Achieving Success with Uncemented Hip Arthroplasty Metal Socket

Key Takeaway
Looking for accurate information on Achieving Success with Uncemented Hip Arthroplasty Metal Socket? Total hip arthroplasty addresses severe hip osteoarthritis, as demonstrated in a 69-year-old female's case. The procedure replaces the hip joint with prosthetic components, often including an uncemented acetabular shell and stem, and a ceramic femoral head with a polyethylene liner. Consideration of hip arthroplasty metal components, like the porous-coated shell, is vital for fixation and long-term success in restoring mobility and reducing pain.
Introduction & Epidemiology
Uncemented hip arthroplasty has evolved significantly since its inception, with the uncemented metal acetabular socket now a cornerstone of modern total hip arthroplasty (THA). The principle relies on the biologic fixation (osseointegration) of bone onto a porous-coated implant surface, providing durable long-term stability. This contrasts with cemented fixation, which relies on a polymethylmethacrylate (PMMA) interface for mechanical interlock.
The initial enthusiasm for uncemented components in the 1980s was met with early challenges, particularly with first-generation designs that often lacked adequate surface porosity, coating adherence, or macro-interlock features, leading to early loosening and revision. Subsequent advancements in material science, surface technologies (e.g., plasma spray titanium, hydroxyapatite coatings), and implant design (e.g., hemispherical press-fit shells, supplementary screw fixation options) have dramatically improved outcomes.
Epidemiologically, uncemented acetabular components have become the preferred choice for a substantial proportion of THAs, particularly in younger, more active patient populations with good bone stock. Data from national joint registries consistently demonstrate excellent long-term survival rates, often exceeding 90-95% at 10-15 years for contemporary uncemented sockets. This widespread adoption is driven by the potential for long-term implant durability, bone stock preservation, and facilitated revision surgery compared to cemented counterparts. The prevalence of uncemented acetabular fixation has surpassed cemented fixation in many regions globally, underscoring its established role in primary THA.
Surgical Anatomy & Biomechanics
Acetabular Bony Anatomy
A comprehensive understanding of acetabular anatomy is paramount for precise component placement and optimizing osseointegration. Key bony landmarks include:
*
Acetabular Rim:
The superior and posterior aspects are critical for primary stability and defining the limits of reaming. Excision of peripheral osteophytes is essential for accurate reaming and proper seating.
*
Acetabular Fossa:
The central, non-articular portion, often containing fat and the ligamentum teres. Reaming progresses from the fossa outwards to the periphery.
*
Teardrop (Köhler's Teardrop):
A radiographic landmark indicating the anterior inferior aspect of the acetabulum, providing a guide for reaming depth and medial wall integrity. Medialization during reaming should generally not transgress the teardrop.
*
Iliopectineal Line (Anterior Column):
Forms the anterior structural support.
*
Posterior Column:
Extends from the greater sciatic notch to the ischial tuberosity, forming the posterior structural support. Preservation is crucial.
*
Transverse Acetabular Ligament:
Bridges the inferior aspect of the acetabular notch. Its resection allows for deeper component seating and is often used as a guide for inferior acetabular reaming.
Acetabular Orientation and Safe Zones
Proper acetabular component orientation is critical to optimize implant longevity, minimize wear, and reduce the risk of dislocation.
*
Inclination:
The angle between the coronal plane and the opening of the acetabular cup. The generally accepted range is 40-45 degrees, though functional inclination can vary with patient posture.
*
Anteversion:
The angle between the transverse plane and the opening of the acetabular cup, measured relative to the sagittal plane or the anterior pelvic plane. The accepted range is typically 15-20 degrees.
*
Lewinnek's Safe Zone:
A widely referenced target for cup placement, defined by an inclination of 40 ± 10 degrees and anteversion of 15 ± 10 degrees. While a useful guide, it is recognized that dislocation risk can occur within these zones, and patient-specific factors (e.g., spinal alignment, pelvic tilt) must be considered.
*
Functional Acetabular Position:
Modern understanding emphasizes that static radiographic measurements may not fully reflect the dynamic functional orientation of the cup in various postures.
Biomechanics of Uncemented Fixation
The success of uncemented metal sockets hinges on achieving robust osseointegration. This process is dependent on two phases:
1.
