Revision of Failed UKA: Your Guide to Successful Treatment

Key Takeaway
Learn more about Revision of Failed UKA: Your Guide to Successful Treatment and how to manage it. The revision of failed Unicompartmental Knee Arthroplasty (UKA) requires identifying the primary failure's etiology. Indications include symptomatic failure due to wear, loosening, or pain. Treatment options range from isolated polyethylene exchange or revision to another UKA, to conversion to a Total Knee Arthroplasty. TKA typically provides a more predictable outcome than re-revising with another UKA.
As an academic orthopedic surgeon and medical educator, the management of a failed unicompartmental knee arthroplasty (UKA) presents a nuanced challenge, demanding a meticulous diagnostic approach and a tailored surgical strategy. While UKA offers distinct advantages for carefully selected patients, including preserved bone stock, better proprioception, and faster recovery compared to total knee arthroplasty (TKA), its failure necessitates a comprehensive understanding of the underlying etiology to ensure successful revision.
Introduction and Epidemiology
Unicompartmental knee arthroplasty has a well-established role in treating isolated compartment osteoarthritis, particularly in the medial compartment. Historically, UKA was plagued by high revision rates. However, modern implant designs, improved patient selection criteria, and enhanced surgical techniques have significantly improved outcomes, with survival rates approaching those of TKA in appropriately selected patient cohorts. Despite these advancements, UKA failure remains a clinical reality, necessitating revision surgery.
The incidence of UKA failure ranges from 1% to 2% per year in many series, often leading to conversion to TKA. Registry data indicate that revision rates for UKA are generally higher than for primary TKA, though this often reflects the differing patient populations and the initial indications for UKA. The increasing volume of primary UKAs performed globally implies a corresponding rise in the number of failed UKAs requiring revision. The successful outcome of revision surgery hinges critically on identifying the precise etiology of the primary procedure's failure, a principle universally applicable across arthroplasty (Knight et al., 1997). This dictates the operative plan, choice of implants, and anticipated rehabilitation.
Surgical Anatomy and Biomechanics
A thorough understanding of the knee's surgical anatomy and biomechanics is paramount when approaching a failed UKA. The pathology leading to failure often alters the native anatomy and soft tissue envelope.
Bone Stock Assessment
One of the primary advantages of UKA is bone preservation. However, failure can involve significant bone loss, particularly from aseptic loosening, infection, or periprosthetic fracture.
* Femoral Component: Loosening can lead to erosion of the distal femur, especially around the condylar cut.
* Tibial Component: Tibial bone loss, particularly posteromedial, is common with subsidence or loosening, complicating subsequent tibial component fixation. The remaining articular cartilage in the un-resurfaced compartments must be assessed for degenerative changes.
* Patellofemoral Compartment: While often spared in primary UKA, progressive osteoarthritis in this compartment is a common mode of failure.
Ligamentous Stability and Joint Line
The anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) are typically preserved in UKA, which contributes to kinematically normal knee function. However, progressive laxity or rupture of the ACL or PCL can occur, leading to instability and failure. Furthermore, the integrity of the medial collateral ligament (MCL) and lateral collateral ligament (LCL) is crucial. A failed UKA often presents with soft tissue imbalance, either residual laxity from the initial procedure, progressive laxity, or contractures from arthrofibrosis. Restoring the mechanical axis and joint line, along with achieving appropriate soft tissue balance, is a complex task made more challenging by altered anatomy and scarring. Deviations in the joint line can significantly impact patellofemoral mechanics and overall knee kinematics.
