Medial Approach to the Knee: Comprehensive Anatomy, Biomechanics, and Surgical Foundations
Key Takeaway
The medial approach to the knee provides essential access for orthopedic surgeons to repair and reconstruct crucial ligamentous and capsular structures. It details the superficial and deep medial collateral ligaments (sMCL, dMCL), posterior oblique ligament (POL), and medial meniscus. Understanding its complex anatomy and biomechanics is fundamental for addressing medial knee instabilities.
Mastering the Medial Approach to the Knee and Its Supporting Structures
Introduction & Epidemiology
The medial approach to the knee provides unparalleled access to the complex ligamentous and capsular structures comprising the medial compartment and posteromedial corner. This approach is fundamental for orthopedic surgeons addressing a spectrum of pathologies, ranging from acute traumatic injuries to chronic instabilities and degenerative conditions affecting this region. While historically utilized for meniscectomy, its modern application predominantly centers on the comprehensive evaluation, repair, and reconstruction of the superficial medial collateral ligament (sMCL), deep medial collateral ligament (dMCL), and posterior oblique ligament (POL), collectively integral to medial knee stability. Furthermore, it offers a pathway for addressing concomitant medial meniscal pathology, osteochondral lesions, and, in specific contexts, serves as an adjunct for anterior cruciate ligament (ACL) reconstruction with associated medial-sided injuries.
Medial knee injuries are prevalent, particularly in athletic populations. Isolated MCL injuries are the most common knee ligamentous injury, with estimates suggesting an incidence of 2.5 per 1000 person-years. These injuries often result from a valgus stress applied to a partially flexed knee. While Grade I and II sprains typically respond to non-operative management, Grade III tears, especially those involving the posteromedial corner or in conjunction with cruciate ligament injuries (e.g., "unhappy triad"), frequently necessitate surgical intervention. Chronic valgus instability or complex multi-ligamentous injuries further expand the indications for meticulous surgical exposure and management via the medial approach. A thorough understanding of the anatomical nuances and biomechanical contributions of each medial structure is paramount for effective surgical planning and execution.
Surgical Anatomy & Biomechanics
A precise understanding of the medial knee anatomy is critical for safe and effective utilization of this approach. The medial compartment is characterized by distinct layers and a complex interplay of static and dynamic stabilizers.
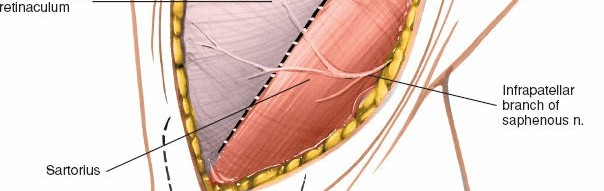
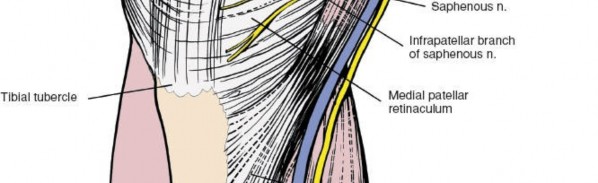
- Skin and Subcutaneous Tissue: The most superficial layers. Care must be taken to identify and protect the great saphenous vein and the saphenous nerve (and its infrapatellar branch), which course anteromedially. The saphenous nerve typically lies anterior to the sartorius muscle and posterior to the saphenous vein at the level of the knee joint.
- Deep Fascia (Fascia Lata): Inferiorly, this contributes to the pes anserinus expansion.
- Pes Anserinus: Composed of the conjoint tendons of the sartorius , gracilis , and semitendinosus muscles. These tendons insert onto the anteromedial aspect of the proximal tibia, superficial to the MCL. The anserine bursa lies beneath these tendons. These muscles provide dynamic medial stability.
-
Superficial Medial Collateral Ligament (sMCL):
The primary static restraint to valgus stress, particularly at 25-30 degrees of knee flexion. It is a broad, flat ligament with distinct femoral and tibial attachments.
- Femoral Attachment: Proximal and posterior to the medial epicondyle, beneath the adductor tubercle.
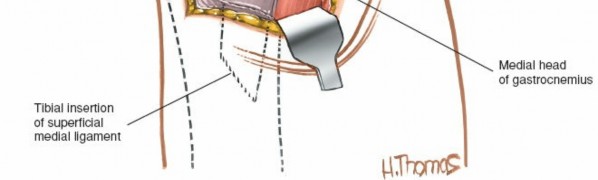
- Tibial Attachment: Distal to the joint line, approximately 5-7 cm from the tibial plateau, posterior to the pes anserinus insertion. It has a superficial, distal attachment and a deeper, more proximal attachment that blends with the capsule.
-
Deep Medial Collateral Ligament (dMCL):
This is a thickening of the joint capsule, intimately attached to the medial meniscus. It consists of two components:
- Meniscofemoral Ligament: Connects the medial meniscus to the medial femoral condyle.
-
Meniscotibial Ligament (Coronary Ligament):
Connects the medial meniscus to the medial tibial plateau.
The dMCL provides secondary restraint to valgus stress and plays a crucial role in internal and external rotation stability.
-
Posterior Oblique Ligament (POL):
A complex, fan-shaped capsular thickening forming a critical component of the posteromedial corner (PMC). It has three distinct components:
- Superficial Arm: Blends with the semimembranosus tendon expansion and attaches to the posteromedial tibia.
- Central Arm: The stoutest portion, inserting on the posterior aspect of the semimembranosus tendon capsule.
-
Capsular Arm:
Blends directly with the posterior joint capsule.
The POL is a key stabilizer against valgus stress in extension and posteromedial rotatory instability.
