Posterior Surgical Approach for Quadrilateral Space Syndrome and Suprascapular Nerve Entrapment
Key Takeaway
Quadrilateral Space Syndrome (QSS) involves the compression of the axillary nerve and posterior circumflex humeral artery within the quadrilateral space. Diagnosis relies on clinical suspicion, MRI, and electromyography. Surgical decompression via a posterior approach, utilizing the Cahill and Palmer technique, is indicated for refractory cases. This involves releasing fibrous bands tethering the neurovascular bundle between the teres minor, teres major, and the long head of the triceps.
INTRODUCTION TO SHOULDER NERVE ENTRAPMENT SYNDROMES
Peripheral nerve entrapment around the shoulder girdle presents a complex diagnostic and therapeutic challenge for the orthopaedic surgeon. Among the most clinically significant, yet frequently underdiagnosed, conditions are Quadrilateral Space Syndrome (QSS) and Suprascapular Nerve Entrapment. Both pathologies manifest with vague, poorly localized shoulder pain, often accompanied by insidious muscle weakness and atrophy that can severely compromise upper extremity function, particularly in overhead athletes and manual laborers.
This comprehensive surgical guide details the intricate pathoanatomy, clinical evaluation, and operative management of these entrapment neuropathies, with a specific focus on the posterior surgical approach for Quadrilateral Space Syndrome utilizing the classic Cahill and Palmer technique.
PATHOPHYSIOLOGY AND APPLIED ANATOMY
Quadrilateral Space Syndrome (QSS)
The quadrilateral space is an anatomic interval in the posterior shoulder. Its boundaries are strictly defined by the surrounding musculotendinous and osseous structures:
* Superiorly: The inferior border of the teres minor muscle and the posterior margin of the glenoid, with fibrous extensions to the posterior glenohumeral capsule.
* Inferiorly: The superior border of the teres major muscle.
* Medially: The lateral border of the long head of the triceps brachii.
* Laterally: The surgical neck of the humerus.
The space serves as the primary conduit for the axillary nerve and the posterior circumflex humeral artery (PCHA) as they exit the axilla to supply the deltoid and teres minor muscles.
Pathologically, QSS occurs when these neurovascular structures are compressed within this confined interval. The compression is most frequently dynamic. The fibrous bands extending from the margin of the glenoid to the posterior glenohumeral capsule tighten significantly during cross-body adduction and internal rotation. This biomechanical tethering compresses the axillary nerve against the muscular boundaries, leading to ischemia, perineural edema, and eventual neuropraxia or axonotmesis.
Biomechanical Pearl: The axillary nerve is most vulnerable to compression when the arm is placed in abduction and external rotation (the late cocking phase of throwing), or in extreme cross-body adduction and internal rotation, which maximally stretches the posterior capsular structures and tightens the anomalous fibrous bands within the space.
Suprascapular Nerve Entrapment
The suprascapular nerve is a mixed motor and sensory nerve derived from the upper trunk of the brachial plexus, formed by the ventral rami of the C5 and C6 nerve roots at Erb's point.
Anatomical Course:
1. The nerve courses laterally and posteriorly, running parallel to the omohyoid muscle, dorsal to the brachial plexus, and deep to the trapezius muscle.
2. It reaches the superior edge of the scapula and passes through the suprascapular notch. The morphology of this notch is highly variable (ranging from a wide U-shape to a narrow V-shape or even a complete bony foramen).
3. The transverse scapular ligament forms the unyielding roof of the suprascapular notch.
4. After traversing the notch, the nerve provides motor branches to the supraspinatus muscle and sensory branches to the shoulder capsule, as well as the glenohumeral and acromioclavicular joints.
5. The nerve then courses laterally and inferiorly, turning around the lateral margin of the scapular spine (the spinoglenoid notch) to provide terminal motor innervation to the infraspinatus muscle.
Sites of Compression:
Most suprascapular nerve entrapments occur at the suprascapular notch. A narrow V-shaped notch or a calcified transverse scapular ligament significantly increases the risk of impingement.
Alternatively, compression can occur distally at the spinoglenoid notch. Here, the nerve may be tethered by the spinoglenoid ligament (also known as the inferior transverse scapular ligament), which arises from the lateral aspect of the root of the scapular spine and inserts at the posterior glenoid margin. Furthermore, space-occupying lesions such as lipomas or ganglion cysts frequently compress the inferior branch of the nerve at this location.
Surgical Warning: Ganglion cysts at the spinoglenoid notch are rarely isolated anomalies; they are almost universally the result of a one-way valve effect from intraarticular pathology, most commonly a posterior labral tear. Addressing the cyst without repairing the underlying labral defect will lead to a high rate of recurrence.
