12533575.](http://www.ncbi.nlm.nih.gov/pubmed/12533575)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12533575)
RESPONSES FOR QUESTIONS 72 THROUGH 75
The figures listed above depict the scenarios described below. Please match the appropriate scenarios and figures.
65
A B
C
D
E F
66
G H
Question 23High Yield
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
The patient has a pectoralis major rupture, an injury that occurs most commonly during weight lifting. Grade III injuries represent complete tears of either the musculotendinous junction or an avulsion of the tendon from the humerus, the most common injury site. Examination will most likely reveal ecchymoses and swelling in the proximal arm and axilla, and strength testing will show weakness with internal rotation and in adduction and forward flexion. Axillary webbing, caused by a more defined inferior margin of the anterior deltoid as the result of rupture of the pectoralis, can be seen as the swelling diminishes. Surgical repair is the treatment of choice for complete ruptures. Nonsurgical treatment is associated with significant losses in adduction, flexion, internal rotation, strength, and peak torque. The pectoralis major originates from the proximal clavicle and the border of the sternum, including ribs two through six. The pectoralis major inserts (rather than originates) on the humerus. The coracoid process is the insertion site for the pectoralis minor, as well as the origin for the conjoined tendon. The pectoralis major has no attachment or origin from the scapula. The anterior deltoid originates from the lateral one third of the clavicle and the anterior acromion.
REFERENCES: Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
REFERENCES: Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Question 24High Yield
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?
Explanation
The patient has a volar displaced two-part intra-articular distal radial fracture-dislocation of the wrist. Although a closed reduction is usually easily obtained, it is very difficult to maintain the reduction without internal fixation. The approach is determined by the direction of the dislocation, in this case volar. Stabilization with a buttress plate neutralizes the axial loading forces on the fractured fragment. A dorsal placed angular stable plate will not provide this buttress effect and will make the reduction difficult.
REFERENCE: Cohen M, McMurtry RY, Jupiter JB: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1328-1335.
REFERENCE: Cohen M, McMurtry RY, Jupiter JB: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1328-1335.
Question 25High Yield
The lesion seen in the MRI scan in Figure 1 is treated with a marrow stimulation technique. The reparative tissue formed by this technique is predominantly composed of
Explanation
The MRI scan shows a full-thickness cartilage defect. When treated with a marrow stimulation technique, such as a microfracture, the reparative tissue is fibrocartilage. Unlike hyaline cartilage, which is composed of only type 2 collagen, fibrocartilage is composed of both type 1 and type 2 collagen.
11
11
Question 26High Yield
When evaluating a patient with hallux rigidus, what is the most important clinical factor indicating the need for an arthrodesis as opposed to a cheilectomy?
Explanation
Cheilectomy has been shown to provide satisfactory pain relief and improved function in long-term studies. It is important to select patients appropriately when choosing a cheilectomy versus an arthrodesis. Pain at the midrange of motion and loss of more than 50% of the metatarsal head cartilage are predictors of a poor outcome following cheilectomy, and these patients should receive an arthrodesis.
REFERENCES: Coughlin MJ, Shurnas PS: Hallux rigidus: Grading and long-term results of operative treatment. J Bone Joint Surg Am 2003;85:2072-2088.
Easley ME, Davis WH, Anderson RB: Intermediate to long-term follow-up of medial-approach dorsal cheilectomy for hallux rigidus. Foot Ankle Int 1999;20:147-152.
REFERENCES: Coughlin MJ, Shurnas PS: Hallux rigidus: Grading and long-term results of operative treatment. J Bone Joint Surg Am 2003;85:2072-2088.
Easley ME, Davis WH, Anderson RB: Intermediate to long-term follow-up of medial-approach dorsal cheilectomy for hallux rigidus. Foot Ankle Int 1999;20:147-152.
Question 27High Yield
Figures 38a and 38b


Explanation
Inversion of the ankle can cause various injuries about the foot and ankle, all via the same mechanism. Fifth metatarsal base avulsion (Figure 35) fractures can be treated with use of a walking boot until pain subsides. Jones fractures (Figure 36) can be treated with surgical or nonsurgical treatment, although young, active patients are perhaps better treated with ORIF, which can decrease disability time. Treatment of an anterior process calcaneus fracture (Figure 37) is similar to that for a fifth metatarsal base avulsion fracture. Figures 38a and 38b show a calcaneal fracture-dislocation, which necessitates ORIF.