Primary Mechanical Stability:
Achieved intraoperatively through a "press-fit" mechanism, often by under-reaming the acetabulum by 1-2 mm relative to the outer diameter of the acetabular shell. Macro-interlock features (e.g., fins, ribs, spikes) further enhance initial grip. Supplemental screw fixation is utilized if primary stability is deemed insufficient, particularly in cases of compromised bone quality or specific defect patterns. This initial stability minimizes micromotion at the bone-implant interface, which is critical; micromotion exceeding 50-150 µm can inhibit osteointegration and lead to fibrous tissue ingrowth.
2.
Secondary Biologic Fixation (Osseointegration):
The long-term stability is established through bone ingrowth into the porous surface of the implant. The porous architecture, typically made of titanium or tantalum, provides a scaffold for osteoblasts to deposit new bone. Hydroxyapatite (HA) coatings can accelerate and enhance this process by providing an osteoconductive surface. HA coatings, generally 50-100 µm thick, resorb over time as bone ingrowth occurs. Titanium plasma spray coatings provide surface roughness and porosity without resorption. The quality of host bone stock, patient biology, and absence of infection are critical for successful osseointegration.
Load transfer occurs via the shell to the host bone. Ideally, stress is uniformly distributed, minimizing stress shielding and its potential sequelae (e.g., periprosthetic bone loss).
Indications & Contraindications
The selection of an uncemented metal acetabular socket is based on a careful assessment of patient factors, bone quality, and pathology.
Operative Indications for Uncemented THA
- Primary Osteoarthritis: The most common indication.
- Inflammatory Arthritis (e.g., Rheumatoid Arthritis): Provided bone quality is adequate for primary stability.
- Avascular Necrosis (AVN) of the Femoral Head: Often seen in younger patients.
- Post-Traumatic Arthritis: Careful assessment of acetabular morphology and bone defects.
- Developmental Dysplasia of the Hip (DDH): With appropriate reconstruction techniques, including potential bone grafting.
- Revision Total Hip Arthroplasty: Uncemented components are frequently preferred due to the need to address bone loss and preserve host bone stock for future revisions.
- Younger, Active Patients: Generally favored due to the excellent long-term durability and potential for easier revision compared to cemented constructs.
- Good Bone Quality: Patients with Dorr Type A or B femoral canal (for femoral component selection, but correlates with overall bone health) and healthy acetabular bone stock are ideal candidates.
Contraindications for Uncemented THA
- Active Periprosthetic Joint Infection: Absolute contraindication.
- Skeletal Immaturity: Open physes.
- Severe Acetabular Bone Loss or Poor Bone Quality: Such as severe osteopenia, pathological fractures, or extensive defects where achieving adequate primary stability is unlikely. In these cases, a cemented component, a custom implant, or an acetabular cage may be more appropriate.
- Neuropathic Arthropathy (Charcot Joint): Relative contraindication due to high risk of loosening and early failure; cemented or constrained components may be considered.
- Significant Medical Comorbidities: Which preclude a prolonged, technically demanding procedure, although this is more a contraindication to THA in general rather than specifically uncemented.
- Known Allergy to Implant Materials: Rare but must be considered.
Summary of Operative vs. Non-Operative Indications
| Factor | Operative Indication (Uncemented THA) | Non-Operative Management (Initially) |
|---|---|---|
| Symptoms | Refractory, debilitating hip pain impacting quality of life despite adequate conservative management | Mild to moderate, intermittent pain, tolerable functional limitations |
| Radiographic Findings | Advanced joint space narrowing, significant osteophytes, subchondral sclerosis, cysts, AVN, DDH | Early arthritic changes, minimal deformity, absence of severe structural damage |
| Age & Activity Level | Younger, physiologically active patients desiring long-term durability | Any age, particularly if symptoms are manageable, or high surgical risk |
| Bone Quality | Adequate host bone stock for primary press-fit stability and subsequent osseointegration | Not directly applicable; however, very poor bone quality may preclude uncemented THA |
| Failure of | All appropriate non-operative modalities (e.g., NSAIDs, physical therapy, injections, activity modification) | Prior to extensive trials of non-operative treatments |
| Functional Impairment | Significant limitation in activities of daily living, sleep disturbance, inability to work | Acceptable functional status, minimal impact on daily activities |
| Co-morbidities | Medically optimized and fit for major surgical intervention | Significant unmanaged medical conditions increasing surgical risk |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is the cornerstone of a successful uncemented hip arthroplasty, particularly for acetabular component placement.
