Achieve Faster Recovery: Hip Minimally Invasive Anterior Approach
Key Takeaway
Looking for accurate information on Achieve Faster Recovery: Hip Minimally Invasive Anterior Approach? The hip minimally invasive anterior approach is a surgical technique mainly for elective joint replacement, also used for femoral neck fractures or hip joint infections. It preserves muscle, potentially allowing faster initial recovery. Surgeons utilize an internervous plane between the sartorius and tensor fasciae latae, often with an image intensifier to compensate for reduced joint exposure during this procedure.
Introduction & Epidemiology
The direct anterior approach (DAA) to the hip has gained significant traction within orthopedic surgery, particularly for total hip arthroplasty (THA). While not a novel approach—initially described by Hueter in 1881 and later popularized by Robert Judet in the 1940s—its resurgence is largely attributed to advancements in instrumentation, surgical technique, and a growing emphasis on minimally invasive surgery and accelerated patient recovery pathways. The DAA is anatomically distinct in that it utilizes an internervous and intermuscular plane, thereby theoretically minimizing muscle dissection and subsequent post-operative pain and dysfunction compared to posterolateral or direct lateral approaches.
Globally, the incidence of THA continues to rise, driven by an aging population, increasing rates of osteoarthritis, and expanding indications for joint replacement. Current projections anticipate a substantial increase in THA procedures over the next two decades. With this surge, there is a parallel demand for techniques that optimize patient outcomes, reduce hospital length of stay, and facilitate a quicker return to functional independence. The DAA is often posited as fulfilling these criteria, contributing to its increasing adoption. Epidemiological studies have demonstrated varying rates of DAA utilization, but a clear upward trend is evident, especially in high-volume centers and among surgeons specializing in minimally invasive techniques. While initially a specialized approach, it is now a fundamental component of many orthopedic residency and fellowship training programs.
Surgical Anatomy & Biomechanics
A thorough understanding of the relevant anatomy is paramount for safe and efficient execution of the DAA. The approach targets the interval between the tensor fasciae latae (TFL) and the sartorius and rectus femoris muscles, providing direct access to the anterior hip capsule without incising key abductor muscles or external rotators.
Superficial Structures and Internervous Plane
The skin incision typically extends from the anterior superior iliac spine (ASIS) distally. Beneath the skin and subcutaneous fat lies the fascia lata, which must be incised. A critical structure in this superficial layer is the lateral femoral cutaneous nerve (LFCN) . This sensory nerve, originating from the L2-L3 spinal levels, typically emerges from the pelvis medial to the ASIS, often passing through or under the inguinal ligament. Its course can be highly variable, making it susceptible to traction, compression, or direct injury during dissection and retraction, leading to meralgia paresthetica.
The key internervous plane is established between:
*
Tensor fasciae latae (TFL):
Laterally, supplied by the superior gluteal nerve (L4-S1).
*
Sartorius:
Medially, supplied by the femoral nerve (L2-L4).
*
Rectus Femoris:
Also medially, deep to the sartorius, supplied by the femoral nerve (L2-L4).
This plane allows for blunt dissection and retraction of these muscle groups without significant denervation or direct muscle fiber injury.
Deeper Structures and Vascular Considerations
Deep to the TFL and rectus femoris, the ascending branch of the lateral circumflex femoral artery and vein are encountered. These vessels typically course beneath the rectus femoris and anterior to the vastus lateralis, providing vascular supply to the anterior thigh musculature. They generally require careful ligation and division to facilitate adequate exposure of the hip capsule, particularly for femoral preparation. Meticulous hemostasis is crucial to minimize post-operative hematoma formation.
The hip capsule lies deep to these structures, covering the femoral head and neck. A precise capsulotomy, typically performed in a T-shape or H-shape, exposes the femoral neck and acetabulum. The anterior capsule itself is innervated and provides proprioceptive feedback; its meticulous repair can potentially enhance joint stability and proprioception, though its routine repair following DAA is debated.
Biomechanical Implications
The muscle-sparing nature of the DAA is its primary biomechanical advantage. By avoiding detachment of the abductor mechanism (gluteus medius and minimus) and external rotators, the functional integrity of these critical muscles is preserved. This preservation is hypothesized to contribute to:
*
Faster initial recovery:
Reduced post-operative pain and improved early ambulation due to intact muscle function.
