Mastering Thumb Metacarpophalangeal Joint Instability: Open Reduction Techniques and UCL Repair
Key Takeaway
Thumb metacarpophalangeal (MCP) joint dislocations and ulnar collateral ligament (UCL) ruptures require precise anatomical understanding for optimal management. Irreducible dorsal dislocations often necessitate a volar open reduction to release the entrapped metacarpal head. Conversely, complete UCL ruptures frequently involve a Stener lesion, mandating surgical repair. This guide details the biomechanics, diagnostic stress radiography, and step-by-step surgical techniques for restoring thumb MCP joint stability.
Introduction to Thumb Metacarpophalangeal Joint Instability
The thumb metacarpophalangeal (MCP) joint is a complex diarthrodial joint that relies on a delicate balance of static and dynamic stabilizers to maintain congruency during the high-stress activities of pinch and grasp. Injuries to this joint span a spectrum from simple sprains to complex, irreducible dislocations and complete ligamentous ruptures. Understanding the intricate pathoanatomy of the volar plate, the collateral ligaments, and the intrinsic musculature is paramount for the orthopedic surgeon. Mismanagement of these injuries—particularly unrecognized Stener lesions or inappropriate traction during dislocation reduction—can lead to chronic instability, debilitating pain, and early-onset arthrosis.
This comprehensive guide delineates the evidence-based protocols for managing thumb MCP joint dislocations, with a specific focus on the volar approach for open reduction, and provides a masterclass on the diagnosis and management of ulnar collateral ligament (UCL) ruptures.
Pathoanatomy of Thumb MCP Joint Dislocations
Dislocations of the thumb MCP joint are predominantly dorsal, resulting from forced hyperextension injuries. Palmar dislocations are exceedingly rare but present unique reconstructive challenges.
Dorsal Dislocations and the "Noose" Effect
In a complete dorsal dislocation, the proximal phalanx comes to rest on the dorsal aspect of the metacarpal head and neck. The primary pathology involves the rupture of the membranous proximal attachment of the volar plate. As the proximal phalanx displaces dorsally, it carries the volar plate with it, interposing the plate between the base of the phalanx and the dorsal aspect of the metacarpal head.
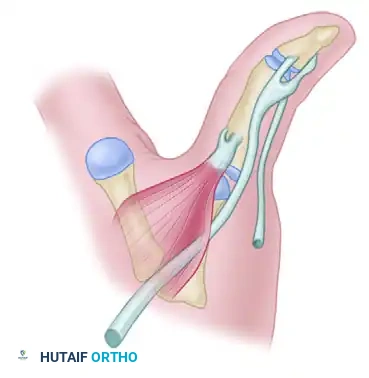
Simultaneously, the metacarpal head is driven volarly, protruding through a rent in the anterior joint capsule and the intrinsic muscle expansions. The metacarpal neck becomes tightly constricted by a "noose" formed by:
* Volar: The natatory ligament and the superficial transverse metacarpal ligament.
* Dorsal: The displaced volar plate.
* Ulnar: The flexor pollicis longus (FPL) tendon and the adductor pollicis.
* Radial: The flexor pollicis brevis (FPB) and abductor pollicis brevis (APB).
🚨 Surgical Warning: The Danger of Longitudinal Traction
Applying longitudinal traction to a dislocated thumb MCP joint is strictly contraindicated. Traction tightens the intrinsic "noose" around the metacarpal neck, converting a potentially reducible simple dislocation into a complex, irreducible dislocation. The metacarpal neck becomes irrevocably caught by the capsular structures.
Palmar Dislocations
Palmar dislocation of the thumb proximal phalanx is a rare entity, typically resulting from a hyperflexion injury combined with a rotational force. While some can be reduced closed, they become irreducible if the metacarpal head becomes trapped between the extensor pollicis longus (EPL) and extensor pollicis brevis (EPB) tendons. In such cases, a dorsal surgical approach is required to open the dorsal aponeurosis and relocate the extensor tendons around the MCP joint.
Closed Reduction Techniques and Pitfalls
Before proceeding to operative intervention, a meticulous closed reduction attempt should be performed under adequate local anesthesia (e.g., a median and radial nerve block or a local hematoma block).
The correct reduction maneuver:
1. Do not apply traction.
2. Adduct the metacarpal to relax the intrinsic muscles.
3. Hyperextend the dislocated MCP joint to unlock the proximal phalanx from the metacarpal neck.
4. Flex the interphalangeal (IP) joint to reduce tension on the flexor pollicis longus (FPL) tendon.
5. Apply direct, distally directed pressure to the dorsal base of the proximal phalanx, pushing it over the metacarpal head while simultaneously flexing the MCP joint.
If this maneuver fails, the dislocation is deemed complex and irreducible, necessitating prompt open reduction.
Surgical Technique: Open Reduction—Volar Approach
The volar approach is the gold standard for addressing irreducible dorsal dislocations of the thumb MCP joint, as it provides direct visualization of the entrapped metacarpal head and the constricting intrinsic musculature.
