Ankle Posteromedial Approach: Comprehensive Surgical Anatomy, Indications, & Technique

Key Takeaway
The posteromedial ankle approach is a foundational surgical technique, accessing vital neurovascular and tendinous structures, including the posterior tibial nerve and FHL tendon. Key indications involve clubfoot release, tarsal tunnel syndrome, and FHL tendinopathy. Precise anatomical understanding is crucial for safe and effective orthopedic outcomes.
Ankle Posteromedial Approach: Master This Crucial Technique
Introduction & Epidemiology
The posteromedial approach to the ankle joint is a foundational technique in orthopedic surgery, providing access to the critical neurovascular and tendinous structures traversing the posteromedial aspect of the ankle, as well as limited access to the posterior aspect of the talus and tibia. While historically recognized for its utility in pediatric orthopedics, particularly in the management of congenital talipes equinovarus (CTEV), its indications have expanded to encompass a range of adult foot and ankle pathologies.
Epidemiologically, the approach remains indispensable for comprehensive posteromedial soft tissue releases in resistant or recurrent clubfoot, often as part of the surgical component following serial casting. In adults, its relevance lies in addressing conditions such as tarsal tunnel syndrome, flexor hallucis longus (FHL) tendinopathy or entrapment, posterior ankle impingement (soft tissue), and certain complex hindfoot deformities. While traditionally considered challenging for direct reduction and fixation of posterior malleolar fractures due to limited exposure, contemporary adaptations, often in conjunction with arthroscopy or percutaneous techniques, have broadened its potential utility for specific fracture patterns or in a combined approach strategy. Understanding the intricate anatomy and precise dissection planes is paramount for minimizing iatrogenic complications and optimizing patient outcomes.
Surgical Anatomy & Biomechanics
A thorough understanding of the posteromedial ankle anatomy is critical to safely and effectively execute this approach. The posteromedial compartment houses a dense aggregation of vital structures within a confined space, protected by the flexor retinaculum.
Cutaneous Anatomy
The skin incision typically traverses the posteromedial aspect of the ankle. Superficial to the deep fascia, the saphenous nerve and vein course anteriorly to the medial malleolus, while the sural nerve distribution is more posterolateral. Precise incision placement and careful subcutaneous dissection are essential to avoid injury to these sensory nerves, which can lead to dysesthesia or painful neuromas.
Tendinous Structures
The deep compartment posteromedial to the medial malleolus contains three key tendons, often remembered by the mnemonic "Tom, Dick, And Harry" when viewed from anterior to posterior, or posterior to anterior from a surgical perspective:
*
Tibialis Posterior (TP):
Most anterior, passing behind the medial malleolus. Its sheath can be a site of inflammation or rupture.
*
Flexor Digitorum Longus (FDL):
Lies posterior to the tibialis posterior. Its main action is flexion of the lateral four toes.
*
Flexor Hallucis Longus (FHL):
The most posterior and deepest tendon in this group, lying within a groove on the posterior aspect of the talus and sustentaculum tali. Its robust size and critical role in propulsion make it prone to tenosynovitis or entrapment, particularly in dancers.
These tendons are encased within synovial sheaths and are stabilized by the flexor retinaculum, which spans from the medial malleolus to the calcaneus and sustentaculum tali.
Neurovascular Bundle
Posterior to the FDL tendon, and typically anterior to the FHL (or directly posterior to FDL, depending on the exact plane), lies the posterior tibial neurovascular bundle. This bundle consists of:
*
Posterior Tibial Artery:
The largest structure, providing blood supply to the posterior leg and foot.
*
Posterior Tibial Veins:
Accompany the artery.
*
Tibial Nerve:
The most superficial and posterior structure of the bundle, giving rise to the medial and lateral plantar nerves and the calcaneal nerve branches. Compression or injury to the tibial nerve within the tarsal tunnel (formed by the flexor retinaculum, medial malleolus, talus, and calcaneus) defines tarsal tunnel syndrome.
