Thumb Metacarpophalangeal Joint Ulnar Collateral Ligament Rupture: Comprehensive Surgical Guide
Key Takeaway
Ulnar collateral ligament (UCL) ruptures of the thumb metacarpophalangeal joint, commonly known as skier's thumb, require meticulous evaluation to rule out a Stener lesion. While incomplete tears are managed conservatively with immobilization, complete ruptures with adductor aponeurosis interposition necessitate prompt surgical repair. This guide details the biomechanics, diagnostic imaging, and step-by-step operative techniques for acute repair, chronic reconstruction, and salvage arthrodesis to restore pinch strength and joint stability.
Introduction and Historical Context
Injury to the ulnar collateral ligament (UCL) of the thumb metacarpophalangeal (MCP) joint is a frequently encountered orthopedic pathology, essential to recognize and treat promptly to preserve the critical pinch and grasp functions of the hand. Historically referred to as "gamekeeper’s thumb," the original description by Campbell in 1955 detailed an attritional, chronic injury pattern observed in Scottish gamekeepers who repeatedly subjected their thumbs to valgus stress while sacrificing small game.
In contemporary practice, acute ruptures are far more common and are typically designated as "skier’s thumb." The classic mechanism of injury involves a fall onto an outstretched hand while grasping an object (such as a ski pole), which imparts a forceful radial and palmar abduction force to the thumb. Despite numerous advancements and modifications in ski pole design, epidemiological data has not demonstrated a significant reduction in the incidence of this injury. Patients typically present with localized pain, profound swelling, ecchymosis over the ulnar aspect of the MCP joint, and subjective weakness during key pinch maneuvers.
Surgical Anatomy and Biomechanics
A profound understanding of the thumb MCP joint anatomy is paramount for accurate diagnosis and anatomic surgical reconstruction. The stability of the thumb MCP joint relies on both static and dynamic restraints.
Static Restraints
The primary static stabilizers are the proper ulnar collateral ligament (pUCL) and the accessory ulnar collateral ligament (aUCL).
* Proper Ulnar Collateral Ligament (pUCL): Originates from the dorsal-ulnar aspect of the metacarpal head and inserts onto the volar-ulnar aspect of the proximal phalanx base. The pUCL is eccentric; it is lax in extension and becomes maximally taut in 30 degrees of MCP joint flexion.
* Accessory Ulnar Collateral Ligament (aUCL): Lies volar to the pUCL, originating from the same metacarpal footprint but inserting onto the volar plate and the sesamoid bones. The aUCL is taut in full extension and lax in flexion.
Clinical Pearl: Differentiating between a pUCL and aUCL injury relies on clinical stress testing. Valgus instability present only in 30 degrees of flexion indicates an isolated pUCL tear. Instability in both full extension and flexion indicates a combined tear of both the pUCL and aUCL, often involving the volar plate.
Anatomic Footprint Dimensions
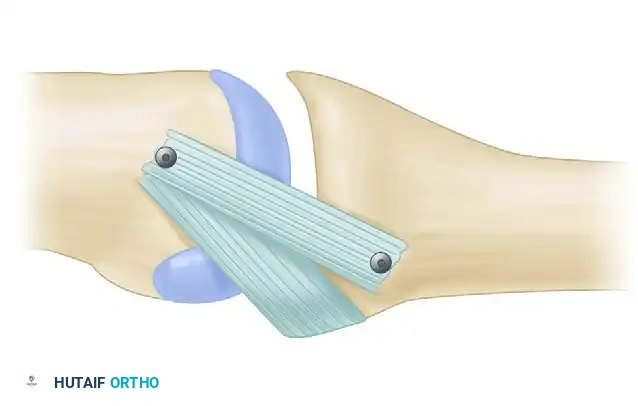
Precise knowledge of the ligamentous footprints is critical to avoid non-anatomic repair, which can lead to a "cam effect" and subsequent loss of joint motion. As demonstrated in biomechanical studies (e.g., Bean et al., 1999), the mean locations of the origin and insertion of the proper UCL must be respected during anchor placement.
