Operative Orthopaedics: Comprehensive Surgical Anatomy and Biomechanics of the Wrist
Key Takeaway
A profound understanding of wrist surgical anatomy and biomechanics is the cornerstone of operative orthopedics. This comprehensive guide details the intricate osseous architecture, capsuloligamentous stabilizers, and vascular networks of the carpus. Designed for orthopedic residents and consultants, it explores the triangular fibrocartilage complex (TFCC), intrinsic and extrinsic ligaments, and kinematic principles essential for executing precise surgical approaches and optimizing patient outcomes in complex wrist disorders.
Introduction to Wrist Surgical Anatomy
The wrist is an anatomically and biomechanically complex transition zone between the forearm and the hand, engineered to provide both multi-planar mobility and rigid stability for grip and prehension. For the operative orthopedic surgeon, a profound, three-dimensional understanding of the distal radioulnar joint (DRUJ), radiocarpal joint, ulnocarpal joint, and the intricate intercarpal articulations is mandatory.
This masterclass synthesizes the foundational anatomical, biomechanical, and kinematic principles of the wrist. It bridges the gap between textbook anatomy and the practical realities of the operating theater, detailing surgical approaches, ligamentous preservation techniques, and evidence-based postoperative protocols.
Osseous Architecture and Articulations
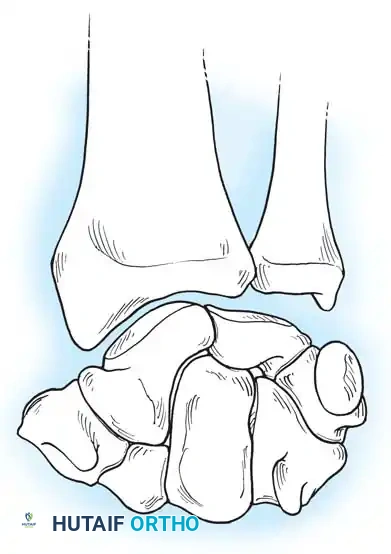
The osseous framework of the wrist comprises the distal radius, the distal ulna, and eight carpal bones arranged into two distinct rows.
The proximal carpal row consists of the scaphoid, lunate, triquetrum, and pisiform. This row acts as an intercalated segment; it has no direct tendinous insertions (with the exception of the flexor carpi ulnaris on the pisiform) and moves entirely in response to mechanical forces exerted by the surrounding articular contours and ligamentous tethers.
The distal carpal row includes the trapezium, trapezoid, capitate, and hamate. These bones are tightly bound to each other and to the metacarpal bases, forming a rigid functional unit that moves synchronously with the hand.
The radiocarpal joint is formed by the articulation of the biconcave distal radius (scaphoid and lunate fossae) with the convex proximal surfaces of the scaphoid and lunate. The triquetrum articulates proximally with the triangular fibrocartilage complex (TFCC) rather than the distal ulna directly.
Clinical Pearl: Viegas has emphasized the considerable anatomical variation found in the fourth carpometacarpal articulation, as well as the scaphotrapeziotrapezoid (STT), capitolunate, and hamatolunate articulations. Recognizing these morphological variants (e.g., a Type II lunate with a medial hamate facet) is critical, as they alter normal wrist kinematics and predispose patients to specific degenerative patterns, such as hamatolunate arthrosis.
The Triangular Fibrocartilage Complex (TFCC)
The distal ulna articulates with the radius at the sigmoid notch, accommodating the ulnar head through approximately two-thirds of its rotational arc. The distal ulna is inclined at approximately 20 degrees relative to the radius.
Separating the hyaline cartilage-covered ulnar head from the carpus is the TFCC, a critical chondroligamentous stabilizer first comprehensively described by Palmer and Werner. The TFCC is the primary stabilizer of the DRUJ and the ulnar carpus.
Components of the TFCC
The TFCC is a multi-structural complex comprising:
* The Articular Disc (TFC proper): A biconcave fibrocartilaginous structure that absorbs axial loads (transmitting approximately 20% of the axial load across the wrist).