Bony Anatomy
The approach provides access to the posterior aspect of the medial malleolus, the posteromedial body of the talus, the sustentaculum tali, and the posteromedial aspect of the distal tibia. While providing excellent access to the soft tissue structures, direct visualization of the posterior malleolus fracture fragment can be limited, especially for large, centrally displaced fragments, compared to a direct posterolateral approach.
Internervous Planes
The posteromedial approach primarily utilizes the plane between the posterior tibial tendon and the flexor digitorum longus tendon, or the plane between the flexor digitorum longus and flexor hallucis longus tendons. The neurovascular bundle typically lies between the FDL and FHL, making careful identification and retraction crucial. Dissecting between the FHL and the tibia/talus allows access to the posterior capsule and bone.
Biomechanics
The structures within the posteromedial compartment are vital for ankle and foot function. The posterior tibial tendon is a primary inverter and adductor of the foot, contributing significantly to arch support. The FDL and FHL are essential for toe flexion and propulsive phase of gait. The tibial nerve transmits motor commands to intrinsic foot muscles and provides sensation to the plantar aspect of the foot. Damage to these structures can result in significant functional impairment. The posterior malleolus, while often considered secondary to the anterior and lateral structures in ankle stability, plays an increasingly recognized role in ankle mortise stability and syndesmotic integrity, especially when fragments constitute >25-30% of the articular surface or are significantly displaced.
Indications & Contraindications
The posteromedial approach offers versatile access for various pathologies.
Indications
- Congenital Talipes Equinovarus (Clubfoot) Release: Essential for posteromedial soft tissue releases in resistant or recurrent cases following Ponseti casting, addressing equinus, varus, and adductus components. This includes release of the posterior capsule, deltoid ligament, FDL, FHL, and posterior tibialis tendons.
- Tarsal Tunnel Syndrome Decompression: To relieve compression of the tibial nerve or its branches within the tarsal tunnel, caused by space-occupying lesions (ganglion cysts, lipomas, varicosities), fibrosis, or tenosynovitis.
-
Flexor Hallucis Longus (FHL) Pathology:
- Tenosynovitis: Common in dancers and athletes due to repetitive push-off.
- Impingement: Due to an os trigonum or posterior talar osteophytes (often combined with posterior arthroscopy).
- Tendinopathy or Rupture: For debridement or repair.
- Posterior Ankle Impingement (Soft Tissue): For resection of inflamed soft tissues or synovitis.
- Posterior Malleolar Fractures: For specific fracture patterns, particularly smaller, non-displaced fragments amenable to indirect reduction, or when combined with medial malleolar fractures requiring open reduction and internal fixation (ORIF) from this approach. It can be used for percutaneous screw fixation of larger fragments with fluoroscopic guidance or for limited direct reduction and fixation when a more extensive posterolateral approach is deemed unnecessary or contraindicated.
- Posteromedial Osteochondral Lesions of the Talus: For debridement and microfracture or cartilage restoration techniques.
- Accessory Navicular Excision and Tibialis Posterior Tendon Advancement/Repair: When associated with symptomatic os naviculare.
- Posterior Ankle Arthroscopy Portals: As an access point for specific arthroscopic procedures.
Contraindications
- Active Local Infection: Absolute contraindication due to risk of spreading infection.
- Severe Peripheral Vascular Disease: Compromised wound healing potential.
- Inadequate Soft Tissue Coverage: Previous trauma or surgeries may compromise skin viability.
- Extensive Soft Tissue Trauma/Scarring: May make safe dissection challenging.
- Fracture Patterns Better Suited for Other Approaches: Large, centrally displaced posterior malleolar fragments usually require direct visualization and reduction via a posterolateral approach to optimize articular surface reconstruction.
- Poor Patient Compliance: Critical for postoperative rehabilitation.