Mean locations of origin and insertion of the proper ulnar collateral ligament of the thumb metacarpophalangeal joint. Note the precise dimensions: the metacarpal origin spans approximately 7mm, located 3mm proximal to the articular margin, while the phalangeal insertion spans 8mm.
Dynamic Restraints
The dynamic stabilizers include the intrinsic muscles of the thumb, most notably the adductor pollicis. The adductor aponeurosis expands over the ulnar aspect of the MCP joint, inserting into the extensor expansion. This structure plays a critical role in the pathoanatomy of complete UCL ruptures.
Pathoanatomy: The Stener Lesion
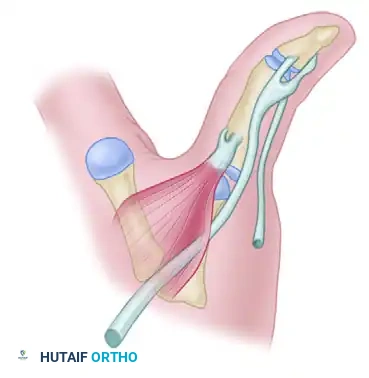
In 1962, Stener described a pathoanatomic phenomenon that fundamentally dictates the surgical management of complete thumb UCL ruptures. When a forceful valgus load causes a complete distal avulsion of the UCL from its insertion on the proximal phalanx, the adductor aponeurosis can forcefully strip the ligament proximally.
As the thumb returns to a resting position, the torn end of the UCL folds back on itself and becomes trapped superficial to the adductor aponeurosis. This interposition of the adductor aponeurosis between the ruptured UCL and its anatomic insertion site on the proximal phalanx physically prevents the ligament from healing. A Stener lesion occurs in approximately 80% of complete UCL ruptures and is an absolute indication for surgical intervention, as conservative management will uniformly result in chronic instability.
Clinical Evaluation and Diagnostic Imaging
Physical Examination
The hallmark of a UCL rupture is pain and laxity over the ulnar aspect of the thumb MCP joint.
1. Palpation: Tenderness is typically maximal at the ulnar base of the proximal phalanx. A palpable mass proximal to the joint line may represent the retracted ligament in a Stener lesion.
2. Valgus Stress Testing: This is the definitive clinical test. It must be performed with the MCP joint in full extension (testing the aUCL and volar plate) and in 30 degrees of flexion (isolating the pUCL).
* Diagnostic Criteria for Complete Rupture: Valgus laxity greater than 30 degrees absolute, or greater than 15 degrees compared to the contralateral, uninjured thumb.
Surgical Warning: If a Stener lesion is suspected, aggressive valgus stress testing should be avoided or performed with extreme caution, as it can theoretically convert an incomplete, non-displaced tear into a displaced Stener lesion.
Diagnostic Imaging
Radiographs: Standard posteroanterior, lateral, and Robert's view radiographs of the thumb are mandatory to rule out associated fractures. A bony avulsion fracture at the ulnar base of the proximal phalanx may be present. If the avulsion fragment is displaced >2 mm or involves >20% of the articular surface, surgical fixation is indicated.
Advanced Imaging: Ultrasonography, arthrography, and Magnetic Resonance Imaging (MRI) have been used successfully to distinguish complete from incomplete tears. MRI is highly sensitive and specific for identifying the retracted ligament and the interposed adductor aponeurosis characteristic of a Stener lesion.

MRI appearance of a Stener lesion. The coronal view demonstrates the completely avulsed ulnar collateral ligament retracted proximally and resting superficial to the low-signal adductor aponeurosis.
Non-Operative Management
Incomplete ruptures (Grade I and Grade II sprains) of the ulnar collateral ligament of the thumb are common and require only proper protection for the restoration of function. In these cases, the ligament remains anatomically aligned, and the adductor aponeurosis is not interposed.