* Dorsal and Volar Radioulnar Ligaments: The primary stabilizers of the DRUJ during pronation and supination.
* Meniscus Homologue: A reflection of fibrous tissue extending from the dorsal radius to the volar carpus.
* Ulnar Collateral Ligament (UCL): Extending from the ulnar styloid to the pisiform and triquetrum.
* Extensor Carpi Ulnaris (ECU) Subsheath: Intimately blended with the dorsal aspect of the TFCC.
* Ulnolunate and Ulnotriquetral Ligaments: Volar extrinsic ligaments that prevent volar subluxation of the ulnar carpus.
Surgical Warning: When performing ulnar-sided surgical approaches or arthroscopy, extreme care must be taken to preserve the foveal attachments of the radioulnar ligaments. Disruption here leads to profound DRUJ instability that cannot be salvaged merely by repairing the articular disc.
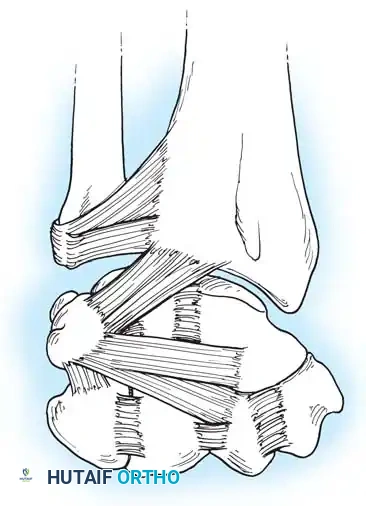
Capsuloligamentous Stabilizers
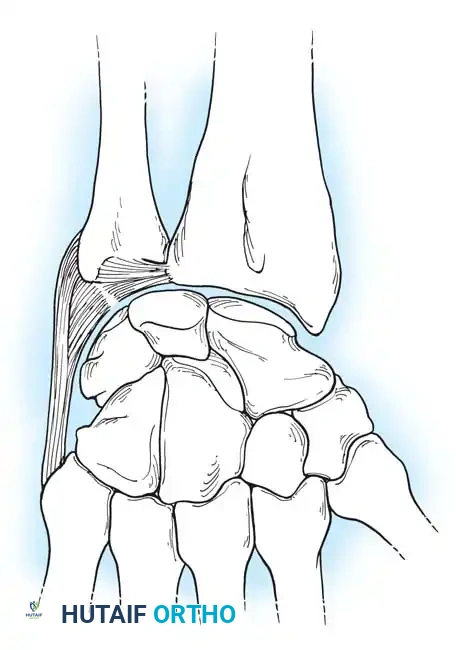
The stability of the carpus relies heavily on a complex network of intrinsic (interosseous) and extrinsic ligaments.
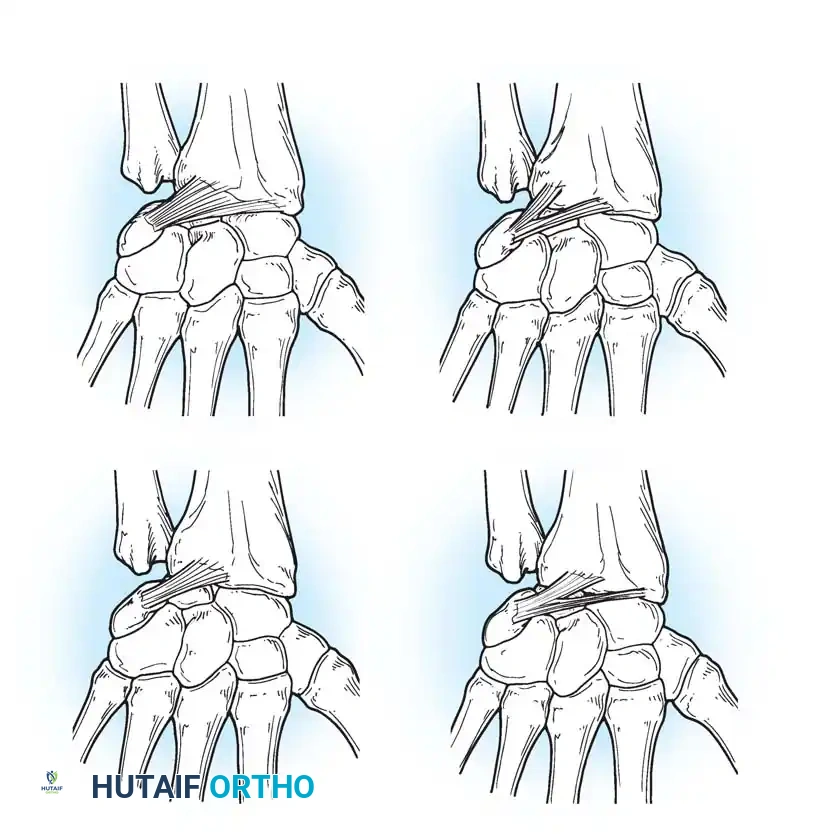
Palmar (Volar) Ligaments
The palmar ligaments are thicker and mechanically stronger than their dorsal counterparts. They are divided into extrinsic ligaments (connecting the forearm to the carpus) and intrinsic ligaments (connecting carpal bones to each other).
Key palmar extrinsic ligaments include:
* Radioscaphocapitate (RSC) Ligament: Acts as a sling supporting the scaphoid waist.
* Long Radiolunate (LRL) Ligament: Prevents ulnar translation of the lunate.