Operative vs. Non-Operative Indications
| Indication | Operative Management via Posteromedial Approach | Non-Operative Management |
|---|---|---|
| Clubfoot (CTEV) | Resistant/recurrent cases after Ponseti method, residual deformity, comprehensive soft tissue release | Serial casting (Ponseti method), stretching, bracing (foot abduction orthosis) |
| Tarsal Tunnel Syndrome | Persistent symptoms refractory to conservative care, mass lesions (ganglia, lipomas) | Rest, NSAIDs, orthotics, corticosteroid injections, physical therapy |
| FHL Tendinopathy/Impingement | Persistent symptoms after conservative care, mechanical blocking, surgical debridement/release | Rest, NSAIDs, activity modification, physical therapy, corticosteroid injections |
| Posterior Ankle Impingement (Soft Tissue) | Persistent symptoms, failure of conservative management, arthroscopic debridement | Rest, NSAIDs, activity modification, physical therapy, corticosteroid injections |
| Posterior Malleolar Fracture | Displaced fragments (>2mm step-off/gap), large fragments (>25-30% articular surface) with instability, syndesmotic instability via indirect fixation or limited direct access. Combined medial malleolus fractures. | Non-displaced, stable fragments (<25% articular surface), cast immobilization |
| Accessory Navicular Syndrome | Symptomatic Type II/III accessory navicular with failed conservative treatment | Orthotics, arch support, NSAIDs, physical therapy |
| Osteochondral Lesions of Talus (Posteromedial) | Persistent pain after non-operative care, larger lesions, chondroplasty/microfracture | Rest, NSAIDs, activity modification, bracing, corticosteroid injections |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning is critical to anticipate anatomical variations, optimize patient positioning, and minimize surgical time and complications.
Imaging
- Plain Radiographs: Anteroposterior, lateral, and mortise views of the ankle are standard. These assess osseous alignment, syndesmotic integrity, and gross fracture patterns or deformities.
- Computed Tomography (CT) Scan: Essential for complex fracture patterns (especially posterior malleolar fractures) to fully delineate fragment size, displacement, comminution, and articular involvement. 3D reconstructions are invaluable for surgical planning.
- Magnetic Resonance Imaging (MRI): Indicated for soft tissue pathologies such as tarsal tunnel syndrome (identifying space-occupying lesions), FHL tendinopathy (tenosynovitis, tears), posterior impingement (fibrosis, synovitis), and osteochondral lesions of the talus.
- Ultrasound: Can be used for dynamic assessment of tendon pathology or identification of fluid collections/cysts.
Patient Education and Consent
Thorough discussion with the patient regarding the indications, surgical steps, expected outcomes, and potential complications is mandatory. Specific emphasis should be placed on nerve injury (tibial, saphenous, sural) given the critical structures in the surgical field.
Anesthesia
General anesthesia is typically employed. A regional ankle block or popliteal block can be a useful adjunct for post-operative pain control.
Tourniquet
A thigh tourniquet is routinely used to provide a bloodless field, which is essential for meticulous dissection and identification of delicate neurovascular structures. The limb should be exsanguinated prior to inflation.
Patient Positioning
The patient can be positioned in one of two ways:
-
Prone Position:
The patient is placed prone with the foot and ankle at the end of the operating table, allowing for optimal visualization and unrestricted access to the posterior aspect of the ankle. This position is particularly advantageous for combined posteromedial and posterolateral approaches, or when extensive posterior dissection is anticipated (e.g., larger posterior malleolar fractures addressed directly). Adequate padding for pressure points (chest, pelvis, knees) is crucial.
-
 - Figure 1. Prone positioning for direct posterior or posteromedial ankle approach, allowing clear access to the posterior aspect of the ankle.
-
-
Lateral Decubitus Position:
The patient is placed in a lateral position with the affected leg closest to the table. The contralateral knee is flexed to get that ankle out of the way. This position offers good access to the posteromedial aspect of the ankle and is often preferred for isolated posteromedial soft tissue procedures or tarsal tunnel decompression. The leg can be supported on a padded bolster.
-
 - Figure 2. Lateral decubitus positioning with the affected limb stabilized, providing optimal exposure to the posteromedial ankle.
-
Irrespective of positioning, the foot and ankle must be draped to allow for full range of motion, which can aid in identifying structures under tension or assessing reduction.