*
Lower dislocation rates:
With the posterior capsule and external rotators left largely undisturbed, the risk of posterior dislocation, the most common type following THA via posterior approach, is theoretically minimized. Anterior dislocation remains a potential, albeit less common, concern if anterior capsular repair is inadequate or component positioning is severely maloriented.
*
Improved gait mechanics:
Preservation of abductor strength can lead to a more physiological gait pattern earlier in the recovery phase.
However, the limited exposure inherent to a truly "minimally invasive" DAA can introduce technical challenges, particularly during femoral preparation, which may necessitate specific instrumentation or maneuvers (e.g., hyper-external rotation and extension of the limb, or direct anterior femoral head extraction techniques).
Indications & Contraindications
The minimally invasive anterior approach to the hip is a versatile surgical pathway, primarily utilized for elective total hip arthroplasty but also applicable in specific trauma and infection scenarios.
Indications
-
Primary Total Hip Arthroplasty (THA):
The most common indication. Suitable for patients with:
- Osteoarthritis: Primary or secondary.
- Rheumatoid Arthritis and other inflammatory arthropathies.
- Avascular Necrosis (AVN) of the femoral head.
- Post-traumatic Arthritis.
- Congenital or developmental hip dysplasia (DDH): Selected cases, often requiring careful pre-operative templating.
-
Fracture Management:
- Displaced Femoral Neck Fractures: In suitable elderly patients where THA or hemiarthroplasty is indicated. The DAA can be advantageous for direct visualization and reduction, especially in cases where internal fixation (ORIF) is preferred, though this is less common via DAA.
-
Infection:
- Drainage of Hip Joint Infections: Provides direct access to the joint for debridement and lavage in acute septic arthritis, particularly when an anterior collection is present.
-
Selected Revision THA:
- Isolated Acetabular Component Revision: When the femoral component is well-fixed and satisfactory.
- Component Repositioning: For specific maloriented components that are amenable to anterior revision. This is generally more technically demanding than primary THA via DAA.
- Hip Arthroscopy: Less commonly used as a primary arthroscopy portal, but can be extended for more complex open procedures from an arthroscopic approach.
Relative Contraindications
While few absolute contraindications exist, several factors may make the DAA more challenging or less appropriate:
*
Severe Obesity (BMI > 40-50):
Increased adipose tissue can significantly hinder surgical exposure, extend operative time, and elevate the risk of wound complications, LFCN injury, and technical difficulties with femoral preparation.
*
Extensive Prior Anterior Hip Surgery/Scarring:
May obscure anatomical landmarks, distort tissue planes, and increase the risk of neurovascular injury.
*
Significant Pre-existing Deformity or Ankylosis:
Severe fixed flexion contractures, significant acetabular protrusio, or extensive heterotopic ossification can complicate exposure and component insertion.
*
Morbidly Muscular Patients:
Particularly those with robust quadriceps and TFL musculature, which can impede retraction and visualization.
*
Severe Femoral Deformity:
Significant proximal femoral bowing, prior hardware, or substantial osteophytes on the femoral neck that require extensive exposure for adequate osteotomy and preparation may be more easily addressed via other approaches.
*
Surgeon Inexperience:
A steep learning curve is widely recognized for the DAA. Surgeons new to the approach may experience longer operative times, increased blood loss, and a higher rate of complications during their initial cases. Adequate training and proctoring are essential.
Table: Indications for Anterior Approach THA vs. Relative Contraindications
| Category | Indications for Anterior Approach THA | Relative Contraindications for Anterior Approach THA |
|---|---|---|
| Primary THA | Osteoarthritis, Rheumatoid Arthritis, Avascular Necrosis, Post-traumatic Arthritis, Selected Dysplasia | Severe obesity (BMI > 40), Extensive prior anterior surgery, Morbidly muscular patients |
| Fracture Management | Displaced femoral neck fractures suitable for THA or hemiarthroplasty | Comminuted femoral neck fractures requiring extensive visualization, unstable intertrochanteric fractures |
| Infection | Drainage and debridement of acute hip joint infections | Extensive soft tissue infection, deep abscesses not well-localized anteriorly |
| Revision THA | Isolated acetabular revision, Component repositioning in well-selected cases | Major bone loss, extensive component removal, significant periprosthetic osteolysis or fracture |
| Anatomical Factors | Minimal-to-moderate hip deformity, absence of severe proximal femoral bowing | Severe fixed flexion contracture, significant proximal femoral deformity (e.g., severe varus/valgus, prior hardware) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and precise patient positioning are critical for successful execution of the DAA, particularly given its inherently limited exposure.
