Posterior Surgical Approach for Suprascapular Nerve Entrapment

Key Takeaway
Suprascapular nerve entrapment at the spinoglenoid notch frequently results from space-occupying lesions like ganglion cysts associated with posterior labral tears. The posterior surgical approach provides direct access to the spinoglenoid notch for cyst excision and nerve decompression. This technique involves precise elevation of the trapezius and reflection of the infraspinatus to expose the posterior glenoid neck, ensuring meticulous neurolysis while preserving the neurovascular bundle.
INTRODUCTION AND PATHOPHYSIOLOGY
Suprascapular nerve entrapment is a well-recognized, albeit relatively uncommon, cause of posterior shoulder pain and profound upper extremity weakness. While the raw historical literature occasionally mislabels this as "subscapular" nerve entrapment due to typographical legacy, the precise anatomical pathology occurs along the course of the suprascapular nerve, most notably at the suprascapular notch or the spinoglenoid notch.
Entrapment at the spinoglenoid notch is uniquely characterized by isolated weakness and atrophy of the infraspinatus muscle, sparing the supraspinatus. The most frequent etiology for compression at this specific anatomical juncture is the formation of a paralabral ganglion cyst. These cysts typically arise from a one-way valve mechanism created by a posterior or posterosuperior labral tear. Synovial fluid is pumped from the glenohumeral joint into the paralabral space during shoulder motion, accumulating in the spinoglenoid notch and exerting direct mechanical pressure on the suprascapular nerve.
Clinical Pearl: Isolated infraspinatus atrophy is pathognomonic for suprascapular nerve compression at the spinoglenoid notch. If both the supraspinatus and infraspinatus are atrophied, the site of compression is almost certainly proximal, typically at the suprascapular notch beneath the transverse scapular ligament.
While modern advancements have popularized arthroscopic management for these lesions, the open posterior surgical approach remains a critical technique in the armamentarium of the orthopedic surgeon. It is particularly indicated for massive, multiloculated cysts, cysts without an identifiable intra-articular communication, solid tumors (e.g., schwannomas), or cases of iatrogenic nerve tethering following prior surgical interventions.
CLINICAL EVALUATION AND DIAGNOSTIC IMAGING
Patients typically present with a vague, deep-seated, aching pain in the posterior aspect of the shoulder, which may radiate down the arm or into the neck. The hallmark physical examination finding is weakness in external rotation with the arm positioned at the side, accompanied by visible hollowing of the infraspinatus fossa due to muscle atrophy.
Diagnostic Modalities
- Electromyography (EMG) and Nerve Conduction Studies (NCS): These remain the physiological gold standard for confirming the diagnosis. Findings will demonstrate denervation potentials (fibrillations, positive sharp waves) isolated to the infraspinatus muscle, with prolonged latencies of the suprascapular nerve when stimulating at Erb's point and recording over the infraspinatus.
- Magnetic Resonance Imaging (MRI): MRI is the anatomical gold standard. It not only visualizes the space-occupying lesion but also identifies the underlying intra-articular pathology (e.g., SLAP tear or posterior labral tear) and assesses the degree of fatty infiltration in the rotator cuff musculature.
The following MR images demonstrate the classic presentation of a paralabral ganglion cyst causing entrapment neuropathy of the suprascapular nerve at the spinoglenoid notch:
FIGURE 46-16A: Axial MR image. Arrowheads indicate a small, low-density shadow situated just posterior to the neck of the glenoid, representing the early formation of a paralabral cyst.

FIGURE 46-16B: Sagittal/Coronal oblique MR image. The solid black arrow highlights a distinct ganglion cyst residing within the region of the spinoglenoid notch, exerting mass effect on the neurovascular bundle.
