Precision Volar Approach to Carpal Tunnel & Wrist: Comprehensive Surgical Guide
Key Takeaway
The precision volar approach is a fundamental surgical technique in orthopedic hand and wrist surgery. It provides crucial access for a broad range of pathologies, including carpal tunnel syndrome, distal radius fractures, and flexor tenosynovitis. This detailed approach emphasizes intricate surgical anatomy, precise visualization of structures like the median nerve, and stable fixation, essential for managing complex upper extremity conditions.
Precision Volar Approach for Carpal Tunnel and Wrist Treatment
Introduction & Epidemiology
The volar approach to the carpal tunnel and wrist represents a fundamental and versatile surgical corridor in orthopedic hand and wrist surgery. This anatomical access point is critical for addressing a broad spectrum of pathologies, ranging from the highly prevalent compressive neuropathy of the median nerve to complex intra-articular fractures and carpal dislocations. Carpal tunnel syndrome (CTS) affects approximately 3-6% of the adult population, making median nerve decompression one of the most frequently performed surgical procedures in the upper extremity. Beyond CTS, the increasing incidence of distal radius fractures, often requiring open reduction and internal fixation (ORIF), further underscores the significance of a well-mastered volar approach. The anatomical complexity of the wrist and hand, coupled with the critical neurovascular structures coursing through the carpal tunnel and its vicinity, necessitates a precise, anatomically informed, and often directly visualized surgical technique. While minimally invasive techniques have gained traction for isolated carpal tunnel release, the comprehensive volar approach remains indispensable for conditions demanding broader exposure, direct visualization of pathology, or robust internal fixation. This detailed guide aims to elucidate the intricate surgical anatomy, indications, step-by-step technique, potential complications, and post-operative management associated with this essential surgical pathway.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy is paramount for safe and effective surgery via the volar approach. The carpal tunnel is an osteofibrous canal defined volarly by the transverse carpal ligament (flexor retinaculum) and dorsally and radially by the carpal bones (scaphoid, trapezium) and ulnarly by the hamate and pisiform.
Within this confined space, the median nerve, nine flexor tendons (flexor digitorum superficialis, flexor digitorum profundus, and flexor pollicis longus), and their respective synovial sheaths traverse into the hand.
Median Nerve
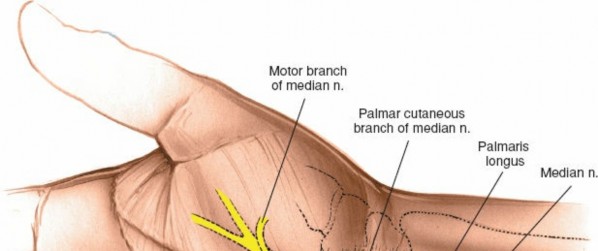
The median nerve is the primary structure of concern in carpal tunnel pathology. It typically enters the carpal tunnel superficial to the flexor digitorum superficialis tendons and deep to the transverse carpal ligament. Crucially, its branches require careful identification and protection.
*
Palmar Cutaneous Branch:
This purely sensory branch typically arises from the radial side of the median nerve in the distal forearm, approximately 5-7 cm proximal to the wrist crease. It then travels superficial to the transverse carpal ligament, supplying sensation to the thenar eminence. Its variable course makes it vulnerable to iatrogenic injury during skin incision and subcutaneous dissection.
*
Recurrent Motor Branch (Thenar Motor Branch):
This branch supplies the thenar musculature (abductor pollicis brevis, opponens pollicis, superficial head of flexor pollicis brevis). Its origin point from the median nerve distal to the transverse carpal ligament is highly variable:
*
Extraligamentous (50%):
Arises distal to the distal edge of the transverse carpal ligament.
*
Subligamentous (30%):
Pierces the transverse carpal ligament.
*
Transligamentous (20%):
Arises within the confines of the ligament, passing through it.
* This variability dictates the need for direct visualization during transverse carpal ligament division to prevent transection.
Flexor Tendons and Synovial Sheaths
The nine flexor tendons are arranged in a specific manner:
*
Superficial Layer:
Flexor digitorum superficialis tendons (FDS) to digits 2-5, with FDS III and IV being more superficial than FDS II and V.
