Medial Parapatellar Approach: Comprehensive Surgical Anatomy & Clinical Applications
Key Takeaway
The medial parapatellar approach is the foundational open knee access, vital for arthroplasty, trauma, and complex repairs. It provides versatile exposure, demanding meticulous surgical anatomical understanding. Key aspects include protecting the infrapatellar nerve, understanding the extensor mechanism, and precise dissection through the medial retinaculum.
Medial Parapatellar Approach: Master This Essential Knee Access
Introduction & Epidemiology
The medial parapatellar approach stands as the foundational "workhorse" for open access to the knee joint, a testament to its unparalleled versatility and comprehensive exposure capabilities. While contemporary orthopedic practice has seen the advent and refinement of numerous arthroscopic and minimally invasive techniques, the traditional medial parapatellar arthrotomy remains indispensable for a multitude of complex intra-articular and periarticular procedures. Its robust utility spans across arthroplasty, trauma, sports medicine, and reconstructive surgery.
Historically, this approach evolved from early open knee interventions, providing consistent and reproducible access to critical structures such as the patellofemoral joint, medial and lateral compartments, cruciate ligaments, and suprapatellar pouch. Its enduring relevance is underscored by its continued application in primary total knee arthroplasty (TKA), patellar fracture fixation, complex meniscal repairs requiring open access, synovectomy, and various ligamentous reconstructions.
Epidemiologically, knee pathologies necessitating surgical intervention are vast. Osteoarthritis, the primary driver for TKA, affects millions globally, with projections indicating a substantial increase in surgical demand. Patellar fractures, often resulting from direct trauma, account for approximately 1% of all skeletal injuries. Furthermore, complex intra-articular fractures of the distal femur or proximal tibia, which may require extensive open reduction and internal fixation, frequently utilize an extended version of this approach to facilitate accurate reconstruction and implant placement. The versatility of the medial parapatellar approach allows surgeons to address these diverse pathologies with a single, well-understood incision. While minimally invasive variations have gained traction, particularly in primary TKA, the fundamental principles of the medial parapatellar exposure remain critical for managing unforeseen challenges or cases with significant anatomical distortion or scarring. Mastery of this approach is therefore a cornerstone of competent knee surgery.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy and biomechanics of the anterior knee is paramount for safe and effective utilization of the medial parapatellar approach. The layers encountered during dissection, from superficial to deep, are critical for navigating this region while preserving vital structures.
1. Skin and Subcutaneous Tissue:
The skin incision typically extends from a point proximal to the patella, across its medial border, and distally towards the tibial tubercle. Beneath the skin, the subcutaneous fat contains superficial neurovascular structures. The most critical nerve to identify and protect here is the
infrapatellar branch of the saphenous nerve
. This purely sensory nerve typically crosses the surgical field obliquely from medial to lateral, usually at or distal to the patellar inferior pole. Injury can result in anterior knee numbness or, more significantly, a painful neuroma. Protection through careful dissection and gentle retraction is essential.
2. Extensor Mechanism:
The extensor mechanism comprises the quadriceps femoris muscle group, the quadriceps tendon, the patella, the patellar tendon (ligament), and its insertion into the tibial tubercle.
*
Quadriceps Tendon:
The confluence of the rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius. The medial parapatellar approach involves an incision extending into the medial aspect of the quadriceps tendon or a separation between the vastus medialis and rectus femoris.
*
Patella:
The largest sesamoid bone, critical for extensor mechanism efficiency. Its posterior articular surface is covered by hyaline cartilage.
*
Patellar Tendon:
Connects the patella to the tibial tubercle.
3. Joint Capsule and Synovium:
Deep to the extensor mechanism lies the joint capsule, which is continuous with the periosteum of the distal femur and proximal tibia. The capsule forms the
suprapatellar pouch
proximally, a crucial area for exposure and débridement. The synovial membrane lines the inner surface of the capsule and extends into the joint, forming the intra-articular fat pad (Hoffa's fat pad) distal to the patella.
4. Medial Retinaculum:
This fascial layer provides static stability to the patella. It includes fibers from the vastus medialis, extending to the patella and patellar tendon. Key components include the
medial patellofemoral ligament (MPFL)
, originating from the medial femoral epicondyle and inserting onto the superomedial patella, providing 50-60% of the resistance to lateral patellar displacement. The medial patellotibial ligament also contributes to medial stability. The arthrotomy incision typically passes through the medial retinaculum.
5. Internervous Planes:
The classic medial parapatellar approach does not strictly follow a true internervous plane in the strictest sense as it incises the medial retinaculum. However, the dissection can be considered to proceed between the fascial investments of the vastus medialis obliquus (VMO) and the deeper rectus femoris/vastus intermedius components of the quadriceps, particularly in its more proximal extension. For approaches aiming to be more "quadriceps-sparing" (e.g., subvastus, midvastus), the principle of maintaining the integrity of the VMO insertion is central, utilizing the fascial plane between the VMO and the medial femoral condyle (subvastus) or splitting the VMO muscle fibers (midvastus). The classic medial parapatellar approach, however, often involves a vertical incision extending into the medial aspect of the quadriceps tendon itself, which then separates the vastus medialis from the other quadriceps components.
