Lateral Ulnar Collateral Ligament Reconstruction for Posterolateral Rotatory Instability
Key Takeaway
Lateral ulnar collateral ligament (LUCL) reconstruction is the gold-standard surgical intervention for chronic posterolateral rotatory instability (PLRI) of the elbow. This comprehensive guide details the modified Kocher approach, precise isometric tunnel placement at the lateral epicondyle and crista supinatoris, and graft tensioning techniques. Designed for orthopedic surgeons, it provides an evidence-based, step-by-step protocol to restore the lateral collateral ligament complex and ensure optimal postoperative joint stability and kinematics.
INTRODUCTION TO POSTEROLATERAL ROTATORY INSTABILITY (PLRI)
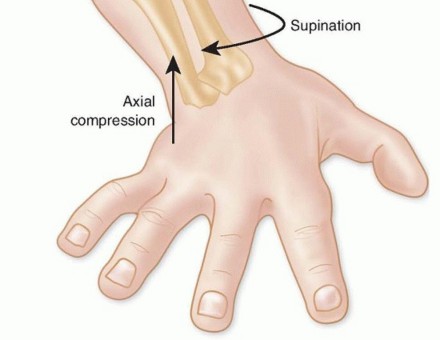
Posterolateral rotatory instability (PLRI) is the most common pattern of chronic elbow instability, typically resulting from a traumatic dislocation or subluxation event that disrupts the lateral collateral ligament (LCL) complex. First comprehensively described by O’Driscoll, Morrey, and Bell, PLRI is characterized by a three-dimensional displacement pattern: the ulna supinates and subluxates posterolaterally away from the trochlea, carrying the radius with it.
The primary pathoanatomic lesion in PLRI is the incompetence or avulsion of the lateral ulnar collateral ligament (LUCL). When conservative management fails and patients experience recurrent symptomatic instability—often described as clicking, locking, or a sensation of the elbow "giving way" during extension, supination, and axial loading—surgical intervention is indicated.
For PLRI that persists due to the disruption of the LUCL and the incompetence of the secondary lateral capsular structures, Nestor, O’Driscoll, and Morrey described a highly reproducible technique utilizing a modified Kocher lateral incision for the anatomic repair or reconstruction of the lateral ligamentous complex.
SURGICAL ANATOMY AND BIOMECHANICS
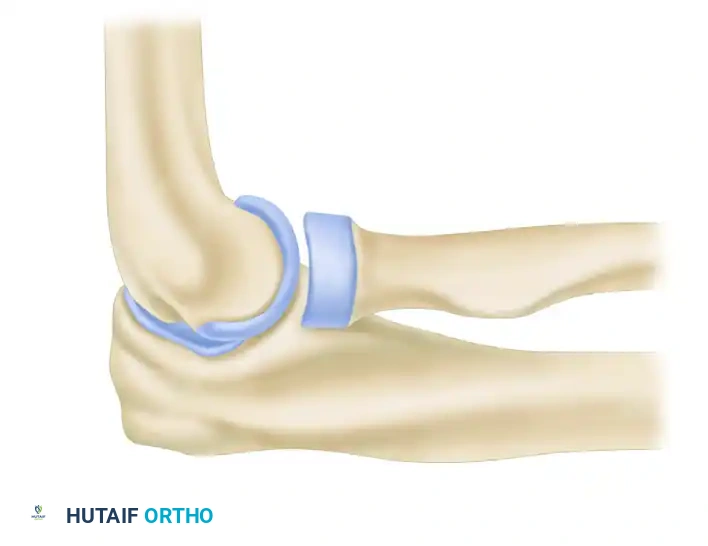
A profound understanding of the lateral ligamentous complex is mandatory for successful reconstruction. The LCL complex consists of four distinct components:
1. Radial Collateral Ligament (RCL): Originates from the lateral epicondyle and blends into the annular ligament.
2. Lateral Ulnar Collateral Ligament (LUCL): The primary restraint to varus and posterolateral rotatory stress. It originates at the lateral epicondyle (sharing a footprint with the RCL) and inserts on the crista supinatoris of the proximal ulna.
