The Posterolateral Approach to the Tibia: Indications, Surgical Anatomy, and Technique Overview

Key Takeaway
The posterolateral approach to the tibia is a critical surgical exposure for complex midshaft and distal tibial pathologies, especially with compromised anterior soft tissues. It enables direct posterior buttress fixation, addressing severe trauma, infected nonunions, and specific posterolateral fracture patterns. Its value lies in providing stable fixation and addressing reconstructive challenges.
Introduction & Epidemiology
The posterolateral approach to the tibia represents a critical, albeit technically demanding, surgical exposure primarily utilized for complex midshaft and distal tibial pathologies where anterior soft tissue envelopes are compromised or a direct posterior buttress is required for stable fixation. While the anteromedial surface of the tibia is often more accessible, certain fracture patterns and clinical scenarios necessitate a posterior or posterolateral trajectory to achieve optimal reduction and stable internal fixation.
Historically, direct posterior approaches to the tibia were less favored due to concerns regarding neurovascular injury within the deep posterior compartment. However, a refined understanding of anatomical planes and advances in surgical technique and instrumentation have expanded the indications for the posterolateral approach. It is particularly valuable in cases of:
* Severe anterior soft tissue damage (e.g., open fractures, crush injuries, degloving injuries) that preclude direct anterior exposure or plating.
* Infected nonunions or malunions where previous anterior surgery has left a compromised soft tissue envelope.
* Specific fracture patterns involving the posterolateral aspect of the tibia, such as certain tibial pilon fractures with significant posterior comminution, posterolateral tibial plateau fractures (Schatzker type IV-VI), and distal tibia fractures with substantial posterolateral involvement.
* The requirement for bone grafting in regions with precarious anterior soft tissue coverage.
* Exposure of the posterior aspect of the fibula, often in conjunction with tibial procedures.
The incidence of tibial fractures is high, with diaphyseal fractures being among the most common long bone injuries. While most can be managed with intramedullary nailing or anterior plating, the subset requiring a posterolateral approach, although smaller, represents a complex patient population often associated with higher energy trauma and significant co-morbidities, underscoring the necessity for a versatile and effective surgical strategy. The ability to utilize the posterolateral approach enhances the orthopedic surgeon's armamentarium, providing solutions for cases that would otherwise present significant reconstructive challenges or higher rates of complications such as chronic infection or nonunion.
Surgical Anatomy & Biomechanics
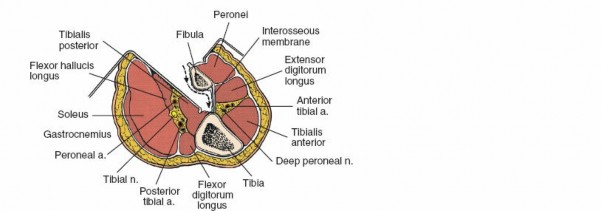
A thorough understanding of the regional anatomy is paramount for safe and effective execution of the posterolateral approach to the tibia. The approach navigates through distinct fascial compartments and internervous planes, minimizing muscle damage and protecting critical neurovascular structures.
Superficial Anatomy
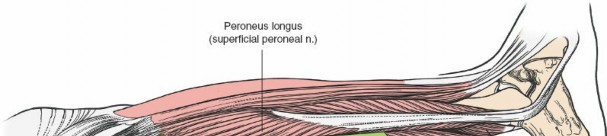
The skin and subcutaneous tissues of the posterolateral calf are generally robust, but the quality can vary significantly in trauma patients. The primary landmark for the incision is the lateral border of the gastrocnemius muscle . This muscle originates from the femoral condyles and forms the superficial layer of the posterior compartment, palpable as it transitions into the Achilles tendon.
Deep Anatomy
Deep to the gastrocnemius lies the
soleus muscle
, which originates from the posterior aspect of the fibula and the soleal line of the tibia. Together, the gastrocnemius and soleus form the triceps surae, inserting via the Achilles tendon.
The posterolateral approach primarily targets the interval between the lateral head of the gastrocnemius/soleus and the deep posterior compartment muscles, or by splitting the soleus.
Muscle Compartments and Internervous Planes:
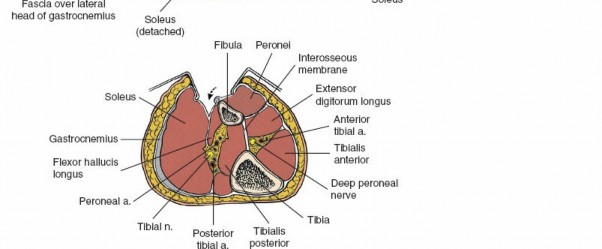
The leg is divided into four main compartments by fascial septa: anterior, lateral, superficial posterior, and deep posterior.
1.
Superficial Posterior Compartment
: Contains the gastrocnemius and soleus muscles (triceps surae) and the plantaris muscle. These are primarily innervated by the
tibial nerve
.
2.