Pre-Operative Planning
-
Radiographic Templating:
- Standardized anteroposterior (AP) pelvis and true lateral hip radiographs are essential.
- Digital templating is performed to estimate component size (acetabular cup and femoral stem), assess restoration of hip center of rotation, and predict leg length and offset.
- Identify potential challenges such as acetabular protrusio, severe osteophytes, heterotopic ossification, or femoral bowing.
- Consider CT imaging for complex anatomy or severe deformities to better understand 3D spatial relationships.
-
Implant Selection:
- Choose implants compatible with the DAA. Many manufacturers offer specific instrumentation designed to facilitate femoral preparation through the DAA.
- Consider stem geometry (straight vs. bowed) based on femoral canal anatomy.
-
Surgeon Experience & Team Preparation:
- Ensure the surgical team (surgeon, assistants, scrub tech, circulating nurse) is familiar with the DAA and the specific instrumentation being used.
- Availability of necessary retractors, specialized tables (if used), and an image intensifier (fluoroscopy) is paramount.
-
Patient Optimization:
- Optimize patient comorbidities.
- Discuss expectations regarding recovery and potential risks, particularly LFCN neuropraxia.
Patient Positioning
The patient is typically placed in a
supine position
on the operating table. This position offers several distinct advantages:
*
Image Intensifier Use:
The supine position permits unrestricted use of a C-arm for fluoroscopic guidance, which is of immense value in:
* Confirming the level of femoral neck osteotomy.
* Assessing acetabular reaming depth and peripheral contact.
* Verifying acetabular component inclination and anteversion.
* Confirming femoral component insertion depth and rotation.
* Accurate assessment of leg length discrepancy during trial reduction.

*Positioning of the patient and C-arm for fluoroscopic assessment during direct anterior approach THA.*
- Leg Length Assessment: Direct comparison of the operated and non-operated limb for real-time leg length assessment is facilitated.
- Anatomical Consistency: The anterior anatomy remains consistent relative to the bony landmarks, aiding orientation.
Specifics of Positioning:
-
Table Type:
- Regular Radiolucent Table: Most commonly used. Requires careful manual manipulation of the limb for femoral exposure. Some surgeons utilize a bump under the ipsilateral hip/buttock to facilitate external rotation and extension of the limb for femoral preparation.
- Traction Table (e.g., Hana table): Provides controlled traction and allows for precise positioning of the limb (hyperextension, external rotation) via automated controls. This can greatly assist in dislocating the hip, performing the femoral neck osteotomy, and achieving femoral exposure for broaching. However, it can complicate real-time leg length assessment and carries a theoretical increased risk of traction-related neurapraxia (e.g., pudendal nerve, LFCN).
Patient positioned supine on a regular radiolucent operating table, prepared for draping. -
Sacral Bump: A small sacral bump or rolled towel is placed under the sacrum to elevate the pelvis slightly. This helps to bring the operative hip forward, allowing for easier manipulation and access.
- Paddings: All pressure points must be meticulously padded, particularly the contralateral hip, ankles, and heels. The LFCN passes under the inguinal ligament, and prolonged compression or extreme traction can contribute to neuropraxia.
- Secure Strapping: The patient's torso and both legs are securely strapped to the table to prevent inadvertent movement during limb manipulation, especially if a regular table is used.
-
Perineal Post (if using a traction table): If a traction table is employed, a well-padded perineal post is essential. Proper cushioning and positioning are crucial to prevent pudendal nerve compression or skin breakdown.
Detailed view of sacral bump placement and securing straps for patient positioning on a regular table, emphasizing pressure point protection.


Detailed Surgical Approach / Technique
The direct anterior approach requires a precise, step-by-step dissection to navigate the internervous plane safely and effectively.
