Solving Severe Acetabular Bone Loss with Cup-Cage Reconstruction

Key Takeaway
Discover the latest medical recommendations for Solving Severe Acetabular Bone Loss with Cup-Cage Reconstruction. Acetabular bone loss, often due to aseptic loosening of hip implants, manifests as acute groin pain and inability to weight bear. Radiological assessment typically reveals severe osteolysis of the ilium and ischium. Diagnosis centers on the extent of acetabular bone loss. Treatment, such as cup-cage reconstruction, aims to address significant defects and restore stability in complex revision total hip arthroplasty cases.
Solving Severe Acetabular Bone Loss with Cup-Cage Reconstruction
Introduction & Epidemiology
Severe acetabular bone loss represents one of the most formidable challenges in revision total hip arthroplasty (THA). This complex clinical scenario is often encountered in cases of failed previous reconstructions, periprosthetic joint infection (PJI), extensive osteolysis, tumor resections, or significant trauma. The etiology is multifactorial, frequently stemming from aseptic loosening, septic loosening, component migration, or osteolysis secondary to polyethylene wear.
The classification of acetabular bone loss is critical for surgical planning. The Paprosky classification is widely adopted, categorizing defects based on the integrity of the host bone:
*
Type 1:
Minimal loss, intact rim and columns.
*
Type 2A:
Mild superior migration, intact columns, deficient superior dome.
*
Type 2B:
Moderate superior migration, intact columns, deficient superior dome and medial wall.
*
Type 2C:
Medial migration with intact columns.
*
Type 3A:
Severe superior migration, compromise of ischial tuberosity and posterior column, often with cavitary and segmental defects.
*
Type 3B:
Extensive superior and medial migration, complete loss of the posterior column and superior dome, often with pelvic discontinuity.
The American Academy of Orthopaedic Surgeons (AAOS) classification also delineates defects based on morphology (cavitary, segmental, combined, protrusio, pelvic discontinuity). Severe bone loss, particularly Paprosky Type 3A and 3B defects, frequently necessitates reconstruction techniques that go beyond conventional cementless hemispheric components with augments.
The cup-cage construct, utilizing a cemented polyethylene liner within a metal cage, or a modular cup designed to articulate within a cage, has emerged as a robust solution for these challenging cases. This reconstructive strategy aims to achieve immediate mechanical stability, bridge critical bone defects, and provide a stable environment for potential host bone ingrowth or graft incorporation, thereby restoring hip biomechanics and function. The increasing prevalence of revision THA in an aging population underscores the importance of mastering these complex reconstructive techniques.
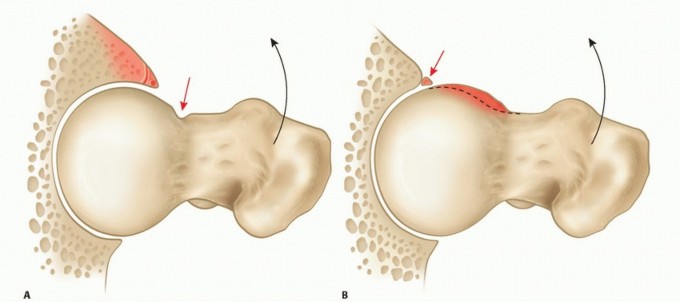
Surgical Anatomy & Biomechanics
A thorough understanding of pelvic anatomy and biomechanics is paramount for successful acetabular reconstruction. The acetabulum is formed by the fusion of the ilium, ischium, and pubis, creating a hemispheric socket. Key anatomical landmarks include:
*
Columns:
The anterior column extends from the anterior superior iliac spine through the anterior acetabulum to the pubic symphysis. The posterior column runs from the posterior ilium through the sciatic notch and posterior acetabulum to the ischial tuberosity.
*
Teardrop:
A radiographic landmark formed by the anterior aspect of the ischial body and the medial acetabular wall.