*
Intermediate Layer:
Flexor digitorum profundus tendons (FDP) to digits 2-5, and flexor pollicis longus (FPL).
* All are encased within a common synovial sheath, which can become inflamed (tenosynovitis) contributing to CTS or requiring synovectomy.
Vascular Structures
The superficial palmar arch, an anastomosis primarily between the ulnar artery and the superficial palmar branch of the radial artery, lies distal and superficial to the carpal tunnel. Proximally, the radial artery lies radial to the flexor carpi radialis (FCR) tendon, and the ulnar artery lies ulnar to the flexor carpi ulnaris (FCU) tendon and ulnar nerve. Care must be taken to avoid injury to these vessels during deeper dissection, particularly when extending proximally for fracture fixation.
Bony Anatomy
For wrist fracture management, the volar aspect of the distal radius is critical. The volar aspect presents distinct anatomical zones, including the watershed line, the pronator quadratus fossa, and the region of the lunate facet. The normal volar tilt of the distal radius and its articulation with the scaphoid and lunate are biomechanically essential for wrist function. Volar lip fractures (Barton's fractures) directly involve the articular surface and necessitate precise anatomical reduction and stable fixation via this approach. Trans-scaphoid perilunate dislocations also frequently require volar exposure for reduction and ligamentous repair or fixation.
Indications & Contraindications
The precision volar approach is indicated for a wide array of conditions affecting the median nerve, flexor tendons, and osseous structures of the distal forearm and carpus.
Indications for Volar Approach:
-
Decompression of the Median Nerve:
- Idiopathic Carpal Tunnel Syndrome (CTS) refractory to non-operative treatment.
- Secondary CTS due to space-occupying lesions (e.g., ganglion, lipoma, tenosynovitis).
- Recurrent CTS requiring revision surgery.
-
Synovectomy of the Flexor Tendons:
- Chronic inflammatory tenosynovitis (e.g., rheumatoid arthritis, non-specific tenosynovitis).
- Infectious tenosynovitis requiring debridement and drainage.
-
Excision of Tumors within the Carpal Tunnel or Wrist:
- Ganglion cysts, lipomas, giant cell tumors of the tendon sheath, neurofibromas.
-
Repair of Lacerations or Ruptures:
- Acute median nerve lacerations.
- Flexor tendon lacerations (FDS, FDP, FPL).
- Acute median nerve or flexor tendon ruptures.
-
Drainage of Sepsis:
- Deep-space infections tracking from the midpalmar space or forearm.
- Septic tenosynovitis.
-
Open Reduction and Internal Fixation (ORIF) of Fractures and Dislocations:
-
Distal Radius Fractures:
- Unstable volar Barton's fractures (volar lip fractures).
- Displaced intra-articular distal radius fractures with volar comminution or displacement, especially those involving the lunate facet.
- High-energy comminuted fractures with significant volar metadiaphyseal comminution requiring robust plate fixation.
- Carpal Fractures: Select scaphoid or lunate fractures (rarely primary indication, often for associated pathology).
-
Carpal Dislocations:
- Volar perilunate or trans-scaphoid perilunate dislocations.
- Complex carpal instabilities requiring ligamentous repair or reconstruction.
-
Distal Radius Fractures:
Contraindications:
-
Absolute Contraindications:
- Active local infection at the surgical site (relative, unless for drainage).
- Unstable medical comorbidities precluding safe anesthesia and surgery.
- Patient refusal.
-
Relative Contraindications:
- Severe overlying scar tissue from previous surgery, necessitating alternative approaches or increased caution.
- Severe peripheral vascular disease compromising wound healing.