- Protocol: A thumb spica cast or a custom-molded thermoplastic functional brace is recommended for 4 to 6 weeks. The IP joint is typically left free to prevent stiffness.
- Prognosis: Patients should be counseled that while stability is reliably restored, mild pain and swelling may persist for several months following the injury.
Surgical Indications
Acute complete rupture of the ulnar collateral ligament (Grade III) should be surgically repaired. Specific indications include:
1. Clinical valgus laxity >30 degrees or >15 degrees compared to the contralateral side.
2. Radiographic or MRI evidence of a Stener lesion.
3. Displaced bony avulsion fractures (>2 mm displacement or significant articular involvement).
4. Chronic symptomatic instability impairing pinch strength.
Operative Technique: Acute Repair
Acute repair is ideally performed within the first 3 weeks of injury. If the diagnosis is delayed for 1 month or longer, fibrosis makes ligament identification and repair significantly more difficult.
1. Positioning and Anesthesia
The procedure is typically performed under regional anesthesia (axillary or supraclavicular block) or general anesthesia. The patient is positioned supine with the operative arm extended on a hand table. A well-padded upper arm tourniquet is applied.
2. Surgical Approach
- A lazy-S or chevron incision is made over the ulnar aspect of the thumb MCP joint, centered over the joint line.
- Blunt dissection is utilized in the subcutaneous tissues to identify and protect the terminal sensory branches of the superficial radial nerve. Neuroma formation in this area is highly morbid.
3. Identification of the Stener Lesion
Once the subcutaneous tissue is cleared, the adductor aponeurosis is visualized. In the presence of a Stener lesion, the ruptured distal end of the UCL will be seen folded back, pointing proximally, and resting superficial to the aponeurosis.

Complete rupture of the ulnar collateral ligament of the metacarpophalangeal joint of the thumb. The ligament is ruptured distally and is folded back so that its distal end points proximally, creating the classic Stener lesion.
4. Joint Exposure and Preparation
- The adductor aponeurosis is carefully incised longitudinally, parallel to the extensor pollicis longus (EPL) tendon, leaving a small cuff for later repair.
- Retracting the aponeurosis exposes the underlying joint capsule and the anatomic footprint of the UCL on the proximal phalanx.
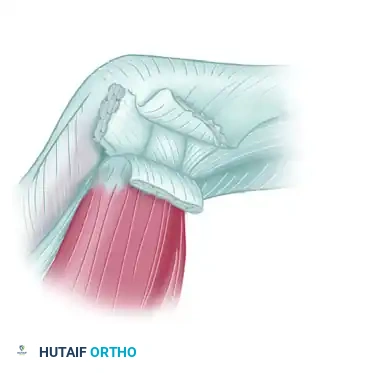
The adductor aponeurosis has been divided and retracted, exposing the underlying joint capsule, the articular surface, and the anatomic insertion site of the ulnar collateral ligament on the proximal phalanx.
- The joint is inspected for osteochondral loose bodies. The anatomic footprint at the volar-ulnar base of the proximal phalanx is debrided of soft tissue and lightly decorticated with a curette or rongeur to provide a bleeding bone bed for ligament healing.
5. Ligament Repair
- Suture Anchor Technique: A micro-suture anchor (typically 1.3 mm to 1.5 mm) is inserted into the prepared footprint on the proximal phalanx. The anchor must be placed precisely at the anatomic insertion to prevent kinematic alterations.
- The sutures are passed through the distal end of the UCL using a locking grasping stitch (e.g., Krackow or modified Kessler).
- The joint is held in slight flexion (10-15 degrees) and slight ulnar deviation to reduce tension, and the sutures are tied securely.
- Alternative (Pull-out Suture): If the distal tissue is highly fragmented, a pull-out suture over a dorsal button can be utilized, though this is less common with modern anchor technology.
