Open Excision and Decompression of Suprascapular Nerve Ganglion Cysts
Key Takeaway
Surgical excision of a ganglion cyst compressing the suprascapular nerve requires a meticulous posterior approach. The procedure involves elevating the trapezius, identifying the suprascapular notch, and releasing the transverse scapular ligament while protecting the underlying nerve and overlying artery. This guide details the step-by-step open technique, anatomical considerations, and postoperative rehabilitation protocols for optimal functional recovery of the shoulder.
Introduction to Suprascapular Nerve Entrapment
Suprascapular neuropathy is a well-recognized cause of posterior shoulder pain and profound weakness, frequently misdiagnosed as primary rotator cuff pathology or cervical radiculopathy. One of the most common etiologies of this neuropathy is compression by a ganglion cyst (paralabral cyst). These cysts typically arise secondary to capsulolabral injuries—most notably Superior Labrum Anterior and Posterior (SLAP) tears—where a capsular defect acts as a one-way valve, allowing synovial fluid to extravasate and pool in the spinoglenoid or suprascapular notch.
While the title of this specific procedure highlights the "inferior branch" (which innervates the infraspinatus and is typically compressed at the spinoglenoid notch), the surgical approach detailed herein focuses on the proximal posterior approach. This approach accesses the suprascapular notch, allowing for the release of the transverse scapular ligament, proximal cyst decompression, and distal exploration toward the spinoglenoid notch.
This masterclass provides a comprehensive, textbook-level guide to the open posterior surgical approach for the removal of a ganglion cyst and the decompression of the suprascapular nerve, tailored for orthopedic residents, fellows, and practicing consultants.
Surgical Anatomy and Biomechanics
A profound understanding of the suprascapular nerve's anatomical course is non-negotiable for safe and effective surgical intervention.
The Suprascapular Nerve Course
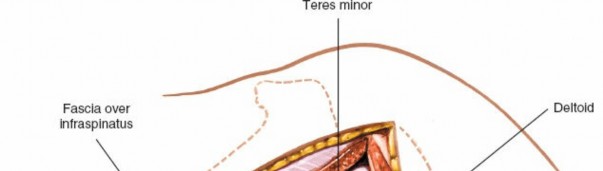
The suprascapular nerve is a mixed motor and sensory nerve originating from the upper trunk of the brachial plexus (C5, C6 roots). It courses through the posterior triangle of the neck, passing deep to the trapezius and omohyoid muscles to reach the superior border of the scapula.
- The Suprascapular Notch: The nerve passes through the suprascapular notch, which is roofed by the superior transverse scapular ligament.
- Vascular Relationship: The suprascapular artery and vein pass over the transverse scapular ligament.
- Motor Branches: After exiting the notch, the nerve provides motor branches to the supraspinatus muscle.
- The Spinoglenoid Notch: The nerve then courses laterally and inferiorly around the base of the scapular spine (the spinoglenoid notch), passing under the spinoglenoid ligament to provide terminal motor innervation to the infraspinatus muscle.
Clinical Pearl: Remember the classic mnemonic "Army over Navy" at the suprascapular notch: The suprascapular Artery passes over the ligament, while the suprascapular Nerve passes under the ligament.
Biomechanics of Compression
Ganglion cysts at the suprascapular notch compress the main trunk of the nerve, leading to denervation of both the supraspinatus and infraspinatus muscles. Conversely, cysts located at the spinoglenoid notch selectively compress the inferior branch, resulting in isolated infraspinatus atrophy and weakness in external rotation, while abduction (supraspinatus function) remains intact.
Indications and Preoperative Planning
Indications for Surgery
Surgical excision and nerve decompression are indicated in the following scenarios:
* Failed Conservative Management: Persistent pain and weakness after 3 to 6 months of non-operative treatment (NSAIDs, physical therapy, image-guided cyst aspiration).
* Progressive Motor Atrophy: Clinical or electromyographic (EMG) evidence of progressive supraspinatus or infraspinatus muscle atrophy.
* Large Compressive Cysts: Massive multiloculated cysts identified on MRI that are unlikely to resolve with aspiration alone.
* Concomitant Intra-articular Pathology: When a SLAP tear requires concurrent surgical repair (often managed arthroscopically, though open cyst excision may still be required for massive, inaccessible extra-articular extensions).
Preoperative Imaging and Diagnostics
- Magnetic Resonance Imaging (MRI): The gold standard. MRI without contrast is highly sensitive for identifying the ganglion cyst, its exact anatomical location (suprascapular vs. spinoglenoid notch), and the degree of fatty infiltration or atrophy in the rotator cuff muscles.
- Electromyography and Nerve Conduction Studies (EMG/NCS): Essential for confirming the diagnosis, localizing the site of compression, and establishing a baseline to monitor postoperative nerve recovery.
Patient Positioning and Anesthesia
Anesthesia
The procedure is performed under general anesthesia. An interscalene regional block may be administered for postoperative pain control, though the surgeon must weigh this against the need for immediate postoperative neurological assessment.