Extensor Mechanism Integrity
The extensor mechanism, comprising the quadriceps femoris, patella, and patellar tendon, must be carefully evaluated. Prior incisions, scarring, and surgical approaches can affect its function. Maltracking of the patella, or subluxation, can be a source of persistent pain and functional limitation after UKA and requires careful consideration during revision.
Indications and Contraindications
The decision to revise a failed UKA is multifaceted, guided by patient symptomatology, functional impairment, radiographic findings, and the specific etiology of failure.
Indications for Revision UKA to TKA
The most common revision procedure for a failed UKA is conversion to a total knee arthroplasty. Indications include:
1. Symptomatic Polyethylene Wear: Excessive wear of the polyethylene insert leading to pain, instability, or inflammatory reaction.
2. Aseptic Loosening: Unstable femoral or tibial components causing pain and often associated with radiographic lucencies.
3. Infection: Periprosthetic joint infection (PJI) is a severe complication requiring a specific management pathway, often involving a two-stage revision.
4. Persistent or Progressive Pain: This can be due to:
* Progression of Osteoarthritis: In an un-resurfaced compartment (typically patellofemoral or contralateral tibiofemoral).
* Malposition of Components: Leading to altered kinematics or impingement.
* Implant Design Issues: Less common with modern implants.
* Arthrofibrosis/Stiffness: Limited range of motion impacting function.
5. Instability: Ligamentous insufficiency (ACL/PCL tear, MCL/LCL laxity) or mal-balancing of the primary UKA leading to symptomatic instability.
6. Periprosthetic Fracture: Fracture around the implant components.
7. Patellofemoral Dysfunction: Progressive patellofemoral pain or maltracking not responsive to conservative measures.
Indications for Revision UKA to UKA (Component Exchange)
The role of revision to another UKA, or selective component exchange, is controversial and has limited indications. Theoretical applications include:
1. Isolated Polyethylene Insert Exchange: For late wear of an otherwise well-fixed, well-positioned modular UKA with no progression of osteoarthritis in other compartments and no other sources of pain.
2. Early Aseptic Loosening: Without significant bone loss or malalignment, and in the absence of other compartment disease, a component exchange could be considered, though this is rare and highly debated. This requires extremely stringent patient selection and meticulous surgical technique.
Contraindications
Contraindications to revision surgery are similar to those for primary arthroplasty, with some additional considerations:
* Active Systemic Infection: Uncontrolled sepsis elsewhere in the body.
* Unrealistic Patient Expectations: Poor understanding of potential outcomes or limitations.
* Severe Comorbidities: Medical conditions that significantly increase surgical risk and preclude safe anesthesia or recovery.
* Poor Soft Tissue Envelope: Compromised skin or muscle integrity that would complicate wound healing.
* Severe Bone Loss: So extensive that stable implant fixation is unachievable, potentially necessitating alternative solutions like arthrodesis or amputation.
Operative vs. Non-Operative Indications
The decision pathway for a failed UKA involves a careful assessment of symptoms and findings.
| Category | Operative Indications | Non-Operative Indications |
|---|---|---|
| Pain | Persistent, debilitating pain despite conservative management, attributable to implant loosening, wear, malposition, or progressive osteoarthritis in an unresurfaced compartment. | Mild, intermittent pain manageable with analgesia, activity modification, or physical therapy, particularly if imaging shows no significant mechanical failure or progression of disease. |