Landmarks and Incision
- Palpation: Meticulously palpate and mark the anterior superior iliac spine (ASIS) and the greater trochanter . In thin patients, these landmarks are readily palpable. In obese patients, careful palpation and sometimes fluoroscopic guidance are necessary.
-
Incision Planning: The incision generally begins 2-3 cm distal and 2 cm lateral to the ASIS, extending distally and slightly laterally towards the mid-patella. Its length can vary from 6-10 cm for a truly "minimally invasive" approach, but it may be extended proximally along the iliac crest or distally along the femur if more exposure is required. Some surgeons prefer an oblique incision more parallel to the inguinal ligament.
Surgical markings for the anterior approach, showing the ASIS and planned incision line.
Initial skin incision for the direct anterior approach, illustrating the typical orientation relative to the ASIS.


Superficial Dissection
- Skin and Subcutaneous Tissue: Incise the skin and subcutaneous fat. Maintain hemostasis.
- Fascia Lata: Identify and incise the fascia lata longitudinally. This fascia overlies the TFL laterally and the sartorius medially.
- Lateral Femoral Cutaneous Nerve (LFCN) Identification: The LFCN typically emerges from the pelvis about 2-3 cm medial to the ASIS. Proximally, it may be visualized and protected. Distally, it often branches and can be more difficult to consistently isolate. Gentle blunt dissection parallel to the nerve's course and meticulous soft tissue handling are crucial to minimize injury. Retraction should be broad and gentle.
Deep Dissection & Internervous Plane
- Identify the Interval: The key internervous interval is established between the tensor fasciae latae (TFL) laterally and the sartorius and rectus femoris muscles medially.
- Blunt Dissection: Bluntly dissect through this interval. The TFL is retracted laterally, while the sartorius and rectus femoris are retracted medially.
- Ascending Branch of Lateral Circumflex Femoral Artery: As dissection deepens, the ascending branch of the lateral circumflex femoral artery and its venae comitantes will typically be encountered. These vessels course obliquely across the surgical field, usually beneath the rectus femoris. They require careful ligation and division to provide adequate exposure of the hip capsule and underlying bone.
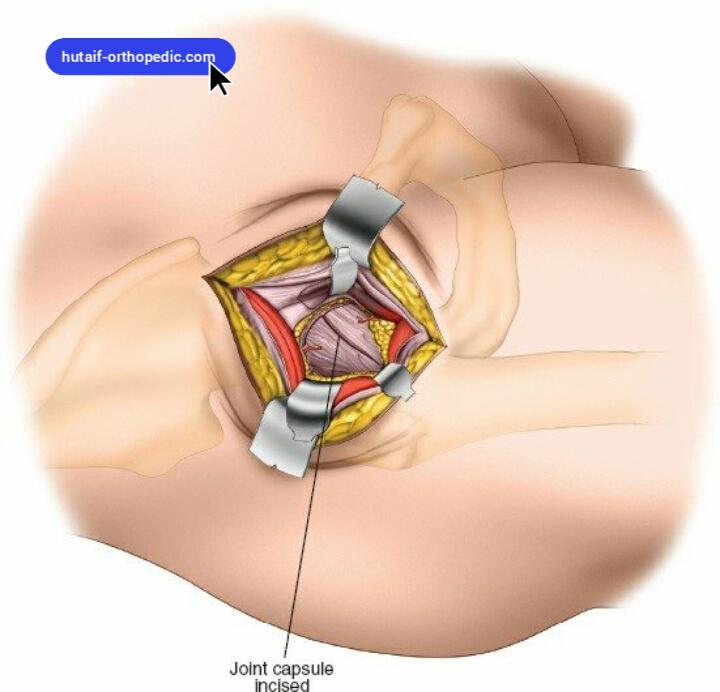
Capsulotomy
- Exposure: The hip capsule is exposed after retraction of the muscle groups and ligation of the ascending vessels. Ensure adequate exposure of the anterior and superior capsule.
- Capsulotomy: A standardized capsulotomy, such as an H-shape or T-shape, is performed. The superior limb of the capsulotomy is typically along the neck-capsule junction, and the inferior limb runs inferiorly from the center. The anterior capsule is generally preserved for potential repair at the end of the procedure, which may contribute to enhanced stability. Complete anterior capsular release is critical to facilitate dislocation and subsequent femoral preparation.