Pre-Operative Planning
- Clinical Assessment: Detailed history (pain characteristics, functional limitations, prior surgeries), physical examination (gait, range of motion, neurovascular status, leg length discrepancy, Trendelenburg sign).
-
Radiographic Evaluation:
- True Anteroposterior (AP) Pelvis: Standardized view (patient supine, feet internally rotated 15 degrees) to assess joint space, osteophytes, subchondral changes, femoral head migration, bone quality, and pelvic landmarks. Templating for acetabular component size and position is performed.
- Cross-table Lateral (or Frog-leg Lateral): To evaluate anterior/posterior acetabular defects and femoral head pathology.
- Full-length AP Femur: For femoral component templating, but also provides context for overall limb alignment.
-
Special Views/Imaging:
- CT Scan: Indicated for complex cases (e.g., severe dysplasia, previous trauma, significant bone loss, revision surgery) to precisely delineate anatomy, bone defects (e.g., Paprosky classification for acetabular defects), and quantify anteversion/inclination.
- MRI: Rarely needed for primary THA planning but can assess soft tissue pathology or early AVN.
-
Templating:
Digital templating is standard.
- Acetabular Side: Identify the true acetabular floor, teardrop, and bony columns. Estimate cup size, desired depth of reaming, and optimal position (inclination, anteversion). Pre-plan for potential bone grafting or supplementary fixation if defects are present. Ensure sufficient bone coverage of the proposed uncemented shell.
- Leg Length and Offset Restoration: Crucial for biomechanics and patient satisfaction. Templating aids in determining how component placement affects these parameters.
- Medical Optimization: Address any medical comorbidities (cardiac, pulmonary, renal, endocrine). Optimize nutrition, manage anemia, and ensure appropriate DVT prophylaxis and antibiotic protocols are in place. Review medications, especially anticoagulants.
Patient Positioning
The choice of patient positioning depends on the selected surgical approach and surgeon preference. Regardless of position, critical elements include:
*
Pelvic Stability:
The pelvis must be rigidly secured to prevent intraoperative rotation or tilt, which can lead to malpositioning of the acetabular component.
*
Access and Exposure:
Optimize surgical field visibility for acetabular preparation and component insertion.
*
Leg Mobility:
Ensure adequate mobility of the operative leg for dislocation, exposure, and reduction maneuvers.
-
Lateral Decubitus Position:
- Common for posterior and direct lateral approaches.
- Patient positioned on the non-operative side, secured with sacral and anterior iliac supports.
- Pillows between the legs.
- Ensures stability and allows for clear exposure of the posterior and superior acetabulum.
- Potential pitfall: Pelvic rotation if not adequately secured, leading to inaccurate cup anteversion.
-
Supine Position:
- Common for direct anterior and anterolateral approaches.
- Patient supine on the operating table, often with a bump under the operative hip for the anterolateral approach, or a specialized table for the direct anterior approach.
- Legs usually placed in stirrups or on a specific leg holder for the direct anterior approach.
- Facilitates intraoperative fluoroscopy for real-time assessment of component position and leg length.
- Potential pitfall: Limited access to the posterior acetabulum, requiring careful release of posterior structures.
Detailed Surgical Approach / Technique
While the specific surgical approach (e.g., posterior, direct anterior, anterolateral) dictates the initial soft tissue dissection, the core principles of acetabular preparation and uncemented socket insertion remain consistent.
Acetabular Exposure
- Capsulotomy/Capsulectomy: Adequate capsular release is critical for exposure and mobility.
- Osteophyte Removal: Circumferential removal of peripheral acetabular osteophytes is crucial. These can impede proper reaming, prevent concentric seating of the acetabular component, and obscure anatomical landmarks.
- Labral Excision: The acetabular labrum is typically excised to allow for full visualization and spherical reaming.
- Femoral Head Excision: After dislocation, the femoral neck is osteotomized (typically at the piriformis fossa level laterally, 1 fingerbreadth above the lesser trochanter medially) and the femoral head removed.
Acetabular Preparation
The goal is to create a hemispherical or near-hemispherical cavity that is concentric with the true acetabulum, ensuring a stable seat for the uncemented shell.
1.