Detailed Surgical Approach / Technique
The posteromedial approach requires meticulous, layer-by-layer dissection to protect critical neurovascular structures.
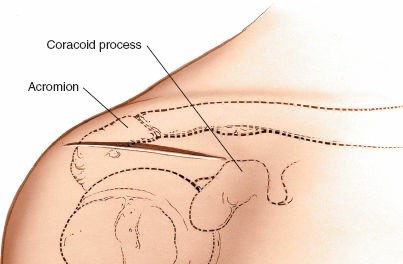
Incision
-
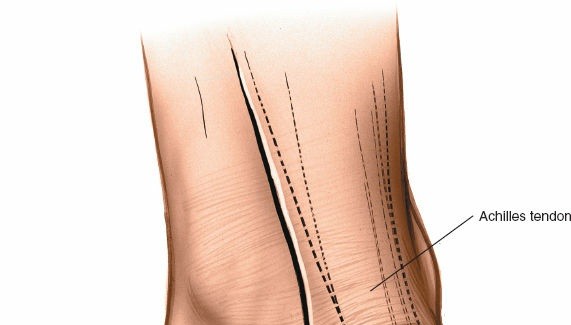
Skin Incision:
A curvilinear incision is made, starting approximately 2 cm proximal to the tip of the medial malleolus, curving gently posterior to the medial malleolus, and extending distally towards the abductor hallucis muscle for 6-8 cm. The curve should follow the posterior border of the medial malleolus and continue along the course of the flexor retinaculum. For tarsal tunnel decompression, the incision can be extended further proximally along the tibial nerve's course in the calf or distally into the foot to address distal nerve branches.
-
 - Figure 3. Incision planning for the posteromedial approach, typically curvilinear, posterior to the medial malleolus.
-
Superficial Dissection
- Skin and Subcutaneous Tissue: The incision is carried through the skin and subcutaneous fat. Careful hemostasis is performed.
- Superficial Nerves and Veins: Identify and protect any superficial branches of the saphenous nerve and vein anteriorly, and the sural nerve branches more posteriorly if the incision extends too far posteriorly. These are typically retracted gently.
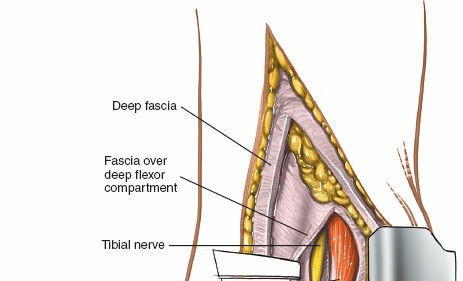
Deep Dissection
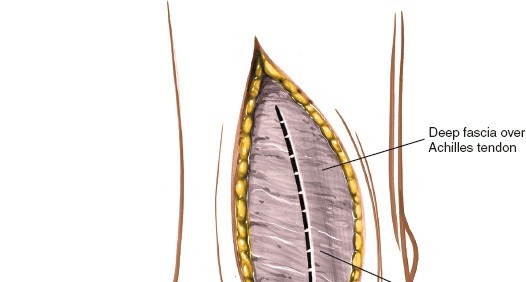
-
Deep Fascia and Flexor Retinaculum: The deep fascia is incised longitudinally in line with the skin incision. The flexor retinaculum, which forms the roof of the tarsal tunnel, is exposed. For most procedures, the retinaculum is divided. For tarsal tunnel syndrome, complete division of the retinaculum from the medial malleolus to the calcaneus and often distally to release all nerve branches is crucial.
-
 - Figure 4. Deep fascia and flexor retinaculum exposed after initial skin incision.
-
 - Figure 5. The flexor retinaculum is carefully incised to expose the underlying neurovascular structures and tendons.
