Surgical Management of the Arthritic Hand: A Comprehensive Guide

Key Takeaway
The surgical management of the arthritic hand requires a profound understanding of altered biomechanics, progressive joint destruction, and soft-tissue imbalances. This comprehensive guide details the evaluation and operative treatment of rheumatoid and osteoarthritic deformities, including swan-neck, boutonnière, and ulnar drift. Emphasizing meticulous preoperative planning, cervical spine clearance, and precise surgical execution, it provides orthopaedic surgeons with evidence-based strategies to relieve pain, restore function, and improve cosmesis in complex arthritic presentations.
INTRODUCTION TO THE ARTHRITIC HAND
The surgical management of the arthritic hand represents one of the most complex and nuanced domains within orthopaedic surgery. Encompassing a spectrum of systemic and localized diseases—most notably Rheumatoid Arthritis (RA) and Osteoarthritis (OA), but also Systemic Lupus Erythematosus (SLE), Psoriatic Arthritis, Reiter Syndrome, Gout, and Scleroderma—the arthritic hand demands a comprehensive understanding of altered biomechanics, progressive joint destruction, and intricate soft-tissue imbalances.
Rheumatoid hand deformities are typically bilateral and symmetrical. The metacarpophalangeal (MCP) joints and the wrist are frequently affected early in the disease process, whereas the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints are typically involved later. The MCP joint is the cornerstone of finger function in rheumatoid disease; its deterioration initiates a cascade of biomechanical failures leading to the classic ulnar deviation and palmar subluxation.
Clinical Pearl: The surgeon must emphatically advise the patient that surgery neither cures the underlying systemic disease nor restores the hand to a normal, pre-disease state. The primary goals of operative intervention are to relieve pain, restore functional pinch and grasp, correct or prevent progressive deformity, and inhibit local disease progression.
PREOPERATIVE EVALUATION AND PATIENT COUNSELING
Systemic and Anesthetic Considerations
Patients with rheumatoid arthritis require meticulous preoperative systemic evaluation. The most critical step before any surgical intervention is the assessment of the cervical spine.
Surgical Warning: Asymptomatic atlantoaxial subluxation or mid-cervical instability is highly prevalent in severe RA. Flexion-extension radiographs of the cervical spine are mandatory to evaluate the atlantodens interval (ADI). An ADI greater than 3.5 mm indicates instability. This alerts the anesthesiologist to the severe risk of spinal cord injury during neck hyperextension or hyperflexion required for endotracheal intubation.
Furthermore, extensive involvement of the temporomandibular joint (TMJ) may restrict mouth opening, necessitating fiberoptic awake intubation.
Functional Assessment and Substitution Patterns
Patients with chronic, slowly progressive deformities often develop complex substitution patterns that enable them to perform activities of daily living (ADLs).
Pitfall: Never interrupt a functional substitution pattern without a careful analysis of the pathological anatomy. This is especially true in older, retired individuals who present with severe deformity but minimal pain. Correcting a deformity for purely cosmetic reasons in a pain-free, functional hand can lead to a disastrous loss of independence.
Informed Consent and Expectations
Hand appearance and pain relief are highly correlated with patient satisfaction. Before surgery, the patient must be thoroughly counseled regarding:
* The anticipated use of Kirschner wires (K-wires) and external splints.
* The location of incisions and expected postoperative cosmesis.
* The prolonged nature of postoperative rehabilitation and hand therapy.
* The realistic functional benefits versus the inherent risks of surgery.
PATHOMECHANICS AND CLASSIFICATION OF FINGER DEFORMITIES
The rheumatoid hand is characterized by a predictable progression of deformities driven by chronic synovitis, which causes capsular distention, ligamentous attenuation, and subsequent alteration of muscle vectors.
Ulnar Drift and MCP Joint Subluxation
Ulnar deviation with palmar subluxation or dislocation of the proximal phalanx is the hallmark of the rheumatoid hand.
* Pathomechanics: Synovitis distends the MCP joint capsule, attenuating the radial sagittal band. The extensor digitorum communis (EDC) tendon subluxates ulnarly into the intermetacarpal valley. The intrinsic muscles contract, pulling the proximal phalanx into palmar flexion and ulnar deviation. Carpal collapse (radial deviation of the wrist) further exacerbates the ulnar deforming forces on the fingers via the Z-collapse mechanism.
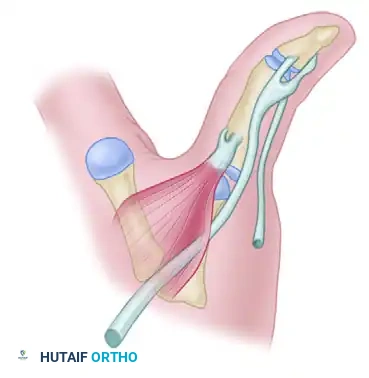
Swan-Neck Deformity
The swan-neck deformity is characterized by hyperextension of the PIP joint and flexion of the DIP joint.