* Short Radiolunate (SRL) Ligament: Stabilizes the lunate to the lunate fossa.
* Radioscapholunate (RSL) Ligament (Ligament of Testut): Primarily a neurovascular conduit rather than a true mechanical stabilizer.
Clinical Pearl: The Space of Poirier is a distinct area of capsular weakness located on the palmar aspect of the midcarpal joint, between the RSC and the palmar radiolunotriquetral ligaments. It overlies the palmar surface of the lunate and is the classic site of capsular failure in perilunate dislocations.
Dorsal Ligaments
The dorsal capsuloligamentous network is thinner but biomechanically vital for preventing dorsal intercalated segment instability (DISI) and guiding carpal kinematics.
The Dorsal Radiocarpal (DRC) Ligament originates from the dorsal radial margin of the lunate fossa, spans the lunotriquetral joint, and inserts onto the dorsal triquetrum. Viegas and Mizuseki classified the DRC into four distinct morphological types based on its thickness and insertion footprint.
The Dorsal Intercarpal (DIC) Ligament originates from the dorsal triquetrum, courses transversely across the midcarpal joint, and inserts onto the dorsal scaphoid waist and trapezoid. Viegas verified three distinct types of DIC ligaments, noting that its laminated structure allows it to change shape dynamically during wrist motion.
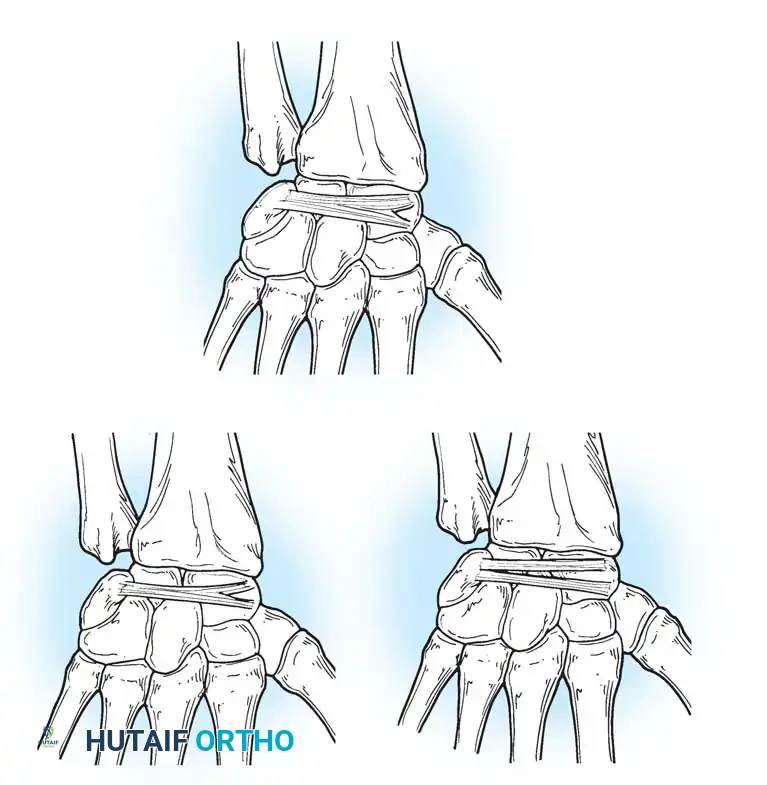
Together, the DRC and DIC form a lateral "V" shape that stabilizes the proximal row and prevents dorsal subluxation during wrist flexion.