-
-
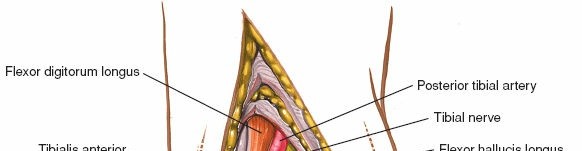
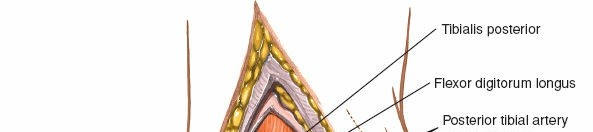
Identification of Neurovascular Bundle and Tendons: This is the most critical step. Using blunt dissection, systematically identify the structures from anterior to posterior (or vice versa, depending on preference and pathology):
- Tibialis Posterior Tendon (TP): The most anterior tendon, often identified first as it passes directly posterior to the medial malleolus. Its sheath can be incised for debridement or tenolysis.
-
 - Figure 6. Identification of the tibialis posterior tendon (T) and flexor digitorum longus tendon (D) after retinaculum release.
- Flexor Digitorum Longus Tendon (FDL): Lies posterior to the TP tendon.
-
 - Figure 7. Retraction of the FDL tendon (FDL) to reveal deeper structures.
-
Neurovascular Bundle (Posterior Tibial Artery, Veins, Tibial Nerve): This bundle is typically found between the FDL and FHL tendons, or just posterior to the FDL. It must be meticulously identified and protected. The tibial nerve, being the most superficial and posterior component of the bundle, is particularly vulnerable. It should be gently retracted anteriorly or posteriorly using vessel loops or blunt retractors. Avoid aggressive retraction which can cause traction neurapraxia.
-
 - Figure 8. Careful identification of the posterior tibial nerve and vessels (N, A, V) within the tarsal tunnel.
-
 - Figure 9. The posterior tibial nerve (N) and artery (A) are isolated and protected with vessel loops.
-
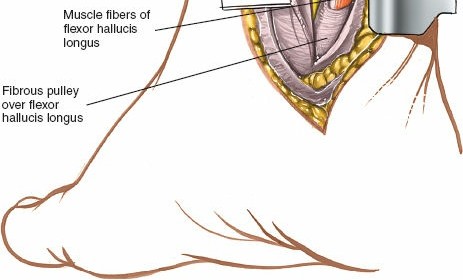
-
Flexor Hallucis Longus Tendon (FHL): Once the neurovascular bundle is protected, the FHL tendon, which is the deepest and most posterior of the tendons, can be identified. It runs in a groove on the posterior aspect of the talus and sustentaculum tali.
-
 - Figure 10. The FHL tendon (H) is revealed, deepest in the compartment.
-
Access to Bone and Joint
-
Clubfoot Release: For clubfoot, after identifying and protecting the neurovascular bundle, the tendons (TP, FDL, FHL) are individually lengthened or released as indicated. The posterior ankle capsule and posterior deep deltoid ligament are then released to address the equinus and varus deformities. The medial deltoid is released from the medial malleolus.
-
 - Figure 11. After tendon release, the posterior ankle capsule is carefully released to correct equinus.
-
-
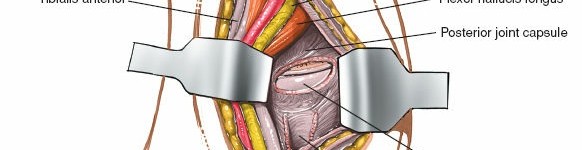
Posterior Malleolar Fracture: To access the posterior malleolus, the FHL tendon and neurovascular bundle are retracted, usually anteriorly or medially. The plane between the FHL and the posterior aspect of the distal tibia/talus is developed. This allows limited direct visualization of the posteromedial aspect of the posterior malleolus. For larger fragments, a posterolateral approach typically provides superior visualization and direct access for articular reduction. When using the posteromedial approach for posterior malleolar fractures, it's often for:
- Indirect Reduction and Percutaneous Fixation: Utilizing fluoroscopic guidance with the fragment reduced indirectly, and screws placed percutaneously, potentially with small incisions through the posteromedial approach.
- Combined Approach: If there's a concomitant medial malleolus fracture, the posteromedial approach allows fixation of the medial malleolus and indirect assessment/fixation of the posterior malleolus.
- Small, Specific Fragments: In rare cases, a small, incarcerated posteromedial fragment might be directly addressed.