- Medial Meniscus: A C-shaped fibrocartilaginous structure increasing contact area and absorbing shock. Its firm attachments to the dMCL are relevant for pathology and surgical considerations. The anterior horn attaches to the tibia anterior to the sMCL, and the posterior horn attaches posterior to the dMCL.
- Semimembranosus Tendon: Its intricate relationship with the POL and posteromedial capsule is vital. Multiple tendinous expansions contribute to dynamic stability of the posteromedial corner and often require careful identification and protection during dissection.
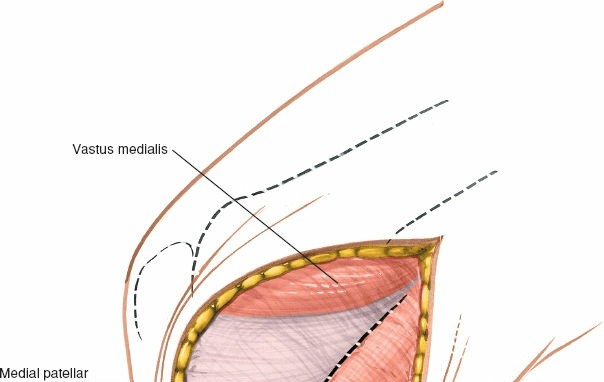
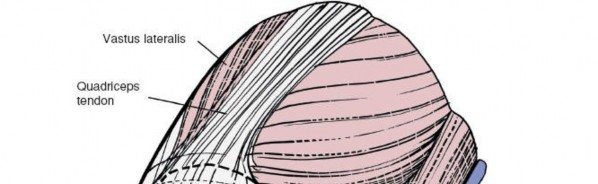
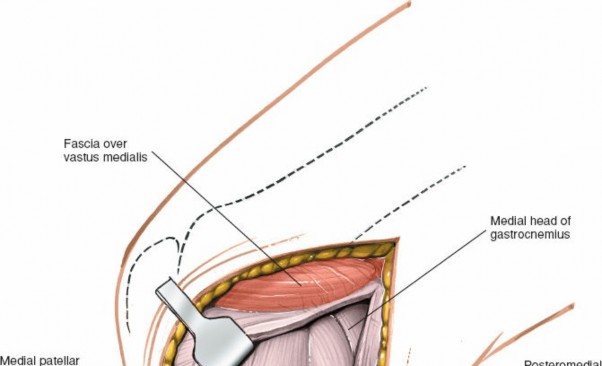
- Vastus Medialis Obliquus (VMO): The most distal part of the quadriceps muscle, inserts onto the medial border of the patella and contributes to medial patellar stability. It forms the anterior border of the surgical field.
Biomechanics:
The medial knee primarily resists valgus forces and external rotation of the tibia.
*
Valgus Stability:
The sMCL is the primary restraint at 20-30 degrees of flexion, with the dMCL and POL acting as secondary restraints. In full extension, the POL, posterior capsule, and cruciates provide significant stability.
*
Rotational Stability:
The POL and dMCL contribute significantly to preventing external rotation of the tibia, especially when combined with valgus stress (posteromedial rotatory instability). The semimembranosus muscle acts as a dynamic stabilizer.
A comprehensive understanding of these structures' individual and synergistic functions is essential for accurate diagnosis and successful surgical restoration of knee stability.
Indications & Contraindications
The medial approach offers versatility for addressing a range of pathologies. Careful patient selection and comprehensive pre-operative assessment are paramount.
Indications
-
Grade III Medial Collateral Ligament (MCL) Tears:
- Acute, complete ruptures, particularly when associated with valgus instability greater than 10-15 mm at 20-30 degrees of knee flexion, or an opening in full extension (indicating posteromedial corner involvement).
- Proximal avulsions from the femoral origin.
- Concomitant injuries to the ACL or PCL ("unhappy triad," multi-ligamentous injuries).
-
Posteromedial Corner (PMC) Injuries:
- Disruption of the Posterior Oblique Ligament (POL), often in combination with sMCL tears, leading to posteromedial rotatory instability.
- Avulsions of the semimembranosus tendon expansions.
-
Medial Meniscal Pathology:
- Complex medial meniscal tears requiring direct visualization for repair (e.g., ramp lesions, meniscocapsular separations, root tears).
- Meniscectomy for irreparable tears or when associated with significant ligamentous instability requiring open repair.
-
Chronic Medial-Sided Instability:
- Persistent valgus instability or posteromedial rotatory instability despite non-operative management or failed previous repairs, often requiring reconstruction.
-
Osteochondral Lesions:
- Medial femoral condyle or tibial plateau osteochondral defects requiring open access for grafting or repair, especially those not amenable to arthroscopic intervention.
-
Medial Patellofemoral Ligament (MPFL) Reconstruction:
- While often performed through a more anterior, separate incision, the medial approach can be extended or utilized if MPFL reconstruction is combined with other medial-sided pathologies.
-
Medial Opening Wedge High Tibial Osteotomy (HTO):
- Used to correct varus malalignment, the approach provides excellent visualization for osteotomy cuts and plate application.
Contraindications
-
Absolute Contraindications:
- Active local or systemic infection.
- Severe peripheral vascular disease.
- Compromised skin integrity or significant scarring overlying the surgical site.
- Uncontrolled systemic comorbidities that preclude safe anesthesia or surgery.
-
Relative Contraindications:
- Mild (Grade I or II) MCL sprains without mechanical instability, which typically respond to conservative management.
- Isolated cruciate ligament injuries without significant medial collateral involvement.
- Patients unwilling or unable to comply with post-operative rehabilitation protocols.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| MCL Injuries |
- Grade III MCL tears with significant valgus instability (>10-15mm opening at 20-30° flexion).