*
Kohler's line:
The radiographic medial border of the pelvic inlet, medial to which a true protrusio occurs.
*
Ilioischial line:
The radiographic medial border of the posterior column.
*
Quadrilateral surface:
The thin bony plate located between the anterior and posterior columns.
*
Ischial tuberosity:
A critical posterior-inferior fixation point for cages.
*
Sacroiliac joint:
The superior weight-bearing articulation of the pelvis.
The pelvis functions as a complex ring structure, transferring axial loads from the spine to the lower extremities. The acetabulum typically supports approximately 4-6 times body weight during single-limb stance. In severe bone loss, particularly with pelvic discontinuity, this load transfer mechanism is compromised, leading to instability and potential migration of components.
The cup-cage construct addresses these biomechanical challenges by:
*
Load Sharing:
The cage provides a stable structural framework, effectively transferring load from the acetabular component to viable host bone, circumventing areas of deficiency.
*
Bridging Defects:
Cages can span large segmental or cavitary defects, providing a scaffold for bone graft material and promoting biological reconstruction.
*
Restoration of Hip Center:
Accurate placement of the cage allows for the restoration of the anatomic or slightly medialized hip center, optimizing hip mechanics, reducing joint reaction forces, and minimizing impingement risk.
*
Pelvic Discontinuity:
Cages can effectively bridge an ununited fracture or osteotomy of the acetabulum, providing immediate stability and allowing for eventual bony union. The cage is fixed to both the superior and inferior segments of the hemipelvis, providing a rigid construct.
The design of anti-protrusio cages (e.g., Burch-Schneider, custom triflange) is specifically engineered to resist medial migration and provide circumferential support, allowing for reconstruction even in cases with extensive medial wall deficiencies. The principles of stable fixation to at least two columns or regions of intact bone (ilium, ischium, pubis) are paramount for long-term success.
Indications & Contraindications
The decision to proceed with cup-cage reconstruction for severe acetabular bone loss is based on a comprehensive assessment of the extent of bone deficiency, patient comorbidities, and functional demands.
Indications for Cup-Cage Reconstruction:
- Paprosky Type 3A and 3B Defects: Especially those with significant superior, medial, or posterior column compromise, and substantial cavitary or segmental bone loss that cannot be addressed by conventional cementless cups with augments.
- Pelvic Discontinuity: Defined as a complete loss of continuity between the superior and inferior acetabular segments, often requiring a cage to bridge the defect and provide stability.
- Failed Prior Reconstructions: Cases where previous attempts with standard components, augments, or allografts have failed due to migration, aseptic loosening, or nonunion.
- Oncological Resections: Following wide resection of periacetabular tumors, where significant bone stock is removed, a cage can reconstruct the defect and provide anchorage for an endoprosthesis.
- Chronic Periprosthetic Joint Infection (PJI): After thorough debridement and management of infection, in a staged revision, a cup-cage construct can provide a durable reconstruction.
- Acetabular Protrusio: Severe medial migration where the femoral head articulates within or through the medial acetabular wall, requiring reconstruction of the medial wall.
- Severe Acetabular Dysplasia: In primary THA settings with extreme dysplasia and large segmental bone deficiencies, although less common than revision settings.
Contraindications for Cup-Cage Reconstruction:
- Active, Uncontrolled Systemic Infection: While cup-cages can be used in staged PJI, ongoing systemic sepsis or local active infection is an absolute contraindication for definitive implantation.
- Insufficient Host Bone for Cage Fixation: If there is inadequate quality or quantity of host bone in the ilium, ischium, or pubis to achieve stable screw fixation of the cage, alternative strategies such as custom triflange components may be required.
- Prohibitive Medical Comorbidities: Patients with severe, uncorrectable medical conditions that significantly increase surgical risk and preclude rehabilitation.
