Mastering Thumb Metacarpophalangeal and Trapeziometacarpal Joint Arthrodesis

Key Takeaway
Thumb metacarpophalangeal (MCP) and trapeziometacarpal (TMC) joint arthrodesis are highly effective salvage procedures for advanced arthritis, paralytic deformities, and severe instability. Achieving a stable, painless thumb ray requires meticulous joint preparation, precise biomechanical positioning—typically 20 degrees of MCP flexion—and rigid internal fixation. This guide details the step-by-step surgical execution of intramedullary screw fixation and tension band wiring, ensuring optimal functional outcomes for high-demand patients.
INTRODUCTION TO THUMB RAY ARTHRODESIS
The thumb ray is the cornerstone of hand biomechanics, responsible for approximately 40% to 50% of overall hand function. Pathologies afflicting the thumb metacarpophalangeal (MCP) and trapeziometacarpal (TMC) joints—ranging from advanced osteoarthritis and rheumatoid arthritis to post-traumatic instability and paralytic deformities—can severely debilitate a patient's grip and pinch strength.
While arthroplasty remains a viable option for many, arthrodesis is the gold standard for achieving a strong, powerful, stable, and painless thumb, particularly in younger, high-demand patients or those with profound neuromuscular impairment. This comprehensive masterclass details the surgical indications, biomechanical considerations, and step-by-step operative techniques for both thumb MCP and TMC joint arthrodesis.
THUMB METACARPOPHALANGEAL (MCP) JOINT ARTHRODESIS
Arthrodesis of the thumb MCP joint is a highly reliable procedure that provides excellent pain relief and stability with minimal functional deficit, provided the interphalangeal (IP) and TMC joints remain mobile.
Indications and Patient Selection
The primary indications for thumb MCP joint arthrodesis include:
* Advanced Osteoarthritis or Rheumatoid Arthritis: Severe articular cartilage destruction with associated deformity (e.g., severe hyperextension or boutonnière deformities).
* Chronic Instability: Failed reconstruction of the ulnar collateral ligament (UCL) or radial collateral ligament (RCL), often seen in chronic gamekeeper's thumb or Stener lesions.
* Paralytic Deformities: Stabilization required in patients with cerebral palsy, tetraplegia, or peripheral nerve palsies (e.g., median/ulnar nerve lesions) to facilitate pinch reconstruction.
* Post-Traumatic Arthrosis: Intra-articular malunions or severe crush injuries.
Clinical Pearl: In patients with concurrent TMC joint arthritis, fusing the MCP joint can exacerbate stresses on the TMC joint. Always evaluate the entire thumb ray. If the TMC joint is symptomatic, address it concurrently or consider alternative reconstructive options.
Preoperative Imaging and Templating
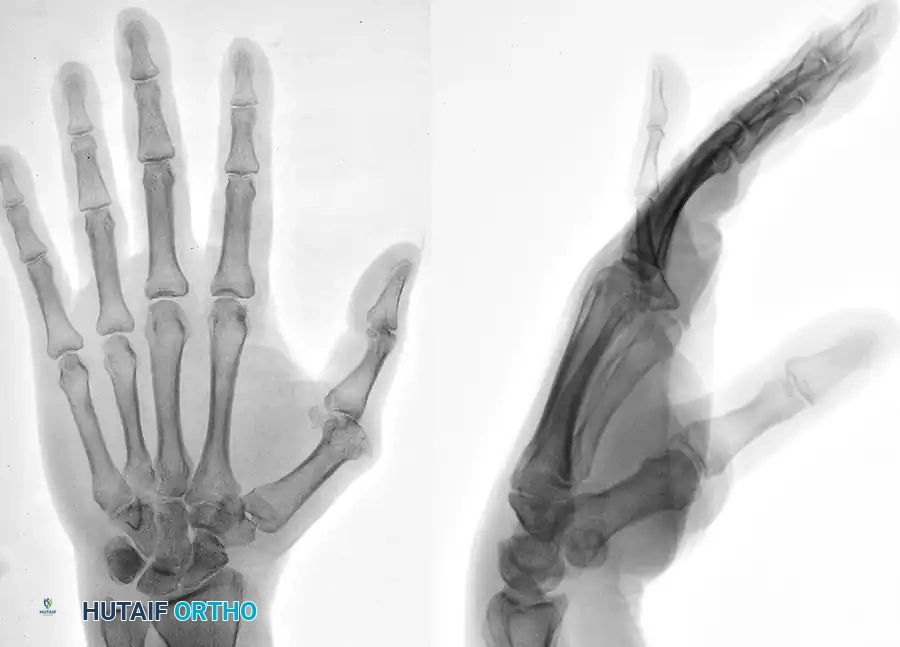
Standard posteroanterior (PA), lateral, and Robert's view radiographs are mandatory to assess bone stock, deformity, and the presence of osteophytes.