Indications and Preoperative Planning
- Indications: Irreducible dorsal dislocation of the thumb MCP joint; delayed presentation of a dislocated joint; suspected intra-articular osteochondral fracture blocking reduction.
- Anesthesia: Regional block (axillary or supraclavicular) or general anesthesia.
- Equipment: Hand tray, fine retractors (Senn, Ragnell), Freer elevator, 0.045-inch Kirschner wires (K-wires), wire driver, fluoroscopy (C-arm).
Positioning and Approach
- Place the patient supine with the operative arm extended on a radiolucent hand table.
- Apply a well-padded upper arm tourniquet and exsanguinate the limb.
- Make a volar or mid-lateral incision. A volar zigzag (Bruner) incision centered over the MCP joint provides excellent exposure while preventing postoperative flexion contractures.
- Carefully dissect through the subcutaneous tissue. Identify and protect the radial and ulnar digital neurovascular bundles, which are often displaced superficially and stretched over the protruding metacarpal head.
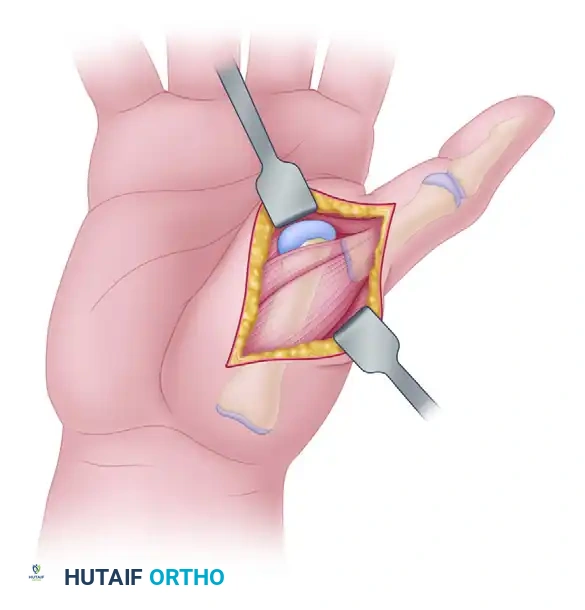
Surgical exposure demonstrating the metacarpal head protruding through the capsular rent, bordered by the flexor pollicis brevis and abductor pollicis brevis.
Deep Dissection and Metacarpal Head Release
- Expose the volar aspect of the MCP joint. The metacarpal head will be immediately visible, protruding through the anterior capsule and the intrinsic muscle bellies.
- Identify the proximal phalangeal base, which lies abnormally on the dorsal aspect of the metacarpal head and neck.
- Locate the flexor pollicis brevis (FPB) muscle, which often forms the radial border of the constricting noose.
- Carefully disengage the FPB muscle and the surrounding capsular rent using a Freer elevator or tenotomy scissors. This critical step releases the tension on the metacarpal neck.
- Identify the volar plate, which is typically avulsed proximally and interposed dorsally within the joint space. Use a blunt hook or elevator to extract the volar plate from the joint space.
Joint Reduction and Fixation
- With the constricting elements released and the volar plate extracted, flex the thumb and gently push the metacarpal head dorsally through the capsular rent to complete the reduction.
- Assess joint stability under direct vision and fluoroscopy.
- Pinning: To protect the soft tissue repair and maintain congruency, secure the joint with a 0.045-inch Kirschner wire. Drive the K-wire obliquely across the MCP joint with the joint held in 20 degrees of flexion.
- Volar Plate Repair: In the rare event that the volar plate is found to be detached from the proximal phalanx (rather than its typical proximal membranous avulsion), surgical repair to the phalangeal base using suture anchors or transosseous sutures is justified.
- Deflate the tourniquet, achieve meticulous hemostasis, and close the skin with non-absorbable sutures.
🔪 Clinical Pearl: K-Wire Placement
Ensure the K-wire does not tether the extensor mechanism dorsally or the flexor tendons volarly. Confirm the pin placement with orthogonal fluoroscopic views to ensure it engages both the metacarpal head and the proximal phalanx securely.
Postoperative Care for MCP Dislocations
- Weeks 0-4: The thumb is immobilized in a well-molded thumb spica plaster splint or cast, holding the MCP joint in 20 degrees of flexion. The IP joint may be left free to prevent stiffness.
- Week 4: The splint and the Kirschner wire are removed in the clinic. Active range of motion (AROM) exercises are initiated.
- Weeks 4-6: A removable thermoplastic splint is used between exercise sessions and at night. Passive range of motion (PROM) and gentle strengthening are gradually introduced.
- Weeks 6+: Unrestricted activity is permitted as tolerated, though maximum medical improvement may take up to 6 months.
Ulnar Collateral Ligament (UCL) Ruptures (Skier's Thumb)
While dislocations involve gross joint failure, isolated ligamentous injuries—particularly to the ulnar collateral ligament (UCL)—are far more common. Historically termed "Gamekeeper's thumb" (chronic attenuation) or "Skier's thumb" (acute rupture), this injury results from forced radial deviation (abduction) of the thumb MCP joint.
