Advanced Ceramic THA: Vitamin E Enhanced for Complex Acetabulum Case

Key Takeaway
For anyone wondering about Advanced Ceramic THA: Vitamin E Enhanced for Complex Acetabulum Case, This 69-year-old male case highlights uncemented total hip arthroplasty for severe right hip osteoarthritis. Due to extensive erosions and poor acetabular bone stock, impaction autografting using the patient’s femoral head was crucial. This procedure, a significant **case title ceramic** consideration in orthopedic surgery, achieved stable implant fixation and improved hip mechanics, resolving pain and inability to walk.
Advanced Ceramic THA: Vitamin E Enhanced for Complex Acetabulum Case
Introduction
We present a challenging case of a 48-year-old active male presenting with end-stage post-traumatic osteoarthritis of the left hip, a sequela of a complex acetabular fracture. This case necessitated a total hip arthroplasty (THA) with particular attention to acetabular reconstruction and the selection of advanced bearing surfaces – specifically, a ceramic femoral head articulating with a Vitamin E enhanced polyethylene (VEXPE) liner – given the patient's age, activity level, and the inherent complexities of the post-traumatic anatomy.
Patient Presentation & History
The patient is a 48-year-old male, a previously active non-smoker with a healthy body mass index of 26 kg/m². He presented to our trauma clinic with a five-year history of progressive, debilitating left hip pain, significantly limiting his functional capacity.
His original injury occurred five years prior in a high-energy motor vehicle collision, resulting in a complex left acetabular fracture involving the posterior column and posterior wall, compounded by a central dislocation of the femoral head. Due to a combination of factors including initial patient comorbidities (unrelated to the current presentation) and the complex nature of the fracture requiring specialized expertise, the fracture was initially managed conservatively at an outside institution. This non-operative approach ultimately led to significant malunion of the acetabulum, severe articular incongruity, and advanced post-traumatic osteoarthritis.
Over the subsequent five years, the patient experienced escalating left hip pain, which he described as deep, aching, and mechanical in nature, exacerbated by weight-bearing and activity. He reported a noticeable limp and a progressive reduction in his ability to participate in recreational activities, particularly cycling, which he previously enjoyed regularly. Prior conservative management, including a structured physiotherapy program, non-steroidal anti-inflammatory drugs (NSAIDs), and intra-articular corticosteroid injections, failed to provide more than transient relief.
Review of systems was unremarkable, with no constitutional symptoms or signs suggestive of inflammatory arthropathy. His past medical history was otherwise benign, limited to an appendectomy in his youth. There was no history of diabetes, hypertension, or osteopenia. He reported no current medication use other than occasional over-the-counter analgesics. Socially, he was employed in an office-based role, which he was increasingly finding difficult due to prolonged sitting and standing discomfort. He lived independently.
Clinical Examination
Upon initial inspection, the patient presented with an antalgic gait pattern, favoring his left lower extremity. He exhibited a fixed external rotation deformity of the left hip, approximately 20 degrees, and a visually apparent leg length discrepancy with shortening of the left limb. Notable atrophy of the left gluteal musculature was observed, consistent with disuse and chronic pain. No surgical scars were present from prior acetabular fixation, confirming the history of non-operative management of the fracture. However, some subtle contour asymmetry of the posterior buttock was noted, potentially related to the initial fracture displacement.
Palpation revealed generalized tenderness around the left greater trochanter and occasionally referred pain to the groin, indicative of the underlying joint pathology. There were no palpable masses, effusions, or signs of acute inflammation. The neurovascular status of the left lower extremity was assessed and found to be intact distally, with symmetric and palpable femoral, popliteal, dorsalis pedis, and posterior tibial pulses. Capillary refill was brisk, and sensation was normal throughout all dermatomes.
Passive and active range of motion (ROM) of the left hip were grossly restricted and elicited significant pain. Flexion was limited to 70 degrees, with severe end-range discomfort. Abduction was severely restricted to 10 degrees, and adduction across the midline was painful and limited. A fixed flexion deformity of approximately 15 degrees was identified, in addition to the fixed external rotation. Internal rotation was virtually absent, further supporting a diagnosis of advanced arthritis.
Neurological assessment confirmed no focal motor or sensory deficits. Strength testing revealed weakness in hip abduction (3/5) and extension (4/5), contributing to a positive Trendelenburg sign on the left. True leg length measurement, from the anterior superior iliac spine (ASIS) to the medial malleolus, revealed a 1.5 cm shortening of the left lower extremity, while apparent leg length discrepancy was approximately 2.5 cm.
