Dorsolateral Approach to Scaphoid Fractures: A Comprehensive Surgical Guide
Key Takeaway
The dorsolateral approach to the scaphoid offers excellent exposure, particularly for the waist and proximal pole, while preserving crucial volar vascularity. It is indicated for complex scaphoid fractures and nonunions, allowing precise anatomical reduction and fixation. Careful attention to surgical anatomy, including the superficial branch of the radial nerve and dorsal carpal artery, is paramount to minimize complications.
Excellent & Safe Approach to the Scaphoid: Dorsolateral Mastery
Introduction & Epidemiology
Scaphoid fractures represent the most common carpal bone fracture, accounting for approximately 60-70% of all carpal injuries and 10% of all hand fractures. These injuries predominantly affect young, active individuals, frequently resulting from a fall onto an outstretched hand with the wrist hyperextended and radially deviated. The unique anatomy, tenuous vascular supply, and biomechanical role of the scaphoid render its fractures prone to complications such as nonunion, malunion, and avascular necrosis (AVN), particularly affecting the proximal pole. Untreated or poorly managed scaphoid fractures can lead to progressive carpal collapse, carpal instability, and debilitating wrist arthritis (SNAC wrist – Scaphoid Nonunion Advanced Collapse).
The optimal management strategy for scaphoid fractures varies based on fracture location, displacement, stability, and patient factors. While stable, undisplaced fractures can often be managed conservatively with cast immobilization, displaced or unstable fractures, as well as established nonunions, typically necessitate surgical intervention. Various surgical approaches have been described for the scaphoid, including volar, dorsal, and dorsolateral. The dorsolateral approach, while less frequently discussed in some literature compared to the volar approach for acute fractures, offers distinct advantages for specific indications, providing excellent exposure to the waist and proximal pole of the scaphoid while preserving crucial volar vascularity. This detailed review aims to delineate the anatomical considerations, indications, surgical technique, potential complications, and post-operative management associated with the dorsolateral approach, emphasizing its utility as a powerful tool in the orthopedic surgeon's armamentarium for complex scaphoid pathology.
Surgical Anatomy & Biomechanics
A thorough understanding of scaphoid anatomy, vascularity, and its contribution to carpal biomechanics is paramount for successful surgical outcomes.
Scaphoid Anatomy and Vascularity
The scaphoid is a boat-shaped carpal bone located in the proximal carpal row, articulating with the radius proximally, the trapezium and trapezoid distally, and the lunate and capitate medially. Its waist is the narrowest part and the most common site of fracture. The scaphoid is largely covered by articular cartilage, making it challenging for extra-osseous vascularization.
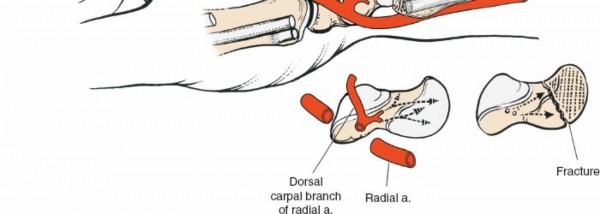
The blood supply to the scaphoid is predominantly intra-osseous and precarious. Approximately 70-80% of the blood supply enters the distal pole via branches of the radial artery (superficial palmar branch and palmar carpal branch). These vessels ascend proximally, supplying the waist and proximal pole in a retrograde fashion. A smaller percentage of vessels (20-30%) enter the dorsal surface of the scaphoid, primarily from the dorsal carpal branch of the radial artery, supplying a portion of the dorsal scaphoid body and sometimes the proximal pole. The critical implication of this retrograde vascularity is that fractures through the waist or proximal pole can disrupt the main blood supply to the proximal fragment, significantly increasing the risk of AVN and nonunion. This dorsal blood supply, while less dominant overall, can be critically important in certain scenarios and must be respected during a dorsal or dorsolateral approach.