RECOMMENDED READINGS
1. [View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23959223)
2. [Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012 Oct;43(10):1626-32. doi: 10.1016/j.injury.2012.03.010. Epub 2012 Mar 30. Review. PubMed PMID: 22465516. ](http://www.ncbi.nlm.nih.gov/pubmed/22465516)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22465516)
3. [Roche AJ, Calder JD. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2013 Jun;21(6):1307-15. doi: 10.1007/s00167-012-2138-8. Epub 2012 Sep 6. Review. PubMed PMID: 22956165. ](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[ ](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22956165)
4. [Berkowitz MJ, Kim DH. Process and tubercle fractures of the hindfoot. J Am Acad Orthop Surg. 2005 Dec;13(8):492-502. Review. PubMed PMID: 16330511. ](http://www.ncbi.nlm.nih.gov/pubmed/16330511)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16330511)
RECOMMENDED READINGS
1. [View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23959223)
2. [Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012 Oct;43(10):1626-32. doi: 10.1016/j.injury.2012.03.010. Epub 2012 Mar 30. Review. PubMed PMID: 22465516. ](http://www.ncbi.nlm.nih.gov/pubmed/22465516)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22465516)
3. [Roche AJ, Calder JD. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2013 Jun;21(6):1307-15. doi: 10.1007/s00167-012-2138-8. Epub 2012 Sep 6. Review. PubMed PMID: 22956165. ](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[ ](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22956165)
4. [Berkowitz MJ, Kim DH. Process and tubercle fractures of the hindfoot. J Am Acad Orthop Surg. 2005 Dec;13(8):492-502. Review. PubMed PMID: 16330511. ](http://www.ncbi.nlm.nih.gov/pubmed/16330511)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16330511)
Question 28High Yield
A 23-year-old college basketball player reports persistent lateral ankle pain after sustaining an inversion injury 6 months ago. Examination reveals pain over the anterolateral ankle, absence of swelling, and no clinical instability. Management consisting of vigorous physical therapy fails to provide relief, and a intra-articular corticosteroid injection provides only temporary relief. Radiographs obtained at the time of injury and subsequent AP and varus stress views are normal. A recent MRI scan fails to show any abnormalities. Management should now include
Explanation
Because the patient has failed to respond to appropriate nonsurgical management and imaging studies are normal, the use of arthroscopy not only aids in the diagnosis of chronic ankle pain, but is also helpful in its treatment. In patients with this condition, typical findings include synovitis in the lateral gutter and fibrosis along the talofibular articulation; syndesmosis chondromalacia of the talus and ankle also may be found. In patients with anterior soft-tissue impingement, approximately 84% who have a poor response to nonsurgical management will have a good to excellent response after arthroscopic synovectomy and debridement.
REFERENCES: Ferkel RD, Fasulo GJ: Arthroscopic treatment of ankle injuries. Orthop Clin North Am 1994;25:17-32.
Ferkel RD, Karzel RP, Del Pizzo W, Friedman MJ, Fischer SP: Arthroscopic treatment of anterolateral impingement of the ankle. Am J Sports Med 1991;19:440-446.
REFERENCES: Ferkel RD, Fasulo GJ: Arthroscopic treatment of ankle injuries. Orthop Clin North Am 1994;25:17-32.
Ferkel RD, Karzel RP, Del Pizzo W, Friedman MJ, Fischer SP: Arthroscopic treatment of anterolateral impingement of the ankle. Am J Sports Med 1991;19:440-446.
Question 29High Yield
Figures 1 through 5 are the radiographs and CT scans of a 59-year- old woman who has had 10 years of worsening right shoulder pain. She reports a progression of symptoms, despite multiple corticosteroid injections, nonsteroidal anti-inflammatory drugs, and physical therapy. Her active and passive forward elevation is 100°, external rotation with the arm at the side is 20°, and internal rotation is to L5. What is the best next step?
Explanation
62
The patient's radiographs and CT scan show advanced glenohumeral osteoarthritis with posterior humeral head subluxation and mild posterior glenoid erosion (Walch type B2 glenoid). The preferred type of shoulder arthroplasty in this setting remains controversial, as there are data to support both anatomic and reverse total shoulder arthroplasty. There is no significant atrophy of the rotator cuff musculature on sagittal CT to suggest a rotator cuff tear, and a rotator cuff repair is likely contraindicated by the degree of underlying arthritis. A glenohumeral joint debridement would be expected to provide only partial/short-term pain improvement, and is unlikely to be a long- term solution. A shoulder hemiarthroplasty has been shown to result in worse pain relief and functional outcomes than total shoulder arthroplasty in this setting.
The patient's radiographs and CT scan show advanced glenohumeral osteoarthritis with posterior humeral head subluxation and mild posterior glenoid erosion (Walch type B2 glenoid). The preferred type of shoulder arthroplasty in this setting remains controversial, as there are data to support both anatomic and reverse total shoulder arthroplasty. There is no significant atrophy of the rotator cuff musculature on sagittal CT to suggest a rotator cuff tear, and a rotator cuff repair is likely contraindicated by the degree of underlying arthritis. A glenohumeral joint debridement would be expected to provide only partial/short-term pain improvement, and is unlikely to be a long- term solution. A shoulder hemiarthroplasty has been shown to result in worse pain relief and functional outcomes than total shoulder arthroplasty in this setting.
Question 30High Yield
Which of the following molecules are present in a hematoma after a fracture and aid in modulating cell proliferation and differentiation:
Explanation
Important concepts to remember regarding signaling proteins include:
Indian hedgehog (IHH) and core binding factor alpha 1 (Cbfa1) influence embryoniCbone formation and fracture healing. Vascular endothelial growth factor (VEGF) plays a role in cartilage hypertrophy at the growth plate and during fracture healing.
Transforming growth factor-beta (TGF-B) and platelet derived growth factor (PDGF) are found in early fracture hematoma, and these factors modulate cell proliferation and differentiation.
Bone morphogenetiCprotein and interleukin 1 and 6 are expressed during cartilage formation. Correct Answer: Transforming growth factor-beta (TGF-B) and platelet derived growth factor (PDGF)
Indian hedgehog (IHH) and core binding factor alpha 1 (Cbfa1) influence embryoniCbone formation and fracture healing. Vascular endothelial growth factor (VEGF) plays a role in cartilage hypertrophy at the growth plate and during fracture healing.
Transforming growth factor-beta (TGF-B) and platelet derived growth factor (PDGF) are found in early fracture hematoma, and these factors modulate cell proliferation and differentiation.
Bone morphogenetiCprotein and interleukin 1 and 6 are expressed during cartilage formation. Correct Answer: Transforming growth factor-beta (TGF-B) and platelet derived growth factor (PDGF)
Question 31High Yield
A 75-year-old woman with rheumatoid arthritis and a long history of oral corticosteroid use sustains a comminuted intra-articular distal humerus fracture. What is the best surgical option?