3. Annular Ligament: Stabilizes the proximal radioulnar joint.
4. Accessory Lateral Collateral Ligament: Assists in stabilizing the annular ligament during varus stress.
💡 Clinical Pearl: The Isometric Point
The humeral origin of the LUCL is the critical axis point of the ulnohumeral joint. This isometric point lies precisely at the intersection of the anterior humeral line and the radiocapitellar axis. Accurate identification of this point is the most critical step in the procedure; non-isometric graft placement will result in either restricted range of motion or recurrent instability.
INDICATIONS AND PREOPERATIVE EVALUATION
Clinical Indications
- Recurrent, symptomatic PLRI failing a minimum of 3 to 6 months of conservative therapy (bracing, targeted dynamic stabilizer strengthening).
- Positive lateral pivot-shift test of the elbow.
- Positive posterolateral rotatory drawer test.
- Positive chair push-up test or tabletop relocation test.
Imaging
- Standard Radiographs: AP, lateral, and oblique views to rule out associated fractures (e.g., radial head, coronoid) or loose bodies.
- Magnetic Resonance Imaging (MRI): The gold standard for evaluating the integrity of the LUCL, common extensor origin, and capsular structures.
- Fluoroscopy: Dynamic examination under anesthesia (EUA) is often performed immediately prior to incision to confirm the pivot-shift phenomenon.
PATIENT POSITIONING AND SETUP
- Anesthesia: General anesthesia is preferred, often supplemented with a regional block (e.g., supraclavicular or axillary nerve block) for postoperative pain control.
- Positioning: The patient is placed in the supine position. The operative arm is draped free and brought across the chest, or placed on a radiolucent arm board.
- Tourniquet: A sterile pneumatic tourniquet is applied high on the brachium and inflated to 250 mm Hg after exsanguination with an Esmarch bandage.
- Graft Harvest Site: If an autograft (e.g., palmaris longus or gracilis) is planned, the ipsilateral forearm or lower extremity must be prepped and draped accordingly.
SURGICAL TECHNIQUE: NESTOR, O’DRISCOLL, AND MORREY APPROACH
1. The Modified Kocher Approach
Approach the elbow through a modified Kocher incision. The incision begins approximately 5 cm proximal to the lateral epicondyle, extending distally across the epicondyle, and curving slightly anteriorly toward the radial head, ending at the level of the annular ligament.
- Superficial Dissection: Incise the deep fascia in line with the skin incision. Identify the internervous plane between the anconeus (innervated by the radial nerve) and the extensor carpi ulnaris (ECU, innervated by the posterior interosseous nerve).
- Deep Dissection: By sharp dissection, carefully elevate the common extensor origin, including a portion of the extensor carpi radialis brevis (ECRB), to reveal the origin of the radial collateral ligament complex at the lateral epicondyle.
⚠️ Surgical Warning: The Posterior Interosseous Nerve (PIN)
The PIN lies within the supinator muscle belly. When dissecting distally, ensure the forearm is maintained in pronation to move the PIN anteriorly and away from the surgical field. Do not place retractors blindly around the radial neck.
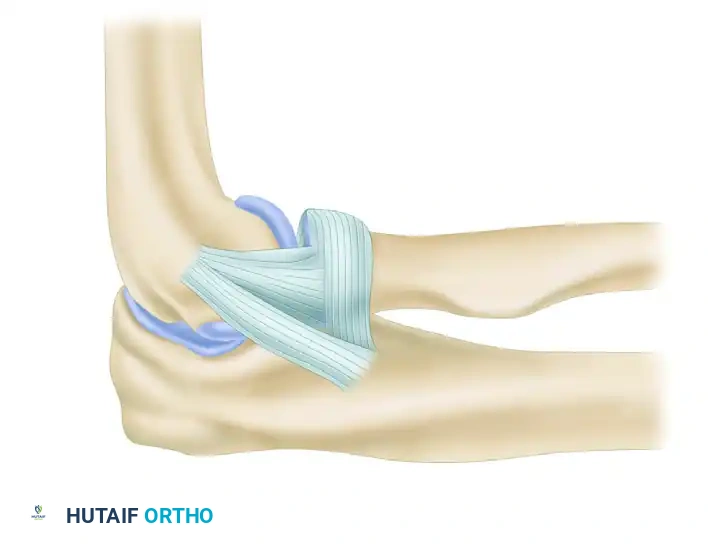
2. Exposure of the Ligamentous Complex
Distally, reflect the anconeus muscle posteriorly and the extensor carpi ulnaris anteriorly. Reflect the extension of the origin of the anconeus to the lateral aspect of the triceps fascia sufficiently to expose the ligament adequately.
