Proximal Biceps Tendon Rupture: Comprehensive Surgical Management and Tenodesis Techniques
Key Takeaway
Proximal biceps tendon ruptures frequently occur in the long head of the biceps brachii, often secondary to chronic microtrauma or acute overload. While nonoperative management suffices for many, active patients and manual laborers benefit from surgical intervention. This guide details the indications, biomechanics, and step-by-step surgical execution of open subpectoral biceps tenodesis, ensuring optimal length-tension restoration and functional recovery.
RUPTURE OF BICEPS BRACHII TENDONS: PATHOPHYSIOLOGY AND BIOMECHANICS
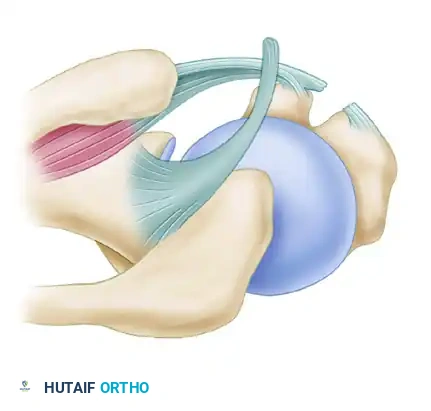
More than half of all ruptures involving the biceps brachii muscle occur through the tendon of its long head (LHB). The LHB is a unique anatomic structure, originating from the supraglenoid tubercle and the superior glenoid labrum, traversing intra-articularly before exiting the shoulder joint via the intertubercular (bicipital) groove.
The rupture is typically transverse and is located either within the shoulder joint itself or within the proximal aspect of the intertubercular groove. While the vast majority of ruptures involve the LHB, a minority occur at the musculotendinous junction or directly at the attachment to the glenoid. Rarely, ruptures may occur through the tendon of the short head, the muscle belly proper, or the distal biceps tendon at the radial tuberosity.
Epidemiology and Etiology
Proximal biceps tendon ruptures exhibit a bimodal distribution based on etiology:
* Degenerative Ruptures (Age 40–60): The most common demographic. These injuries are frequently the culmination of chronic impingement syndrome, rotator cuff arthropathy, or repetitive microtrauma. The LHB tendon undergoes mucoid degeneration, tenosynovitis, and eventual mechanical failure as it glides within a stenotic or osteophytic bicipital groove.
* Traumatic Ruptures (Younger Cohorts): Occur in younger, highly active individuals during heavy weightlifting, forceful eccentric loading, or high-impact sports activities (e.g., football, rugby, soccer, snowboarding). Traumatic falls onto an outstretched hand (FOOSH) can also precipitate acute avulsion or mid-substance tearing.
Clinical Pearl: A spontaneous rupture of the LHB in a patient over 50 years of age is highly predictive of concomitant rotator cuff pathology, particularly tears of the supraspinatus or subscapularis. Always evaluate the rotator cuff when assessing an LHB rupture.
Biomechanical Consequences of Rupture
The long head of the biceps acts as a humeral head depressor and an anterior stabilizer of the glenohumeral joint, in addition to its primary roles in elbow flexion and forearm supination.
Acute rupture of the proximal biceps tendon is associated with measurable biomechanical deficits:
* Elbow Flexion: A 20% decrease in peak elbow flexion power.
* Shoulder Abduction: The power of shoulder abduction with the arm in external rotation is reduced by approximately 17% compared to the contralateral, uninjured side.
* Forearm Supination: While not explicitly quantified in all studies, supination endurance is often notably diminished.
With an acute injury, patients typically present with localized ecchymosis and a characteristic prominent lump on the anterolateral aspect of the middle third of the arm—the classic "Popeye" deformity—resulting from the distal retraction of the muscle belly. Interestingly, in chronic or late-presenting ruptures, patients often report no appreciable weakness in either elbow flexion or shoulder abduction, as the short head of the biceps and the brachialis muscle undergo compensatory hypertrophy.