Deep Posterior Compartment
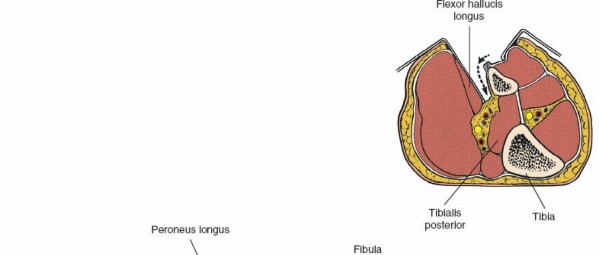
: Contains the
tibialis posterior
,
flexor digitorum longus (FDL)
, and
flexor hallucis longus (FHL)
muscles. All are innervated by the
tibial nerve
.
*
Tibialis Posterior
: Lies directly on the interosseous membrane and the posterior aspect of the tibia. Its tendon passes behind the medial malleolus.
*
Flexor Digitorum Longus
: Lies medial to the tibialis posterior, originating from the posterior tibia.
*
Flexor Hallucis Longus
: Lies lateral to the tibialis posterior, originating from the posterior fibula.
The surgical internervous plane for the posterolateral approach is typically between the lateral head of the gastrocnemius/soleus complex and the peroneal muscles laterally, or, more commonly, by splitting the soleus longitudinally. The deeper plane is between the soleus and the deep posterior compartment muscles (tibialis posterior, FDL, FHL). Retraction of the soleus and gastrocnemius medially exposes the deep posterior compartment structures. The tibialis posterior muscle is then elevated subperiosteally off the tibia to expose the posterior surface of the bone.
Neurovascular Structures:
The deep posterior compartment is critical due to the presence of the main neurovascular bundle of the leg:
*
Tibial Nerve
: Travels inferiorly, superficial to the tibialis posterior and FDL, typically deep to the soleus. It supplies all posterior compartment muscles.
*
Posterior Tibial Artery and Veins
: Accompanies the tibial nerve. These vessels are positioned medial to the nerve in the proximal leg and become more lateral distally.
*
Peroneal Artery and Veins
: Arise from the posterior tibial artery and lie more laterally, running along the posteromedial aspect of the fibula, usually between the tibialis posterior and FHL muscles. This bundle is vulnerable during fibular exposure or aggressive lateral retraction.
Careful identification and protection of these structures are paramount. The posterior tibial neurovascular bundle, along with the tibialis posterior muscle, acts as a protective shield for the posterior surface of the tibia. Subperiosteal elevation of the tibialis posterior allows direct access to the posterior tibia while minimizing neurovascular compromise.
Biomechanics:
The posterolateral approach allows direct application of a buttress plate to the posterior or posterolateral tibial cortex, providing inherent stability against posterior translation and shear forces. For fractures with significant posterior comminution, such as certain pilon fractures or metaphyseal tibial fractures, a posterior buttress plate is biomechanically superior to an anterior plate in preventing posterior collapse and maintaining articular reduction. This approach often results in a better soft tissue envelope over the implant compared to an anterior approach in cases of compromised anterior skin, reducing the risk of wound dehiscence and hardware exposure.
Indications & Contraindications
The selection of the posterolateral approach is dictated by the specific fracture pattern, soft tissue status, and patient factors. It is a technically challenging approach reserved for complex scenarios where conventional exposures are suboptimal or contraindicated.
Indications
-
Compromised Anterior Soft Tissue Envelope
:
- Severe scarring from previous surgeries, trauma, or burns.
- Open fractures with extensive anterior wound contamination or tissue loss.
- Chronic osteomyelitis requiring debridement and stable fixation where anterior soft tissues are unhealthy.
- Post-traumatic skin grafts or flaps on the anterior surface.
- Compartment syndrome fasciotomies leaving exposed or vulnerable anterior muscle.
-
Specific Fracture Patterns Requiring Posterior Buttressing
:
- Distal Tibia (Pilon) Fractures : Especially those with significant posterior or posterolateral articular and metaphyseal comminution (e.g., AO/OTA 43-C3, certain Ruedi-Allgöwer Type III). A posterior plate can buttress the articular fragments and resist posterior displacement.
- Tibial Plateau Fractures : Primarily posterolateral plateau fractures (e.g., Schatzker Type IV, VI) where direct visualization and buttress plating are necessary. This approach can be combined with a lateral approach for bicondylar fixation.
- Midshaft Tibia Fractures : Particularly those with complex posterior comminution or those involving the posterolateral cortex that require direct reduction and fixation, especially in osteopenic bone where rotational stability is crucial.
- Tibial Malunions/Nonunions : Posterior malunions or nonunions requiring osteotomy, debridement, bone grafting, and rigid fixation, especially if the anterior aspect has been previously operated on.
- Peroneal Artery Access : If needed for vascular repair or grafting in conjunction with a tibial procedure, though this is not a primary indication for the tibial exposure itself.
-
Pathological Lesions
:
- Biopsy or resection of tumors located on the posterior aspect of the tibia.