Positioning
The patient can be positioned in either the lateral decubitus or prone position, depending on surgeon preference.
* Prone Position: Often preferred for open posterior approaches as it provides excellent, stable exposure of the scapular spine and posterior shoulder musculature. The operative arm is draped free to allow for manipulation.
* Preparation: The entire shoulder girdle, hemithorax, and arm are prepped and draped in a standard sterile fashion.
Surgical Technique: Step-by-Step Posterior Approach
The open posterior approach requires meticulous dissection to avoid iatrogenic injury to the trapezius, supraspinatus, and the neurovascular bundle.
1. Skin Incision and Superficial Dissection
- Palpate the spine of the scapula. Make a linear incision parallel to and just superior to the scapular spine, extending from the acromion medially toward the medial border of the scapula.
- Dissect through the subcutaneous tissue to expose the deep fascia overlying the trapezius muscle.
- Incise the trapezius fascia in line with the skin incision. Carefully detach the trapezius insertion from the superior aspect of the scapular spine.
Surgical Warning: When elevating the trapezius, maintain a strict subperiosteal plane to ensure a robust tissue cuff remains for later repair. Poor repair of the trapezius can lead to postoperative weakness and cosmetic deformity.
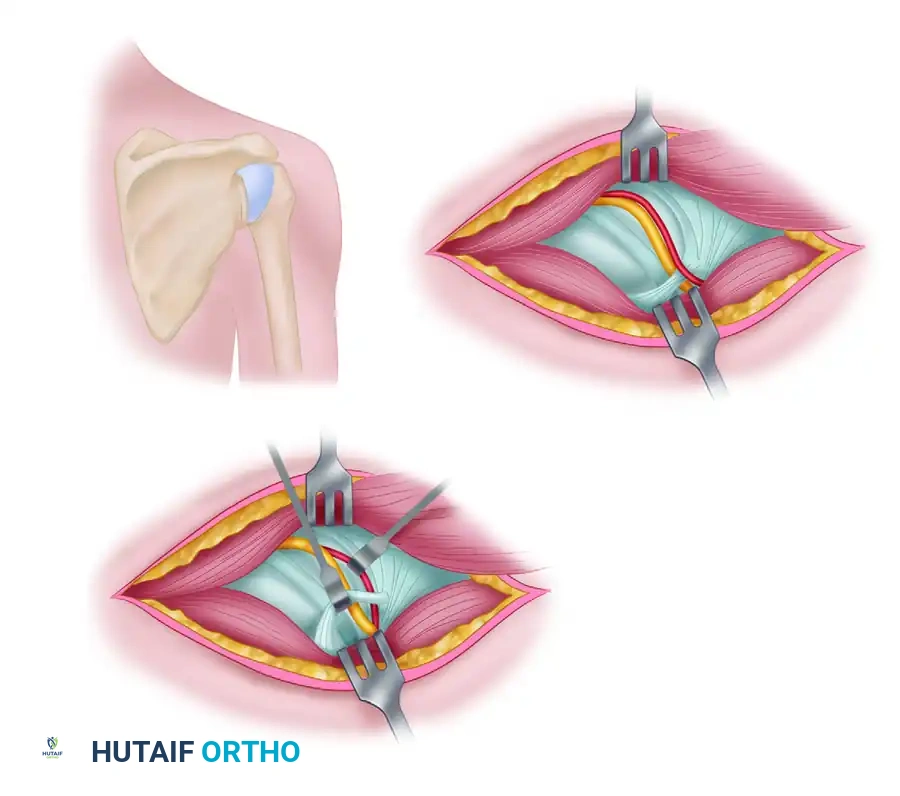
2. Deep Dissection and Muscle Retraction
- As the fibers of the trapezius and periosteum are elevated, a thin, fatty areolar layer becomes visible between the undersurface of the trapezius and the supraspinatus muscle.
- Crucial Step: Do not elevate the supraspinatus muscle from its fossa. Doing so risks devascularization and denervation of the muscle belly.
- Retract the mobilized trapezius muscle cephalad (superiorly) using a wide, blunt retractor (e.g., a Richardson or Kolbel retractor) to expose the supraspinatus fascia.
3. Locating the Suprascapular Notch
- Using blunt dissection—ideally with a wet, gloved finger—gently palpate along the superior border of the scapula, moving medially to laterally until the suprascapular notch and the overlying transverse scapular ligament are identified.
- Only minimal distal (inferior) retraction of the supraspinatus muscle is required to visualize the notch. Over-retraction can stretch the motor branches supplying the muscle.
4. Isolation and Release of the Transverse Scapular Ligament
- Once the notch is palpated, use a blunt elevator (such as a Freer or a small Cobb elevator) to meticulously clean the soft tissue off the suprascapular ligament.
- Vascular Protection: Identify and protect the suprascapular artery and vein, which run immediately superficial to the ligament. Gently retract these vessels superiorly or laterally.
- Introduce a blunt nerve hook or a small right-angle clamp under the transverse scapular ligament to protect the underlying suprascapular nerve.