Imaging & Diagnostics
Radiographs
Initial diagnostic imaging included a standard series of radiographs: an anteroposterior (AP) view of the pelvis and Judet views (iliac oblique and obturator oblique views) of the left hip. These revealed severe, concentric joint space narrowing of the left hip. Extensive osteophyte formation was evident around the femoral head and acetabular rim, particularly along the posterior and superior aspects. Subchondral sclerosis and cystic changes were noted in both the acetabulum and femoral head.
Crucially, the radiographs demonstrated significant acetabular deformity consistent with the previous posterior column and wall fracture. Evidence of malunion was present, with irregular bone remodeling. There was superior and medial migration of the femoral head, with components of protrusio acetabuli, indicating substantial medial wall compromise. Heterotopic ossification (HO) was visible around the joint, classified as Brooker Grade II-III, which likely contributed to the severely restricted range of motion. The femoral head itself exhibited signs of secondary deformation and flattening.
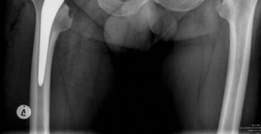
Figure 1: Pre-operative AP Pelvis radiograph demonstrating severe post-traumatic osteoarthritis of the left hip with joint space narrowing, extensive osteophytosis, and superior-medial migration of the femoral head, indicative of significant acetabular bone loss and deformity.
Computed Tomography (CT) Scan with 3D Reconstruction
Given the complexity of the acetabular deformity observed on plain radiographs, a computed tomography (CT) scan with 3D reconstructions of the pelvis and left hip was imperative for detailed pre-operative planning. The CT scan provided a precise assessment of the extent and location of acetabular bone loss, confirming significant deficiency of the medial wall, superior dome, and posterior column. The 3D reconstructions were invaluable in visualizing the three-dimensional architecture of the malunion and identifying areas of sclerotic, non-viable bone versus healthy cancellous bone stock.
The scan quantified the degree of protrusio acetabuli and precisely mapped the altered hip center of rotation. It also allowed for accurate measurement of the true femoral offset and leg length discrepancy, which are critical parameters for restoring optimal biomechanics during THA. The presence and extent of heterotopic ossification were clearly delineated, aiding in the surgical approach and planning for potential resections. This detailed information was crucial for templating the appropriate acetabular component size, type (e.g., standard hemispheric vs. extended rim), and potential need for bone grafting or modular augments.

Figure 2: Pre-operative 3D CT reconstruction of the left acetabulum, highlighting the complex post-traumatic deformity with significant bone loss in the superior-posterior dome and medial wall, consistent with a Paprosky Type IIIB defect. This imaging was crucial for surgical planning.
Templating
Digital templating was meticulously performed using the CT data. This process allowed us to:
* Accurately predict the size and position of the acetabular cup to restore the anatomical hip center, optimize coverage, and maximize host bone contact.
* Select the appropriate femoral stem size and offset to match the patient's anatomy and restore leg length.
* Anticipate the requirement for supplemental fixation, such as acetabular screws, and identify safe zones for their placement.
* Plan for the management of the bone defect, considering options like structural allografting or modular augments to support the acetabular component.
* Pre-plan the reaming trajectory and assess potential risks of pelvic perforation given the protrusio and medial wall thinning.