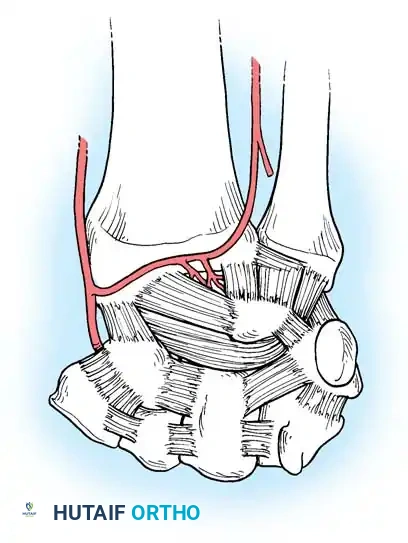
Vascular Anatomy of the Carpus
Understanding the extraosseous and intraosseous vascularity of the wrist is paramount, particularly when managing fractures of the scaphoid and lunate, which are highly susceptible to avascular necrosis (AVN).
Gelberman et al. mapped the terminal branches of the radial, ulnar, and anterior interosseous arteries, which form three dorsal and three palmar transverse arterial arches.
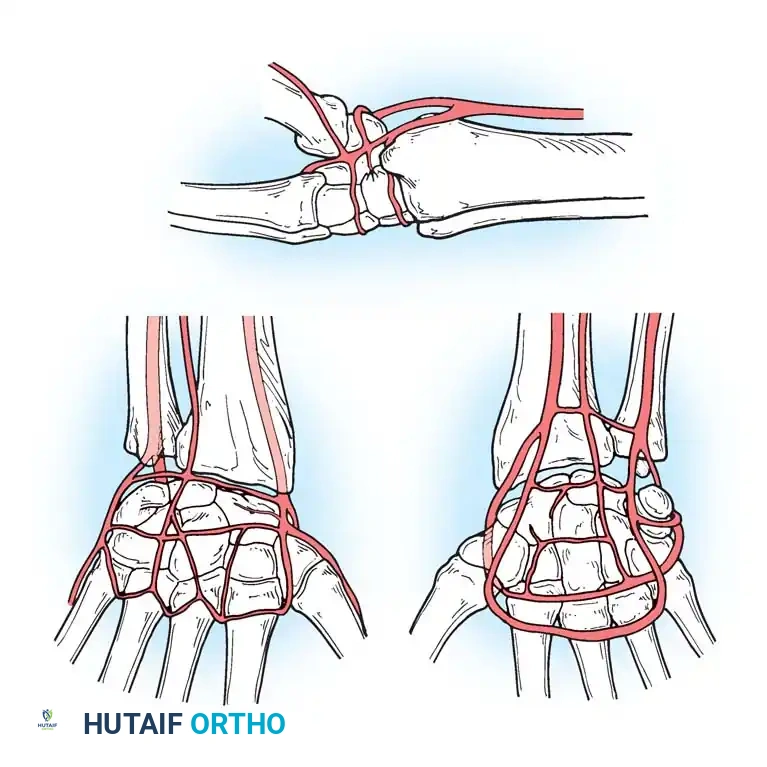
Dorsal Arterial Arches
- Dorsal Radiocarpal Arch: Supplies the proximal lunate and triquetrum.