- Severe Soft Tissue Compromise: Extensive soft tissue defects or compromised vascularity around the hip may complicate wound healing and increase infection risk, potentially contraindicating complex reconstruction.
- Poor Patient Compliance: Unreliable patients who cannot adhere to post-operative weight-bearing restrictions or rehabilitation protocols may be at higher risk for complications.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management (Cup-Cage) | Non-Operative Management |
|---|---|---|
| Acetabular Bone Loss | Paprosky 3A, 3B defects (segmental, cavitary, pelvic discontinuity) | Paprosky 1 or 2 defects (manageable with standard components/augments) |
| Progressive pain and instability due to bone loss | Asymptomatic or mildly symptomatic, stable implant | |
| Functional Impairment | Severe pain, inability to ambulate, poor quality of life | Mild pain, manageable with analgesics, maintained mobility |
| Pelvic Discontinuity | Symptomatic, unstable discontinuity | Asymptomatic, stable fibrous union or non-operative candidate |
| Infection | Staged revision for chronic PJI after debridement and eradication | Active systemic infection, unmanaged local infection |
| Patient Health | Medically optimized for major surgery | Severe comorbidities precluding safe surgical intervention |
| Bone Stock | Adequate host bone for robust cage fixation | Insufficient host bone quality/quantity for stable implant fixation |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful cup-cage reconstruction. It minimizes intraoperative surprises and optimizes outcomes.
Pre-Operative Planning:
-
Clinical Assessment:
- Thorough history and physical examination, including assessment of pain, instability, limb length discrepancy, and neurological status.
- Infection workup: ESR, CRP, joint aspiration for cell count, differential, and cultures (aerobic, anaerobic, fungal).
- Nutritional assessment: Albumin, prealbumin, total lymphocyte count, especially in revision cases.
- Evaluation of comorbidities and medical optimization.
-
Imaging Studies:
- Plain Radiographs: AP pelvis, lateral hip, and Judet views (obturator oblique and iliac oblique) are essential for initial assessment. Full-length hip-to-ankle radiographs are crucial for limb length assessment and global alignment.
- Computed Tomography (CT) Scan with 3D Reconstruction: Indispensable for detailed assessment of bone loss morphology (cavitary vs. segmental), localization of remaining host bone, quantification of bone stock in the ilium, ischium, and pubis, and precise templating for component sizing and screw trajectories. 3D models can be particularly helpful for visualizing complex defects like pelvic discontinuity.
- Advanced Imaging (Optional): MRI if tumor is suspected. Bone scan or PET/CT for infection workup in equivocal cases.
-
Classification of Bone Loss:
- Based on imaging, precisely classify the acetabular defect using Paprosky and/or AAOS systems to guide implant selection.
-
Templating:
- Acetabular Component: Determine the size and type of the inner articular component (e.g., polyethylene liner or modular shell).
- Cage Selection: Select the appropriate cage type (e.g., Burch-Schneider anti-protrusio cage, triflange cage, custom-designed cage). Template cage size and screw length/trajectory to ensure optimal fixation to viable host bone (ilium, ischium, pubis) while avoiding neurovascular structures.
- Grafting Material: Plan for the use of morselized autograft/allograft, structural allografts (femoral head, acetabular dome), or metal augments to fill cavitary defects or reconstruct segmental losses.
- Implant Availability: Ensure all necessary implants are available, including various cage sizes, long screws (up to 120 mm), augments, bone graft materials, specialty instruments, and potential backup options (e.g., custom triflange if cage fixation is not achievable).
- Surgical Plan: Develop a step-by-step operative plan, including surgical approach, sequence of reconstruction, expected challenges, and contingency plans.
Patient Positioning:
-
Lateral Decubitus Position:
This is the most common position for posterior or posterolateral approaches, providing excellent access to the posterior acetabulum.
- Ensure adequate padding to prevent nerve compression (peroneal nerve at fibular head, ulnar nerve at elbow).