Explanation
DISCUSSION:
TEA is the best surgical option. McKee and associates published a multicenter randomized controlled trial comparing ORIF with TEA in elderly patients. TEA resulted in better 2-year clinical functional scores and more predictable outcomes compared with ORIF. TEA was also likely to result in a lower resurgical rate; one- quarter of patients with fractures randomized to ORIF could not achieve stable fixation. Further, Frankle and associates reported a comparative study of TEA versus ORIF in 24 elderly women. TEA outcomes were again
superior to ORIF at a minimum of 2 years of follow-up. TEA was especially useful in patients with comorbidities that compromise bone stock, including osteoporosis and oral corticosteroid use. Closed
reduction and percutaneous pinning studies have not been published on the adult population.
DISCUSSION:
TEA is the best surgical option. McKee and associates published a multicenter randomized controlled trial comparing ORIF with TEA in elderly patients. TEA resulted in better 2-year clinical functional scores and more predictable outcomes compared with ORIF. TEA was also likely to result in a lower resurgical rate; one- quarter of patients with fractures randomized to ORIF could not achieve stable fixation. Further, Frankle and associates reported a comparative study of TEA versus ORIF in 24 elderly women. TEA outcomes were again
superior to ORIF at a minimum of 2 years of follow-up. TEA was especially useful in patients with comorbidities that compromise bone stock, including osteoporosis and oral corticosteroid use. Closed
reduction and percutaneous pinning studies have not been published on the adult population.
Question 32High Yield
A 45-year-old distance runner has a hyaluronic acid injection to his knee because of degenerative arthritis. He immediately develops a severe rash and a systemic hypersensitivity reaction. This patient most likely is also allergic to which of the following?
Explanation
DISCUSSION: Preparations of hyaluronic acid can be divided into low and high molecular weight compounds. Contraindications to intra-articular hyaluronic acid include joint or skin infection, overlying skin disease, and allergies to chicken or egg products if using a preparation derived from rooster comb.
REFERENCES: Gloyscen DN, Gillespie MJ, Schenek RC: The effects of medication in sports injuries, in DeLee JC, Drez D Jr, Miller MD (eds): Orthopedic Sports Medicine: Principles and Practice, ed 2.
Philadelphia, PA, WB Saunders, 2003, vol 1, pp 121-124.
Schenck RC Jr: New approaches to the treatment of osteoarthritis: Oral glucosamine and chondroitin sulfate. Instr Course Lect 2000;49:491-494.
DISCUSSION: Preparations of hyaluronic acid can be divided into low and high molecular weight compounds. Contraindications to intra-articular hyaluronic acid include joint or skin infection, overlying skin disease, and allergies to chicken or egg products if using a preparation derived from rooster comb.
REFERENCES: Gloyscen DN, Gillespie MJ, Schenek RC: The effects of medication in sports injuries, in DeLee JC, Drez D Jr, Miller MD (eds): Orthopedic Sports Medicine: Principles and Practice, ed 2.
Philadelphia, PA, WB Saunders, 2003, vol 1, pp 121-124.
Schenck RC Jr: New approaches to the treatment of osteoarthritis: Oral glucosamine and chondroitin sulfate. Instr Course Lect 2000;49:491-494.
Question 33High Yield
A 35-year-old man has substantial pain at the base of his dominant right thumb. Orthosis use, anti-inflammatory medication, and corticosteroid injections have failed to improve his symptoms. Which condition is a contraindication to the surgery shown in the radiograph (Figure 38)?

Explanation
There are multiple surgical options for treatment of symptomatic thumb carpometacarpal (CMC) joint arthritis, including trapeziectomy with or without suspensionplasty and with or without tendon interposition, prosthetic replacement, or arthrodesis. However, for a young manual laborer, a more robust solution is required so he can withstand the rigors of occupational activities. Arthrodesis of the CMC joint provides good pain relief but a relatively high nonunion rate (8%-21%). Presence of STT arthritis is a contraindication to CMC fusion because the STT joint will undergo increased stresses following CMC fusion, which will cause early failure of the surgical intervention. Bilateral thumb CMC fusions can be performed, and bilateral disease is not a contraindication to this procedure. Concomitant wrist arthritis does not preclude CMC fusion because this can be addressed with scaphoid excision and partial wrist fusion, which is not compromised by CMC fusion. Lack of MCP joint hyperextension does not preclude CMC fusion; substantial MCP hyperextension should be addressed at the time of arthroplasty for CMC arthritis with MCP fusion or volar capsulodesis.
RECOMMENDED READINGS
25. [Rizzo M, Moran SL, Shin AY. Long-term outcomes of trapeziometacarpal arthrodesis in the management of trapeziometacarpal arthritis. J Hand Surg Am. 2009 Jan; 34(1):20-6. doi: 10.1016/j.jhsa.2008.09.022. PubMed PMID: 19121726.](http://www.ncbi.nlm.nih.gov/pubmed/19121726)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19121726)
26. [Goldfarb CA, Stern PJ. Indications and techniques for thumb carpometacarpal arthrodesis. Tech Hand Up Extrem Surg. 2002 Dec;6(4):178-84. PubMed PMID: 16520598. ](http://www.ncbi.nlm.nih.gov/pubmed/16520598)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16520598)
RECOMMENDED READINGS
25. [Rizzo M, Moran SL, Shin AY. Long-term outcomes of trapeziometacarpal arthrodesis in the management of trapeziometacarpal arthritis. J Hand Surg Am. 2009 Jan; 34(1):20-6. doi: 10.1016/j.jhsa.2008.09.022. PubMed PMID: 19121726.](http://www.ncbi.nlm.nih.gov/pubmed/19121726)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19121726)
26. [Goldfarb CA, Stern PJ. Indications and techniques for thumb carpometacarpal arthrodesis. Tech Hand Up Extrem Surg. 2002 Dec;6(4):178-84. PubMed PMID: 16520598. ](http://www.ncbi.nlm.nih.gov/pubmed/16520598)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16520598)
Question 34High Yield
Which of the following is considered the appropriate initial management protocol for an unconscious football player without spontaneous respirations?
