Mastering Severe Bone Loss: Highly Porous Metal for Revision THA

Key Takeaway
For anyone wondering about Mastering Severe Bone Loss: Highly Porous Metal for Revision THA, Pelvic discontinuity with severe acetabular bone loss, often seen in revision hip arthroplasty, is addressed by options like cup-cage reconstruction. This complex procedure frequently utilizes a large, highly porous metal cup and a spanning ilioischial cage. This approach provides mechanical stability and encourages biological fixation, crucial for overcoming poor bone quality.
Introduction & Epidemiology
Revision total hip arthroplasty (THA) for severe bone loss represents one of the most challenging endeavors in reconstructive orthopedic surgery. The incidence of primary THA continues to rise, and with it, the number of patients requiring revision surgery. Severe bone loss, typically defined by extensive cavitary, segmental, or combined defects classified as Paprosky Type IIB, III, or IV for the acetabulum, and Type II, III, or IV for the femur, significantly complicates surgical planning and execution. These defects often result from aseptic loosening, periprosthetic joint infection (PJI), osteolysis, or multiple prior revisions.
Traditional reconstruction techniques for severe bone loss, including impaction grafting, bulk allografts, or custom prostheses, have demonstrated variable long-term success rates and specific associated complications, such as allograft resorption, fracture, or non-union. The advent of highly porous metal (HPM) implants has revolutionized the approach to these complex cases. HPMs, characterized by their high porosity (70-80%), low modulus of elasticity (closer to bone than solid metals), and osteoconductive scaffold, promote robust biological ingrowth and provide immediate mechanical stability. This allows for restoration of joint mechanics, reconstruction of bone defects, and a durable biological fixation interface, offering a significant advantage in the management of severe bone loss in revision THA. The growing experience and long-term data on HPMs underscore their role as a critical tool in the armamentarium of the revision arthroplasty surgeon.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanical principles is paramount when addressing severe bone loss in revision THA. The hip joint's stability, load-bearing capacity, and range of motion are intricately linked to the integrity of the bony architecture and surrounding soft tissues.
Acetabular Anatomy and Bone Loss
The acetabulum, formed by the ilium, ischium, and pubis, presents a complex three-dimensional structure. Severe bone loss often involves critical load-bearing areas such as the superior dome, anterior and posterior columns, and the medial wall. The Paprosky classification system is invaluable for categorizing acetabular defects:
*
Type I:
Minimal bone loss, intact rim.
*
Type IIA:
Contained cavitary defect, intact columns.
*
Type IIB:
Segmental bone loss, typically superior, intact columns, compromised rim.
*
Type IIC:
Medial wall defect, intact columns.
*
Type IIIA:
Major column compromise, contained cavitary defect, stable host bone.
*
Type IIIB:
Major column compromise, uncontained segmental defect, severe instability.
*
Type IV:
Pelvic discontinuity.
HPMs are particularly advantageous in Paprosky Type IIB, III, and IV defects. Their high frictional characteristics provide immediate stability against host bone, while their interconnected pore structure promotes osteointegration, crucial for long-term fixation. The lower modulus of elasticity compared to solid implants may also mitigate stress shielding, encouraging load transfer to the host bone.
Femoral Anatomy and Bone Loss
The proximal femur, with its distinct cortical and cancellous architecture, presents a different set of challenges. Femoral bone loss can range from isolated calcar defects to extensive diaphyseal loss, often classified by Paprosky:
*
Type I:
Minimal metaphyseal bone loss.
*
Type II:
Metaphyseal bone loss, intact diaphysis, often with widening of the canal.
*
Type IIIA:
Extensive metaphyseal and diaphyseal bone loss, leaving at least 4 cm of intact distal host bone.
*
Type IIIB:
Severe diaphyseal bone loss, less than 4 cm of intact distal host bone, often cortical fenestrations or thin cortex.
*
Type IV:
Femoral discontinuity or complete loss of proximal femoral support.
HPMs, such as modular femoral sleeves or fully porous-coated stems, offer solutions for Type II, III, and IV defects. Sleeves can provide robust metaphyseal fill and achieve proximal biologic fixation, bypassing deficiencies in the host cancellous bone. Longer, fully porous stems can engage distal diaphyseal bone to achieve stable fixation where proximal bone is severely compromised. The biomechanical goal is to achieve adequate initial stability to allow for bone ingrowth, restore leg length and offset, and provide a durable construct that can withstand physiological loads.