Key Neurovascular Structures
Several critical neurovascular structures are in proximity to the dorsolateral approach and must be identified and protected:
- Superficial Branch of the Radial Nerve (SBRN): This nerve emerges from beneath the brachioradialis tendon approximately 9 cm proximal to the radial styloid. It crosses the first dorsal compartment tendons (abductor pollicis longus, APL; extensor pollicis brevis, EPB) to supply sensation to the dorsoradial aspect of the hand, thumb, and radial 2.5 fingers. It is highly vulnerable during dorsolateral incisions, particularly when extending proximally or dissecting superficially.
- Cephalic Vein: Located subcutaneously along the radial border of the forearm and wrist, this vein can be quite prominent and should be identified and protected or ligated carefully.
- Dorsal Carpal Branch of the Radial Artery: This branch courses distally over the dorsal aspect of the wrist, contributing to the dorsal carpal arch and supplying some of the scaphoid's dorsal vascularity. It runs beneath the extensor retinaculum and often overlies the scapholunate ligament. Its preservation is important.
- First Dorsal Compartment Tendons: The APL and EPB tendons form the radial border of the anatomical snuffbox. These tendons must be retracted, or their sheaths incised, to gain access to the scaphoid.
- Extensor Pollicis Longus (EPL) Tendon: This tendon forms the ulnar border of the anatomical snuffbox and can be retracted ulnarly.
Carpal Biomechanics
The scaphoid acts as a critical link between the proximal and distal carpal rows, effectively bridging the radiocarpal and midcarpal joints. It undergoes significant motion during wrist flexion-extension and radial-ulnar deviation, translating forces between the radius and the distal carpal row (trapezium, trapezoid, capitate). Disruption of the scaphoid's integrity or its articulations can lead to aberrant carpal kinematics, progressive instability, and ultimately degenerative changes. Successful surgical management aims to restore the scaphoid's anatomical alignment and stable fixation, thereby preserving normal carpal biomechanics.
Indications & Contraindications
The dorsolateral approach offers an excellent and safe exposure of the scaphoid bone. Its major drawback is that it endangers the superficial branch of the radial nerve, and it also may interfere with the dorsal blood supply of the scaphoid. This approach is generally preferred when direct visualization and access to the dorsal aspect of the scaphoid, particularly the proximal pole and waist, are required.
Indications for the Dorsolateral Approach:
- Bone grafting for nonunion: Especially effective for established scaphoid nonunions, particularly those with proximal pole AVN or significant bone loss, as it allows direct visualization of the nonunion site, débridement, and placement of structural or cancellous bone grafts.
- Excision of the proximal fragment of a nonunited scaphoid: In cases of severe proximal pole AVN, collapse, or significant bone loss where salvage is not feasible, excision of the necrotic proximal fragment may be considered, often as a salvage procedure.
- Excision of the radial styloid in combination with either of the two above procedures: Radial styloidectomy can be performed concurrently to address impinging osteophytes, treat localized degenerative changes (e.g., radioscaphoid arthritis), or improve access to the scaphoid.
-
Open reduction and internal fixation of fractures of the scaphoid:
- Proximal pole fractures: This approach provides direct access to difficult-to-reduce proximal pole fractures.
- Displaced scaphoid waist fractures: Especially those with dorsal comminution or displacement that is difficult to reduce from a volar approach.
- Failed percutaneous fixation: When percutaneous attempts fail to achieve adequate reduction or fixation.
- When combined with a volar approach to the scaphoid: A combined dorsolateral and volar approach (two-portal approach) can be utilized for complex fractures, difficult reductions, or when simultaneous access to both poles is required for screw placement or bone grafting. This might be necessary for very comminuted fractures or when a headless compression screw needs to be placed from both ends for maximum stability and compression.
- Repair of complete ruptures of the scapholunate ligament: While typically a dorsal approach, the dorsolateral variant can provide excellent visualization for direct repair or reconstruction of scapholunate instability, particularly for augmenting posterior capsular repair or addressing associated scaphoid pathology.
- Scaphoid Cysts or Osteochondral Lesions: Direct access for débridement or grafting.
Contraindications:
- Significant volar displacement or comminution: Where primary access and reduction are better achieved volarly.