Identify the supinator crest (crista supinatoris) of the ulna. This bony ridge is the anatomic insertion site of the LUCL and serves as the primary landmark for ulnar tunnel placement. Typically, upon exposure, a lax ulnar band of the radial collateral ligament is observed, and the abnormal, attenuated portion of the ligament is identified.
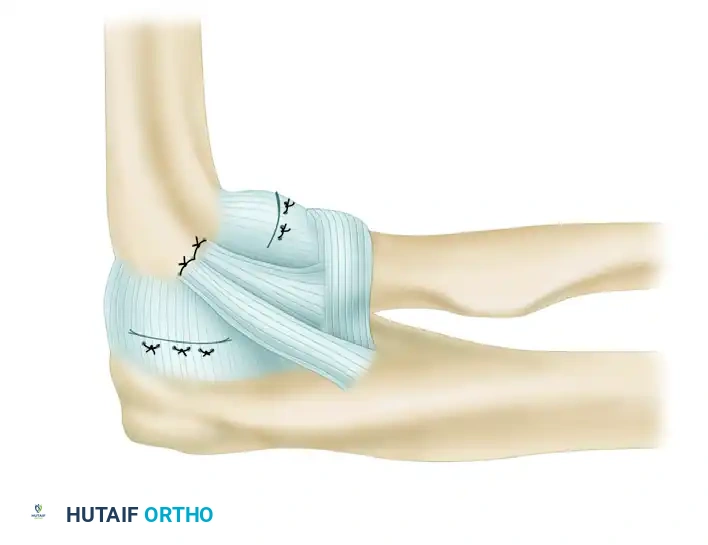
3. Ligament Imbrication and Advancement
Before graft placement, the native, attenuated tissues are managed. Perform an imbrication and advancement of the ulnar band of the radial collateral ligament and the radial part of the radial collateral ligament. This is accomplished using a Bunnell suture technique, placing the sutures through drill holes at the anatomical origin of the ligament in the humerus. This plicates the posterior and anterior capsule, providing a robust secondary restraint.
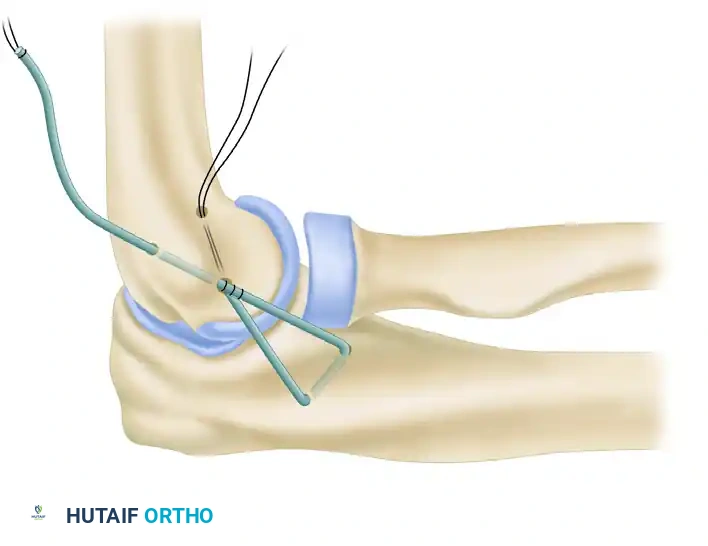
4. Ulnar Tunnel Preparation
Attention is now turned to the ulna. The ulnar tunnel must be placed precisely in the crista supinatoris tubercle.
* Using a high-speed burr or a 3.2-mm drill, create two converging drill holes at the supinator crest.