Indications & Contraindications
The decision to utilize highly porous metal implants in revision THA is guided by specific indications related to the nature and severity of bone loss, coupled with an assessment of the patient's overall health and functional goals.
Indications for Highly Porous Metal Implants in Revision THA
- Aseptic Loosening with Severe Bone Loss: This is the most common indication. For acetabular defects, Paprosky Type IIB, III, and IV, where structural support is compromised, HPM acetabular components (shells, augments, cones, or triflange components) can restore the acetabular dome and provide a stable base for the liner. For femoral defects, Paprosky Type II, III, and IV, HPM femoral sleeves combined with modular stems or long, fully porous-coated stems are indicated to bypass defects and achieve robust diaphyseal fixation.
- Periprosthetic Joint Infection (PJI) - Staged Reconstruction: Following successful eradication of infection, often confirmed by negative cultures and normalization of inflammatory markers, HPM implants are considered for definitive reconstruction in cases with significant bone deficits. The biological fixation of HPMs is particularly beneficial as it reduces reliance on cement, which can act as a nidus for recurrent infection.
- Periprosthetic Fracture with Bone Loss: Fractures around existing implants (Vancouver B2/B3 for femur, or acetabular fractures) that result in substantial bone loss often require HPMs to reconstruct the defect and achieve stable fixation for the new components.
- Severe Acetabular Protrusio: When the medial wall is significantly compromised, leading to protrusion of the femoral head into the pelvis, HPM components can be used to reconstruct the medial wall and provide adequate containment.
- Prior Failed Allograft Reconstruction: In cases where previous bulk allografts have failed due to resorption, fracture, or non-union, HPMs can offer a more predictable and durable solution for bone defect reconstruction.
- Correction of Major Deformity: HPM components, especially modular systems, allow for greater flexibility in restoring hip biomechanics, including leg length, offset, and version, even in the presence of complex bone defects.
Contraindications for Highly Porous Metal Implants in Revision THA
- Active, Uncontrolled Periprosthetic Joint Infection: The presence of an active, untreated infection is an absolute contraindication for definitive implantation of any prosthetic device, including HPMs. Infection must be thoroughly eradicated prior to reconstructive surgery.
- Insufficient Host Bone for Initial Stability: While HPMs are excellent for bone ingrowth, there must be a minimum amount of viable host bone available to achieve initial mechanical stability (press-fit or screw fixation) until biological fixation occurs. In rare cases of extreme bone loss, other options like custom implants or even limb salvage procedures may be considered.
- Severe Systemic Comorbidities: Patients with significant medical comorbidities that preclude major surgical intervention and prolonged rehabilitation are poor candidates.
- Unrealistic Patient Expectations: Clear communication regarding potential functional outcomes, limitations, and the lengthy rehabilitation process is essential.
- Allergy to Implant Materials: While rare, a documented allergy to specific implant materials (e.g., nickel in some alloys) would necessitate alternative materials.
- Severe Soft Tissue Compromise: Compromised soft tissue envelope or poor wound healing potential can increase the risk of infection and wound dehiscence, potentially jeopardizing the success of the revision.
Operative vs. Non-Operative Indications
The following table outlines considerations for operative intervention using HPMs versus non-operative management for hip pathology, recognizing that severe bone loss often mandates surgery.
| Feature | Operative (Revision THA with HPM) | Non-Operative (Conservative Management) |
|---|---|---|
| Primary Indication | Symptomatic aseptic loosening, severe osteolysis, PJI (staged), periprosthetic fracture with significant bone loss. | Mild, stable loosening; asymptomatic implant; severe medical comorbidities precluding surgery. |
| Pain | Persistent, debilitating pain affecting daily activities. | Manageable pain with analgesics, activity modification. |
| Functional Impairment | Significant limitation in ambulation, ADLs, or severe instability. | Acceptable functional status within patient's goals. |
| Radiographic Findings | Progressive implant migration, subsidence, significant bone loss (Paprosky IIB-IV acetabulum/femur). | Stable implant position over time, minimal or non-progressive bone loss. |
| Infection Status | Eradicated PJI. | No evidence of infection, or patient deemed unsuitable for infection management. |
| Patient Health | Medically optimized, reasonable life expectancy, ability to participate in rehabilitation. | Significant comorbidities, poor surgical risk, limited rehabilitation potential. |
| Bone Stock | Sufficient host bone for initial HPM implant stability and potential ingrowth. | Insufficient bone stock, extreme diffuse osteopenia where fixation is unattainable. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of a successful revision THA with severe bone loss, particularly when employing highly porous metal implants.
