Acetabular Fractures: Epidemiology, Surgical Anatomy, Biomechanics, & Treatment Principles
Key Takeaway
Acetabular fractures are complex hip injuries, typically from high-energy trauma. Understanding their epidemiology, detailed surgical anatomy (Judet & Letournel columns, neurovascular structures), and biomechanics is crucial. This expertise guides precise treatment, restoring hip congruity to prevent post-traumatic osteoarthritis and ensure long-term function.
Introduction & Epidemiology
Acetabular fractures represent a significant challenge in orthopedic trauma, often resulting from high-energy mechanisms such as motor vehicle collisions, falls from height, or industrial accidents. These injuries are complex, frequently associated with life-threatening systemic trauma, and demand meticulous attention to both acute resuscitation and definitive orthopedic management. The primary goal of treatment is to restore the anatomical congruity of the hip joint, thereby minimizing the risk of post-traumatic osteoarthritis (PTOA), avascular necrosis (AVN) of the femoral head, and chronic pain.
The epidemiology of acetabular fractures shows a bimodal distribution, affecting younger patients involved in high-energy trauma and, increasingly, elderly individuals with osteoporotic bone undergoing low-energy falls. While the underlying bone quality differs significantly, the principles of anatomical reduction and stable fixation remain paramount, though surgical strategies may be modified for geriatric patients. The incidence is approximately 3-6 per 100,000 population, with male predominance in younger cohorts. Early recognition and accurate classification, particularly using the Judet and Letournel system, are critical for guiding surgical planning and predicting outcomes. Associated injuries are common and can include head trauma, chest and abdominal injuries, pelvic ring fractures, and extremity fractures, necessitating a comprehensive trauma evaluation.
Surgical Anatomy & Biomechanics
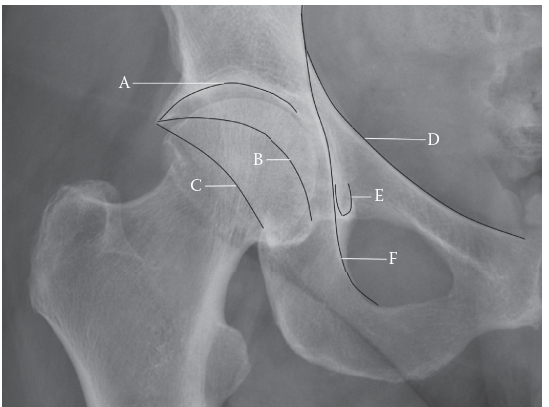
A thorough understanding of acetabular anatomy and its biomechanical function is fundamental for effective treatment of these fractures. The acetabulum is a hemispherical socket on the lateral aspect of the innominate bone, comprising contributions from the ilium (superior), ischium (posterior-inferior), and pubis (anterior-inferior). These three bones fuse at the triradiate cartilage during skeletal maturation.
Key Anatomical Structures
-
Acetabular Columns (Judet and Letournel concept):
- Anterior Column: Extends from the anterior superior iliac spine (ASIS) through the iliopectineal line, crossing the anterior acetabulum to the superior pubic ramus. It includes the ASIS, anterior inferior iliac spine (AIIS), and the anterior half of the acetabular roof.
- Posterior Column: Extends from the ischial tuberosity through the ischial spine and the posterior acetabulum to the posterior iliac wing. It includes the posterior half of the acetabular roof.
- Biomechanical Significance: The anterior and posterior columns function as major load-bearing buttresses, transmitting axial forces from the femoral head to the axial skeleton. Disruption of these columns significantly compromises hip stability and articular congruence.
-
Walls:
- Anterior Wall: The anterosuperior portion of the acetabulum, lateral to the iliopectineal eminence.
- Posterior Wall: The posterosuperior portion, crucial for hip stability, especially during flexion and internal rotation. Its integrity is vital.
- Quadrilateral Surface: The medial wall of the acetabulum, thin and often comminuted in complex fracture patterns. It forms the lateral boundary of the true pelvis and is bounded by the iliopectineal line (anterior) and ilioischial line (posterior).
- Acetabular Fossa: The central, non-articular portion of the acetabulum, occupied by the ligamentum teres and fat pad.
- Acetabular Notch: The inferior defect in the acetabular rim, bridged by the transverse acetabular ligament.
-
Neurovascular Structures:
- Sciatic Nerve: Exits the pelvis through the greater sciatic foramen, immediately posterior to the posterior column. Highly vulnerable during posterior approaches and with posterior dislocations/fractures.
- Femoral Neurovascular Bundle: Located anteriorly, medial to the iliopectineal eminence. Contains the femoral artery, vein, and nerve, at risk during anterior approaches.
- Superior Gluteal Artery and Nerve: Emerge above the piriformis, supplying the gluteus medius and minimus. Vulnerable during extended iliofemoral and Kocher-Langenbeck approaches, particularly near the greater sciatic notch.