| Instability | Symptomatic gross instability (ligamentous laxity, subluxation, giving way) impacting daily activities. | Mild, occasional sensation of instability not significantly impacting function, or easily managed with bracing/muscle strengthening. |
| Functional Loss | Significant restriction in range of motion, ambulation, or activities of daily living due to UKA failure. | Acceptable functional status despite some limitations, especially if pain is well-controlled. |
| Imaging Findings | Radiographic evidence of aseptic loosening (progressive lucency >1-2mm), severe polyethylene wear, periprosthetic fracture, significant component malposition, or end-stage osteoarthritis in un-resurfaced compartments. | Stable implants, minimal or non-progressive lucencies, mild cartilage degeneration in other compartments, or incidental findings not correlating with patient symptoms. |
| Infection | Confirmed periprosthetic joint infection (PJI) via aspiration, microbiology, or inflammatory markers. | Negative or inconclusive infection workup; symptoms more likely attributable to mechanical failure. |
| Specific UKA Type | Revision of mobile-bearing UKA due to dislocation. Revision of fixed-bearing UKA due to gross wear. | Isolated polyethylene wear in a well-fixed, well-aligned UKA if conservative measures provide adequate relief and patient does not desire surgery (though typically this is an operative indication for polyethylene exchange). |
| Patient Factors | Patient fit for surgery, realistic expectations, willingness to undergo rehabilitation. | Significant medical comorbidities precluding surgery, patient preference for conservative management, unrealistic expectations regarding surgical outcomes. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful revision UKA surgery. This phase is more complex than primary arthroplasty, requiring detailed evaluation of the failure etiology, assessment of bone loss, and meticulous surgical strategy.
Etiology Identification
The primary step is to definitively identify the cause of failure.
* Detailed History: Elicit pain characteristics (onset, location, severity, aggravating/alleviating factors), instability symptoms, mechanical symptoms (clicking, locking), and prior surgical details.
* Physical Examination: Assess gait, range of motion, ligamentous stability (varus/valgus stress in extension and 30 degrees flexion), patellar tracking, effusion, tenderness, and neurovascular status.
* Laboratory Studies:
* Complete Blood Count (CBC) with Differential, Erythrocyte Sedimentation Rate (ESR), C-Reactive Protein (CRP): Screen for infection.
* Joint Aspiration: Crucial for suspected PJI. Send fluid for cell count, differential, bacterial culture (aerobic/anaerobic), fungal culture, and crystal analysis. Newer markers like alpha-defensin or leukocyte esterase strips can aid rapid diagnosis.
* Prior Operative Notes and Implant Identification: Retrieve records to ascertain the original implant type, size, position, and any intraoperative details (e.g., ligament releases). This informs removal strategies and templating.
Imaging Studies
Comprehensive imaging is indispensable for evaluating bone loss, component position, and overall limb alignment.
* Plain Radiographs:
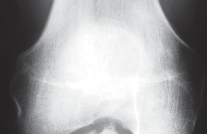
* Anteroposterior (AP) View (Fig. 1A): Assess for component loosening (lucent lines >1-2mm), subsidence, implant fracture, and signs of progressive osteoarthritis.
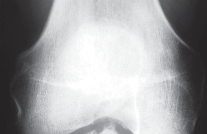
* Lateral View (Fig. 1B): Evaluate femoral and tibial component position, posterior tibial slope, and patellofemoral articulation.
* Sunrise (Axial Patella) View: Crucial for assessing patellofemoral tracking and osteoarthritis.
* Standing Hip-to-Ankle Films (Fig. 2A): Essential for evaluating the mechanical axis of the entire lower extremity, detecting varus/valgus malalignment, and assessing compensatory changes.
* Stress Radiographs: May be helpful in assessing ligamentous laxity.
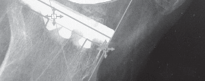
Fig. 1A: Anteroposterior radiograph of a failed UKA, demonstrating component malposition and potential loosening.

