Femur Neck Fracture: Uncover Symptoms & Best Treatment
Key Takeaway
Discover the latest medical recommendations for Femur Neck Fracture: Uncover Symptoms & Best Treatment. A femur neck fracture is a break in the neck of the femur bone, which connects the femoral head to the femoral shaft. This common type of proximal femoral fracture primarily affects older adults, leading to significant pain, discomfort, and mobility issues. Most cases require surgical intervention to repair the break and restore function.
Introduction & Epidemiology
Proximal femoral fractures, particularly those involving the femoral neck, represent a significant orthopedic challenge due to their profound impact on patient morbidity, mortality, and healthcare resource utilization. These fractures occur in the upper part of the femur bone, connecting the femoral head and the femoral shaft, and typically result from low-energy trauma in older adults with osteoporotic bone. However, high-energy mechanisms can lead to similar injuries in younger populations, presenting distinct treatment considerations.
A femur neck fracture is a break in the neck of the femur, the critical region joining the femoral head to the shaft. This anatomical segment is inherently vulnerable to fracture due to its narrow geometry and the complex biomechanical forces it experiences. The incidence of femoral neck fractures rises exponentially with age, predominantly affecting individuals over 65 years, with a higher prevalence in females due to post-menopausal osteoporosis. The lifetime risk for a hip fracture is estimated to be 1 in 6 for women and 1 in 10 for men, with femoral neck fractures comprising approximately 45-50% of all hip fractures.
The clinical presentation typically involves acute onset of severe pain in the groin or hip, inability to bear weight, and often, a shortened and externally rotated lower extremity. The intracapsular nature of these fractures carries a substantial risk of disruption to the tenuous blood supply to the femoral head, predisposing patients to complications such as avascular necrosis (AVN) and non-union, particularly with displaced injuries.
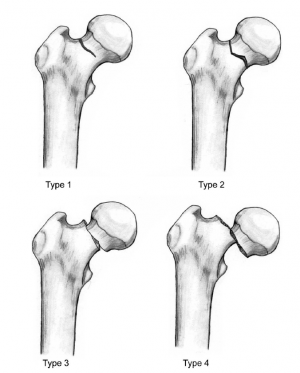
The original seed content introduced a simplified classification based on displacement:
*
Non-displaced fractures
: These fractures do not move out of alignment.
*
Partially displaced fractures
: These fractures move slightly out of alignment.
*
Completely displaced fractures
: These fractures are completely out of alignment.
This aligns with the fundamental principles of the Garden classification, a widely adopted system for femoral neck fractures based on radiographic appearance, guiding prognosis and treatment selection:

- Garden I: Incomplete or impacted valgus fracture. The medial trabeculae are buckled, but the lateral trabeculae remain intact. Considered stable.
- Garden II: Complete but non-displaced fracture. The fracture line extends across the entire femoral neck, but the fragments remain in anatomical alignment. Considered potentially unstable.
- Garden III: Complete, partially displaced fracture. The fracture is complete, and there is partial displacement, often with varus deformity and posterior tilt. The femoral head maintains some connection to the acetabulum.
- Garden IV: Complete, fully displaced fracture. There is total loss of continuity between the head and neck fragments, with no bony contact. The head often remains aligned within the acetabulum, but its connection to the femoral neck is completely severed.
Another critical classification system is the Pauwels classification, which categorizes fractures based on the angle of the fracture line relative to the horizontal plane, providing insight into the biomechanical stability and the magnitude of shear forces:
*
Pauwels Type I:
Fracture angle less than 30 degrees. Primarily subjected to compressive forces, relatively stable.
*
Pauwels Type II:
Fracture angle between 30 and 50 degrees. Experience both compressive and significant shear forces.
*
Pauwels Type III:
Fracture angle greater than 50 degrees. Predominantly subjected to high shear forces, highly unstable with a high risk of non-union.
These classifications are instrumental in guiding surgical decision-making, influencing the choice between internal fixation and arthroplasty, and ultimately impacting patient outcomes. The management of these fractures necessitates a multidisciplinary approach, focusing on prompt surgical intervention, medical optimization, and comprehensive rehabilitation to mitigate the severe consequences associated with these injuries.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the proximal femur is paramount for effective treatment of femoral neck fractures. The femoral neck, connecting the femoral head to the greater and lesser trochanters, is characterized by its anteversion and angle of inclination, both critical determinants of hip joint mechanics and fracture patterns.
The normal angle of inclination (neck-shaft angle) typically ranges from 125 to 135 degrees. A larger angle (coxa valga) increases the compressive forces across the neck, while a smaller angle (coxa vara) increases shear forces and bending moments. Femoral anteversion, the anterior rotation of the femoral neck relative to the transcondylar axis of the knee, typically ranges from 10-20 degrees. Aberrations in these angles can predispose to certain fracture configurations or alter stress distribution within the bone.
The internal architecture of the femoral neck consists of a complex network of trabeculae organized into distinct systems:
*
Primary Compressive Trabeculae:
Extend from the medial cortex of the femoral shaft superiorly to the subchondral bone of the femoral head.