- Obturator Nerve and Vessels: Travel along the inner aspect of the pelvic ring, deep to the quadrilateral plate.
- Corona Mortis (Aberrant Obturator Artery): An anatomical variant, a vascular connection between the obturator and external iliac/inferior epigastric arteries, often crossing the superior pubic ramus. Laceration can lead to significant hemorrhage during Stoppa or ilioinguinal approaches.
- Soft Tissue Attachments: Gluteal muscles (maximus, medius, minimus), iliopsoas, rectus femoris, adductors, and hip capsule are critical for stability and can be involved in fracture displacement.
Biomechanics
The hip joint is a diarthrodial ball-and-socket joint, designed for significant load transmission and mobility. The acetabulum, with its articular cartilage (lunate surface), articulates with the femoral head. Normal hip joint mechanics depend on:
1.
Concentric Reduction:
A perfectly spherical femoral head articulating concentrically within the acetabulum.
2.
Smooth Articular Surface:
Intact hyaline cartilage for low-friction movement.
3.
Intact Labrum:
Enhances stability and deepens the socket.
4.
Stable Bony Architecture:
Intact anterior and posterior columns and walls to resist physiological loads.
Fractures disrupting these elements lead to abnormal stress distribution, joint incongruity, and ultimately, accelerated degeneration.

Indications & Contraindications
The decision for operative versus non-operative management of acetabular fractures is complex, balancing patient factors, fracture characteristics, and available resources. The primary goal of surgery is anatomical reduction and stable internal fixation to restore joint congruity and allow early motion, thus preventing long-term complications.
Indications for Operative Management
- Displacement: Intra-articular displacement of ≥ 2 mm (some argue for 1 mm in younger patients in the weight-bearing dome).
- Instability: Demonstrated hip instability, often due to significant posterior wall or both column fractures.
- Incongruity: Loss of concentric reduction of the femoral head within the acetabulum.
- Associated Hip Dislocation: Unreducible dislocation, or a stable reduction that becomes unstable, or associated with intra-articular fragments.
- Intra-articular Fragments: Loose bodies that may lead to chondral damage or block reduction.
- Femoral Head Impaction/Chondral Injury: Direct trauma to the femoral head or significant chondral damage on CT.
-
Specific Fracture Patterns:
- Posterior wall fractures: If > 40-50% of the articular surface is involved, or if the fracture results in hip instability.
- Transverse fractures: Displaced or unstable.
- T-type fractures: Displaced.
- Anterior column/wall fractures: Displaced and affecting the weight-bearing dome.
- Both column fractures: Always considered operative due to inherent instability and loss of articular support.
Contraindications for Operative Management
-
Absolute Contraindications:
- Medically Unstable Patient: Uncontrolled hemorrhage, severe sepsis, active infection, or other life-threatening conditions precluding surgery.
- Severe Comorbidities: Morbid obesity, severe cardiac, pulmonary, or renal disease with prohibitive anesthetic risk.
- Absolute Contraindication to Anesthesia: Rare, but can occur.
-
Relative Contraindications:
- Non-displaced or Minimally Displaced Fractures (< 2 mm): If concentric reduction is maintained and hip stability is preserved.
- Non-ambulatory Patient: Pre-existing neurological deficits or severe comorbidities that prevent ambulation, rendering the benefits of surgery marginal.
- Advanced Age with Osteoporosis: While not an absolute contraindication, extremely poor bone quality may compromise fixation, and primary total hip arthroplasty (THA) or non-operative management may be considered in selected cases.
- Delay to Surgery (>3 Weeks): While not an absolute contraindication, significant callus formation and early consolidation make reduction more challenging and increase the risk of iatrogenic injury. Each week of delay reduces the likelihood of achieving anatomical reduction.
- Severe Local Soft Tissue Injury: Open fractures with significant contamination, severe degloving, or extensive crush injuries that increase the risk of infection and wound complications.
Operative vs. Non-Operative Indications
| Indication | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Displacement | ≥ 2 mm articular displacement (some advocate for 1 mm in specific areas/patients) | < 2 mm articular displacement, concentric reduction maintained |
| Hip Stability | Unstable hip joint (e.g., significant posterior wall fracture with subluxation, both column fractures) | Stable hip joint with no subluxation |
| Associated Dislocation | Unreducible hip dislocation, persistently unstable reduction, intra-articular fragments following reduction | Stable reduction of hip dislocation, no intra-articular fragments |
| Femoral Head Involvement | Impaction injury, chondral damage, associated AVN risk factors | No significant femoral head injury |
| Intra-articular Fragments | Presence of loose bodies within the joint | Absence of intra-articular fragments |
| Patient Status | Medically stable, good surgical candidate, absence of severe local soft tissue damage | Medically unstable, severe comorbidities, non-ambulatory, severe local soft tissue injury contraindicating surgery |
| Specific Fracture Patterns | Displaced posterior wall (>40-50%), displaced transverse, displaced T-type, displaced anterior column/wall affecting dome, all displaced both column fractures | Non-displaced or minimally displaced elementary fractures (e.g., small anterior wall, stable posterior column), dome-impaction fractures without significant articular displacement |
| Time Since Injury | Generally within 7-14 days (up to 3 weeks in selected cases) | May be indicated for delayed presentations where callus formation makes reduction prohibitive, or for medically unfit patients |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful acetabular fracture surgery. This involves a thorough assessment of the patient, detailed imaging analysis, and careful strategizing for surgical approach and implant selection.