- MCL tears with valgus instability in full extension (indicates PMC involvement). - Concomitant ACL/PCL tears requiring multi-ligamentous reconstruction. - Proximal MCL avulsion from bone. - Chronic symptomatic valgus instability. |
- Grade I MCL sprains (tenderness without laxity).
- Grade II MCL sprains (tenderness with laxity but a firm endpoint). - Isolated Grade III MCL tears without significant rotatory instability or full extension instability (controversial, but often initially treated non-operatively with bracing). |
| Posteromedial Corner |
- Acute disruption of POL with posteromedial rotatory instability.
- Avulsion fractures involving the PMC structures. - Chronic posteromedial rotatory instability. |
- Mild PMC sprains without significant instability. |
| Medial Meniscus |
- Symptomatic meniscal tears requiring repair or meniscectomy with concomitant ligamentous repair.
- Large, unstable tears (e.g., bucket-handle, radial, root tears, ramp lesions) best addressed with open repair. |
- Small, stable meniscal tears.
- Asymptomatic meniscal tears. - Degenerative tears without mechanical symptoms, often managed with physical therapy and injections. |
| Osteochondral Lesions | - Symptomatic osteochondral defects on medial femoral condyle or tibial plateau requiring open repair/grafting. |
- Small, asymptomatic lesions.
- Lesions responding to conservative measures (e.g., activity modification, bracing). |
| Knee Osteoarthritis | - Varus malalignment requiring medial opening wedge high tibial osteotomy. | - Mild to moderate osteoarthritis managed with physical therapy, NSAIDs, injections, and activity modification. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and optimal patient positioning are critical for maximizing exposure, minimizing complications, and ensuring successful outcomes.
Pre-Operative Planning
- Clinical Assessment: Thorough history and physical examination, including assessment of range of motion, ligamentous stability (valgus stress testing at 0° and 30° flexion, external rotation recurvatum test), and neurovascular status.
-
Imaging Review:
- Radiographs: Weight-bearing anteroposterior, lateral, patellofemoral, and Rosenberg views to assess alignment, joint space, and any bony avulsions. Stress radiographs (valgus stress views) are invaluable for quantifying laxity.
- Magnetic Resonance Imaging (MRI): Essential for detailed visualization of soft tissue injuries (ligaments, menisci, capsule), cartilage status, and identification of concomitant pathologies (e.g., ACL tears).
- CT Scan: Useful for complex fracture patterns or bony avulsions, or for pre-operative templating for hardware placement in osteotomy cases.
- Anesthesia Consultation: Evaluation of patient comorbidities and selection of appropriate anesthetic technique (general, regional, or combined).
- Tourniquet: Placement of a pneumatic tourniquet high on the thigh is standard to optimize visualization and minimize blood loss. Ensure appropriate padding.
- Equipment and Implants: Prepare all necessary instruments for soft tissue dissection, ligament repair/reconstruction (suture anchors, graft harvest instruments if applicable), meniscal repair, and potential fixation (e.g., for osteotomy).
Patient Positioning
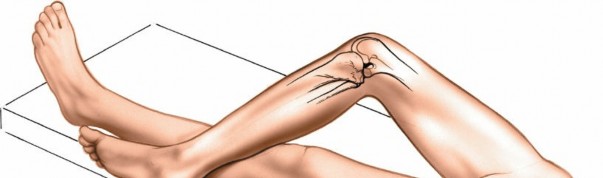
The patient is positioned supine on the operating table. The goal is to provide unrestricted access to the medial aspect of the knee while allowing for intraoperative manipulation.
- Supine Position: The patient lies flat on their back.
- Hip Abduction and External Rotation: The ipsilateral hip is slightly abducted and externally rotated. This helps to relax the medial soft tissues and brings the medial knee into a more accessible position.
-
Knee Flexion:
The knee is typically flexed to approximately 45-60 degrees. This can be achieved by placing a bump or folded blanket under the distal femur, allowing the knee to drop into flexion. Alternatively, a foot holder or leg post can be utilized, providing stable support and allowing the leg to be free-draped for full range of motion.
- For specific ligamentous repairs, especially of the posteromedial corner, intraoperative flexion/extension and valgus stress may be required, necessitating a free-draped extremity.
-
Prepping and Draping:
The limb is prepped circumferentially from the hip to the foot. A sterile tourniquet cover is applied. The foot can be placed in a sterile foot holder, or the entire limb can be free-draped to allow for dynamic intraoperative assessment of stability.

Illustrates standard supine positioning and limb preparation.

Demonstrates the sterile draping to isolate the operative field.

Shows the knee in a flexed position, ready for incision.

Provides a wider view of the prepped and draped limb with the knee positioned for surgery.
Landmarks and Incision Marking
Accurate identification of anatomical landmarks is crucial for precise incision placement and dissection.
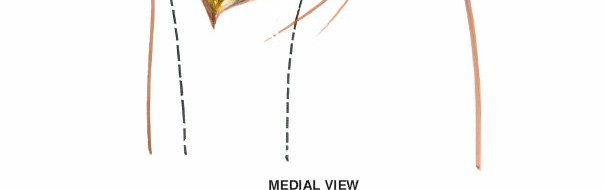
-
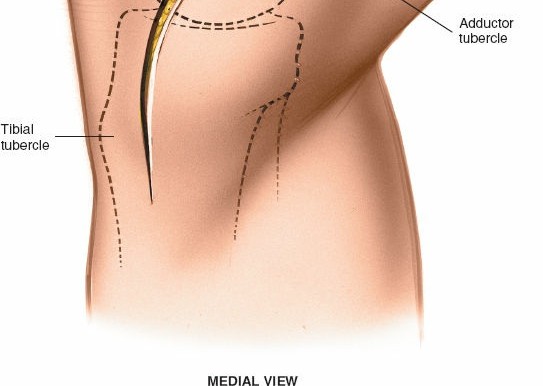
Adductor Tubercle:
Palpate the prominence on the medial surface of the medial femoral condyle. This serves as the proximal extent of the sMCL and a key reference for the femoral origin of the POL. It lies in the natural depression between the vastus medialis and hamstring muscles.