Explanation
The on-field evaluation and management of the seriously injured athlete requires advance preparation and planning. It is imperative that the health care team have a game plan in place and the proper equipment readily available. The initial step consists of stabilizing the head and neck by manually holding the head and neck in a neutral position. Then, in the following order, check for breathing, pulses, and level of consciousness. If the athlete is breathing, simply remove the mouth guard and maintain the airway. If the athlete is not breathing, the face mask must be removed and the chin strap left in place. An open airway must be established, followed by assisted breathing. CPR is only instituted when breathing and circulation are compromised. If the athlete is unconcious or has a suspected cervical spine injury, the helmet must not be removed until the athlete has been transported to an appropriate facility and the cervical spine has been completely evaluated.
REFERENCES: McSwain NE, Garnelli RL: Helmet removal from injured patients. Bull Am Coll Surg 1997;82:42-44.
Vegso JJ, Lehman RC: Field evaluation and management of head and neck injuries. Clin Sports Med 1987;6:1-15.
Arndt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-101.
REFERENCES: McSwain NE, Garnelli RL: Helmet removal from injured patients. Bull Am Coll Surg 1997;82:42-44.
Vegso JJ, Lehman RC: Field evaluation and management of head and neck injuries. Clin Sports Med 1987;6:1-15.
Arndt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-101.
Question 35High Yield
All of the following may be seen with preganglionic lesion EXC EPT:
Explanation
Tinel sign is seen with postganglionic lesions.
Question 36High Yield
In addition to physical therapy, what is the best course of treatment at this time?
Explanation
- Ankle-foot orthosis
Question 37High Yield
After performing an uneventful partial palmar fasciectomy for Dupuytren contracture of the palm and ring finger, a general postsurgical pain medication prescription should include how many narcotic pills?
Explanation
After the designation of pain as the fifth vital sign, opioid analgesic use has steadily increased. Many surgeons routinely prescribe 30 or more pills after elective hand surgery. However, studies show that patients generally use fewer than 30 pills. Patients who underwent bone procedures used 14 pills, and those undergoing soft-tissue procedures used 9 pills. Education and decision aids may help physicians size prescriptions appropriately to avoid overmedication. Patients undergoing small soft-tissue surgeries such as trigger releases should not need narcotics. Those undergoing small-joint surgeries, carpal tunnel releases, and Dupuytren fasciectomy may benefit from a prescription of 10 pills. More extensive surgery, such as open fracture treatment, may justify more pills, but prescriptions should not exceed 40 tablets _under typical circumstances._
Question 38High Yield
Figures 1a and 1b are the MR images of a 69-year-old woman with bilateral leg pain that is worse with ambulation. She feels better when she is sitting down or leaning on a grocery cart. Which condition or structure is indicated by the arrows?

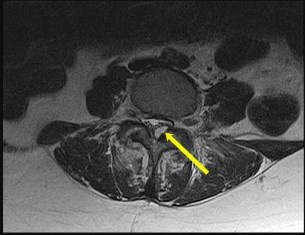
Explanation
This patient has neurogenic claudication as demonstrated by her “shopping cart” sign. Typically, spinal stenosis is attributable to bony spurs and/or a thick ligamentum flavum. However, for this patient, a large synovial cyst is the main contributing factor to stenosis. A cyst typically is filled with gelatinous material. If symptomatic, surgical excision is typically recommended because success with aspiration is unreliable. The need for fusion is debatable.
A disk herniation is not bright on T2. An arachnoid cyst is a sac filled with cerebrospinal fluid. Spinal arachnoid cysts are relatively uncommon, and typically are intradural, but they also can be extradural. Epidural lipomatosis is a condition caused by excessive accumulation of fat within the epidural space. It is not well circumscribed as seen with this lesion.
RECOMMENDED READINGS
1. [Epstein NE, Baisden J. The diagnosis and management of synovial cysts: Efficacy of surgery versus cyst aspiration. Surg Neurol Int. 2012;3(Suppl 3):S157-66. doi: 10.4103/2152-7806.98576. Epub 2012 Jul 17. PubMed PMID: 22905322. ](http://www.ncbi.nlm.nih.gov/pubmed/22905322)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22905322)
2. [View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20173680)
A disk herniation is not bright on T2. An arachnoid cyst is a sac filled with cerebrospinal fluid. Spinal arachnoid cysts are relatively uncommon, and typically are intradural, but they also can be extradural. Epidural lipomatosis is a condition caused by excessive accumulation of fat within the epidural space. It is not well circumscribed as seen with this lesion.