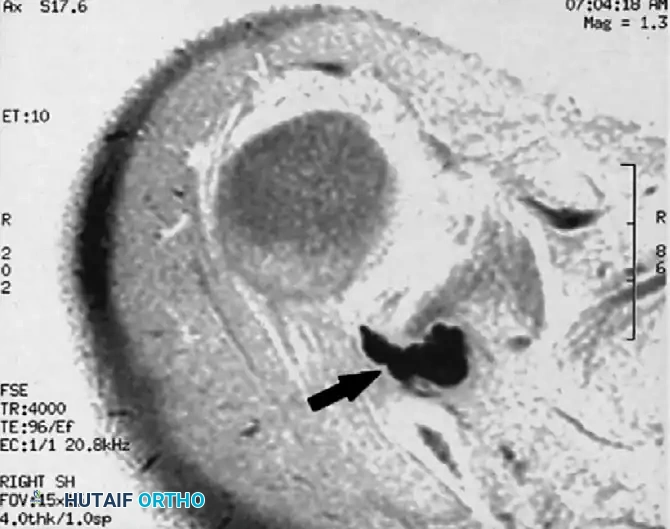
FIGURE 46-16C: Axial MR image demonstrating a large, multiloculated ganglion cyst (arrow). The cyst clearly appears to originate from the posterosuperior aspect of the glenohumeral joint, tracking posteriorly to fill the spinoglenoid notch.
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of the posterior shoulder anatomy is mandatory before undertaking this approach. The suprascapular nerve arises from the upper trunk of the brachial plexus (C5, C6). It courses laterally through the posterior triangle of the neck, passing beneath the trapezius and through the suprascapular notch (under the superior transverse scapular ligament).
After providing motor branches to the supraspinatus, the nerve descends obliquely along the floor of the supraspinous fossa. It then wraps around the base of the scapular spine to enter the spinoglenoid notch. Here, it passes beneath the spinoglenoid ligament (inferior transverse scapular ligament)—a fibrous band present in approximately 50% to 80% of individuals. The nerve is accompanied by the suprascapular artery and vein, which typically run superficial to the ligament.
Surgical Warning: The suprascapular nerve is relatively tethered at both the suprascapular and spinoglenoid notches. Excessive medial retraction of the infraspinatus during the posterior approach can cause iatrogenic traction injury to the nerve. Dissection must remain meticulous and strictly within the defined anatomical planes.
OPEN POSTERIOR SURGICAL APPROACH
The open posterior approach is executed through a combination of established techniques, primarily drawing from the foundational work of Post and Mayer, as well as Thompson, Schneider, and Kennedy.
Positioning and Preparation
- Patient Positioning: Place the patient in a semiprone (lateral decubitus with a slight anterior tilt) or full prone position. The lateral decubitus position is often preferred as it allows for simultaneous arthroscopic evaluation if deemed necessary.
- Arm Draping: The operative arm must be draped free to allow for full manipulation during the procedure. Internal rotation of the arm can help bring the posterior structures under tension, facilitating dissection.
- Landmark Identification: Palpate and mark the spine of the scapula, the acromion, and the posterior joint line.
Superficial Dissection: The Post and Mayer Technique
The initial exposure focuses on safely navigating the superficial muscular layers to access the scapular spine.
- Incision: Make a linear incision approximately 10 to 12 cm in length. The incision should run parallel and slightly cephalad (superior) to the spine of the scapula.
- Trapezius Elevation: Deepen the incision through the subcutaneous tissue to expose the deep fascia overlying the trapezius muscle. Sharply incise the fascia and elevate the trapezius muscle off the scapular spine.
- Hemostasis: The posterior shoulder is highly vascular. Utilize electrocautery meticulously to control bleeding from the muscular perforators.
- Retraction: Retract the trapezius superiorly and medially. Be highly cognizant of the spinal accessory nerve and the transverse cervical artery, which lie medial to the operative field; aggressive medial dissection must be avoided.
Deep Exposure and Decompression: The Thompson, Schneider, and Kennedy Technique
Once the scapular spine is cleared, the focus shifts to the infraspinatus and the spinoglenoid notch.
- Infraspinatus Detachment: Identify the infraspinatus muscle occupying the infraspinous fossa. Carefully detach the superior and medial origins of the infraspinatus muscle from the scapular body.
- Muscle Reflection: Reflect the infraspinatus muscle laterally and inferiorly (toward the vertebral border of the scapula, as described historically, though lateral reflection often provides better access to the notch). This maneuver exposes the posterior shoulder capsule and the posterior neck of the glenoid.
- Identification of the Spinoglenoid Notch: Palpate the base of the scapular spine laterally to locate the spinoglenoid notch.
- Ganglion Excision and Neurolysis:
- Carefully dissect through the fibro-fatty tissue within the notch to identify the suprascapular neurovascular bundle.