- Debridement of chronic osteomyelitis primarily affecting the posterior cortex.
- Concomitant Fibula Exposure : The approach facilitates exposure of the middle posterior aspect of the fibula, useful for concurrent fibular fixation or osteotomy.
Contraindications
- Healthy Anterior Soft Tissue and Simple Fracture Patterns : If the anterior soft tissue envelope is pristine and the fracture pattern is amenable to anterior plating or intramedullary nailing with good outcomes, the posterolateral approach's morbidity often outweighs its benefits.
- Active Infection in the Posterior Compartment : While the approach can be used for debridement, widespread infection within the deep posterior compartment may complicate the dissection and increase the risk of neurovascular injury.
- Severe Posterior Soft Tissue Injury : Extensive posterior crush injury, open wounds, or degloving of the posterior calf.
- Inadequate Surgical Experience : This is a technically challenging approach; lack of familiarity with the anatomy and technique by the operating surgeon is a relative contraindication.
- Anatomical Variants : Rare but significant anatomical variations of the neurovascular bundle that could increase surgical risk.
Summary of Indications
| Category | Operative Indications | Non-Operative Considerations (Rare for this approach) |
|---|---|---|
| Soft Tissue |
- Significant anterior soft tissue compromise (scarring, infection, wounds, previous surgery)
- Need for superior soft tissue coverage over implant |
- Generally, if the posterolateral approach is considered, it implies a complex fracture or soft tissue issue precluding non-operative management.
- Extremely stable, non-displaced fractures with healthy soft tissues might be managed non-operatively, but these rarely require consideration of this specific approach in the first place. This approach is typically for operative fixation. |
| Fracture Type |
- Distal Tibia (Pilon) fractures with extensive posterior/posterolateral comminution
- Posterolateral Tibial Plateau fractures (Schatzker IV-VI) - Midshaft Tibia fractures with complex posterior comminution - Tibial malunions/nonunions requiring posterior access |
- Stable, non-displaced extra-articular fractures (rarely an indication for surgery via
any
approach, let alone posterolateral).
- Stress fractures of the tibia. - Isolated, non-displaced avulsion fractures (e.g., posterior malleolus without significant posterior articular involvement). |
| Pathology |
- Chronic osteomyelitis affecting the posterior tibia, requiring debridement and reconstruction
- Tumors or lesions on the posterior aspect of the tibia requiring biopsy/resection |
- Acute osteomyelitis amenable to systemic antibiotics without surgical debridement.
- Benign lesions not requiring surgical intervention. |
| Concomitant Needs |
- Concurrent fibular exposure for fixation or grafting
- Need for local muscle flap coverage (e.g., soleus flap) in conjunction with tibial fixation. |
- None directly related to the unique advantages of the posterolateral approach; if these needs exist, they invariably lean towards operative intervention. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are crucial for successful outcomes and minimizing complications with the posterolateral approach.
Pre-Operative Planning
-
Imaging Review
:
- Standard Radiographs : Anteroposterior, lateral, and oblique views to assess fracture pattern, displacement, and comminution.
- Computed Tomography (CT) Scans : Essential, especially for articular fractures (pilon, plateau). CT with 3D reconstructions provides invaluable information regarding fragment orientation, articular step-off, and the extent of posterior or posterolateral involvement. It helps determine the optimal plate trajectory and screw length.
- Magnetic Resonance Imaging (MRI) : May be useful for assessing soft tissue damage, ligamentous injuries, or tumor extension, though less commonly required for acute fracture planning.
- Fracture Classification & Morphology : Thorough understanding of the specific fracture pattern (e.g., posterior pilon, posterolateral tibial plateau) and the degree of comminution. Identify key articular fragments that require direct reduction.
-
Surgical Strategy
:
- Reduction Techniques : Plan for indirect reduction methods (traction, ligamentotaxis) and direct reduction (bone clamps, temporary K-wires, joysticks).
- Hardware Selection : Determine the type, length, and contour of plates (e.g., contoured posterolateral plates for pilon fractures, locking plates for metaphyseal comminution, one-third tubular plates for fibular fixation). Select appropriate screw sizes and lengths.
- Bone Grafting : Assess if bone grafting (autograft or allograft) will be required for metaphyseal defects or nonunion.
- Tourniquet Considerations : Plan for tourniquet use, including cuff size and anticipated inflation time.
- Soft Tissue Assessment : Evaluate the skin and soft tissue quality both anteriorly and posteriorly. Document any pre-existing scars, open wounds, or signs of infection. Consider consultation with plastic surgery if extensive soft tissue reconstruction is anticipated.
- Surgeon Familiarity : Ensure the operating surgeon and assisting team are familiar with the anatomical landmarks and the step-by-step dissection of this demanding approach.
Patient Positioning
The patient is typically placed in the lateral decubitus position with the affected limb uppermost. This provides optimal access to the posterolateral aspect of the leg and facilitates C-arm imaging.