Diagnostic Workup and Bone Loss Assessment
- Radiographs: Standard AP pelvis, true lateral hip, and full-length femur radiographs are essential. These provide a baseline assessment of implant position, integrity, and preliminary evaluation of bone defects. Comparative views of the contralateral hip can aid in templating and understanding leg length discrepancy.
-
Computed Tomography (CT) Scan:
A CT scan with metal artifact reduction sequence (MARS) is invaluable. It provides detailed, three-dimensional information regarding the extent and morphology of bone defects, aiding in precise Paprosky classification for both acetabulum and femur. It helps delineate cavitary versus segmental defects, assess column integrity, and identify areas of cortical fenestration or thinning. This information guides the selection of specific HPM augments, cones, or sleeves.
 - Infection Workup: For all revisions, PJI must be ruled out. This includes serum erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and potentially aspiration of the hip joint for cell count, differential, and microbial cultures, as well as alpha-defensin testing.
- Nutritional Status: Assess patient's nutritional status (albumin, prealbumin). Malnutrition is a significant risk factor for complications, including delayed wound healing and impaired osteointegration.
Component Selection and Templating
Digital templating is crucial. Utilize software to:
*
Assess Implant Size and Type:
Determine the appropriate HPM acetabular shell size, potential need for augments or cones, and their optimal placement. For the femur, assess stem length, diameter, and the need for modular sleeves to reconstruct proximal defects.
*
Restoration of Biomechanics:
Plan for restoration of leg length, femoral offset, and acetabular anteversion/inclination. HPM components often come in modular designs, offering flexibility in achieving these goals.
*
Contingency Planning:
Always have a range of implant sizes, types, and supplementary materials (e.g., allograft chips, structural allograft, bone cement) available in the operating room. Consideration for a custom triflange acetabular component may be warranted for extreme Paprosky Type IIIB or Type IV defects.
Patient Optimization
- Medical Clearance: Ensure thorough medical evaluation and optimization of chronic conditions (e.g., diabetes, cardiovascular disease).
- Smoking Cessation: Encourage cessation of smoking for at least 6-8 weeks pre-operatively to improve bone healing and reduce wound complications.
- Physical Therapy: Pre-operative physical therapy can improve muscle strength and range of motion, aiding in post-operative recovery.
Patient Positioning
- Lateral Decubitus Position: This is the most common position for posterior or posterolateral approaches. Ensure the patient is securely positioned and adequately padded at all pressure points. The operative limb is draped free to allow for full range of motion assessment during trial reduction.
- Supine Position: Used for anterior approaches (e.g., direct anterior). This position may offer benefits in certain reconstruction scenarios but potentially limits exposure in complex posterior column or posterior femoral defects.
- Considerations: Regardless of position, ensure adequate access to both the acetabulum and the entire femoral shaft, as extension osteotomies may be required.
Detailed Surgical Approach / Technique
The surgical technique for revision THA with severe bone loss utilizing highly porous metals demands meticulous attention to detail, extensive exposure, and strategic management of bone defects. The specific approach and sequence of steps will vary based on the primary etiology, location, and severity of bone loss.
General Principles
- Exposure: Obtain wide surgical exposure. This may necessitate extensile approaches, trochanteric osteotomies, or even femoral osteotomy to safely remove existing implants and address severe bone loss.
- Debridement: Thoroughly debride all fibrous tissue, granuloma, cement, and necrotic bone. Send samples for culture, especially if PJI is suspected.
- Bone Loss Assessment: Re-evaluate the bone defects intraoperatively, comparing findings to pre-operative imaging. This may necessitate adjustments to the planned reconstruction strategy.
Acetabular Reconstruction with Highly Porous Metal
The goal is to restore the hip center, achieve immediate stability, and provide a scaffold for long-term osteointegration.