6. Closure and Dynamic Reinforcement
- The detached tendinous insertion of the adductor muscle (adductor aponeurosis) is repaired over the reconstructed ligament. It can be advanced slightly and reattached to furnish a dynamic reinforcement to the medial joint line.
- The skin is closed with non-absorbable sutures, and a sterile dressing and thumb spica splint are applied.
Operative Technique: Chronic Reconstruction
If the repair is attempted several months after the injury, direct primary repair is often impossible due to ligamentous retraction, atrophy, and extensive fibrosis. While repair can sometimes be achieved by dissecting out the ligament from within the fibrotic mass and reattaching it appropriately, a free tendon graft is frequently required to replace the incompetent ligament.
Graft Selection
Common autograft choices include:
* Palmaris Longus Tendon: The most common choice due to ease of harvest and minimal donor site morbidity.
* Extensor Pollicis Brevis (EPB) Tendon: Can be used either split or in total.
* Strip of Fascia Lata: Rarely required but provides robust tissue.
Reconstruction Technique
- Bone Tunnels: Drill holes are created at the anatomic origin on the metacarpal head and the insertion on the proximal phalanx.
- Graft Routing: The graft can be configured in a "box-like" or "figure-of-eight" pattern. The tendon is passed through the proximal and distal attachments of the ligament.
- Fixation: The graft is threaded through the bone tunnels and attached via interference screws, suture anchors, or a pull-out technique. Tensioning is performed with the MCP joint in 30 degrees of flexion to ensure stability without over-constraining the joint.
Pitfall: Over-tensioning the graft during chronic reconstruction is a common error. This will result in a severe loss of MCP joint flexion. The graft should be tensioned to eliminate valgus laxity while still allowing full passive flexion of the joint prior to final fixation.
Salvage Procedure: MCP Joint Arthrodesis
Arthrodesis (fusion) of the thumb metacarpophalangeal joint is a highly reliable salvage procedure. It is specifically indicated when:
* There are advanced osteoarthritic changes within the MCP joint.
* There is global joint instability (combined severe volar plate, radial, and ulnar collateral ligament incompetence).
* Previous ligamentous reconstructions have failed.
Arthrodesis Technique
- The joint surfaces are prepared using a cup-and-cone reamer system to maximize bony contact while allowing for precise positioning.
- The ideal position for fusion is 10 to 15 degrees of flexion, 5 degrees of valgus, and slight pronation to maximize pinch strength against the index finger.
- Fixation is typically achieved using a dorsal low-profile titanium plate and screws, or crossed Kirschner wires combined with a tension band construct.
Postoperative Protocol and Rehabilitation
Meticulous postoperative care is essential to balance ligamentous healing with the prevention of joint stiffness.
- Weeks 0-4: The thumb is immobilized in a short-arm thumb spica cast or rigid splint. The interphalangeal (IP) joint is left free, and the patient is encouraged to perform active IP joint range of motion exercises immediately to prevent extensor lag.
- Weeks 4-6: The cast is removed, and the patient is transitioned to a removable custom thermoplastic thumb spica splint. Active range of motion (AROM) of the MCP joint is initiated. Passive range of motion (PROM) and valgus stress are strictly avoided.
- Weeks 6-8: The splint is gradually weaned for light activities of daily living. Gentle PROM is introduced if stiffness persists.
- Weeks 8-12: Progressive strengthening exercises, focusing on key pinch and grip strength, are initiated.
- Return to Play: Athletes may return to sports at 10 to 12 weeks postoperatively, often requiring a protective playing splint or taping for an additional 1 to 2 months, particularly in contact sports or skiing.
By adhering to strict anatomic principles, recognizing the presence of Stener lesions, and executing precise surgical techniques, orthopedic surgeons can reliably restore stability and function to the thumb MCP joint following severe ulnar collateral ligament ruptures.
You Might Also Like