- Unrealistic patient expectations regarding outcomes.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Carpal Tunnel Syndrome | Symptoms refractory to conservative care (duration >3-6 months, severe symptoms, motor weakness, thenar atrophy, objective electrodiagnostic severity). | Mild to moderate symptoms, short duration, nocturnal symptoms only. Splinting, NSAIDs, steroid injection. |
| Flexor Tenosynovitis | Chronic, persistent, painful swelling, trigger finger refractory to conservative care; infectious tenosynovitis. | Early stages, steroid injection, splinting, NSAIDs. |
| Tumors of Carpal Tunnel | Symptomatic (pain, nerve compression), rapidly growing, definitive diagnosis uncertain, large size. | Small, asymptomatic, benign lesions confirmed by imaging (e.g., small ganglion). |
| Nerve/Tendon Lacerations | All complete or functionally significant partial lacerations. | Partial tendon lacerations (<50%) in specific zones with preserved function. |
| Sepsis | Drainage of deep-space infections, septic tenosynovitis. | Cellulitis without abscess or deep collection; systemic antibiotics. |
| Distal Radius Fractures | Unstable, displaced intra-articular fractures (e.g., volar Barton's, comminuted articular fractures), significant volar tilt or shortening, open fractures, polytrauma patients requiring early mobilization. | Stable, non-displaced or minimally displaced extra-articular fractures, stable intra-articular fractures managed with casting/splinting. |
| Carpal Dislocations | Acute, irreducible, or unstable perilunate/trans-scaphoid perilunate dislocations. | Isolated stable carpal instabilities (rare). |
Pre-Operative Planning & Patient Positioning
Pre-Operative Planning
Comprehensive pre-operative planning is essential for optimizing outcomes and mitigating risks.
*
Clinical Evaluation:
Thorough history and physical examination, including neurovascular assessment and documentation of pre-existing deficits. For CTS, electrodiagnostic studies (nerve conduction velocity, electromyography) are standard.
*
Imaging Studies:
*
Radiographs:
Anteroposterior, lateral, and oblique views of the wrist are standard for fracture assessment. Stress views or specific carpal views may be necessary.
*
Computed Tomography (CT):
Indicated for complex intra-articular distal radius fractures, comminuted fractures, suspected carpal fractures, or occult carpal pathology. Essential for precise fracture mapping, articular surface assessment, and surgical planning.
*
Magnetic Resonance Imaging (MRI):
Useful for evaluating soft tissue masses, tenosynovitis, ligamentous injuries, occult fractures, or nerve pathology.
*
Surgical Templating:
For fracture fixation, selecting the appropriate volar locking plate size and configuration, and pre-operative templating based on contralateral wrist anatomy or standard measurements, can enhance efficiency.
*
Patient Education:
Discuss the nature of the condition, the planned surgical procedure, potential risks, expected recovery course, and post-operative restrictions. Obtain informed consent.
*
Anesthesia:
Local, regional (e.g., axillary block), or general anesthesia may be employed. Regional anesthesia offers excellent post-operative analgesia.
*
Tourniquet:
A pneumatic tourniquet is routinely used on the upper arm for a bloodless field, typically inflated to 250 mmHg for normotensive patients.
Patient Positioning
The standard patient position for a volar wrist approach is supine on the operating table.
- Arm Positioning: The ipsilateral arm is abducted and placed on a specialized hand table, allowing the elbow to be flexed to 90 degrees.
- Forearm Supination: The forearm is maximally supinated so that the palm faces directly upward. This position provides optimal exposure of the volar aspect of the wrist and hand.
-
Exsanguination:
An exsanguinating bandage (e.g., an Esmarch bandage) is applied from the fingertips to the proximal forearm to empty the limb of venous blood.
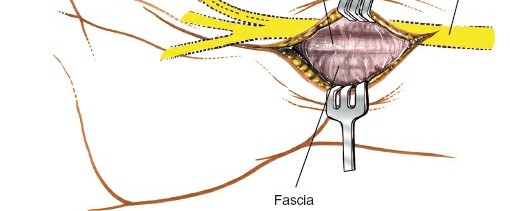
Figure 1: Patient positioned supine on the operating table with the arm abducted and forearm supinated on a hand table.
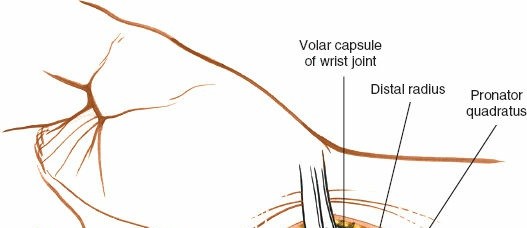
Figure 2: Application of an exsanguinating bandage and pneumatic tourniquet to the upper arm.

Figure 3: Close-up view of the forearm resting on the hand table, ensuring maximal supination and stable positioning. - Tourniquet Inflation: The pneumatic tourniquet is then inflated to the desired pressure (e.g., 250 mmHg for a normotensive adult) to maintain a bloodless surgical field.