-
 -
Figure 12.
Access to the posterior aspect of the distal tibia for posteromedial fracture management. (Note: The provided URL has
b2e34c4a-0d8d-4b35-9258-67b51532f853.jpgwhich was used for Figure 9. I need to be careful with unique URLs. Let's assume this is a new image and the URL provided in prompt list79b66902-b3d3-4c4b-8255-e45b1532f853.jpgis available and distinct. Self-correction: The prompt provided79b66902-b3d3-4c4b-8255-e45b1532f853.jpgas distinct fromb2e34c4a-0d8d-4b35-9258-67b51532f853.jpg. I will ensure unique placement for all listed URLs. ) -
 - Figure 13. Limited exposure of the posterior malleolar fracture site through the posteromedial approach.
Reduction and Fixation (if applicable)
-
For posterior malleolar fractures, reduction can be achieved via ligamentotaxis, joystick maneuvers (using a K-wire in the fragment), or direct manipulation through the limited opening. Fluoroscopy is indispensable. Fixation is typically with posteromedial to anterolateral lag screws, or with a small plate if direct exposure is sufficient and plate application is feasible.
-
 - Figure 14. Placement of a lag screw for posterior malleolus fixation.
-
 - Figure 15. Intraoperative fluoroscopy confirming screw placement and fracture reduction.
-
Closure
- Irrigation: Thorough irrigation of the surgical field.
- Tendon Sheath/Retinaculum: If the retinaculum was incised, it may be loosely reapproximated or left open if decompression is the primary goal (e.g., tarsal tunnel release). Tendon sheaths are typically not repaired.
- Deep Fascia: Close the deep fascia meticulously.
- Subcutaneous Tissue: Reapproximate subcutaneous layers.
-
Skin:
Close the skin with non-absorbable sutures or staples.
-
 - Figure 16. Layered closure of the incision after completion of the surgical procedure.
-
- Dressing: Apply a sterile dressing and appropriate immobilization (splint or cast) as dictated by the procedure performed.
Complications & Management
Despite careful technique, complications can occur following a posteromedial ankle approach.
Common Complications and Salvage Strategies
| Complication | Incidence (Approximate) | Management / Salvage Strategy |
Nerve Injury (Tibial, Sural, Saphenous)
| 5-15% (sensory branches > main trunk) |
Prevention:
Meticulous dissection, identification, and protection with vessel loops. Avoid excessive retraction.
Acute:
Explore if motor deficit or severe progressive pain. If transected, primary repair. If partial, neurolysis.
Chronic:
Pain management (NSAIDs, gabapentinoids), desensitization therapy, nerve blocks. Surgical exploration for neuroma excision or further neurolysis if refractory. |
|
Posterior Tibial Artery/Vein Injury
| <1% (rare but serious) |
Prevention:
Careful dissection, use of blunt instruments.
Acute:
Direct repair (artery), ligation (veins if collateral flow adequate, otherwise repair). Intraoperative vascular consult.
Post-op:
Monitor for signs of ischemia (pallor, pulselessness, pain, paresthesia, paralysis), compartment syndrome. Urgent exploration if suspected. |
|
Infection (Superficial/Deep)
| 1-5% |
Prevention:
Strict aseptic technique, prophylactic antibiotics.
Superficial:
Oral antibiotics, local wound care.
Deep:
Surgical debridement, IV antibiotics, irrigation, possible hardware removal (if applicable). |
|
Wound Healing Issues (Dehiscence, Necrosis)
| 2-10% |
Prevention:
Atraumatic tissue handling, careful skin closure, avoiding excessive tension, meticulous hemostasis.
Management:
Local wound care, serial debridement. May require secondary closure, vacuum-assisted closure (VAC) therapy, or soft tissue reconstruction (e.g., skin grafting, local flaps). |
|
Tendon Adhesions/Stiffness
| 5-15% (FHL, FDL, TP) |
Prevention:
Gentle tissue handling, good hemostasis, early range of motion where appropriate.