*
Primary Tensile Trabeculae:
Arise from the lateral cortex of the femoral shaft and arch superomedially to the superior aspect of the femoral head.
*
Secondary Compressive & Tensile Trabeculae:
Provide additional support.
*
Ward's Triangle:
A relatively weaker area devoid of dense trabeculae, located between the primary compressive, primary tensile, and secondary compressive systems. This region, particularly vulnerable in osteoporotic bone, is a common site for crack initiation.
The blood supply to the femoral head is predominantly via the medial circumflex femoral artery (MCFA) and, to a lesser extent, the lateral circumflex femoral artery (LCFA). These vessels arise from the deep femoral artery and contribute to an extracapsular arterial ring at the base of the femoral neck. From this ring, retinacular arteries (also known as the ascending cervical branches or subsynovial vessels of Weitbrecht) ascend along the femoral neck, penetrating the bone to supply the femoral head. The MCFA, specifically its posterior retinacular branches, is the primary arterial supply to the majority of the femoral head, particularly the superior and posterior aspects. The artery of the ligamentum teres (a branch of the obturator artery), while important in childhood, typically provides only a minor or negligible supply in adulthood.
The intracapsular nature of femoral neck fractures is crucial. The synovial fluid within the joint capsule, when mixed with fracture hematoma, can tamponade the retinacular vessels, further compromising the already precarious blood supply. This disruption, compounded by the degree of fracture displacement, significantly increases the risk of avascular necrosis (AVN) of the femoral head. Displaced fractures (Garden III and IV) are particularly prone to AVN and non-union due to severe vascular disruption.
Biomechanically, the femoral neck is subjected to substantial bending and shear forces during weight-bearing. The fracture mechanism often involves an axial load combined with external rotation, or a direct impact on the greater trochanter. In osteoporotic bone, even a low-energy fall can generate sufficient stress to overcome the diminished bone strength. The Pauwels classification directly addresses the biomechanical implications of the fracture line angle: a steeper angle (Pauwels III) indicates a greater component of shear stress, leading to inherent instability and higher rates of non-union if not adequately stabilized. Optimal surgical fixation must counteract these forces, providing stable reduction and compression to promote healing while preserving the critical vascular supply.
Indications & Contraindications
The choice of treatment for femoral neck fractures is highly individualized, contingent upon patient factors (age, physiological status, comorbidities, functional demands), fracture characteristics (displacement, comminution, bone quality), and surgeon experience. The primary goals are pain relief, early mobilization, and restoration of functional independence.
Indications for Operative Management
The vast majority of femoral neck fractures require operative intervention.
-
Internal Fixation (Cannulated Screws, Dynamic Hip Screw (DHS)):
- Younger Patients (<60-65 years): Preservation of the native femoral head is paramount. Internal fixation is the preferred treatment for all fracture types (displaced or non-displaced), even with the inherent risks of AVN and non-union, which are managed with close follow-up and potential revision.
- Non-displaced or Impacted Fractures (Garden I & II) in Older Adults: In physiologically active elderly patients, internal fixation may be considered. The risk of AVN and non-union is lower compared to displaced fractures.
-
Specific Subtypes:
- Garden I (Impacted Valgus): While some highly stable, asymptomatic Garden I fractures might theoretically be managed non-operatively in very select, non-ambulatory patients, surgical fixation is generally favored to prevent displacement and facilitate early mobilization.
- Garden II (Complete, Non-Displaced): These are inherently unstable and require fixation.
-
Arthroplasty (Hemiarthroplasty (HA) or Total Hip Arthroplasty (THA)):
-
Displaced Fractures (Garden III & IV) in Older Adults (>65-70 years):
These fractures carry a high risk of AVN and non-union with internal fixation, making arthroplasty the gold standard.
- Hemiarthroplasty (HA): Typically indicated for less active elderly patients with no pre-existing symptomatic hip arthritis, offering a faster recovery and lower dislocation risk than THA. Unipolar or bipolar options exist, with bipolar often favored for reduced acetabular wear.
- Total Hip Arthroplasty (THA): Indicated for physiologically active elderly patients with pre-existing symptomatic hip arthritis, or those with high functional demands who can comply with precautions. THA provides superior functional outcomes and a lower reoperation rate than HA but carries a higher upfront risk of dislocation and longer surgical time.
- Failed Internal Fixation: Revision to HA or THA is common after failed internal fixation for any age group, especially if AVN or symptomatic non-union develops.
- Pathological Fractures: In cases of metastatic disease, arthroplasty may be preferred to achieve immediate stability and pain relief.
-
Displaced Fractures (Garden III & IV) in Older Adults (>65-70 years):
These fractures carry a high risk of AVN and non-union with internal fixation, making arthroplasty the gold standard.
Contraindications for Operative Management
Absolute contraindications for operative management are rare and typically relate to the patient's immediate medical stability.
- Moribund Patient: Extremely frail, non-ambulatory patients with severe, uncorrectable comorbidities (e.g., severe sepsis, end-stage organ failure) where the risks of anesthesia and surgery far outweigh any potential benefits. Palliative care and comfort measures may be prioritized.