Highlights the palpation of the adductor tubercle, a critical bony landmark. - Medial Joint Line: Palpate the joint line between the medial femoral condyle and the medial tibial plateau.
- Medial Tibial Flare / Pes Anserinus Insertion: Palpate the broad bony prominence of the medial tibia, distal to the joint line, where the pes anserinus inserts.
-
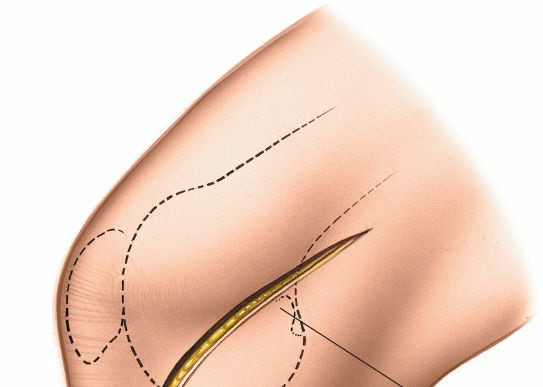
Incision:
- A slightly curved or straight longitudinal incision is typically made, centered over the area of pathology.
- It generally extends from approximately 2-3 cm proximal to the adductor tubercle to 3-4 cm distal to the medial joint line, ending over the medial tibial flare.
- For extensive posteromedial corner exposure, the incision may need to be longer and slightly more posterior.
-
Ensure the incision is sufficiently long to provide adequate exposure without excessive traction on the skin edges.
Illustrates the planned incision line marked on the skin, typically extending from proximal femur to distal tibia.
Detailed Surgical Approach / Technique
The medial approach provides wide exposure, but careful, layered dissection is essential to protect neurovascular structures and precisely identify the various components of the medial knee.
1. Skin Incision and Subcutaneous Dissection
-
Make the skin incision with a #10 blade, ensuring it is deep enough to penetrate the dermis but not extend into the subcutaneous fat initially.
Shows the initial skin incision being made. -
Using electrocautery, perform subcutaneous dissection to raise full-thickness skin flaps, anteriorly and posteriorly. This creates the superficial working space.
-
Crucial step:
Identify and protect the
great saphenous vein
and
saphenous nerve
(and its infrapatellar branch). These structures lie anterior to the sartorius fascia and often require retraction anteriorly. The saphenous nerve typically runs parallel to the saphenous vein.
Depicts subcutaneous dissection, highlighting the identification and careful retraction of neurovascular structures (saphenous vein and nerve).
-
Crucial step:
Identify and protect the
great saphenous vein
and
saphenous nerve
(and its infrapatellar branch). These structures lie anterior to the sartorius fascia and often require retraction anteriorly. The saphenous nerve typically runs parallel to the saphenous vein.
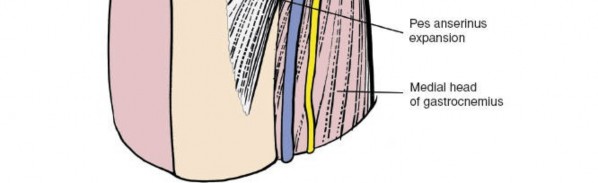
2. Deep Fascia and Pes Anserinus
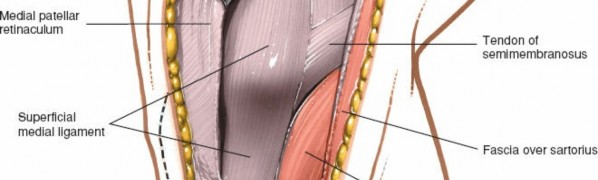
- Identify the deep fascia (fascia lata) and the underlying sartorius muscle . The sartorius forms the most superficial layer of the pes anserinus.
- The pes anserinus , formed by the sartorius, gracilis, and semitendinosus, inserts onto the anteromedial tibia. To expose the sMCL, this complex must be mobilized.
- Option 1 (Posterior Retraction): Make a longitudinal incision through the fascia overlying the sartorius, allowing the sartorius and its underlying gracilis and semitendinosus tendons to be retracted posteriorly. This preserves their integrity and attachments. This is often preferred for MCL repair.
-
Option 2 (Release):
In cases requiring extensive exposure, particularly for posteromedial corner reconstruction or wide access to the medial tibia, the pes anserinus can be detached from its tibial insertion and reflected proximally. This allows for excellent visualization but necessitates reattachment during closure.

Illustrates the deep fascia and the initial exposure of the pes anserinus, likely prior to its mobilization.
3. Exposure of the Superficial Medial Collateral Ligament (sMCL)
- Once the pes anserinus is mobilized, the sMCL comes into view. It is a broad, flat structure extending from the medial femoral epicondyle to the proximal tibia.
- Carefully clear any remaining adipose tissue or bursa superficial to the sMCL.
-
Evaluate the sMCL for the location and extent of the tear (proximal, mid-substance, distal).