- Implant Removal: Carefully remove the existing acetabular component and any remaining cement. Use specialized tools to minimize further bone loss.
- Defect Preparation: Prepare the host bone bed. Debride sclerotic bone to reveal bleeding cancellous bone. Ream the acetabulum to a spherical contour, aiming for concentric reaming to the native acetabular floor where possible.
-
Contained Defects (Paprosky Type IIA/B, IIC):
- For contained cavitary defects, impact cancellous allograft chips to fill the void.
- Select an appropriately sized HPM acetabular shell for press-fit fixation. HPM cups offer high friction coefficients, providing excellent initial stability even in compromised bone.
-
Augment the cup with multiple screws into stable bone (e.g., ilium, ischium, pubis).

-
Uncontained Defects (Paprosky Type IIB/IIIA):
- Augments: For superior segmental defects (IIB/IIIA) or column deficiencies, HPM augments (often crescent-shaped or oblong) are invaluable. They are contoured to fit the defect and then secured to the host bone with screws. The main HPM acetabular shell is then implanted, often achieving fixation partly into the augment and partly into host bone.
-
 - Cones: For Paprosky Type IIIA defects, particularly those involving central medial protrusion or superior-central bone loss, HPM cones can be inserted first. These cones are press-fit into the remaining host bone and provide structural support for the HPM acetabular shell, effectively centralizing the load. The cone is typically fixed with screws.
-

-
Severe Uncontained Defects / Pelvic Discontinuity (Paprosky Type IIIB/IV):
- These cases may require a combination of HPM augments and cones, or even custom triflange acetabular components.
- Triflange Components: Custom HPM triflange components are specifically designed based on pre-operative CT scans to match the complex defect, providing fixation to the remaining ilium, ischium, and pubis, essentially creating a new acetabulum. This is a salvage option for extreme cases.
- Reconstruct the columns first, using HPM augments or structural allograft, then proceed with cup fixation.
Femoral Reconstruction with Highly Porous Metal
The objective is to achieve stable fixation, restore limb length and offset, and provide a durable construct that can withstand loading.
- Implant Removal: Careful removal of the existing femoral stem and cement, especially if there's significant ingrowth or a well-fixed stem, often requires extended trochanteric osteotomy (ETO) or creation of cortical windows.
- Defect Assessment: Assess the remaining femoral bone stock using the Paprosky classification. Address any cortical defects or fenestrations.
- Canal Preparation: Ream the femoral canal to the appropriate diameter, typically under-reaming slightly to ensure a tight press-fit.
-
Proximal Femoral Reconstruction (Paprosky Type II/IIIA):
- Highly Porous Sleeves: For significant metaphyseal bone loss and widened canals (Paprosky Type II and IIIA), HPM sleeves are frequently used. These sleeves are press-fit into the proximal femur, providing robust metaphyseal fill and immediate stability through hoop stress. They are often fixed with screws if additional stability is needed.
-
 - A modular tapered stem (often coated with HPM for ingrowth) is then inserted through the sleeve, engaging distal diaphyseal bone. This construct allows for independent adjustment of leg length and offset.
-
 -

-
Diaphyseal Fixation for Severe Bone Loss (Paprosky Type IIIB/IV):
- For extensive diaphyseal bone loss (Paprosky Type IIIB) where proximal fixation is compromised, long, fully porous-coated stems are used to achieve stable fixation in the distal diaphysis, bypassing the defects. These stems may be tapered or cylindrical.
- For Type IV defects or those requiring extensive cortical reconstruction, custom stems or allograft-prosthesis composites may be necessary.
-

- Bone Grafting: Autograft or allograft chips can be impacted into any remaining cavitary defects to provide osteoconductive material and promote bone regeneration around the HPM implants.
Reduction and Stability Assessment
- Trial Reduction: Insert trial components to assess joint stability through a full range of motion, evaluate leg length, and ensure appropriate soft tissue tension. Make necessary adjustments to head and liner size.
- Final Implants: Once optimal stability and biomechanics are achieved, implant the final HPM components and liner.
Closure
Perform meticulous layered closure of the capsule, short external rotators, vastus lateralis (if trochanteric osteotomy was performed), muscle fascia, subcutaneous tissue, and skin. Ensure thorough hemostasis and consider drain placement based on surgical bleeding.