- Anesthesia : General or regional anesthesia is suitable.
-
Positioning on Operating Table
:
- Place the patient on their side, ensuring the affected leg is uppermost.
- Utilize a beanbag or vacuum mattress to stabilize the patient. Securely mold and deflate the beanbag around the torso and pelvis to prevent rolling.
-
 - Protect Bony Prominences : Meticulously pad all pressure points on the dependent leg and torso to prevent nerve palsies (e.g., peroneal nerve at the fibular head, ulnar nerve at the elbow) and pressure sores. An axillary roll should be placed under the dependent axilla to protect the brachial plexus and ensure adequate blood flow to the dependent arm. The lower leg's hip, knee, and ankle should be flexed, and padding placed between the knees.
- Limb Preparation : The entire limb, from mid-thigh to toes, should be prepared and draped to allow free manipulation of the ankle and knee for reduction maneuvers and C-arm access.
- Tourniquet Placement : A sterile or non-sterile pneumatic tourniquet is applied high on the thigh. The limb is exsanguinated by elevating it for 5 minutes, followed by inflation of the tourniquet to a pressure typically 100-150 mmHg above systolic blood pressure, or a pre-determined safe pressure.
- C-Arm Access : Confirm adequate C-arm access for intraoperative fluoroscopy in anteroposterior, lateral, and oblique projections. This is crucial for confirming reduction and hardware placement.
Detailed Surgical Approach / Technique
The posterolateral approach requires precise dissection and meticulous handling of tissues to protect neurovascular structures and achieve optimal exposure.
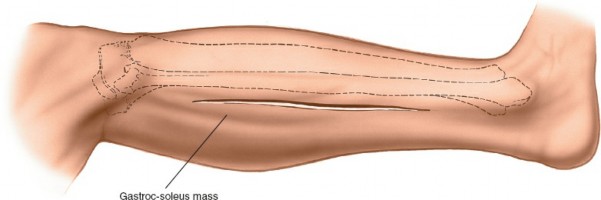
Landmark and Incision
-
Landmark
: The primary anatomical landmark is the
lateral border of the gastrocnemius muscle
, which is readily palpable in the mid-calf. In the distal leg, the lateral border of the Achilles tendon can also be used as a guide.
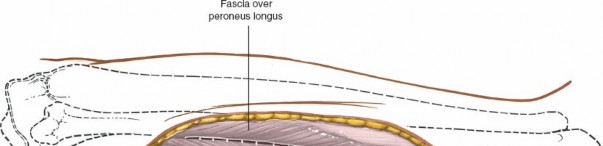
-
(This image could illustrate palpation of the gastrocnemius border and the planned incision.)
-
- Incision : A longitudinal skin incision is made directly over the lateral border of the gastrocnemius muscle. The length of the incision is dictated by the extent of pathology and the required exposure, but typically a minimum of 10-15 cm is necessary. Center the incision over the fracture or target pathology. In the distal third of the leg, this incision may lie just lateral to the Achilles tendon.
Superficial Dissection
- Skin and Subcutaneous Tissue : Incise the skin and subcutaneous tissue down to the deep fascia. Meticulous hemostasis is performed.
- Deep Fascia : Incise the deep fascia of the calf in line with the skin incision.
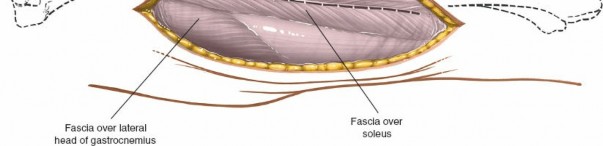
-
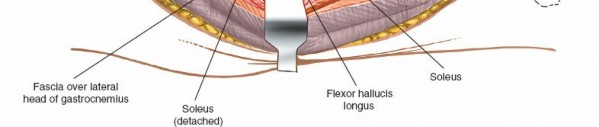
Identify Gastrocnemius and Soleus
: The lateral head of the gastrocnemius muscle will be evident. The goal is to identify the interval between the gastrocnemius/soleus complex and the peroneal muscles laterally. Often, it's more direct to split the soleus muscle longitudinally.
-
(This image could depict the initial incision through skin and fascia, exposing the gastrocnemius.)
-
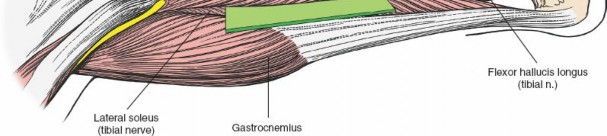
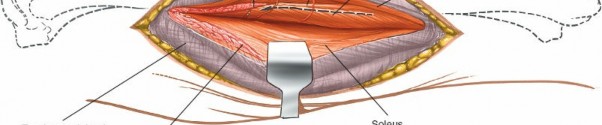
Exposure of the Deep Posterior Compartment
-
Splitting the Soleus
: Carefully incise the soleus muscle longitudinally. The soleus muscle is usually adherent to the deep fascia of the deep posterior compartment. Retract the soleus and gastrocnemius medially.