Initial Reaming:
Begin with a small-diameter reamer to find the true acetabular floor. Progressively increase reamer size in 1-2 mm increments. Ream concentrically, aiming to preserve the posterior column.
2.
Medialization & Containment:
Ream only until bleeding cancellous bone is exposed, indicating a vascular bed for osseointegration. Avoid over-reaming, which can compromise the medial wall (leading to protrusion) or posterior column. The endpoint of reaming is often signaled by the exposure of the teardrop or the medialization of the reamer to the depth of the transverse acetabular ligament.
*

*

* These images likely depict the sequential reaming process, showing the progressively larger reamers shaping the acetabulum, aiming for a bleeding cancellous bone bed, and preserving the critical bony landmarks.
3.
Bone Grafting (if necessary):
For contained defects (e.g., cavitary defects), morselized autograft or allograft can be impacted to restore contour and support. Uncontained defects often require alternative strategies (e.g., augments, cages).
4.
Acetabular Wash:
Thoroughly irrigate the acetabulum to remove debris and expose the prepared bone surface.
Implant Selection & Insertion
- Shell Sizing: The final reamer size determines the inner diameter of the prepared acetabulum. For a press-fit uncemented shell, the chosen shell is typically 1-2 mm larger in outer diameter than the final reamer size (e.g., if reamed to 50mm, a 51mm or 52mm shell is inserted). This creates the necessary equatorial interference fit.
-
Component Orientation:
- Use an alignment guide (e.g., using the anterior superior iliac spines and pubic symphysis as references for the anterior pelvic plane) to achieve the desired inclination (40-45 degrees) and anteversion (15-20 degrees).
- Impact the shell firmly and steadily into the prepared acetabulum until fully seated. Listen for a change in tone of the impaction, indicating solid fixation.
-
 - This image likely shows the acetabular shell being impacted into the prepared socket, demonstrating the use of an impaction handle and proper alignment.
- Primary Stability Assessment: After impaction, manually test the stability of the shell. It should resist rotational and translational forces.
-
Supplementary Screw Fixation (if indicated):
If primary press-fit stability is deemed insufficient (e.g., in softer bone, large defects, or when using a screw-in design), supplemental screws are placed through pre-drilled holes in the shell.
- Safe Quadrants for Screw Placement: Screws should generally be placed in the posterior-superior quadrant (ilioischial bone) or the anterior-superior quadrant (iliopubic bone).
- Avoid: Inferior (obturator neurovascular bundle) and anterior-inferior (femoral neurovascular bundle, external iliac vessels) quadrants. Superior screws should be directed superiorly and posteriorly to engage the thickest bone while avoiding penetration into the pelvis.
- Screw Length: Critical to ensure bicortical purchase where appropriate, but avoid neurovascular structures. Intraoperative fluoroscopy can be invaluable for confirming screw trajectory and length, especially in revision cases or those with distorted anatomy.
-
 - This image could illustrate the placement of supplemental screws, potentially showing the drill holes or the screws themselves securing the acetabular shell.
-
Liner Insertion:
Once the metal shell is securely fixed, the bearing surface liner (e.g., highly cross-linked polyethylene, ceramic, metal) is inserted and locked into place using the implant-specific locking mechanism. Ensure proper seating and engagement of the locking mechanism.
-
 - This image might depict the insertion of the polyethylene or ceramic liner into the metal shell, or a trial reduction to confirm stability and range of motion.
-
- Trial Reduction & Final Reduction: If the femoral component has also been implanted, perform trial reductions to assess stability, range of motion, and leg length. Once satisfied, the definitive femoral head is impacted onto the taper, and the hip is reduced.
-
Closure: Layered closure with attention to soft tissue tension.
-
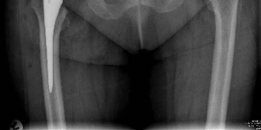 - This final image likely represents a post-operative radiograph of a successfully implanted uncemented acetabular component, demonstrating good position and fixation.
-
Complications & Management
Despite significant advancements, uncemented hip arthroplasty carries potential complications, both intra- and post-operatively. Recognition and appropriate management are crucial for optimal outcomes.
Intraoperative Complications
-
Acetabular Fracture:
- Incidence: 0.5-2%, higher in osteoporotic bone or complex revisions.
- Causes: Over-reaming, forceful impaction, stress risers from screw holes, pre-existing bone defects.