Pre-Operative Planning
-
Patient Assessment:
- ATLS Protocol: Ensure the patient is hemodynamically stable. Acetabular fractures are often part of polytrauma.
- Neurovascular Exam: Document baseline neurological status (especially sciatic and femoral nerves) and vascular integrity (femoral pulses).
- Associated Injuries: Screen for other orthopedic injuries (e.g., ipsilateral knee dislocation, pelvic ring fractures) and visceral injuries.
- Comorbidities: Optimize medical conditions, manage DVT prophylaxis, and consider heterotopic ossification (HO) prophylaxis (NSAIDs or radiation therapy).
- Timing: Optimal timing is generally within 7-14 days. Delay beyond 3 weeks significantly increases surgical difficulty due to early callus formation and fibrous union.
-
Imaging Analysis:
-
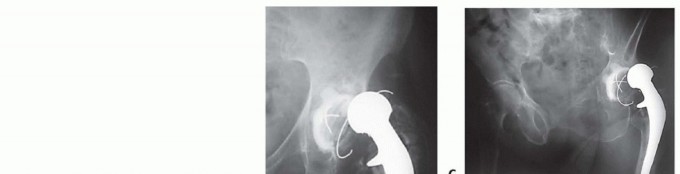
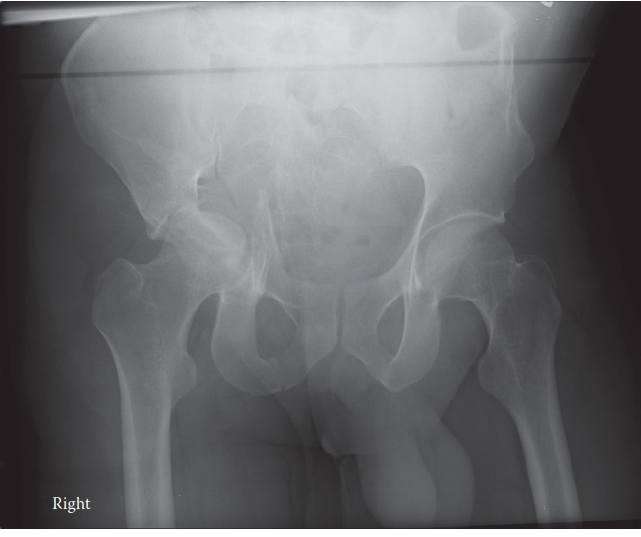
Plain Radiographs:
- AP Pelvis: Provides an overview of the pelvic ring and hip joint.
- Iliac Oblique (Judet View): Visualizes the posterior column and anterior wall.
- Obturator Oblique (Judet View): Visualizes the anterior column and posterior wall.
- Goal: These views help classify the fracture according to Judet and Letournel.
-
Computed Tomography (CT) Scan:
Essential
for definitive diagnosis and surgical planning.
- Thin-slice CT with 2D and 3D Reconstructions: Provides detailed visualization of fracture lines, comminution, articular step-off, intra-articular fragments, quadrilateral surface involvement, and femoral head integrity. It is invaluable for understanding fracture morphology and choosing the appropriate surgical approach.
- Special attention: Assess for impaction of the femoral head, hip capsule integrity, and size/location of intra-articular fragments.
- MRI: Rarely indicated acutely unless there is suspicion of significant labral tear, chondral injury not evident on CT, or soft tissue interposition.
- CT Angiography: May be considered if major vascular injury is suspected, particularly in severe displacement.
-
Plain Radiographs:
-
Surgical Strategy Development:
- Fracture Mapping: Use CT 3D reconstructions to identify all fracture fragments, their displacement, and their relationship to stable anatomical landmarks. Mentally rehearse the reduction sequence.
-
Approach Selection:
Based on the fracture pattern (Judet & Letournel classification) and fragment location.
- Posterior Column/Wall: Kocher-Langenbeck approach.
- Anterior Column/Wall, Quadrilateral Surface: Ilioinguinal or Stoppa approach.
- Both Column Fractures: Often require an anterior approach (Ilioinguinal, Stoppa) or a combined approach (e.g., Kocher-Langenbeck + Ilioinguinal staged, or extended iliofemoral).
- Implant Selection: Determine plate type (reconstruction plates, buttress plates, specific column plates), screw length and trajectory, and reduction clamps needed.