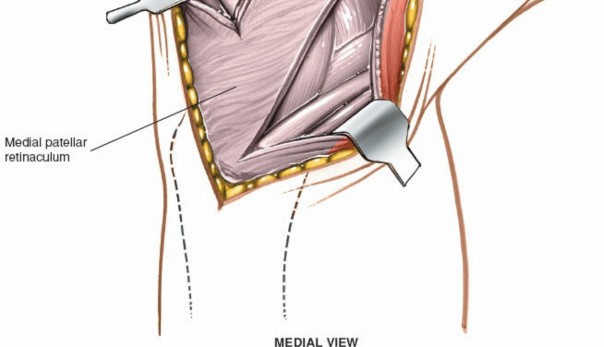
Shows the exposed superficial MCL after retraction of the pes anserinus.
Detailed view of the sMCL, possibly demonstrating a tear or site of pathology.
4. Posteromedial Corner Dissection and Deep MCL
- To access the deep MCL and posteromedial structures, the sMCL must often be incised or elevated.
- Approach 1 (Subluxation/Elevation): If the sMCL is intact or minimally injured, it can be carefully elevated from the underlying deep layer, creating a plane between the superficial and deep MCL. This typically involves an incision along its posterior border.
- Approach 2 (Incise and Repair): If the sMCL is ruptured, the disrupted edges are identified. The tear itself provides access to the deeper structures. For a planned incision through an intact sMCL (e.g., for extensive PMC reconstruction), a longitudinal incision parallel to its fibers, or a transverse incision at the level of the joint line, can be made. This must be meticulously repaired later.
-
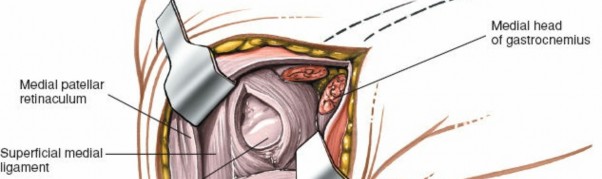
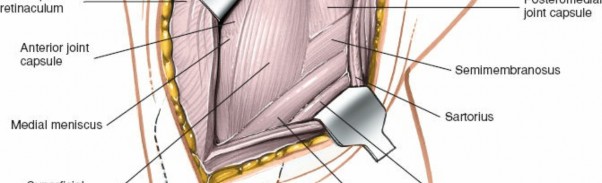
Deep Medial Collateral Ligament (dMCL):
Once the sMCL is retracted, the dMCL, which is a thickening of the joint capsule and is intimately attached to the medial meniscus, becomes visible. It comprises the meniscofemoral and meniscotibial ligaments.
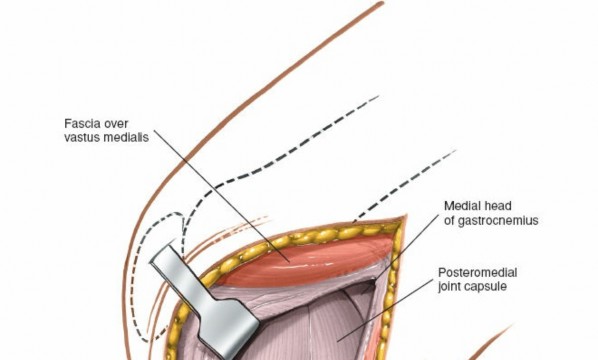
Illustrates the deeper layers, likely showing the dMCL or meniscocapsular structures after superficial layers have been opened or retracted. -
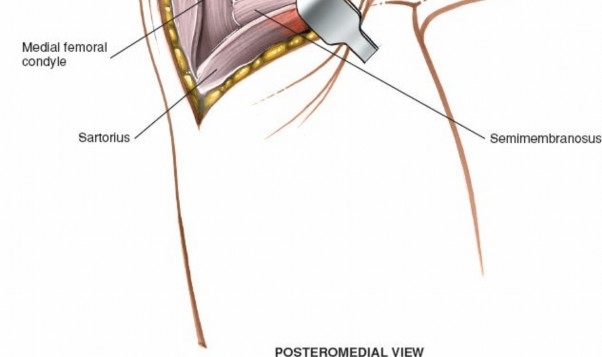
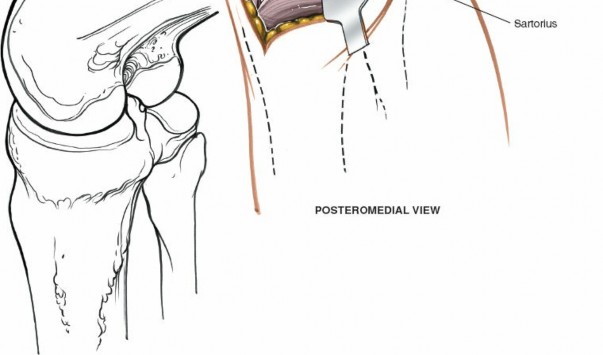
Posterior Oblique Ligament (POL):
This fan-shaped structure is found posterior to the sMCL and dMCL. It blends with the semimembranosus tendon expansions. The POL consists of three main components: superficial, central, and capsular arms. Carefully dissecting along the posterior border of the sMCL and dMCL, and retracting the semimembranosus attachments, allows for identification of the POL.
-
The
semimembranosus tendon
has multiple insertions and expansions around the posteromedial corner. These must be identified and protected, or carefully mobilized, to access the POL.

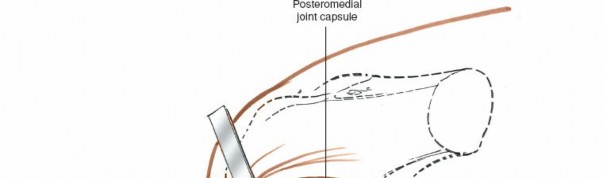
Shows the posteromedial corner, with structures like the POL or semimembranosus expansions being identified or addressed.