Contraindications for Specific Operative Techniques
-
Internal Fixation:
- Severely Displaced Fractures (Garden III/IV) in Older Adults: High risk of AVN and non-union; arthroplasty is generally superior.
- Severe Comminution of the Femoral Neck: Unlikely to achieve stable fixation, leading to high failure rates.
- Poor Bone Quality (Severe Osteoporosis): Inadequate screw purchase for stable fixation.
- Delay to Surgery (>48-72 hours) for Displaced Fractures: Increased risk of AVN, especially in older patients; arthroplasty may be more predictable.
-
Hemiarthroplasty:
- Pre-existing Symptomatic Acetabular Arthritis: HA would likely result in persistent pain due to acetabular disease; THA is indicated.
- High Functional Demands in Very Active Elderly: While HA provides pain relief, THA offers better long-term function and less acetabular wear in this cohort.
-
Total Hip Arthroplasty:
- Very Young Patients (<50-60 years): High probability of aseptic loosening or wear over their lifetime; internal fixation is preferred initially.
- Active Infection: Absolute contraindication for primary THA; requires infection control before definitive arthroplasty.
- Neuropathic Arthropathy: Risk of recurrent dislocation and loosening.
Summary of Operative vs. Non-Operative Indications
| Factor / Indication | Non-Operative Management | Operative Management (Internal Fixation) | Operative Management (Hemiarthroplasty) | Operative Management (Total Hip Arthroplasty) |
|---|---|---|---|---|
| Patient Age | Moribund, non-ambulatory, severe comorbidities, poor prognosis | Physiologically young (<60-65 years) | Physiologically older (>65-70 years), lower functional demands | Physiologically older (>65-70 years), higher functional demands, pre-existing arthritis |
| Fracture Displacement | N/A (rarely considered, even for impacted fractures) | Non-displaced (Garden I, II), or reducible displaced in young | Displaced (Garden III, IV) | Displaced (Garden III, IV) |
| Bone Quality | N/A | Good-to-moderate bone quality | Moderate-to-poor bone quality (osteoporosis) | Moderate-to-poor bone quality (osteoporosis) |
| Pre-existing Hip Arthritis | N/A | N/A | None | Symptomatic arthritis |
| Functional Demand | Non-ambulatory, bedridden | High, desire for native hip preservation | Low-to-moderate | High |
| Risk of AVN/Non-union | N/A | Managed risk (higher for displaced fractures) | Low for head necrosis, but risk of acetabular wear with unipolar | Low for head necrosis, stable long-term outcome |
| Timing of Presentation | N/A | Optimal within 24-48 hours, especially for displaced fractures | Optimal within 24-48 hours | Optimal within 24-48 hours |
| Comminution | N/A | Minimal | Moderate to severe, especially of femoral neck | Moderate to severe, especially of femoral neck |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are crucial for successful outcomes in femoral neck fracture surgery, minimizing complications and optimizing surgical efficiency.
Pre-Operative Planning
-
Patient Assessment and Optimization:
- Medical Workup: A comprehensive medical evaluation is essential to identify and optimize comorbidities (cardiac, pulmonary, renal, endocrine, nutritional status). This often involves consultation with internal medicine, cardiology, or anesthesiology. Fluid and electrolyte balance, anemia correction, and control of chronic diseases (e.g., diabetes, hypertension) are vital.
- Anesthesia Assessment: A thorough pre-anesthetic evaluation determines fitness for surgery and helps select the most appropriate anesthetic technique (general, spinal, or regional block).
- Anticoagulation Management: Assess current anticoagulant/antiplatelet medications. A protocol for bridging or cessation must be established in collaboration with cardiology or internal medicine, balancing thrombotic risk reduction with surgical bleeding risk.
- Informed Consent: Detailed discussion with the patient (and family/legal proxy if applicable) regarding the nature of the fracture, proposed surgical intervention, alternatives, potential risks (infection, DVT/PE, AVN, non-union, hardware failure, limb length discrepancy, dislocation), expected outcomes, and rehabilitation.
-
Imaging Review and Templating:
- Standard Radiographs: AP pelvis and cross-table lateral views are essential for fracture classification (Garden, Pauwels), assessment of displacement, and comminution.
- CT Scan: May be useful in select cases, particularly in younger patients, to evaluate comminution, impaction, or complex fracture patterns, aiding in reduction strategy.
- Templating: For arthroplasty cases (HA or THA), templating with AP pelvis radiographs (calibrated with a known magnification marker) is critical for predicting implant size, assessing leg length, and determining femoral offset. This helps in pre-selecting implants and anticipating any challenges.
-
Timing of Surgery:
- Current evidence strongly supports early surgical intervention, ideally within 24-48 hours of injury, for most femoral neck fractures. This has been shown to reduce rates of medical complications (e.g., pneumonia, pressure ulcers, DVT), length of hospital stay, and overall mortality, especially in the elderly. Delays can increase the risk of AVN in displaced fractures.
-
Blood Management:
- Type and screen/cross-match should be performed. Blood conservation strategies, including anti-fibrinolytics (e.g., tranexamic acid), may be considered.