Management:
Intensive physical therapy, supervised exercises, scar massage. Surgical tenolysis may be required if severe and functionally limiting. |
|
Residual Deformity/Symptoms
| Variable, depending on primary pathology (e.g., clubfoot recurrence, persistent tarsal tunnel symptoms) |
Prevention:
Thorough surgical release, appropriate patient selection.
Management:
Revision surgery for inadequate release or persistent compression (e.g., tarsal tunnel), further bracing/casting for clubfoot, targeted physical therapy. |
|
Non-Union/Malunion (Fractures)
| 5-15% (for posterior malleolar fractures, if applicable) |
Prevention:
Anatomical reduction, stable fixation, appropriate bone grafting if needed.
Non-union:
Revision surgery with bone grafting, stable fixation, and possibly biological augmentation.
Malunion:
Corrective osteotomy if symptomatic and functionally limiting. |
|
Complex Regional Pain Syndrome (CRPS)
| <1% |
Prevention:
Gentle tissue handling, adequate pain control.
Management:
Multimodal approach including physical therapy, pain medication (NSAIDs, gabapentinoids, tricyclic antidepressants), nerve blocks, psychological support. Early diagnosis is key. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing outcomes and preventing complications. Protocols vary significantly based on the primary pathology and extent of surgical intervention.
General Principles
- Pain Management: Multimodal analgesia including NSAIDs, acetaminophen, nerve blocks, and short-term opioids as needed.
- Wound Care: Maintain a dry, sterile dressing. Monitor for signs of infection or wound healing issues. Suture removal typically at 2-3 weeks.
- Edema Control: Elevation, compression wraps, and gentle ankle pumps (if permitted) to minimize swelling.
Specific Protocols
1. Clubfoot Release
- Immobilization: Long leg cast (knee flexed ~90°) for 4-6 weeks, followed by a short leg cast or a foot abduction orthosis (FAO) for several months, often worn full-time initially, then during sleep.
- Weight-bearing: Non-weight-bearing (NWB) in the cast.
-
Physical Therapy:
- After Cast Removal: Focus on gentle passive and active range of motion (ROM) of the ankle and foot, addressing dorsiflexion, eversion, and abduction. Stretching exercises.
- Strengthening: Gradual strengthening as tolerated.
- Gait Training: Re-education once weight-bearing is permitted.
- Long-term: Continued bracing and regular follow-up for several years to prevent recurrence.
2. Tarsal Tunnel Syndrome Decompression
- Immobilization: Short leg splint or walking boot with the ankle in a neutral position for 1-2 weeks for comfort and wound healing.
- Weight-bearing: Weight-bearing as tolerated (WBAT) immediately or within a few days, depending on comfort.
-
Physical Therapy:
- Early (0-2 weeks): Gentle ankle ROM (dorsiflexion, plantarflexion, inversion, eversion) within pain limits. Nerve gliding exercises.
- Intermediate (2-6 weeks): Gradual increase in ROM, gentle stretching. Progression to strengthening exercises for foot intrinsic muscles and ankle musculature.
- Late (>6 weeks): Full activity progression. Address any residual neurological symptoms (desensitization).
3. FHL Tenosynovitis/Impingement Release
- Immobilization: Short leg walking boot or protected weight-bearing for 2-4 weeks, or until pain subsides.
- Weight-bearing: Protected weight-bearing initially, progressing to full WBAT as comfort allows.
-
Physical Therapy:
- Early (0-2 weeks): Gentle passive and active ROM of the ankle and great toe. FHL gliding exercises.
- Intermediate (2-6 weeks): Gradual progression of great toe and ankle strengthening. Proprioceptive training.
- Late (>6 weeks): Return to sport-specific or activity-specific training, emphasizing controlled FHL loading.
4. Posterior Malleolar Fracture Fixation (via posteromedial approach)
- Immobilization: Non-weight-bearing in a posterior splint or short leg cast for 4-6 weeks to allow fracture healing.
- Weight-bearing: Gradual progression of weight-bearing after radiographic evidence of healing, typically in a walking boot. PWB for 2-4 weeks, then WBAT.