-
(This image could show the soleus muscle being carefully incised or retracted.)
-
-
Identify Neurovascular Bundle
: As the soleus is retracted medially, the
tibial nerve
and
posterior tibial artery and veins
will come into view, lying on the surface of the tibialis posterior and flexor digitorum longus muscles. These structures run deep to the soleus. It is critical to identify and protect this neurovascular bundle throughout the entire procedure. Use blunt dissection and gentle retraction.
-
(This image could highlight the posterior tibial neurovascular bundle, demonstrating its identification and protection.)
-
-
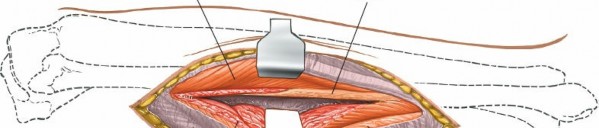
Retraction of Deep Posterior Compartment Muscles
: The posterior tibial neurovascular bundle and the flexor digitorum longus and tibialis posterior muscles are carefully retracted anteriorly and medially. This exposes the posterior surface of the tibia and the interosseous membrane.
-
(This image could show the medial retraction of the neurovascular bundle and deep posterior muscles, exposing the underlying bone.)
-
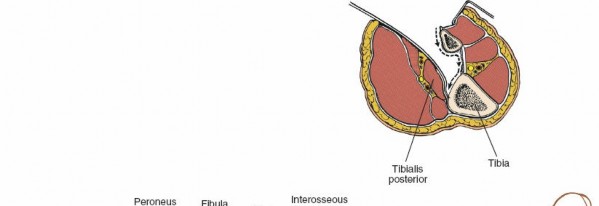
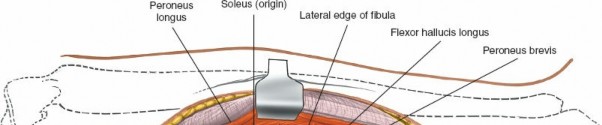
Subperiosteal Exposure of the Tibia and Fibula
- Periosteal Incision : Once the deep posterior compartment muscles and neurovascular structures are safely retracted, incise the periosteum longitudinally along the posterolateral border of the tibia.
-
Subperiosteal Elevation
: Using a periosteal elevator, carefully elevate the tibialis posterior muscle and periosteum from the posterior aspect of the tibia. Maintain constant visualization of the retracted neurovascular bundle to prevent inadvertent injury. This allows direct access to the posterior and posterolateral tibial shaft.
-
(This image could depict the subperiosteal elevation, showcasing the exposed posterior tibia.)
-
- Fibular Exposure (Optional) : If access to the posterior fibula is also required, the dissection can be extended laterally, carefully identifying and protecting the peroneal neurovascular bundle if necessary. The flexor hallucis longus muscle originates from the posterior fibula and can be elevated.
Fracture Reduction and Fixation
- Debridement and Visualization : Debride the fracture hematoma and carefully visualize the fracture fragments. For articular fractures, identify key fragments for anatomical reduction.
-
Reduction
:
- Indirect Reduction : Apply longitudinal traction to the foot and ankle, often using a fracture table or assistant. This helps restore length and align major fragments.
- Direct Reduction : Use reduction clamps, temporary K-wires, or pointed bone clamps to manipulate and reduce individual fragments. For articular fractures, achieve anatomical reduction of the articular surface fragments first, typically using small K-wires for provisional fixation.
-
(This image could demonstrate a reduction maneuver, e.g., using a reduction clamp across a fracture.) -
(Another image showing a different angle or tool for fracture reduction.)
-
Provisional Fixation
: Once reduction is achieved, maintain it with temporary K-wires. Confirm reduction with intraoperative fluoroscopy in multiple planes.
-
(Image showing temporary K-wire fixation or another specific instrument used for holding reduction.)
-
-
Plate Application
:
- Select an appropriate locking plate (e.g., LCP posterolateral distal tibia plate or a small fragment LCP). Contour the plate as necessary to match the posterolateral contour of the tibia.
- Slide the plate submuscularly or subperiosteally along the posterior tibia, ensuring it spans the fracture adequately while leaving sufficient space for screw placement in healthy bone proximal and distal to the fracture.
-
(This image could show the contoured plate being positioned on the posterior tibia.) -
(Another view of plate application, perhaps showing a specific design or contour.)
-
Screw Insertion
:
- Begin with a lag screw (if applicable) across simple fracture lines to achieve interfragmentary compression.
- Insert locking screws bicortically, ensuring appropriate length and trajectory to avoid intra-articular penetration (for articular fractures) or compromise of the intramedullary canal (if future IMN is considered).
- Use a drill guide and depth gauge for accurate screw placement.
-
(Image illustrating screw insertion, perhaps showing the drill or screwdriver.)
-
Final Assessment
: After all screws are inserted, re-check reduction and fixation stability with fluoroscopy in multiple planes (AP, lateral, obliques). Confirm screw lengths and absence of intra-articular penetration.
