Acetabulum Fractures Diagnosis: Crucial Steps for Recovery
Key Takeaway
This topic focuses on Acetabulum Fractures Diagnosis: Crucial Steps for Recovery, **Acetabulum fractures diagnosis** primarily involves radiographic imaging. Initial assessment utilizes dedicated pelvis radiographs, including AP and Judet views (obturator and iliac oblique). For comprehensive evaluation and surgical planning, a CT pelvis is frequently required to precisely identify fracture patterns and any associated injuries, ensuring an accurate and detailed diagnosis.
Introduction & Epidemiology
Acetabulum fractures are critical injuries involving the articular surface of the hip joint. These pelvic fractures present a complex challenge due to their intra-articular nature, proximity to vital neurovascular structures, and significant potential for long-term morbidity, particularly post-traumatic osteoarthritis (PTOA). The inherent stability of the hip joint is compromised, demanding precise diagnostic evaluation and often meticulous surgical intervention to restore anatomical congruity and biomechanical function.
The diagnosis hinges primarily on high-quality radiographic assessment. Initial evaluation typically involves dedicated pelvis radiographs, including anterior-posterior (AP), iliac oblique (Judet), and obturator oblique (Judet) views. These specialized projections are crucial for characterizing the fracture pattern by visualizing the anterior and posterior columns and walls of the acetabulum. However, the complex three-dimensional anatomy and frequent comminution necessitate advanced imaging, specifically computed tomography (CT) of the pelvis with multiplanar reconstructions and 3D volumetric rendering. CT is indispensable for surgical planning, providing intricate detail regarding fragment displacement, articular step-off, marginal impaction, and incarcerated intra-articular fragments.
Acetabulum fractures exhibit a bimodal distribution in their epidemiology.
Incidence:
Approximately 4 per 100,000 per year.
Demographics:
*
Younger Patients:
High-energy trauma mechanisms predominate, such as motor vehicle accidents (MVAs), falls from significant height, or direct crush injuries. These patients often present with polytrauma, requiring adherence to Advanced Trauma Life Support (ATLS) protocols.
*
Elderly Patients:
Low-energy trauma, typically falls from standing height, accounts for a substantial proportion in this demographic. These fractures are often characterized by osteoporotic bone quality, influencing fracture patterns, surgical fixation strategies, and rehabilitation protocols.
Etiology & Pathoanatomy:
The fracture pattern is predominantly determined by:
*
Force Vector:
The direction and magnitude of the impact force on the greater trochanter or flexed knee.
*
Position of the Femoral Head:
The position of the hip joint (flexion, extension, abduction, adduction) at the moment of impact dictates the areas of stress concentration and subsequent fracture propagation. The femoral head acts as a "hammer" within the acetabulum.
*
Bone Quality:
Osteoporosis in the elderly contributes to more comminuted patterns and challenges in achieving stable fixation.
Associated Conditions:
These injuries frequently occur in conjunction with other significant orthopaedic and systemic traumas.
*
Orthopaedic Manifestations:
* Lower extremity injury (e.g., ipsilateral knee dislocation, femoral shaft fracture): 36%
* Nerve palsy (most commonly sciatic nerve): 13%
* Spine injury: 4%
*
Systemic Injuries:
* Head injury: 19%
* Chest injury: 18%
* Abdominal injury: 8%
* Genitourinary injury: 6%
Thorough systemic evaluation is paramount to identify and manage these concurrent injuries prior to definitive acetabular reconstruction.

Figure 1: Schematic representation of an acetabulum fracture, highlighting the involvement of the articular surface and the relationship to the femoral head.
Surgical Anatomy & Biomechanics
A profound understanding of acetabular anatomy and biomechanics is foundational for accurate diagnosis, precise surgical planning, and successful outcomes in acetabulum fractures.
Osteology
The acetabulum is a hemispherical socket on the lateral aspect of the innominate bone, formed by the fusion of the ilium, ischium, and pubis. It is typically inclined laterally and anteriorly.
*
Acetabular Inclination & Anteversion:
1.
Mean Lateral Inclination:
The angle between the anterior pelvic plane and a line connecting the superior and inferior horns of the acetabulum, typically 40-50 degrees.
2.
Mean Anteversion:
The angle between the anterior pelvic plane and a line perpendicular to the posterior wall, typically 15-20 degrees. Both angles are critical for hip stability and range of motion.
*
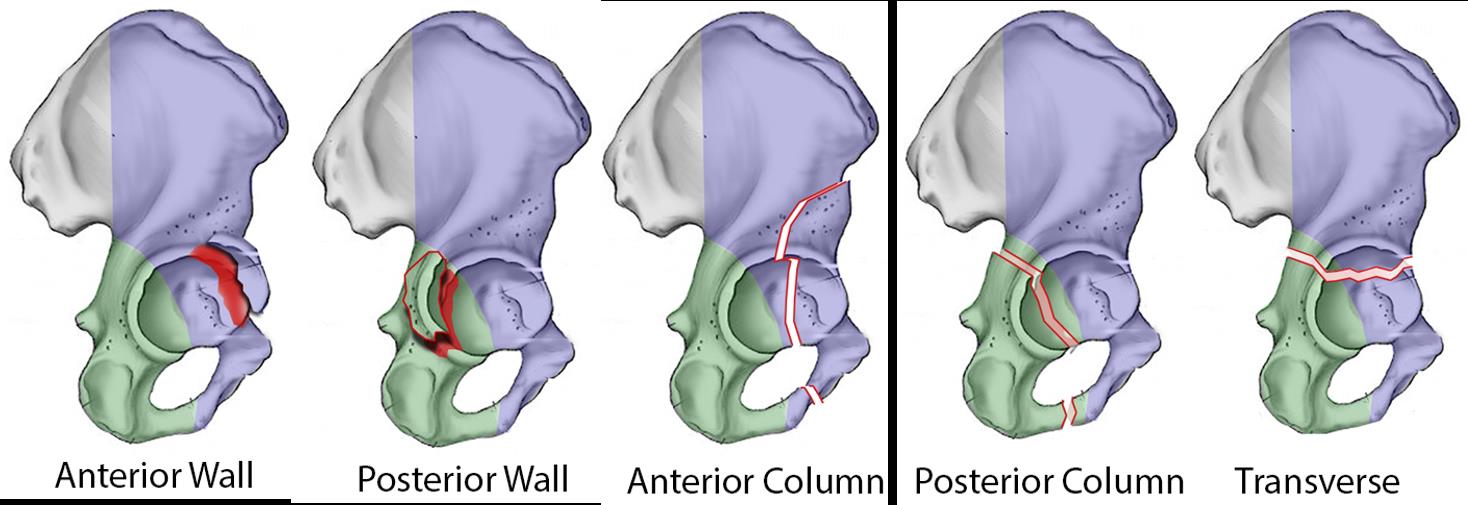
Columns of the Acetabulum (Judet and Letournel Classification):
*
Anterior Column:
Consists of the anterior part of the ilium, the anterior acetabular wall, the superior pubic ramus, and the obturator ring. It is bounded posteriorly by the iliopectineal line.