Fig. 1B: Lateral radiograph of a failed UKA, highlighting issues with component alignment and posterior tibial slope.

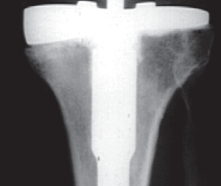
Fig. 2A: Standing hip-to-ankle film illustrating overall limb alignment in a patient with a failed UKA.
- Computed Tomography (CT) Scan: Indicated for detailed assessment of bone loss, especially on the femoral and tibial sides. It precisely delineates bone defects and helps in planning for augments, stems, or cones. It is also useful for assessing component rotation and identifying occult fractures.
- Magnetic Resonance Imaging (MRI): Less commonly used unless soft tissue pathology (e.g., meniscal tear, osteonecrosis) is suspected in the contralateral compartment, or if patellofemoral issues are unclear. MRI can also reveal occult stress fractures or inflammatory conditions.
- Bone Scintigraphy: May be useful in differentiating between aseptic loosening and infection, though its specificity is limited.
Templating and Component Selection
Based on the etiology and imaging, a detailed surgical plan is formulated:
1. Implant Removal Strategy: Plan for specific instruments (osteotomes, cutting guides, explant tools) based on the original implant type (cemented vs. uncemented, specific design).
2. Bone Defect Management:
* Classification: Utilize a system like the Anderson Orthopaedic Research Institute (AORI) classification for femoral and tibial bone defects.
* Reconstruction: Plan for the use of cement, modular metal augments, metal cones, structural allografts, or impaction bone grafting. The goal is to restore the joint line and achieve stable fixation.
3. TKA Component Selection:
* Constraint: Determine the required level of constraint (cruciate-retaining (CR), posterior-stabilized (PS), constrained condylar knee (CCK), or rotating hinge knee (RHK)) based on ligamentous integrity and soft tissue balance. Many UKA revisions require at least PS or CCK.
* Stems: Assess the need for intramedullary stems (femoral and/or tibial) to bypass bone defects, distribute load, and enhance stability.
* Patellofemoral: Decide whether to resurface the patella.
4. Specialized Instruments: Ensure availability of instruments for implant removal, bone defect preparation, and the chosen revision TKA system.
Patient Positioning
The patient is typically placed in a supine position on the operating table.
* Tourniquet: A high thigh tourniquet is routinely used for optimal hemostasis.
* Leg Holder: A rigid leg holder allows for full flexion and extension and facilitates exposure.
* Draping: Standard sterile draping of the affected limb, allowing for full range of motion. Consideration should be given to draping for extensile exposures if anticipated (e.g., if a quadriceps snip or V-Y plasty is required).
* Preoperative Antibiotics: Administer intravenous prophylactic antibiotics (e.g., Cefazolin) typically 30-60 minutes before incision.
Detailed Surgical Approach and Technique
Converting a failed UKA to a TKA is often more challenging than a primary TKA due to altered anatomy, scar tissue, bone loss, and potential soft tissue contractures. The goal is to remove the existing components, address bone defects, restore the mechanical axis and joint line, achieve ligamentous balance, and implant a stable revision TKA.
Incision and Exposure
- Incision: Whenever possible, utilize the previous skin incision. If multiple incisions exist, select the most lateral one, extending it proximally and distally as needed. In cases of significant scarring or anticipated difficulty, an extensile approach may be considered from the outset.
- Soft Tissue Dissection: Carefully dissect through scar tissue. The medial parapatellar approach is most commonly employed. Manage the capsular and retinacular tissues meticulously to preserve vascularity.
- Extensile Options: If exposure is limited due to contracture or previous surgery:
- Quadriceps Snip: A limited release of the vastus medialis obliquus (VMO) from the quadriceps tendon.
- V-Y Quadriceps Plasty: A more extensive lengthening of the quadriceps mechanism, providing excellent exposure but with potential for increased extensor lag.
- Tibial Tubercle Osteotomy: Reserved for the most difficult exposures or cases with significant extensor mechanism pathology, allowing for reflection of the entire extensor mechanism. Requires careful fixation and carries risks of non-union or fracture.
Implant Removal
This is a critical, often difficult, step where bone preservation is paramount.
1. Polyethylene Insert: If present, remove the polyethylene insert. This is usually straightforward.
2. Tibial Component Removal:
* If uncemented: Carefully use osteotomes around the periphery to release ingrowth, then use a specialized explant tool.
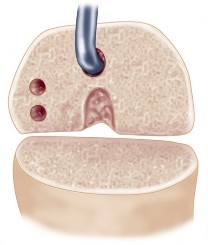
* If cemented: Use narrow osteotomes at the cement-bone interface. A small osteotome can be tapped gently into the implant-cement interface to loosen it. Consider using a Gigli saw or burr to cut away the cement mantle. The tibial tray is often the most challenging component to remove without excessive bone loss, especially if there is significant subsidence or strong cement fixation. Heat application can sometimes aid in debonding.
* Bone Loss: Pay careful attention to the posteromedial tibia, which is prone to bone loss after UKA.

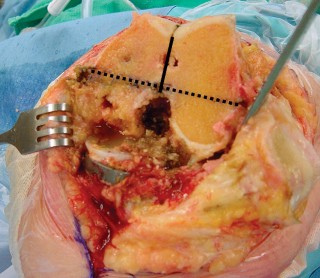
Fig. 3A: Intraoperative image showing removal of a failed tibial UKA component.