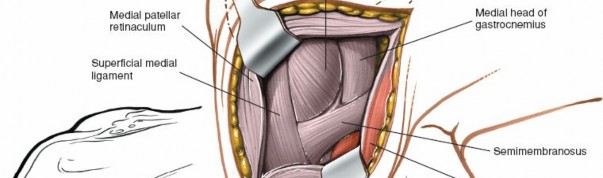
Further detailed view of the posteromedial corner anatomy.
-
The
semimembranosus tendon
has multiple insertions and expansions around the posteromedial corner. These must be identified and protected, or carefully mobilized, to access the POL.
5. Access to the Medial Meniscus and Articular Cartilage
- Access to the medial meniscus is achieved by incising the meniscotibial portion of the deep MCL (coronary ligament) or utilizing existing tears in the deep capsule.
- Carefully inspect the meniscus for tears (ramp lesions, posterior horn tears, root tears) and assess its stability.
-
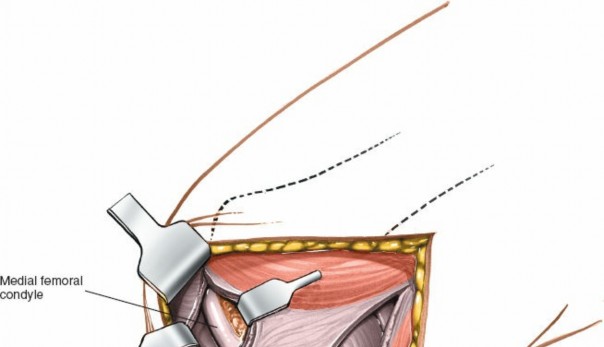
Through this opening, the medial femoral condyle and medial tibial plateau articular surfaces can be visualized for osteochondral pathology.
Depicts access to the medial joint compartment, likely showing visualization of the medial meniscus and articular surfaces.
6. Repair and Reconstruction
-
MCL Repair:
- Direct repair of proximal or distal avulsions using suture anchors or bone tunnels.
- Mid-substance tears can be directly repaired with strong non-absorbable sutures in a horizontal mattress or figure-of-eight fashion.
-
Augmentation with a semitendinosus autograft may be considered for severe tears or chronic instability.
Illustrates a suture being placed or tied for MCL repair, possibly at its femoral attachment.
Shows a specific repair technique or placement of sutures within the MCL substance.
-
POL Repair/Reconstruction:
- Direct repair of acute tears can be performed using suture anchors.
-
Reconstruction for chronic instability typically involves a graft (semitendinosus, gracilis, or allograft) anchored to the femoral origin of the POL and woven into the tibial attachment of the semimembranosus and posterior capsule.
Depicts a repair or reconstruction technique for the POL, possibly involving graft passage.
Further illustration of a reconstruction technique, showing anchor placement or graft tensioning.
Detailed view of the completed repair or reconstruction of the posteromedial corner.
-
Medial Meniscus Repair/Meniscectomy:
- Repair performed with inside-out, outside-in, or all-inside techniques, depending on the tear location and pattern.
-
Meniscectomy involves partial resection of unstable or irreparable meniscal tissue.
Shows a specific repair or meniscectomy technique being performed on the medial meniscus.
Further detail on meniscal intervention, possibly suture placement for repair.
Final view of the meniscal repair or partial meniscectomy.
Internervous Plane
There is no true internervous plane in the classic definition for the medial approach to the knee. However, the dissection is generally considered safe because the major nerves supplying the knee (tibial, common peroneal, saphenous) and major vessels (popliteal artery/vein) lie posteriorly within the popliteal fossa, well away from the primary surgical field.
The main neurovascular structures at risk are the saphenous nerve and its infrapatellar branch , and the great saphenous vein . These structures are superficial to the deep fascia and typically lie anterior to the sartorius. They are identified during the initial subcutaneous dissection and carefully retracted anteriorly with the skin flap. The infrapatellar branch of the saphenous nerve crosses the patellar tendon and can be particularly vulnerable during incisions crossing the patella or its distal pole. Careful blunt dissection and protection of these structures minimizes the risk of neurapraxia or neuroma formation.
7. Closure
- Thorough irrigation of the wound.
- Perform repair of the deep MCL and capsule if they were incised to access the joint.
- Reattach the pes anserinus if it was released from its tibial insertion. If retracted, ensure it returns to its anatomical position.
- Repair the sMCL meticulously.
- Close the deep fascia over the sMCL (if applicable) with absorbable sutures.
- Reapproximate the subcutaneous layers.
- Close the skin with staples or sutures.
-
Consider a drain if extensive dissection or reconstruction was performed, or if significant bleeding is anticipated.
Shows the repair of the medial collateral ligament, providing stability before final closure.
Depicts the layered closure, starting with the deeper fascial structures.
Final skin closure with staples or sutures, completing the surgical approach.
Complications & Management
Despite meticulous surgical technique, complications can arise following the medial approach to the knee. A comprehensive understanding of potential issues and their management is crucial for optimal patient care.
General Surgical Complications
-
Infection:
Superficial or deep wound infection. Incidence varies but is generally low (0.5-2%).
- Management: Superficial infections may respond to oral antibiotics and local wound care. Deep infections typically require surgical debridement, intravenous antibiotics, and potentially hardware removal.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
Risk is present with any lower extremity surgery.
- Management: Prophylaxis (mechanical/pharmacological) is standard. Treatment involves anticoagulation.
-
Hemorrhage / Hematoma:
Can result from inadequate hemostasis or unrecognized vessel injury.