- Purely distal pole fractures: These are generally well-vascularized and often amenable to percutaneous fixation or a smaller volar approach.
- Extensive volar soft tissue injury: Where a volar approach would compromise tissue viability.
- Patient factors: Severe coagulopathy, active local infection, or medical comorbidities precluding surgery.
- Prior surgery or scarring that would complicate a dorsolateral dissection and jeopardize critical structures, though this is a relative contraindication.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management (Dorsolateral Approach Often Preferred) | Non-Operative Management (Cast Immobilization) |
|---|---|---|
| Acute Fractures |
- Displaced fractures (>1mm)
- Unstable fractures (e.g., radioscaphoid angle >60°, intraluminal angle >35°, carpal collapse) - Proximal pole fractures - Vertical oblique fractures - Comminuted fractures - Failed conservative treatment |
- Nondisplaced, stable fractures of the waist or distal pole (e.g., type A or B1 Herbert classification)
- Suspected scaphoid fracture with negative initial radiographs but positive MRI/CT, managed with thumb spica cast until confirmed union. |
| Scaphoid Nonunions |
- Symptomatic nonunion
- Nonunion with deformity (e.g., humpback deformity) - Nonunion with avascular necrosis of the proximal pole - Progressive carpal collapse (SNAC wrist) |
- Asymptomatic nonunion (rarely, especially in older, less active patients, with informed consent and close monitoring for progression of arthritis)
- High surgical risk patients where nonunion is tolerated. |
| Scapholunate Ligament | - Complete ruptures (acute or chronic repair/reconstruction) | - Partial tears or dynamic instability (often managed with immobilization, activity modification, or observation) |
| Associated Pathology |
- Radial styloid impingement/osteophytes
- Symptomatic scaphoid cysts/osteochondral lesions |
- Asymptomatic radial styloid impingement without associated scaphoid pathology. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing outcomes and minimizing complications.
Pre-Operative Planning
-
Imaging Review:
- Plain Radiographs: Standard scaphoid series (PA, lateral, oblique, and scaphoid views) are the initial diagnostic tool, assessing fracture location, displacement, and pre-existing degenerative changes.
- Computed Tomography (CT): Essential for detailed evaluation of fracture morphology, comminution, displacement, cortical defects, and presence of nonunion or AVN. Coronal, sagittal, and 3D reconstructions are invaluable for surgical planning.
- Magnetic Resonance Imaging (MRI): Useful for assessing vascularity of the proximal pole (especially in nonunions), detecting bone edema, occult fractures, and ligamentous injuries (e.g., scapholunate).
-
Surgical Strategy:
- Determine the exact fracture pattern, stability, and presence of bone loss or AVN.
- Plan the type of fixation (e.g., cannulated headless compression screw, conventional screw, K-wires) and the desired trajectory.
- Decide on the need for bone grafting (autograft vs. allograft, structural vs. cancellous) and its harvest site if autograft is chosen (e.g., distal radius, iliac crest).
- Consider the need for radial styloidectomy or combined approaches.
- Equipment Preparation: Ensure all necessary instruments, drills, guide wires, screws (various lengths/diameters), bone graft harvesting tools, and fluoroscopy unit are readily available and sterile.
Patient Positioning
Place the patient supine on the operating table, with the arm extended on an arm board. Pronate the forearm to expose the dorsoradial aspect of the wrist. This pronated position brings the dorsolateral aspect of the scaphoid into better view and facilitates access. A sterile tourniquet is applied to the upper arm, and an exsanguinating bandage (e.g., Esmarch) is used prior to inflation of the tourniquet (see Fig. 5-1 in the original context, implying an image of general tourniquet application and arm board setup).

The forearm is positioned on an arm board. The elbow is flexed slightly. The hand is pronated, and the wrist is slightly ulnar deviated, which can help bring the scaphoid more dorsally. Some surgeons prefer a traction tower for fluoroscopic control during reduction, although direct visualization often obviates this for the dorsolateral approach.
Detailed Surgical Approach / Technique
The dorsolateral approach to the scaphoid prioritizes direct visualization and meticulous dissection to protect vital structures.