* Pathomechanics: This deformity can originate at the MCP, PIP, or DIP joint. Primary PIP joint synovitis stretches the volar plate, allowing the lateral bands to subluxate dorsally to the axis of rotation. Alternatively, intrinsic tightness or MCP joint volar subluxation increases tension on the central slip, driving the PIP joint into hyperextension.
Figure 1: Dorsal view of a severe rheumatoid hand demonstrating profound ulnar drift, MCP joint palmar subluxation, and varying severities of swan-neck deformities in the digits.
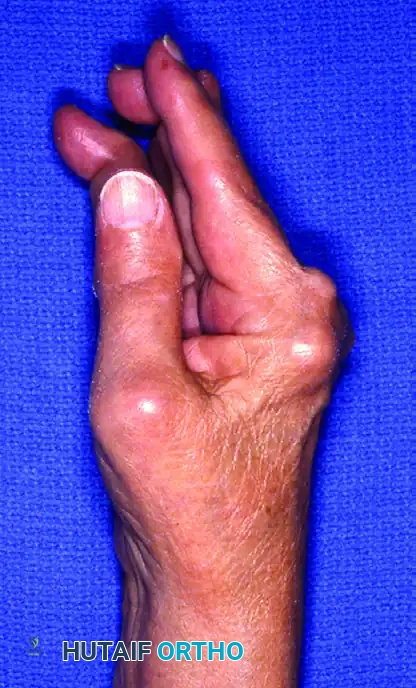
Figure 2: Lateral/oblique perspective highlighting the hyperextension of the PIP joints (swan-neck deformity) and the complex multi-planar deformities of the thumb.
Buttonhole (Boutonnière) Deformity
The boutonnière deformity consists of PIP joint flexion and DIP joint hyperextension.
* Pathomechanics: Chronic PIP joint synovitis attenuates and eventually ruptures the central slip of the extensor mechanism. The lateral bands subluxate volarly, falling below the axis of rotation of the PIP joint. They become flexors of the PIP joint while maintaining their extensor pull on the DIP joint, leading to the classic posture.
SURGICAL STAGING AND DECISION MAKING
When multiple joints are involved, the staging of operations is critical. The general principle is to correct proximal deformities before distal ones, as proximal alignment dictates distal biomechanics.
1. Wrist: The wrist is the foundation of the hand. A radially deviated, unstable wrist must be stabilized (via arthrodesis or arthroplasty) before or concurrent with MCP joint reconstruction.
2. MCP Joints: Reconstructed next to restore the primary arc of finger flexion and correct ulnar drift.
3. PIP/DIP Joints: Addressed last, as their function depends heavily on the balanced extrinsic and intrinsic forces crossing the MCP joint.
Prophylactic procedures, such as tenosynovectomy and synovectomy, are highly effective if performed before irreversible articular cartilage destruction or tendon rupture occurs.
OPERATIVE TECHNIQUES FOR FINGER DEFORMITIES
Intrinsic Release
Indicated for intrinsic plus deformity (positive Bunnell test) to prevent the progression of swan-neck deformities.
* Technique: A dorsal longitudinal or transverse incision is made over the MCP joints. The ulnar intrinsic wing is identified and resected. In severe cases, the radial intrinsic wing may also require release. Care is taken to preserve the transverse fibers of the intrinsic hood to maintain active MCP flexion.
Metacarpophalangeal Joint Arthroplasty
Silicone implant arthroplasty remains the gold standard for severe rheumatoid MCP joint destruction with fixed ulnar drift and palmar subluxation.
* Surgical Steps:
1. A transverse dorsal incision is made across the metacarpal heads.
2. The dorsal veins are meticulously preserved to prevent postoperative edema.
3. The extensor hood is incised longitudinally on the radial side of the EDC tendon (or through the attenuated radial sagittal band).
4. The metacarpal head is resected at the metaphyseal flare using an oscillating saw, perpendicular to the shaft.
5. A comprehensive synovectomy is performed.
6. The volar plate is released to correct palmar subluxation.
7. The medullary canals of the metacarpal and proximal phalanx are broached.
8. Appropriately sized silicone implants are inserted using a no-touch technique.
9. The radial sagittal band is imbricated and repaired to centralize the EDC tendon.
10. The intrinsic tendons on the ulnar side may be released or transferred to the radial side of the adjacent digit to augment radial stability.
Proximal Interphalangeal Joint Interventions
- Synovectomy: Indicated for persistent PIP synovitis without joint destruction.
- Arthroplasty: Silicone arthroplasty is preferred for the ring and small fingers to preserve grip span.
- Arthrodesis: Preferred for the index and middle fingers to provide a stable post for pinch against the thumb. The joint is typically fused at 25° to 40° of flexion, increasing from radial to ulnar digits.
TENDON RUPTURES AND TENOSYNOVITIS
Extensor Tenosynovitis and Rupture
Dorsal tenosynovitis often presents as a painless, boggy swelling over the wrist. If left untreated, the hypertrophic synovium invades the tendons, leading to rupture.
* Vaughan-Jackson Syndrome: The sequential rupture of the extensor tendons, beginning ulnarly with the extensor digiti minimi (EDM) and progressing radially to the EDC of the ring, middle, and index fingers. This is typically caused by attrition over a dorsally subluxated distal ulna (Mannerfelt lesion).