Complications & Management
Revision THA with severe bone loss carries a higher risk of complications compared to primary THA due to compromised host bone, extensive dissection, and often, prior infection. The use of highly porous metals, while offering significant advantages, does not eliminate these risks.
Intraoperative Complications
-
Periprosthetic Fracture:
Incidence is 1-5%.
- Acetabular: Fracture of columns or rim during reaming or cup insertion.
- Femoral: Intraoperative fracture during stem removal, reaming, or stem insertion.
- Management: Varies from cerclage wiring, plating, or revision to a longer stem or different HPM component (e.g., using augments or cones to bridge a defect). Careful intraoperative assessment and immediate fixation are paramount.
-
Neurovascular Injury:
Incidence <1%. Sciatic nerve palsy, femoral nerve palsy, or injury to major vessels (femoral, external iliac).
- Management: Immediate recognition, neurological consultation, and prompt vascular repair if indicated. Careful dissection and retraction are crucial for prevention.
-
Uncontrolled Hemorrhage:
Can occur due to extensive scarring, previous surgery, or difficulty achieving hemostasis in compromised bone.
- Management: Meticulous hemostasis, judicious use of electrocautery, bone wax, and hemostatic agents. Transfusion support as needed.
Early Post-Operative Complications
-
Periprosthetic Joint Infection (PJI):
Incidence 1-4%.
- Management: Early recognition (fever, wound drainage, pain, elevated inflammatory markers), fluid aspiration for culture, and staged revision with thorough debridement, antibiotic spacers, and subsequent reimplantation of HPM components.
-
Dislocation:
Incidence 3-10%, higher than primary THA.
- Management: Closed reduction. If recurrent, evaluate for component malposition, soft tissue imbalance, or patient factors. Open reduction, constrained liners, or revision for component repositioning may be required.
-
Deep Venous Thrombosis (DVT) / Pulmonary Embolism (PE):
Incidence 1-5%.
- Management: Prophylactic anticoagulation is standard. Treatment involves therapeutic anticoagulation.
-
Wound Complications:
Hematoma, seroma, wound dehiscence. Incidence 5-10%.
- Management: Minor complications may resolve with conservative management. Hematomas may require evacuation. Dehiscence may require debridement and resuturing.
-
Early Aseptic Loosening:
Failure of initial fixation before bone ingrowth occurs. Rare with HPM if stable primary fixation achieved.
- Management: May require early re-revision with further bone reconstruction.
Late Post-Operative Complications
-
Aseptic Loosening / Osteolysis:
Incidence 5-15% over 10 years, depending on defect severity. Failure of osteointegration or subsequent bone resorption.
- Management: Symptomatic loosening requires re-revision. HPMs are designed to mitigate this, but severe osteolysis can still occur.
-
Chronic Infection:
Persistent low-grade infection.
- Management: Similar to early PJI, often requiring explantation, debridement, and staged reconstruction.
-
Heterotopic Ossification (HO):
Incidence 10-30%. Bone formation in soft tissues around the hip.
- Management: Prophylaxis with NSAIDs or radiation in high-risk patients. Symptomatic HO may require surgical excision.
-
Implant Fracture:
Rare, but can occur with fatigue failure of HPM components or the underlying stem.
- Management: Re-revision, often involving complex implant removal and reconstruction.
-
Femoral Stem Subsidence:
More common with longer stems and compromised bone quality.
- Management: Close observation for asymptomatic, stable subsidence. Symptomatic or progressive subsidence requires revision.
- Nerve Palsies: Can manifest later if related to scar tissue impingement or chronic stretch.