Landmarks and Incision
The landmarks are crucial for accurate incision placement and safe dissection:
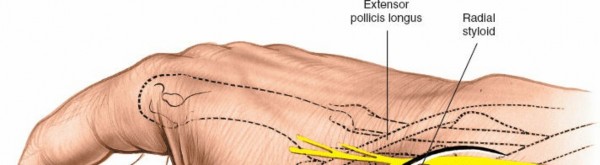
- Radial Styloid Process: This is the most prominent bony landmark on the radial side of the wrist. It is truly lateral when the hand is in the anatomic position. Palpate it in this position and then pronate the arm, keeping a finger on the styloid process.
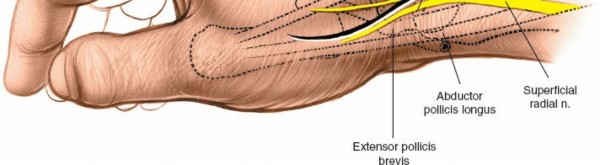
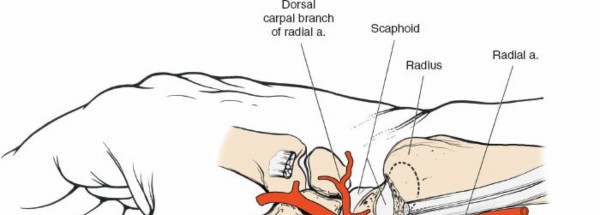
- Anatomic Snuff-box: This small depression is located immediately distal and slightly dorsal to the radial styloid process. It is bordered radially by the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons, and ulnarly by the extensor pollicis longus (EPL) tendon. The floor of the snuffbox is formed by the scaphoid and trapezium. The scaphoid tubercle can be palpated distally and volarly within the snuffbox. The radial artery courses through the floor of the snuffbox.
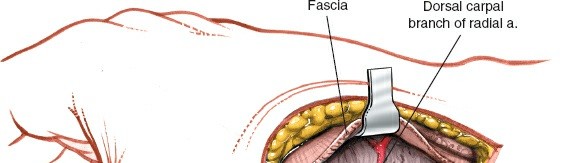
Illustration of anatomic snuffbox and radial styloid landmarks.
An incision is planned longitudinally, centered over the anatomical snuffbox, extending approximately 3-4 cm. It can commence just distal to the radial styloid and extend distally towards the base of the thumb metacarpal. A slight curvilinear extension proximally can be made parallel to the SBRN, or a more distal transverse limb can be added for increased exposure (modified Wiesel incision).
Depiction of the planned incision over the dorsolateral aspect of the wrist.
Dissection
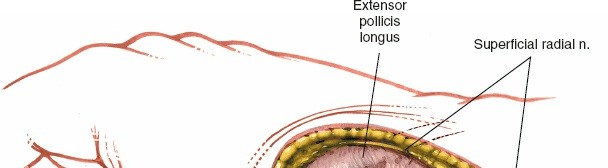
- Skin and Subcutaneous Tissues: Incise the skin and subcutaneous fat. The superficial branch of the radial nerve (SBRN) and the cephalic vein lie superficially in this region. The SBRN typically courses obliquely across the first dorsal compartment. Identify these structures immediately and protect them meticulously throughout the procedure. The nerve branches often run in the subcutaneous fat. Mobilize the SBRN branches and retract them radially or ulnarly, employing careful blunt dissection to avoid traction injury or neurotmesis. The cephalic vein, if encountered, can be ligated or retracted.
Superficial dissection showing careful identification and protection of the SBRN.
Another view emphasizing the superficial nature of the SBRN branches requiring protection.
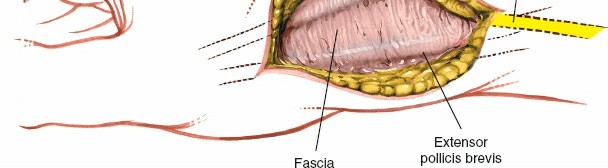
- First Dorsal Compartment: Identify the tendons of the abductor pollicis longus (APL) and extensor pollicis brevis (EPB), which define the radial border of the snuffbox. The tendon sheaths can be incised longitudinally to allow for gentle retraction. These tendons are retracted radially to expose the floor of the snuffbox.