- Position the patient firmly with sacral support and anterior/posterior posts to prevent rotation.
- Drape to allow for free manipulation of the limb for stability testing and dislocation maneuvers.
- Ensure fluoroscopy access for intraoperative imaging if needed.
-
Supine Position:
Used for anterior or anterolateral approaches.
- Padding for sacrum, heels, and arms.
- A bump under the ipsilateral hip can aid exposure.
- Fluoroscopy access.
Detailed Surgical Approach / Technique
The choice of surgical approach depends on the primary pathology, extent of bone loss, and surgeon preference. The posterior (Kocher-Langenbeck) approach is frequently employed due to its extensile nature and excellent exposure of the acetabulum, particularly the posterior column and ischium, which are critical for cage fixation.
Surgical Approach (Posterior - Kocher-Langenbeck):
- Incision: A curvilinear incision centered over the greater trochanter, extending proximally towards the posterior superior iliac spine and distally along the femoral shaft.
-
Muscle Dissection:
- Incise the fascia lata and split the gluteus maximus fibers in line with the skin incision.
- Identify and incise the piriformis and obturator internus tendons at their insertion on the greater trochanter. Carefully dissect and tag the external rotators (gemelli, quadratus femoris) for later repair. This exposes the posterior capsule.
- Crucial Landmark: Protect the sciatic nerve, which lies deep and medial to the quadratus femoris.
- Capsulotomy: Perform a T-shaped or inverse T-shaped capsulotomy to fully expose the femoral head and acetabulum.
- Femoral Head Dislocation/Removal: Dislocate the femoral head, typically by internally rotating and adducting the leg. If a previous stem is present, it may need to be revised first. Remove any existing acetabular components, cement, or fibrous tissue.
Acetabular Preparation:
-
Defect Assessment:
Re-assess the intraoperative bone defect using the Paprosky or AAOS classification.
- Debridement: Remove all remaining cement, granulomatous tissue, fibrous membranes, and osteolytic lesions. Ream to bleeding cancellous bone to promote vascularity and graft incorporation.
-
Containment of Defects:
- Cavitary Defects: Fill with morselized autograft or allograft. Impaction grafting can be used to create a stable bed.
-
Segmental Defects:
Reconstruct large segmental defects (e.g., superior rim, posterior column) with structural allografts (e.g., femoral head autograft/allograft shaped to fit) or metal augments. Fix these grafts securely with screws or wires to provide a stable foundation.


Cage Implantation:
- Trial Cage Placement: Carefully trial the selected cage to ensure optimal fit, coverage of defects, and stable contact with robust host bone. The cage should be positioned to restore the hip center of rotation.
-
Cage Fixation:
- Burch-Schneider or Anti-Protrusio Cage: The superior flange is seated against the ilium, and the inferior flange against the ischium (or anterior pubic ramus if accessible).
- Secure the cage with multiple cancellous or cortical screws. Screws are typically directed into the dense bone of the ilium (superiorly), ischium (inferiorly), and pubis (anteriorly). Use fluoroscopy to confirm screw trajectory and length, avoiding intrapelvic penetration and neurovascular injury.
-
Pelvic Discontinuity:
If a pelvic discontinuity is present, the cage must bridge the fracture site, obtaining rigid fixation in both the superior and inferior fragments. Compression across the discontinuity (if possible) prior to final screw tightening is ideal.

Cup Implantation:
-
Liner/Shell Insertion:
Once the cage is securely fixed, insert the polyethylene liner or modular metal shell into the cage. For certain designs (e.g., Burch-Schneider), the liner is cemented into the cage. Ensure proper orientation and secure locking mechanisms.
Femoral Preparation & Reduction:
- Femoral Stem Revision (if needed): If the femoral stem requires revision, proceed with standard techniques for explantation and re-implantation.
- Trial Reduction: Perform a trial reduction with the chosen femoral head and neck components. Assess hip stability through a full range of motion, evaluate leg length, and confirm appropriate offset. Adjust component sizes or neck lengths as necessary.
