Scaphotrapezial-Trapezoid (STT) Fusion: A Comprehensive Surgical Guide

Key Takeaway
Scaphotrapezial-trapezoid (STT) fusion, or triscaphe arthrodesis, is a limited carpal fusion designed to stabilize the radial column while preserving functional wrist motion. Primary indications include isolated STT osteoarthritis and dynamic scapholunate instability. Successful outcomes rely on meticulous joint decortication, precise anatomical reduction of the scaphoid to prevent radioscaphoid impingement, and rigid Kirschner wire fixation augmented with cancellous bone graft to ensure robust union.
Introduction to Scaphotrapezial-Trapezoid (STT) Fusion
Scaphotrapezial-trapezoid (STT) fusion, originally popularized by H. Kirk Watson as the "triscaphe arthrodesis," is a highly effective limited carpal arthrodesis. The procedure is designed to surgically unite the scaphoid, trapezium, and trapezoid into a single biomechanical block. By stabilizing the radial column of the carpus, STT fusion effectively halts the progression of localized degenerative changes while preserving a functional arc of radiocarpal and midcarpal motion.
This procedure is technically demanding. It requires a profound understanding of carpal kinematics, meticulous joint preparation, and precise spatial reduction of the scaphoid. Failure to anatomically position the scaphoid during fixation inevitably leads to altered radiocarpal mechanics, dorsal impingement, and accelerated adjacent-segment arthrosis.
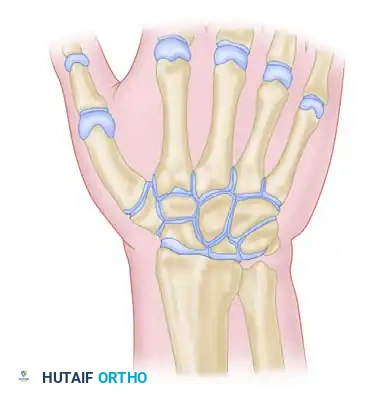
Surgical Anatomy and Biomechanics
The scaphoid functions as a critical tie-rod connecting the proximal and distal carpal rows. It is subjected to significant shear and compressive forces during normal wrist motion. The STT joint itself is a complex, multi-planar articulation that facilitates the transmission of forces from the thumb and radial digits to the radiocarpal joint.
When the STT joint is fused, the scaphoid is locked to the distal carpal row. This eliminates the normal flexion and extension of the scaphoid independent of the trapezium and trapezoid. Consequently, the entire triscaphe unit moves synchronously. If the scaphoid is fused in an excessively extended (vertical or longitudinal) position, its proximal pole will impinge against the dorsal rim of the radial styloid during wrist extension, severely limiting motion and causing pain.
Indications and Contraindications
Primary Indications
- Isolated STT Osteoarthritis: Often presenting with radial-sided wrist pain exacerbated by radial deviation and thumb loading.
- Scapholunate Advanced Collapse (SLAC) - Early Stages: Specifically for dynamic or static rotary subluxation of the scaphoid where the radiocarpal articular cartilage remains pristine.
- Kienböck’s Disease (Stage III): Utilized to unload the lunate by transferring forces through the fused radial column.
- Midcarpal Instability: Selected cases of palmar midcarpal instability.
Contraindications
Surgical Warning: Triscaphe arthrodesis is strictly contraindicated in the presence of significant radioscaphoid arthritis. If degenerative changes are identified at the scaphoid fossa of the distal radius, an STT fusion will exacerbate the pain. In such instances, a SLAC wrist reconstruction (e.g., four-corner fusion or proximal row carpectomy) must be performed instead.
Preoperative Planning and Core Principles
Watson outlined five foundational principles that must be strictly observed to achieve a successful triscaphe arthrodesis:
- Careful Planning: Preoperative radiographic templating and advanced imaging (CT scan) are essential to assess bone stock and the extent of arthrosis.
- Minimize Fused Joints: Only the minimum necessary joints (scaphoid, trapezium, trapezoid) should be included in the fusion mass.
- Adequate Bone Grafting: Packed, autologous cancellous bone graft must be used in sufficient quantities to promote osteogenesis.
- Maintain External Dimensions: The external dimensions of the fused triscaphe unit must perfectly equal the external dimensions of the same bones in their native, normal state to prevent carpal collapse or over-distraction.