- Dorsal Intercarpal Arch: The largest arch, supplying the distal carpal row and providing anastomotic flow to the lunate and triquetrum.
- Basal Metacarpal Arch: Supplies the distal carpal row and metacarpal bases.
Palmar Arterial Arches
- Palmar Radiocarpal Arch: Supplies the palmar lunate and triquetrum.
- Palmar Intercarpal Arch: Highly variable; rarely contributes nutrient vessels to the carpus.
- Deep Palmar Arch: Consistent arch communicating with the dorsal basal metacarpal arch.
Surgical Warning: The scaphoid receives 70-80% of its blood supply from branches of the radial artery entering the dorsal ridge, perfusing the bone in a retrograde fashion. Fractures at the scaphoid waist or proximal pole disrupt this delicate supply, leading to high rates of nonunion and AVN. Surgical approaches must meticulously preserve the dorsal ridge vasculature.
Biomechanics and Kinematics
The kinematics of the wrist are dictated by the articular geometry and the tethering ligaments. The center of rotation for global wrist motion (flexion/extension and radial/ulnar deviation) is located within the proximal head of the capitate.
The Dart-Thrower's Motion
Most functional activities of daily living do not occur in pure orthogonal planes (pure flexion or pure deviation). Instead, they occur in an oblique plane known as the "dart-thrower's motion"—moving from radial extension to ulnar flexion. This motion occurs primarily at the midcarpal joint, with minimal movement of the proximal carpal row (specifically the scaphoid and lunate), making it a safe rehabilitation arc following scapholunate ligament repairs.
Carpal Instability Patterns
Mayfield, Johnson, and Kilcoyne described the progressive stages of perilunar instability resulting from wrist hyperextension, ulnar deviation, and intercarpal supination:
* Stage I: Scapholunate dissociation (SL ligament tear).
* Stage II: Capitate dislocation (Space of Poirier disruption).
* Stage III: Lunotriquetral dissociation (LT ligament tear).
* Stage IV: Lunate dislocation (lunate extrudes volarly into the carpal tunnel).
Master Surgical Approaches to the Wrist
Executing flawless surgical approaches requires strict adherence to internervous planes and meticulous handling of the capsuloligamentous structures to prevent iatrogenic instability.
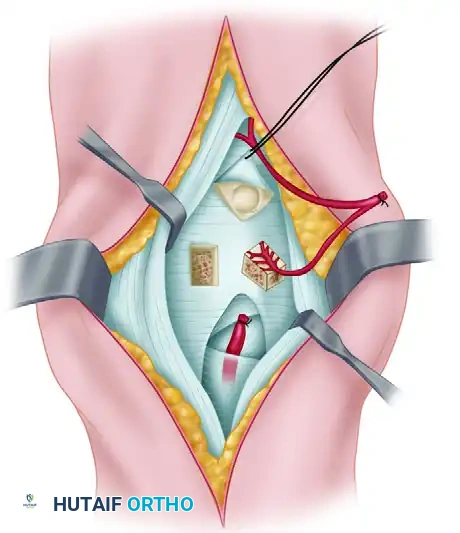
The Dorsal Approach to the Wrist
Indications: Open reduction internal fixation (ORIF) of distal radius fractures (dorsal shear), proximal row carpectomy, four-corner arthrodesis, total wrist arthrodesis, and dorsal ganglion excision.
Positioning: Supine, arm on a hand table, forearm fully pronated. A well-padded pneumatic tourniquet is applied to the proximal arm.
Step-by-Step Surgical Technique:
1. Incision: A longitudinal incision is made centered over the Lister tubercle, extending proximally over the distal radius and distally toward the base of the third metacarpal.
2. Superficial Dissection: Elevate full-thickness fasciocutaneous flaps to protect the dorsal sensory branches of the radial and ulnar nerves.