-
Preparation and Draping:
The arm, hand, and wrist are meticulously prepped with an antiseptic solution and sterilely draped, ensuring a wide operative field for potential extension proximally or distally if necessary.

Figure 4: The limb is prepped and draped, exposing the volar aspect of the wrist and hand for surgical access.
Detailed Surgical Approach / Technique
Landmarks and Incision
Accurate incision planning is crucial for both effective exposure and minimizing complications.
*
Key Landmarks:
* Proximal wrist crease.
* Distal edge of the thenar eminence.
* Longitudinal axis of the ring finger or between the ring and long fingers.
* Flexor carpi ulnaris (FCU) and Flexor carpi radialis (FCR) tendons (if exposure extends proximally).
*
Incision Options:
*
Standard Carpal Tunnel Incision:
A curvilinear incision along the ulnar border of the thenar crease, extending proximally across the wrist crease into the distal forearm. It typically begins 1-2 cm distal to the wrist crease, directly in line with the radial border of the ring finger or the third web space, and extends proximally for 2-3 cm past the wrist crease. This avoids crossing the wrist crease at a right angle, reducing scar contracture.
*
Extended Volar Incision (for fracture fixation or extensive pathology):
A longer, straight or slightly curvilinear incision centered over the FCR tendon, extending from the distal palmar crease proximally along the forearm for 5-10 cm or more, depending on the required exposure of the distal radius. This incision provides excellent visualization of the distal radius and carpus.
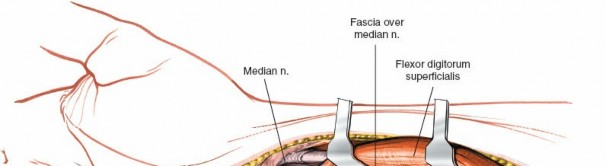
Figure 5: Marking of a standard curvilinear incision for carpal tunnel release, beginning distal to the wrist crease and extending proximally.
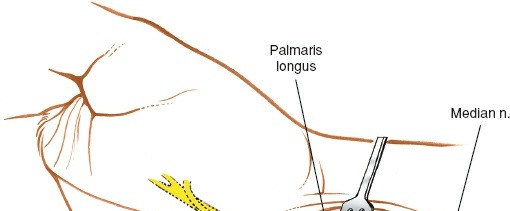
Figure 6: A more detailed view of the curvilinear incision in the palm, respecting the thenar eminence and skin creases.
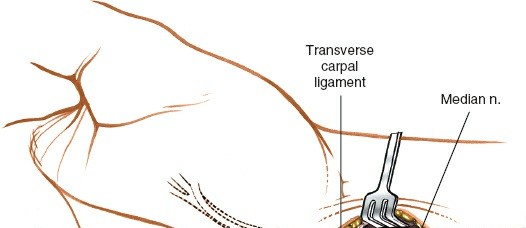
Figure 7: A longer, straight volar incision extending into the forearm, often used for distal radius fracture fixation or extensive wrist pathology.
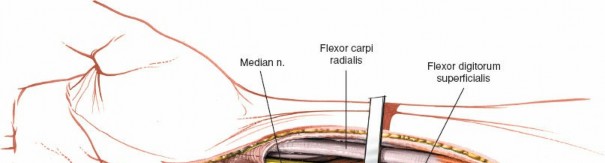
Dissection (Layer by Layer)
-
Skin and Subcutaneous Tissue:
- Incise the skin with a No. 15 blade.
- Carefully dissect through the subcutaneous fat using a scalpel or electrocautery. Identify and protect any superficial veins and sensory nerves, most critically the palmar cutaneous branch of the median nerve. This branch often lies radial to the incision in the distal forearm. Retract it gently.
- In the palm, identify and protect the superficial palmar arch and its branches, which lie distal to the carpal tunnel.
-
Palmar Aponeurosis and Transverse Carpal Ligament:
- The palmar aponeurosis is visualized superficial to the transverse carpal ligament in the palm. It may need to be incised.
- The underlying transverse carpal ligament (flexor retinaculum) appears as a glistening, whitish, fibrous band. Its proximal border is typically at the wrist crease, and it extends distally for 2-3 cm.