*
Posterior Column:
Comprises the posterior part of the ilium, the posterior acetabular wall, the ischial tuberosity, and the inferior pubic ramus. It is bounded anteriorly by the ilioischial line.
*
Walls of the Acetabulum:
*
Anterior Wall:
Formed by the anterior aspect of the ilium and superior pubic ramus.
*
Posterior Wall:
Formed by the posterior aspect of the ilium and ischium. This wall is critical for posterior hip stability.
*
Quadrilateral Surface:
The medial wall of the acetabulum, providing a broad, thin bony surface through which the femoral head can displace medially in both-column fractures.
*
Weight-Bearing Dome (Roof):
The superior, most robust portion of the acetabulum, crucial for transmitting axial loads. Fractures involving the dome significantly impair hip mechanics.
*
Key Bony Landmarks for Surgical Approaches:
*
Iliac Crest:
Origin of many muscles, guides the approach to the ilium.
*
Anterior Superior Iliac Spine (ASIS):
A key landmark for ilioinguinal and modified Stoppa approaches.
*
Ischial Tuberosity:
Important for posterior column orientation.
*
Pubic Symphysis:
An anterior landmark.
Ligamentous and Capsular Anatomy
- Articular Cartilage: Covers the horseshoe-shaped lunate surface, crucial for joint movement. The acetabular notch inferiorly is non-articular.
- Labrum: A fibrocartilaginous rim attached to the acetabular margin, deepening the socket and contributing to hip stability. It can be detached or torn in fractures.
- Joint Capsule: Strong fibrous capsule enveloping the hip joint, reinforced by distinct ligaments (iliofemoral, pubofemoral, ischiofemoral) that limit specific ranges of motion.
Neurovascular Anatomy
A detailed understanding of the adjacent neurovascular structures is paramount to prevent iatrogenic injury during surgical approaches.
*
Posterior Aspect:
*
Sciatic Nerve:
The largest nerve in the body, it courses deep to the piriformis muscle and superficial to the obturator internus, superior gemellus, inferior gemellus, and quadratus femoris muscles. It is highly susceptible to injury in posterior acetabular fractures or during posterior approaches (e.g., Kocher-Langenbeck).
*
Superior Gluteal Nerve and Vessels:
Emerge superior to the piriformis, supplying the gluteus medius and minimus. Vulnerable during approaches to the iliac wing.
*
Inferior Gluteal Nerve and Vessels:
Emerge inferior to the piriformis, supplying the gluteus maximus.
*
Anterior Aspect:
*
Femoral Nerve:
Lies lateral to the femoral artery in the femoral triangle, supplying the quadriceps femoris. At risk in anterior approaches to the pelvis.
*
Femoral Artery and Vein:
Occupy the middle and medial compartments of the femoral triangle, respectively.
*
Obturator Nerve and Vessels:
Course through the obturator foramen, supplying adductor muscles. Vulnerable during anterior approaches to the obturator ring or medial window.
*
Lateral Femoral Cutaneous Nerve:
Crosses the iliac crest near the ASIS, susceptible to stretch or transection in anterior approaches, leading to meralgia paresthetica.
*
Corona Mortis (Aberrant Obturator Artery):
An anatomical variant where an anomalous branch of the inferior epigastric artery (or external iliac) connects with the obturator artery. It crosses the superior pubic ramus and is at high risk of injury during dissection of the medial window of the ilioinguinal approach or the modified Stoppa approach, potentially leading to life-threatening hemorrhage. Preoperative imaging (CT angiogram) can identify this variant.

Figure 2: Comprehensive anatomical view of the acetabulum and surrounding structures, illustrating the columns, walls, and critical neurovascular bundles.
Biomechanics of Acetabulum Fractures
The mechanism of injury dictates the fracture pattern due to the interaction of force vectors and femoral head position.
*
Posterior Wall/Column Fractures:
Typically result from a direct blow to the flexed knee (dashboard injury) or a fall onto the greater trochanter with the hip flexed and internally rotated. The femoral head is driven posteriorly, impacting the posterior wall.
*
Anterior Wall/Column Fractures:
Less common, often resulting from a direct blow to the greater trochanter or a fall with the hip extended and externally rotated. The femoral head impacts the anterior rim.
*
Transverse Fractures:
Result from an axial load along the femoral shaft, driving the femoral head into the acetabulum. The fracture line crosses the articular surface from anterior to posterior.