Fig. 3B: Diagram illustrating careful osteotome use to debond a cemented tibial component.
- Femoral Component Removal:
- If uncemented: Gentle tapping with a mallet on an explant tool, or careful osteotome use at the ingrowth interface.
- If cemented: Use narrow osteotomes at the cement-bone interface. The component typically detaches with less difficulty than the tibial component. Avoid excessive force to prevent femoral condyle fracture.
- Any cement remaining in the bone must be thoroughly removed using curettes, burrs, or pulsed lavage.

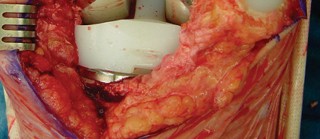
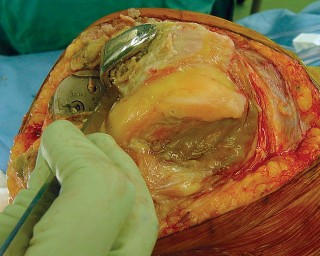
Fig. 4A: Femoral UKA component removal.
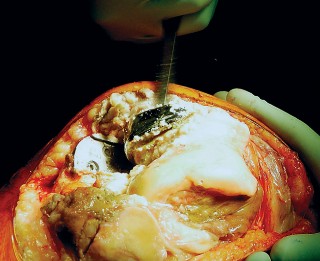
Fig. 4B: Appearance of the distal femur after UKA component removal, often revealing bone loss.
Bone Defect Management
After component removal and thorough cement débridement, address any bone defects.
1. Small Defects: Can often be filled with cement.
2. Moderate Defects (AORI Type 1 or 2A):
* Femoral: Often managed with intramedullary stems and distal femoral augments.
* Tibial: Tibial augments, cement, or impaction grafting. The goal is to restore the joint line and create a stable foundation for the new components.
3. Large Defects (AORI Type 2B or 3):
* Metal Cones: Increasingly popular for severe metaphyseal bone loss on both the femoral and tibial sides. They provide excellent stability and allow for bony ingrowth.
* Structural Allografts: Used for very large defects, particularly segmental ones. Requires careful shaping and fixation.
* Custom Implants: In rare, extreme cases.
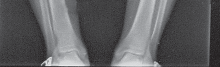
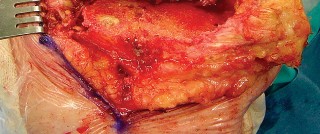
Fig. 5A: Example of a tibial bone defect after UKA removal.

Fig. 5B: Augments and stems utilized to reconstruct significant bone loss in revision TKA.
Preparation for Revision TKA
- Intramedullary Canal Preparation: Ream the femoral and tibial canals for intramedullary stems, if indicated. Ensure proper alignment and rotation.
- Distal Femoral Resection: Create a new distal femoral cut, aiming to restore the distal femoral joint line, which is crucial for soft tissue balance. Use specialized cutting guides for revision TKA that account for bone loss and stem placement.
- Proximal Tibial Resection: Make a new proximal tibial cut, typically aiming for 3 degrees of posterior slope. Restore the tibial joint line, addressing defects with augments or cones as planned.
- Flexion and Extension Gap Balancing: This is arguably the most challenging aspect of revision arthroplasty.
- Extension Gap: Assess in full extension. Release tight structures (e.g., posteromedial capsule, deep MCL) or augment deficient ones.
- Flexion Gap: Assess in 90 degrees of flexion. Ensure the flexion gap is symmetrical and rectangular to the extension gap. Release tight structures (e.g., PCL, IT band).
- Trial Components: Utilize trial components to accurately assess stability throughout the range of motion. Adjust component sizes, augments, and polyethylene thickness to achieve optimal balance.
- Patellofemoral Tracking: Assess patellar tracking with trial components in place. Decide whether to resurface the patella. If resurfacing, aim for central tracking without tilt. Address patellar clunk or impingement.