Differential Diagnosis
The comprehensive evaluation pointed strongly towards end-stage post-traumatic osteoarthritis. However, in the context of hip pain and deformity, other conditions were considered in the differential diagnosis:
| Feature | Post-traumatic Osteoarthritis (PTOA) (Primary Dx) | Primary Osteoarthritis | Avascular Necrosis (AVN) of the Femoral Head | Inflammatory Arthropathy (e.g., RA) |
|---|---|---|---|---|
| Etiology | Direct consequence of specific high-energy trauma (acetabular fracture) | Idiopathic, multifactorial, age-related | Trauma (e.g., dislocation, fracture), steroid use, alcoholism, systemic diseases | Autoimmune disorder, systemic inflammation, genetic predisposition |
| History | Clear antecedent high-energy trauma to the hip 5 years prior | Insidious onset, often without clear inciting event | History of femoral head injury or risk factors (steroids, alcohol) | Often polyarticular symptoms, constitutional symptoms (fatigue, fever) |
| Pain Pattern | Progressive, mechanical pain, directly correlates with activity and weight-bearing | Similar mechanical pain, but often slower onset and progression | Groin pain, initially intermittent, can progress to constant with collapse | Symmetrical polyarticular pain, morning stiffness > 30 min, improves with activity |
| Physical Exam | Antalgic gait, severe ROM restriction, fixed deformities, LLD, gluteal atrophy, previous fracture sequelae | Restricted ROM, often less severe LLD/deformity than PTOA initially | Restricted ROM, particularly internal rotation; often painful arc | Polyarticular synovitis, tender and swollen joints, systemic signs (e.g., nodules) |
| Radiographs | Asymmetric joint space narrowing, extensive osteophytes, subchondral sclerosis/cysts, clear evidence of malunited acetabular fracture (deformity, HO, incongruity) | Superior/superolateral joint space narrowing, osteophytes, subchondral cysts; generally more concentric in advanced stages, no fracture history | Early: often normal. Later: subchondral lucency (crescent sign), collapse of femoral head, secondary degenerative changes | Concentric joint space narrowing, marginal erosions, diffuse osteopenia, protrusio acetabuli (often bilateral) |
| CT/MRI Findings | CT shows precise extent of bone loss, malunion, HO, articular incongruity; MRI (if done) confirms cartilage loss | Cartilage loss, subchondral cysts, osteophytes, well-preserved bone architecture | MRI is highly sensitive for early AVN (double-line sign); later stages show collapse and secondary OA | Synovitis, bone erosions, pannus formation, cartilage destruction, often diffuse bone loss |
| Lab Markers | Typically normal inflammatory markers (ESR, CRP) | Typically normal inflammatory markers | May have underlying risk factors identified (e.g., hypercoagulable states, lipid abnormalities) | Elevated ESR/CRP, positive Rheumatoid Factor (RF), anti-CCP antibodies |
| Management Principle | Surgical reconstruction (THA) to address severe pain and structural failure caused by prior trauma | Surgical reconstruction (THA) for relief of pain and restoration of function | Early: core decompression, osteotomy. Late: THA due to femoral head collapse and secondary arthritis | Medical management with DMARDs, biologics; THA for end-stage joint destruction |
Surgical Decision Making & Classification
The decision for operative intervention was straightforward due to the patient's severe, unrelenting pain, profound functional impairment, and the failure of all conservative measures. Radiographic and CT evidence confirmed end-stage post-traumatic osteoarthritis with significant structural degradation of the acetabulum, making reconstructive osteotomy or other joint-preserving procedures unfeasible. The patient’s desire to return to an active lifestyle further supported the need for a definitive surgical solution.
Acetabular Bone Defect Classification
Based on the detailed CT imaging, the acetabular defect in this patient was classified using established systems:
- Paprosky Classification of Acetabular Bone Defects: This case presented with features consistent with a Paprosky Type IIIB defect. This classification is characterized by a cavitary defect involving the superior and medial walls, often with severe superior migration of the femoral head, significant bone loss, and compromise of the medial wall integrity. The presence of a substantial superior defect and medial protrusio indicated that a standard hemispheric cup would not achieve adequate coverage or stability without significant reconstruction.
- AAOS Classification of Acetabular Bone Defects: The extensive nature of the bone loss, involving elements of both the superior dome and medial wall, would place this defect into a Combined Defect (Type B) category, indicating a need for comprehensive reconstruction.
Rationale for THA with Advanced Bearings
The selection of a ceramic-on-Vitamin E enhanced polyethylene (VEXPE) bearing couple was a critical decision driven by several factors:
- Patient Demographics and Activity Level: At 48 years old, the patient is relatively young with a high demand for long-term implant survivorship. His active pre-injury lifestyle and desire to return to activities like cycling mandate a bearing surface with maximal wear resistance to mitigate the risk of revision surgery due to osteolysis and aseptic loosening, particularly relevant over a projected long lifespan.
- Complex Acetabular Reconstruction: The inherent challenges in achieving optimal acetabular cup position and stability in a severely deformed and reconstructed acetabulum mean that biomechanics may not be perfectly restored, potentially leading to increased contact stresses or edge loading. An extremely durable bearing can better withstand these potentially suboptimal conditions.