3. Extensor Retinaculum: Identify the extensor retinaculum. Open the third extensor compartment and transpose the Extensor Pollicis Longus (EPL) tendon radially.
4. Subperiosteal Elevation: Elevate the second and fourth compartments subperiosteally to expose the dorsal wrist capsule.
5. Capsulotomy (Berger's Flap): To preserve the critical DRC and DIC ligaments, perform a ligament-sparing capsulotomy. Create a distally based, V-shaped flap following the fibers of the DRC and DIC.
6. Deep Exposure: Reflect the capsular flap distally to expose the radiocarpal and midcarpal joints.
Closure: The capsular flap is meticulously repaired with non-absorbable sutures to restore dorsal stability. The extensor retinaculum is repaired, leaving the EPL transposed subcutaneously to prevent attrition rupture.
The Volar (Henry) Approach to the Wrist
Indications: ORIF of volar distal radius fractures, scaphoid waist fractures, perilunate dislocations, and volar marginal lip fractures.
Positioning: Supine, arm on a hand table, forearm supinated.
Step-by-Step Surgical Technique:
1. Incision: A longitudinal incision is made over the course of the Flexor Carpi Radialis (FCR) tendon, zig-zagging across the wrist crease if extending into the palm.
2. Superficial Dissection: Incise the superficial fascia. Identify and protect the palmar cutaneous branch of the median nerve, which lies ulnar to the FCR tendon.
3. Internervous Plane: Incise the FCR tendon sheath and retract the FCR tendon ulnarly (protecting the median nerve). Retract the radial artery radially.
4. Deep Dissection: Expose the deep fascial layer covering the Flexor Pollicis Longus (FPL) and the pronator quadratus (PQ).
5. Pronator Quadratus Elevation: Incise the PQ along its radial and distal borders (the "L" incision) and elevate it ulnarly to expose the volar surface of the distal radius.
6. Capsulotomy: If accessing the carpus (e.g., for scaphoid ORIF), perform a longitudinal or T-shaped volar capsulotomy, taking care to repair the strong volar extrinsic ligaments (RSC, LRL) upon closure.
Closure: The volar capsule is repaired if opened. The pronator quadratus is reapproximated to the radial border to cover the hardware and prevent flexor tendon irritation. The FCR sheath is left open to prevent stenosis.
Postoperative Rehabilitation Protocols
The success of wrist surgery is inextricably linked to the postoperative rehabilitation protocol. While specific timelines vary based on the procedure (e.g., rigid internal fixation vs. ligamentous reconstruction), general principles apply:
- Phase I (0-2 Weeks) - Protection and Edema Control: The wrist is immobilized in a bulky dressing and volar splint. Digital range of motion (ROM) is initiated immediately to prevent tendon adhesions and stiffness. Elevation and compressive wraps are utilized to manage edema.
- Phase II (2-6 Weeks) - Early Protected Motion: For stable fractures (e.g., volar plated distal radius), a custom thermoplastic splint is fabricated, and active ROM exercises (including the dart-thrower's motion) are initiated. For ligament repairs, rigid immobilization is maintained for 6-8 weeks.
- Phase III (6-12 Weeks) - Strengthening and Proprioception: Once clinical and radiographic union is achieved, passive stretching and progressive resistance exercises are introduced. Proprioceptive training is critical for restoring dynamic neuromuscular control of the carpus.
- Phase IV (12+ Weeks) - Return to Function: Work-specific or sport-specific conditioning is implemented. Maximum medical improvement is typically reached between 6 and 12 months postoperatively.
Conclusion
Mastery of wrist surgery demands an uncompromising respect for its intricate anatomy and biomechanics. From the delicate vascular supply of the scaphoid to the robust ligamentous architecture of the TFCC and carpal rows, every surgical maneuver must be executed with precision. By adhering to evidence-based surgical approaches and prioritizing ligamentous preservation, the operative orthopedist can successfully navigate the complexities of wrist disorders and restore optimal function to the patient.
===CONTENT===
You Might Also Like