6. Vascularity:
The geniculate arteries (superior medial and inferior medial) contribute to the rich vascular supply around the knee. While generally not directly transected by the capsular incision, meticulous hemostasis is important, and care should be taken to avoid extensive dissection that might compromise the peripatellar vascular ring.
Biomechanics:
The efficacy of the medial parapatellar approach lies in its ability to facilitate patellar eversion or lateral subluxation, allowing for broad visualization of the trochlear groove, femoral condyles, tibial plateau, and menisci. This maneuver temporarily disrupts the normal patellofemoral articulation. The extent of soft tissue release required for patellar eversion can impact post-operative patellar tracking. Excessive medial release, or an overly tight closure, can alter extensor mechanism alignment and contribute to patellofemoral pain or instability. Minimally invasive approaches aim to preserve the extensor mechanism by avoiding patellar eversion, which, while reducing post-operative pain and improving early functional recovery, can limit visualization, particularly of the distal femoral cut in TKA, and necessitate advanced imaging or navigation for accurate implant positioning.
Indications & Contraindications
The medial parapatellar approach is a highly versatile incision, indicated for a broad spectrum of knee pathologies requiring open surgical access. Its indications reflect its capacity to provide comprehensive exposure to the anterior, medial, and central compartments of the knee.
Indications
-
Total Knee Arthroplasty (TKA):
- Primary TKA for osteoarthritis, inflammatory arthritis, or post-traumatic arthritis.
- Certain revision TKAs where extensive exposure is required, though more extensile approaches (e.g., V-Y quadriceps plasty, tibial tubercle osteotomy) may be necessary for complex revisions.
-
Patellar Fractures:
- Open reduction and internal fixation (ORIF) of displaced patellar fractures (e.g., transverse, comminuted, pole fractures).
- Patellectomy (partial or complete) in cases of severe comminution or non-reconstructible fractures.
-
Distal Femur & Proximal Tibia Fractures:
- Selected intra-articular or juxta-articular fractures of the distal femur requiring ORIF, particularly those with a significant sagittal component or extension into the trochlear groove.
- Proximal tibia fractures (tibial plateau fractures), especially those involving the medial plateau or requiring anterior column visualization, although lateral approaches are more common for lateral plateau fractures.
-
Ligamentous Reconstruction:
- Medial Patellofemoral Ligament (MPFL) Reconstruction: Although often performed through smaller, targeted incisions, the medial parapatellar approach can be utilized, particularly if other intra-articular procedures are concurrent or if wider exposure is deemed beneficial.
- Anterior Cruciate Ligament (ACL) or Posterior Cruciate Ligament (PCL) Reconstruction: Historically, this approach provided access for graft harvest and tunnel drilling. Modern arthroscopic techniques have largely superseded open approaches for primary cruciate ligament reconstruction, but the parapatellar approach can be used for open reconstructions or for managing specific complications requiring open exposure.
-
Meniscal Repair/Meniscectomy:
- While most meniscal pathology is managed arthroscopically, complex meniscal repairs, large bucket-handle tears, or cases requiring meniscal transplantation may occasionally benefit from limited open access via a small parapatellar incision, often in conjunction with arthroscopy.
-
Synovectomy:
- For inflammatory arthropathies (e.g., rheumatoid arthritis, PVNS) or other conditions requiring extensive synovial débridement.
-
Removal of Loose Bodies or Chondral Débridement:
- For larger or multiple loose bodies, or extensive chondral lesions requiring debridement, microfracture, or osteochondral grafting not amenable to arthroscopic management.
-
Correction of Patellofemoral Malalignment:
- Procedures such as tibial tubercle osteotomy (e.g., Elmslie-Trillat, Fulkerson) for patellar instability or anterior knee pain, often performed via a modified medial parapatellar skin incision.
-
Biopsy or Excision of Intra-articular Lesions:
- For suspicious intra-articular masses or lesions requiring excisional biopsy.
-
Infection Débridement:
- Septic arthritis unresponsive to arthroscopic lavage, or in cases of severe joint destruction requiring open débridement.
Contraindications
- Prior Surgery with Lateral Approach: Significant scarring or compromised soft tissue envelope from previous lateral surgical approaches may render a medial parapatellar approach suboptimal or increase the risk of wound complications.
- Severe Cutaneous Compromise: Active infection, significant burns, dermatitis, or severely compromised skin integrity over the anterior knee.
- Vascular Impairment: Severe peripheral vascular disease compromising local tissue viability.
- Extensive Patella Baja: In cases of severe patella baja (inferior patellar position), exposure of the trochlea and proximal tibia can be significantly limited, potentially necessitating an extensile approach like a V-Y quadriceps plasty or tibial tubercle osteotomy.