Preoperative radiograph demonstrating severe arthritic involvement, joint space narrowing, and subluxation of the thumb metacarpophalangeal joint.
Biomechanics and Optimal Positioning
The functional success of an MCP arthrodesis hinges entirely on the fusion angle.
* Flexion: The joint must be fused at 15 to 20 degrees of flexion. Excessive flexion impairs the ability to open the hand for large objects, while absolute extension (0 degrees) severely weakens pinch strength and limits dexterity.
* Pronation/Supination: The thumb should be positioned in neutral to slight pronation (5 to 10 degrees) to maximize pulp-to-pulp contact with the index and middle fingers.
* Abduction/Adduction: Neutral alignment is required; avoid any ulnar or radial deviation.
SURGICAL TECHNIQUE: MCP ARTHRODESIS WITH INTRAMEDULLARY SCREW FIXATION
Intramedullary screw fixation provides rigid, low-profile osteosynthesis, allowing for early mobilization and high union rates.
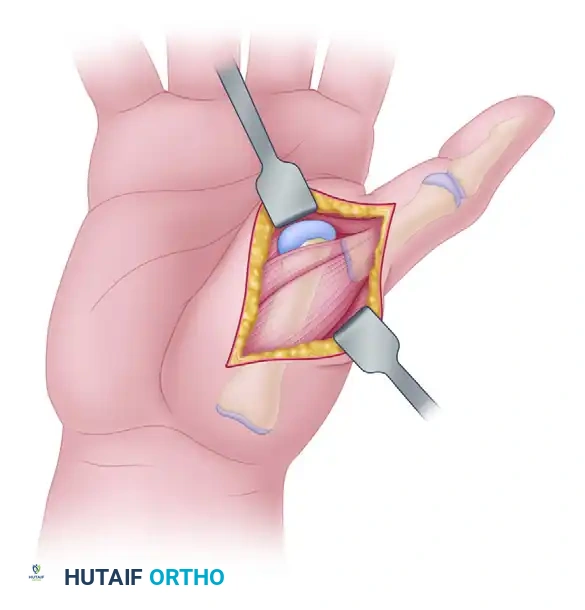
Step 1: Surgical Approach and Exposure
- Incision: Make a dorsal longitudinal or slightly curvilinear incision over the thumb MCP joint, measuring approximately 3 to 4 cm.
- Tendon Management: Identify and protect the sensory branches of the superficial radial nerve. Incise the extensor hood longitudinally. The extensor pollicis longus (EPL) tendon is typically retracted ulnarly, and the extensor pollicis brevis (EPB) is retracted radially, or the interval between them is split.
- Capsulotomy: Perform a longitudinal dorsal capsulotomy to expose the articular surfaces of the metacarpal head and the base of the proximal phalanx. Release the collateral ligaments to allow complete joint subluxation and visualization.
Step 2: Articular Preparation
- Cartilage Removal: Use rongeurs, a coarse-tooth oscillating saw, or congruent cup-and-cone reamers to denude the articular cartilage down to bleeding subchondral bone.
- Contouring: Prepare the subchondral bone to achieve exactly a 20-degree flexion angle. The cup-and-cone technique is highly recommended as it allows for minor adjustments in pronation and flexion while maintaining maximal cancellous bone contact.
- Coaptation: Ensure full, flush contact of the raw cancellous metacarpal and proximal phalangeal surfaces.
Step 3: Guide Wire Placement and Reaming
- Positioning: Hold the MCP joint at the desired 20-degree angle with maximal cancellous contact.
- Wire Insertion: Drive a guide wire antegrade from the dorsal base of the proximal phalanx, across the prepared joint space, and into the medullary canal of the first metacarpal.
- Fluoroscopic Verification: Verify the guide wire position, joint angle, and rotation using orthogonal fluoroscopy.
- Reaming: Pass a cannulated reamer over the guide wire, sizing it according to the planned screw diameter (typically a 3.0 mm or 3.5 mm headless compression screw or standard cortical screw).