- Selective Pinning: Only the joints intended for fusion should be crossed with fixation pins.
Surgical Technique: STT Fusion Step-by-Step
1. Patient Positioning and Anesthesia
After satisfactory induction of regional or general anesthesia, the patient is positioned supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The hand, wrist, and forearm are prepped and draped in a standard sterile fashion.
2. Incision and Exposure
- Make a transverse or slightly curved longitudinal incision in the skin on the dorsum of the wrist, centered directly over the STT articulation.
- Carefully dissect through the subcutaneous tissues. Identify and gently retract the dorsal sensory branches of the superficial radial nerve and the accompanying dorsal venous network.
- Open the extensor retinaculum longitudinally along the course of the extensor pollicis longus (EPL) tendon (third dorsal compartment). Transpose the EPL radially.
- Approach Options:
- Standard Approach: Enter the wrist capsule between the tendons of the extensor carpi radialis longus (ECRL) and the extensor carpi radialis brevis (ECRB).
- Kleinman’s Modification: Expose the wrist capsule between the first and second dorsal extensor compartments. This provides excellent exposure of the adjacent surfaces of the STT joint while allowing safe retraction of the radial artery.
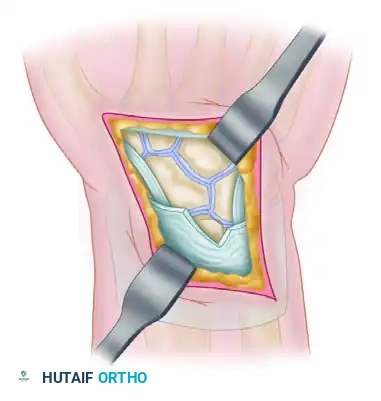
3. Joint Evaluation and Preparation
Open the STT joint capsule and extend the capsulotomy proximally to expose the proximal articular surface of the scaphoid and the scaphoid fossa of the radius. Inspect the radiocarpal joint meticulously to rule out radioscaphoid arthrosis.
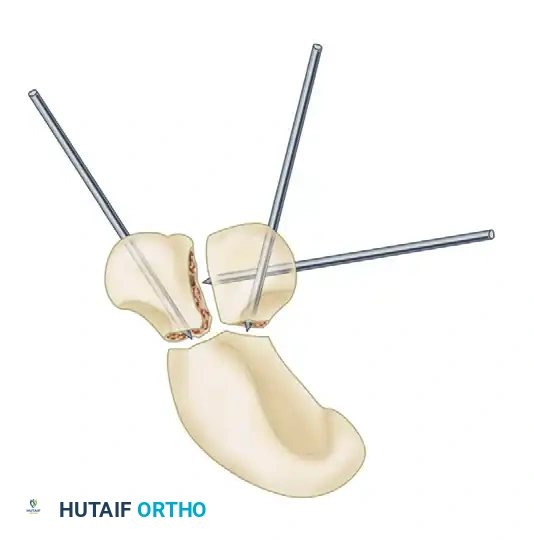
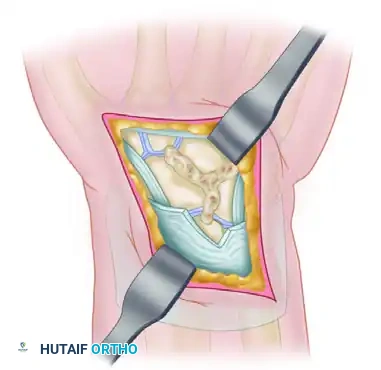
- Using a combination of rongeurs, sharp osteotomes, and high-speed burrs, remove the articular cartilage and subchondral bone from the opposing surfaces of the trapezium, trapezoid, and distal scaphoid.
- Decorticate down to healthy, bleeding cancellous bone to optimize the fusion bed.
Clinical Pearl (Kleinman’s Modification): Rather than removing the entire articular surface, Kleinman recommends removing only the dorsal two-thirds of the articular surfaces. This critical modification preserves the palmar one-third of the joint, which maintains native carpal height and prevents volar collapse of the fusion mass during compression.
4. Scaphoid Reduction
Anatomical reduction of the scaphoid is the most critical biomechanical step of the procedure.