- Isolated Lateral Compartment Pathology: While versatile, if pathology is strictly confined to the lateral compartment and accessible via a less invasive or lateral approach, a medial parapatellar incision may be unnecessarily extensive.
- Patient Inability to Tolerate Anesthesia: General contraindications to surgery.
Table: Operative vs. Non-Operative Indications
| Condition | Operative Management (often via Medial Parapatellar Approach) | Non-Operative Management (Approach NOT Indicated) |
|---|---|---|
| Knee Osteoarthritis | Advanced stages requiring Total Knee Arthroplasty (TKA) | Early to moderate stages, pain controllable with NSAIDs, PT, injections |
| Patellar Fracture | Displaced or comminuted fractures | Non-displaced, stable fractures amenable to immobilization |
| Distal Femur/Proximal Tibia Fractures | Displaced intra-articular fractures, open fractures | Non-displaced, stable extra-articular fractures |
| Patellofemoral Instability | Recurrent dislocations, failed conservative management, significant malalignment | First-time dislocation, conservative management with bracing & PT |
| Meniscal Tears | Large, unstable tears (e.g., bucket-handle), tears in vascular zone suitable for repair | Small, stable tears, degenerative tears in avascular zone (symptomatic) |
| Intra-articular Loose Bodies | Symptomatic loose bodies causing locking or pain | Asymptomatic loose bodies |
| Septic Arthritis | Persistent infection after aspiration/arthroscopy, severe destruction | Early stage, responsive to aspiration & antibiotics |
| Intra-articular Tumors/Masses | Symptomatic or suspicious lesions requiring biopsy/excision | Asymptomatic, benign lesions under surveillance |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and precise patient positioning are critical determinants of a successful outcome when employing the medial parapatellar approach. These steps ensure optimal exposure, minimize complications, and facilitate efficient surgery.
Pre-Operative Planning
- Clinical Assessment: A comprehensive history and physical examination are foundational. Assess skin integrity, range of motion, neurovascular status, and identify any pre-existing deformities or scars.
-
Radiographic Evaluation:
- Standard X-rays: Anteroposterior (AP), lateral, and patellar skyline views are essential for assessing joint space, alignment, patellar position (patella alta/baja), and the nature of fractures or osteoarthritic changes.
- Full-Length Mechanical Axis Views: Crucial for TKA planning to evaluate coronal and sagittal plane deformities and determine component sizing and alignment.
- Stress Views: May be useful for assessing ligamentous instability.
- Computed Tomography (CT) Scan: Indicated for complex intra-articular fractures (e.g., patellar, distal femur, tibial plateau) to delineate fracture patterns, articular involvement, and guide reduction strategies. Also valuable for assessing rotational alignment in TKA or for complex patellofemoral issues.
- Magnetic Resonance Imaging (MRI): Useful for evaluating soft tissue pathology (meniscus, ligaments, cartilage, synovial lesions), particularly when arthroscopy is not initially planned or if the open approach needs to address specific soft tissue findings.
- Templating: For TKA, pre-operative templating using radiographs or digital templating software helps predict implant size, resections, and component placement, thereby streamlining the intra-operative process.
- Anesthetic Consultation: Discuss patient comorbidities, anesthetic options (general, spinal, epidural), and pain management strategies.
- Informed Consent: Clearly explain the procedure, expected outcomes, and potential complications specific to the medial parapatellar approach, including nerve injury, wound issues, stiffness, and patellofemoral dysfunction.
- Equipment and Implant Preparation: Ensure all necessary instruments, retractors, and implants (e.g., TKA components, fracture fixation hardware) are available and sterilized. For TKA, specific navigation or robotic systems may be integrated into the planning.
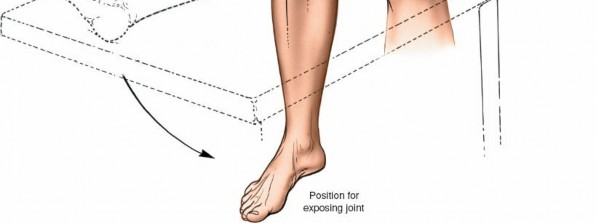
Patient Positioning
- Supine Position: The patient is positioned supine on the operating table. This allows for excellent access to the anterior aspect of the knee.
- Tourniquet Application: A pneumatic tourniquet is routinely applied high on the thigh. Inflation prior to incision minimizes blood loss and improves visualization. The limb should be exsanguinated using an Esmarch bandage before inflation.
-
Leg Holder vs. Free-Draping:
- Leg Holder: Often used in TKA to stabilize the femur and allow controlled flexion and extension during bony resections and gap balancing.
- Free-Draping: If a leg holder is not used, the foot of the table is typically dropped to allow full knee flexion. The limb is often draped free (e.g., using a stockinette and impervious drape) to permit manipulation of the knee through a full range of motion, which is crucial for assessing stability, patellar tracking, and implant fit, especially in revision cases or for fracture fixation.
- Sterile Preparation and Draping: The entire leg, from the tourniquet to the toes, is meticulously prepared with an antiseptic solution (e.g., povidone-iodine or chlorhexidine) and then sterilely draped to isolate the operative field.