-
A critical step is identifying its ulnar border. The median nerve lies just radial to the FPL tendon and superficial to the FDS tendons. The motor branch may arise from any aspect of the median nerve or penetrate the ligament itself.
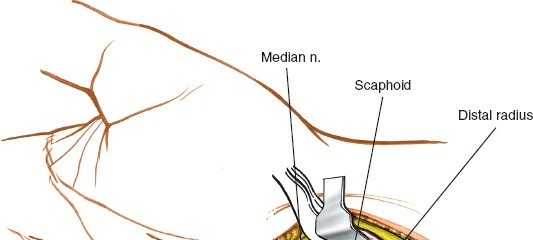
Figure 8: Deep dissection showing exposure of the transverse carpal ligament (flexor retinaculum), a thick fibrous band.
-
Transverse Carpal Ligament Release (Carpal Tunnel Specific):
- Elevate the distal aspect of the transverse carpal ligament with a curved hemostat or small blunt hook.
- Under direct visualization, carefully divide the ligament from distal to proximal using a scalpel, blunt-tipped scissors, or a dedicated carpal tunnel knife. Ensure the median nerve and its motor branch are directly visualized and protected throughout.
- Continue the release proximally into the distal forearm fascia as needed.
-
Inspect the median nerve for any constricting bands or masses.
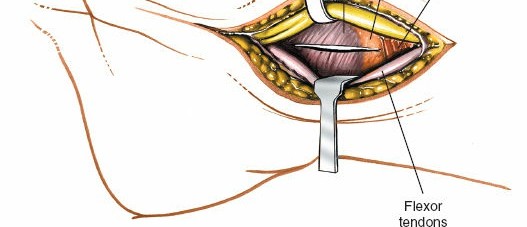
Figure 9: The transverse carpal ligament is being divided under direct visualization, carefully protecting the underlying median nerve and flexor tendons.
Figure 10: Post-release, the median nerve is fully decompressed and visible within the carpal tunnel, appearing less constricted.
Specific Procedures
Carpal Tunnel Release
- Once the transverse carpal ligament is completely divided, confirm full decompression of the median nerve.
- Inspect the nerve for any gross abnormalities. Perform an epineurotomy only if significant internal hourglass constriction is observed.
- Explore the carpal tunnel for other pathologies (e.g., tenosynovitis, tumors) and address them as indicated.
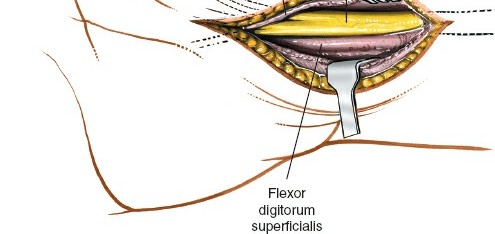
Flexor Tenosynovectomy
- Following carpal tunnel release, retract the median nerve gently.
- Identify the involved flexor tendons and their inflamed synovial sheaths.
- Using fine instruments, meticulously debride the hypertrophic synovium from around the tendons, preserving the smooth gliding surfaces of the tendons.
- Ensure complete removal of diseased tissue while avoiding tendon injury.
Tumor Excision
- Carefully expose the tumor, preserving surrounding neurovascular structures.
- Excision is typically performed en bloc. For nerve sheath tumors, consider intraoperative neurophysiological monitoring.
- Send specimens for histopathological analysis.
Open Reduction and Internal Fixation (ORIF) of Distal Radius Fractures
This requires a broader exposure and more extensive dissection.
1.
Proximal Extension:
Extend the incision proximally along the forearm, usually between the FCR tendon (radial) and the radial artery (more radial). The interval between the FCR and the radial artery offers direct access to the volar surface of the distal radius. Alternatively, an incision ulnar to the FCR can be used, reflecting the FCR radially.
2.
Pronator Quadratus Dissection:
* Identify the pronator quadratus muscle, which covers the volar surface of the distal radius.
* The muscle can be sharply elevated from its radial insertion and reflected ulnarly, exposing the bare bone of the distal radius. This allows preservation of the muscle. Alternatively, a longitudinal incision can be made through the pronator quadratus if necessary for exposure.

Figure 11: Deeper dissection exposing the volar aspect of the distal radius, with the pronator quadratus muscle reflected or incised to reveal the fracture site.
3.