RECOMMENDED READINGS
1. [Epstein NE, Baisden J. The diagnosis and management of synovial cysts: Efficacy of surgery versus cyst aspiration. Surg Neurol Int. 2012;3(Suppl 3):S157-66. doi: 10.4103/2152-7806.98576. Epub 2012 Jul 17. PubMed PMID: 22905322. ](http://www.ncbi.nlm.nih.gov/pubmed/22905322)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22905322)
2. [View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20173680)
Question 39High Yield
When performing an index finger ray amputation, the orthopaedic surgeon should move the
Explanation
Ray amputation often is performed to improve function and decrease pain by removing the digit through the metacarpal. Hyperesthesia and painful light touch are the most disabling complications. The digital nerves should be placed proximal to the wound to prevent a symptomatic neuroma. The radial and ulnar digital nerves can be sutured together, transposed to the interosseous muscle, or resected proximally, although no technique is superior. Excessive mobilization is discouraged, and care is taken to protect the radial digital nerve to the long finger at the time of index ray amputation. Transfer of the first dorsal interosseous, EIP and FDS to the long finger are procedures that have fallen out of favor because of lack of benefit and resulting stiffness.
RECOMMENDED READINGS
57. Blazar PE, Garon MT. Ray Resections of the Fingers: Indications, Techniques, and Outcomes. J Am Acad Orthop Surg. 2015 Aug;23(8):476-84. doi: 10.5435/JAAOS-D-14-00056. Review. PubMed PMID: 26209144.
58. Murray JF, Carman W, MacKenzie JK. Transmetacarpal amputation of the index finger: a clinical assessment of hand strength and complications. J Hand Surg Am. 1977 Nov;2(6):471-
81/. PubMed PMID: 925334.
CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 55
A 60-year-old man has a symptomatic contracture of his dominant-hand ring finger. Treatment options are discussed, and he elects to proceed with palmar fasciectomy.
RECOMMENDED READINGS
57. Blazar PE, Garon MT. Ray Resections of the Fingers: Indications, Techniques, and Outcomes. J Am Acad Orthop Surg. 2015 Aug;23(8):476-84. doi: 10.5435/JAAOS-D-14-00056. Review. PubMed PMID: 26209144.
58. Murray JF, Carman W, MacKenzie JK. Transmetacarpal amputation of the index finger: a clinical assessment of hand strength and complications. J Hand Surg Am. 1977 Nov;2(6):471-
81/. PubMed PMID: 925334.
CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 55
A 60-year-old man has a symptomatic contracture of his dominant-hand ring finger. Treatment options are discussed, and he elects to proceed with palmar fasciectomy.
Question 40High Yield
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on**
Explanation
The patient has heterotopic ossification, a more common finding in patients who have sustained head injuries. Treatment will require removal of the heterotopic bone and anterior and posterior capsulectomies. The main concern about timing is the possible recurrence of heterotopic bone. While an extended wait was once thought necessary, this is no longer true. The timing is based on the time since injury and evidence of bone maturation on plain radiographs. A sharp marginal demarcation of the new bone and a trabecular pattern within it are usually present 3 to 6 months after onset, indicating that it is safe to proceed with surgical excision. It is not necessary to wait more than 6 months. Bone scan results are not good indicators because they may remain “hot” for long periods of time. The levels of alkaline phosphatase and serum calcium-phosphorus product do not need to be measured.
REFERENCE: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 325-335.
REFERENCE: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 325-335.
Question 41High Yield
The anatomic structure responsible for the development of an interdigital neuroma is:
Explanation
The deep transverse metatarsal ligament passes between the undersurface of the metatarsal heads and connects the volar plate
to the adjacent soft tissue structures. The common digital nerve becomes irritated under the sharp edge of the distal portion of the ligament, resulting in nerve swelling and formation of the neuroma.
to the adjacent soft tissue structures. The common digital nerve becomes irritated under the sharp edge of the distal portion of the ligament, resulting in nerve swelling and formation of the neuroma.
Question 42High Yield
A 58-year-old woman returns for an evaluation of right knee pain after a twisting injury. A small pop was felt at the time of injury. Her pain is medial and she is unable to bear weight. A complete physical examination demonstrated range of motion is 0°to 125°; significant medial joint line tenderness; negative flexion McMurray; negative Lachman; stable to varus and valgus stress at 0° and 30° and negative posterior drawer. Based on her history, physical examination, and the MRI scan shown in Figure 1, what is the diagnosis?
Explanation
63
The low likelihood that common symptoms associated with meniscal body injury will manifest in patients with root tears makes clinical diagnoses challenging. For instance, patients with a posterior root tear injury may experience joint line pain, but the absence of mechanical symptoms such as locking or catching is probable. Meniscal root tears are also not typically associated with an inciting traumatic event. MRI has become increasingly used in the diagnosis of meniscal root tears. Telltale signs of a root tear include the presence or absence of a ghost sign, which is the absence of an identifiable meniscus in the sagittal plane or high signal replacing the normal dark meniscal signal. The posterior meniscus is seen in sagittal MRI view in all images up to the one that shows the PCL. The posterior root of the medial meniscus attaches anterior to the posterior cruciate ligament (PCL).
The low likelihood that common symptoms associated with meniscal body injury will manifest in patients with root tears makes clinical diagnoses challenging. For instance, patients with a posterior root tear injury may experience joint line pain, but the absence of mechanical symptoms such as locking or catching is probable. Meniscal root tears are also not typically associated with an inciting traumatic event. MRI has become increasingly used in the diagnosis of meniscal root tears. Telltale signs of a root tear include the presence or absence of a ghost sign, which is the absence of an identifiable meniscus in the sagittal plane or high signal replacing the normal dark meniscal signal. The posterior meniscus is seen in sagittal MRI view in all images up to the one that shows the PCL. The posterior root of the medial meniscus attaches anterior to the posterior cruciate ligament (PCL).