* The holes should be separated by a 1.5 to 2.0 cm bone bridge to prevent cortical blowout during graft tensioning.
* The tunnel is oriented to have optimal alignment with the isometric point on the lateral epicondyle.
5. Graft Harvest and Passage
The palmaris longus tendon is the graft of choice due to its accessibility and biomechanical properties. If absent, a strip of triceps fascia or a gracilis autograft may be utilized.
* Harvest the graft and prepare the ends with running locking sutures (e.g., #2 non-absorbable suture).
* Pass the graft through the prepared ulnar tunnel.
* Create a "yoke stitch" to secure the graft upon itself at the ulnar insertion, ensuring a low-profile and secure anchor point before passing the limbs proximally toward the humerus.
6. Humeral Tunnel Preparation and Isometry
Identifying the isometric point on the lateral epicondyle is paramount.
* A tunnel is made in the humerus at the isometric origin.
* The primary entry hole is expanded in a posterosuperior direction to emerge posterior and superior to the point of isometry.
* A second humeral tunnel is drilled to exit posterior and inferior from the common entry site, creating a V-shaped or Y-shaped intraosseous pathway.
💡 Clinical Pearl: Testing Isometry
Before drilling the final humeral tunnels, place a K-wire at the presumed isometric point. Loop a suture around the K-wire and the ulnar bone bridge. Take the elbow through a full range of motion. The suture should not change length by more than 1-2 mm. If it stretches in flexion, the pin is too anterior; if it stretches in extension, the pin is too posterior.
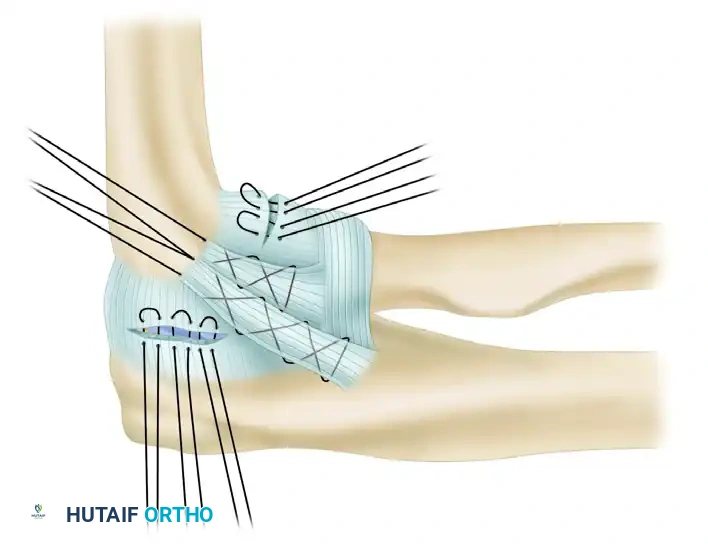
7. Graft Tensioning and Final Fixation
The two limbs of the palmaris longus tendon are drawn proximally and introduced into the humeral tunnels.
* The graft is tensioned with the elbow held in approximately 30 to 40 degrees of flexion and the forearm in full pronation. Pronation is critical as it closes the lateral joint space and reduces the posterolateral subluxation.
* Apply a varus stress to ensure the joint is fully reduced while tensioning.
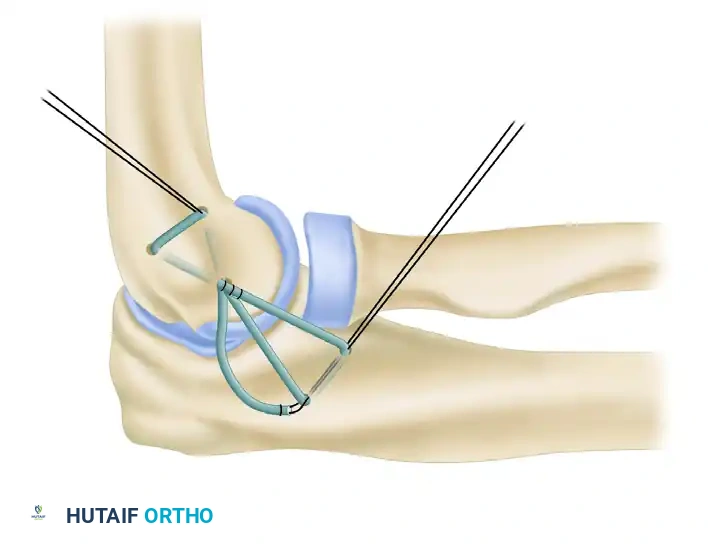
Once optimal tension is achieved, the palmaris longus tendon limbs are drawn through the ulnar and humeral tunnels and tied to themselves after recrossing the joint. This figure-of-eight or docking configuration provides a robust, anatomic reconstruction of the LUCL. The native capsular flaps and common extensor origin are then meticulously repaired over the graft to provide additional dynamic stability.