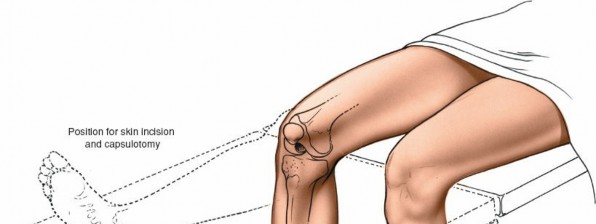
- Patellar Position: The knee should be slightly flexed (15-30 degrees) or in full extension initially to facilitate the skin incision. Adjustments will be made throughout the procedure. Adequate padding for the heels, sacrum, and upper extremities is crucial to prevent pressure injuries. The ipsilateral hip may be slightly abducted and externally rotated for optimal surgical field ergonomics.
Detailed Surgical Approach / Technique
The medial parapatellar approach is a systematic dissection that provides extensive access to the knee joint. Adherence to a methodical sequence ensures comprehensive exposure while minimizing damage to critical structures.
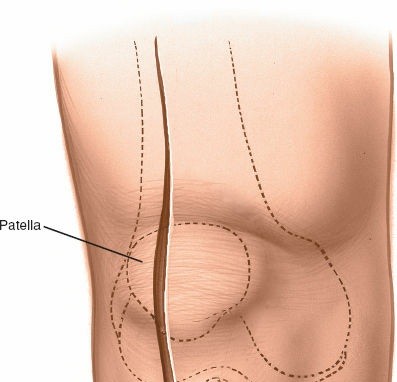
1. Skin Incision
The incision typically begins approximately 3-5 cm proximal to the superior pole of the patella, curves slightly medially along the patellar border, and extends distally parallel to the medial border of the patellar tendon, terminating approximately 2-3 cm distal to the tibial tubercle. A straight midline longitudinal incision is an alternative, particularly when combined with a medial parapatellar capsular approach for TKA, offering a large exposure. The length and curvature of the incision are tailored to the specific procedure and patient anatomy.
Initial skin incision marked, extending proximally along the quadriceps, medially to the patella, and distally along the patellar tendon.
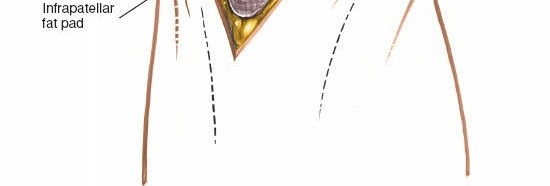
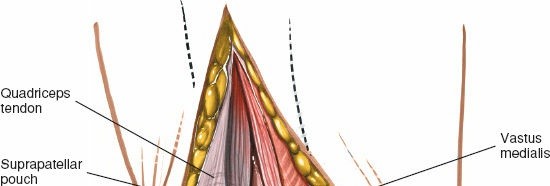
2. Subcutaneous Dissection
- The skin and subcutaneous tissues are incised.
- Careful dissection is performed to identify and protect the infrapatellar branch of the saphenous nerve . This nerve typically courses obliquely across the anterior knee, often near the distal extent of the patella or patellar tendon. It lies within the subcutaneous fat and should be identified and carefully retracted, ideally preserved intact, to minimize post-operative dysesthesia or neuroma formation.
-
Electrocautery is used for hemostasis of superficial vessels. The fat pad (prepatellar bursa) is encountered.
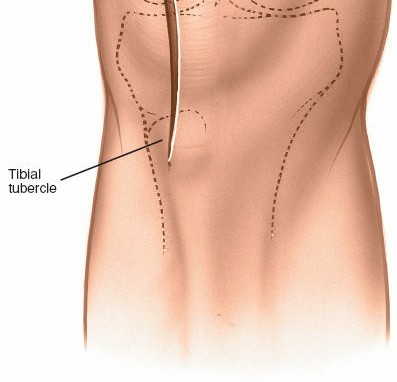
Deepening the incision through subcutaneous fat, exposing the retinaculum and the patella. The infrapatellar branch of the saphenous nerve should be carefully protected.
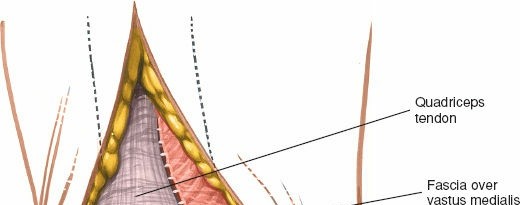
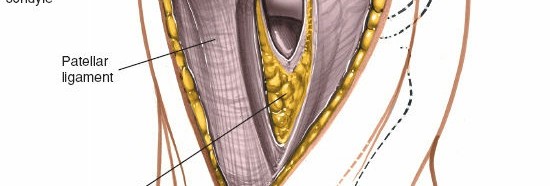
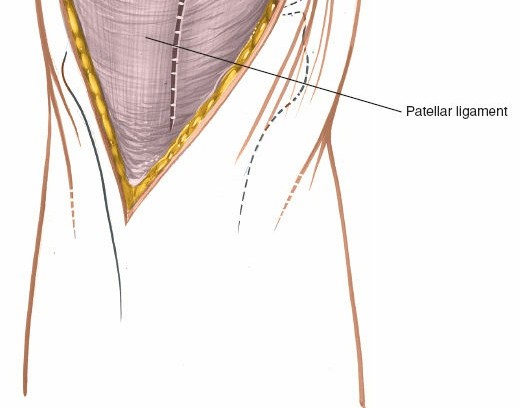
3. Medial Parapatellar Arthrotomy (Capsular Incision)
This is the defining step of the approach.