Femoral Neck Osteotomy
- Dislocation: The hip is typically dislocated anteriorly by internally rotating and extending the limb. A specialized corkscrew or bone hook can aid in femoral head elevation.
- Osteotomy Level: Using fluoroscopy, the femoral neck osteotomy level is marked. Typically, this is 10-15 mm above the lesser trochanter, ensuring adequate femoral neck resection for prosthetic implantation.
-
Osteotomy: The femoral neck osteotomy is performed using an oscillating saw. Ensure the cut is square to the femoral shaft axis. The excised femoral head is then removed.
Fluoroscopic image depicting the femoral neck osteotomy. The C-arm confirms the accurate level of resection.

Acetabular Preparation
- Exposure: The remaining femoral head and neck fragments are cleared. The acetabular fossa is exposed by careful retraction of the surrounding soft tissues (anterior acetabular wall, iliopsoas). Specialized acetabular retractors designed for the DAA provide optimal visualization.
- Reaming: Progressive reaming of the acetabulum is performed to achieve a hemispherical socket, removing osteophytes and diseased cartilage, and preparing the subchondral bone for press-fit cup fixation.
- Cup Insertion: The definitive acetabular component is inserted. Fluoroscopy is used to confirm optimal inclination (typically 40-45 degrees) and anteversion (typically 15-20 degrees). Proper cup positioning is crucial for stability and minimizing impingement. Secure fixation is paramount.
Femoral Preparation
Femoral exposure is often the most challenging aspect of the DAA due to the limited surgical window.
1.
Femoral Exposure:
The remaining proximal femur is exposed. This often requires significant limb manipulation:
*
"Table-break" Maneuver (regular table):
The operative leg is brought into hyperextension, adduction, and external rotation by dropping the foot end of the table or extending the limb off the table. This brings the proximal femur anteriorly and facilitates exposure.
*
Traction Table Maneuvers:
Specific programs on the traction table can be used to position the limb for femoral exposure.
*
Femoral Lift Devices:
Specialized retractors or elevators may be used to lift the proximal femur anteriorly.
*
External Rotation and Extension:
The leg is externally rotated and extended, causing the greater trochanter to roll anteriorly and expose the femoral canal. This maneuver must be performed cautiously to avoid excessive soft tissue tension and potential neural injury.
2.
Broaching and Reaming:
The femoral canal is prepared sequentially using rasps (broaches) or reamers to match the chosen femoral stem's size and geometry. Fluoroscopy can be used to confirm stem alignment and depth.
3.
Trial Reduction:
Trial femoral and acetabular components are inserted. The hip is reduced. Assess leg length, offset, and dynamic stability through a full range of motion. Adjust trial components as necessary.
4.
Definitive Femoral Stem Insertion:
Once optimal trials are confirmed, the definitive femoral stem is inserted, either cemented or press-fit, depending on bone quality and implant choice. The femoral head is then impacted onto the taper.
Reduction & Stability Assessment
- Final Reduction: The definitive components are reduced.
- Range of Motion and Stability: The hip is moved through a full range of motion (flexion, extension, internal/external rotation, abduction/adduction) to assess for impingement and stability. No "hip precautions" are typically needed for the DAA due to muscle preservation, but extremes of motion, particularly combined extension, adduction, and external rotation, should be assessed for anterior impingement.
- Leg Length and Offset: Final fluoroscopic or clinical assessment of leg length and offset.
Wound Closure
- Irrigation: Thorough irrigation of the surgical site.
- Capsular Repair: Many surgeons advocate for anterior capsular repair or plication to further enhance stability and potentially reduce heterotopic ossification.
-
Layered Closure: Deep fascia is closed, followed by subcutaneous tissue and skin. A drain may be placed selectively, though often not required.
Final wound closure after direct anterior approach THA.