-
(This image could show the final construct with plate and screws in place.) -
(Intraoperative fluoroscopic image confirming reduction and fixation.) -
(Another intraoperative fluoroscopic image from a different view.)
-
Wound Closure
- Hemostasis : Achieve meticulous hemostasis.
- Irrigation : Lavage the wound thoroughly with sterile saline.
- Drainage (Optional) : A suction drain may be placed in the deep compartment if significant bleeding is anticipated.
- Fascial Closure : Close the deep fascia and the split soleus muscle with absorbable sutures. This helps to restore the anatomical layers and minimize dead space.
-
Subcutaneous and Skin Closure
: Close the subcutaneous tissue and skin in layers.
-
(Image showing the completed surgical incision closure.) -
(Image of the post-operative dressing.) -
(Perhaps a post-operative clinical photograph of the leg.)
-
Finally, release the tourniquet and confirm adequate perfusion to the limb. Apply a sterile dressing.
Complications & Management
Despite its advantages in specific scenarios, the posterolateral approach to the tibia carries a unique set of potential complications that surgeons must be aware of and prepared to manage. The overall complication rate can be higher compared to less invasive approaches due to the complexity of the fractures and the inherent difficulty of the exposure.
General Complications
- Infection : As with any surgical procedure, infection is a risk, particularly in open fractures or cases involving pre-existing infection. Incidence varies but can be higher in complex trauma.
- Nonunion/Malunion : Despite stable fixation, biological factors (e.g., severe comminution, soft tissue devitalization, patient comorbidities) can lead to delayed union or nonunion. Malunion can occur if reduction is not anatomical.
- Hardware Failure : Breakage, loosening, or migration of implants.
- Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) : Thromboembolic events are a risk, especially in lower extremity trauma and prolonged immobilization.
- Compartment Syndrome : Rare post-operatively with this approach, but should be monitored for if pain is disproportionate or neurological deficits develop.
Specific Complications of the Posterolateral Approach
-
Neurovascular Injury
:
- Tibial Nerve/Posterior Tibial Artery/Veins : These structures are directly in the surgical field. Improper identification, excessive retraction, or inadvertent dissection can lead to nerve palsy, vessel laceration, or thrombosis.
- Peroneal Artery/Veins : Vulnerable during lateral extension of the dissection to expose the fibula.
- Incidence : Reports vary but can range from 1-5% for temporary neuropraxia to rare but devastating vascular injuries.
- Wound Complications : Despite the robust soft tissue coverage, skin edge necrosis, dehiscence, or hematoma can occur, particularly in patients with poor peripheral circulation or significant soft tissue trauma.
- Muscular Damage : Excessive splitting or devitalization of the soleus or gastrocnemius can lead to muscle weakness or functional deficits.
- Synostosis (Tibiofibular) : Rare, but direct trauma or extensive subperiosteal dissection near the interosseous membrane can lead to abnormal bone formation between the tibia and fibula.
Management Strategies
| Complication | Estimated Incidence (Variable) | Salvage/Treatment Strategies |
|---|---|---|
| Neurovascular Injury | 1-5% (neuropraxia/transient) |
Immediate recognition is key.
- Nerve Injury : - Neuropraxia/Axonotmesis : Observation, protective splinting, physical therapy, pain management. Most recover over weeks to months. - Neurotmesis (laceration) : Urgent surgical exploration and primary nerve repair or grafting, if feasible. - Vascular Injury (Posterior Tibial/Peroneal Arteries) : - Laceration/Thrombosis : Immediate vascular surgery consultation for primary repair, interpositional graft, or bypass. Fasciotomy may be necessary to prevent compartment syndrome. Close post-op monitoring for limb viability. |
| Infection | 2-10% (can be higher) |
-
Superficial
: Local wound care, oral antibiotics.
- Deep/SSI : Surgical debridement, thorough irrigation, culture-directed intravenous antibiotics. Retention or removal of hardware depending on stability and organism. May require plastic surgery consultation for flap coverage. Negative pressure wound therapy (NPWT). - Chronic Osteomyelitis : Staged debridement, antibiotic cement beads, external fixation, bone transport, or vascularized free tissue transfer. |
| Nonunion | 5-15% (depending on fracture) |
-
Hypertrophic
: Revision internal fixation (e.g., exchange nailing, heavier plate), bone grafting (autograft/allograft), electrical stimulation.
- Atrophic : Aggressive debridement of fibrous tissue at fracture site, rigid re-fixation, extensive bone grafting (autograft preferred), potentially bone morphogenetic proteins (BMPs). External fixation for stabilization or compression. |
| Malunion | Varies, dependent on reduction |
-
Symptomatic
: Corrective osteotomy and re-fixation.
- Asymptomatic : Observation. |
| Wound Complications | 5-10% |
-
Hematoma
: Evacuation.