- Management: Small hematomas may resolve spontaneously. Larger, symptomatic hematomas may require surgical evacuation.
- Anesthetic Complications: Related to the type of anesthesia used and patient comorbidities.
-
Wound Healing Issues:
Delayed healing, dehiscence, excessive scarring (hypertrophic or keloid).
- Management: Optimization of wound care, debridement if necrotic tissue is present, scar management techniques.
Specific Complications of the Medial Approach
-
Saphenous Nerve Injury:
- Incidence: Neurapraxia (temporary numbness or dysesthesia) is relatively common (up to 30%), persistent symptoms less so (5-10%). Due to its superficial course, the infrapatellar branch is particularly vulnerable.
- Management: Most neurapraxias resolve spontaneously. Persistent painful neuromas may require surgical excision or nerve grafting in rare cases. Patient counseling pre-operatively regarding the risk of numbness in the saphenous nerve distribution is essential.
-
Great Saphenous Vein Injury:
- Incidence: Low if meticulous dissection is performed.
- Management: Ligation or repair, depending on the size and location of the injury.
-
Stiffness / Arthrofibrosis:
Excessive scar tissue formation leading to restricted range of motion.
- Incidence: Varies depending on the extent of injury and surgical procedure (e.g., higher with combined multi-ligamentous reconstructions).
- Management: Intensive physical therapy, dynamic splinting, manipulation under anesthesia, or arthroscopic/open arthrolysis if conservative measures fail.
-
Recurrent Instability:
Failure of the repair or reconstruction, leading to persistent valgus or posteromedial rotatory laxity.
- Incidence: Depends on original injury severity, surgical technique, and patient compliance.
- Management: Thorough evaluation to identify the cause of failure (graft failure, inadequate fixation, unrecognized concomitant injury). Revision surgery with stronger grafts, improved fixation, or addressing other instabilities may be required.
-
Hardware-Related Complications:
If sutures, anchors, or screws are used.
- Incidence: Low.
- Management: Symptomatic hardware may require removal after healing is complete.
-
Medial Joint Line Pain:
Can result from scar tissue, meniscal pathology, or articular cartilage issues.
- Management: Physical therapy, injections, arthroscopy for persistent mechanical symptoms.
Table of Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approximate) | Salvage Strategies |
|---|---|---|
| Infection | 0.5-2% | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, IV antibiotics, hardware removal (if applicable). |
| Saphenous Nerve Injury (Numbness) | 10-30% (neurapraxia) | Observation (most resolve). Persistent painful neuroma: Local injections, neurectomy, nerve grafting. Patient education on sensory changes. |
| Hematoma | 1-5% | Observation for small, asymptomatic. Large/symptomatic: Surgical evacuation, irrigation, and drainage. |
| Arthrofibrosis/Stiffness | 5-15% | Intensive physical therapy, dynamic splinting, manipulation under anesthesia. Severe cases: Arthroscopic or open arthrolysis. |
| Recurrent Instability | 5-10% | Thorough diagnostic workup (stress views, MRI) to identify failure mode. Revision surgery with stronger graft, improved fixation, addressing concomitant instabilities. |
| Wound Dehiscence | <1% | Debridement of non-viable tissue, secondary closure, negative pressure wound therapy. |
| DVT/PE | <1% (with prophylaxis) | DVT: Anticoagulation, compression. PE: Anticoagulation, respiratory support. Emphasis on pre-operative prophylaxis. |
| Hardware Irritation | 2-5% | Observation. Symptomatic hardware (e.g., suture anchors, staples): Surgical removal after ligamentous healing is complete (typically 6-12 months post-op). |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as crucial as the surgical procedure itself in restoring knee function and preventing re-injury. Protocols vary depending on the specific structures repaired or reconstructed and the surgeon's preference, but generally follow a phased approach.
General Principles
- Protection of Repair/Reconstruction: Initial emphasis on protecting the surgically treated structures from undue stress (valgus, external rotation).
- Pain and Swelling Control: Early use of RICE (rest, ice, compression, elevation), analgesics, and anti-inflammatory medications.
- Gradual Restoration of Motion: Progressive increase in range of motion (ROM) while respecting tissue healing timelines.
- Progressive Strengthening: Sequential strengthening of quadriceps, hamstrings, and hip musculature.
- Neuromuscular Control and Proprioception: Essential for dynamic stability.
- Return to Activity: Criteria-based progression, not time-based alone.
Phased Rehabilitation Example (for MCL/PMC Repair)
Phase I: Immediate Post-Operative (Weeks 0-4)
- Goals: Protect repair, control pain/swelling, achieve full extension, initiate controlled flexion.
-
Immobilization:
- Hinged knee brace locked in extension for 1-2 weeks initially, then unlocked for ROM within a protected arc.
- Valgus stress protection.
-
Weight-Bearing:
- Touch-down weight-bearing (TDWB) or non-weight-bearing (NWB) with crutches for 2-4 weeks.
- Progress to partial weight-bearing (PWB) as tolerated.
-
Range of Motion:
- Passive ROM (PROM) 0-30° initially, progressing to 0-90° by week 4.
- Avoid excessive valgus stress during ROM exercises.
-
Exercises:
- Ankle pumps, quad sets, gluteal sets.
- Gentle hamstring curls (prone).
- Straight leg raises (SLRs) in various planes with brace on.
- Patellar mobilizations.
Phase II: Intermediate Protection (Weeks 4-12)
- Goals: Restore full ROM, improve strength, begin proprioception.
- Brace: Continue hinged brace for protection during ambulation and activity, often unlocked, discontinued around week 8-12.
-
Weight-Bearing:
- Progress to full weight-bearing (FWB) as tolerated, typically by week 6-8.