CLINICAL EVALUATION AND INDICATIONS FOR SURGERY
Diagnostic Assessment
The diagnosis of a proximal biceps tendon rupture is primarily clinical. Patients often report an audible "pop" or tearing sensation in the anterior shoulder, followed by sharp pain that paradoxically subsides, leaving a dull ache.
- Physical Examination: Look for the "Popeye" sign, which becomes more pronounced during active elbow flexion or resisted supination. Provocative tests for LHB pathology (prior to complete rupture) include Speed’s test and Yergason’s test.
- Imaging:
- Radiographs: Standard trauma series (AP, Scapular Y, Axillary) to rule out fractures or assess for acromiohumeral interval narrowing (suggestive of rotator cuff tear).
- Ultrasound: Highly sensitive and specific for identifying an empty bicipital groove and the retracted tendon stump.
- MRI: The gold standard for evaluating the intra-articular stump, the degree of retraction, and, crucially, the integrity of the rotator cuff and superior labrum.
Indications for Operative Management
Nonoperative management (rest, NSAIDs, physical therapy) is highly successful for elderly, sedentary patients, or those who are not bothered by the cosmetic deformity. However, surgical intervention is indicated in specific populations:
- Young, Active Patients: Athletes and individuals who require maximal upper extremity strength and endurance.
- Manual Laborers: Occupations requiring repetitive lifting, carrying, or forceful supination (e.g., carpenters, mechanics).
- Cosmetic Concerns: Patients who find the "Popeye" deformity unacceptable.
- Symptomatic Cramping: Patients experiencing chronic, painful cramping in the biceps muscle belly due to altered length-tension relationships.
- Concomitant Pathology: Patients requiring surgical intervention for associated rotator cuff tears or labral pathology.
SURGICAL ANATOMY AND PREOPERATIVE PLANNING
Successful repair via tenodesis requires an intimate understanding of the anterior shoulder anatomy.
* Deltopectoral Interval: The primary surgical window, bordered by the deltoid laterally and the pectoralis major medially. The cephalic vein marks this interval and is typically retracted laterally with the deltoid.
* Intertubercular Groove: Located between the greater and lesser tuberosities, roofed by the transverse humeral ligament.
* Pectoralis Major Insertion: The inferior border of the pectoralis major tendon serves as the critical landmark for the subpectoral tenodesis approach.
* Neurovascular Structures: The musculocutaneous nerve penetrates the coracobrachialis approximately 5 to 8 cm distal to the coracoid process. Dissection medial to the conjoined tendon must be strictly avoided to prevent devastating neurological injury.
REPAIR OF PROXIMAL BICEPS TENDON RUPTURE: SURGICAL TECHNIQUES
The goal of surgery is to restore the anatomic length-tension relationship of the biceps muscle by anchoring the tendon to the humerus (tenodesis). The subpectoral approach is widely considered the gold standard, as it removes the tendon from the bicipital groove entirely, eliminating the groove as a source of persistent pain.
Patient Positioning and Anesthesia
- Anesthesia: General anesthesia is typically utilized, often supplemented with an interscalene regional nerve block for postoperative pain control.
- Positioning: The patient is placed in a modified beach-chair position with the head secured. The operative arm is draped free, allowing for full manipulation, and rested on an arm board or supported by a mechanical arm positioner.
Step-by-Step Surgical Execution: Open Subpectoral Tenodesis
🔪 Surgical Technique: Subpectoral Biceps Tenodesis
Step 1: Proximal Exposure and Tendon Identification
* Make an anterior incision over the deltopectoral groove.
* Develop the interval between the deltoid and the pectoralis major, retracting the cephalic vein laterally.
* Expose the tendon of the long head of the biceps by opening the intertubercular groove. This requires sharp division of the transverse humeral ligament.
* Identify the ruptured LHB tendon. If the tendon is incarcerated within the joint or groove, carefully mobilize it.