- Team Preparation: Ensure the operating room staff, anesthesia team, and scrub techs are familiar with the specific approach and instrumentation.
Patient Positioning
Correct patient positioning is critical for adequate exposure, ease of reduction, and fluoroscopic visualization.
-
Lateral Decubitus Position (for Kocher-Langenbeck Approach):
- The patient is placed in a true lateral decubitus position on a standard operating table or a radiolucent table.
- The operative side is up.
- Beanbag positioner and hip/chest rolls are used to stabilize the patient.
- The operative leg is flexed at the hip and knee, often supported by a sterile bolster or leg holder, allowing access to the posterior aspect.
- The non-operative leg is usually straight.
- Fluoroscopy: Ensure adequate AP, iliac oblique, and obturator oblique views are achievable with the C-arm prior to draping. This often requires tilting the table or rotating the C-arm.
-
Supine Position (for Ilioinguinal or Stoppa Approach):
- The patient is placed supine on a radiolucent operating table.
- A large bump is often placed under the ipsilateral hip to elevate it, allowing better access to the medial aspect of the pelvis.
- Both legs are usually positioned straight.
- Fracture Table vs. Radiolucent Table: A fracture table may be used for preliminary traction to disengage fragments, but often a standard radiolucent table is preferred to allow better manipulation of the limb and access to the groin. The image intensifier needs to be positioned for optimal AP, iliac oblique, and obturator oblique views.
- Pad Positioning: Ensure adequate padding to prevent pressure neuropathies (e.g., ulnar nerve at the elbow, peroneal nerve at the fibular head).
- Self-correction : For Stoppa approach, particularly, a beanbag can be used for slight external rotation of the hip.
-
Combined Approaches:
- If sequential approaches are required (e.g., anterior then posterior), the patient may be re-positioned or initially placed on a specialized frame or fracture table that allows for easier turning. This adds complexity and operative time.
- Extended Iliofemoral: Typically supine with a rolled blanket under the hip, or slightly obliqued.
The final positioning must ensure surgical access, unimpeded fluoroscopic imaging in all necessary projections, and patient safety throughout the procedure.
Detailed Surgical Approach / Technique
Surgical reduction and internal fixation of acetabular fractures demand precision, experience, and adherence to established principles. The choice of surgical approach is dictated by the fracture pattern, fragment displacement, and the surgeon's familiarity.
General Principles of Reduction and Fixation
- Timing: Optimal timing is typically 5-10 days post-injury, allowing for soft tissue swelling to subside while avoiding significant callus formation. In cases of associated hip dislocation or severe instability, earlier intervention may be warranted.
- Goals: Anatomical reduction of the articular surface (ideally <1-2 mm step-off/gap), stable internal fixation, and restoration of mechanical axis.
- Blood Loss Management: Acetabular surgery can be associated with significant blood loss. Pre-operative blood ordering, cell-saver use, and meticulous hemostasis are crucial.
- Fluoroscopic Control: Intra-operative fluoroscopy with AP, iliac oblique, and obturator oblique views is essential to verify reduction and implant position.
- Soft Tissue Handling: Atraumatic dissection, careful retraction, and preservation of periosteal blood supply are critical to minimize complications.
Surgical Approaches
1. Kocher-Langenbeck Approach (Posterior Approach)
- Indications: Fractures of the posterior column, posterior wall, T-type (primarily posterior limb), and transverse fractures with posterior displacement.
- Patient Position: Lateral decubitus, operative hip up.
- Incision: Curved skin incision from the posterior aspect of the greater trochanter, extending proximally along the iliac crest (or slightly medial to it) and distally along the shaft of the femur.
-
Dissection:
- Superficial Fascia: Incision through the fascia lata.
- Gluteus Maximus: The gluteus maximus is split longitudinally along its fibers, typically between its middle and distal thirds. Care must be taken to protect the superior and inferior gluteal neurovascular bundles.
- Short External Rotators: The piriformis, obturator internus with gemelli, and quadratus femoris are identified. The piriformis is often detached from its insertion on the greater trochanter. The obturator internus and gemelli can be detached as a confluent block, exposing the posterior capsule.
- Sciatic Nerve: CRITICAL: The sciatic nerve lies deep to the piriformis and obturator internus, medial to the lesser sciatic notch. It must be carefully identified, protected, and retracted (usually medially). Traction on the limb during surgery should be monitored to prevent iatrogenic nerve stretch.
- Capsule: The hip capsule can be incised (capsulotomy) to visualize the articular surface and remove intra-articular fragments, especially in posterior wall fractures with marginal impaction.
-
Reduction & Fixation:
- Posterior Wall: Fragments are typically reduced using pointed reduction clamps, bone hooks, or joysticks. Marginal impaction is elevated and bone grafted. Fixation involves buttress plates (e.g., 3.5 mm reconstruction plate) contoured to the posterior rim, secured with bicortical screws.