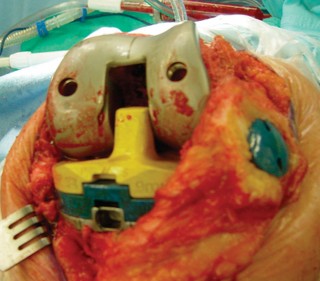
Fig. 6A: Intraoperative image demonstrating trial components in place for assessing stability and alignment.
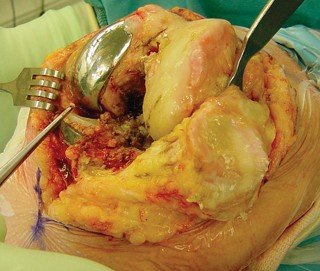
Fig. 6B: Assessment of patellar tracking during trial reduction.
Definitive Component Implantation
- Component Insertion: Once satisfied with alignment, stability, and range of motion with trial components, proceed with definitive component implantation.
- Cementation: Most revision TKAs are cemented, especially in cases of bone loss requiring augments or stems, to ensure immediate stability and fill voids. Meticulous cement technique is essential.
- Uncemented Options: Uncemented stems and cones can be used, particularly in younger patients with good bone stock, to facilitate biological ingrowth.
- Patellar Component: If resurfacing, use a cemented patellar button.
- Polyethylene Insert: Insert the final polyethylene bearing component.

Fig. 7A: Final femoral component cemented in place.

Fig. 7B: Final tibial component with augments and stem cemented.
Closure
- Irrigation: Thoroughly irrigate the joint with antibiotic saline.
- Drains: Placement of an intra-articular drain may be considered for large revisions to manage postoperative hematoma.
- Capsular Closure: Close the capsule and retinaculum carefully.
- Layered Closure: Close the subcutaneous tissues and skin in a standard fashion.
Specific Considerations for Revision UKA to UKA
While rare, if the indication is solely isolated polyethylene wear in a perfectly well-aligned, well-fixed UKA with no progression of osteoarthritis in other compartments, a polyethylene exchange can be performed.
* Technique: A standard medial parapatellar arthrotomy. Carefully remove the old polyethylene. Ensure no wear on the metallic components or evidence of loosening. Meticulously clean the components. Insert a new polyethylene insert of the appropriate size and thickness to restore stability.

Fig. 8: Isolated polyethylene insert exchange for late wear of a well-fixed UKA.
Complications and Management
Revision UKA to TKA carries a higher risk profile than primary TKA due to the complexity of the surgery, altered anatomy, and often compromised soft tissue envelope. Proactive recognition and management are crucial for optimal outcomes.
Common Complications and Salvage Strategies
| Complication | Incidence | Management Strategies |
|---|---|---|
| Periprosthetic Joint Infection (PJI) | 1-5% (Higher than primary TKA) | Early (within 3 weeks): Irrigation and debridement (I&D) with polyethylene exchange and antibiotic therapy. Late or chronic: Two-stage revision (implant removal, antibiotic spacer, systemic antibiotics, then reimplantation of definitive TKA) is standard. One-stage revision considered in highly selected cases. Arthrodesis or amputation for intractable infection or failed two-stage revision. |
| Aseptic Loosening | 5-10% | Re-revision: Exchange of loose components. Often requires further bone defect management (augments, cones, stems) and increased constraint. May involve modular revision TKA components or custom implants for severe cases. |
| Instability | 2-8% | Surgical: Revision to a more constrained implant (CCK or RHK). Ligamentous reconstruction is rarely successful in isolation. Careful re-balancing during revision is critical. Non-surgical: Bracing, physical therapy for muscle strengthening. |
| Arthrofibrosis / Stiffness | 5-15% | Conservative: Aggressive physical therapy, continuous passive motion (CPM). Surgical: Manipulation under anesthesia (MUA) for early stiffness (within 3 months post-op). Arthroscopic or open arthrolysis for chronic, resistant stiffness. Prevention through meticulous surgical technique and early, aggressive rehabilitation. |
| Periprosthetic Fracture | 1-3% | Surgical: Depends on fracture location, type, and stability of implants. May require open reduction internal fixation (ORIF) with plates/screws, or component revision with stems and/or constrained implants. Often requires protected weight-bearing. |
| Neurovascular Injury | <1% (rare but devastating) | Surgical: Immediate consultation with vascular or neurosurgery specialist for repair. Vigilant intraoperative attention to anatomical landmarks and careful retraction are crucial. |
| Patellofemoral Complications | 5-10% | Patellar maltracking, patellar fracture, extensor mechanism disruption. Management: Patellar resurfacing (if not already done), component realignment, lateral retinacular release, revision of patellar component, repair of extensor mechanism. |
| Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) | 1-2% (clinical) | Prophylaxis: Chemical (anticoagulants) and mechanical (TED stockings, intermittent pneumatic compression devices). Management: Anticoagulation for DVT, and hospitalization for PE. |
| Extensor Lag | Variable (post-quad snip/V-Y) | Conservative: Aggressive quadriceps strengthening. Surgical: Revision of extensor mechanism, quadriceps lengthening or reconstruction if severe and persistent, though these are rare for isolated lag. |
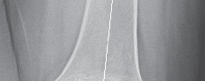
Fig. 9: Postoperative radiograph showing periprosthetic fracture after revision TKA.