Fracture Reduction:
* Utilize ligamentotaxis with gentle longitudinal traction on the fingers, potentially combined with manual manipulation.
* Direct reduction with elevators, bone hooks, or small clamps to restore articular congruity and overall alignment.
* Fluoroscopic guidance is essential to confirm reduction in multiple planes (AP, lateral, oblique views).
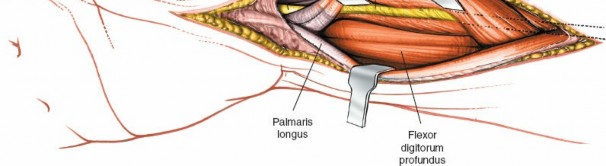
Figure 12: Intraoperative image demonstrating reduction maneuvers, including traction and direct manipulation, to restore anatomical alignment of the fractured distal radius.
4.
Plate Application:
* Select an anatomically contoured volar locking plate (e.g., LCP Distal Radius Plate). Position the plate on the volar surface of the distal radius, ensuring its distal edge is proximal to the watershed line to avoid flexor tendon impingement.
* Confirm proper plate position with fluoroscopy.
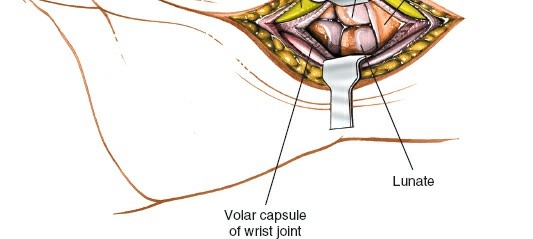
Figure 13: Application of a volar locking plate to the reduced distal radius, ensuring proper positioning relative to the watershed line and articular surface.
5.
Screw Insertion:
* Insert proximal bicortical locking or non-locking screws through the plate into the radial shaft, providing stable diaphyseal fixation.
* Insert distal unicortical locking screws into the radial head, aiming for subchondral bone support. Ensure screws do not penetrate the articular surface. Use fluoroscopy to confirm screw length and absence of intra-articular violation.
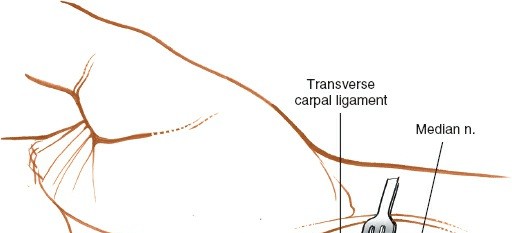
Figure 14: Insertion of proximal screws into the radial shaft, providing secure fixation of the plate to the diaphyseal bone.
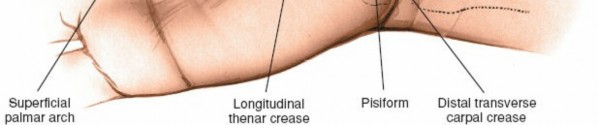
Figure 15: Insertion of distal locking screws into the radial head, carefully avoiding intra-articular penetration. Fluoroscopy is typically used to confirm placement.

Figure 16: Final construct with the volar locking plate securely fixed by both proximal and distal screws, demonstrating stable internal fixation.
Closure
- Hemostasis: Ensure meticulous hemostasis using electrocautery and direct pressure.
- Pronator Quadratus: If elevated, the pronator quadratus muscle can be reapproximated over the plate and screws to provide a soft tissue buffer and minimize tendon irritation.
- Deep Fascia: Close the deep fascia loosely.
- Subcutaneous Tissue: Close the subcutaneous tissue with absorbable sutures to minimize dead space.
-
Skin Closure:
Close the skin with non-absorbable sutures or staples.
Figure 17: Thorough irrigation of the wound to remove debris and reduce the risk of infection.
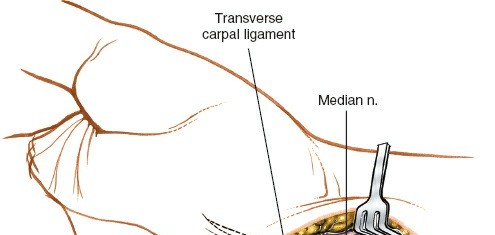
Figure 18: Layered closure of the deep tissues, including the pronator quadratus and subcutaneous layers.