*
Both-Column Fractures:
These are complex injuries where the articular surface is completely dissociated from the axial skeleton. The ilioischial and iliopectineal lines are disrupted. These fractures usually result from high-energy lateral compression or an axial load with the hip in abduction.
Understanding these biomechanical principles helps in interpreting radiographic findings, classifying the fracture, and planning the most appropriate reduction and fixation strategy.
Indications & Contraindications
The decision for operative versus non-operative management of acetabulum fractures is multifactorial, depending on fracture pattern, displacement, joint stability, patient comorbidities, and surgeon experience. Accurate diagnosis and classification (Judet and Letournel) are paramount in this decision-making process.
Non-Operative Indications
Non-operative management aims to achieve hip congruity and stability through conservative means, typically for select stable fracture patterns.
-
Minimally Displaced Fractures:
- Articular step-off or gap less than 2 mm on all radiographic views.
- No significant marginal impaction.
-
Stable Posterior Wall Fractures:
- Involvement of less than 20% of the posterior wall (based on radiographic measurement).
- Absence of hip instability (e.g., no subluxation on stress radiographs, absence of posterior sag).
- No incarcerated intra-articular fragments.
-
Select Anterior Column Fractures:
- Non-displaced or minimally displaced and without significant medial displacement of the femoral head or joint incongruity.
-
Both-Column Fractures with Secondary Congruity:
- A rare pattern where despite dissociation of both columns, the fractured fragments rotate such that the articular surface appears congruent with the femoral head. Close observation is required due to the potential for late displacement.
-
Medically Unstable Patient:
- Severe comorbidities (e.g., significant cardiac, pulmonary, or neurological compromise) that preclude safe anesthesia and surgery.
- Polytrauma patients with ongoing hemodynamic instability, coagulopathy, or uncontrolled sepsis.
-
Elderly Patients with Severe Osteoporosis:
- Extensive comminution in severely osteoporotic bone may make stable internal fixation difficult to achieve or maintain, leading to high complication rates. Non-operative management or primary total hip arthroplasty (THA) may be considered in these cases, although the latter is usually delayed.
-
Non-Ambulatory Patient/Limited Functional Demand:
- Patients with extremely low functional expectations or those who are already non-ambulatory may be considered for non-operative management if pain can be controlled.
Operative Indications
Operative fixation aims to restore anatomical joint congruity, stability, and biomechanical function, minimizing the risk of post-traumatic osteoarthritis.
-
Displaced Fractures:
- Articular step-off or gap ≥ 2 mm. This is the most critical indication, as articular incongruity directly correlates with the development of PTOA.
-
Hip Instability:
- Evidence of hip subluxation or dislocation that is irreducible by closed means, or unstable after closed reduction.
- Posterior wall fractures involving >20-30% of the posterior wall, especially with associated hip instability.
- Marginal impaction of the articular cartilage, particularly if it compromises hip stability or congruity.
-
Incarcerated Intra-articular Fragments:
- Bone or cartilage fragments lodged within the joint space, preventing concentric reduction or causing joint incongruity.
-
Irreducible Hip Dislocation:
- Dislocation that cannot be reduced by closed maneuvers, often due to an incarcerated fragment, soft tissue interposition, or significant fracture displacement. This constitutes a surgical emergency to prevent avascular necrosis of the femoral head.
-
Associated Femoral Head Fractures:
- Pipkin I-IV fractures in conjunction with acetabular fractures often necessitate operative intervention.
-
Sciatic Nerve Palsy Due to Fragment Compression:
- While controversial, persistent or worsening nerve palsy potentially attributable to a specific fracture fragment may warrant operative intervention for decompression.
Contraindications
-
Absolute Contraindications:
- Severe Medical Instability: Uncontrolled hemorrhage, severe head injury with elevated intracranial pressure, uncontrolled sepsis, myocardial infarction, or severe respiratory failure where the risks of anesthesia and surgery outweigh the potential benefits.
- Severe Soft Tissue Compromise: Extensive open wounds, severe degloving injuries, or necrotizing fasciitis that precludes a safe surgical approach.
- Active Infection: Cellulitis or osteomyelitis in the surgical field.
-
Relative Contraindications:
- Extensive Comminution with Poor Fixation Potential: Fractures with severe comminution that may not allow for stable fixation, especially in osteoporotic bone. Primary THA might be considered in the future if the patient is symptomatic.
- Significant Delay to Surgery (>3 Weeks): While not an absolute contraindication, operative intervention beyond 3 weeks significantly increases the difficulty of reduction due to fibrous union, requiring osteotomies and leading to higher complication rates and poorer outcomes.
- Pre-existing Arthritis: In patients with pre-existing symptomatic osteoarthritis of the hip, primary total hip arthroplasty may be considered in conjunction with or instead of osteosynthesis, especially in older patients.
Table: Operative vs. Non-Operative Indications for Acetabulum Fractures
| Feature/Indication | Non-Operative Management | Operative Management |
|---|---|---|
| Articular Displacement | < 2 mm step-off/gap | ≥ 2 mm step-off/gap |
| Hip Stability | Stable (no subluxation, <20% posterior wall involved) | Unstable (subluxation, >20-30% posterior wall, marginal impaction) |
| Intra-articular Fragments | Absent | Present (incarcerated bone/cartilage) |
| Fracture Pattern | Select non-displaced (e.g., stable posterior wall, anterior column without incongruity, secondary congruity) | Displaced Judet & Letournel elementary or associated patterns |
| Irreducibility of Dislocation | Reducible by closed means | Irreducible by closed means (surgical emergency) |
| Medical Status | Medically unstable (polytrauma, severe comorbidities) | Medically stable, amenable to surgery |
| Bone Quality | Severe osteoporosis precluding stable fixation | Adequate bone quality for stable fixation |
| Timing of Injury | Usually within first 2-3 weeks post-injury | Ideally within 3-10 days (to avoid fibrous union), urgent for irreducible dislocation |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful acetabular fracture reconstruction. It allows the surgeon to anticipate challenges, select the optimal approach, and prepare for potential complications.