-
Specific Advantages of Ceramic-on-VEXPE:
- Ceramic Femoral Head: Modern third and fourth-generation ceramic materials (e.g., BIOLOX Delta) possess exceptional hardness, polish, and wettability, resulting in an ultra-low coefficient of friction when articulating with polyethylene. This significantly reduces wear particle generation compared to metal-on-polyethylene. While ceramic fracture remains a rare concern, its incidence has drastically decreased with advancements in material science. The scratch resistance of ceramic is also a notable advantage, preventing adverse wear patterns.
- Vitamin E Enhanced Polyethylene (VEXPE): Highly cross-linked polyethylene (HXLPE) has dramatically reduced wear rates compared to conventional UHMWPE. However, the cross-linking process involves irradiation, which generates free radicals that can lead to oxidative degradation and embrittlement of the polymer over time. Vitamin E (alpha-tocopherol) is a potent antioxidant incorporated directly into the polyethylene matrix during its manufacturing. It acts as a sacrificial free-radical scavenger, preventing oxidative damage without compromising the mechanical properties or cross-link density of the HXLPE. This significantly improves the long-term oxidative stability and mechanical integrity of the liner, offering the best of both worlds: the low wear rates of HXLPE combined with enhanced durability and resistance to long-term embrittlement. For a young, active patient with a high life expectancy, this combination offers the most robust solution for implant longevity.
Surgical Technique / Intervention
The surgical procedure was performed under general anesthesia with close monitoring of somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs) due to the proximity of the sciatic nerve in such a complex post-traumatic setting.
Patient Positioning and Approach
The patient was positioned in the left lateral decubitus position on a standard operating table, ensuring careful padding of all pressure points. The left hip was prepared and draped in the usual sterile fashion to allow extensive exposure to the posterior pelvis and proximal femur.
A standard posterior approach (Kocher-Langenbeck) was utilized. This approach offers excellent visualization of the posterior acetabulum, vital for addressing the posterior bone loss and heterotopic ossification, as well as providing direct access to the sciatic nerve for protection.
Surgical Steps
- Incision and Dissection: A curvilinear incision was made centered over the greater trochanter. The fascia lata was incised, and the gluteus maximus fibers were split. Meticulous dissection was performed to identify and carefully release the short external rotators (piriformis, gemelli, obturator internus, quadratus femoris) from their femoral insertions. Tagging sutures were placed on these muscles for anatomical repair at the conclusion of the procedure. This exposed the posterior capsule.
- Capsulotomy and Dislocation: A circumferential capsulotomy was performed. Due to extensive osteophyte formation, severe joint incongruity, and heterotopic ossification, dislocation of the femoral head was challenging. This required careful use of osteotomes to free the head from the acetabulum and excise impeding HO.
- Femoral Neck Osteotomy: A precise femoral neck osteotomy was performed. The level of resection was guided by pre-operative templating to restore optimal leg length and femoral offset. The resected femoral head was reserved for potential autograft, though a structural allograft was primarily planned for the extensive acetabular defect.
-
Acetabular Preparation and Reconstruction (Critical Phase): This was the most complex part of the procedure.
- Debridement: Extensive debridement of all remaining articular cartilage, fibrous tissue, osteophytes, and heterotopic ossification was performed to expose healthy, bleeding host bone.
-
Reaming and Bone Loss Management:
Initial reaming commenced with small hemispheric reamers (e.g., 40mm) to establish the true acetabular cavity. Given the Paprosky Type IIIB defect, significant superior and medial bone loss was encountered.
- Medial Wall Deficiency/Protrusio: The medial wall was significantly thinned. Reaming in this area was performed with extreme caution, using depth gauges and fluoroscopy to prevent pelvic perforation. The goal was to create a stable, contained cavity for the cup.
- Superior-Posterior Deficiency: A large superior and posterior defect was evident. To reconstruct this, a pre-contoured structural femoral head allograft was utilized. This allograft was meticulously shaped to fill the superior-posterior defect, restoring the acetabular dome and providing a stable platform. The allograft was secured to the host pelvis with multiple cancellous screws, ensuring rigid fixation.
- Progressive reaming was then continued over the reconstructed bed and remaining host bone, aiming for a true hemispherical shape that achieved excellent contact with at least 50-70% of healthy, bleeding host bone. The final reaming size was chosen to provide a 1-2mm press-fit for the definitive cup.
- Trial acetabular components were inserted to confirm optimal position (45 degrees inclination, 15-20 degrees anteversion), coverage, and stability of the reconstruction.