- Posterior Column: Reduction often involves clamps applied to the posterior aspect of the column. Fixation typically requires a longer reconstruction plate spanning from the posterior ilium to the ischium.
- Fluoroscopy: AP, iliac oblique, and obturator oblique views are used to confirm reduction and implant placement. The obturator oblique view is especially useful for checking posterior column length and rotation.
-
Closure:
Reattachment of short external rotators and piriformis (if detached), closure of gluteus maximus split, fascia lata, and skin.
2. Ilioinguinal Approach (Anterior Approach)
- Indications: Fractures of the anterior column, anterior wall, both column fractures, and some transverse fractures with anterior displacement. Provides excellent access to the quadrilateral surface and anterior pelvic brim.
- Patient Position: Supine on a radiolucent table.
- Incision: Bikini-line incision (inguinal crease) from the ASIS to the pubic symphysis.
-
Dissection:
The approach utilizes "windows" to access different anatomical regions.
- Superficial Dissection: Incision through skin and subcutaneous fat. The external oblique aponeurosis is identified.
- Identify Spermatic Cord/Round Ligament: This structure runs from deep to superficial, medial to the ASIS. It is mobilized inferiorly.
-
Lateral Window:
- Between the iliopsoas muscle/femoral nerve (medially) and the tensor fascia lata/sartorius (laterally).
- Accesses: Iliac wing, sacroiliac joint, lateral aspect of the anterior column, AIIS.
- Retraction: Iliopsoas/femoral nerve medially, sartorius/TFL laterally.
-
Middle Window:
- Between the iliopsoas muscle/femoral nerve (laterally) and the external iliac artery/vein (medially).
- Accesses: Anterior column, pelvic brim, lateral aspect of the quadrilateral surface.
- Retraction: Iliopsoas/femoral nerve laterally, femoral vessels medially. CRITICAL: Protection of the femoral neurovascular bundle is paramount.
-
Medial Window:
- Between the external iliac artery/vein (laterally) and the rectus abdominis/pubic symphysis (medially).
- Accesses: Superior pubic ramus, pubic symphysis, medial aspect of the quadrilateral surface.
- Retraction: Femoral vessels laterally. CRITICAL: Identify and ligate the "Corona Mortis" (anastomosis between obturator and external iliac/inferior epigastric vessels) if present, to prevent significant hemorrhage.
-
Reduction & Fixation:
- Anterior Column: Fragments are reduced using pointed reduction clamps, reduction forceps applied through the windows. Fixation usually involves a reconstruction plate contoured along the pelvic brim.
- Quadrilateral Surface: Reduction of medial displacement is often challenging. Direct visualization through the medial window allows placement of a buttress plate (e.g., specific quadrilateral surface plate) to push the fragment laterally, or screws from the iliac crest directed medially to buttress the plate.
- Both Columns: Requires reduction of the entire acetabular articular segment. Often involves a posterior-to-anterior reduction sequence. Fixation with plates on the anterior column (along the pelvic brim) and screws for the posterior column, or specialized plates.
- Fluoroscopy: AP and obturator oblique views are critical for anterior column reduction, while the iliac oblique helps for superior extension of fracture.
3. Stoppa Approach (Modified Ilioinguinal / Pararectus Approach)
- Indications: Similar to ilioinguinal, but particularly useful for fractures involving the quadrilateral surface, anterior column, anterior aspects of both columns, and dome fractures with medial impaction. It offers more direct access to the quadrilateral surface without extensive lateral dissection.
- Patient Position: Supine on a radiolucent table.
- Incision: Vertical or oblique skin incision, typically paramedian, often extending from the umbilicus to the pubic symphysis, or less commonly, a transverse incision in the suprapubic region.
-
Dissection:
- Rectus Sheath: The anterior rectus sheath is incised, and the rectus abdominis muscle is mobilized laterally or medially, exposing the posterior rectus sheath and transversalis fascia.
- Preperitoneal Space: Dissection proceeds in the preperitoneal space, sweeping the peritoneum and its contents (including bladder) medially and superiorly.
- Access: This approach provides direct access to the inner table of the ilium, pelvic brim, quadrilateral surface, superior pubic ramus, and even the sacroiliac joint.
- Neurovascular Protection: The femoral neurovascular bundle is typically lateral to the operative field, reducing direct risk. The obturator nerve and vessels are visualized directly on the quadrilateral surface.
-
Reduction & Fixation:
Allows for direct application of buttress plates to the quadrilateral surface to restore the medial wall, preventing secondary displacement and ensuring femoral head containment. Reconstruction plates along the pelvic brim are used for anterior column fixation. Percutaneous screws can also be inserted from the iliac crest for quadrilateral surface buttressing.

4. Extended Iliofemoral Approach
- Indications: Complex both column fractures, T-type fractures, or associated iliac wing fractures that cannot be adequately addressed by more limited approaches. It offers wide exposure of the outer aspect of the ilium, anterior and posterior columns.
- Patient Position: Supine or lateral decubitus.