* The incision through the joint capsule and retinaculum begins proximally, extending through the medial aspect of the quadriceps tendon.
* It then follows the border between the vastus medialis obliquus (VMO) and the patella, curving distally along the medial border of the patella.
* The incision continues distal to the patella, medial to the patellar tendon, into the synovium and capsule.
* The extent of the proximal and distal incision depends on the required exposure. For TKA, it is typically extended well into the quadriceps tendon proximally and to the tibial tubercle distally.

The medial retinaculum and vastus medialis obliquus are exposed. The proposed capsular incision along the medial patellar border is outlined.
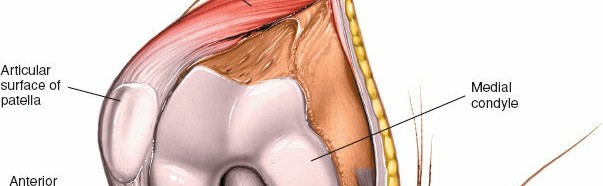
4. Patellar Eversion/Subluxation
Once the arthrotomy is complete, the patella is typically everted laterally or subluxated to gain full access to the trochlear groove, femoral condyles, tibial plateau, and menisci.
*
Traditional Approach (Patellar Eversion):
The patella is gently grasped and everted laterally, typically by flexing the knee to facilitate this maneuver. This provides excellent visualization of all compartments.
Initial stages of patellar eversion, showing retraction of the medial soft tissues and initiation of lateral displacement of the patella.
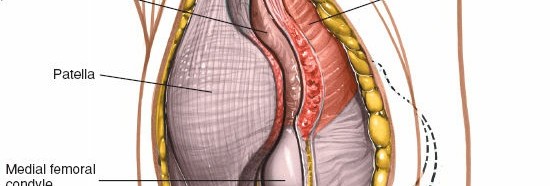
Further lateral displacement of the patella, demonstrating improved exposure of the trochlear groove and femoral condyle.

Full patellar eversion, offering wide access to the intra-articular structures of the knee, including the femoral condyles and tibial plateau.
*
Minimally Invasive Approaches (Patellar Non-Eversion/Lateral Subluxation):
In some minimally invasive TKA techniques, the patella is not fully everted but rather laterally subluxated or merely retracted. This aims to preserve the extensor mechanism. While reducing surgical trauma, it can significantly limit visualization, particularly of the distal femur and posterior aspects of the joint. Advanced imaging, computer-assisted surgery (CAS), or robotic guidance systems may be beneficial to ensure accurate implant positioning in these scenarios.
Example of exposure with patella subluxated rather than fully everted, typically employed in minimally invasive techniques.
5. Exposure of Joint Structures
- With the patella everted, the suprapatellar pouch is accessible. This is often adherent in osteoarthritic knees and requires sharp dissection to release adhesions and fully visualize the distal femur.
- The fat pad (Hoffa's fat pad) lies anterior to the intercondylar notch. It may be partially resected if it obstructs visualization, though excessive resection can contribute to anterior knee pain.
-
Retractors are strategically placed to maintain exposure of the femoral condyles, tibial plateau, menisci, and cruciate ligaments.

Detailed view of the exposed knee joint after patellar eversion. The menisci, articular cartilage, and cruciate ligaments are visible.
6. Internervous Planes & Tissue Handling
The classic medial parapatellar approach involves an incision through the retinaculum and quadriceps tendon. While not a true internervous plane like some muscle-sparing approaches, careful dissection within the tissues of the extensor mechanism is important.
*
Vastus Medialis Obliquus (VMO):
The incision often passes through the VMO or at its periphery. Preserving as much of the VMO insertion onto the patella as possible is desirable to maintain patellar tracking stability.
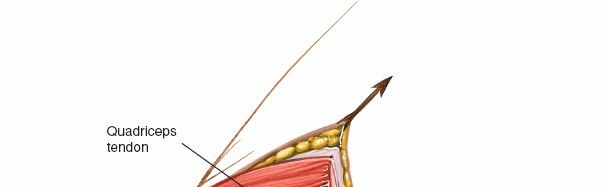
*
Quadriceps Tendon:
The proximal extension of the arthrotomy enters the quadriceps tendon. A limited "quadriceps snip" can aid in patellar eversion without significantly weakening the tendon.