Figure 3: Intraoperative image demonstrating acetabular preparation following debridement and reconstruction with a structural allograft (visible superiorly) to address the significant bone defect. Reaming is in progress to create a concentric cavity for the definitive cup. -
Definitive Acetabular Component Implantation:
- A 56mm uncemented, porous-coated hemispheric acetabular cup was selected and impacted firmly into the reconstructed acetabulum, achieving excellent press-fit stability.
- Three cancellous screws were strategically placed through the cup into healthy host bone (superior-anterior and posterior safe zones) to augment primary stability and rotational control.
- A 36mm inner diameter Vitamin E enhanced polyethylene (VEXPE) liner was then securely locked into the shell, ensuring its correct orientation.
- Femoral Preparation: The femoral canal was prepared using sequential reamers until cortical chatter indicated appropriate fit and fill. A trial femoral stem was inserted to assess fit, stability, and restoration of leg length and offset.
- Definitive Femoral Component Implantation: A size 12 uncemented, proximally porous-coated femoral stem was impacted into the femur. The taper was meticulously cleaned and a 36mm ceramic femoral head (short neck length) was carefully affixed to the stem taper.
- Reduction and Stability Assessment: The hip joint was reduced. A thorough assessment of hip stability was performed through a full range of motion, checking for impingement in flexion, extension, internal rotation, and external rotation. Leg length discrepancy was reassessed and found to be well-equalized.
- Closure: The short external rotators and posterior capsule were repaired primarily using strong sutures, reinforcing stability. The gluteus maximus fascia, subcutaneous layers, and skin were closed in layers. A suction drain was placed given the extensive dissection.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Period (Day 0-3)
- Pain Management: A multimodal analgesia regimen was initiated, combining a periarticular local anesthetic infiltration performed intraoperatively, scheduled acetaminophen, NSAIDs (if no contraindications), and judicious use of opioid analgesics as needed.
- DVT Prophylaxis: Mechanical prophylaxis with sequential compression devices (SCDs) was started immediately, supplemented by pharmacological prophylaxis (low molecular weight heparin) as per institutional guidelines.
- Mobility: Early mobilization was encouraged. The patient was made weight-bearing as tolerated (WBAT) with the assistance of a walker or crutches, given the excellent primary stability of the uncemented components and the secure allograft fixation.
- Physiotherapy: Initial physiotherapy focused on gentle active and passive range of motion exercises for the ankle and knee, isometric quadriceps and gluteal sets, and instruction on strict hip precautions (avoiding flexion beyond 90 degrees, adduction past midline, and internal rotation to minimize dislocation risk).
- Wound Care: The incision was dressed daily, and the suction drain was removed on post-operative day 2 once output was minimal.
Early Rehabilitation (Weeks 1-6)
- Weight-Bearing Progression: The patient gradually progressed from walker to crutches, with the goal of transitioning to a single cane by week 6.
- Strengthening: A progressive strengthening program was initiated, focusing on regaining strength in the hip abductors, extensors, and core musculature. This began with isometric exercises and advanced to isotonic, low-resistance exercises.
- Range of Motion: Active and passive ROM exercises continued, gradually increasing the arc within the established hip precautions.
- Gait Training: Intensive gait training was implemented to correct any residual antalgic pattern and promote a symmetrical, efficient gait.
Mid-Term Rehabilitation (Weeks 7-12)
- Assistive Device Weaning: The patient worked towards independent ambulation without an assistive device.
- Functional Training: Balance and proprioceptive exercises were incorporated. Low-impact functional activities such as stationary cycling and swimming were introduced.
- Resistance Training: Progressive resistance exercises using bands and light weights were advanced for all major hip muscle groups.
Late Rehabilitation (Months 3-6+)
- Return to Activity: The patient was gradually cleared to return to recreational activities, with strong emphasis on avoiding high-impact sports (e.g., running, jumping) to protect the implant from excessive stress. Activities such as road cycling, swimming, and golf were encouraged.
- Long-Term Monitoring: Regular clinical and radiographic follow-up was scheduled annually to monitor for signs of component loosening, polyethylene wear, osteolysis, or other complications.
- Patient Education: Continuous reinforcement of hip precautions and activity modification strategies was provided to maximize the longevity of the implant.

Figure 4: Post-operative AP Pelvis radiograph demonstrating a well-positioned uncemented acetabular component with screws, a ceramic femoral head, and an uncemented femoral stem, with restoration of the hip center of rotation, leg length, and offset.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- Comprehensive Pre-operative Planning: For complex acetabular deformities, meticulous pre-operative planning using plain radiographs (AP pelvis, Judet views) and, critically, a CT scan with 3D reconstructions is non-negotiable. This allows for precise classification of bone defects (e.g., Paprosky Type IIIB), templating of component sizes, and anticipation of reconstructive needs (allografts, augments). Understanding the true anatomy of the defect prevents intraoperative surprises.