- Recognition: Audible crack, loss of press-fit, radiographic crack line.
-
Management:
- Minor (non-displaced): Smaller uncemented cup, supplementary screws/wires, or conversion to a cemented cup.
- Displaced: Open reduction and internal fixation with screws/plates, then a smaller uncemented cup or a cemented cup. Consideration of acetabular cages for extensive defects.
-
Neurovascular Injury:
- Incidence: Rare (<1%).
- Nerves: Sciatic (posterior), femoral (anterior), obturator (medial).
- Vessels: Femoral artery/vein, external iliac artery/vein, obturator artery/vein.
- Causes: Direct trauma during exposure, reaming, screw placement, or retraction.
- Management: Immediate recognition, neurovascular consultation for repair. Careful screw placement and avoidance of inferior/anterior-inferior quadrants for screws.
-
Malpositioning of Acetabular Component:
- Incidence: Variable, often related to surgical experience and patient factors.
- Causes: Inaccurate alignment guides, uncorrected pelvic tilt/rotation, surgeon error.
- Management: Immediate revision of component position if identified intraoperatively. Post-operative malpositioning leading to instability or impingement often requires revision.
Early Post-operative Complications
-
Dislocation:
- Incidence: 1-5%, depends on approach, patient factors, and component positioning. Uncemented components alone do not inherently increase dislocation risk.
- Causes: Component malposition, inadequate soft tissue tension, patient non-compliance with precautions, impingement.
- Management: Closed reduction, often followed by an abduction brace. Recurrent dislocations may require revision (liner exchange, component repositioning, dual mobility articulation, constrained liner).
-
Periprosthetic Joint Infection (PJI):
- Incidence: 0.5-2%.
- Causes: Intraoperative contamination, hematogenous spread.
- Diagnosis: Persistent pain, fever, elevated ESR/CRP, aspirate for cell count, culture, alpha-defensin.
- Management: Debridement, antibiotics, and implant retention (DAIR) for acute infections. Chronic infections often require two-stage exchange arthroplasty (excision of components, antibiotic spacer, reimplantation).
-
Leg Length Discrepancy (LLD):
- Incidence: Perceived LLD is common, true LLD can be 1-2 cm.
- Causes: Inaccurate templating, errors in component placement, failure to restore offset.
- Management: Shoe lift for minor discrepancies. Significant functional LLD may require revision.
-
Early Aseptic Loosening:
- Incidence: Rare with modern uncemented cups.
- Causes: Failure of primary stability leading to excessive micromotion, hindering osseointegration.
- Diagnosis: Persistent groin pain, radiographic evidence of migration or progressive radiolucent lines.
- Management: Revision arthroplasty.
Late Post-operative Complications
-
Aseptic Loosening of Acetabular Component:
- Incidence: Main long-term failure mode for uncemented components, often <1% at 5 years, 5-10% at 10-15 years for modern designs.
- Causes: Failure of osseointegration, late disengagement of porous coating, osteolysis from wear particles.
- Diagnosis: Progressive groin/buttock pain, radiographic signs (migration, progressive lucencies at implant-bone interface, broken screws).
- Management: Revision arthroplasty, often requiring cup exchange, bone grafting, augments, or cage constructs for significant bone loss.
-
Periprosthetic Osteolysis:
- Incidence: Varies with bearing surface and time.
- Causes: Inflammatory reaction to wear particles (polyethylene, ceramic, metal).
- Diagnosis: Radiographic lytic lesions around the implant, often asymptomatic until advanced.
- Management: Observation for small, non-progressive lesions. Larger or progressive lesions may require debridement, bone grafting, liner exchange, or full component revision.
-
Bearing Surface Wear/Failure:
- Incidence: Highly variable depending on bearing materials.
- Causes: Polyethylene wear, ceramic fracture, metal-on-metal wear (historical context).
- Management: Liner exchange, revision of affected components.
-
Heterotopic Ossification (HO):
- Incidence: Clinical significance 5-20%, radiographic up to 60%.
- Causes: Post-surgical inflammation and bone formation in soft tissues.
- Management: Prophylaxis with NSAIDs or single-dose radiation. Symptomatic HO (pain, restricted ROM) may require surgical excision after maturation.