Fig. 10: Revision TKA with significant bone loss managed with a metal cone and long stem.
Post Operative Rehabilitation Protocols
Postoperative rehabilitation after revision UKA to TKA is critical for maximizing functional recovery and differs somewhat from primary TKA due to the increased surgical complexity and potential for bone graft or stem fixation. Protocols must be individualized based on intraoperative findings, the extent of bone reconstruction, and implant stability.
Immediate Postoperative Phase (Days 0-7)
- Pain Management: Multimodal analgesia (opioids, NSAIDs, acetaminophen, nerve blocks) is essential.
- Deep Vein Thrombosis (DVT) Prophylaxis: Continue chemical (e.g., LMWH, oral anticoagulants) and mechanical (compression stockings, intermittent pneumatic compression) prophylaxis.
- Wound Care: Monitor incision for signs of infection or hematoma.
- Early Mobilization:
- Weight-Bearing: This is highly dependent on surgical stability. If extensive bone grafting or long stems were used, protected weight-bearing (toe-touch or partial weight-bearing) with crutches or a walker may be prescribed for 6-12 weeks. If stable cement fixation and minimal bone loss, weight-bearing as tolerated may be initiated.
- Range of Motion (ROM): Begin gentle active-assisted and passive ROM exercises. Continuous passive motion (CPM) may be used but its efficacy remains debated. The goal is to achieve 0-90 degrees of flexion by discharge.
- Therapeutic Exercises: Quadriceps and gluteal sets, ankle pumps, active knee extension to 0 degrees, gentle flexion exercises.
Early Rehabilitation Phase (Weeks 1-6)
- Progressive Weight-Bearing: Advance weight-bearing status as tolerated and as allowed by the surgeon based on radiographic healing and implant stability.
- Range of Motion: Continue striving for improved flexion. Goal is typically 0-110 degrees by 6 weeks.
- Strengthening: Introduce progressive resistance exercises for quadriceps, hamstrings, and hip abductors/adductors. Begin with isometric exercises and progress to isotonic.
- Gait Training: Focus on proper gait mechanics, gradually reducing reliance on assistive devices.
- Scar Mobilization: Gentle massage around the incision to prevent adhesions and improve pliability.

Fig. 11: Patient performing quadriceps strengthening exercises post-revision TKA.
Intermediate Rehabilitation Phase (Weeks 6-12)
- Full Weight-Bearing: Typically achieved by this phase, assuming adequate bone healing and implant stability.
- Advanced Strengthening: Incorporate closed-chain exercises (mini-squats, lunges, step-ups) and balance training.
- Endurance Training: Stationary cycling, swimming, elliptical trainer.
- Functional Activities: Work towards independence in daily activities.