- Seroma : Aspiration, drain placement. - Dehiscence/Necrosis : Local wound care, debridement, secondary closure, or plastic surgery consultation for flap reconstruction (e.g., gastrocnemius or soleus rotational flaps, free flaps). NPWT can be beneficial. |
| Hardware Failure | 2-5% |
-
Early (without union)
: Typically indicates inadequate reduction, nonunion, or excessive loading. Requires revision surgery with more rigid fixation, bone grafting, or switch to alternative fixation (e.g., IMN).
- Late (after union) : Removal of symptomatic hardware is an option. |
| DVT/PE | 1-3% |
-
Prevention
: Pharmacological prophylaxis (LMWH, direct oral anticoagulants), mechanical prophylaxis (compression stockings, intermittent pneumatic compression devices).
- Treatment : Anticoagulation (heparin, warfarin, DOACs). |
| Compartment Syndrome | <1% (post-op) |
-
Early recognition
: Monitor clinical signs (pain out of proportion, pallor, paresthesia, pulselessness, paralysis).
- Treatment : Emergency fasciotomy of all involved compartments. |
| Muscular Damage/Weakness | Varies (often mild) | - Physical therapy and rehabilitation. Most deficits are transient and improve with time. Persistent severe weakness may warrant EMG and nerve conduction studies. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following a posterolateral approach to the tibia is tailored to the specific fracture pattern, the stability of fixation, and the quality of soft tissue repair. The primary goals are to protect the repair, facilitate bone healing, maintain range of motion (ROM), restore strength, and enable a progressive return to function.
Immediate Post-Operative Period (Day 0-14)
-
Immobilization/Protection
:
- Initially, the limb is typically immobilized in a well-padded splint (e.g., posterior slab) or a removable boot (CAM walker) for comfort and protection against inadvertent weight-bearing or excessive motion.
- Elevation of the limb is crucial to minimize swelling.
-
(This image could show the post-op dressing and splint/boot.)
-
Weight-Bearing (WB)
:
- Non-Weight Bearing (NWB) is almost universally prescribed for 6-12 weeks, depending on fracture stability, comminution, and bone quality. The posterolateral approach is often used for complex fractures, necessitating a cautious approach to loading.
- Crutches or a walker are provided, and patients are instructed in NWB ambulation.
-
Range of Motion (ROM)
:
- Ankle ROM : Gentle, active and passive dorsiflexion and plantarflexion exercises within a pain-free range, usually after the initial swelling subsides and wound is stable. This helps prevent stiffness and DVT.
- Knee ROM : If the fracture is distal and knee motion is not compromised by the surgical approach or associated injuries, gentle active knee flexion/extension can commence.
- Pain Management : Adequate pain control is essential for patient comfort and participation in early rehabilitation.
- Wound Care : Regular wound checks, dressing changes, and monitoring for signs of infection or dehiscence. Sutures/staples are typically removed at 10-14 days.
Early Rehabilitation Phase (Week 2-6)
- Weight-Bearing : Continued NWB.
-
ROM
:
- Progressive increase in active and passive ankle and knee ROM (if not restricted by fracture type or approach).
- Gentle stretching exercises.
-
Muscle Strengthening
:
- Isometric exercises for quadriceps, hamstrings, and hip abductors/adductors.
- Light resisted ankle exercises (e.g., with resistance bands) for dorsiflexors, plantarflexors, invertors, and evertors, only if cleared by the surgeon based on fracture stability .
- Scar Management : Gentle massage of incision sites once wound is healed to minimize scar adhesion and improve soft tissue mobility.
Mid-Rehabilitation Phase (Week 6-12)
-
Weight-Bearing Progression
:
- Radiographic evidence of early callus formation is usually required before advancing weight-bearing.
- Touch-Down Weight-Bearing (TDWB) or Partial Weight-Bearing (PWB) in a CAM walker or brace, with gradual progression to full weight-bearing (FWB) over several weeks, guided by clinical and radiographic assessment.
- Instruction on gait training with assistive devices.
- ROM : Continue to work towards full, pain-free ankle and knee ROM.
-
Strengthening
:
- Progressive resistive exercises for all lower extremity muscle groups.
- Focus on eccentric control and single-leg balance.
- Initiate stationary cycling with low resistance, gradually increasing as tolerated.
- Proprioception and Balance : Begin balance exercises (e.g., single-leg stance, wobble board) in a controlled environment.
Late Rehabilitation Phase (Week 12+)
- Weight-Bearing : Progression to FWB without assistive devices, once clinical and radiographic union is evident.
-
Strength and Conditioning
:
- Advanced strengthening exercises, incorporating functional movements.
- Progress from isolated muscle exercises to compound movements (e.g., squats, lunges, calf raises).
- Gradual introduction of agility drills and plyometrics, if appropriate for the patient's goals and bone healing status.
-
Return to Activity
:
- Phased return to recreational activities, sports, or demanding occupations, typically 4-6 months post-surgery, or longer for high-impact activities.
- Activity modification may be necessary for an extended period.