Patient Positioning
Proper positioning is crucial for surgical access, image intensifier (C-arm) freedom, and prevention of iatrogenic injury.
-
Operating Table Selection:
- Fracture Table: Commonly used for internal fixation with cannulated screws or DHS. It allows for controlled traction, abduction/adduction, and rotation of the affected limb, facilitating closed reduction and maintaining it during fixation. The contralateral limb is typically placed in an abduction-flexion-external rotation position in a well-padded boot stirrup to allow C-arm access.
- Radiolucent Operating Table: Preferred for arthroplasty (HA or THA) as it offers greater flexibility for various surgical approaches (e.g., posterolateral, direct anterior, anterolateral). The limb can be manipulated freely for dislocation and reduction, and C-arm can be used for stem alignment or acetabular component positioning.
-
Supine Position:
- The patient is positioned supine for all approaches. Careful padding of all bony prominences (heels, sacrum, elbows, shoulders) is essential to prevent pressure sores or nerve palsies.
- For Fracture Table: The affected leg is placed in a fracture boot, and gentle traction is applied to achieve initial reduction. The amount of traction and rotational alignment (internal rotation for femoral neck fractures) is critical. The perineal post should be well-padded to prevent nerve compression.
- For Radiolucent Table: The patient is positioned supine, with a bump or beanbag placed under the ipsilateral hip for direct anterior or anterolateral approaches. For posterolateral, the patient may be placed in a lateral decubitus position or semi-lateral. Ensure adequate space for C-arm entry and exit.
-
C-arm Access:
- Ensure unrestricted C-arm access for both AP and lateral views of the hip during internal fixation. For arthroplasty, C-arm is often used intermittently to verify component position, particularly for the femoral stem in uncemented cases or for acetabular inclination.
-
Surgical Field Preparation:
- Thorough preparation and draping of the surgical site, extending from the iliac crest to below the knee, ensuring sterility for potential extended approaches or contingencies.
Detailed Surgical Approach / Technique
The detailed surgical approach and technique for femoral neck fractures are dictated by the patient's age, physiological status, fracture classification (Garden and Pauwels), and surgeon preference. The main treatment modalities are internal fixation and arthroplasty (hemiarthroplasty or total hip arthroplasty).
Fracture Classification Review (as it guides treatment)
-
Garden Classification:
- Garden I (Incomplete, Impacted Valgus): Typically stable, but fixation is recommended to prevent displacement and enable early weight-bearing.
- Garden II (Complete, Non-Displaced): Complete fracture, but fragments in alignment. Inherently unstable and requires fixation.
- Garden III (Complete, Partially Displaced): Complete fracture with partial displacement, often varus. High risk of AVN and non-union; decision for fixation vs. arthroplasty depends heavily on age and activity.
- Garden IV (Complete, Fully Displaced): Complete fracture with no bony contact. Highest risk of AVN and non-union; arthroplasty is generally indicated for older adults.
-
Pauwels Classification:
- Pauwels Type I (<30°): Low shear forces, more stable, amenable to internal fixation.
- Pauwels Type II (30-50°): Moderate shear forces.
- Pauwels Type III (>50°): High shear forces, highly unstable. Pauwels III fractures, even when Garden I or II, can indicate a higher risk of fixation failure.
Treatment Options and Techniques
1. Internal Fixation (for Young Patients, Garden I/II in active elderly)
The primary goal is anatomical reduction and stable internal fixation to preserve the femoral head.
-
Closed Reduction Maneuvers:
- Typically performed on a fracture table under fluoroscopic guidance.
- Traction: Longitudinal traction is applied to the affected limb to disimpact and restore length.
- Internal Rotation: Corrects the typical external rotation deformity.
- Abduction/Adduction and Flexion/Extension: Used to optimize the fracture fragment alignment. Often, the Allgöwer maneuver (hip extension, abduction, and internal rotation) or Leadbetter maneuver (hip flexion to 90 degrees, internal rotation, then extension) can be employed.
- Radiographic verification (AP and lateral views) is essential for adequate reduction (Garden alignment index of 160-180 degrees on AP and 180 degrees on lateral).
-
Percutaneous Cannulated Screw Fixation (Standard for Garden I/II):
- Approach: Small lateral incision distal to the greater trochanter.
- Internervous Plane: Dissection through skin, subcutaneous tissue, fascia lata (split), vastus lateralis, directly to the lateral femoral cortex. No major internervous plane involved.
-
Technique:
- After satisfactory closed reduction, maintain with traction.
- Position C-arm for true AP and lateral views.
- Make a small lateral incision (approx. 2-3 cm) below the vastus ridge.
- Insert 3 cannulated guide wires in a triangular or inverted triangular configuration. The ideal placement is to aim for the center of the femoral head on the AP view and slightly inferior-posterior on the lateral view to engage the strong cortical bone and avoid the weight-bearing superior articular cartilage. The screws should be divergent, not parallel. The distal-most screw should typically engage the inferior cortex of the neck and enter the subchondral bone.
- Measure screw lengths.
- Overdrill for partially threaded cannulated screws (typically 6.5mm or 7.3mm). Ensure adequate thread purchase across the fracture site and into the subchondral bone of the femoral head.