Initial Assessment & Resuscitation
For high-energy trauma, ATLS protocols must be strictly followed. Hemodynamic stability, control of hemorrhage, and management of associated life-threatening injuries take precedence. Serial physical examinations are essential, with particular attention to neurovascular status of the lower extremities, especially the sciatic nerve. Compartment syndrome must be ruled out.
Imaging and Fracture Classification
- Dedicated Pelvic Radiographs: AP, iliac oblique, and obturator oblique (Judet views) are the initial standard. These define the fracture lines in relation to the columns and walls, enabling initial Judet and Letournel classification (Elementary: posterior wall, posterior column, anterior wall, anterior column, transverse; Associated: T-type, posterior column and wall, anterior column and posterior hemitransverse, both columns).
-
Computed Tomography (CT) Scan:
Mandatory for all acetabular fractures intended for operative management.
- Thin-cut axial images (1-2 mm slices): Essential for detailed visualization of fracture lines, articular step-off, comminution, and incarcerated fragments.
- Multiplanar Reconstructions (MPR): Coronal and sagittal views enhance understanding of fracture geometry.
- 3D Reconstructions: Provide invaluable spatial orientation of fragments, aiding in surgical approach selection, reduction strategy, and hardware placement. They allow for virtual manipulation and templating.
- CT Angiography: May be considered in cases of suspected major vascular injury or to map the "Corona Mortis" (aberrant obturator artery) if an anterior approach is planned.
- Magnetic Resonance Imaging (MRI): Not routinely used for acute fracture evaluation but can be helpful in cases of suspected labral injury, femoral head osteonecrosis, or ligamentum teres injury, though typically deferred post-fixation.
Timing of Surgery
- Urgent (within hours): Irreducible hip dislocation (to prevent avascular necrosis of the femoral head).
- Early (within 24-72 hours): Open fractures, rapidly deteriorating neurological status.
- Delayed (3-10 days): The majority of acetabular fractures are managed electively once the patient is medically optimized, swelling has subsided, and thorough pre-operative planning is complete. This "window of opportunity" allows for resolution of soft tissue edema and often improves outcomes compared to immediate surgery in a non-optimized patient. Operating beyond 3 weeks significantly increases technical difficulty due to fibrous union.
Surgical Approach Selection
The choice of surgical approach is dictated by the fracture pattern, column involvement, displacement, and surgeon familiarity. The goal is to obtain adequate exposure for anatomical reduction and stable fixation while minimizing iatrogenic injury.
-
Posterior Fractures (Posterior Wall, Posterior Column, Posterior Column and Wall, T-type, Transverse):
- Kocher-Langenbeck (K-L) Approach: The workhorse approach for posterior column and wall fractures. Allows excellent visualization of the posterior acetabulum.
-
Anterior Fractures (Anterior Wall, Anterior Column, Both Columns, Anterior Column and Posterior Hemitransverse):
- Ilioinguinal Approach: Provides exposure to the inner surface of the ilium, anterior column, and quadrilateral surface via three distinct windows.
- Modified Stoppa (Pararectus) Approach: Gaining popularity for anterior column and quadrilateral surface fractures due to potentially lower morbidity than ilioinguinal (less dissection of the spermatic cord/round ligament and improved visualization of the quadrilateral surface).
-
Combined Approaches:
- Extended Iliofemoral Approach: Reserved for highly complex both-column fractures or difficult reductions, providing wide exposure to the entire outer aspect of the ilium and both columns. Associated with higher morbidity.
- Sequential Approaches: Two separate approaches (e.g., K-L followed by ilioinguinal) often performed in two stages or by two teams, especially for complex associated fractures.
- Periacetabular Osteotomy (PAO) Principles: Sometimes an osteotomy may be required for specific complex reductions.
Templating and Hardware Selection
- Fracture Map: Using 3D CT reconstructions, the surgeon creates a mental or physical map of the fracture lines, fragment locations, and sequence of reduction.
- Plate Bending: Pre-contouring reconstruction plates (e.g., 3.5 mm pelvic reconstruction plates, LCP systems) on a pelvic model or using 3D printed templates can significantly reduce operative time.
- Screw Lengths and Types: Careful templating helps determine appropriate screw lengths to engage strong bone without violating the joint or neurovascular structures. Lag screws for interfragmentary compression, positional screws, and buttress plates are commonly used.
Patient Positioning and Surgical Setup
- C-Arm Fluoroscopy: Essential for intra-operative assessment of reduction and hardware placement. Requires clear access to the pelvis in AP, Judet, and outlet views.
- Traction Table: Often utilized for initial closed reduction of dislocations, fracture manipulation, and maintaining length. Requires careful padding and positioning to avoid nerve injury.
-
Specific Positions:
- Lateral Decubitus: For Kocher-Langenbeck approach. The patient is positioned lateral, often tilted slightly posteriorly, with the affected hip superior. Beanbag and hip spica help secure position.
- Supine: For ilioinguinal, modified Stoppa, or sometimes the anterior intrapelvic approaches. Legs often positioned "frog-leg" style for C-arm access.
Detailed Surgical Approach / Technique
Successful surgical management of acetabulum fractures requires meticulous attention to detail, precise anatomical dissection, and expert application of reduction and fixation techniques. The following outlines general principles and detailed steps for common approaches.
General Principles of Acetabular Fracture Surgery
- Anatomic Reduction: The primary goal is to restore the anatomical congruity of the articular surface. Residual step-off or gap of even 1-2 mm significantly increases the risk of PTOA.