- Hardware removal may be considered typically 12-18 months post-op, if symptomatic or for young active individuals.
Throughout all phases, close collaboration between the surgeon, physical therapist, and patient is essential. Clinical signs of pain, swelling, or instability should prompt re-evaluation. Radiographic healing benchmarks are paramount in guiding weight-bearing progression.
Summary of Key Literature / Guidelines
The posterolateral approach to the tibia, while a specialized technique, has gained increasing acceptance and refinement in orthopedic trauma surgery due to improved understanding of fracture biomechanics and advancements in plating technology. Key literature and guidelines often highlight its utility in specific contexts.
Pilon Fractures
For complex tibial pilon fractures (e.g., AO/OTA 43-C3, specifically those with significant posterior involvement), the posterolateral approach offers several advantages. Early studies by Rüedi and Allgöwer advocated for anatomical reduction and stable internal fixation. Modern consensus, supported by biomechanical studies and clinical series, emphasizes the importance of addressing the posterior column separately.
*
Biomechanical studies
have demonstrated that posterior buttress plating for posteriorly comminuted pilon fractures provides superior stability and prevents posterior collapse compared to anterior plating alone. This is particularly relevant given the high compressive forces across the ankle joint.
*
Clinical series
have reported favorable outcomes with low rates of malunion and acceptable complication profiles when the posterolateral approach is used for appropriate pilon fracture patterns. Authors like Borens et al. and Franke et al. have detailed surgical techniques and results for posterior pilon plating, showing good functional outcomes and union rates, comparable to or superior to traditional anterior approaches in selected cases, especially with less soft tissue compromise over the implant.
Tibial Plateau Fractures
The posterolateral approach is indispensable for certain tibial plateau fractures.
*
Schatzker Type IV, V, and VI fractures
with significant posterolateral depression or split components benefit from direct visualization and buttress plating via this approach. It allows direct reduction of the posterolateral fragment, which can be challenging to access through standard anterolateral or medial approaches.
*
Posterolateral Corner Instability
: In cases of combined fracture-ligamentous injuries involving the posterolateral corner, this approach can facilitate both bony fixation and potential ligamentous repair or reconstruction.
*
Combined Approaches
: Often, the posterolateral approach is combined with an anteromedial or lateral approach (dual incisions) for bicondylar tibial plateau fractures, allowing for comprehensive reduction and fixation of all articular segments. Studies by Luo et al. and Kfuri et al. detail different surgical strategies for complex plateau fractures, often including various posterior approaches to address specific fragment morphology.
Midshaft and Distal Tibial Shaft Fractures
While intramedullary nailing remains the gold standard for most midshaft tibial fractures, the posterolateral approach is a viable alternative for:
*
Plate fixation of midshaft fractures with severe anterior soft tissue compromise
or in cases of chronic osteomyelitis where anterior incisions are undesirable.
*
Distal metaphyseal-diaphyseal junction fractures
where the posterior cortex requires buttressing and angular stability.
*
Nonunions
: For recalcitrant nonunions, especially those with posterior gapping or malalignment, this approach allows for debridement, bone grafting, and rigid posterior plating.
Soft Tissue Considerations
A significant advantage emphasized in the literature is the ability of the posterolateral approach to utilize a relatively pristine soft tissue envelope, particularly when the anterior compartment has been compromised by previous trauma or surgery. This can reduce rates of wound dehiscence and infection, which are common and debilitating complications in tibial fracture management. The ability to directly elevate the soleus muscle provides a muscular flap for coverage if needed, enhancing local tissue viability.
Technical Demands and Learning Curve
The literature consistently highlights the technical difficulty and steep learning curve associated with the posterolateral approach. Surgeons undertaking this approach must possess an advanced understanding of lower leg anatomy, particularly the neurovascular bundle in the deep posterior compartment. Meticulous dissection and careful retraction are repeatedly stressed as paramount to minimizing iatrogenic injury. Cadaveric dissection and mentorship are often recommended for trainees.
Current Trends
Current trends in tibial fracture management, particularly for articular fractures, favor specific anatomical approaches that allow direct visualization and reduction of fracture fragments. The posterolateral approach aligns with this philosophy, offering a direct conduit to the posterior and posterolateral aspects of the tibia for precise anatomical restoration and stable fixation, especially with the use of precontoured locking plates. The move towards minimally invasive plate osteosynthesis (MIPO) through smaller incisions is also being explored with posterolateral approaches, leveraging indirect reduction techniques to preserve soft tissue while still achieving direct plate application.
In conclusion, the posterolateral approach to the tibia is a powerful, albeit challenging, tool in the orthopedic surgeon's arsenal. Its indications are well-defined, primarily driven by complex fracture patterns, articular involvement, and compromised anterior soft tissue. Adherence to meticulous surgical technique and a thorough understanding of anatomical considerations are critical for successful outcomes and minimizing complications, as consistently supported by contemporary literature and surgical guidelines.
Clinical & Radiographic Imaging


You Might Also Like