Proximal extension of the arthrotomy, showing incision into the quadriceps tendon to facilitate further exposure.
7. Performing the Specific Procedure
-
Total Knee Arthroplasty (TKA):
Once exposed, the distal femoral and proximal tibial bone cuts are performed, often guided by intramedullary or extramedullary alignment systems. Ligament balancing is then achieved through sequential releases.
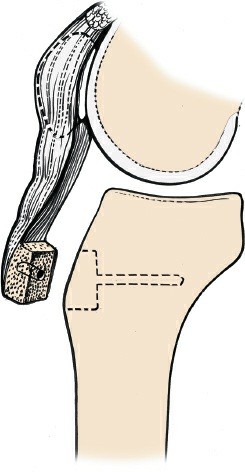
Initial bone cuts in Total Knee Arthroplasty, demonstrating the precise surgical field achieved with the medial parapatellar approach.
Further bone resections in TKA, highlighting the unobstructed view for accurate jig placement and cutting. - Fracture Fixation: Reduction of fracture fragments under direct visualization, followed by temporary fixation with K-wires, then definitive fixation with plates, screws, or cerclage wires as dictated by the fracture pattern.
- Meniscal/Ligament Surgery: Direct repair, excision, or reconstruction of specific structures.
8. Closure
A meticulous, layered closure is essential to restore joint integrity and extensor mechanism function.
*
Capsular/Retinacular Repair:
The arthrotomy is closed with a strong, interrupted, or running non-absorbable or slowly absorbable suture. Particular attention is paid to reapproximating the medial patellofemoral ligament and the quadriceps tendon components. This step is critical for restoring patellar tracking and joint stability.

Initiation of the capsular and retinacular repair, showing initial suture placement for primary closure of the arthrotomy.
Progress of the capsular repair, carefully reapproximating the medial soft tissues to restore patellar tracking and joint integrity.
*
Subcutaneous Closure:
The subcutaneous layer is closed with absorbable sutures to obliterate dead space and reduce tension on the skin incision.
*
Skin Closure:
The skin is closed with staples, sutures, or adhesive strips, ensuring proper eversion of the skin edges.
Subcutaneous closure, demonstrating careful tissue apposition to minimize dead space and support the skin layer.
Final skin closure with staples, ensuring a well-approximated wound with appropriate tension.
* A sterile dressing is applied, and often a compression bandage or knee immobilizer is used depending on the procedure and surgeon preference.

Application of a sterile dressing to the closed incision site.
Final external bandage applied, providing compression and protection to the operative knee.
Complications & Management
While the medial parapatellar approach is a reliable and safe surgical access, it is not without potential complications. Awareness of these issues and strategies for their prevention and management are crucial for optimal patient care.
General Surgical Complications
These are risks inherent to any open surgical procedure:
*
Infection:
Superficial or deep wound infection.
*
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
Thromboembolic events.
*
Neurovascular Injury:
Although rare with this approach, direct injury to major vessels or nerves.
*
Anesthetic Complications:
Related to the chosen anesthesia method.
*
Systemic Complications:
Cardiac events, pneumonia, renal failure, etc., particularly in elderly or comorbid patients.
Specific Complications of the Medial Parapatellar Approach
The nature of the dissection and exposure carries specific risks:
-
Extensor Mechanism Compromise:
- Patellar Fracture: Can occur intra-operatively during patellar eversion or post-operatively, especially in osteoporotic bone or with aggressive manipulation.
- Patellar Tendon Rupture: Rare but devastating, often due to excessive tension or prior degeneration.
- Quadriceps Tendon Rupture: Similar to patellar tendon rupture, often linked to excessive force or compromised tissue.
- Patellofemoral Instability/Maltracking: Excessive medial release can lead to lateral patellar subluxation or dislocation. Inadequate closure or overtight medial structures can lead to patellofemoral pain or stiffness.
-
Neurological Injury:
- Infrapatellar Branch of the Saphenous Nerve (IPBSN) Injury: The most common nerve injury, leading to an area of numbness on the anterior aspect of the knee. Can result in a painful neuroma, affecting approximately 10-20% of patients.
-
Wound Healing Issues:
- Wound Dehiscence / Necrosis: Compromised blood supply, excessive tension, or infection can lead to delayed healing or wound breakdown. More common in patients with diabetes, obesity, or vascular disease.
- Hematoma/Seroma: Accumulation of blood or serous fluid in the wound, which can increase infection risk and delay healing.
-
Arthrofibrosis / Stiffness:
- Post-operative scarring within the suprapatellar pouch or around the patella can lead to a significant loss of knee flexion and extension. This is more prevalent in cases of prolonged immobilization, inadequate rehabilitation, or underlying inflammatory conditions.
-
Heterotopic Ossification (HO):
- Aberrant bone formation in soft tissues, particularly within the quadriceps mechanism, can restrict range of motion. Incidence is variable but typically low for primary TKA.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Infrapatellar Branch Nerve Injury | 10-20% symptomatic paresthesia/neuroma |
Prevention:
Careful subcutaneous dissection, identification, and protection/retraction.