Complications & Management
While the DAA offers potential benefits, it is not without specific complications that surgeons must be prepared to anticipate and manage. The incidence rates can vary significantly based on surgeon experience and institutional volume.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (%) | Salvage / Management Strategy |
|---|---|---|
| Lateral Femoral Cutaneous Neuropraxia | 10-80% (sensory) | Prevention: Meticulous dissection, gentle broad retraction, avoid aggressive traction. Management: Reassurance, observation (most resolve spontaneously within 6-12 months), neuropathic pain medication (gabapentin, pregabalin) for symptomatic cases. Rarely, surgical neurolysis or neurectomy for severe, persistent symptoms. |
| Intra-operative Femoral Fracture | 0.5-2.0% | Prevention: Careful pre-operative templating, appropriate broach/reamer sizing, avoid excessive force during stem insertion, ensure adequate cortical support. Management: Depending on fracture pattern (Vancouver classification): cerclage wiring, revision to a longer or different stem design (e.g., modular or calcar-loading), plate fixation, or combination. |
| Periprosthetic Femoral Fracture | 0.5-1.5% | Prevention: Similar to intra-operative fractures. Management: Classified by Vancouver system. ORIF (plates, wires, screws), revision THA, or allograft strut augmentation, individualized based on fracture pattern, implant stability, and bone quality. |
| Surgical Site Infection (SSI) | <1% (comparable to other approaches) | Prevention: Standard perioperative infection control protocols (antibiotics, skin prep, sterile field). Management: Debridement and implant retention (DAIR) for acute infections, single-stage revision (selected cases), two-stage revision (gold standard for chronic infection), chronic antibiotic suppression. |
| Dislocation | 0.5-2.0% (lower than other approaches) | Prevention: Meticulous component positioning (inclination 40-45°, anteversion 15-20°), restore leg length and offset, consider capsular repair. Management: Closed reduction for primary dislocation. Recurrent dislocations may necessitate component revision for malposition, soft tissue repair (capsular plication), or conversion to constrained liner. |
| Leg Length Discrepancy (LLD) | 5-15% (perceived or true) | Prevention: Accurate pre-operative templating, intra-operative fluoroscopic measurement, comparison to contralateral limb, careful attention to hip center restoration. Management: For minor, asymptomatic LLD, reassurance or shoe lift. Significant, symptomatic LLD (typically >10-15 mm) may necessitate revision to adjust component position. |
| Vascular Injury (Femoral Artery/Vein) | Rare (<0.1%) | Prevention: Maintain awareness of medial vascular bundle, careful medial retraction. Management: Immediate surgical repair by orthopedic or vascular surgeon, often requiring conversion to an extensile approach. |
| Nerve Injury (Other) | Rare (<0.1%) | Prevention: Awareness of obturator, sciatic, and femoral nerve pathways; avoid excessive traction or direct trauma. Management: Observation, supportive care, neuropathic pain management. Recovery often spontaneous. |
| Heterotopic Ossification (HO) | 5-10% (clinical significance) | Prevention: Prophylactic NSAIDs (e.g., indomethacin) for 3-6 weeks or single-dose post-operative radiation therapy, especially in high-risk patients (e.g., prior HO, ankylosing spondylitis). Management: Excision for symptomatic HO after maturation, combined with prophylaxis to prevent recurrence. |
| Wound Healing Issues | 1-5% | Prevention: Atraumatic tissue handling, meticulous hemostasis, careful skin closure, optimize nutritional status. Management: Local wound care, débridement, wound VAC, flap reconstruction if severe. |
Specific Considerations for DAA Complications
- Learning Curve: The DAA has a recognized learning curve, during which a surgeon may experience higher rates of complications such as prolonged operative time, blood loss, LFCN injury, and femoral fracture. This emphasizes the importance of proper training, proctoring, and a gradual adoption strategy.
- Femoral Exposure Difficulties: Insufficient femoral exposure can lead to technical errors, including varus malalignment, undersizing of the stem, or femoral fractures during broaching or stem insertion. Modifications like extensile releases, direct anterior femoral head extraction, or specialized instruments can help mitigate this.
- Component Malposition: While fluoroscopy significantly aids in component positioning, inappropriate inclination or anteversion can still occur, particularly if images are not routinely correlated with anatomical landmarks or if the surgeon relies solely on fluoroscopy without adequate anatomical understanding.