Exposure of the first dorsal compartment tendons after careful skin incision.
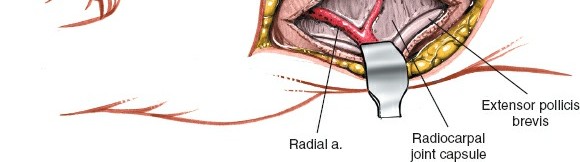
- Floor of the Snuffbox and Radial Artery: Deep to the first dorsal compartment tendons, the floor of the snuffbox is exposed. The radial artery traverses the floor of the snuffbox. Carefully identify and retract the radial artery ulnarly. Proximally, the artery passes deep to the APL/EPB tendons. Distally, it passes over the trapezium.
Deep dissection showcasing the radial artery within the snuffbox, retracted for access.
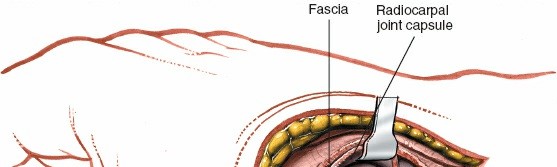
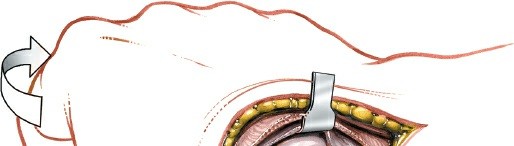
- Dorsal Carpal Ligaments and Capsule: After retracting the radial artery, the dorsal capsule of the wrist and the dorsal carpal ligaments are visualized. The dorsal carpal branch of the radial artery may be seen here. Carefully incise the capsule longitudinally, extending across the interval between the radius and scaphoid, and distally over the scaphoid waist. A dorsal capsulotomy is performed, raising a flap of capsule if necessary for later repair.
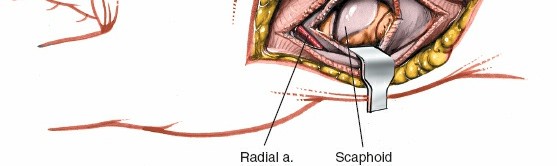
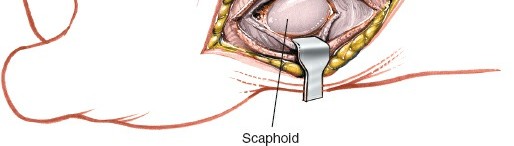
Capsulotomy revealing the underlying carpal bones, including the scaphoid.
Scaphoid Exposure and Fracture Management
- Scaphoid Exposure: With the capsule incised and retracted, the scaphoid is directly exposed. Its characteristic boat-shape, waist, and proximal pole become visible. In cases of nonunion, the fibrous tissue filling the nonunion gap will be apparent. For acute fractures, the fracture line itself will be seen.
Direct visualization of the scaphoid after capsulotomy, exposing the fracture or nonunion site.
-
Debridement (Nonunions): For nonunions, meticulously debride all fibrous tissue and sclerotic bone from the fracture fragments. Curettage and burr can be used until healthy, bleeding bone is reached. This is critical for promoting vascularity and osteointegration of a bone graft. Address any "humpback" deformity by careful resection of the dorsal prominence of the scaphoid until proper alignment is achieved.
-
Fracture Reduction:
- Direct Visualization: The dorsolateral approach allows direct visualization of the dorsal aspect of the scaphoid and its fragments.
- "Joystick" Techniques: Small K-wires can be inserted into the fragments and used as "joysticks" to manipulate and reduce displaced fragments. Gentle traction and pronation of the hand can aid in reduction.