8. Closure
- The common extensor origin is securely reattached to the lateral epicondyle using transosseous sutures or suture anchors.
- The subcutaneous tissue is closed with absorbable sutures.
- The skin is closed with a subcuticular stitch or surgical staples.
- A sterile dressing is applied, and the arm is placed in a well-padded posterior splint.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol is designed to protect the healing graft while preventing elbow stiffness, a common complication of elbow trauma and surgery.
Phase I: Immediate Postoperative (Weeks 0-2)
- Immobilization: With the forearm in full pronation, the elbow is placed in 70 to 80 degrees of flexion and held in this position in a posterior splint for 10 to 14 days.
- Rationale: Full pronation utilizes the brachioradialis and common extensor musculature as a dynamic splint, compressing the radiocapitellar joint and protecting the lateral reconstruction from varus stress.
Phase II: Protected Range of Motion (Weeks 2-6)
- Bracing: At 10 to 14 days, the splint is removed, sutures are extracted, and the patient is transitioned to a hinged elbow brace.
- Motion: Protected movement is allowed in the hinged brace. The brace is typically locked in 30 degrees of extension to prevent terminal extension, which places the highest stress on the LUCL graft. The forearm must remain in pronation during early flexion-extension exercises.
- Restrictions: Avoid shoulder abduction and internal rotation during elbow extension, as this creates a gravity-induced varus moment across the elbow.
Phase III: Strengthening and Weaning (Weeks 6-12)
- Brace Weaning: After 6 weeks, the hinged brace can be removed for light activity and physical therapy.
- Strengthening: Isometric and progressive isotonic strengthening of the dynamic stabilizers (triceps, biceps, brachioradialis, and common extensors) is initiated.
- Discontinuation: The brace is discontinued completely at the end of an additional 6 weeks (12 weeks total post-op).
Phase IV: Return to Play (Months 3-12)
- Patients are encouraged to protect the elbow from heavy activity and sudden varus loads.
- Lifting Mechanics: The patient is advised to protect the elbow from stresses during activities of daily living, such as lifting weights. We recommend that patients lift weights only in the plane of elbow flexion and extension, keeping the shoulder adducted and the elbow close to the body.
- Clearance: Full, unrestricted activity is generally allowed at 6 months. Participation in heavy contact sports or high-demand overhead athletics is allowed at 1 year, contingent upon the restoration of full strength and dynamic stability.
COMPLICATIONS AND PITFALLS
- Recurrent Instability: The most common cause of failure is non-isometric tunnel placement, particularly placing the humeral tunnel too anteriorly. Failure to maintain the forearm in pronation during the initial healing phase can also stretch the graft.
- Elbow Stiffness: Over-tensioning the graft or prolonged immobilization beyond 14 days can lead to severe flexion or extension contractures. Early, protected, arc-controlled motion is vital.
- Nerve Injury: The posterior interosseous nerve (PIN) is at risk during the distal exposure of the supinator crest. Maintaining pronation during dissection drops the PIN anteriorly, protecting it from iatrogenic injury.
- Hardware/Tunnel Complications: Cortical blowout at the crista supinatoris can occur if the bone bridge is too narrow (<1.5 cm). If this occurs, the surgeon must be prepared to use suture anchors as a salvage technique for ulnar fixation.
You Might Also Like