- Morbidity: High morbidity due to extensive muscle detachment (gluteus medius/minimus, vastus lateralis origin) and devascularization of the iliac crest, leading to increased blood loss, HO, and abductor weakness. Rarely used today due to advent of combined approaches and improved techniques for limited approaches.
5. Combined Approaches (Staged or Simultaneous)
- Indications: Complex fracture patterns (e.g., some both column fractures, T-type) that require access to both anterior and posterior aspects of the acetabulum.
- Technique: May involve a staged approach (e.g., anterior approach on day 1, posterior approach on day 3-5 after patient recovery) or simultaneous approach with two surgical teams if patient tolerance allows.
- Benefit: Allows comprehensive visualization and reduction of complex fracture patterns.
- Drawbacks: Increased operative time, blood loss, and risk of complications.
The choice of approach is individualized, demanding a surgeon with extensive experience in acetabular fracture management. The goal is always anatomical reduction with minimal soft tissue disruption and stable internal fixation.
Complications & Management
Acetabular fracture surgery is associated with a wide array of potential complications, both intra-operative and post-operative, reflecting the complexity of the anatomy, the high energy of injury, and the invasiveness of the procedures. Proactive recognition and management are crucial for optimizing patient outcomes.
Common Complications and Management Strategies
| Complication | Incidence | Description & Management Strategy |
|---|---|---|
| Intra-operative Nerve Injury | 5-15% |
Sciatic Nerve:
Most common in posterior approaches (Kocher-Langenbeck). Presents as foot drop, sensory deficit in posterior leg/foot.
Management: Meticulous retraction, short external rotators as a buffer, avoid excessive traction, pre-op assessment. If recognized intra-op, release traction, re-inspect nerve. If persistent deficit post-op, consider EMG/NCS, physiotherapy, AFO. Femoral Nerve: Common in anterior approaches (Ilioinguinal). Presents as quadriceps weakness, sensory deficit in anterior thigh. Management: Careful neurovascular bundle retraction, protect with Penrose drain. |
| Vascular Injury / Hemorrhage | 2-5% |
Damage to superior gluteal, external iliac, obturator vessels, or Corona Mortis. Can lead to significant blood loss.
Management: Pre-op planning (CT angio if high risk), meticulous dissection, prompt ligation/repair of bleeding vessels. Cell-saver use, blood product transfusion. Pre-op embolization may be considered for large retroperitoneal hematoma. |
| Malreduction / Non-anatomic Fixation | 5-20% (depending on study) |
Inadequate restoration of articular congruity or column alignment. Associated with poor long-term outcomes (PTOA).
Management: Meticulous pre-op planning, intra-op fluoroscopic control (AP/obliques), direct visualization, appropriate reduction clamps/techniques. Revision surgery if severe displacement or early signs of joint degeneration. |
| Infection | 1-5% |
Superficial or deep surgical site infection (SSI). Higher risk with extensive approaches, prolonged surgery, open fractures, or reoperations.
Management: Strict aseptic technique, prophylactic antibiotics, meticulous wound care. Debridement, irrigation, antibiotic beads/spacers, and potentially hardware removal for deep infections. |
| Heterotopic Ossification (HO) | 10-50% (clinical), higher radiographically |
Ectopic bone formation around the hip joint, leading to pain and decreased range of motion. More common with extended approaches, head injury, male sex, concomitant elbow injury.
Management: Prophylactic NSAIDs (e.g., Indomethacin) for 3-6 weeks post-op, or single-dose post-op radiation therapy (700-800 cGy). Excision for severe, mature HO affecting function. |
| Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) | DVT 5-15% (clinical), PE <1% |
Life-threatening thromboembolic events. Risk factors include trauma, immobility, surgery.
Management: Pharmacological prophylaxis (LMWH, Factor Xa inhibitors) initiated pre- or post-op, early mobilization, mechanical prophylaxis (SCDs). |
| Post-Traumatic Osteoarthritis (PTOA) | 20-80% (long-term) |
Progressive degeneration of the articular cartilage, leading to pain, stiffness, and functional limitation. Directly correlated with quality of reduction.
Management: Optimal anatomical reduction and stable fixation. Conservative management (NSAIDs, PT, activity modification). If severe and debilitating, conversion to total hip arthroplasty (THA). Early signs of PTOA may necessitate earlier intervention. |
| Avascular Necrosis (AVN) of Femoral Head | 2-10% (fracture pattern dependent) |
Compromise of blood supply to the femoral head, leading to collapse. Risk factors include associated hip dislocation (especially irreducible or delayed reduction), severe comminution.
Management: Urgent reduction of hip dislocations. No proven surgical salvage for established AVN short of THA. |
| Nonunion / Malunion | Rare (<5%) |
Failure of fracture fragments to unite, or healing in a suboptimal position.
Management: Revision surgery with bone grafting, improved fixation, or corrective osteotomy for malunion. |
| Hardware Related Complications | 5-10% |
Prominent hardware requiring removal, screw pull-out, plate breakage.