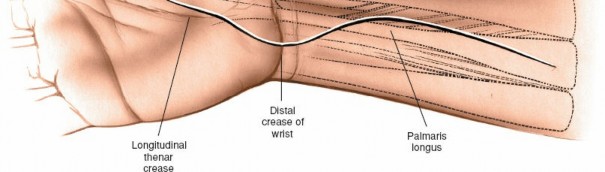
Figure 19: Meticulous skin closure using sutures or staples to achieve good wound apposition. -
Dressing and Splinting:
Apply a sterile dressing. For carpal tunnel release, a soft bulky dressing is typically sufficient. For fracture fixation, a volar splint or cast may be applied to provide initial protection and immobilization.

Figure 20: Application of a sterile dressing to the closed incision.
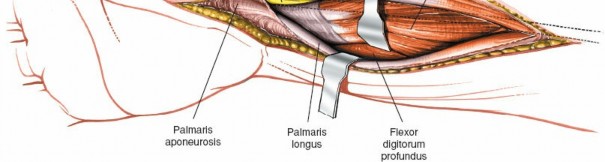
Figure 21: A post-operative volar splint or cast applied for protection and immobilization, especially after fracture fixation.
Complications & Management
While the volar approach is generally safe and effective, surgeons must be cognizant of potential complications.
Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Median Nerve Injury | <0.5% (CTS release) | Immediate re-exploration for transection or severe crush. Neurolysis for entrapment. Nerve repair or grafting for complete transection. Close observation for neuropraxia. |
| Palmar Cutaneous Nerve Injury | 5-10% (dysesthesia) | Local steroid injections for mild dysesthesia. Neuroma excision or neurolysis if persistent, severe, and localized. Rarely, nerve repair. |
| Recurrent Motor Branch Injury | <0.1-0.5% | Re-exploration, nerve repair (microsurgical), or tendon transfer (e.g., opponensplasty) for persistent deficits. |
| Pillar Pain (Post-CTR) | 25-50% | Non-steroidal anti-inflammatory drugs (NSAIDs), physical therapy, corticosteroid injections. Typically self-limiting (resolves within 6-12 months). |
| Incomplete Carpal Tunnel Release | 1-5% | Revision carpal tunnel release, ensuring complete division of the transverse carpal ligament and potentially forearm fascia. |
| Infection | 1-3% | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, intravenous antibiotics, hardware removal (if applicable and fracture healed). |
| Hematoma Formation | 1-5% | Compression dressing, elevation. Evacuation for large, expanding, or symptomatic hematomas, especially if causing nerve compression. |
| Flexor Tendon Adhesions/Rupture | <1% | Early mobilization, tenolysis for adhesions. Tendon repair or reconstruction for rupture, often involving graft or transfer. Risk is higher with prominent hardware. |
| Vascular Injury | Rare | Direct repair of lacerated vessels (e.g., radial artery). Ligation of smaller branches if collateral flow is adequate. |
| Complex Regional Pain Syndrome (CRPS) | 2-5% | Multimodal pain management (NSAIDs, neuromodulators, regional blocks), aggressive physical and occupational therapy, psychological support. Early diagnosis and intervention are critical. |
| Malunion/Nonunion (Fracture Fixation) | Variable | Malunion: Corrective osteotomy. Nonunion: Revision surgery with bone grafting, revision fixation, or alternative fixation methods. |
| Hardware Irritation/Failure | 5-10% (prominence) | Hardware removal after fracture healing or if symptomatic. Revision fixation for failure. |
| Loss of Reduction (Fracture Fixation) | 1-2% | Revision ORIF with more stable construct, external fixation, or conversion to arthroplasty in rare severe cases. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is integral to achieving optimal functional outcomes, tailored to the specific procedure performed.
General Principles
- Pain and Edema Control: Elevation, cryotherapy, and appropriate analgesia are initiated immediately post-operatively.
- Wound Care: Daily dressing changes as directed, monitoring for signs of infection. Sutures or staples are typically removed at 10-14 days.
Carpal Tunnel Release (Isolated)
-
Immediate (Day 0-7):
- Bulky soft dressing, gentle active range of motion (AROM) of fingers and thumb.
- Avoid heavy gripping or lifting.
-
Early (Week 1-3):
- Initiate gentle wrist AROM as pain allows.