- Restoration of Hip Center of Rotation: This is paramount for optimizing hip biomechanics, restoring the abductor lever arm, equalizing leg lengths, and minimizing stresses on the implant. Utilize the acetabular reconstruction to achieve this, even if it means placing the cup slightly superior or lateral to the native, deformed hip center.
- Rigid Acetabular Reconstruction: When addressing significant bone loss, aim for maximum host bone contact (at least 50-70%) for the uncemented cup. Do not hesitate to use structural allografts or modular augments to reconstruct large contained or segmental defects, providing a stable platform for cup integration. Augment initial stability with strategically placed screws into healthy host bone, especially in reconstructed areas.
- Ceramic-on-VEXPE for Young, Active Patients: This bearing couple offers the highest wear resistance and oxidative stability currently available. Understanding the specific benefits of Vitamin E incorporation (antioxidant properties, preventing long-term embrittlement) is key to advocating for its use in young, high-demand patients where implant longevity is critical.
- Posterior Approach for Post-Traumatic Acetabula: This approach provides excellent visualization of the posterior column and wall, allowing for thorough debridement of heterotopic ossification, removal of impeding osteophytes, and direct access to the sciatic nerve for protection. Its extensile nature is advantageous in complex cases.
- Meticulous Soft Tissue Management: Careful dissection, release, and repair of the short external rotators and posterior capsule are essential for both nerve protection and post-operative stability.
- Trial Reduction and Stability Assessment: Always perform comprehensive trial reductions. Assess stability throughout the full range of motion (flexion, extension, internal, external rotation) to confirm no impingement, subluxation, or dislocation. Adjust neck length or component position as needed to achieve optimal stability and leg length equalization.
- Sciatic Nerve Protection: In post-traumatic cases, the sciatic nerve can be scarred, tethered, or at increased risk of injury due to limb lengthening or extensive dissection. Intraoperative neurological monitoring (SSEPs/MEPs) can be a valuable adjunct.
Pitfalls
- Underestimation of Bone Loss: Failure to accurately quantify acetabular bone loss pre-operatively can lead to undersizing of the cup, inadequate coverage, poor primary stability, and increased risk of early aseptic loosening or pelvic perforation.
- Pelvic Perforation: Aggressive or uncontrolled reaming, particularly in cases of medial wall deficiency or protrusio, can result in iatrogenic pelvic perforation, potentially causing significant hemorrhage, vascular injury, or visceral damage. Utilize incremental reaming, palpation, and intraoperative fluoroscopy cautiously.
- Sciatic Nerve Injury: This is a significant complication, especially in revision or post-traumatic THA via a posterior approach. Factors contributing to injury include direct trauma during dissection, thermal injury, compression, or excessive limb lengthening (more than 4cm). Careful dissection, identification of the nerve, and avoidance of excessive lengthening are crucial.
- Dislocation: The risk of post-operative dislocation is higher in complex cases due to altered anatomy, soft tissue imbalances, or suboptimal component positioning. Inadequate soft tissue repair, improper cup anteversion/inclination, or failure to restore adequate offset can all contribute.
- Heterotopic Ossification (HO): Post-traumatic THA patients are at high risk for severe HO. Failure to provide prophylaxis (e.g., NSAIDs like indomethacin or targeted radiation therapy) can lead to severe ROM restriction and pain.
- Component Impingement: Incorrect component placement (e.g., excessive cup anteversion or retroversion, long neck length, or residual osteophytes) can lead to impingement between the femoral neck and the acetabular rim or the liner. This causes pain, limits ROM, and increases the risk of dislocation and accelerated liner wear.
- Aseptic Loosening: Poor primary stability, inadequate bone stock for osseointegration, or suboptimal biological response can lead to early aseptic loosening of uncemented components. This underscores the need for meticulous bone preparation and fixation.
- Ceramic Fracture: While rare with modern materials, handling errors (e.g., impact to the ceramic head during insertion or contamination of the taper) can weaken the ceramic, increasing the risk of fracture. Strict adherence to manufacturer guidelines for ceramic handling is paramount.
Clinical & Radiographic Imaging
You Might Also Like