- Fluoroscopic Guidance: Intermittent fluoroscopy (AP, lateral, and oblique views) is indispensable to confirm anatomical reduction in all planes. The goal is to restore scaphoid length, alignment, and eliminate any humpback deformity. A temporary K-wire across the scaphotrapeziotrapezoid (STT) joint or radioscaphoid joint may be used to hold length and prevent collapse during reduction.
Radiographic confirmation of fracture reduction using K-wires for temporary stabilization.
-
Bone Grafting (Nonunions): If significant bone loss or AVN is present, bone grafting is performed after reduction.
- Cancellous Graft: For small gaps or areas of poor bone quality, cancellous autograft (e.g., from distal radius, iliac crest) is packed into the defect.
- Structural Graft: For larger defects or unstable nonunions, a structural graft (e.g., vascularized or non-vascularized corticocancellous block graft) may be required. This is typically precisely shaped and impacted into the defect to restore scaphoid morphology.
-
Internal Fixation:
- Screw Selection: Cannulated headless compression screws (e.g., Herbert, Acutrak) are commonly used due to their ability to provide interfragmentary compression and their low profile. Conventional cortical screws can also be used.
- Guide Wire Placement: Under fluoroscopic guidance, a guide wire is inserted from the dorsal aspect, through the proximal pole, across the fracture site, and into the distal pole. The ideal trajectory aims for the central axis of the scaphoid, maximizing cortical purchase in both fragments. Ensure the guide wire is not intra-articular.
- Drilling and Screw Insertion: The appropriate drill bit is used to create a pilot hole over the guide wire. The screw length is measured, and the selected headless compression screw is inserted. The screw should be fully countersunk below the articular surface to prevent impingement. Compression across the fracture site should be observed fluoroscopically.
- Multiple Screws/K-wires: For highly unstable or comminuted fractures, a second screw or additional K-wires may be used to enhance rotational stability or supplement fixation.

Intra-operative fluoroscopic image showing the guide wire placement and initial screw trajectory.
Final fluoroscopic image demonstrating stable screw fixation across the scaphoid fracture.
Closure
- Capsular Repair: The dorsal wrist capsule is carefully repaired using absorbable sutures. This helps to restore carpal stability and prevent dorsal impingement.
- Tendons: The first dorsal compartment tendon sheaths can be loosely repaired, or left open if no impingement is noted.
- Subcutaneous and Skin Closure: Subcutaneous tissues are closed with absorbable sutures. The skin is closed with non-absorbable sutures or staples.
- Dressing and Splint: A sterile dressing is applied, followed by a well-padded thumb spica splint or cast, ensuring the wrist is in slight extension and radial deviation to optimize healing.
Complications & Management
Despite meticulous technique, complications can arise following the dorsolateral approach to the scaphoid. A thorough understanding of these risks and their management is essential.
Common Complications and Salvage Strategies
| Complication | Incidence (Approximate) | Etiology | Management / Salvage Strategy |
|---|---|---|---|
| Superficial Radial Nerve (SBRN) Injury | 5-20% | Direct transection, traction, entrapment during closure, neuroma formation |
Prevention:
Meticulous identification and careful retraction of SBRN branches. Use of loupe magnification.
Mild Neuropraxia/Paresthesia: Observation, conservative management (nerve gliding exercises, desensitization). Persistent Neuroma/Severe Pain: Excision of neuroma and nerve grafting (e.g., sural nerve) or targeted denervation. Consider nerve blocks. |
| Scaphoid Nonunion | 5-15% (post-operative) | Inadequate reduction/fixation, poor vascularity, infection, premature mobilization, persistent bone loss. |
Prevention:
Anatomic reduction, rigid fixation, bone grafting as indicated.
Early Failure: Revision surgery with re-débridement, stable fixation, structural bone grafting (e.g., vascularized graft if AVN present). Late Failure/AVN: Salvage procedures such as wrist fusion (four-corner fusion or radiolunate fusion), proximal row carpectomy (PRC), or total wrist arthroplasty, depending on articular cartilage integrity and patient demands. |
| Avascular Necrosis (AVN) of Proximal Pole | 5-20% | Predominantly pre-existing or exacerbated by surgical disruption of dorsal vascularity. |
Prevention:
Careful dissection, minimizing disruption of dorsal capsular attachments, judicious use of bone grafting.