- Sharply release the ligament using a #15 scalpel or a Kerrison rongeur.
Clinical Pearl: Further exploration of the nerve or extensive intraneural neurolysis is generally unnecessary and contraindicated. The primary goal is decompression via ligament release and cyst excision. Excessive manipulation of the nerve can lead to iatrogenic neuropraxia or axonotmesis.
5. Ganglion Cyst Excision and Decompression
- With the ligament released, inspect and palpate the surrounding region (extending toward the spinoglenoid notch if necessary) to locate the ganglion cyst.
- Carefully dissect the cyst wall from the surrounding areolar tissue. If the cyst is massive, it may be intentionally punctured and aspirated to decompress it, allowing for easier dissection of the cyst wall.
- Trace the stalk of the cyst to its origin (often a capsular defect at the glenoid rim). Ligate or cauterize the stalk to minimize the risk of recurrence.
6. Closure and Trapezius Reattachment
- Irrigate the suprascapular fossa copiously with sterile saline. Ensure absolute hemostasis, particularly from the suprascapular vessels.
- Trapezius Repair: The reattachment of the trapezius muscle to the spine of the scapula must be mechanically secure.
- Place several drill holes (using a 2.0mm drill bit) along the superior edge of the scapular spine.
- Pass heavy, nonabsorbable sutures (e.g., #2 FiberWire or Ethibond) through the drill holes and utilize a horizontal mattress configuration to securely tie the trapezius tendon back to its anatomical footprint.
- Close the deep fascial layers, subcutaneous tissue, and skin in a routine, layered manner.
- Apply a sterile dressing and place the patient's arm in a standard shoulder sling for immobilization.
Postoperative Protocol and Rehabilitation
The postoperative rehabilitation protocol must balance the protection of the trapezius repair with the prevention of shoulder stiffness.
Phase I: Protection (Weeks 0–4)
- Immobilization: The patient remains in a sling for 4 to 6 weeks to protect the transosseous trapezius repair.
- Range of Motion (ROM): Active ROM of the elbow, wrist, and hand is encouraged immediately. Pendulum exercises may begin at week 2.
- Restrictions: Strictly avoid active shoulder elevation, abduction, and any resisted movements of the shoulder girdle.
Phase II: Early Motion (Weeks 4–8)
- Sling Weaning: Discontinue the sling at 4 to 6 weeks.
- Passive and Active-Assisted ROM: Initiate formal physical therapy focusing on passive range of motion (PROM) and progressing to active-assisted range of motion (AAROM) in all planes.
- Scapular Mechanics: Begin gentle scapular retraction and stabilization exercises.
Phase III: Strengthening (Weeks 8–12+)
- Active ROM: Progress to full active range of motion (AROM).
- Strengthening: Initiate isotonic strengthening of the rotator cuff and periscapular musculature. Focus heavily on supraspinatus and infraspinatus recruitment, utilizing biofeedback if necessary.
- Return to Activity: Return to heavy lifting or overhead sports is typically permitted between 4 to 6 months, contingent upon the return of full strength and symmetrical muscle bulk.
Complications and Pitfalls
While generally safe, the open posterior approach carries specific risks that the orthopedic surgeon must mitigate:
- Iatrogenic Nerve Injury: The suprascapular nerve is highly vulnerable during the release of the transverse scapular ligament. Blind cutting of the ligament without a protective instrument underneath is strictly prohibited.
- Vascular Injury: Laceration of the suprascapular artery can cause significant hemorrhage, obscuring the surgical field and increasing the risk of secondary nerve injury during attempts at hemostasis.
- Trapezius Dehiscence: Failure to achieve a secure transosseous repair of the trapezius can lead to muscle retraction, chronic pain, and severe shoulder dysfunction.
- Incomplete Decompression/Recurrence: Failure to identify and ligate the cyst stalk, or failure to address a concomitant intra-articular labral tear, significantly increases the risk of ganglion recurrence.
Arthroscopic vs. Open Considerations
It is important to note that the paradigm of treating paralabral cysts has evolved. As noted in the broader literature (and referenced as Chapter 52 in standard operative texts), arthroscopic internal cyst decompression combined with SLAP repair has become highly successful and is often considered the first-line surgical treatment.
During the arthroscopic procedure, the capsulolabral defect is identified, and the cyst is decompressed intra-articularly through the defect. The labrum is then repaired, sealing the one-way valve.
However, the open posterior approach detailed in this guide remains an essential technique in the orthopedic surgeon's armamentarium. It is specifically indicated for:
* Massive cysts that cannot be adequately decompressed arthroscopically.
* Cysts with thick, organized walls that require complete excision.
* Cases of primary nerve entrapment by an ossified transverse scapular ligament without an associated labral tear.
* Revision cases where arthroscopic management has failed.
By mastering both the open anatomical approach and modern arthroscopic techniques, the orthopedic surgeon can ensure comprehensive, patient-specific management of suprascapular neuropathy.
You Might Also Like