Management: Conservative (NSAIDs, desensitization) for paresthesia. If persistent painful neuroma, local anesthetic injections, neurolysis, or neurectomy may be considered. |
| Wound Infection | 0.5-2% for primary TKA (deep) |
Prevention:
Meticulous aseptic technique, prophylactic antibiotics, careful tissue handling, optimal glycemic control.
Management: Superficial: wound care, oral antibiotics. Deep: surgical débridement, irrigation, retention vs. removal of implants (depending on type of surgery/stability), IV antibiotics. May require multiple debridements or staged reconstruction. |
| Arthrofibrosis / Stiffness | 5-10% (requiring manipulation/lysis) |
Prevention:
Early, aggressive rehabilitation, adequate pain control.
Management: Intensive physical therapy, dynamic splinting. If conservative measures fail (often after 3-6 months), surgical manipulation under anesthesia, arthroscopic or open lysis of adhesions (arthrolysis) to restore range of motion. For severe cases, revision arthroplasty may be considered if implant malposition or failure is a contributing factor. |
| Patellar Fracture | 0.5-1.5% in TKA |
Prevention:
Avoid excessive force during eversion, careful patellar preparation (TKA).
Management: Non-displaced: immobilization. Displaced: ORIF (tension band wiring, screws, partial patellectomy). Total patellectomy for severe comminution. |
| Patellofemoral Instability/Maltracking | <1% (lateral dislocation/subluxation) |
Prevention:
Balanced soft tissue release and tensioning, meticulous capsular closure.
Management: Conservative for mild maltracking. If recurrent instability or significant pain, consider patellofemoral realignment procedures (e.g., lateral retinacular release, medial plication, tibial tubercle transfer) or revision arthroplasty if component malposition is identified. |
| Hematoma/Seroma | 5-10% |
Prevention:
Meticulous hemostasis, drain placement (controversial for TKA).
Management: Aspiration (if symptomatic/large), wound compression. Surgical evacuation if large or infected. |
| DVT/PE | <1% with prophylaxis |
Prevention:
Early mobilization, mechanical and/or pharmacological prophylaxis (anticoagulation).
Management: Anticoagulation, inferior vena cava filter for recurrent PE or contraindication to anticoagulation. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following a medial parapatellar approach is paramount for restoring knee function, minimizing complications, and achieving optimal long-term outcomes. Protocols are tailored to the specific surgical procedure performed (e.g., TKA, fracture fixation, soft tissue repair) and patient factors, but general principles apply.
Immediate Post-Operative Phase (Days 0-7)
- Pain Management: Multimodal analgesia (NSAIDs, acetaminophen, nerve blocks, opioids) to facilitate early mobilization.
- Wound Care: Maintain a sterile, dry dressing. Monitor for signs of infection or hematoma. Drain removal typically within 24-48 hours.
-
Weight-Bearing:
- TKA: Typically weight-bearing as tolerated (WBAT) with assistive devices (walker, crutches) immediately post-op.
- Patellar Fracture/Complex Fractures: Often non-weight bearing (NWB) or touch-down weight bearing (TDWB) in a brace for 4-8 weeks, depending on fracture stability and fixation strength.
-
Range of Motion (ROM):
- TKA: Early, continuous passive motion (CPM) may be used (controversial evidence), but active-assisted and active ROM exercises are key. Aim for 0-90 degrees flexion by day 3-5.
- Fracture Fixation: Often restricted initially, with a hinged knee brace controlling flexion (e.g., 0-30 degrees initially) to protect the repair.
- Quadriceps Activation: Isometric quadriceps sets are initiated immediately to prevent atrophy and maintain patellar mobility.
- Edema Control: Elevation, compression stockings, and cryotherapy to reduce swelling.
- DVT Prophylaxis: Continue pharmacological and mechanical prophylaxis.
Early Rehabilitation Phase (Weeks 1-6)
- Progressive ROM: Gradually increase flexion and extension. For TKA, aim for >100-110 degrees of flexion by week 4-6, with full extension.
-
Strengthening:
- Quadriceps: Progress from isometric to isotonic exercises (e.g., straight leg raises, mini-squats, partial lunges) in pain-free range.
- Hamstrings & Gluteals: Strengthen these supporting muscle groups.
- Patellar Mobilization: Gentle patellar glides (medial, lateral, superior, inferior) to prevent adhesions and maintain patellofemoral mobility.
- Gait Training: Progress from assistive devices to independent ambulation as strength and balance improve. Focus on normalized gait pattern.
- Scar Management: Gentle massage once the wound is well-healed to minimize adhesions.
- Fracture-specific: X-rays typically taken at 4-6 weeks to assess fracture healing before advancing weight-bearing or ROM.
Intermediate Rehabilitation Phase (Weeks 6-12)
- Advanced Strengthening: Incorporate closed-chain exercises, functional training (stair climbing, balance exercises), and light resistance training.
- Proprioception & Balance: Single-leg stance, wobble board exercises.