CLINICAL EVALUATION AND DIAGNOSTICS
Patient Presentation
Patients with QSS typically present with deep, aching, diffuse posterior shoulder pain that is exacerbated by overhead activities or prolonged positioning in abduction and external rotation. They may complain of subjective weakness in external rotation and abduction. Muscle atrophy of the teres minor (and occasionally the deltoid) may or may not be clinically apparent.
In contrast, suprascapular nerve entrapment presents differently depending on the site of compression:
* Suprascapular Notch Entrapment: Causes deep, poorly localized posterior shoulder pain, accompanied by weakness and atrophy of both the supraspinatus and infraspinatus muscles.
* Spinoglenoid Notch Entrapment: Often presents as painless weakness. Painless atrophy of the infraspinatus is a hallmark sign of isolated compression at the spinoglenoid notch.
Diagnostic Modalities
Electromyography (EMG) and Nerve Conduction Studies (NCS):
EMG is the gold standard for confirming the diagnosis of both QSS and suprascapular neuropathy. However, for QSS, the diagnosis may only be confirmed on EMG if the surgeon explicitly alerts the electromyographer to the physical findings and the proposed diagnosis. The electromyographer must specifically test the teres minor and deltoid muscles, which are often overlooked in routine upper extremity screens.
Magnetic Resonance Imaging (MRI):
MRI is invaluable for identifying space-occupying lesions (e.g., ganglion cysts, lipomas) compressing the suprascapular nerve at the spinoglenoid notch. It is also highly sensitive for detecting denervation edema (acute phase) or fatty infiltration and atrophy (chronic phase) in the affected musculature. In QSS, MRI may show isolated fatty atrophy of the teres minor.
Magnetic Resonance Angiography (MRA):
For QSS, MRA or conventional angiography can demonstrate dynamic occlusion of the posterior circumflex humeral artery when the arm is placed in abduction and external rotation (the ABER position).
SURGICAL INDICATIONS
Surgical intervention is indicated in patients who have failed a comprehensive non-operative rehabilitation program (typically 3 to 6 months of physical therapy, NSAIDs, and activity modification) and possess clear clinical, electromyographic, or advanced imaging evidence of nerve entrapment.
POSTERIOR SURGICAL APPROACH FOR QUADRILATERAL SPACE SYNDROME (CAHILL AND PALMER TECHNIQUE)
The posterior approach to the quadrilateral space, popularized by Cahill and Palmer, provides direct visualization of the axillary nerve and posterior circumflex humeral artery, allowing for the meticulous release of tethering fibrous bands.
Step 1: Patient Positioning and Preparation
The patient is placed in the lateral decubitus position with the operative arm draped free. A beanbag or pegboard is used to secure the torso. The arm is supported by a sterile hydraulic arm holder, allowing the surgeon to dynamically manipulate the limb during the procedure to assess the tension on the neurovascular structures. Alternatively, the prone position can be utilized based on surgeon preference.
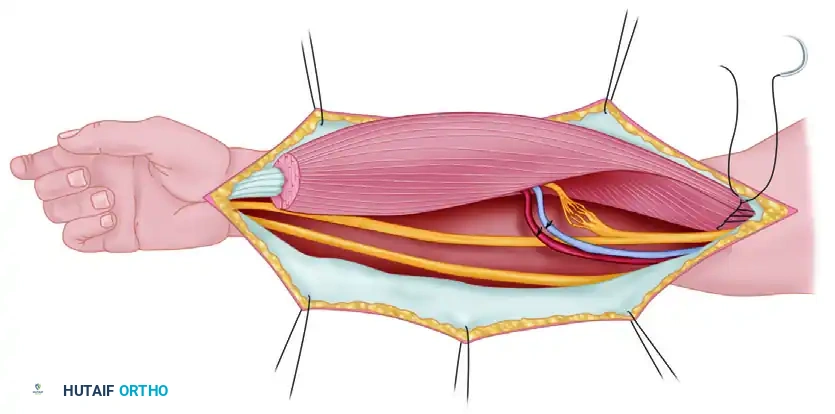
Step 2: Skin Incision
A transverse or gently curved longitudinal incision is made over the posterior aspect of the shoulder, centered over the palpable interval between the posterior border of the deltoid and the teres minor.
Figure 1: Skin incision for the posterior surgical approach to the quadrilateral space.
Step 3: Superficial Dissection and Deltoid Retraction
Subcutaneous tissues are sharply dissected to expose the deep fascia overlying the deltoid muscle. The posterior border of the deltoid is identified. The fascia is incised, and a blunt retractor (such as a Richardson or a specialized deltoid retractor) is placed under the inferior border of the deltoid. The deltoid is gently reflected superiorly and laterally to expose the underlying short external rotators.
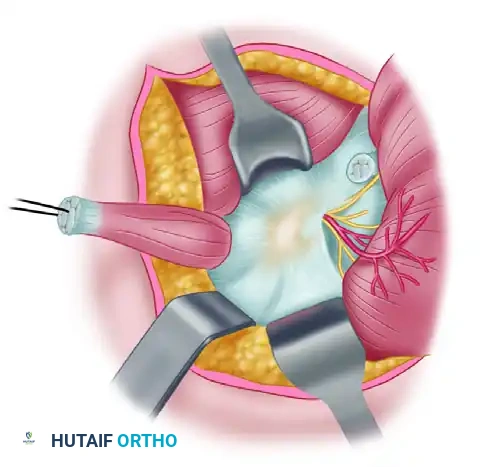
Figure 2: Retractor placed under the border of the deltoid, reflecting it to expose the underlying musculature.
Step 4: Identification of the Quadrilateral Space
With the deltoid retracted, the anatomical boundaries of the quadrilateral space are identified. The teres minor is visualized superiorly, the teres major inferiorly, and the long head of the triceps medially. The surgical neck of the humerus forms the lateral boundary.
Surgical Pitfall: Care must be taken not to confuse the teres minor with the infraspinatus. The teres minor is located more inferiorly and has a distinct fascial separation from the infraspinatus.
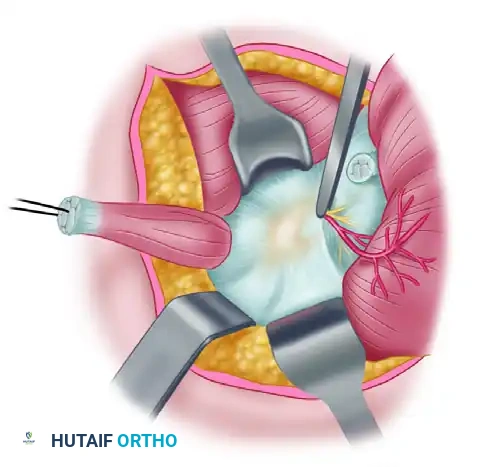
Step 5: Decompression and Release of Fibrous Bands
The teres minor is gently mobilized. A traction suture may be placed into the teres minor to retract it superiorly, enhancing visualization of the space. The neurovascular bundle (axillary nerve and posterior circumflex humeral artery) is identified as it exits the space.
Anomalous fibrous bands are typically found traversing the quadrilateral space, tethering the neurovascular bundle to the teres major, the long head of the triceps, or the posterior glenohumeral capsule. A right-angle clamp is carefully passed beneath these fibrous bands to isolate them from the underlying nerve and artery.
Figure 3: The teres minor is held by a suture on the left (with the circular area on the right representing the insertion of the teres minor). A clamp holds the fibrous bands traversing the quadrilateral space that tether the neurovascular bundle. The deltoid is reflected to the right.
Step 6: Completion of Dissection
The isolated fibrous bands are sharply resected. The surgeon must ensure that the axillary nerve is completely free from compression throughout its course within the quadrilateral space. The arm is taken through a full range of motion, specifically cross-body adduction and internal rotation, to confirm that no dynamic tethering remains.
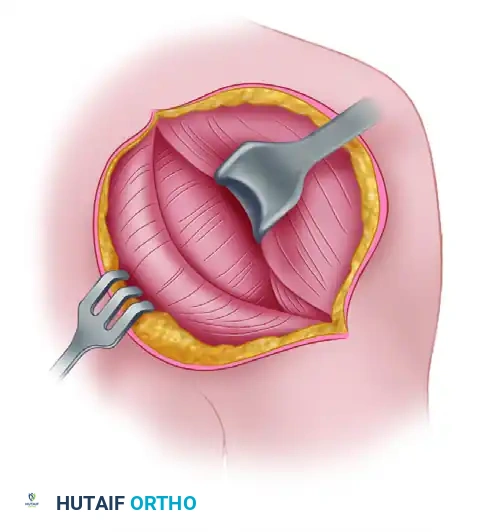
Figure 4: Dissection is complete. The fibrous bands have been meticulously dissected away from the neurovascular bundle, ensuring complete decompression of the axillary nerve and posterior circumflex humeral artery.
Step 7: Closure
The wound is irrigated copiously with sterile saline. Hemostasis is achieved using bipolar electrocautery to avoid thermal injury to the axillary nerve. The deltoid fascia is loosely reapproximated, and the subcutaneous tissue and skin are closed in a layered fashion. A sterile dressing is applied.
SURGICAL MANAGEMENT OF SUPRASCAPULAR NERVE ENTRAPMENT
While the focus of this text is the posterior approach for QSS, it is imperative to understand the surgical principles for suprascapular nerve entrapment, as the clinical presentations often overlap.
Suprascapular Notch Decompression
For entrapment at the suprascapular notch, an open superior approach or an arthroscopic approach can be utilized. The goal is the complete transection of the transverse scapular ligament.
1. The trapezius is split in line with its fibers.
2. The supraspinatus is retracted posteriorly to expose the notch.
3. The suprascapular artery (which typically runs over the ligament) is protected, and the ligament (running over the nerve) is excised.
Spinoglenoid Notch Decompression
For entrapment at the spinoglenoid notch, usually secondary to a ganglion cyst, an arthroscopic approach is currently the gold standard.
1. Diagnostic arthroscopy is performed to identify the posterior labral tear.
2. The capsulolabral junction is opened, allowing intra-articular drainage of the paralabral cyst.
3. The labrum is then anatomically repaired using suture anchors to eliminate the one-way valve mechanism, preventing cyst recurrence.
4. If the spinoglenoid ligament is hypertrophied and causing direct compression, it can be released arthroscopically or via a limited open posterior approach.
POSTOPERATIVE REHABILITATION PROTOCOL
Successful outcomes following nerve decompression rely heavily on a structured, phased rehabilitation program.
Phase I: Protection and Healing (Weeks 0-2)
* The patient is placed in a standard shoulder sling for comfort.
* Immediate initiation of active range of motion (ROM) for the elbow, wrist, and hand.
* Pendulum exercises and gentle passive ROM of the shoulder are permitted within pain-free limits.
* Avoid aggressive cross-body adduction and internal rotation to prevent stress on the healing posterior tissues.
Phase II: Early Motion (Weeks 2-6)
* Discontinue the sling.
* Progress to active-assisted and active ROM exercises.
* Initiate periscapular strengthening and isometric exercises for the rotator cuff and deltoid.
* Focus on restoring normal scapulothoracic kinematics.
Phase III: Strengthening and Return to Activity (Weeks 6-12+)
* Advance to isotonic strengthening of the rotator cuff, deltoid, and periscapular stabilizers.
* Incorporate proprioceptive and neuromuscular control drills.
* For overhead athletes, initiate a progressive throwing or sport-specific interval program around 10-12 weeks, provided full, painless ROM and symmetric strength have been achieved.
* Maximal nerve recovery and muscle hypertrophy may take up to 12 to 18 months post-decompression.
COMPLICATIONS AND SURGICAL PITFALLS
While surgical decompression is highly effective, several complications must be avoided:
- Iatrogenic Nerve Injury: The axillary nerve is highly susceptible to traction injury during deltoid retraction or thermal injury from indiscriminate use of electrocautery. Meticulous, blunt dissection and the use of bipolar cautery are mandatory.
- Incomplete Release: Failure to identify and resect all anomalous fibrous bands within the quadrilateral space will lead to persistent dynamic compression and failure of symptom resolution. Dynamic intraoperative testing is crucial.
- Hematoma Formation: The posterior circumflex humeral artery and its accompanying venous plexus are fragile. Meticulous hemostasis must be achieved prior to closure to prevent a postoperative hematoma, which could cause secondary compressive neuropathy.
- Misdiagnosis: Operating on the quadrilateral space when the primary pathology is cervical radiculopathy (C5/C6), Parsonage-Turner syndrome (brachial neuritis), or an undiagnosed posterior labral tear will result in poor clinical outcomes. A rigorous preoperative diagnostic workup is non-negotiable.
📚 Medical References
- Quadrilateral space syndrome, J Hand Surg 8:65, 1983.
- Calvert PT, Packer NP, Stoker DJ, et al: Arthrography of the shoulder after operative repair of the torn rotator cuff, J Bone Joint Surg 68B:147, 1986.
- Chan KC, Burkhart SS: How to switch posts without rethreading when tying half-hitches, Arthroscopy 15:444, 1999.
- Chang EY, Moses DA, Babb JS, et al: Shoulder impingement: objective 3D shape analysis of acromial morphologic features, Radiology 239:497, 2006.
- Chen AL, Rokito AS, Zuckerman JD: The role of the
You Might Also Like