Early Detection: MRI. Established AVN (without collapse): Vascularized bone graft (e.g., 1,2 intercompartmental supraretinacular artery (1,2-ICSRA) flap, distal radius pedicled graft). Established AVN (with collapse/arthritis): Salvage procedures as for nonunion (e.g., PRC, four-corner fusion). |
| Infection | <1% | Contamination during surgery. |
Prevention:
Standard sterile technique, prophylactic antibiotics.
Superficial: Oral antibiotics, local wound care. Deep: Surgical irrigation and débridement, intravenous antibiotics, removal of hardware if necessary. |
| Malunion | <5% | Inadequate reduction, fixation loss. |
Prevention:
Anatomical reduction confirmed by fluoroscopy/CT, stable fixation.
Symptomatic Malunion (e.g., humpback deformity, loss of carpal height): Corrective osteotomy and grafting. Asymptomatic Malunion: Observation, watchful waiting for progressive arthritis. Severe Deformity/Arthritis: Salvage procedures (PRC, fusion). |
| Hardware-related Issues | 5-10% | Screw prominence (articular or dorsal), fracture of hardware. |
Prevention:
Careful sizing, countersinking screws below articular cartilage.
Symptomatic Prominence: Hardware removal. Hardware Fracture: If associated with nonunion, revision fixation and débridement/grafting. If union achieved, observation or removal if symptomatic. |
| Wrist Stiffness | 10-25% | Prolonged immobilization, scar tissue formation, capsular adhesions. |
Prevention:
Early controlled range of motion (ROM) as appropriate, judicious splinting, surgical débridement of scar tissue (arthrolysis).
Management: Hand therapy, dynamic splinting. If severe, surgical release of adhesions, capsulotomy. |
| Radioscaphoid Arthritis | Variable | Pre-existing, nonunion, malunion, continued abutment/instability. |
Prevention:
Achieve anatomical reduction and union.
Early Symptoms: NSAIDs, activity modification, steroid injections. Advanced Arthritis: Radial styloidectomy (if localized), PRC, four-corner fusion, wrist fusion, or total wrist arthroplasty depending on severity and global wrist function. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical component of successful scaphoid fracture management, aiming to optimize union rates, restore function, and minimize complications such as stiffness. Protocols may vary based on fracture stability, fixation achieved, and surgeon preference, but generally follow a structured progression.
Phase I: Immobilization & Protection (0-6 weeks post-op)
- Goal: Protect the operative site, allow for initial bone healing, minimize swelling.
-
Immobilization:
- 0-2 weeks: Forearm-based sugar tong splint or short arm thumb spica splint with the wrist in slight extension and radial deviation. Digits are free.
- 2-6 weeks: Conversion to a removable custom thermoplastic short arm thumb spica splint or cast.
-
Activities:
- Elevation of the hand to reduce swelling.
- Gentle active range of motion (AROM) for the elbow, shoulder, and uninvolved digits (MCPs, IPs of thumb).
- No weight-bearing, gripping, or active wrist motion.
- Ice application for pain and swelling.
- Wound Care: Maintain clean, dry surgical dressing. Suture removal typically at 10-14 days.
Phase II: Controlled Mobilization (6-12 weeks post-op)
- Goal: Initiate controlled wrist motion, maintain tendon gliding, improve soft tissue extensibility, and continue bone healing.
- Imaging: Repeat radiographs (and potentially CT) at 6-8 weeks to assess signs of union. The initiation of active wrist motion is contingent upon radiographic evidence of early union or stability of fixation.
-
Therapy:
- Splinting: Continue removable thumb spica splint for protection during activities of daily living and at night. Remove for exercises.
- Wrist AROM: Begin gentle, pain-free active range of motion exercises for the wrist (flexion/extension, radial/ulnar deviation). Start with passive range of motion (PROM) if tolerated and indicated.
- Forearm Pronation/Supination: Begin gentle AROM.
- Thumb Mobilization: Progress active and passive thumb motion.