Step 4: Screw Insertion and Construct Evaluation
- Fixation: Advance the intramedullary screw over the wire. Seat the screw head just beneath the dorsal cortex of the metacarpal neck or proximal phalanx (depending on the trajectory) to prevent hardware prominence.
- Compression: Ensure robust compression across the arthrodesis site. Evaluate the stability of the construct under direct vision and fluoroscopy.
Postoperative radiograph demonstrating successful thumb metacarpophalangeal arthrodesis utilizing rigid intramedullary screw fixation.
Step 5: Closure
- Capsular Repair: Close the joint capsule over the low-profile construct using 4-0 absorbable sutures.
- Extensor Mechanism: Reapproximate the extensor pollicis brevis and the extensor hood with a 4-0 nonabsorbable braided suture to restore extensor biomechanics.
- Skin Closure: Close the skin with interrupted nonabsorbable sutures and apply a bulky, sterile thumb spica splint.
ALTERNATIVE TECHNIQUE: MCP ARTHRODESIS WITH TENSION BAND WIRING
In cases of severe bone loss, osteopenia, or when intramedullary screw fixation is anatomically unfeasible, tension band wiring provides excellent biomechanical stability by converting dorsal tensile forces into volar compressive forces.
Step-by-Step Execution
- Joint Preparation: Prepare the subchondral bone to a 20-degree flexion angle with full cancellous contact, identical to the screw technique.
- Transverse Drill Hole: Make a transverse hole using a 0.045-inch Kirschner (K-) wire in the distal third of the proximal phalangeal neck. This hole will serve as the anchor for the tension band wire.
- Wire Passage: Pass a 22-gauge spool wire (cerclage wire) through this transverse hole.
- Longitudinal K-wire Fixation: Hold the MCP joint in the desired position. Drive two 0.045-inch K-wires longitudinally (or slightly crossed) across the fusion site from the metacarpal neck into the proximal phalangeal medullary canal. Verify their position via fluoroscopy.
- Tension Band Construct: Cross the 22-gauge wire in a figure-of-eight fashion. Place one limb beneath the proximal ends of the K-wires projecting from the metacarpal neck.
- Tensioning: Take the slack out of the 22-gauge wire. Twist the wire symmetrically to generate compression across the arthrodesis site, cut the excess, and bury the twisted end deep into the soft tissues adjacent to the fusion site to prevent skin irritation.
- K-wire Management: Hold the protruding K-wires and bend their ends.
> Surgical Pearl: Use a neurotip sucker or a dedicated wire bender to create tight hooked ends. Cut the excess wire and tamp the hooks firmly into the metacarpal neck cortex to prevent migration and soft tissue tethering. - Closure: Close the capsule and the extensor pollicis brevis over the construct as described previously.
TRAPEZIOMETACARPAL (TMC) JOINT ARTHRODESIS
While trapeziometacarpal joint arthroplasty (e.g., Ligament Reconstruction Tendon Interposition - LRTI) provides excellent mobility and pain relief for older, lower-demand patients, TMC arthrodesis is the procedure of choice for specific demographics requiring absolute stability.
Indications and Patient Selection
Arthrodesis is highly recommended for:
* Younger, High-Demand Patients: Manual laborers, mechanics, and athletes who require a strong, powerful, and stable pinch grip.
* Post-Traumatic Arthritis: Isolated TMC joint destruction following Bennett or Rolando fractures.
* Neuromuscular Disorders: Stabilization of congenital deformities, paralytic hands, or spasticity associated with cerebral palsy.
Surgical Warning: Arthrodesis provides a stable and strong joint strictly at the expense of thumb mobility. Patients must be extensively counseled that they will lose the ability to place the thumb flat on a table (loss of extreme extension/abduction).
Differential Diagnosis of Radial Sided Wrist Pain
Before committing to a TMC arthrodesis, the surgeon must meticulously rule out other causes of pain in the radial wrist:
* de Quervain Tenosynovitis: Pain on passive thumb adduction and wrist ulnar deviation (positive Finkelstein test) indicates first extensor compartment pathology.
* Carpal Tunnel Syndrome (CTS): Typical symptoms of median nerve compression must be evaluated via Tinel's sign, Phalen's test, and EMG/NCS if necessary.
* Flexor Carpi Radialis (FCR) Tendinitis: Tenderness localized to the FCR fibro-osseous tunnel.