Post-Operative Rehabilitation Protocols
The post-operative rehabilitation protocol following a DAA THA is often characterized by accelerated progression, capitalizing on the muscle-sparing nature of the approach. The primary goals are early mobilization, pain control, restoration of range of motion, and progressive strengthening.
Immediate Post-Operative Phase (Day 0 - Day 3)
- Weight-Bearing: Typically weight-bearing as tolerated (WBAT) immediately post-operatively, unless specific intra-operative events (e.g., unrecognized femoral fracture, compromised fixation) necessitate restrictions. This is a significant advantage over approaches that might require protected weight-bearing for soft tissue healing.
- Pain Management: Multimodal analgesia is critical, often including regional blocks (e.g., periarticular injection, fascia iliaca block), oral opioids, NSAIDs, and acetaminophen. Effective pain control facilitates early mobilization.
-
Early Mobilization:
- Day 0: Initiate bedside activities such as ankle pumps, quad sets, gluteal sets. Supervised out-of-bed to chair transfers and short ambulation with an assistive device (walker) are encouraged, often within hours of surgery.
- Day 1-3: Progressive ambulation distance and frequency. Focus on proper gait mechanics. Begin gentle active and passive range of motion exercises (flexion, extension, abduction).
- Hip Precautions: Due to the preservation of the posterior capsule and external rotators, traditional hip precautions (avoiding extreme flexion, adduction, internal rotation for posterior approach; or adduction, extension for anterior approach) are often not explicitly mandated following DAA. However, many surgeons advise common sense precautions to avoid extremes of motion, particularly combined extension, adduction, and external rotation, for the initial 6 weeks to allow for soft tissue healing. Patients are generally advised to avoid pivoting on the operative leg or crossing legs.
Early Rehabilitation Phase (Weeks 1-6)
- Assistive Devices: Progress from a walker to crutches or a single cane as strength, balance, and pain control improve.
- Gait Training: Focus on normalizing gait pattern, improving stride length, and minimizing compensatory movements.
-
Strengthening:
- Quadriceps: Straight leg raises (supine, side-lying), quad sets, short-arc quads.
- Gluteals: Gluteal sets, hip abduction (side-lying), bridge exercises, standing hip abduction/extension.
- Core Stability: Gentle core strengthening to support pelvic stability.
- Range of Motion (ROM): Continue working on restoring full hip flexion and extension within comfort. Avoid aggressive stretching initially.
- Functional Activities: Practice stair climbing (leading with the unaffected leg up, affected leg down), car transfers, and safe maneuvering in daily activities.
- Discharge: Most patients are discharged home within 1-3 days, often with home health physical therapy or outpatient physical therapy.
Intermediate Rehabilitation Phase (Weeks 6-12)
- Progressive Strengthening: Advance to resistance exercises (resistance bands, light weights). Incorporate closed-chain exercises (mini-squats, lunges, step-ups).
- Balance and Proprioception: Introduce balance exercises (single-leg stance, unstable surfaces).
- Return to Activities: Gradually return to light recreational activities (e.g., walking for exercise, swimming, cycling on a stationary bike). Avoid high-impact activities or those involving twisting motions.
- Discontinue Assistive Devices: Aim to discontinue all assistive devices if gait is normalized and stability is achieved.
Advanced Rehabilitation Phase (Months 3+)
- Full Strength & Endurance: Continue with progressive strengthening and conditioning exercises.
- Return to Sport: For patients engaged in sports, a gradual, sport-specific return-to-activity program is implemented. Low-impact sports are generally encouraged, while high-impact or contact sports are typically discouraged.
- Lifetime Activity: Encourage a healthy, active lifestyle with regular, appropriate exercise to maintain hip function and overall health.
The key differentiator of DAA rehabilitation is often the rapid progression through the initial phases, leading to a quicker return to functional independence. However, the long-term outcomes in terms of implant longevity and overall function are comparable across different approaches when performed competently. Individual patient factors, comorbidities, and surgeon preference will always influence the specific details of a rehabilitation protocol.
Summary of Key Literature / Guidelines
The literature surrounding the direct anterior approach for THA has expanded exponentially, providing a robust body of evidence for its efficacy and comparative outcomes.
Faster Recovery and Early Outcomes
Numerous meta-analyses and systematic reviews have investigated the claims of faster recovery.