Complications Table
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Intraoperative Fracture | 1-5% | Cerclage wiring, plate fixation, revision to longer/different HPM implant, bone graft. |
| Neurovascular Injury | <1% | Immediate recognition, vascular repair, nerve exploration/repair, neurological consultation. |
| PJI (Early/Late) | 1-4% | Debridement, antibiotic irrigation, spacer, staged revision with appropriate antibiotics, HPM reimplantation. |
| Dislocation | 3-10% | Closed reduction, activity modification, bracing, revision for component repositioning, constrained liner. |
| Aseptic Loosening | 5-15% (10yr) | Re-revision with further bone reconstruction using HPMs, impaction grafting, custom implants. |
| Osteolysis | Variable | Debridement of granuloma, bone grafting, component exchange, revision. |
| Heterotopic Ossification | 10-30% | Prophylactic NSAIDs/radiation, surgical excision for symptomatic cases. |
| Femoral Subsidence | 2-5% | Observation, revision with longer stem or more robust diaphyseal fixation. |
| Wound Complications | 5-10% | Debridement, re-suturing, wound VAC, muscle flap coverage. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following revision THA with highly porous metal implants for severe bone loss is critical for optimizing outcomes and ensuring successful biological ingrowth and long-term implant survival. Protocols must be tailored to the specific reconstruction, stability of fixation, and patient comorbidities.
Phase I: Immediate Post-Operative (0-6 Weeks)
Goals: Protect the surgical repair, manage pain and swelling, prevent complications, initiate early mobilization, and educate the patient on precautions.
-
Weight-Bearing Status:
This is highly dependent on intraoperative stability and the quality of host bone.
- Typically Partial Weight-Bearing (PWB) or Toe-Touch Weight-Bearing (TTWB): For most HPM reconstructions, especially large acetabular defects or extensive femoral reconstructions, to allow for bone ingrowth without excessive shear forces.
- Weight-Bearing as Tolerated (WBAT): May be permissible for smaller defects with excellent primary stability, but often restricted initially.
- Non-Weight-Bearing (NWB): Rarely indicated unless there is significant concern for fracture or extreme instability.
-
Activity Restrictions:
- Hip Precautions: Maintain standard posterolateral (avoid hip flexion >90°, adduction past midline, internal rotation) or anterior (avoid hip extension, external rotation) precautions as per surgical approach, typically for 6-12 weeks.
- Avoid twisting motions and impact loading.
-
Therapeutic Exercises:
- Ankle Pumps: To prevent DVT.
- Gentle Isometric Exercises: Quadriceps sets, gluteal sets.
- Supine Hip Abduction/Adduction: Small range, within pain limits, avoiding hip flexion.
- Assisted Ambulation: With walker or crutches, adhering to prescribed weight-bearing.
- Pain Management: Multimodal analgesia, including nerve blocks, oral opioids, and NSAIDs (if not contraindicated).
- Wound Care: Monitor for signs of infection or hematoma.
Phase II: Intermediate (6-12 Weeks)
Goals: Gradually increase weight-bearing, restore range of motion, improve muscle strength, and progress functional activities.
- Weight-Bearing Progression: Progress from TTWB/PWB to WBAT as radiographic signs of ingrowth appear (usually by 6-8 weeks) and pain allows.
-
Therapeutic Exercises:
- Active-Assisted/Active Range of Motion: Hip flexion (within precautions), abduction, adduction, external rotation.
- Strengthening: Light resistance exercises for hip abductors, extensors, and flexors (e.g., resisted hip abduction, mini-squats, hip extension in standing).
- Core Strengthening: Crucial for trunk stability and proper gait mechanics.
- Proprioception and Balance Training: Single-leg stance (supported initially).
- Gait Training: Progress from walker to cane, focusing on normal gait patterns and equal weight distribution.
- Activity Restrictions: Continue hip precautions. Avoid high-impact activities.
Phase III: Advanced (3-6 Months)
Goals: Achieve full functional range of motion, maximize strength and endurance, improve balance, and prepare for return to modified activities.
- Weight-Bearing: Full weight-bearing as tolerated without assistive devices.
-
Therapeutic Exercises:
- Progressive Resistance Exercises: Increase intensity and resistance for all hip musculature.
- Functional Training: Stair climbing, uneven surfaces, light agility drills (if appropriate).
- Sport-Specific Training: For patients aiming to return to low-impact sports (e.g., swimming, cycling).
- Activity Restrictions: Hip precautions may be discontinued if cleared by the surgeon and therapist based on clinical and radiographic stability. Avoid running, jumping, and contact sports.
Phase IV: Maintenance (6 Months Onwards)
Goals: Maintain strength, flexibility, and endurance; ensure long-term joint health; encourage lifelong exercise habits.
- Self-Management: Patients encouraged to continue home exercise programs.
- Low-Impact Activities: Swimming, cycling, walking, elliptical training.