- Stable Fixation: Once reduced, fragments must be held securely with plates and screws to allow for early mobilization and prevent secondary displacement.
- Preservation of Soft Tissues: Minimize soft tissue stripping, as extensive dissection can compromise vascularity and increase the risk of infection and heterotopic ossification (HO).
- Neurovascular Protection: Constant awareness of adjacent nerves and vessels to prevent iatrogenic injury.
- Timing: Optimal timing (3-10 days post-injury) allows for decreased tissue edema and patient optimization.
- Intraoperative Fluoroscopy: Essential for verifying reduction, hardware placement, and assessing articular congruity.
Kocher-Langenbeck (K-L) Approach (For Posterior Column/Wall Fractures)
This approach provides excellent exposure to the posterior acetabulum, gluteal region, and proximal femur.
- Patient Positioning: Lateral decubitus position, with the affected hip superior. The operating table is usually tilted slightly posteriorly to provide a clearer view of the hip. The pelvis is secured with a beanbag, and the knee is flexed approximately 45 degrees. A posterior approach drape allows for free movement of the limb.
- Incision: A curvilinear incision centered over the greater trochanter, extending proximally along the posterior aspect of the iliac crest and distally along the posterolateral aspect of the thigh for varying lengths depending on the fracture extent.
-
Dissection & Internervous Plane:
- The fascia lata is incised.
- The gluteus maximus is split longitudinally along its fibers, identifying and protecting the inferior gluteal nerve and vessels.
- Retract the gluteus maximus to expose the underlying short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus, quadratus femoris).
- Identify the sciatic nerve , which lies deep to the piriformis and superficial to the short external rotators. It must be carefully protected throughout the entire procedure. A Penrose drain or vessel loop is typically placed around it for gentle retraction.
- The short external rotators (often including piriformis) are detached from their insertions on the greater trochanter. This exposes the posterior aspect of the hip capsule and the posterior acetabulum.
- Capsulotomy: A T-shaped or H-shaped capsulotomy provides access to the hip joint for inspection, removal of incarcerated fragments, and direct visualization of the articular surface. The labrum is inspected for tears.
-
Reduction Techniques:
- Direct Visualization: The posterior wall and column fragments are directly visualized.
- Femoral Head Manipulation: The surgeon may use traction, internal/external rotation, or flexion/extension of the hip to manipulate the femoral head, which can aid in reducing fragments.
- Reduction Clamps: Pointed reduction clamps (e.g., Faraboeuf, Matta, Verbrugge) are used to grasp and reduce fragments. Care must be taken to avoid crushing bone or soft tissues.
- Bone Hooks/Joysticks: May be used to manipulate larger fragments.
- Marginal Impaction: Impacted articular fragments are gently elevated and bone grafted if there is a metaphyseal void beneath.
-
Fixation:
- Temporary Fixation: K-wires are used to provisionally hold reduced fragments.
-
Definitive Fixation:
- Posterior Wall: Buttress plates (e.g., 1/3 tubular or reconstruction plates) are contoured to the posterior column and fixed with screws. Lag screws are often used for interfragmentary compression.
- Posterior Column: Reconstruction plates are molded along the posterior column. Longer screws may be used to engage the anterior column for improved stability.
- Quadrilateral Surface: For fractures involving the quadrilateral surface (often in associated patterns), an anterior plate (via a modified Stoppa approach) or an intra-pelvic buttress plate from the posterior approach may be necessary.
- Closure: Reattach the short external rotators and capsule if possible. Close gluteus maximus split, fascia lata, subcutaneous tissues, and skin. Drain may be placed.
Ilioinguinal Approach (For Anterior Column/Wall, Both-Column Fractures)
This approach allows extensive exposure of the inner wall of the ilium, anterior column, and quadrilateral surface.
- Patient Positioning: Supine on a radiolucent table. The hip is positioned to allow full range of motion. Both legs are often "frog-legged" to allow optimal C-arm access.
- Incision: A classic "bikini" incision follows the iliac crest and extends medially along the inguinal crease. The incision typically extends from the ASIS to the pubic symphysis.
-
Dissection & Internervous Planes (Three Windows):
- The superficial dissection identifies the lateral femoral cutaneous nerve emerging near the ASIS. It is identified and protected to minimize the risk of meralgia paresthetica.
- The external oblique aponeurosis is incised, and the inguinal ligament is identified and detached from the ASIS and sometimes the rectus sheath.
- Lateral Window (Iliopectineal Fossa): Between the iliopsoas muscle laterally and the external iliac vessels medially. Exposure of the inner aspect of the iliac wing and the iliopectineal line. The femoral nerve lies lateral to the iliopsoas.
- Middle Window (Retropubic Space): Between the external iliac vessels laterally and the spermatic cord (males) or round ligament (females) medially. Exposure of the superior pubic ramus and pectineus muscle. The corona mortis (if present) must be identified and ligated/coagulated in this window.
- Medial Window (Retropubic Space): Medial to the spermatic cord/round ligament, lateral to the rectus abdominis muscle. Exposure of the pubic symphysis and obturator foramen.
-
Exposure and Reduction:
- Careful dissection and blunt retraction of the neurovascular bundle (femoral nerve, artery, vein) and the spermatic cord/round ligament.
- Reduction of the fracture fragments is achieved using traction, pointed reduction clamps, bone hooks, and elevators. The traction table may be used to aid in preliminary reduction.
- Special attention to the quadrilateral surface and medial displacement. An intra-pelvic plate may be necessary to buttress this area.
-
Fixation:
- Temporary Fixation: K-wires are critical for maintaining reduction.