- Insert the cannulated screws. Compression at the fracture site is achieved by the partially threaded design as the screw advances into the femoral head.
- Final fluoroscopic images (AP and lateral) to confirm screw position and fracture stability.
- Wound closure.
-
Dynamic Hip Screw (DHS) with Derotational Screw:
- Indication: Select cases, particularly for basicervical fractures or those with a more vertical Pauwels angle where strong compression and controlled collapse are desired. Less commonly used for typical transcervical neck fractures.
- Approach: Lateral incision, similar to proximal femoral nailing, extending proximally from the vastus ridge.
- Technique: Guide wire for the lag screw is placed, followed by reaming, tapping, and insertion of the lag screw. A side plate is then attached. Often, an additional anti-rotation screw is placed superiorly to prevent rotation of the femoral head.
- Challenges: Larger dissection, higher blood loss than cannulated screws, potential for lag screw cut-out.
2. Arthroplasty (for Older Adults, Garden III/IV, Failed Fixation)
-
Approach Options:
- Posterolateral Approach: Most common. Internervous plane between gluteus maximus (superior gluteal nerve) and gluteus medius/short external rotators (superior gluteal nerve/sciatic nerve). Muscles split: Gluteus maximus. Muscles detached: Piriformis, superior/inferior gemelli, obturator internus, quadratus femoris.
- Direct Anterior Approach: Increasingly popular. Internervous plane between tensor fascia lata (superior gluteal nerve) and sartorius/rectus femoris (femoral nerve). No muscles detached, but rectus femoris may be retracted.
- Anterolateral Approach (Hardinge): Internervous plane between gluteus medius/minimus (superior gluteal nerve) and tensor fascia lata (superior gluteal nerve). Requires partial detachment of gluteus medius/minimus.
- The choice of approach depends on surgeon training, patient anatomy, and comorbidities.
-
Hemiarthroplasty (HA) (Unipolar vs. Bipolar):
- Indication: Displaced fractures (Garden III/IV) in elderly, lower-demand patients without pre-existing arthritis.
-
Technique (e.g., Posterolateral Approach):
- Patient positioned in lateral decubitus or supine with bolsters.
- Incision: Curvilinear incision centered over the greater trochanter, extending proximally and distally.
- Dissection: Split gluteus maximus fibers. Identify and protect the sciatic nerve posteriorly.
- Short External Rotator Release: Detach piriformis and other short external rotators from the greater trochanter. Capsulotomy.
- Hip Dislocation: Flexion, adduction, and internal rotation to dislocate the femoral head posteriorly.
- Femoral Head Resection: Perform an osteotomy of the femoral neck at the appropriate level (typically 1 cm proximal to the lesser trochanter, matching templated offset).
- Femoral Canal Preparation: Sequential reaming and broaching of the femoral canal to prepare for the stem. Aim for appropriate anteversion and version.
- Trial Implants: Insert trial stem, neck, and unipolar/bipolar head. Reduce the hip. Assess leg length, offset, and stability in various positions.
- Final Implant Insertion: Insert the definitive stem (cemented or uncemented), then the chosen femoral head and unipolar/bipolar component.
- Reduction: Reduce the hip.
- Closure: Repair the posterior capsule and short external rotators (if possible/desired for stability), layer closure.
-
Total Hip Arthroplasty (THA):
- Indication: Displaced fractures (Garden III/IV) in active elderly patients with pre-existing symptomatic arthritis, or those with high functional demands.
-
Technique:
Follows HA technique for femoral preparation, but includes acetabular preparation:
- After femoral head resection, expose the acetabulum.
- Acetabular Reaming: Sequentially ream the acetabulum to appropriate size and depth, aiming for 40-45 degrees inclination and 15-20 degrees anteversion.
- Trial Acetabular Component: Insert trial shell and liner to verify stability and range of motion.
- Definitive Acetabular Component: Insert the definitive acetabular shell (press-fit or cemented), followed by the liner.
- Femoral Component: As with HA, prepare the femur and insert the stem.
- Head Insertion: Choose the appropriate femoral head length for optimal leg length and soft tissue tension.
- Reduction: Reduce the hip.
- Stability and Range of Motion Check: Assess through full range of motion.
- Closure: Layered closure.
Regardless of the technique, careful soft tissue handling, meticulous hemostasis, and accurate component positioning are essential to minimize complications and optimize long-term outcomes.
Complications & Management
Femoral neck fractures and their surgical management are associated with a significant incidence of complications, particularly given the typical patient demographic and the tenuous vascular supply of the femoral head.
Early Complications (within days to weeks)
-
Mortality:
- Incidence: Up to 10% at 30 days, 20-30% at 1 year. Significantly higher in elderly, frail patients with comorbidities.
- Management: Proactive medical optimization, early surgery, aggressive post-operative care, DVT/PE prophylaxis.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
- Incidence: High without prophylaxis (clinical DVT 40-60%, PE 1-5%).