-
Final Component Insertion:
Insert the definitive femoral head, perform a final reduction, and confirm stability.



Closure:
- Irrigation: Thoroughly irrigate the wound.
- Capsule/Rotator Repair: Repair the external rotators and posterior capsule to enhance stability, especially if they were elevated.
- Layered Closure: Close the fascia lata, subcutaneous tissues, and skin in layers.
-
Drains:
Consider placing a drain, particularly in extensive revisions or cases with significant bleeding.

Complications & Management
Cup-cage reconstruction for severe acetabular bone loss is a complex procedure associated with a higher risk of complications compared to primary THA. Vigilant intraoperative technique and meticulous postoperative care are essential.
Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Intraoperative Hemorrhage | 10-30% | Meticulous hemostasis, judicious use of electrocautery, topical hemostatic agents, rapid transfusion protocol, consider pre-operative embolization for highly vascular lesions. |
| Nerve Injury (Sciatic, Femoral) | 1-5% | Careful retraction, identification and protection of nerves, avoidance of excessive limb manipulation, judicious screw placement (fluoroscopy guidance). Management ranges from observation to neurolysis; persistent deficits may require bracing or tendon transfers. |
| Periprosthetic Fracture (Pelvic) | 2-10% | Avoid over-reaming, careful screw insertion, prophylactic fixation of stress risers. Management depends on fracture pattern and stability; may require additional internal fixation (plates, screws), prolonged protected weight-bearing, or revision of the construct. |
| Pelvic Discontinuity Nonunion | 5-15% | Achieved rigid initial fixation of the cage bridging the discontinuity, impaction bone grafting. Management includes prolonged protected weight-bearing, bracing, or revision surgery with enhanced fixation (e.g., custom triflange, extended cage) and robust bone grafting with biologics. |
| Periprosthetic Joint Infection (PJI) | 2-10% (higher than primary) | Meticulous aseptic technique, perioperative antibiotics, debridement and irrigation, meticulous wound closure. Management typically involves surgical debridement and implant retention (DAIR) in acute cases or two-stage revision (explantation, debridement, antibiotic spacer, then reimplantation) for chronic cases. |
| Aseptic Loosening/Migration | 5-20% (long-term) | Secure cage fixation to host bone, proper bone grafting, restoration of hip center, appropriate weight-bearing restrictions. Management involves revision surgery, potentially with a custom triflange, further bone grafting, or explantation to a Girdlestone resection arthroplasty as a last resort. |
| Dislocation | 5-15% | Restoration of appropriate offset and leg length, proper component orientation, soft tissue tensioning, meticulous repair of posterior structures, patient education on precautions. Management involves closed reduction, bracing, or revision for recurrent instability (component malposition, soft tissue imbalance). |
| Heterotopic Ossification (HO) | 10-30% (clinical) | Prophylaxis with NSAIDs or single-dose radiation therapy (especially for high-risk patients). Management for symptomatic HO includes surgical excision once mature, often with repeat prophylaxis. |
| Screw Breakage/Migration | Variable (often asymptomatic) | Pre-operative templating for optimal screw length/trajectory, meticulous intraoperative fluoroscopy. Asymptomatic screw breakage usually requires observation. Symptomatic migration or articular penetration requires removal or revision. |
| Thromboembolic Events (DVT/PE) | 1-5% | Appropriate pharmacologic and mechanical prophylaxis. Early mobilization. Management includes anticoagulation; caval filter in selected high-risk patients with contraindications to anticoagulation or recurrent PE. |
| Wound Complications | 5-10% | Meticulous soft tissue handling, appropriate skin closure, infection prevention. Management includes local wound care, debridement, negative pressure wound therapy, or flap coverage for persistent defects. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following cup-cage reconstruction is critical for optimizing outcomes and preventing complications. The protocol must be individualized based on the stability of the reconstruction, the quality of bone graft incorporation, patient comorbidities, and surgeon preference. The primary goals are to protect the reconstructive construct, promote bone healing, restore muscle strength, and regain functional mobility.