Table of Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approx. %) | Salvage Strategies |
|---|---|---|
| Intraoperative | ||
| Acetabular Fracture | 0.5-2 | Smaller uncemented cup + screws/wires; conversion to cemented cup; ORIF + cup. |
| Neurovascular Injury | <0.1 | Immediate repair by neurovascular surgeon. |
| Malpositioning (Intra-op) | Variable | Immediate repositioning of cup. |
| Early Postoperative | ||
| Dislocation | 1-5 | Closed reduction, abduction brace. Recurrent: Liner exchange, component revision, dual mobility. |
| Periprosthetic Infection | 0.5-2 | DAIR (acute), one/two-stage exchange (chronic), Girdlestone. |
| Early Aseptic Loosening | <1 | Revision arthroplasty (cup exchange). |
| Leg Length Discrepancy | Common (perceived) | Shoe lift, physiotherapy. Severe: Revision. |
| Late Postoperative | ||
| Aseptic Loosening | 5-10 (at 10-15 yrs) | Revision arthroplasty: Cup exchange, bone grafting, augments, cages. |
| Periprosthetic Osteolysis | Varies with bearing | Observation, liner exchange, debridement/grafting, component revision. |
| Bearing Surface Wear/Failure | Variable | Liner exchange, head/liner exchange, or full component revision. |
| Heterotopic Ossification | 5-20 (clinical) | NSAID/radiation prophylaxis. Symptomatic: Excision after maturation. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following uncemented hip arthroplasty is critical for maximizing functional outcomes and minimizing complications. The primary goal for uncemented components is to allow for safe weight-bearing to promote osseointegration while protecting soft tissue repairs.
Immediate Post-Operative Period (Day 0 - Week 2)
- Pain Management: Multimodal analgesia including regional blocks, oral/IV pain medications.
- DVT Prophylaxis: Pharmacological (e.g., LMWH, DOACs) and mechanical (e.g., compression stockings, SCDs).
-
Mobilization:
- Weight-Bearing: Typically full weight-bearing as tolerated (FWBAT) for stable uncemented acetabular and femoral components. This encourages bone ingrowth. For more complex cases (e.g., significant bone defects, revision with grafting), protected weight-bearing (e.g., touch-down weight-bearing, partial weight-bearing) may be prescribed initially.
- Early Ambulation: Begin standing and walking with an assistive device (walker, crutches) on post-operative day 0 or 1.
-
Exercises:
- Ankle pumps, quadriceps sets, gluteal sets to maintain muscle tone and circulation.
- Gentle active and passive range of motion (ROM) exercises within comfortable limits, respecting surgical precautions.
-
Precautions:
- Posterior Approach: Avoid hip flexion > 90 degrees, adduction past midline, and internal rotation.
- Direct Anterior Approach: Avoid hip extension past neutral, external rotation, and combined extension/adduction.
- Anterolateral Approach: Generally fewer restrictions than posterior, but typically avoid extremes of extension and external rotation.
- Patient Education: Reinforce precautions, transfer techniques, and signs of complications (infection, DVT).
Phase I: Early Recovery (Weeks 2 - 6)
- Goals: Reduce pain and swelling, restore basic ambulation independence, improve hip ROM and strength.
- Weight-Bearing: Continue FWBAT unless specified. Progress from walker to crutches, then a single cane.
-
Exercises:
- Progressive strengthening exercises for hip abductors, extensors, and core musculature (e.g., straight leg raises, hip abduction/adduction in supine, bridging).
- Continue ROM exercises, aiming for functional ranges.
- Initiate stationary cycling (low resistance) and aquatic therapy if available.
- Gait Training: Focus on normal gait mechanics, equal weight distribution, and reducing reliance on assistive devices.
Phase II: Intermediate Recovery (Weeks 6 - 12)
- Goals: Full independence with ambulation, improved strength, balance, and endurance.
- Weight-Bearing: Discontinue assistive devices as strength and balance allow.
-
Exercises:
- Advance strengthening exercises: light resistance bands, bodyweight squats, lunges.
- Balance and proprioception training.
- Continue low-impact cardiovascular activities (walking, cycling, swimming).
- Stair climbing training.
- Activity Modification: Avoid high-impact activities (running, jumping) for the lifetime of the implant. Return to light recreational activities (golf, doubles tennis) as tolerated and cleared by the surgeon.
Phase III: Advanced Recovery (Months 3 - 6+)
- Goals: Return to most desired functional activities, maximal strength and endurance.