- Careful attention is required to avoid fixing the scaphoid in an excessively longitudinal (vertical) or dorsiflexed position.
- Reduction Technique: Introduce a curved elevator or dental pick palmar to the distal neck of the rotated scaphoid. Use the instrument to gently dorsiflex the distal pole. This maneuver reduces the scaphoid to its anatomical posture, securing the proximal pole congruently within the scaphoid fossa of the radius.
- The longitudinal axis of the scaphoid should be set to 30 degrees or more relative to the radius. An angle less than 30 degrees indicates excessive longitudinal orientation, which will inevitably lead to radioscaphoid impingement during wrist extension.
- Correlate the reduction by directly inspecting the dorsal surface of the proximal pole of the scaphoid and its relationship to the dorsal aspect of the lunate. Ensure closure of any preoperative scapholunate diastasis.
5. Bone Graft Harvesting
Autologous bone graft is mandatory for a high union rate. Graft can be obtained from the ipsilateral distal radius or the iliac crest.
- Distal Radius Harvest: Retract the proximal skin flap or make a separate transverse incision over the distal radial metaphysis.
- Expose the radius between the ECRL and the extensor pollicis brevis (EPB).
- Incise and elevate the periosteum to expose the flat cortical area of the distal dorsoradial metaphysis.
- Use a small gouge to create a cortical window. Harvest the underlying cancellous bone using curettes.
- Achieve hemostasis with bone wax if necessary, and close the donor site.
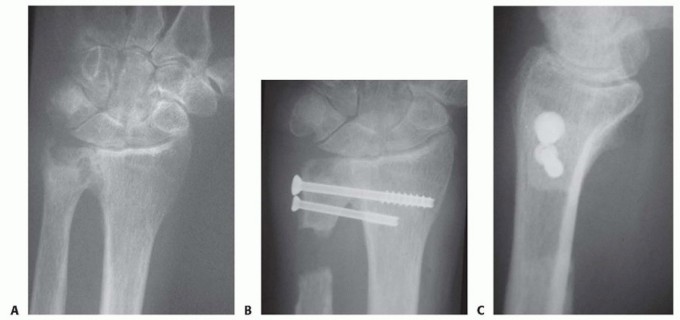
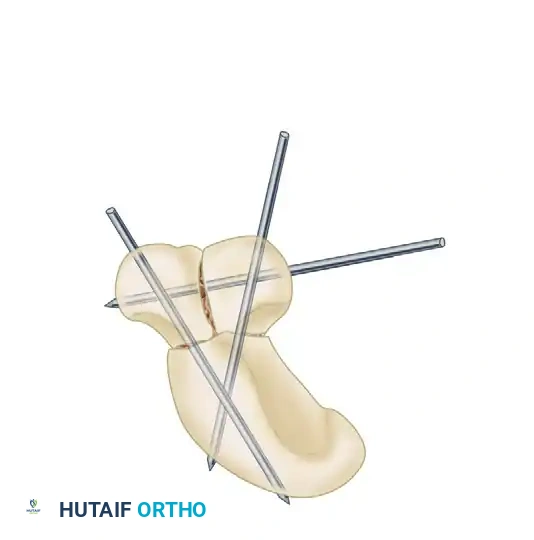
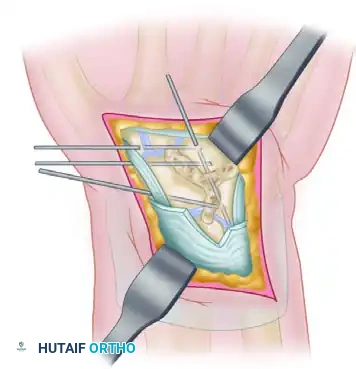
6. Kirschner Wire Fixation and Grafting
Fixation is typically achieved using three 0.045-inch Kirschner wires (K-wires).
- Presetting the Pins: Following Watson’s recommendation, pass the 0.045-inch K-wires in a retrograde fashion out through the raw bony surfaces of the trapezium and trapezoid before final reduction.
- Temporary Fixation: Once the scaphoid is anatomically reduced (distal pole elevated, proximal pole seated), two temporary K-wires can be driven from the scaphoid into the capitate to hold the reduction.