- Light Grip Strengthening: Begin with soft putty or sponge, avoiding excessive resistance.
- Scar Massage: Initiate once wound is fully healed to improve tissue mobility and reduce hypersensitivity.
- Precautions: Avoid heavy lifting, aggressive gripping, or activities that put undue stress on the scaphoid.
Phase III: Strengthening & Functional Return (12+ weeks post-op)
- Goal: Progress strengthening, restore full range of motion, and facilitate return to full activities.
- Imaging: Continue radiographic assessment (typically at 12-16 weeks) to confirm complete union.
-
Therapy:
- Splinting: Discontinue splinting once full union is confirmed and adequate strength is regained, or transition to a light wrist support as needed.
- Progressive Strengthening: Advance strengthening exercises using hand weights, resistance bands, and functional tools. Focus on wrist extensors, flexors, radial/ulnar deviators, and grip strength.
- Proprioception and Dexterity: Incorporate exercises to improve coordination and fine motor control.
- Return to Activity: Gradually progress to sport-specific or work-specific activities. Return to full unrestricted activities (e.g., contact sports, heavy manual labor) is typically allowed only after definitive radiographic union and satisfactory strength/ROM are achieved, which may be 4-6 months or longer.
- Considerations: Patients with nonunion, AVN, or more complex fractures may have a protracted recovery period and may not achieve full pre-injury function. Persistent pain or stiffness may necessitate further intervention or therapy modifications.
Summary of Key Literature / Guidelines
The management of scaphoid fractures and nonunions remains an area of ongoing research and evolving consensus. The dorsolateral approach, while often considered secondary to the volar approach for acute fractures, is a critical technique for specific, challenging presentations.
- Nonunion and AVN: For scaphoid nonunions, particularly those involving the proximal pole or associated with AVN, the dorsolateral approach combined with structural bone grafting (vascularized or non-vascularized) and internal fixation has demonstrated reliable union rates (70-90%). Literature, such as studies by Rikli et al. and Waitayawinyoo et al., has highlighted the effectiveness of dorsal approaches for addressing humpback deformity and allowing direct visualization for graft placement and fixation.
- Proximal Pole Fractures: Displaced proximal pole fractures are challenging due to their precarious blood supply and difficulty in achieving stable fixation. The dorsolateral approach is favored for these injuries, allowing direct reduction and accurate screw placement without compromising the critical volar blood supply. Studies by Herbert and Fisher demonstrated the advantages of headless compression screws via a dorsal approach for these difficult fractures.
- Combined Approaches: For complex cases, such as highly comminuted fractures or established nonunions with significant deformity, a combined volar and dorsolateral approach may be advantageous. This allows for optimal reduction, access for bone grafting, and bidirectional screw placement to maximize stability, as described by various authors advocating for a two-portal approach in specific scenarios.
- Minimally Invasive Techniques: While this review focuses on the open dorsolateral approach, it is important to acknowledge the role of percutaneous fixation techniques for appropriately selected, undisplaced acute fractures. However, for the indications listed, open reduction via a dorsolateral approach remains the gold standard for achieving anatomical reduction and stable fixation.
- Evidence on Outcomes: Long-term studies consistently show that anatomical reduction and rigid internal fixation are crucial for preventing nonunion and subsequent degenerative arthritis. While specific outcomes for the dorsolateral approach vs. volar approaches can be difficult to isolate due to varied indications, both approaches, when correctly applied, lead to comparable union rates and functional outcomes for their respective indications. The risk of SBRN injury remains a concern with the dorsolateral approach, emphasizing the need for meticulous surgical technique.
In conclusion, the dorsolateral approach to the scaphoid is a highly versatile and effective technique for managing complex scaphoid pathology, including displaced proximal pole fractures, scaphoid nonunions with or without AVN, and specific instances of scapholunate instability. Mastery of its anatomical nuances, meticulous surgical dissection, and adherence to sound biomechanical principles are paramount to achieving excellent and safe outcomes.
Clinical & Radiographic Imaging
You Might Also Like