Management: Symptomatic hardware removal after fracture healing. Revision fixation for hardware failure. |
| Wound Dehiscence / Necrosis | 2-5% |
Occurs due to excessive tension, poor soft tissue handling, or infection. Higher risk with extensive approaches or compromised soft tissue envelopes.
Management: Local wound care, debridement, negative pressure wound therapy. Flap coverage may be required for large defects. |
Salvage Strategies
- Revision Surgery: For severe malreduction, nonunion, or failed hardware, revision surgery may involve re-reduction and re-fixation, potentially with bone grafting.
- Total Hip Arthroplasty (THA): The definitive salvage procedure for severe, symptomatic post-traumatic osteoarthritis. It can also be considered as a primary treatment in elderly, osteopenic patients with complex acetabular fractures that are difficult to fix and are likely to fail. This is a complex procedure in a deformed pelvis with scar tissue, often requiring specialized implants (e.g., cages, custom components) and significant experience.
- Arthrodesis: Rarely performed as a salvage option for young, active patients with severe PTOA who cannot tolerate THA, but generally offers poorer long-term quality of life.
- Resection Arthroplasty (Girdlestone): Reserved for intractable infection or severe, painful nonunion in non-ambulatory patients where other options are contraindicated.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as crucial as the surgery itself in determining the functional outcome after acetabular fracture fixation. Protocols aim to protect the fracture fixation, prevent complications, and restore hip function. Protocols are individualized based on fracture pattern, quality of fixation, patient comorbidities, and surgeon preference.
General Principles
- Protection of Fixation: The primary goal in the early phase is to protect the meticulously achieved anatomical reduction and stable internal fixation.
- Prevention of Complications: Prophylaxis against DVT, HO, and wound complications continues post-operatively.
- Restoration of Motion & Strength: Gradually progressing from passive to active range of motion, followed by strengthening exercises.
- Gradual Weight-Bearing: Typically initiated once radiographic evidence of healing is present and deemed safe.
Phased Rehabilitation Protocol (Example)
Phase 1: Immediate Post-Operative (Weeks 0-6)
-
Weight-Bearing:
- Non-Weight Bearing (NWB) on the operative extremity. Ambulation with crutches or a walker.
- Foot-flat weight-bearing or toe-touch weight-bearing (TTWB) may be allowed by some surgeons for stability, but NWB is generally safer.
-
Range of Motion (ROM):
- Continuous Passive Motion (CPM) Machine: May be used for 4-6 hours daily to promote cartilage health and prevent stiffness, though evidence for improved long-term outcomes is mixed.
- Active-Assisted ROM (AAROM) and Gentle Passive ROM (PROM): Within pain limits. Focus on flexion, abduction, adduction, and rotation. Avoid extremes of motion, especially positions that stress the fracture fragments (e.g., deep flexion, adduction, internal rotation for posterior fractures).
- Hip Flexion Restriction: Some surgeons restrict hip flexion to 60-90 degrees to protect fixation, especially for anterior column fractures.
-
Exercises:
- Ankle pumps, quadriceps sets, gluteal sets, heel slides (gentle).
- Upper extremity and core strengthening.
-
Precautions:
- DVT Prophylaxis: Continue pharmacological agents (LMWH or oral anticoagulants) for 4-6 weeks or until fully weight-bearing.
- HO Prophylaxis: Continue NSAIDs (e.g., Indomethacin) for 3-6 weeks.
- Hip Precautions: Based on the surgical approach. For posterior approaches, avoid hip flexion >90°, adduction past midline, and internal rotation. For anterior approaches, avoid excessive extension and external rotation.
- Wound care.
Phase 2: Early Healing & Progressive Motion (Weeks 6-12)
-
Weight-Bearing:
- Transition to Toe-Touch Weight Bearing (TTWB) or Partial Weight Bearing (PWB) with crutches/walker, gradually increasing as tolerated and guided by radiographic healing.
- Radiographs at 6 weeks assess initial callus formation.
-
Range of Motion:
- Progress to Active ROM (AROM) , increasing flexion, abduction, and rotation as tolerated.
- Continue gentle stretching.
-
Exercises:
- Isometric hip exercises (flexion, extension, abduction, adduction).
- Gentle resisted exercises (e.g., with theraband).
- Pool therapy (non-weight bearing exercises in water).
- Proprioceptive exercises.
Phase 3: Advanced Healing & Strengthening (Weeks 12-24)
-
Weight-Bearing:
- Progress to Full Weight Bearing (FWB) as tolerated, typically around 10-12 weeks, with gradual weaning from assistive devices based on radiographic union and strength.
- Radiographs at 12 weeks to confirm bridging callus and early union.
-
Range of Motion:
- Continue to regain full, pain-free ROM.
-
Exercises:
- Progressive resistive exercises for all hip muscle groups (quadriceps, hamstrings, gluteals, adductors).