- Endurance Training: Stationary cycling, swimming.
- Return to Activities: Gradually introduce low-impact activities. For TKA, typically return to normal daily activities. For fracture patients, gradual increase in weight-bearing and functional load as bone healing progresses.
Advanced Rehabilitation & Return to Sport (Weeks 12+)
- High-Level Strengthening: Progress to higher resistance and advanced functional exercises.
- Sport-Specific Training: For athletes, incorporate agility, plyometrics, and sport-specific drills, ensuring adequate strength, power, and neuromuscular control.
- Gradual Return to Sport: Phased return to high-impact or competitive sports, typically 6-12 months post-surgery for complex knee injuries or revisions, after meeting objective criteria for strength, balance, and agility. For TKA, high-impact activities are generally discouraged.
- Long-Term Maintenance: Encourage ongoing exercise and healthy lifestyle to maintain strength, flexibility, and joint health.
Key Considerations:
*
Individualization:
Protocols must be individualized based on patient factors (age, co-morbidities, pre-operative function), surgical findings, and the specific procedure.
*
Communication:
Close collaboration between the surgeon, physical therapist, and patient is crucial for success.
*
Complications:
Early identification and management of complications like arthrofibrosis, infection, or extensor mechanism weakness are vital.
Summary of Key Literature / Guidelines
The medial parapatellar approach has been extensively studied and documented, forming the cornerstone of many open knee procedures. Key literature and guidelines reflect its utility, evolution, and ongoing refinement.
1. Foundational Work & Total Knee Arthroplasty (TKA):
The efficacy and predictability of the medial parapatellar approach for TKA are well-established. Early studies by Insall, Ranawat, and Coventry laid the groundwork for modern TKA, and this approach was integral to their techniques. These works highlighted the excellent visualization it provides for component sizing, bone cuts, and soft tissue balancing, leading to reproducible results in addressing varus and valgus deformities. Randomized controlled trials and systematic reviews consistently demonstrate its reliability for primary TKA, achieving favorable long-term outcomes in terms of pain relief and functional improvement.
2. Evolution Towards Minimally Invasive Approaches (MIA):
The late 1990s and early 2000s saw a surge of interest in MIA for TKA, aimed at reducing surgical morbidity, accelerating recovery, and improving patient satisfaction. The seed content correctly notes that such approaches often involve avoiding full patellar eversion.
*
Quadriceps-Sparing Approaches:
The subvastus and midvastus approaches emerged as alternatives to the classic medial parapatellar, attempting to preserve the quadriceps mechanism. Studies comparing MIA (including quad-sparing techniques) to traditional approaches have shown mixed results. While some demonstrate faster short-term recovery, reduced pain, and earlier discharge, long-term functional outcomes are often comparable.
*
Challenges of MIA:
A consistent finding in the literature is the compromise in surgical exposure with MIA, particularly for visualizing the posterior condyles and distal femoral cuts. This has led to concerns about potential implant malposition, especially in less experienced hands or complex deformities. The use of advanced technologies like
computer-assisted surgery (CAS)
and
robotics
has been explored to mitigate these visualization limitations and improve accuracy with MIA, with growing evidence supporting their role in enhancing precision and reducing outliers in component alignment.
3. Patellofemoral Considerations:
The impact of the medial parapatellar approach on the patellofemoral joint has been a recurring theme. Studies investigate the effect of medial retinacular release, patellar eversion, and closure techniques on patellar tracking and anterior knee pain. While the approach itself involves incision of the medial retinaculum, careful repair is crucial to restore native patellar kinematics. Persistent patellofemoral pain or instability post-TKA, though multifactorial, can sometimes be linked to issues related to patellar tracking influenced by the surgical approach or component malposition.
4. Complications and Risk Mitigation:
Literature extensively covers complications such as wound healing issues, infection, and neurological injury (e.g., infrapatellar branch of the saphenous nerve). Studies emphasize meticulous tissue handling, strict aseptic technique, and careful identification and protection of the IPBSN to minimize these risks. The incidence of infrapatellar nerve neuroma, while relatively low, remains a recognized drawback. Efforts to prevent arthrofibrosis through early and aggressive rehabilitation are also a consistent recommendation across various surgical guidelines.
5. Guidelines and Recommendations:
Major orthopedic societies (e.g., AAOS, AAHKS) acknowledge the medial parapatellar approach as a standard and effective method for TKA and other open knee surgeries. While there is increasing adoption of minimally invasive techniques, the consensus is that the choice of approach should be based on surgeon experience, patient anatomy, and the complexity of the pathology. For complex primary TKAs, revisions, or cases with significant deformity or scarring, the comprehensive exposure offered by the medial parapatellar approach often remains the preferred option. The literature supports that regardless of the skin incision or capsular approach, precision in bone cuts, ligament balancing, and meticulous soft tissue handling are the ultimate determinants of long-term success. The medial parapatellar approach, when mastered, provides the most reliable pathway to achieve these critical surgical goals.
Clinical & Radiographic Imaging
You Might Also Like