-
Range of Motion:
- Work towards full knee flexion (130°+) by week 8-10.
-
Exercises:
- Continue Phase I exercises, increasing resistance.
- Initiate closed-chain exercises: mini-squats, leg press (limited depth, avoiding valgus stress), stationary cycling (high seat, low resistance).
- Core strengthening.
- Gentle proprioceptive exercises: balance board (progress to single leg).
- Avoid resisted knee flexion beyond 90 degrees if semitendinosus was used as a graft.
Phase III: Advanced Strengthening & Neuromuscular Control (Weeks 12-24)
- Goals: Maximize strength, power, endurance, sport-specific preparation.
- Brace: Typically discontinued for daily activities, may be used for higher-risk activities.
-
Exercises:
- Progressive resistance exercises (PREs) for quadriceps and hamstrings.
- Plyometric training (jump training, box jumps) with good form.
- Agility drills (shuttle runs, cutting maneuvers).
- Advanced balance and proprioception.
- Initiate sport-specific drills.
- Swimming, elliptical.
Phase IV: Return to Activity/Sport (Months 6+ or 9+ for multi-ligament)
- Goals: Full return to unrestricted activities, sport-specific training.
-
Criteria for Return to Sport:
- No pain or swelling.
- Full, symmetrical ROM.
- Strength testing: Isokinetic testing (quads/hams) ≥ 90% of contralateral limb.
- Functional testing: Hop tests (single-leg hop, triple hop, crossover hop) ≥ 90% of contralateral limb.
- Satisfactory performance in sport-specific drills.
- Absence of apprehension during valgus or rotational stress.
- Physician clearance.
- Considerations: Contact sports may require longer restrictions. Education on proper landing mechanics and injury prevention.
Specific Considerations
- Meniscal Repair: May necessitate stricter weight-bearing restrictions or limited flexion for the initial 6 weeks to protect the repair.
- HTO: Weight-bearing is typically restricted to TDWB for 6-8 weeks, followed by gradual progression as callus formation is evident on radiographs.
- Chronic Instability / Reconstruction: Rehabilitation may be more protracted, with a slower progression to protect the graft.
Close collaboration between the surgeon, physical therapist, and patient is essential for individualizing the protocol and addressing any setbacks.
Summary of Key Literature / Guidelines
The understanding and management of medial knee pathologies have evolved significantly, guided by both landmark anatomical studies and clinical outcomes research.
-
Anatomical and Biomechanical Foundations:
- Hughston et al. (1976): Pioneering work on the medial and posteromedial structures, emphasizing the "oblique popliteal ligament" (now understood as part of the POL complex) and its role in rotational stability. This work highlighted the multi-layered nature of the medial knee.
- Grood et al. (1981): Classic biomechanical studies quantifying the load-sharing characteristics of knee ligaments, definitively establishing the sMCL as the primary restraint to valgus stress.
- LaPrade et al. (2007, 2010): Extensive detailed anatomical and biomechanical studies elucidating the distinct attachments and functional roles of the sMCL, dMCL, and POL, particularly their femoral footprints and the precise components of the posteromedial corner. Their work has informed contemporary reconstruction techniques.
-
MCL Injury Management:
- Non-Operative vs. Operative: Consensus generally supports non-operative management for isolated Grade I and II MCL injuries. Grade III injuries, particularly those with valgus instability at 0° flexion or in the setting of multi-ligamentous injury (e.g., ACL rupture), often warrant surgical repair or augmentation.
- Early Surgical Intervention: Studies by Indelicato (1995) and others have shown excellent results with early surgical repair of acute Grade III MCL tears, especially those with bony avulsions or significant instability, particularly when combined with ACL reconstruction.
- Repair vs. Reconstruction: Acute tears, especially avulsions, are often amenable to direct repair. Chronic or severely attenuated structures, or those with significant substance loss, frequently require reconstruction using autografts (semitendinosus, gracilis) or allografts.
-
Posteromedial Corner (PMC) Injuries:
- Recognition of the PMC as a distinct functional entity, contributing significantly to valgus stability in extension and controlling posteromedial tibial rotation.
- Techniques for PMC repair and reconstruction are increasingly refined, aiming to restore the anatomical insertions of the sMCL and POL. LaPrade's anatomical reconstruction is a widely referenced technique for complex posteromedial instability, utilizing separate femoral and tibial tunnels to recreate the sMCL and POL.
-
Combined Injuries:
- The medial approach is critical in the management of multi-ligamentous knee injuries, often allowing simultaneous repair or reconstruction of medial structures alongside cruciate ligament reconstruction (e.g., ACL or PCL).
- Sequential vs. Staged Approach: Debates exist regarding the optimal timing for combined reconstructions. Acute repair of the medial structures, followed by staged or concomitant cruciate reconstruction, is common.
-
Rehabilitation Guidelines:
- Accelerated vs. Protected Rehabilitation: Modern protocols tend towards earlier protected motion and weight-bearing compared to historical approaches, but strict adherence to valgus and rotational precautions remains paramount during the initial healing phases.
- Criteria-Based Progression: Current guidelines emphasize functional and strength-based criteria over purely time-based progression for return to sport, ensuring the knee is robustly stable and controlled.
In summary, the medial approach to the knee remains a versatile and indispensable surgical tool for orthopedic surgeons. Its mastery requires an in-depth understanding of the complex regional anatomy, the biomechanics of medial knee stability, precise surgical technique, and a well-structured post-operative rehabilitation program. Continuous evaluation of outcomes and integration of evolving literature are essential for optimizing patient care in this challenging anatomical region.
Clinical & Radiographic Imaging

You Might Also Like