-
Exercises:
- Higher-level strengthening, plyometrics (if appropriate for patient age/activity level, with caution), sport-specific training.
- Maintain flexibility and strength through a home exercise program.
- Long-term Monitoring: Regular clinical and radiographic follow-up (e.g., at 1 year, then every 3-5 years) to monitor implant integrity, bone remodeling, and identify potential issues like osteolysis or loosening.
Summary of Key Literature / Guidelines
The landscape of uncemented hip arthroplasty has been shaped by extensive research, registry data, and professional guidelines.
Long-term Outcomes and Registry Data
National and international joint registries (e.g., National Joint Registry for England and Wales, Swedish Hip Arthroplasty Register, Australian Orthopaedic Association National Joint Replacement Registry) provide invaluable insights into implant survival and trends. These registries consistently report excellent long-term survival rates for modern uncemented acetabular components, often exceeding 90-95% at 10-15 years, with some designs showing survival beyond 20 years. This robust data supports the widespread adoption of uncemented cups, particularly in younger patients. Failure modes typically involve aseptic loosening, osteolysis, or polyethylene wear.
Comparison to Cemented Components
For decades, cemented THA was the gold standard. However, uncemented technology has proven superior in certain patient populations:
*
Younger Patients:
Uncemented components are generally favored due to their potential for lifelong durability through osseointegration, preserving bone stock for potential future revisions, and avoiding issues associated with cement mantle fatigue.
*
Older Patients/Poor Bone Quality:
Cemented fixation remains a viable, and often preferred, option in elderly patients with poor bone quality (e.g., severe osteoporosis) where achieving adequate primary press-fit stability for an uncemented cup is challenging. Cemented fixation offers immediate, predictable mechanical stability independent of bone ingrowth.
*
Bone Preservation:
Uncemented implants, particularly on the acetabular side, are thought to preserve more host bone compared to cemented options, which can be advantageous in revision scenarios.
Bearing Surfaces and Wear
The evolution of bearing surfaces has profoundly impacted the longevity of uncemented THA.
*
Conventional Polyethylene:
Prone to wear and subsequent osteolysis.
*
Highly Cross-Linked Polyethylene (XLPE):
Introduced to reduce wear and osteolysis, XLPE has shown superior wear characteristics in vivo, becoming the standard for polyethylene liners.
*
Ceramic-on-Ceramic (CoC):
Offers extremely low wear rates but carries risks of ceramic fracture and squeaking.
*
Ceramic-on-Polyethylene (CoP):
Combines the advantages of a hard ceramic femoral head with the low wear of XLPE.
*
Metal-on-Metal (MoM):
Historically used, but largely abandoned due to concerns over pseudotumor formation, metallosis, and adverse local tissue reactions related to metal ion release.
Design Principles
Modern uncemented acetabular shells incorporate key design features:
*
Porous Coatings:
Titanium plasma spray and/or hydroxyapatite (HA) coatings promote bone ingrowth. HA coatings can accelerate initial bone ingrowth.
*
Macro-interlock Features:
Fins, spikes, or screws provide enhanced primary stability.
*
Hemispherical Shape:
Most common design, aiming for a concentric fit with the reamed acetabulum.
*
Modularity:
Allows for independent selection of shell and liner to optimize bearing surfaces and address specific patient needs.
Professional Guidelines
Organizations such as the American Academy of Orthopaedic Surgeons (AAOS) and the American Association of Hip and Knee Surgeons (AAHKS) regularly publish clinical practice guidelines relevant to THA. These cover various aspects, including:
*
Antibiotic Prophylaxis:
Standardized protocols to reduce the risk of periprosthetic joint infection.
*
Thromboprophylaxis:
Guidelines for prevention of venous thromboembolism (VTE).
*
Post-operative Pain Management:
Recommendations for multimodal pain control strategies.
*
Preoperative Planning and Optimization:
Emphasis on patient selection, medical optimization, and informed consent.
In conclusion, achieving success with uncemented hip arthroplasty metal sockets requires meticulous pre-operative planning, precise surgical technique, appropriate component selection, and adherence to evidence-based post-operative protocols. The robust long-term outcomes and ongoing advancements cement its position as a highly effective treatment for end-stage hip pathology in suitable patients.
Clinical & Radiographic Imaging

You Might Also Like