- Management: Universal pharmacological prophylaxis (LMWH or direct oral anticoagulants) per institutional guidelines, mechanical prophylaxis (sequential compression devices), early mobilization. Symptomatic DVT/PE requires therapeutic anticoagulation; IVC filter for contraindications to anticoagulation.
-
Infection (Surgical Site Infection - SSI):
- Incidence: 1-5% for internal fixation, 0.5-2% for arthroplasty (deep infection).
- Management: Strict aseptic technique, prophylactic antibiotics (pre-incision and for 24 hours post-op), meticulous wound care. Superficial infections: wound care, oral antibiotics. Deep infections: surgical debridement and irrigation (DAIR), prolonged IV antibiotics. For arthroplasty, early deep infection may necessitate a two-stage revision (implant removal, spacer, antibiotics, then reimplantation).
-
Neurovascular Injury:
- Incidence: Rare (<1%), sciatic nerve (posterolateral approach), femoral nerve (direct anterior approach), obturator nerve, vascular injury.
- Management: Meticulous surgical technique, careful retraction, clear anatomical identification. Early recognition of neurological deficit post-op requires investigation (imaging, EMG/NCS) and possible exploration.
-
Periprosthetic Fracture (for Arthroplasty):
- Incidence: 0.5-2%, often intraoperative during stem insertion.
- Management: Intraoperative fractures often managed with cerclage wires or cables, or revised to a longer stem. Post-operative fractures (Vancouver classification) require revision surgery (fixation or reimplantation).
-
Dislocation (for Arthroplasty):
- Incidence: 2-5% for HA, 1-3% for THA (higher with posterolateral approach without posterior soft tissue repair).
- Management: Closed reduction under sedation is typically the first line. Recurrent dislocations may require revision to a larger head, constrained liner, or revision of component malposition.
-
Hardware Malposition / Cut-out (for Internal Fixation):
- Incidence: Variable, depends on reduction quality and bone stock.
- Management: Immediate revision of fixation or conversion to arthroplasty if malposition is recognized intraoperatively or very early post-op. Cut-out often leads to non-union or loss of reduction, necessitating conversion to arthroplasty.
-
Bleeding / Hematoma:
- Incidence: Common, requiring transfusions in some cases.
- Management: Meticulous hemostasis, drains (controversial), tranexamic acid. Large hematomas may require evacuation.
Late Complications (weeks to years)
-
Avascular Necrosis (AVN) of the Femoral Head (for Internal Fixation):
- Incidence: Varies widely, 10-30% for Garden I/II, up to 30-50% for Garden III/IV. Higher incidence with displaced fractures, poor reduction, and delayed surgery.
- Management: Symptomatic AVN usually requires conversion to HA or THA.
-
Non-union / Malunion (for Internal Fixation):
- Incidence: 10-30%, higher with displaced fractures, poor bone quality, inadequate fixation, or delayed weight-bearing. Malunion can lead to pain and altered biomechanics.
- Management: Symptomatic non-union typically requires revision to HA or THA. Malunion may require corrective osteotomy or arthroplasty.
-
Leg Length Discrepancy (LLD):
- Incidence: Common after arthroplasty, often perceived rather than true anatomical.
- Management: Careful pre-operative templating, intraoperative assessment (e.g., direct measurement, shuck test). Symptomatic LLD: shoe lift for shortening; for severe lengthening, sometimes revision is considered.
-
Heterotopic Ossification (HO):
- Incidence: 5-15%, higher with specific approaches (e.g., direct anterior).
- Management: Prophylaxis with NSAIDs (e.g., indomethacin) or low-dose radiation in high-risk patients. Symptomatic HO (pain, restricted ROM) may require surgical excision after maturation.
-
Prosthetic Loosening (Aseptic / Septic) (for Arthroplasty):
- Incidence: Long-term complication. Aseptic loosening is related to wear and biological response. Septic loosening is due to chronic infection.
- Management: Revision arthroplasty. Septic loosening requires a two-stage revision protocol.
-
Chronic Pain:
- Incidence: Can result from persistent hardware, malunion, arthrosis, or nerve irritation.
- Management: Multimodal pain management, hardware removal (if applicable), physical therapy, nerve blocks, or revision surgery.