- Definitive Fixation: Reconstruction plates are contoured along the pelvic brim (iliopectineal line) and secured with screws. Additional plates (e.g., spring plate, buttress plate) may be applied to the quadrilateral surface or to stabilize the anterior column.
- Closure: Reattach the inguinal ligament. Repair the external oblique aponeurosis, subcutaneous tissues, and skin.
Modified Stoppa (Pararectus) Approach (For Anterior Column/Wall, Quadrilateral Surface Fractures)
This approach offers advantages for anterior column and quadrilateral surface fractures, with reduced morbidity compared to the ilioinguinal approach.
- Patient Positioning: Supine on a radiolucent table.
- Incision: A longitudinal incision lateral to the midline, paramedian, extending from just above the umbilicus to the pubic symphysis.
-
Dissection & Internervous Plane:
- The anterior rectus sheath is incised longitudinally. The rectus abdominis muscle is retracted laterally (or medially).
- The posterior rectus sheath is opened transversally.
- The preperitoneal space is entered. The peritoneum is swept superiorly and medially, exposing the internal iliac fossa, obturator fossa, and quadrilateral surface.
- Crucial difference: This approach avoids extensive dissection around the inguinal canal and spermatic cord/round ligament, potentially reducing nerve injury and groin pain. The external iliac vessels and femoral nerve are generally visualized from their medial aspect.
-
Exposure and Reduction:
- Direct visualization of the entire anterior column, superior pubic ramus, and the critical quadrilateral surface.
- Reduction is performed from the inside-out. The bladder and peritoneum are protected.
- Specialized reduction clamps and internal manipulators are used to reduce fragments and counter medial displacement of the quadrilateral surface.
-
Fixation:
- Reconstruction plates are applied along the pelvic brim and specifically buttress the quadrilateral surface. A separate plate for the quadrilateral surface is often used, fixed from the inner aspect of the pelvis.
- Lag screws for interfragmentary compression.
- Closure: Repair the posterior and anterior rectus sheaths, subcutaneous tissues, and skin.

Figure 3: Intraoperative view during an acetabular fracture repair, demonstrating reduction clamps applied to fracture fragments.

Figure 4: Radiographic image showing internal fixation of an acetabulum fracture with plates and screws, demonstrating restoration of articular congruity.
Complications & Management
Acetabular fracture surgery is associated with a spectrum of potential complications, both early and late, which can significantly impact patient outcomes. Proactive prevention, early recognition, and effective management are crucial.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Management & Salvage Strategies |
|---|---|---|
| Nerve Injury | 5-25% (Sciatic most common) | Prevention: Meticulous dissection, careful retraction, intraoperative nerve monitoring. Management: Early recognition, EMG/NCS, conservative management (observation, physiotherapy), surgical exploration/decompression if deficit worsens or is complete, especially with evidence of direct compression. |
| Heterotopic Ossification (HO) | 15-50% (severe: 1-5%) | Prevention: Indomethacin (for 6 weeks) or single-dose radiation (700-800 cGy within 72 hrs post-op). Management: Prophylaxis, observation, surgical excision if functionally limiting after maturity (usually 6-12 months post-op). |
| Post-Traumatic Osteoarthritis (PTOA) | 20-50% | Prevention: Anatomic reduction (<1-2mm step-off/gap), stable fixation, early range of motion. Management: Non-operative (NSAIDs, PT, injections), activity modification. If severe and debilitating: Total Hip Arthroplasty (THA) (often technically challenging due to distorted anatomy, hardware, HO), sometimes hip arthrodesis in young active individuals as a last resort. |
| Infection (Superficial/Deep) | 1-5% | Prevention: Strict sterile technique, prophylactic antibiotics. Management: Superficial: wound care, oral antibiotics. Deep: surgical debridement, irrigation, retention of hardware if stable and no gross infection, or explantation/exchange (Girdlestone or THA in two stages) if unstable or septic. Long-term IV antibiotics. |
| DVT/Pulmonary Embolism (PE) | DVT: 15-40%, PE: 1-5% | Prevention: Mechanical (compression stockings, IPCs) and pharmacological prophylaxis (LMWH, fondaparinux) from admission until fully weight-bearing/ambulatory. Management: Anticoagulation (therapeutic), IVC filter if contraindication to anticoagulation. |
| Avascular Necrosis (AVN) of Femoral Head | 5-15% | Prevention: Urgent reduction of hip dislocation, careful soft tissue handling, avoid excessive traction. Management: Early stages: non-operative, core decompression. Late stages (collapse): THA. |
| Malunion/Nonunion | <5% | Prevention: Anatomic reduction, stable fixation, appropriate rehabilitation. Management: Symptomatic malunion: corrective osteotomy. Symptomatic nonunion: revision internal fixation with bone grafting, or THA. |
| Hardware Complications | 5-10% | Prevention: Proper implant selection, careful placement, avoidance of joint penetration. Management: Symptomatic hardware: hardware removal after fracture union. Joint penetration: urgent revision, removal, or adjustment. Plate breakage/screw pullout (due to nonunion or early weight-bearing): revision fixation, often with bone graft. |
| Hemorrhage | Significant in complex cases | Prevention: Careful pre-operative planning, intraoperative hemostasis, meticulous dissection, identification/ligation of vessels (e.g., Corona Mortis). Management: Intraoperative transfusion, embolization for recalcitrant bleeding, close monitoring. |
| Iatrogenic Fracture | <5% | Prevention: Gentle handling of fragments, appropriate screw lengths, avoiding stress risers. Management: Intraoperative fixation of new fracture, post-operative protection. |
Detailed Discussion of Key Complications
-
Nerve Injury:
- Sciatic Nerve: Most frequently injured, particularly in posterior fractures or during Kocher-Langenbeck approaches. Can result from direct trauma, traction, compression by fragments/hematoma, or iatrogenic injury during dissection/retraction.