- Identify the ganglion cyst. It often presents as a bluish, tense, cystic structure.
- Meticulously dissect the ganglion cyst away from the suprascapular nerve. The primary objective is to leave the nerve entirely intact and uninjured.
- Trace the stalk of the cyst to its origin at the posterior glenohumeral joint capsule. Ligate or cauterize the stalk to minimize the risk of recurrence.
- If a hypertrophied spinoglenoid ligament is present and contributing to the compression, it should be carefully released.
Surgical Pitfall: Attempting to aggressively enucleate the cyst without first identifying the nerve can lead to catastrophic transection of the suprascapular nerve. Always identify the nerve proximally in normal tissue and trace it distally into the zone of compression.
THE ARTHROSCOPIC PARADIGM SHIFT
While the open posterior approach detailed above is a foundational orthopedic technique, it is imperative to acknowledge the modern evolution of treatment. More recently, arthroscopic treatment has become the preferred method for suprascapular nerve entrapment at the spinoglenoid notch when the etiology is a paralabral ganglion cyst.
Because these cysts almost universally result from intra-articular pathology—specifically a posterior labral tear or a posterior SLAP lesion—arthroscopy allows the surgeon to address the root cause of the problem.
The Arthroscopic Approach involves:
1. Diagnostic arthroscopy to identify the labral tear.
2. Capsulotomy adjacent to the tear to access the paralabral space.
3. Intra-articular decompression (marsupialization) of the ganglion cyst using a shaver.
4. Anatomical repair of the labral tear using suture anchors, thereby closing the "one-way valve" and preventing recurrence.
The open posterior approach is now generally reserved for cases where arthroscopic decompression fails, the cyst is exceptionally large and multiloculated extending far medially, or the pathology is non-cystic (e.g., a primary nerve sheath tumor or isolated spinoglenoid ligament entrapment without a labral tear).
POSTOPERATIVE REHABILITATION PROTOCOL
Postoperative care following an open posterior approach for suprascapular nerve decompression must balance the need to protect the reattached musculature (trapezius and infraspinatus) with the prevention of adhesive capsulitis.
Phase I: Immediate Postoperative (Weeks 0-2)
* Immobilization: The arm is placed in a standard shoulder sling for comfort.
* Range of Motion (ROM): Active motion of the elbow, wrist, and hand is encouraged immediately. Active-assisted and passive range of motion (PROM) of the shoulder is allowed within 10 to 14 days after surgery.
* Restrictions: Avoid active external rotation and active elevation to protect the healing infraspinatus and trapezius muscles.
Phase II: Intermediate Phase (Weeks 2-6)
* ROM: Active motion is gradually introduced and increased as pain permits. Focus on restoring full passive and active-assisted ROM.
* Strengthening: Begin gentle, submaximal isometric exercises for the deltoid and intact rotator cuff.
Phase III: Advanced Strengthening (Weeks 6-12+)
* Progression: Once full, painless ROM is achieved and the muscular reattachments are clinically healed (typically around 6 weeks), progressive isotonic strengthening is initiated.
* Targeted Therapy: Specific focus is placed on rehabilitating the infraspinatus. It is important to counsel the patient that while pain relief is often rapid following decompression, the return of infraspinatus muscle bulk and external rotation strength may take 6 to 12 months, depending on the chronicity of the preoperative nerve compression.
COMPLICATIONS AND SURGICAL PITFALLS
- Incomplete Decompression: Failure to fully trace the cyst to its articular origin or failure to release a tight spinoglenoid ligament can result in persistent symptoms.
- Cyst Recurrence: If the underlying labral tear is not addressed (a limitation of the isolated open approach without concurrent arthroscopy), the cyst may recur.
- Iatrogenic Nerve Injury: The suprascapular nerve is highly vulnerable during the deep dissection phase. Excessive traction or errant use of electrocautery near the spinoglenoid notch can cause permanent denervation.
- Hematoma Formation: The posterior musculature is highly vascular. Inadequate hemostasis during the elevation of the trapezius or infraspinatus can lead to a postoperative hematoma, increasing the risk of infection and delaying rehabilitation. Careful layered closure over a surgical drain is recommended in cases of extensive dead space.
You Might Also Like