- Graft Packing: Thoroughly pack the harvested cancellous bone graft into the decorticated STT joint spaces. Ensure the external dimensions of the fusion unit match a normal wrist.
- Final Fixation: Drive the preset pins across the fusion site in an antegrade direction. Typically, two pins pass from the trapezoid into the scaphoid, and one pin passes across the trapezium-trapezoid articulation.
Surgical Pitfall: Strictly avoid passing the definitive intercarpal arthrodesis pins into the radius or ulna. Check wrist motion under fluoroscopy to ensure no pins obstruct radiocarpal kinematics.
- Dorsal Cortical Bridge (Optional): A cortical bone graft can be mortised or notched into the dorsal surface to bridge the fusion site, providing additional structural stability.
- Cut the K-wires just beneath the skin to prevent pin-tract infections while allowing easy removal later.
7. Closure
Deflate the tourniquet and obtain meticulous hemostasis. Insert closed-suction drains if necessary. Close the capsule, extensor retinaculum, and skin in layers. Apply a bulky compression dressing reinforced with a long-arm plaster splint.
Other Limited Wrist Arthrodeses
While STT fusion is highly effective, other limited intercarpal fusions are utilized depending on the specific pattern of carpal pathology. These include arthrodesis of the scaphocapitate, scaphocapitolunate, lunotriquetral, and radiolunate joints.
It is imperative to note that limited carpal fusions carry a significant complication profile. McAuliffe et al. reported complications in 36 of 50 patients treated with various limited intercarpal fusions, with nonunion being the most frequent complication. Similarly, Fortin and Louis reported complications in 11 of 14 patients following STT arthrodesis, highlighting radiocarpal arthrosis, trapeziometacarpal arthrosis, and nonunion as primary concerns.
Scaphocapitolunate Arthrodesis
For broader midcarpal instability or specific degenerative patterns, a scaphocapitolunate fusion may be indicated. The principles of decortication, grafting, and pinning remain consistent with STT fusion.
-
Incision: A dorsal longitudinal or slightly oblique incision extending from the ulnar aspect of the distal radius to the distal pole of the scaphoid.
-
Exposure: The scaphocapitolunate articulation is exposed between the third and fourth dorsal compartments. The capsule is typically opened in an inverted-T fashion.
-
Preparation and Grafting: The articular surfaces are decorticated down to bleeding bone, and the resulting voids are densely packed with autologous cancellous bone graft.
-
Fixation: Rigid fixation is achieved using multiple K-wires, often placed in a triangular configuration to neutralize multi-planar forces across the scaphoid, capitate, and lunate.
Postoperative Care and Rehabilitation
The postoperative protocol must balance the need for rigid immobilization to achieve bony union with the goal of preventing debilitating wrist stiffness.
- Initial Phase (0 to 7-10 Days): The bulky compression dressing and long-arm splint are left undisturbed. Elevation and active digital motion are highly encouraged to minimize edema.
- Cast Immobilization (1 to 6 Weeks): At 7 to 10 days, the initial dressing is removed, sutures are extracted, and a cast is applied.
- Watson's Protocol: Recommends a long-arm cast with volar extension to support the index and long fingers in the intrinsic-plus position.
- Kleinman's Protocol: Suggests a well-molded short-arm thumb spica cast is sufficient, avoiding the morbidity of elbow and metacarpophalangeal joint immobilization.
- Pin Removal (6 to 8 Weeks): The cast is removed, and interval radiographs are obtained. If clinical and radiographic signs of early consolidation are present, the subcutaneous K-wires are removed in the clinic.
- Transition Phase (8 to 10 Weeks): Depending on radiographic healing and patient compliance, a short-arm cast or removable thermoplastic splint is utilized for an additional 1 to 2 weeks.
- Rehabilitation: Once satisfactory bony union is confirmed, the wrist is fully mobilized. Patients undergo a graduated physical therapy program focusing on active and active-assisted range of motion.
- Long-Term Expectations: Motion is typically limited initially but progressively improves over the first 12 months postoperatively. Patients must be monitored closely for signs of Complex Regional Pain Syndrome (CRPS) or shoulder-hand syndrome; if symptoms arise, aggressive therapeutic intervention is instituted immediately.
You Might Also Like