- Femoral Nerve: Less common but can occur with anterior approaches (ilioinguinal, modified Stoppa) due to retraction or direct injury.
- Lateral Femoral Cutaneous Nerve: Prone to stretch or transection in anterior approaches, leading to meralgia paresthetica (sensory deficit and pain in the anterolateral thigh).
- Superior/Inferior Gluteal Nerves: Risk during extensive dissection of the gluteal muscles.
- Management: Pre-operative neurological assessment is critical. Intraoperative nerve monitoring (SSEP, EMG) can be considered. Post-operative re-evaluation. If a new or worsened deficit, careful observation, electrodiagnostic studies, and sometimes surgical exploration are indicated.
-
Heterotopic Ossification (HO):
- Abnormal bone formation in soft tissues around the joint. Common after acetabular surgery (especially with extensive muscle dissection, multiple procedures, or delayed surgery).
- Classification: Brooker Classification (I-IV).
- Prophylaxis: Indomethacin (NSAID) 25 mg TID for 6 weeks, or a single dose of radiation therapy (700-800 cGy) within 72 hours pre- or post-operatively, particularly for high-risk patients (e.g., severe head injury, delay to surgery, associated elbow fractures).
- Management: If severe and functionally limiting, surgical excision is performed after the HO has matured (usually 6-12 months post-op, confirmed by bone scan or radiographs showing stable ossification).
-
Post-Traumatic Osteoarthritis (PTOA):
- The most significant long-term complication, directly related to residual articular incongruity (>1-2 mm step-off or gap), articular cartilage damage at the time of injury, and development of AVN or malunion.
- Prevention: The ultimate goal of anatomical reduction and stable fixation.
- Management: Initially conservative. If debilitating, total hip arthroplasty (THA) is the gold standard salvage procedure. However, post-traumatic THA is technically more challenging due to distorted anatomy, scarring, HO, and retained hardware, leading to potentially higher complication rates (dislocation, infection) and shorter implant survival compared to primary THA.
-
Avascular Necrosis (AVN) of the Femoral Head:
- Occurs due to interruption of the blood supply to the femoral head, particularly in cases of hip dislocation or severe capsular disruption.
- Prevention: Prompt reduction of hip dislocation (ideally within 6 hours), careful handling of the capsule and retinacular vessels.
- Management: Non-operative for early stages. If collapse occurs, THA is indicated.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing functional recovery, preventing complications, and mitigating the long-term impact of acetabular fractures. Protocols vary based on fracture pattern, surgical approach, quality of fixation, patient comorbidities, and surgeon preference. The general principles involve protection of the repair, gradual increase in weight-bearing, and restoration of range of motion and strength.
General Principles
- Pain Management: Multimodal approach including opioids, NSAIDs, acetaminophen, and regional nerve blocks.
- DVT Prophylaxis: Continued mechanical and/or chemical prophylaxis.
- Wound Care: Routine wound inspection and dressing changes.
- Prophylaxis for HO: As discussed, continuation of Indomethacin or single-dose radiation.
Phase 1: Protective Phase (Weeks 0-6)
Goal: Protect fixation, minimize pain and swelling, initiate early, safe motion, prevent stiffness.
-
Weight-Bearing (WB):
- Non-Weight-Bearing (NWB) or Touch-Down Weight-Bearing (TDWB): For the operated extremity. This is typically maintained for 6-8 weeks to allow for initial fracture healing and integration of fixation.
- Crutches or a walker are used.
-
Range of Motion (ROM):
- Passive Range of Motion (PROM): Gentle, pain-free PROM within protected arcs. Avoid extreme flexion, adduction, and internal rotation for posterior approaches (risk of dislocation) and extreme extension/external rotation for anterior approaches.
- Continuous Passive Motion (CPM) machine may be used for 2-4 hours/day to encourage articular cartilage health and prevent stiffness, though evidence for its routine benefit is mixed.
- Active-Assisted Range of Motion (AAROM): Progress as tolerated.
-
Strengthening:
- Isometric Exercises: Quadriceps sets, gluteal sets (e.g., glute squeezes) to maintain muscle tone without stressing the fracture site.
- Upper Extremity and Core Strengthening: Essential for ambulation with crutches/walker.
-
Transfers & Mobility:
- Instruction in safe bed mobility, transfers, and use of assistive devices (walker/crutches).
- Education: Patient education on precautions, signs of complications, and importance of adherence to restrictions.
Phase 2: Intermediate Phase (Weeks 6-12)
Goal: Gradual increase in weight-bearing, restore functional ROM, initiate strengthening.
-
Weight-Bearing (WB):
- Partial Weight-Bearing (PWB): Gradually progress from TDWB to 25-50% PWB, often guided by radiographic evidence of healing. Use bathroom scale for biofeedback.
- Progression to full weight-bearing (FWB) over the next 4-6 weeks as tolerated and with radiographic confirmation of healing.
-
Range of Motion (ROM):
- Progress to full AROM as tolerated, respecting pain limits.
- Gentle stretching to regain flexibility.
-
Strengthening:
- Progressive Resistance Exercises: Hip abduction, adduction, flexion, extension, knee flexion/extension (e.g., resistance bands, light weights).
- Closed kinetic chain exercises as tolerated (e.g., mini-squats with support).
- Proprioceptive exercises (e.g., single-leg stance with support).
- Gait Training: Focus on normal gait mechanics with assistive devices, progressing to independent ambulation.
Phase 3: Advanced Strengthening & Functional Return (Weeks 12+)
Goal: Maximize strength, endurance, and proprioception; prepare for return to full activity.
- Weight-Bearing (WB): Full weight-bearing without assistive devices.
-
Strengthening:
- Continue progressive resistance exercises.
- Functional exercises: lunges, step-ups, balance activities.