Question 43High Yield
A 45-year-old IV drug abuser has sternoclavicular (SC) joint pain for the past 2 weeks. He is afebrile and physical exam findings include point tenderness and swelling. He most likely has septic arthritis of the
sternoclavicular joint. If so, what is the most likely infecting organism?
sternoclavicular joint. If so, what is the most likely infecting organism?
Explanation
Risk factors for sternoclavicular septic arthritis include IV drug abuse, diabetes, and HIV.
According to the reference by Ross et al, Staphylococcus aureus accounts for 49% of infections. SC joint arthritis accounts for 1% of septic arthritis in the general population but 17% in the IV drug abuse population. Symptoms include spontaneous swelling with the appearance of joint subluxation and localized pain. These patients are not uncommonly afebrile.
According to the reference by Ross et al, Staphylococcus aureus accounts for 49% of infections. SC joint arthritis accounts for 1% of septic arthritis in the general population but 17% in the IV drug abuse population. Symptoms include spontaneous swelling with the appearance of joint subluxation and localized pain. These patients are not uncommonly afebrile.
Question 44High Yield
Dupuytrenâs cord tissue is characterized by what change from normal:
Explanation
C ompared to normal palmar fascia, the fibrous bands in Dupuytrenâs disease have an increased ratio of type III to type I
collagen, and an overall increase in the amount of type III collagen.
collagen, and an overall increase in the amount of type III collagen.
Question 45High Yield
Figure 60 is the radiographs of a patient who underwent surgery to alleviate pain under her second metatarsal that is worsened by wearing high heel shoes. What is the most common complication of the osteotomy shown in the radiographs?
Explanation
The radiographs show a Weil osteotomy that is used to treat metatarsalgia, which is often associated with severe claw toes. The most common complication is a floating toe, or dorsiflexion contracture
at the MTP joint. This is because the interossei muscles move dorsally with respect to the axis of the MTP joint due to depression of the plantar fragment and that the center of rotation is altered after the osteotomy. Multiple studies have shown that the floating toe is the main complication and that the other listed complications rarely occur with this type of osteotomy.
at the MTP joint. This is because the interossei muscles move dorsally with respect to the axis of the MTP joint due to depression of the plantar fragment and that the center of rotation is altered after the osteotomy. Multiple studies have shown that the floating toe is the main complication and that the other listed complications rarely occur with this type of osteotomy.
Question 46High Yield
A 46-year-old male construction worker has right hip pain that has failed to respond to nonsurgical management. His body mass index (BMI) is 32, he is 6’2” tall, and he has no other medical comorbidities. AP and lateral radiographs of the right hip are shown in Figures 23a and 23b. The patient inquires about his suitability for metal- on-metal hip resurfacing. The patient should be educated that he is at higher risk for failure secondary to which of the following?

Explanation
DISCUSSION: This young patient has osteonecrosis of the femoral head with a large area of collapse.
The results of hip resurfacing arthroplasty have been reported to be best in young, male patients who are younger than 55 years of age with a diagnosis of osteoarthritis. Although some authors advocate metal- on-metal hip resurfacing as an option for patients with osteonecrosis of the femoral head, in this particular patient, given the size of the necrotic segment, he would be at higher risk for failure and a conventional total hip arthroplasty would be a more conservative option. As the acetabulum is resurfaced in metal- on-metal hip resurfacing, the secondary changes of the acetabulum are not an issue and his BMI is in an acceptable range for the procedure.
REFERENCES: Mont MA, Ragland PS, Etienne G, et al: Hip resurfacing arthroplasty. J Am Acad Orthop Surg 2006;14:454-463.
Revell MP, McBryde CW, Bhatnagar S, et al: Metal-on-metal hip resurfacing in osteonecrosis of the femoral head. J Bone Joint Surg Am 2006;88:98-103.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65. Question 24
A 31-year-old woman had disabling right knee pain. An arthroscopic assessment reveals chondromalacia of both the lateral femoral condyle and tibial plateau. The standing femorotibial axis measures 10 degrees of valgus. The
optimum treatment of this condition should include
1. ### distal femoral varus osteotomy.
2. ### osteoarticular transplant to the lateral femoral condyle.
3. ### unicondylar arthroplasty.
4. ### high tibial osteotomy.
5. ### Fulkerson tibial tubercle transfer. PREFERRED RESPONSE: 1
DISCUSSION: The long-term outcome of a distal femoral varus osteotomy has been quite favorable and should remain the primary choice for this young active woman. Sharma and associates have shown that a 5-degree valgus malalignment has a five-fold chance of progressing at least one grade within 18 months, making a corrective osteotomy the most important surgical maneuver.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and function decline in knee osteoarthritis. JAMA 2001 ;286:188-195.
Murray PB, Rand JA: Symptomatic valgus knee: The surgical options. J Am Acad Orthop Surg 1993; 1:19.
Figure 25a Figure 25b Figure 25c
The results of hip resurfacing arthroplasty have been reported to be best in young, male patients who are younger than 55 years of age with a diagnosis of osteoarthritis. Although some authors advocate metal- on-metal hip resurfacing as an option for patients with osteonecrosis of the femoral head, in this particular patient, given the size of the necrotic segment, he would be at higher risk for failure and a conventional total hip arthroplasty would be a more conservative option. As the acetabulum is resurfaced in metal- on-metal hip resurfacing, the secondary changes of the acetabulum are not an issue and his BMI is in an acceptable range for the procedure.
REFERENCES: Mont MA, Ragland PS, Etienne G, et al: Hip resurfacing arthroplasty. J Am Acad Orthop Surg 2006;14:454-463.