Fig. 12: Patient performing balance exercises.
Late Rehabilitation Phase (Beyond 12 Weeks)
- Return to Activity: Gradual return to low-impact recreational activities (walking, golf, swimming). High-impact sports are generally discouraged.
- Proprioception and Agility: Advanced balance and agility drills for those seeking higher-level function.
- Long-Term Maintenance: Emphasize maintaining strength and flexibility through a home exercise program. Regular follow-up with the surgeon is essential.
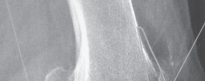
Fig. 13: Functional return to cycling post-revision TKA.
Summary of Key Literature and Guidelines
The literature on revision of failed UKA largely focuses on conversion to TKA, reflecting its prevalence as the treatment of choice. Several key themes emerge:
Outcomes of UKA Revision to TKA
- Satisfactory but Inferior to Primary TKA: Numerous studies consistently report that the clinical outcomes (e.g., Knee Society Score, Western Ontario and McMaster Universities Osteoarthritis Index – WOMAC) following revision of UKA to TKA are generally good, with significant pain relief and functional improvement. However, these outcomes are typically not as robust as those achieved after primary TKA.
- Higher Complication Rates: Revision TKA following UKA failure has been associated with higher rates of complications, including infection, instability, and aseptic loosening, compared to primary TKA. This is attributed to the altered anatomy, bone loss, and scar tissue.
- Survival Rates: Long-term survival rates for revision TKA from UKA are generally lower than for primary TKA, but respectable, often in the range of 80-90% at 10 years. Registry data from various countries (e.g., National Joint Registry for England, Wales, Northern Ireland, and the Isle of Man; Australian National Joint Replacement Registry) provide valuable insights into these trends, highlighting specific failure mechanisms and outcomes.
- Impact of Failure Etiology: The cause of UKA failure significantly influences revision outcomes. Revision for aseptic loosening or polyethylene wear tends to have better outcomes than revision for infection or unexplained pain.
Controversy of UKA to UKA Revision
- Limited Role: The literature generally supports a very limited role for revision of a failed UKA with another UKA component. Isolated polyethylene insert exchange for wear in an otherwise well-functioning, stable UKA without evidence of other compartment arthritis is the most accepted indication.
- Poor Outcomes for Component Revision: Studies attempting to revise a loose or malpositioned UKA component with another UKA component generally report inferior outcomes and higher re-revision rates compared to conversion to TKA. This is due to the inherent difficulties in correcting alignment, addressing subtle bone loss, and achieving ligamentous balance within the confined space of a partial replacement.
Guidelines and Best Practices
- Meticulous Preoperative Planning: This is consistently emphasized across the literature as the most critical factor for success. Comprehensive clinical assessment, detailed imaging (including full-length alignment films and potentially CT for bone loss), and identification of the failure etiology are paramount.
- Bone Defect Management: The use of modular augments, metal cones, and intramedullary stems is a well-established strategy for managing bone loss, aiming to restore joint line and provide stable fixation.
- Ligamentous Balancing: Restoring soft tissue balance in both flexion and extension is crucial, often requiring careful releases and the use of more constrained TKA designs (e.g., PS, CCK).
- Addressing Patellofemoral Pathology: Patellofemoral issues, either as the cause of failure or as a result of altered kinematics, must be addressed at the time of revision.
In conclusion, the revision of a failed UKA, predominantly to a TKA, is a complex yet rewarding procedure. While outcomes are generally good, they do not consistently reach the level of primary TKA. A meticulous, individualized approach, grounded in a thorough understanding of the failure mechanism, advanced preoperative planning, and precise surgical execution, is essential to optimize patient outcomes and minimize complications. Ongoing research continues to refine our understanding and techniques, but the core principles of revision arthroplasty remain centered on restoration of anatomy, stability, and function.

Fig. 14: Postoperative radiographs after revision TKA showing good alignment.

Fig. 15: Postoperative lateral radiograph of a revised TKA.

Fig. 16: Clinical image showing successful range of motion after revision TKA.
Clinical & Radiographic Imaging




You Might Also Like