- Sport-specific training for athletes.
-
Activity Progression:
- Gradual return to recreational activities, low-impact sports.
- High-impact activities and contact sports may be restricted for up to 6-12 months, depending on fracture severity, healing, and the patient's goals.
- Monitoring: Continued monitoring for pain, ROM limitations, signs of HO, or other complications. Radiographic follow-up to assess healing and detect late complications like PTOA.
Special Considerations
- Older Patients: May require a slower progression of weight-bearing and greater emphasis on balance and fall prevention due to bone quality and comorbidities.
- Associated Injuries: Rehabilitation must be coordinated with the management of other orthopaedic or systemic injuries.
- Surgeon Communication: Close collaboration between the surgeon, physical therapist, and patient is essential for a safe and effective rehabilitation program. Any deviation from the protocol due to pain, instability, or delayed healing requires direct communication and potential modification of the plan.
Summary of Key Literature / Guidelines
The management of acetabular fractures has evolved significantly since the pioneering work of Judet and Letournel in the 1960s, which established the anatomical basis and classification system that remains the standard today. Modern literature emphasizes the critical role of anatomical reduction, stable fixation, and precise surgical technique to optimize long-term outcomes.
-
Judet and Letournel Classification: This system, based on specific radiographic lines (iliopectineal and ilioischial), categorizes fractures into five elementary and five associated patterns. Its enduring relevance is underscored by its continued use in guiding surgical approach selection and predicting outcomes. While the original description relied on plain radiographs, modern interpretation heavily utilizes 3D CT reconstructions.
-
Importance of Anatomical Reduction: Numerous studies have consistently demonstrated a strong correlation between residual articular incongruity and the development of post-traumatic osteoarthritis (PTOA). Matta et al. (1986, 1996) showed that excellent or good results were achieved in over 90% of cases with an anatomical reduction (0-1 mm step-off), whereas results plummeted to 20% with poor reductions (>3 mm). This finding underscores the imperative for meticulous surgical technique aimed at achieving near-perfect joint reconstruction.
-
Timing of Surgery: The optimal window for definitive fixation is generally considered to be 3 to 10 days post-injury. Early stabilization (within 72 hours) for patients with high-energy trauma and associated systemic injuries can decrease complications related to prolonged immobility but may be challenging in hemodynamically unstable patients or those with significant soft tissue swelling. Conversely, delaying surgery beyond 3 weeks significantly increases the technical difficulty due to early fibrous union and leads to higher complication rates and poorer outcomes. Irreducible hip dislocation remains an orthopaedic emergency requiring immediate reduction to minimize the risk of femoral head avascular necrosis (AVN).
-
Surgical Approaches and Outcomes:
- Kocher-Langenbeck (K-L): Remains the workhorse for posterior column and wall fractures. Studies have shown good to excellent outcomes in a high percentage of cases when anatomical reduction is achieved. Nerve injury (sciatic) is a known risk.
- Ilioinguinal: Effective for anterior column, anterior wall, and specific both-column fractures. It provides excellent visualization of the anterior pelvic brim and quadrilateral surface. Complications include lateral femoral cutaneous nerve injury and potential for substantial bleeding if the corona mortis is not managed.
- Modified Stoppa (Pararectus) Approach: A relatively newer approach, gaining traction due to its direct access to the quadrilateral surface and anterior column while potentially reducing morbidity (e.g., lower risk of LFCN injury, less disruption of the inguinal canal) compared to the ilioinguinal approach. Comparative studies suggest similar efficacy with potentially fewer complications in experienced hands.
- Extended Iliofemoral: Reserved for complex associated fractures due to its extensive exposure but higher morbidity profile (e.g., greater blood loss, higher rates of HO, increased risk of nerve injury).
-
Complication Management:
- Heterotopic Ossification (HO): Prophylactic regimens (NSAIDs like indomethacin or single-dose radiation) are strongly supported by literature, especially for high-risk patients, to reduce the incidence and severity of HO.
- Post-Traumatic Osteoarthritis (PTOA): Despite anatomical reduction, a significant proportion of patients may still develop PTOA due to initial articular cartilage damage. Salvage total hip arthroplasty (THA) is the most common solution, though it is technically more demanding in the post-traumatic setting with higher rates of complications compared to primary THA.
-
Advances in Technology and Techniques:
- 3D Printing and Pre-operative Planning: The use of 3D-printed anatomical models for pre-operative plate contouring and simulation of reduction maneuvers has been shown to decrease operative time, blood loss, and improve accuracy of reduction, particularly in complex fractures.
- Minimally Invasive/Percutaneous Techniques: While less commonly applied to highly displaced acetabular fractures, there is ongoing research into percutaneous screw fixation for specific fracture patterns or augmentation in elderly patients.
- Robotics and Navigation: Emerging technologies like robotics and computer-assisted navigation are being explored to improve accuracy of screw placement and reduction, though their routine application in acetabular fracture surgery is still in nascent stages.
-
Evidence-Based Guidelines: Current guidelines emphasize a multidisciplinary approach, patient optimization, meticulous surgical technique, and structured rehabilitation. The evidence supports surgical intervention for displaced articular fractures to minimize PTOA, with outcomes directly correlated to the quality of reduction. Functional outcomes are often assessed using scores like the modified Merle D'Aubigné and Postel score and the Harris Hip Score.
In conclusion, the successful management of acetabulum fractures remains a demanding aspect of orthopaedic trauma surgery. A thorough diagnostic evaluation, anchored by high-resolution CT, precisely guides a well-executed surgical plan. Adherence to established principles of anatomical reduction, stable internal fixation, and comprehensive post-operative rehabilitation, informed by decades of clinical experience and evolving literature, offers the best chance for optimal long-term functional recovery.
You Might Also Like