-
Physical Therapy:
- Early (0-4 weeks, NWB): Isometric exercises for ankle musculature (if permitted and pain-free). Core and hip strengthening.
- Intermediate (4-8 weeks, PWB to WBAT): Gentle non-weight-bearing ankle ROM initially. Progress to active-assisted and active ROM. Introduction of strengthening exercises.
- Late (>8 weeks): Progression to full weight-bearing. Balance and proprioception training. Return to activity gradually. The timing of rehabilitation is dependent on fracture stability and healing.
Summary of Key Literature / Guidelines
The posteromedial approach remains a cornerstone in foot and ankle surgery, particularly for soft tissue pathologies. Its applications and nuances continue to be refined in the literature.
For Clubfoot , the advent of the Ponseti method in the mid-20th century revolutionized management, emphasizing serial casting with a limited posterior Achilles tenotomy. However, for complex, rigid, or recurrent clubfoot deformities, a comprehensive posteromedial release remains a standard surgical intervention. Classic papers by Turco (1979) described the extensive nature of the soft tissue releases required, involving lengthening of posterior tendons (Achilles, FHL, FDL, TP) and capsular releases of the ankle, subtalar, and talonavicular joints. Modern surgical techniques often attempt to limit the extent of release while achieving correction, with growing emphasis on preserving joint capsule integrity where possible, reflecting a shift towards less invasive procedures. The timing and extent of posteromedial release are guided by the severity of the deformity and response to non-operative treatment, with most guidelines advocating for surgical intervention only after failure of comprehensive Ponseti casting.
For Tarsal Tunnel Syndrome , the posteromedial approach is the standard for surgical decompression. Studies by Gould (1987) and others have detailed the technique for complete division of the flexor retinaculum, emphasizing the need to identify and decompress all branches of the tibial nerve, including the calcaneal nerves. The literature highlights the importance of thorough exploration for any extrinsic or intrinsic compressive lesions. Outcomes are generally favorable, though complete symptom relief can be elusive in cases of long-standing neuropathy or when an underlying etiology remains unaddressed. Electrodiagnostic studies are crucial for diagnosis and surgical planning.
In the context of Flexor Hallucis Longus (FHL) pathology , the posteromedial approach is widely accepted. Research by Hamilton et al. (1992) and others has described the incidence of FHL tendinopathy in dancers, with surgical release or tenosynovectomy showing good results for symptomatic relief and return to activity. The debate between open posteromedial and arthroscopic posterior approaches for posterior ankle impingement and FHL issues continues, with arthroscopy offering benefits of minimally invasive access and joint visualization, while the open posteromedial approach provides direct access for extensive tendon debridement or mass excision.
Regarding Posterior Malleolar Fractures , the role of the posteromedial approach has evolved significantly. Historically, these fractures were often managed indirectly or through a posteromedial approach for specific fragments. However, contemporary literature, spearheaded by studies from Müller (1965) and later refined by various authors (e.g., Haraguchi et al., 2006; Bartoníček et al., 2015), has underscored the importance of anatomical reduction and stable fixation of posterior malleolar fragments, particularly for those involving >25-30% of the articular surface or causing syndesmotic instability. Direct visualization via a posterolateral approach is now often favored for large or complex fragments to ensure accurate articular surface reduction. The posteromedial approach for posterior malleolar fractures is typically reserved for smaller fragments, indirect reduction with percutaneous fixation under fluoroscopic guidance, or in conjunction with medial malleolus fixation. Some authors advocate for a combined posteromedial and posterolateral approach for complex trimalleolar fractures with significant posterior involvement, allowing access to both posteromedial and posterolateral aspects for comprehensive reduction and fixation.
In summary, while the posteromedial approach remains an essential tool, its specific applications have been refined by advancements in imaging, arthroscopic techniques, and a deeper understanding of ankle biomechanics, particularly in the management of posterior malleolar fractures. Surgeons must critically assess each case to determine the most appropriate approach or combination of approaches to optimize patient outcomes.
Clinical & Radiographic Imaging

You Might Also Like