Revell MP, McBryde CW, Bhatnagar S, et al: Metal-on-metal hip resurfacing in osteonecrosis of the femoral head. J Bone Joint Surg Am 2006;88:98-103.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65. Question 24
A 31-year-old woman had disabling right knee pain. An arthroscopic assessment reveals chondromalacia of both the lateral femoral condyle and tibial plateau. The standing femorotibial axis measures 10 degrees of valgus. The
optimum treatment of this condition should include
1. ### distal femoral varus osteotomy.
2. ### osteoarticular transplant to the lateral femoral condyle.
3. ### unicondylar arthroplasty.
4. ### high tibial osteotomy.
5. ### Fulkerson tibial tubercle transfer. PREFERRED RESPONSE: 1
DISCUSSION: The long-term outcome of a distal femoral varus osteotomy has been quite favorable and should remain the primary choice for this young active woman. Sharma and associates have shown that a 5-degree valgus malalignment has a five-fold chance of progressing at least one grade within 18 months, making a corrective osteotomy the most important surgical maneuver.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and function decline in knee osteoarthritis. JAMA 2001 ;286:188-195.
Murray PB, Rand JA: Symptomatic valgus knee: The surgical options. J Am Acad Orthop Surg 1993; 1:19.
Figure 25a Figure 25b Figure 25c
Question 47High Yield
Figure 1
A 19-year-old man presents for treatment in the emergency department following a motorcycle accident. He sustained an isolated injury to his foot and ankle. The recommended treatment is:
A 19-year-old man presents for treatment in the emergency department following a motorcycle accident. He sustained an isolated injury to his foot and ankle. The recommended treatment is:
Explanation
The prognosis following fracture dislocation of the navicular is not good regardless of treatment. Although one may be tempted to perform an open reduction and immediate primary talonavicular arthrodesis, this is not necessary. Following open reduction and internal fixation, arthritis of the talonavicular joint may occur.
Question 48High Yield
A 45-year-old male injures his wrist during Live Action Role Play in Chicago two weeks ago. He underwent operative fixation by and presents to your clinic for his 2 week follow-up visit. You review his operative note in which the surgeon reports having to apply a volar
locking plate in a distal position to secure the difficult intra-articular fracture. The patient shows you the lateral film in Figure A. You remove his splint, he has no difficulty moving any fingers, very minimal pain, and is not taking any narcotic medication. How do you counsel him about his post-operative period?
locking plate in a distal position to secure the difficult intra-articular fracture. The patient shows you the lateral film in Figure A. You remove his splint, he has no difficulty moving any fingers, very minimal pain, and is not taking any narcotic medication. How do you counsel him about his post-operative period?


Explanation
This patient’s volar locking plate (VLP) is distal to the "watershed line", extending volarly beyond the most volar aspect of the distal radius. He is at greatest risk for an attritional rupture of the FPL.
A VLP placed this distal and volar is more likely to cause flexor tendon injury.
Up to 12% of all patients undergoing volar plate fixation will experience flexor tendon injury, and the FPL is the most common tendon associated with the VLP (57% of total flexor tendon ruptures). The average time from fixation to flexor tendon rupture has been cited at 9 months. To judge if a plate is volar to the watershed line, a plum line can be made in the proximal direction from the most volar edge of the distal radius. If a plate is volar to this (Soong) line, the patient is thought to be at a higher risk for flexor tendon injury. As a result, this patient should be followed closely and if pain with thumb flexion is present after 3 months, the surgeon should consider plate removal so long as the fracture is healed to reduce the chance of FPL rupture. Ruptured tendons require repair, grafting, or transfer with hardware removal.
Griffin and Chhabra comprehensively reviewed the risk factors and adverse events following VLP fixation of distal radius fractures, including flexor tendonitis and rupture. They found that risk factors for flexor tendon rupture following VLP fixation included plate placement distal to the watershed line and that PQ repair does not seem to affect flexor tendonitis.
Agnew et al. analyzed wrist MRIs to determine the relationship between the flexor tendons and the watershed line. They found that at 3mm proximal to the watershed line, the FPL and FDP to the index finger were 2.6 and 2.2mm anterior to the volar rim of the distal radius. The authors suggested that distally placed plates are incredibly close to the flexor tendons.
Chilelli et al. described 24 of 48 wrists which had VLP following distal radius fracture and went on to experiences loss of FPL flexion post-operatively. They found that FPL ROM generally returned after 52 days, however with an associated average loss of 11° in thumb IPJ ROM. The authors attribute this to stripping of FPL from the bone during the volar approach.
Soong et al. divided patients who underwent VLP fixation for distal radius fractures into three groups according to position of plate relative to a plum line extending proximally from the most volar and distal aspect of the distal radius: those with a VLP dorsal to the Soong line (grade 0), those with the VLP volar to the Soong line but proximal to the rim (grade 1), and those with a VLP volar to the Soong line and at or distal to rim (grade 2). Of the 73 cases reviewed, the authors reported three flexor tendon ruptures, two of which were grade 2 position. The authors concluded that both position of plate and type of plate were contributors to flexor tendon injury following VLP fixation.
Figure A is a lateral radiograph of the wrist demonstrating appropriate reduction and fixation but with the VLP volar to the "watershed" or Soong line.
Illustration A is a lateral radiograph with Soong's line drawn to show that this plate is too volar.
Incorrect Answers:
Answer 2: The FCR is very superficial and is not commonly injured following VLP fixation of distal radius fractures.
Answer 3: While the FDP to the index finger is the second most common flexor tendon injury following VLP, injury to the FDS to the index finger is unlikely.
Answer 4: The patient is only two weeks from fixation and has no symptoms. The reduction appears appropriate on the imaging seen. Therefore there is no need for urgent revision fixation.