* Remove the degenerative infraglenoid portion of the tendon.
* Crucial Step: If the tendon was previously intact (e.g., surgery performed for severe biceps tendinitis rather than acute rupture), place a marking suture in the tendon at the superior border of the pectoralis major so that proper anatomic length can be retained during fixation.
Step 2: The Inferior Axillary (Subpectoral) Approach
* Make a secondary inferior axillary incision (or extend the primary incision distally), centered precisely on the inferior border of the pectoralis major tendon.
* Identify the short head of the biceps and the coracobrachialis muscle belly.
* Incise the overlying deep fascia longitudinally to expose the underlying structures.
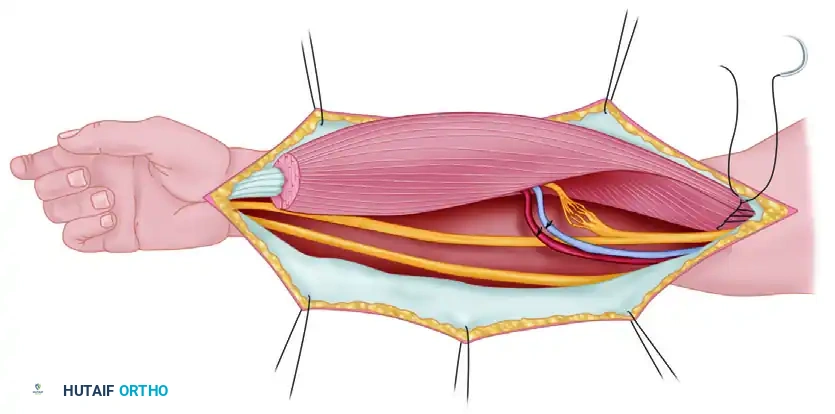
Step 3: Tendon Retrieval and Preparation
* Place a Hohmann retractor under the pectoralis major tendon and retract the muscle proximally and laterally. This exposes the humeral shaft at the level of the bicipital groove's distal extent.
* Deliver the ruptured long head of the biceps into the subpectoral incision. Use blunt dissection to free any adhesions preventing distal excursion.
* Prepare the tendon end. Using a heavy non-absorbable suture (e.g., #2 FiberWire), place a locking whipstitch (Krackow or similar configuration) into the distal 2 to 3 cm of the tendon.
Step 4: Restoring the Length-Tension Relationship
* Determining the correct length is the most critical step to prevent postoperative cramping or residual weakness.
* At the location of the intended tenodesis (typically 1 cm distal to the inferior border of the pectoralis major, in the bicipital groove), calculate the required tendon length.
* The 25 mm Rule: Add 25 mm to the length of the biceps tendon from the musculotendinous junction to account for the portion of the tendon that will be docked into the humeral bone socket. Excise the remaining redundant proximal tendon.
Surgical Warning: Failure to accurately tension the biceps tendon will result in either a persistent "Popeye" deformity (if tensioned too loosely) or severe postoperative stiffness and muscle cramping (if tensioned too tightly). Ensure the elbow is extended and the forearm fully supinated when assessing final tension.
Step 5: Bony Preparation and Fixation
Fix the tendon to the bone using one of several validated techniques. Interference screw fixation is the most biomechanically robust for early mobilization.
-
Interference Screw Technique:
- Drill a guide pin into the anterior humeral cortex at the planned tenodesis site (unicortical).
- Over-ream the guide pin with a cannulated reamer matching the measured diameter of the prepared tendon (usually 7 to 8 mm). Ream to a depth of approximately 25 to 30 mm.
- Pass the whipstitch sutures through the cannulation of a bioabsorbable or PEEK interference screw.
- Dock the tendon into the socket by applying tension to the sutures.
- Advance the interference screw over the guide wire and into the socket, compressing the tendon against the cortical bone. Ensure the screw is flush with the anterior cortex.