*
Pain:
While initial pain scores may be lower in the immediate post-operative period (first few days to weeks), this difference often diminishes by 6-12 weeks when compared to posterior or lateral approaches. The muscle-sparing nature is hypothesized to contribute to this early pain advantage.
*
Hospital Length of Stay (LOS):
Studies consistently demonstrate a shorter LOS for DAA patients, often aligning with enhanced recovery after surgery (ERAS) protocols. This contributes to lower healthcare costs and improved patient satisfaction.
*
Early Ambulation and Functional Milestones:
Patients undergoing DAA often achieve independent ambulation, stair climbing, and discharge readiness earlier than those via other approaches. This is typically observed in the first 2-6 weeks post-operatively.
*
Gait Biomechanics:
Some studies suggest superior gait kinematics and kinetics in the early post-operative phase with DAA, though long-term differences are less pronounced.
Dislocation Rates
One of the most frequently cited advantages of the DAA is a purported lower dislocation rate.
*
Systematic Reviews:
Meta-analyses have generally reported lower dislocation rates for DAA compared to the posterior approach, and often comparable to or slightly lower than the direct lateral approach. This is attributed to the preservation of the posterior soft tissue structures.
*
Mechanism of Dislocation:
When dislocations do occur after DAA, they are more commonly anterior or anterosuperior, contrasting with the predominantly posterior dislocations seen after a posterior approach.
Complications
As detailed previously, the DAA has a unique profile of potential complications:
*
Nerve Injury:
Higher rates of lateral femoral cutaneous nerve (LFCN) neuropraxia are consistently reported, although most cases are transient and resolve spontaneously. Other nerve injuries (femoral, sciatic) are rare but possible.
*
Femoral Fracture:
The learning curve for DAA is associated with a higher incidence of intraoperative and periprosthetic femoral fractures, particularly during femoral preparation. Experience and specialized instrumentation mitigate this risk.
*
Blood Loss:
Blood loss is generally comparable to or slightly lower than other approaches.
*
Heterotopic Ossification (HO):
Some studies suggest a potentially higher risk of HO with DAA, possibly due to increased muscle trauma despite the "intermuscular" nature, or due to aggressive soft tissue retraction. Prophylaxis is often considered.
Learning Curve
A significant learning curve for the DAA is well-documented. Surgeons new to the technique typically experience:
*
Increased Operative Time:
Longer initial operative times that decrease with experience.
*
Higher Complication Rates:
Elevated rates of LFCN injury, femoral fracture, and other complications during the initial 20-100 cases.
*
Surgeon Volume:
Outcomes tend to improve significantly with increasing surgeon experience and caseload. Institutional guidelines often recommend proctoring and a structured training pathway for surgeons adopting the DAA.
Long-Term Outcomes
- Implant Survival: Long-term implant survival rates for DAA are comparable to those achieved with other established approaches (posterior, lateral). There is no evidence to suggest a superior or inferior long-term prosthetic longevity based solely on surgical approach.
- Functional Outcomes: While early functional advantages are noted, long-term functional outcome scores (e.g., Harris Hip Score, WOMAC) tend to equalize between DAA and other approaches by 1-2 years post-surgery.
Guidelines and Consensus
Professional orthopedic societies, such as the American Academy of Orthopaedic Surgeons (AAOS) and the American Association of Hip and Knee Surgeons (AAHKS), acknowledge the DAA as a viable and effective approach for THA.
* Current guidelines emphasize that the choice of surgical approach should be individualized, considering patient factors, surgeon experience, and specific pathologies.
* The DAA is particularly well-suited for patients seeking accelerated recovery and potentially lower dislocation rates.
* Its integration into ERAS pathways has further solidified its role in modern THA practice.
In conclusion, the minimally invasive direct anterior approach to the hip is a technically demanding but highly effective surgical option for THA, offering distinct advantages in terms of early recovery and potentially reduced dislocation risk, provided the surgeon has overcome the inherent learning curve and adheres to meticulous technique. Its long-term outcomes are comparable to traditional approaches, making it a valuable tool in the armamentarium of the contemporary orthopedic surgeon.
Clinical & Radiographic Imaging


You Might Also Like