Answer 5: The VLP shown is volar to the watershed line is therefore not in an appropriate position.
A VLP placed this distal and volar is more likely to cause flexor tendon injury.
Up to 12% of all patients undergoing volar plate fixation will experience flexor tendon injury, and the FPL is the most common tendon associated with the VLP (57% of total flexor tendon ruptures). The average time from fixation to flexor tendon rupture has been cited at 9 months. To judge if a plate is volar to the watershed line, a plum line can be made in the proximal direction from the most volar edge of the distal radius. If a plate is volar to this (Soong) line, the patient is thought to be at a higher risk for flexor tendon injury. As a result, this patient should be followed closely and if pain with thumb flexion is present after 3 months, the surgeon should consider plate removal so long as the fracture is healed to reduce the chance of FPL rupture. Ruptured tendons require repair, grafting, or transfer with hardware removal.
Griffin and Chhabra comprehensively reviewed the risk factors and adverse events following VLP fixation of distal radius fractures, including flexor tendonitis and rupture. They found that risk factors for flexor tendon rupture following VLP fixation included plate placement distal to the watershed line and that PQ repair does not seem to affect flexor tendonitis.
Agnew et al. analyzed wrist MRIs to determine the relationship between the flexor tendons and the watershed line. They found that at 3mm proximal to the watershed line, the FPL and FDP to the index finger were 2.6 and 2.2mm anterior to the volar rim of the distal radius. The authors suggested that distally placed plates are incredibly close to the flexor tendons.
Chilelli et al. described 24 of 48 wrists which had VLP following distal radius fracture and went on to experiences loss of FPL flexion post-operatively. They found that FPL ROM generally returned after 52 days, however with an associated average loss of 11° in thumb IPJ ROM. The authors attribute this to stripping of FPL from the bone during the volar approach.
Soong et al. divided patients who underwent VLP fixation for distal radius fractures into three groups according to position of plate relative to a plum line extending proximally from the most volar and distal aspect of the distal radius: those with a VLP dorsal to the Soong line (grade 0), those with the VLP volar to the Soong line but proximal to the rim (grade 1), and those with a VLP volar to the Soong line and at or distal to rim (grade 2). Of the 73 cases reviewed, the authors reported three flexor tendon ruptures, two of which were grade 2 position. The authors concluded that both position of plate and type of plate were contributors to flexor tendon injury following VLP fixation.
Figure A is a lateral radiograph of the wrist demonstrating appropriate reduction and fixation but with the VLP volar to the "watershed" or Soong line.
Illustration A is a lateral radiograph with Soong's line drawn to show that this plate is too volar.
Incorrect Answers:
Answer 2: The FCR is very superficial and is not commonly injured following VLP fixation of distal radius fractures.
Answer 3: While the FDP to the index finger is the second most common flexor tendon injury following VLP, injury to the FDS to the index finger is unlikely.
Answer 4: The patient is only two weeks from fixation and has no symptoms. The reduction appears appropriate on the imaging seen. Therefore there is no need for urgent revision fixation.
Answer 5: The VLP shown is volar to the watershed line is therefore not in an appropriate position.
Question 49High Yield
Which of the following nerves is most commonly injured during revision surgery following a Bristow procedure?
Explanation
Because of the previously transferred bone block of coracoid and short arm flexors, the musculocutaneous nerve often scars along the anteroinferior glenohumeral capsule. Mobilization of this tissue places the nerve at greatest risk. The axillary nerve is also potentially at risk, but this is nonspecific to prior surgery, particularly the Bristow procedure.
REFERENCES: Norris TR: Complications following anterior instability repairs, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993,
pp 98-116.
Flatow EL, Bigliani LU, April EW: An anatomic study of the musculocutaneous nerve and its relationship to the coracoid process. Clin Orthop 1989;244:166-171.
REFERENCES: Norris TR: Complications following anterior instability repairs, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993,
pp 98-116.
Flatow EL, Bigliani LU, April EW: An anatomic study of the musculocutaneous nerve and its relationship to the coracoid process. Clin Orthop 1989;244:166-171.
Question 50High Yield
Two weeks after being treated for a nondisplaced type II odontoid fracture with a halo fixator, a 78-yearold man reports left anterior pin site pain. On examination, the left anterior pin fixation site is tender andfocal erythema with mild loosening is noted. The patient denies fevers, chills, or any other constitutional symptoms. What is the most appropriate course of action at this time?
Explanation
One of the most common complications of halo device fixation is pin loosening. In adults, pin loosening can occur in up to 36% of patients and most commonly occurs in the anterior pins. If there is no infection present, a loose pin can be managed by simply retightening the screw one to two turns. Infection at the pin site is the second most common complication of the halo device, occurring in about 20% of patients.
Infection can be either superficial or deep. Superficial infections can be treated with oral antibiotics and wound care at the pin site. Pin loosening does not always occur with pin site infection. The infection can be treated with or without removing the pin. If a deep infection develops, the pin should be removed. If an abscess develops, parenteral antibiotics and drainage of the abscess may be necessary. A new pin may be placed in a new position. Other complications from halo fixation include skin breakdown and intracranial penetration.
Infection can be either superficial or deep. Superficial infections can be treated with oral antibiotics and wound care at the pin site. Pin loosening does not always occur with pin site infection. The infection can be treated with or without removing the pin. If a deep infection develops, the pin should be removed. If an abscess develops, parenteral antibiotics and drainage of the abscess may be necessary. A new pin may be placed in a new position. Other complications from halo fixation include skin breakdown and intracranial penetration.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon