Mastering Shoulder Impingement and Anterior Acromioplasty: A Comprehensive Surgical Guide
Key Takeaway
Shoulder impingement syndrome represents a spectrum of rotator cuff pathology, ranging from reversible edema to full-thickness tendon tears. Accurate diagnosis relies on comprehensive clinical evaluation and targeted imaging, including Grashey and supraspinatus outlet views. When conservative management fails, anterior acromioplasty remains a cornerstone of surgical intervention. This guide details the biomechanics, acromial morphology, and step-by-step surgical technique for open anterior acromioplasty to optimize patient outcomes and restore glenohumeral kinematics.
DIAGNOSTIC IMAGING IN SHOULDER PATHOLOGY
The initial evaluation of a patient presenting with shoulder pain mandates a systematic and comprehensive radiographic series. Plain radiographs remain the cornerstone of initial diagnostic imaging and must be obtained in at least two orthogonal planes. A standard comprehensive shoulder series should include an anteroposterior (AP) view, an axillary lateral view, and a supraspinatus outlet view.
Plain Radiography Techniques and Indications
Anteroposterior radiographs can be captured with the glenohumeral joint in neutral, internal rotation, or external rotation, each offering distinct diagnostic advantages:
* Internal Rotation AP View: Highly sensitive for detecting Hill-Sachs lesions (posterolateral humeral head impaction fractures) associated with anterior glenohumeral instability.
* External Rotation AP View: Provides an optimal profile of the greater tuberosity. In skeletally immature patients, it is invaluable for assessing the proximal humeral physis.
* True AP (Grashey) View: Obtained by rotating the patient 30 to 45 degrees toward the affected side, aligning the beam perpendicular to the glenoid fossa. This view eliminates the overlap of the humeral head and glenoid, providing the most accurate assessment of the glenohumeral articular cartilage and joint space narrowing.
Clinical Pearl: The Grashey view is indispensable for diagnosing early glenohumeral osteoarthritis, as standard AP views often falsely project a preserved joint space due to the natural anteversion of the glenoid.
The axillary lateral view is critical for evaluating the spatial relationship of the glenohumeral joint, ruling out subtle posterior or anterior dislocations. Furthermore, it delineates the anatomy of the glenoid rim (assessing for bony Bankart lesions), the acromion, the coracoid process, and the proximal humerus.
The supraspinatus outlet view (a true lateral view of the scapula with the radiographic tube angled 10 to 15 degrees caudad) is essential for evaluating patients with suspected rotator cuff disease. This projection profiles the coracoacromial arch, allowing the surgeon to classify acromial morphology and identify subacromial spurring that may contribute to extrinsic impingement.
Ultrasonography in Rotator Cuff Evaluation
Dynamic high-resolution ultrasound scanning has emerged as a powerful, noninvasive, and cost-effective modality for evaluating the rotator cuff. Current literature reports a sensitivity ranging from 58% to 100%, a specificity of 85% to 100%, and an overall diagnostic accuracy of 80% to 94% in the detection of full-thickness rotator cuff tears.
Advantages of ultrasonography include its rapid acquisition, lack of ionizing radiation, and the ability to perform dynamic assessments. Dynamic ultrasound is particularly useful for confirming subacromial impingement in real-time, assessing glenohumeral capsular laxity, and identifying biceps tendon subluxation or tenosynovitis.
Diagnostic Pitfall: The primary limitation of ultrasonography is its steep learning curve. The accuracy of the scan is highly operator-dependent and relies heavily on the quality of the transducer and the experience of the musculoskeletal ultrasonographer.
PATHOPHYSIOLOGY OF IMPINGEMENT SYNDROME
The conceptual understanding of impingement syndrome has evolved significantly since Jarjavay’s initial description of subacromial bursitis in 1867. In 1931, E.A. Codman revolutionized shoulder pathology by noting that the inability to abduct the arm was frequently caused by incomplete or complete ruptures of the supraspinatus tendon, rather than isolated bursal inflammation.
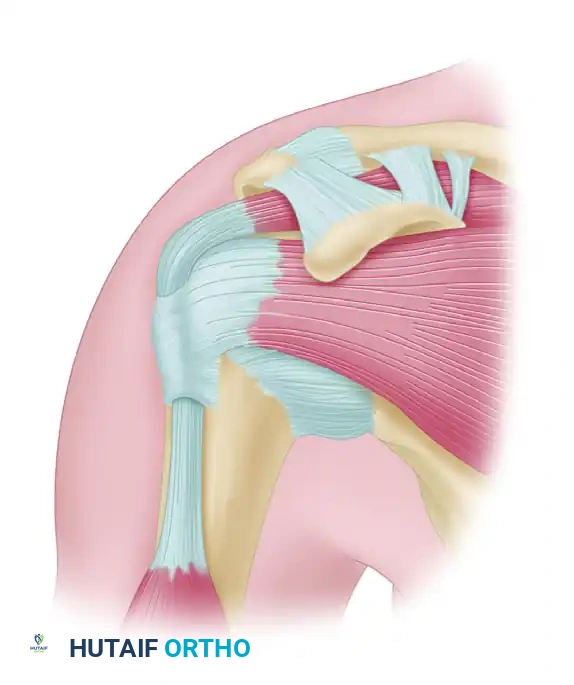
In 1972, Charles Neer introduced the modern concept of impingement syndrome. He characterized it as a mechanical conflict caused by a ridge of proliferative spurs and excrescences on the undersurface of the anterior process of the acromion. This abutment is exacerbated by repeated impingement of the rotator cuff and the humeral head against the coracoacromial arch during forward elevation and internal rotation.
Figure 46-3: Impingement syndrome. The supraspinatus tendon is visualized passing directly beneath the rigid coracoacromial arch, highlighting the anatomical bottleneck susceptible to mechanical compression.
Neer identified that the anterior third of the acromion and its anterior lip were the primary offending structures. He subsequently introduced the concept of a pathological continuum, categorizing impingement syndrome into three distinct developmental stages.
Neer’s Developmental Stages of Impingement Syndrome
Stage 1: Edema and Hemorrhage
* Typical Age: < 25 years old.
* Pathology: Reversible inflammatory changes within the tendon and bursa resulting from excessive overhead activity.
* Differential Diagnosis: Glenohumeral subluxation, acromioclavicular joint pathology.
* Clinical Course: Reversible with rest and rehabilitation.
* Treatment: Strictly conservative (rest, NSAIDs, physical therapy).
Stage 2: Fibrosis and Tendinitis
* Typical Age: 25 to 40 years old.
* Pathology: Repeated mechanical inflammation leads to irreversible fibrotic changes and thickening of the subacromial bursa and rotator cuff tendons.
* Differential Diagnosis: Adhesive capsulitis (frozen shoulder), calcific tendinitis.
* Clinical Course: Recurrent pain with overhead activity; refractory to prolonged rest.
* Treatment: Extended conservative management; operative intervention (bursectomy or division of the coracoacromial ligament) may be considered if refractory.
Stage 3: Bone Spurs and Tendon Rupture
* Typical Age: > 40 years old.
* Pathology: Chronic mechanical wear leads to partial or full-thickness rotator cuff tears, biceps tendon lesions, and structural bony alterations (acromial spurring).
* Differential Diagnosis: Cervical radiculopathy, glenohumeral osteoarthritis, occult neoplasm.
* Clinical Course: Progressive disability, weakness, and night pain.
* Treatment: Surgical intervention (anterior acromioplasty, rotator cuff repair).
CLASSIFICATIONS OF IMPINGEMENT
Since Neer’s seminal work, the taxonomy of impingement has expanded to encompass four distinct pathophysiological entities:
1. Primary Impingement (Extrinsic vs. Intrinsic)
Primary impingement occurs in the absence of underlying glenohumeral instability. It is subdivided into:
* Extrinsic Impingement: Occurs when the subacromial space is physically diminished. Causes include subacromial spurring, a pathological os acromiale, malunited acromial fractures, or inferiorly projecting osteophytes from the acromioclavicular (AC) joint.
* Intrinsic Impingement: Occurs when the structures passing beneath the arch become pathologically enlarged. Examples include intratendinous calcium deposits, profound bursal hypertrophy, or intrinsic degenerative thickening of the rotator cuff tendons.
2. Secondary Impingement
Secondary impingement is a byproduct of underlying glenohumeral instability. Microinstability or capsular laxity allows abnormal translation of the humeral head (typically anteriorly or superiorly), resulting in secondary contact of the rotator cuff against the coracoacromial arch. This is frequently observed in young, overhead athletes.
3. Subcoracoid Impingement
First described by Goldthwait in 1909, this involves painful contact between the subscapularis/rotator cuff and the coracoid process. It is often iatrogenic (e.g., following a Trillat osteotomy for anterior instability) but can be idiopathic due to a prominent coracoid. Diagnosis relies on a positive coracoid impingement test and CT imaging demonstrating a coracohumeral distance of less than 6.8 mm.
4. Internal Impingement
Predominantly affecting throwing athletes, internal impingement occurs when the articular surface of the posterior rotator cuff abuts the posterosuperior glenoid labrum. This occurs in the late-cocking phase of throwing (extreme abduction and external rotation). It is strongly associated with Glenohumeral Internal Rotation Deficit (GIRD). Treatment focuses heavily on posterior capsular stretching before considering surgical intervention.
ACROMIAL MORPHOLOGY AND BIOMECHANICS
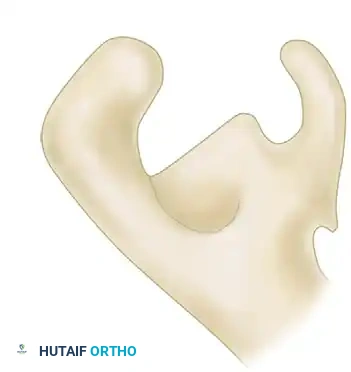
Acromial morphology plays a critical role in the pathogenesis of extrinsic impingement. Bigliani, Morrison, and April famously classified the acromion into three distinct morphological types based on the supraspinatus outlet view.
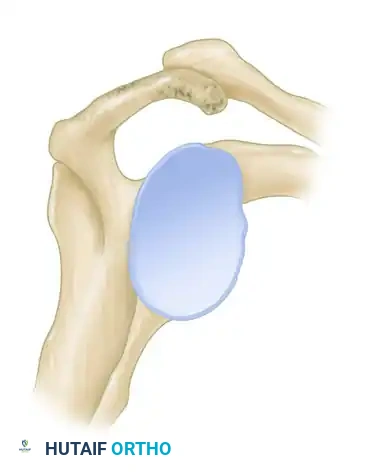
Figure 46-4 (Type I): A flat acromion with minimal compromise of the supraspinatus outlet. Associated with the lowest risk of rotator cuff pathology.
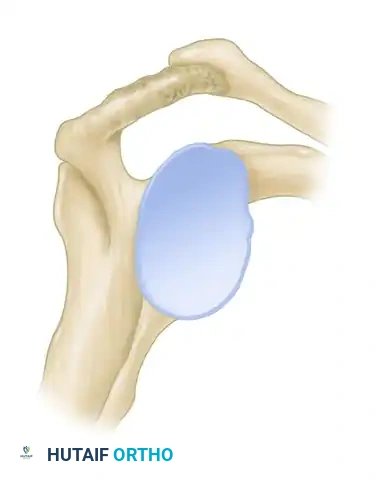
Figure 46-4 (Type II): A curved acromion that parallels the contour of the humeral head, moderately reducing the subacromial space.
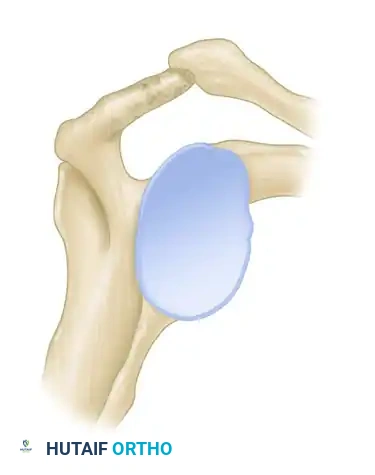
Figure 46-4 (Type III): A hooked acromion with a prominent anterior-inferior projection. This morphology severely compromises the supraspinatus outlet.
Cadaveric studies have demonstrated a profound correlation between acromial morphology and rotator cuff integrity. In a landmark study of 140 shoulders, 73% of all full-thickness rotator cuff tears were found in shoulders possessing a Type III (hooked) acromion. Patients with a decreased acromial slope are inherently predisposed to subacromial stenosis and subsequent mechanical attrition of the underlying tendons.
The Intrinsic Degeneration Theory
While mechanical abutment is a proven factor, contemporary literature also heavily supports the intrinsic degeneration theory. Senescence of tendon fibroblasts leads to age-related disruption of tendon architecture. Histological studies of aging rotator cuffs reveal decreased cellularity, fascicular thinning, accumulation of granulation tissue, and dystrophic calcification.
Furthermore, the "critical zone" of the supraspinatus (approximately 1 cm proximal to its insertion on the greater tuberosity) exhibits relative hypovascularity. Differential shear stresses within the tendon layers, combined with this poor blood supply, precipitate fiber failure. As intrinsic degeneration progresses, the rotator cuff force couples fail, leading to uninhibited superior translation of the humeral head by the deltoid, thereby causing secondary mechanical impingement.
SURGICAL MANAGEMENT: ANTERIOR ACROMIOPLASTY
When a well-executed nonoperative regimen (comprising NSAIDs, targeted physical therapy, and a maximum of two subacromial corticosteroid injections) fails after 3 to 6 months, surgical intervention is indicated.
Arthroscopic or open anterior acromioplasty remains the gold standard for structural impingement syndrome. Historical data from large series of open acromioplasties demonstrate an overall success rate of approximately 85%.
Surgical Warning: Failures in acromioplasty are most frequently attributed to diagnostic errors (e.g., missed cervical radiculopathy, unrecognized instability, or adhesive capsulitis) or technical inadequacy. Inadequate bone resection, particularly failing to remove the anterior lip and the bone anterior to the clavicular border, will result in persistent outlet stenosis.
Core Principles of Neer’s Acromioplasty
Whether performed open or arthroscopically, the procedure must adhere to Neer's original biomechanical principles:
1. Release of the Coracoacromial Ligament: The ligament should be released from the acromion. Note: Complete resection is currently losing favor. Preserving the ligament allows it to heal back to the acromion, preventing anterosuperior escape of the humeral head in cases of massive, irreparable rotator cuff tears.
2. Resection of the Anterior Lip: Removal of the anterior-inferior hooked portion of the acromion.
3. Lateral Edge Contouring: Smoothing the lateral edge to prevent secondary abrasion.
4. Distal Clavicle Excision (if indicated): Removal of the distal 1 to 1.5 cm of the clavicle if concomitant, symptomatic AC joint osteoarthritis is present.
SURGICAL TECHNIQUE 46-1: OPEN ANTERIOR ACROMIOPLASTY
Preoperative Setup and Positioning
- Anesthesia: Administer general endotracheal anesthesia, ideally supplemented with an interscalene regional block for optimal postoperative pain control.
- Positioning: Place the patient in a semi-upright beach chair position, with the head elevated 30 to 35 degrees.
- Stabilization: Place a towel roll or an intravenous fluid bag medial to the scapula to stabilize the shoulder girdle. This specific degree of head elevation positions the superior acromial surface parallel to the floor, providing an intuitive spatial reference for the acromial osteotomy.
- Preparation: Drape the arm free using a sterile U-drape to permit full, unhindered glenohumeral rotation during the procedure.
Incision and Superficial Dissection
- Landmark Identification: Use a sterile surgical marker to outline the bony contours of the shoulder: the lateral acromial border, the coracoid process, the AC joint, and the distal clavicle.
- Incision Planning: Outline a 4 to 6 cm skin incision along Langer’s lines. Infiltrate the planned incision site with 10 mL of 1:500,000 epinephrine solution to induce local vasoconstriction and minimize dermal bleeding.
- Skin Incision: Make the incision starting from the lateral aspect of the anterior acromion, extending medially toward the coracoid process.
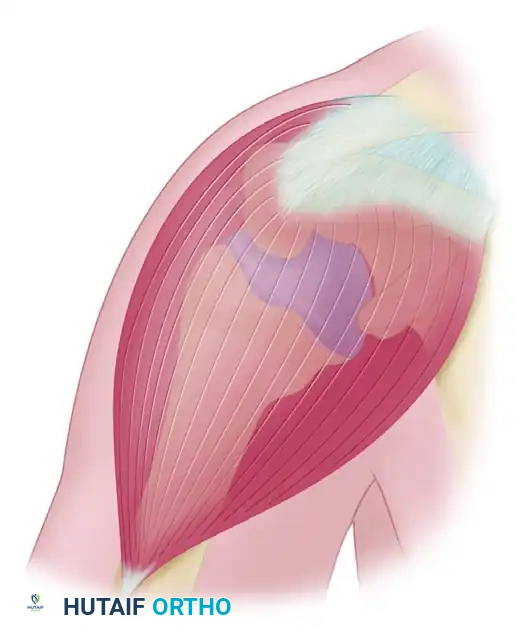
Figure 46-5: Anterior acromioplasty approach. The skin incision is made within the skin lines across the anterior corner of the acromion. The underlying acromion is exposed via a precise incision in the tendinous raphe between the anterior and middle heads of the deltoid.
Deep Dissection and Deltoid Management
- Subcutaneous Mobilization: Elevate the subcutaneous tissues to expose the underlying deltoid fascia.
- Identifying the Raphe: Carefully identify the avascular tendinous raphe separating the anterior and middle thirds of the deltoid muscle.
- Deltoid Split: Split the deltoid distally along this raphe for no more than 3 to 4 cm to avoid iatrogenic injury to the terminal branches of the axillary nerve.
- Deltoid Detachment: Using electrocautery, carefully detach the anterior deltoid origin from the anterior lip of the acromion. Leave a robust cuff of fibro-tendinous tissue attached to the acromion to facilitate a secure, anatomic repair during closure.
The Acromioplasty
- Ligament Release: Identify the coracoacromial ligament inserting onto the undersurface of the anterior acromion. Release it sharply from its bony attachment.
- Subacromial Inspection: Insert a blunt retractor to depress the humeral head. Inspect the subacromial bursa and excise any hypertrophic bursal tissue to visualize the underlying supraspinatus tendon.
- Osteotomy: Using a broad osteotome or an oscillating microsaw, perform the anterior acromioplasty. The cut should begin at the anterior lip and angle posteriorly, removing the anterior-inferior prominence (the "hook").
- Contouring: Ensure that the resection extends medially to include the portion of the acromion anterior to the anterior border of the clavicle. Use a motorized burr or a rasp to smooth the undersurface, ensuring a flat, Type I morphology.
- Cuff Inspection: Rotate the arm through a full range of motion to ensure the impingement has been completely eradicated and to inspect the rotator cuff for occult tears.
Closure
- Irrigation: Copiously irrigate the subacromial space to remove all bone debris, which could otherwise lead to heterotopic ossification.
- Deltoid Repair: This is the most critical step of the closure. Reattach the anterior deltoid firmly to the acromion using heavy, non-absorbable transosseous sutures (e.g., #2 FiberWire). A secure repair is mandatory to prevent postoperative deltoid dehiscence.
- Superficial Closure: Close the subcutaneous layer with absorbable sutures and the skin with a subcuticular stitch or surgical staples.
POSTOPERATIVE PROTOCOL
- Phase I (0-2 Weeks): The patient is placed in a standard shoulder sling for comfort. Passive range of motion (PROM) exercises, including pendulum exercises, are initiated immediately to prevent adhesive capsulitis. Active use of the hand and elbow is encouraged.
- Phase II (2-6 Weeks): Sling is discontinued. Active-assisted range of motion (AAROM) progresses to active range of motion (AROM). Avoid heavy active forward elevation to protect the deltoid repair.
- Phase III (6-12 Weeks): Progressive isotonic strengthening of the rotator cuff and periscapular stabilizers begins.
- Phase IV (3-6 Months): Return to full, unrestricted occupational and athletic activities once symmetric strength and painless, full range of motion are achieved.
📚 Medical References
You Might Also Like