* Scaphotrapezial Trapezoidal (STT) Arthritis: Radiographic evidence of adjacent joint arthritis. Fusing the TMC joint in the presence of STT arthritis will rapidly accelerate STT degeneration and pain.
* TMC Pathology Confirmation: Pain elicited on passive rotation of the thumb metacarpal with axial compression against the trapezium (a positive "grind test") reliably localizes the pathology to the TMC joint.
Biomechanics and Optimal Positioning for TMC Arthrodesis
The functional utility of the hand relies heavily on the spatial orientation of the fused first metacarpal.
* Pinch Kinematics: The position of the first metacarpal must permit effortless pulp-to-pulp pinch to the index finger. Furthermore, with thumb interphalangeal (IP) joint flexion, the thumb pulp must be able to reach the middle finger.
* Fist Clearance: Extension of the thumb MCP joint must move the thumb sufficiently out of the palm to permit a full, unobstructed fist with all ulnar digits.
* Standard Angles: The generally accepted position is 35 to 40 degrees of palmar abduction, 10 to 15 degrees of radial extension, and 15 degrees of pronation.
Surgical Techniques and Fusion Constructs
Achieving a solid union at the TMC joint can be challenging due to the dense cortical bone of the trapezium and the high shear forces across the joint. Several techniques have been developed to maximize fusion rates (historically >90% when performed correctly).
- The "Cone and Cup" Technique (Bamberger et al.):
This technique utilizes congruent reamers to create a convex surface on the trapezium and a concave surface on the metacarpal base. This maximizes cancellous bone contact and allows for multi-planar micro-adjustments before definitive fixation. - The Sliding Graft Technique (Doyle):
Involves taking a sliding cortical-cancellous graft from the dorsal first metacarpal and advancing it across the decorticated TMC joint into a slot created in the trapezium. This provides intrinsic biological bridging and structural stability. - Hardware Selection:
Fixation can be achieved using multiple K-wires, tension band constructs, staples, or specialized locking plates.
> Surgical Pitfall: Increased nonunion rates (up to 20-30% in some series) have been reported when screws alone are used to attempt fusion. The shear forces at the base of the thumb frequently overcome the compression of a single screw. If screws are utilized, they must be augmented with a neutralization plate or a tension band construct.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Rigorous postoperative management is critical to prevent nonunion and hardware failure in both MCP and TMC arthrodesis.
- Phase I (0 to 4 Weeks):
- The patient is placed in a rigid, well-molded fiberglass thumb spica cast immediately postoperatively.
- Strict elevation is maintained to control edema.
- Active range of motion (AROM) of the unoperated digits (IP joint of the thumb, fingers, and wrist if not included in the cast) is encouraged immediately to prevent stiffness and tendon adhesions.
- Phase II (4 to 8 Weeks):
- The cast is removed, and clinical/radiographic evaluation is performed.
- If early bridging trabeculae are visible, the patient is transitioned to a custom thermoplastic thumb spica splint.
- Gentle AROM of the adjacent joints is progressed. Heavy lifting and forceful pinch are strictly prohibited.
- Phase III (8 to 12 Weeks):
- Once radiographic union is confirmed (typically 8 to 10 weeks), the splint is gradually weaned.
- Progressive strengthening, focusing on pinch and grip strength, is initiated under the guidance of a certified hand therapist (CHT).
- Full unrestricted activity is generally permitted by 12 weeks postoperatively, provided clinical and radiographic union is absolute.
COMPLICATIONS AND MANAGEMENT
- Nonunion: The most significant complication, particularly in TMC arthrodesis using standalone screws. Management requires revision surgery with robust bone grafting (iliac crest or distal radius) and rigid plate osteosynthesis.
- Hardware Prominence: Common with K-wires and dorsal plates. Symptomatic hardware should be removed only after solid bony union is confirmed (minimum 6 months post-op).
- Malunion: Fusing the MCP joint in hyperextension or the TMC joint in inadequate palmar abduction severely limits pinch mechanics. Prevention through meticulous intraoperative fluoroscopic evaluation is paramount. Corrective osteotomy is required for symptomatic malunions.
- Adjacent Segment Disease: Fusing the TMC joint increases stress on the STT and MCP joints. Patients should be monitored long-term for the development of compensatory arthritis.
By adhering to strict biomechanical principles, ensuring meticulous joint preparation, and selecting the appropriate fixation construct, orthopedic surgeons can reliably restore powerful, pain-free thumb function through MCP and TMC arthrodesis.
===FINAL_DONE===
You Might Also Like