Phase 1: Immediate Post-Operative (Days 0-6 Weeks)
-
Weight-Bearing:
This is often the most critical variable.
- Protected Weight-Bearing: Typically toe-touch weight-bearing (TTWB) or partial weight-bearing (PWB) with crutches or a walker for 6-12 weeks is recommended. This allows for bone graft incorporation and healing of the pelvic discontinuity, if present, without undue stress on the cage fixation.
- Strict Non-Weight-Bearing (NWB): May be indicated in cases of tenuous cage fixation, extensive bone grafting, or if pelvic discontinuity remains a concern for initial stability.
- Full Weight-Bearing (FWB): Generally avoided immediately and only considered if the surgeon is highly confident in the primary stability and there were no significant defects requiring extensive grafting (rare with cup-cage indications).
-
Range of Motion (ROM):
- Controlled, Pain-Free ROM: Initiate gentle active-assisted and passive ROM exercises within prescribed precautions.
- Dislocation Precautions: Maintain standard hip precautions (e.g., avoid hip flexion > 90 degrees, adduction past midline, internal rotation beyond neutral for posterior approach) to minimize dislocation risk.
-
Strengthening:
- Isometric Exercises: Gentle isometric quadriceps, gluteal, and hamstring sets to maintain muscle tone and promote circulation.
- Ankle Pumps: Essential for DVT prophylaxis.
-
Mobility:
- Begin with bed mobility, transfers (bed to chair), and short-distance ambulation with appropriate assistive devices and strict weight-bearing restrictions.
- Occupational therapy for ADL training with precautions.
- Wound Care: Monitor wound for signs of infection or hematoma. Drain removal typically within 24-48 hours.
Phase 2: Early Rehabilitation (Weeks 6-12)
- Weight-Bearing Progression: Gradually advance weight-bearing from TTWB/PWB to 50% body weight, depending on radiographic evidence of bone healing and clinical stability. This transition is guided by surgeon assessment and serial radiographs.
- ROM: Continue with progressive ROM exercises, gradually increasing the arc of motion while respecting precautions.
-
Strengthening:
- Gentle Isotonic Strengthening: Introduce low-resistance hip abduction, extension, and flexion exercises (e.g., supine slides, gravity-eliminated exercises).
- Core Stability: Initiate core strengthening exercises to improve trunk stability.
- Gait Training: Focus on normalized gait pattern with appropriate assistive devices. Wean from walker to crutches.
Phase 3: Intermediate Rehabilitation (Months 3-6)
- Weight-Bearing: Progress to full weight-bearing as tolerated, typically around 3-4 months, once radiographic evidence of graft incorporation and solid cage fixation is confirmed. Wean off assistive devices.
- ROM: Continue to work on restoring full pain-free ROM.
-
Strengthening:
- Progressive Resistance Exercises: Increase intensity and resistance for hip and core musculature.
- Balance and Proprioception: Introduce balance exercises.
- Functional Activities: Gradually return to light recreational activities (e.g., walking, swimming, stationary cycling). Avoid high-impact activities.
Phase 4: Advanced Rehabilitation / Return to Activity (Months 6+)
- Full Weight-Bearing & Activity: Patient should be fully weight-bearing without assistive devices.
- Strengthening: Continue advanced strengthening and conditioning tailored to functional goals.
- Return to Sport/Work: Gradual return to more demanding recreational activities or work, with continued caution regarding high-impact or contact sports. Individualized assessment is crucial.
Monitoring:
- Radiographic Follow-up: Serial radiographs (AP pelvis, lateral hip) are essential at regular intervals (e.g., 6 weeks, 3 months, 6 months, 1 year, then annually) to monitor cage position, screw integrity, bone graft incorporation, and signs of loosening or osteolysis.