Summary of Common Complications and Salvage Strategies
| Complication | Incidence (Approx.) | Salvage Strategy |
|---|---|---|
| Early Complications | ||
| Mortality (1-year) | 20-30% | Aggressive medical optimization, early surgery, DVT/PE prophylaxis, comprehensive post-op care. |
| DVT/PE | 1-5% (clinical PE) | Pharmacological & mechanical prophylaxis. Therapeutic anticoagulation for symptomatic events, IVC filter if contra. |
| Deep Infection | 0.5-2% | Surgical debridement & irrigation (DAIR), IV antibiotics. Two-stage revision for arthroplasty. |
| Neurovascular Injury | <1% | Meticulous surgical technique, careful retraction. Urgent exploration for profound deficits. |
| Periprosthetic Fracture | 0.5-2% | Intraoperative: cerclage, longer stem. Post-op: revision (fixation or reimplantation) per Vancouver classification. |
| Dislocation (Arthroplasty) | 2-5% | Closed reduction. Recurrent: larger head, constrained liner, component revision. |
| Hardware Malposition/Cut-out | Variable | Revision of fixation or conversion to arthroplasty. |
| Late Complications | ||
| Avascular Necrosis (AVN) | 10-50% | Conversion to hemiarthroplasty or total hip arthroplasty. |
| Non-union / Malunion | 10-30% | Conversion to hemiarthroplasty or total hip arthroplasty. Corrective osteotomy for specific malunions. |
| Leg Length Discrepancy (LLD) | Common (perceived) | Shoe lift. Severe cases: revision arthroplasty. |
| Heterotopic Ossification (HO) | 5-15% | Prophylaxis (NSAIDs/radiation). Surgical excision for symptomatic, mature HO. |
| Aseptic Loosening (Arthroplasty) | Long-term | Revision arthroplasty. |
| Chronic Pain | Variable | Multimodal pain management, hardware removal, physical therapy, revision if indicated. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is an integral component of the overall management of femoral neck fractures, aiming to restore functional independence, optimize mobility, and prevent secondary complications. Protocols are tailored to the specific surgical intervention, patient's pre-injury functional status, and bone quality.
General Principles
- Pain Management: Aggressive, multimodal pain control (opioids, NSAIDs, acetaminophen, regional nerve blocks) to facilitate early mobilization.
- DVT/PE Prophylaxis: Continue pharmacological and mechanical prophylaxis until the patient is fully ambulatory.
- Early Mobilization: Crucial for preventing deconditioning, pneumonia, pressure ulcers, and DVT. Initiated on post-operative day 0 or 1.
- Progressive Weight-Bearing: Dictated by the stability of fixation or prosthesis.
- Patient Education: Instruct on weight-bearing restrictions, hip precautions (if applicable), and exercise progression.
Internal Fixation (e.g., Cannulated Screws)
The goal is to protect the fracture site while allowing for healing. Weight-bearing status is critical and often guarded due to the risk of re-displacement or non-union.
-
Phase I: Acute Post-operative (Day 0 - Week 6-12)
-
Weight-Bearing:
- Non-displaced / Impacted (Garden I/II): Touch-down weight-bearing (TDWB) or toe-touch weight-bearing (TTWB) with crutches or walker. Progression to partial weight-bearing (PWB) as pain allows and radiographic healing progresses (typically around 6 weeks). Full weight-bearing (FWB) may be delayed until 12 weeks or later, depending on fracture consolidation.
- Displaced (Reduced and Fixed): Often TTWB for 6-12 weeks, with progression to PWB/FWB only after radiographic signs of bridging callus and clinical stability. Some surgeons advocate for strict non-weight-bearing (NWB) for longer periods in young patients.
-
Exercises:
- Ankle pumps, quadriceps sets, gluteal sets.
- Gentle active-assisted and active range of motion (ROM) of the hip and knee within pain limits. Avoid extreme ranges (e.g., excessive external rotation) that may stress the fixation.
- Supervised transfers (bed to chair), sit-to-stand, gait training with appropriate assistive device.
-
Weight-Bearing:
-
Phase II: Intermediate (Week 6-12 onwards)
- Weight-Bearing: Progress from PWB to FWB as tolerated, based on radiographic evidence of healing and clinical examination (lack of pain, stability).
-
Exercises:
- Progressive strengthening of hip abductors, adductors, flexors, and extensors (e.g., resisted hip flexion/extension, abduction/adduction with bands).
- Core stability exercises.
- Balance and proprioception training.
- Increased gait distance and endurance training, progressing from walker to crutches to cane.
-
Phase III: Advanced / Return to Activity (Week 12 onwards)
- Weight-Bearing: Full weight-bearing, pain-free.
- Exercises: Continue strengthening. Incorporate functional activities, sport-specific training (if applicable for younger patients).
- Return to light activities of daily living (ADLs) and recreational activities. Avoid high-impact activities until complete healing and bone remodeling, often 6-12 months.
- Monitor for signs of AVN or non-union.
Arthroplasty (Hemiarthroplasty or Total Hip Arthroplasty)
Arthroplasty provides immediate stability, allowing for more aggressive weight-bearing protocols, which is particularly beneficial for elderly patients.
-
Phase I: Acute Post-operative (Day 0 - Week 6)
- Weight-Bearing: Weight-bearing as tolerated (WBAT) with an assistive device (walker or crutches) is typically allowed immediately, unless there are concerns about cement mantle, fixation of uncemented components, or a periprosthetic fracture.
-
Hip Precautions:
Crucial for THA, especially with posterolateral approach, to prevent dislocation.
- Posterolateral: Avoid hip flexion >90 degrees, internal rotation, and adduction past midline.
- Direct Anterior/Anterolateral: Typically allow for fewer restrictions, but often advise against hip extension, external rotation, and abduction. Follow surgeon's specific recommendations.
-
Exercises:
- Ankle pumps, quadriceps sets, gluteal sets.
- Gentle active-assisted and active ROM of the hip and knee.
- Supine hip abduction slides, heel slides.
- Supervised transfers, sit-to-stand, gait training with WBAT.