* Treatment: Dorsal tenosynovectomy, resection of the distal ulna (Darrach procedure or Suave-Kapandji), and tendon transfer (e.g., Extensor Indicis Proprius to EDC) or side-to-side tenodesis.
Flexor Tenosynovitis and Rupture
Flexor tenosynovitis can cause trigger digits, carpal tunnel syndrome, or tendon rupture (Mannerfelt-Norman syndrome, typically FPL rupture over a scaphoid osteophyte).
* Treatment: Volar tenosynovectomy, release of the A1 pulley (with caution in RA, as A1 release can exacerbate ulnar drift; often, resection of the ulnar slip of the FDS is preferred), and tendon grafting or transfer for ruptures.
DEFORMITIES OF THE THUMB
Thumb involvement severely compromises hand function. Deformities are classified based on the joint where the primary pathology initiates (Nalebuff Classification).
Classification of Rheumatoid Thumb Deformities
- Type I (Boutonnière): The most common type. Initiated by MCP joint synovitis. The EPB attenuates, leading to MCP flexion and secondary IP joint hyperextension.
- Type II: Similar to Type I, but accompanied by trapeziometacarpal (CMC) joint arthritis and subluxation.
- Type III (Swan-Neck): Initiated by CMC joint disease. Dorsal subluxation of the CMC joint leads to adduction contracture of the first metacarpal, secondary MCP joint hyperextension, and IP joint flexion.
- Type IV (Gamekeeper's): Initiated by MCP joint synovitis leading to attenuation of the ulnar collateral ligament, resulting in radial deviation of the proximal phalanx.
Correction of Arthritic Thumb Deformities
Surgical intervention is dictated by the specific type of deformity and the degree of joint destruction.
* Synovectomy and Extensor Reconstruction: For early Type I deformities, MCP synovectomy and rerouting of the EPB can restore balance.
* Arthrodesis of Thumb Joints:
* MCP Joint Arthrodesis: Highly effective for advanced Type I and Type IV deformities. Fusing the MCP joint at 10° to 15° of flexion provides a stable, pain-free post for pinch while preserving CMC and IP motion.
* IP Joint Arthrodesis: Indicated for severe instability or fixed flexion contractures, fused at 0° to 15° of flexion.
* Trapeziometacarpal Arthroplasty: Indicated for severe OA or RA of the CMC joint (Type III deformities).
* Technique (Ligament Reconstruction Tendon Interposition - LRTI): A Wagner or dorsal incision is utilized. The superficial branches of the radial nerve are meticulously protected. The trapezium is excised piecemeal or en bloc. The Flexor Carpi Radialis (FCR) tendon is harvested, passed through a drill hole in the base of the first metacarpal to reconstruct the anterior oblique ligament, and the remainder of the tendon is rolled into an anchovy and interposed into the trapezial space.
RHEUMATOID DEFORMITIES OF THE WRIST
The wrist is the keystone of hand function. Rheumatoid disease frequently targets the radiocarpal and distal radioulnar joints (DRUJ).
Synovitis of the Wrist
Early radiocarpal synovitis stretches the radiocarpal ligaments, leading to ulnar translocation of the carpus and supination of the carpus on the forearm.
* Treatment: Early synovectomy and radiocarpal stabilization can prevent irreversible carpal collapse.
Wrist Arthrodesis and Arthroplasty
- Total Wrist Arthrodesis: The gold standard for the severely destroyed, painful, and unstable rheumatoid wrist. It provides reliable pain relief and a stable platform for finger function. The wrist is typically fused in neutral to slight extension (10°-15°) using a dorsal locking plate.
- Total Wrist Arthroplasty (TWA): An alternative for low-demand patients with bilateral wrist involvement who require preserved motion for personal hygiene and ADLs. Modern third-generation implants have improved survivorship, but TWA remains contraindicated in patients with heavy labor demands, severe bone loss, or absent wrist extensors.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The success of arthritic hand surgery is inextricably linked to specialized postoperative hand therapy.
* Immobilization: Following MCP arthroplasty, the hand is immobilized in a bulky compressive dressing with a volar plaster splint holding the wrist in neutral, MCP joints in full extension, and PIP joints free.
* Dynamic Splinting: At 3 to 5 days postoperatively, a dynamic extension splint with outriggers is applied to maintain MCP extension and radial alignment while allowing active flexion.
* Therapy Progression: Active and active-assisted range of motion exercises are initiated early to prevent adhesion formation. Night splinting in extension is maintained for a minimum of 12 weeks to prevent recurrent flexion contractures and ulnar drift.
Clinical Pearl: The rehabilitation protocol must be tailored to the individual's tissue quality. In rheumatoid patients with profound soft-tissue attenuation, slower progression and prolonged splinting may be necessary to prevent the recurrence of deformity.
By adhering to strict biomechanical principles, staging procedures logically, and executing meticulous surgical techniques, the orthopaedic surgeon can profoundly improve the quality of life for patients suffering from the debilitating effects of the arthritic hand.
You Might Also Like