- Regular Follow-up: Routine clinical and radiographic follow-up to monitor implant integrity and bone ingrowth.
Key Considerations for HPM:
The robust osteoconductive nature of HPM implies that early mechanical stability is critical for successful long-term biological fixation. Adherence to prescribed weight-bearing is paramount to allow for bone ingrowth without micromotion, which could lead to fibrous tissue interposition rather than bone. Rehabilitation protocols may be slightly more conservative initially compared to primary THA to safeguard this ingrowth process.
Summary of Key Literature / Guidelines
The evolution of highly porous metals has significantly advanced the field of revision THA, particularly for severe bone loss. Initial HPMs were primarily composed of tantalum (e.g., Trabecular Metal™), known for its high porosity, low modulus of elasticity, and excellent biocompatibility. More recently, porous titanium and other alloys have entered the market, offering similar biomechanical advantages.
Key Findings from Literature:
- Osteointegration and Biocompatibility: Studies consistently demonstrate superior osteointegration and biocompatibility of HPMs compared to traditional plasma-sprayed or beaded surfaces. The interconnected pore structure (typically 500-700 µm pore size) facilitates bone ingrowth and ongrowth, providing a robust biological interface. Histological studies have confirmed direct bone apposition onto HPM structures.
- Modulus of Elasticity: The modulus of elasticity of HPMs (e.g., 3-10 GPa for Trabecular Metal) is closer to that of cancellous bone (1-20 GPa) than solid titanium (110 GPa) or cobalt-chromium (230 GPa). This "stress-shielding" effect is reduced, theoretically promoting more physiological load transfer to the host bone and potentially reducing peri-implant bone loss.
- Frictional Stability: HPMs exhibit high coefficients of friction, providing immediate mechanical stability upon impaction into host bone. This is crucial in compromised bone stock, allowing for primary stability that is essential for subsequent biological fixation.
-
Acetabular Reconstruction:
- Long-term Survival: Several studies report excellent long-term survival rates for HPM acetabular components in revision THA with severe bone loss. For Paprosky Type II and III defects, 10-year survivorships typically range from 85-95%, with many series exceeding 90%.
- Augments and Cones: The use of HPM augments and cones has proven particularly effective in reconstructing large contained and uncontained defects (Paprosky IIB, III). These constructs allow for restoration of the hip center and provide a stable platform for definitive cup fixation, often bridging extensive segmental defects.
- Pelvic Discontinuity: While challenging, HPM triflange custom components offer a viable, albeit complex, solution for Paprosky Type IV pelvic discontinuities, with reported success rates depending on patient selection and surgeon experience.
-
Femoral Reconstruction:
- Modular Sleeves: HPM femoral sleeves, used in conjunction with modular stems, have shown promising results for Paprosky Type II and IIIA femoral defects. They provide reliable metaphyseal fixation and allow for independent restoration of limb length and offset. Studies report durable fixation with low rates of aseptic loosening.
- Diaphyseal Fixation: For more extensive defects (Paprosky IIIB/IV), long, fully porous-coated stems achieving distal diaphyseal fixation have demonstrated good long-term outcomes, especially when combined with impaction grafting for cavitary defects.
- Infection Management: HPMs are commonly used in staged revisions for PJI. Their ability to achieve biological fixation without cement can be advantageous, as cement can harbor bacteria and complicate future infection management.
- Guidelines: Current guidelines from major orthopedic associations (e.g., AAOS, AAHKS) emphasize detailed pre-operative planning with advanced imaging, meticulous surgical technique, and individualized rehabilitation protocols for revision THA with bone loss. The use of HPMs is increasingly supported as a standard of care for moderate to severe bone defects due to their established biological and biomechanical advantages.
In conclusion, highly porous metal implants represent a significant advancement in the armamentarium for managing severe bone loss in revision THA. Their unique properties promote robust biological ingrowth, provide immediate mechanical stability, and offer versatility in reconstructing complex defects. While demanding meticulous surgical technique and careful patient selection, the accumulating body of evidence supports their efficacy and durability in achieving successful long-term outcomes in these challenging patients.
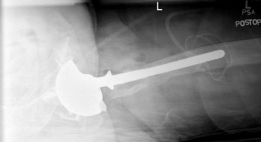
Clinical & Radiographic Imaging

You Might Also Like