-
Phase II: Intermediate (Week 6-12)
- Weight-Bearing: Progress to cane or no assistive device as strength and balance improve.
-
Exercises:
- Progressive strengthening of hip musculature (abductors, extensors are key).
- Stationary cycling, aquatic therapy.
- Balance and gait training (e.g., tandem walking, stepping exercises).
- Continue with hip precautions until soft tissue healing and stability are confirmed (usually 6-12 weeks).
-
Phase III: Advanced / Return to Activity (Week 12 onwards)
- Weight-Bearing: Full, independent ambulation.
- Exercises: Continue strengthening and conditioning. Integrate functional activities.
- Low-impact activities (swimming, cycling, walking) are encouraged. High-impact sports (running, jumping, contact sports) are generally discouraged to minimize implant wear and loosening risk.
- Regular follow-up to monitor for implant loosening or other late complications.
Importance of Multidisciplinary Team: The success of rehabilitation hinges on a coordinated effort involving orthopedic surgeons, physical therapists, occupational therapists, nurses, and social workers to address the patient's physical, functional, and psychosocial needs. Individualized protocols and regular reassessment are key.
Summary of Key Literature / Guidelines
The management of femoral neck fractures has evolved significantly, guided by extensive research and the development of evidence-based guidelines. Several landmark studies and professional society recommendations inform current best practices.
-
Timing of Surgery:
- Multiple systematic reviews and meta-analyses consistently demonstrate that early surgical intervention (within 24-48 hours) for hip fractures, including femoral neck fractures, is associated with reduced 30-day and 1-year mortality, lower rates of post-operative complications (e.g., pneumonia, pressure sores), and shorter hospital stays. Guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the National Institute for Health and Care Excellence (NICE) in the UK strongly recommend surgery within this timeframe for most patients, provided medical optimization is rapidly achievable.
-
Treatment of Displaced Femoral Neck Fractures in Older Adults:
- For displaced femoral neck fractures (Garden III/IV) in physiologically older patients (typically >65-70 years) , arthroplasty is the preferred treatment due to high rates of AVN and non-union with internal fixation.
-
Hemiarthroplasty (HA) vs. Total Hip Arthroplasty (THA):
- The HEALTH (Hip fracture Evaluation of pAtient-specific treatment) trial (2019) , a large, multicenter RCT, compared HA and THA for displaced femoral neck fractures in patients over 50 years. It found no significant difference in reoperation rates at 2 years. However, secondary analyses and other studies often suggest that THA provides superior functional outcomes and lower rates of revision for any cause compared to HA in active, cognitively intact elderly patients without severe comorbidities, particularly for those with pre-existing arthritis. THA, however, has a higher risk of early dislocation.
- Cemented HA has generally been shown to provide better pain relief and lower revision rates than uncemented HA, especially in osteoporotic bone.
-
Treatment of Non-Displaced and Impacted Femoral Neck Fractures:
- Non-displaced or impacted femoral neck fractures (Garden I/II) in most patient populations are typically treated with internal fixation (e.g., cannulated screws) . This aims to prevent displacement and preserve the native hip joint. The risk of AVN and non-union is lower than in displaced fractures but still present.
-
Treatment of Femoral Neck Fractures in Young Adults (<60-65 years):
- For younger patients with femoral neck fractures , anatomical reduction and stable internal fixation remain the gold standard, regardless of displacement. The goal is to preserve the femoral head, even with the recognized risks of AVN and non-union, as primary arthroplasty is undesirable due to potential for multiple revisions over a lifetime.
- The FAITH (Fixation Using Alternative Implants for the Treatment of Hip Fractures) trial (2017) compared sliding hip screws with cannulated screws for femoral neck fractures (though not exclusively young patients). It found no significant difference in reoperation rates or health-related quality of life between the two implants, but cannulated screws are generally preferred due to less invasive approach.
-
DVT Prophylaxis:
- All patients undergoing hip fracture surgery should receive pharmacological prophylaxis for DVT/PE (e.g., LMWH, fondaparinux, DOACs) for at least 10-14 days post-operatively, often extending for up to 35 days, in addition to mechanical prophylaxis. The specific agent and duration should follow institutional guidelines.
-
Post-Operative Rehabilitation:
- Early mobilization is a cornerstone of post-operative care, with physical therapy beginning on post-operative day 0 or 1.
- Weight-bearing protocols vary: WBAT for most arthroplasty patients, while internal fixation often requires protected weight-bearing for several weeks to months, depending on fracture stability and healing.
-
Future Directions and Ongoing Debates:
- Ongoing research focuses on refining indications for THA versus HA in specific elderly subgroups, optimizing internal fixation techniques to reduce AVN and non-union rates in younger patients (e.g., direct reduction, capsulotomy, bone grafting), and the role of robotic assistance in arthroplasty for fracture. The long-term outcomes and cost-effectiveness of various implant choices continue to be evaluated.
In conclusion, current literature strongly supports prompt surgical intervention, tailored treatment based on patient age and fracture displacement, and adherence to established protocols for DVT prophylaxis and rehabilitation to improve outcomes for patients with femoral neck fractures.
You Might Also Like