Biomechanics and the Stener Lesion
The UCL provides primary restraint to valgus stress at the MCP joint. It consists of a proper collateral ligament (taut in flexion) and an accessory collateral ligament (taut in extension).
Differentiating between an incomplete (sprain) and a complete UCL rupture is critical because incomplete ruptures are treated nonoperatively, whereas complete ruptures almost universally require surgery. This dichotomy is primarily due to the Stener lesion.
Described by Stener in 1962, this anatomical pathology was found in 25 out of 39 complete ruptures of the UCL. When the UCL completely avulses from its distal insertion on the proximal phalanx, the adductor aponeurosis can slip beneath the torn ligament. As the thumb returns to a neutral position, the adductor aponeurosis becomes interposed between the ruptured UCL and its anatomical insertion site.
🚨 Pathological Consequence of the Stener Lesion
If left uncorrected, the interposed adductor aponeurosis physically prevents the UCL from healing back to the bone. This leads to chronic, debilitating pinch instability and subsequent early-onset arthrosis of the MCP joint.
Clinical Evaluation and Differential Diagnosis
Patients present with pain, swelling, and ecchymosis over the ulnar aspect of the thumb MCP joint. Tenderness is greatest over the ulnar aspect but may be diffuse initially.
On clinical examination, a prominent lump can often be palpated proximal to the MCP joint line. This mass represents the retracted UCL being proximally and superficially displaced by the adductor aponeurosis (the clinical hallmark of a Stener lesion). Pathological rotation of the thumb during pinch may also be evident.
Other injuries associated with valgus stress must be ruled out, including:
* Avulsion fractures of the proximal phalanx base.
* Dorsal capsular tears.
* Volar plate tears.
Radiographic Evaluation and Stress Testing
A strict diagnostic protocol is recommended to differentiate between complete and incomplete tears.
1. Plain Radiographs:
Standard posteroanterior (PA), lateral, and oblique radiographs must be obtained before any stress testing is performed.
* A minimally displaced (< 2 mm) avulsion fracture signifies a complete avulsion without a Stener lesion (the bony fragment prevents the ligament from retracting past the aponeurosis). This fracture usually heals well with cast immobilization.
* Contraindication: To prevent the iatrogenic creation of a Stener lesion, the joint should not be stressed if a non-displaced fracture is present. Furthermore, if a Salter-Harris type I or type II fracture is present in a pediatric patient, stress films are strictly contraindicated.
2. Stress Radiography:
After plain radiographs have ruled out contraindicating fractures, anteroposterior stress radiographs should be obtained of both thumbs for comparison. A local anesthetic (ulnar digital nerve block) is often necessary to eliminate muscle guarding and obtain an accurate assessment.
The surgeon may manually stress the joint while obtaining the radiographs, but this can be awkward and exposes the surgeon's hands to radiation, even with lead gloves. Standardized, patient-driven stress tests are preferred:
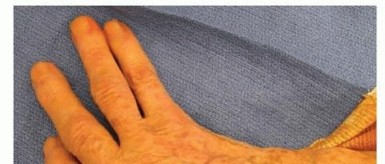
- The Tape Fulcrum Method: Tape the tips of both thumbs together. Have the patient actively abduct both thumbs over a roll of tape placed as a fulcrum between the thumb MCP joints while the AP radiograph is taken.
- The Rubber Band Method: Both thumbs are held together at the interphalangeal joint level with a stout rubber band. An image is obtained while the patient actively tries to separate their hands.

Clinical photograph demonstrating the rubber band technique. The rubber band apposes the interphalangeal joints while the patient actively attempts to separate their hands, applying a valgus stress to both MCP joints simultaneously.

Stress radiograph obtained during the rubber band test, demonstrating significant differential laxity. The injured thumb shows marked radial deviation at the MCP joint compared to the contralateral side.
Diagnostic Criteria: An injured thumb that demonstrates more than 30 degrees of absolute valgus instability, or greater than 15 degrees of instability compared with the uninjured contralateral side, indicates a complete UCL rupture.
Indications for Operative Intervention
Surgical repair is indicated for:
1. Complete UCL ruptures (clinical or radiographic instability >30 degrees).
2. Presence of a palpable Stener lesion.
3. Displaced avulsion fractures (>2 mm) or fractures involving >20% of the articular surface.
4. Chronic symptomatic instability.
Operative treatment typically involves a dorsal-ulnar incision, identification and splitting of the adductor aponeurosis, retrieval of the retracted UCL, and anatomical reattachment to the base of the proximal phalanx using suture anchors or transosseous routing.
Conclusion
The management of thumb metacarpophalangeal joint instability demands a profound respect for the local anatomy. Irreducible dorsal dislocations require a meticulous volar approach to release the constricting intrinsic muscles and extract the interposed volar plate, strictly avoiding longitudinal traction. Similarly, the accurate diagnosis of UCL ruptures via stress radiography is essential to identify Stener lesions, which mandate surgical repair to restore the vital pinch mechanics of the hand. Adherence to these evidence-based surgical principles ensures optimal functional recovery and prevents the debilitating sequelae of chronic instability.
You Might Also Like