- Tie the remaining suture limbs over the top of the screw for secondary backup fixation.
-
Alternative Fixation Methods: If interference screws are unavailable or contraindicated (e.g., poor bone quality), the tendon may be fixed using suture anchors (double-loaded anchors placed in the groove) or via a traditional bony trough with transosseous drill holes. Cortical button techniques (onlay or inlay) are also highly effective and increasingly popular.
Step 6: Closure
* Irrigate the wound copiously with sterile saline.
* Ensure meticulous hemostasis.
* Close the deep fascial layers over a suction drain if necessary.
* Close the subcutaneous tissue with interrupted absorbable sutures and the skin with a subcuticular closure or surgical staples.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The success of a biceps tenodesis relies heavily on strict adherence to a phased postoperative rehabilitation protocol. Premature eccentric loading can lead to catastrophic failure of the fixation.
Phase I: Protection Phase (Weeks 0–4)
- Immobilization: Postoperatively, the arm is rested in a sling for several days to 4 weeks, depending on the security of the fixation and surgeon preference.
- Range of Motion (ROM): Passive range of motion (PROM) for the shoulder and elbow is initiated early to prevent stiffness. Active extension of the elbow is permitted, but active flexion and supination are strictly prohibited to protect the tenodesis site.
- Activities: The patient is encouraged to resume light, non-weight-bearing activities of daily living as tolerated.
Phase II: Active Motion Phase (Weeks 4–8)
- Sling Weaning: The sling is discontinued.
- Active ROM: Active-assisted and active range of motion (AROM) for elbow flexion and forearm supination are initiated.
- Strengthening: Light isometric strengthening may begin late in this phase, but heavy lifting remains contraindicated.
Phase III: Strengthening Phase (Weeks 8–12)
- Progressive Resistance: Isotonic strengthening exercises for the biceps and rotator cuff are introduced.
- Functional Training: Patients begin closed kinetic chain exercises and progressive loading.
Phase IV: Return to Play (Weeks 12+)
- Sports Participation: Participation in heavy manual labor, contact sports, or heavy weightlifting should be delayed for at least 12 weeks.
- Clearance: Full return to unrestricted activities is permitted only when the patient has achieved full, painless ROM and symmetric strength compared to the contralateral extremity.
COMPLICATIONS AND PITFALLS
While proximal biceps tenodesis is generally a highly successful procedure with excellent patient satisfaction, complications can occur:
- Nerve Injury: The musculocutaneous nerve is at risk during aggressive medial retraction or deep dissection. Symptoms include lateral forearm numbness and profound weakness in elbow flexion.
- Fixation Failure: Pull-out of the tendon from the bone socket can occur due to poor bone quality, undersized interference screws, or patient non-compliance with postoperative restrictions. This results in a recurrent "Popeye" deformity.
- Persistent Pain: Often due to inadequate resection of the proximal tendon stump, leaving degenerative tissue within the bicipital groove, or unrecognized concomitant rotator cuff pathology.
- Cosmetic Asymmetry: Even with successful healing, slight alterations in the muscle belly contour may persist. Preoperative patient counseling regarding cosmetic expectations is mandatory.
- Stiffness: Arthrofibrosis of the shoulder or elbow can result from prolonged immobilization. Early, controlled passive motion is the best preventative measure.
By meticulously adhering to anatomic principles, ensuring precise length-tension restoration, and utilizing robust fixation techniques, the orthopedic surgeon can reliably restore function and alleviate pain in patients suffering from proximal biceps tendon ruptures.
📚 Medical References
- biceps tendon rupture: a new technique using the EndoButton, J Shoulder Elbow Surg 9:120, 2000.
- Balabaud L, Ruiz C, Nonnemacher J, et al: Repair of distal biceps tendon ruptures using a suture anchor and an anterior approach, J Hand Surg 29B:178, 2004.
- Berlet GC, Johnson JA, Milne AD, et al: Distal biceps brachii
You Might Also Like