- Closed-chain exercises (e.g., mini-squats, lunges).
- Balance and proprioception training.
- Low-impact cardio (e.g., stationary bike, elliptical).
- Gait training to normalize walking pattern.
Phase 4: Return to Activity (Weeks 24 onwards)
- Weight-Bearing: Full, unrestricted.
- Range of Motion: Should be near normal.
-
Exercises:
- Advanced strengthening, agility, and sport-specific training.
- Gradual return to recreational activities, avoiding high-impact sports initially.
- Long-Term Monitoring: Patients should be counseled on the risk of PTOA and AVN, requiring long-term follow-up and symptom monitoring.
Close communication between the surgeon and physical therapist is vital. Adjustments to the protocol are common based on individual patient progress and fracture healing.
Summary of Key Literature / Guidelines
The management of acetabular fractures has evolved significantly over the past half-century, largely guided by seminal work and advancements in imaging and surgical techniques.
Classic Contributions
- Judet and Letournel Classification (1964, 1980): Maurice Judet and Émile Letournel revolutionized the understanding and treatment of acetabular fractures with their detailed anatomical studies and radiographic classification system. Their work, published initially in French and later translated, categorized fractures into elementary (posterior wall, posterior column, anterior wall, anterior column, transverse) and associated (both column, T-type, posterior column with posterior wall, transverse with posterior wall, anterior with posterior hemi-transverse) patterns. This classification remains the universal language for describing these injuries and guides surgical approach selection. Their emphasis on anatomical reduction and early mobilization laid the groundwork for modern treatment principles.
- Biomechanics and Surgical Approaches: Their detailed descriptions of surgical approaches (Kocher-Langenbeck, Ilioinguinal, Extended Iliofemoral) and reduction maneuvers are still foundational. Subsequent modifications, such as the Stoppa approach, have refined access to specific regions, particularly the quadrilateral surface.
Modern Advancements and Current Debates
- Imaging: The advent of CT with 3D reconstructions has been a game-changer, allowing unprecedented pre-operative visualization of complex fracture patterns, articular involvement, and fragment displacement, significantly enhancing surgical planning and reducing operative surprises.
-
Surgical Techniques and Implants:
- Minimally Invasive Approaches: While direct open reduction remains the gold standard, there's growing interest in percutaneous screw fixation and limited open approaches, especially for certain simple patterns or in combination with direct techniques.
- Advanced Fixation: Development of specialized plating systems, pre-contoured plates, and internal fixators (e.g., for quadrilateral surface buttressing) has improved fixation stability.
- Intraoperative Navigation: While not routine, some centers explore the use of computer navigation systems to guide screw placement and verify reduction, particularly in complex cases.
- Timing of Surgery: The optimal window for definitive fixation is generally considered 5-10 days post-injury, balancing soft tissue swelling resolution with avoiding premature callus formation. However, "damage control orthopedics" principles guide management of polytrauma patients, sometimes necessitating staged procedures. Emergent reduction of associated hip dislocation (within 6 hours) is crucial to minimize AVN risk.
- Management in the Elderly: Acetabular fractures in osteoporotic elderly patients present unique challenges. While anatomical reduction and fixation are still desirable, bone quality can make fixation tenuous. Debates continue regarding the role of primary total hip arthroplasty (THA) in severely comminuted or multi-column fractures in this population, as it may offer earlier mobilization and potentially better functional outcomes in selected cases, despite being a more extensive procedure.
- Role of Arthroplasty for PTOA: For patients who develop severe post-traumatic osteoarthritis despite initial successful fixation, conversion to total hip arthroplasty is the most common salvage procedure. This can be technically challenging due to distorted anatomy, scar tissue, and retained hardware.
- Outcomes Data: Long-term follow-up studies consistently demonstrate a strong correlation between anatomical reduction (< 1-2 mm step-off/gap) and superior functional outcomes, reduced rates of PTOA, and less need for subsequent THA. Surgeon experience and high-volume centers are also consistently associated with better outcomes.
Current Guidelines and Recommendations
While no universally accepted, rigid guidelines exist, the consensus among academic orthopedic surgeons and trauma societies emphasizes:
*
Comprehensive initial assessment
(ATLS, neurovascular exam).
*
High-quality imaging
(AP, Judet views, thin-slice CT with 3D).
*
Accurate Judet and Letournel classification.
*
Timely anatomical reduction and stable internal fixation
for displaced fractures in appropriate candidates.
*
Individualized surgical approach selection.
*
Aggressive DVT and HO prophylaxis.
*
Structured, progressive post-operative rehabilitation.
*
Long-term follow-up
to monitor for PTOA, AVN, and other complications.
The management of acetabular fractures remains a demanding subspecialty, requiring highly skilled surgeons working within experienced multidisciplinary teams to achieve the best possible outcomes for these complex, high-energy injuries.
Clinical & Radiographic Imaging
You Might Also Like