- Clinical Follow-up: Regular clinical visits to assess pain, function, gait, and compliance with precautions.
Summary of Key Literature / Guidelines
The existing literature on cup-cage reconstruction for severe acetabular bone loss, while primarily consisting of retrospective case series and single-center studies, consistently demonstrates that this technique offers a durable and effective solution for complex revision scenarios. Long-term outcomes, however, remain challenging due to the inherent complexity of the patient population and bone deficiencies.
Key Findings from Literature:
- Clinical Outcomes: Multiple studies report favorable clinical outcomes, with significant improvements in pain and functional scores (e.g., Harris Hip Score, WOMAC) in a majority of patients. While not achieving the same outcomes as primary THA, cup-cage constructs generally lead to substantial improvement from pre-operative status.
- Survival Rates: Mid-term implant survival rates for cup-cage constructs typically range from 70-90% at 5-10 years, with revision for aseptic loosening being the most common reason for failure. Long-term survival data beyond 10-15 years is more limited but shows a decline in survivorship, particularly in patients with significant comorbidities or initial poor bone quality.
- Pelvic Discontinuity: Cup-cage constructs are considered a gold standard for managing pelvic discontinuity, with reported union rates ranging from 60-90%. Factors influencing union include rigid fixation, meticulous bone grafting, and strict adherence to protected weight-bearing protocols. Nonunion of the discontinuity is a significant contributor to revision.
- Bone Grafting: The use of autograft and allograft (morselized or structural) to reconstruct defects and promote biological ingrowth is a critical adjunct to cage reconstruction. Successful graft incorporation is essential for long-term stability and reduction of micromotion.
-
Comparison to Other Techniques:
- Custom Triflangeless Acetabular Components (CTACs): CTACs, often 3D-printed based on pre-operative CT scans, offer a highly customized solution for extremely complex defects, particularly when there's insufficient host bone for standard cage fixation. While initially showing promising results, they are more expensive and technically demanding. Comparative studies are ongoing, but both cup-cages and CTACs represent viable options for Paprosky 3B defects.
- Massive Allografts: Once a popular option, massive acetabular allografts have generally fallen out of favor due to high rates of nonunion, resorption, and infection, leading to inferior long-term survival compared to modern cage constructs. They may still have a role in specific situations (e.g., tumor reconstruction).
- Jumbo Cups with Augments: For Paprosky 2B/2C and some 3A defects, large cementless hemispheric cups combined with metal augments can provide satisfactory results. However, for true Paprosky 3B or pelvic discontinuity, the structural support provided by a cage is often superior.
- Complication Rates: As noted in the previous section, complication rates are higher than in primary THA. PJI, aseptic loosening, and dislocation remain significant concerns.
-
Guidelines:
While no universal "cup-cage" specific guidelines exist from major orthopedic bodies like AAOS or EFORT, the general principles for revision THA apply:
- Thorough pre-operative planning with advanced imaging.
- Meticulous debridement and bone bed preparation.
- Stable fixation of components to healthy host bone.
- Restoration of hip biomechanics (center of rotation, offset, leg length).
- Appropriate post-operative weight-bearing and rehabilitation.
Future Directions:
Advancements in 3D printing technology, improved biomaterials for augments and cages (e.g., porous tantalum, trabecular titanium), and enhanced understanding of bone biology continue to evolve the landscape of acetabular reconstruction. The long-term performance of these newer materials and techniques against established cup-cage constructs will require ongoing research and follow-up.
In conclusion, cup-cage reconstruction remains a cornerstone technique for addressing severe acetabular bone loss in revision THA. When performed with meticulous planning, precise surgical technique, and appropriate post-operative care, it offers a durable and functional solution for patients facing these complex challenges.
Clinical & Radiographic Imaging

You Might Also Like