- Scar massage once the wound is healed to minimize hypersensitivity and adhesion.
- Neuromobilization exercises for the median nerve.
- Gradual return to light daily activities.
-
Intermediate (Week 3-6):
- Progressive strengthening exercises for grip and pinch.
- Increased activity tolerance, gradual return to pre-injury activities.
-
Late (Beyond Week 6):
- Full return to activities as tolerated. Continued scar management.
Distal Radius Fracture ORIF (Volar Plating)
Rehabilitation protocols are dependent on fracture stability, fixation achieved, and surgeon preference.
*
Immediate (Day 0-14):
* Immobilization in a sugar tong splint or volar splint in a neutral position (or slight dorsiflexion) for comfort and protection.
* Strict elevation.
* AAROM/AROM of digits, thumb, elbow, and shoulder to prevent stiffness.
*
Early (Week 2-6):
*
Initiate guarded wrist motion:
Once radiographic stability is confirmed and soft tissue healing allows, begin gentle AROM of the wrist (flexion, extension, pronation, supination).
* A removable custom splint may be used for protection during activities.
* Light functional tasks.
*
Intermediate (Week 6-12):
*
Progressive strengthening:
Gradual introduction of resistance exercises for grip, pinch, and wrist movements.
* Increased loading and functional activities.
* Close monitoring for signs of tendon irritation from hardware.
*
Late (Beyond Week 12):
* Advanced strengthening and conditioning.
* Return to sport or heavy labor, typically 3-6 months post-op, with full clearance based on radiographic healing and functional recovery. Hardware removal considered if symptomatic after complete healing.
Flexor Tenosynovectomy / Nerve or Tendon Repair
- Often requires specific controlled active or passive motion protocols (e.g., Duran or Kleinert protocols for flexor tendon repair) to prevent adhesions while allowing healing. Immobilization is typically shorter than for fractures, focusing on early protected motion.
Summary of Key Literature / Guidelines
The literature strongly supports the efficacy and safety of the precision volar approach for various wrist and hand pathologies.
-
Carpal Tunnel Syndrome:
- The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines for Carpal Tunnel Syndrome (updated 2016) strongly recommend surgical carpal tunnel release for patients with moderate to severe CTS or those who fail non-operative treatment. Evidence supports similar long-term outcomes for open and endoscopic techniques, though open release may have lower recurrence rates in some series and is generally favored for revision cases or when additional pathology (e.g., mass) is suspected. The open volar approach, allowing direct visualization, minimizes the risk of median nerve or recurrent motor branch injury compared to endoscopic methods, particularly given the anatomical variations described by Lanz.
- Studies by Seiler and colleagues have further delineated the anatomical variations of the motor branch and emphasized the importance of adequate visualization.
-
Distal Radius Fractures:
- Volar locking plate fixation for unstable distal radius fractures has become the gold standard, demonstrating superior radiographic and functional outcomes compared to traditional casting or external fixation, especially for displaced intra-articular fractures. The volar approach allows direct visualization and restoration of articular congruity and volar tilt, which are crucial for wrist biomechanics and long-term function.
- Key literature by Orbay and Touliatos, along with numerous randomized controlled trials, highlights the benefits of volar locking plates in allowing earlier mobilization and reducing complications like malunion compared to non-operative treatment or K-wire fixation in unstable fractures.
- Concerns regarding flexor tendon irritation or rupture with prominent volar plates emphasize the need for meticulous plate positioning and soft tissue coverage, often achieved by repairing or approximating the pronator quadratus.
-
General Principles:
- Across all indications, the literature consistently emphasizes the critical role of a profound anatomical understanding, meticulous surgical technique, and individualized post-operative rehabilitation. Outcomes research, utilizing patient-reported outcome measures like the Disabilities of the Arm, Shoulder, and Hand (DASH) score, Michigan Hand Outcomes Questionnaire (MHQ), and SF-36, consistently demonstrates significant functional improvement and pain relief following appropriately indicated and executed volar wrist surgery.
- The evolution of instrumentation, particularly smaller-profile plates and specialized retractors, has further refined the precision and reduced the invasiveness of the volar approach, while maintaining its core principles of direct visualization and anatomical reconstruction.
Clinical & Radiographic Imaging
You Might Also Like