Operative Management of the Arthritic Hand: Rheumatoid and Osteoarthritic Reconstructions
Key Takeaway
The surgical management of the arthritic hand requires a profound understanding of altered biomechanics, progressive deformity, and soft-tissue attenuation. This comprehensive guide details evidence-based operative interventions for rheumatoid and osteoarthritis, including metacarpophalangeal joint arthroplasty, basal joint reconstruction, tendon transfers, and interphalangeal arthrodesis. Tailored for orthopedic surgeons, it provides step-by-step surgical techniques, implant selection criteria, and postoperative rehabilitation protocols to optimize functional outcomes in complex hand deformities.
Pathoanatomy and Biomechanics of the Arthritic Hand
The surgical management of the arthritic hand remains one of the most complex domains in operative orthopedics, requiring an intricate understanding of biomechanics, soft-tissue balancing, and joint kinematics. The pathophysiology of hand arthritis broadly bifurcates into inflammatory arthropathies (predominantly Rheumatoid Arthritis [RA], Psoriatic Arthritis, and Systemic Lupus Erythematosus) and degenerative conditions (Osteoarthritis [OA]).
In rheumatoid disease, the primary insult is synovial hypertrophy leading to capsular distension, ligamentous attenuation, and secondary articular cartilage destruction. The classic rheumatoid hand deformity—radial deviation of the radiocarpal joint with reciprocal ulnar drift and volar subluxation of the metacarpophalangeal (MCP) joints—is a biomechanical cascade. As the carpus translates ulnarly, the metacarpals deviate radially. The flexor tendons displace ulnarly and volarly, creating a deforming vector that exacerbates MCP joint subluxation.
Conversely, osteoarthritis typically targets the trapeziometacarpal (basal) joint and the distal interphalangeal (DIP) joints, driven by articular wear, osteophyte formation, and asymmetric loading.
Clinical Pearl: In the rheumatoid hand, never address the distal deformities without first evaluating and stabilizing the proximal segments. A perfectly reconstructed MCP joint will rapidly fail if a severe, uncorrected radial deviation of the wrist is left untreated.
Soft-Tissue Procedures and Tendon Reconstruction
Soft-tissue procedures in the arthritic hand serve both prophylactic and reconstructive roles. Early intervention can prevent catastrophic tendon ruptures and irreversible joint destruction.
Tenosynovectomy and Tendon Ruptures
Proliferative tenosynovitis in RA frequently leads to tendon rupture through a combination of direct enzymatic degradation and mechanical attrition.
Extensor Tendon Ruptures (Vaughan-Jackson Syndrome):
The distal radioulnar joint (DRUJ) is frequently involved in RA, leading to dorsal subluxation of the distal ulna (Caput Ulnae Syndrome). The prominent, eroded ulnar head acts as a saw, progressively rupturing the extensor tendons from ulnar to radial (starting with the Extensor Digiti Minimi [EDM], followed by the Extensor Digitorum Communis [EDC] to the small, ring, and middle fingers).
* Surgical Management: Treatment requires addressing the osseous pathology via a Darrach procedure (distal ulna resection) or a Sauvé-Kapandji procedure, combined with dorsal tenosynovectomy and extensor retinaculum relocation.
* Tendon Reconstruction: Primary repair is rarely possible due to tendon retraction and degeneration. Reconstruction relies on tendon transfers (e.g., Extensor Indicis Proprius [EIP] to EDC) or side-to-side tenodesis of the ruptured distal stumps to an intact adjacent EDC tendon.
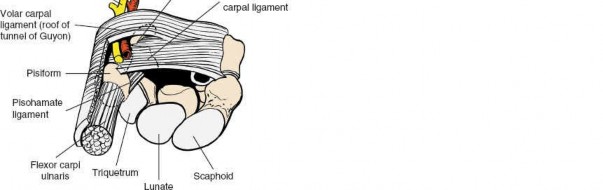
Flexor Tendon Ruptures (Mannerfelt Lesion):
Flexor tendon ruptures commonly occur at the wrist level secondary to attrition over a volar osteophyte of the scaphoid or trapezium. The Flexor Pollicis Longus (FPL) is typically the first to rupture.
* Surgical Management: Volar tenosynovectomy, excision of the offending osteophyte, and tendon reconstruction. For FPL ruptures, an interphalangeal joint arthrodesis or a Flexor Digitorum Superficialis (FDS) transfer (usually from the ring finger) is indicated.
Swan-Neck and Boutonnière Deformities
Digital deformities in RA are driven by intrinsic muscle contractures and central slip/lateral band displacement.
- Swan-Neck Deformity: Characterized by PIP joint hyperextension and DIP joint flexion. It originates from terminal tendon rupture (mallet deformity), volar plate laxity at the PIP joint, or intrinsic tightness.
- Operative Correction: Depends on joint mobility (Nalebuff classification). Flexible deformities are treated with intrinsic release, flexor tenodesis, or lateral band mobilization (e.g., SORL ligament reconstruction). Rigid deformities require PIP joint arthrodesis or arthroplasty.
- Boutonnière Deformity: Characterized by PIP joint flexion and DIP joint hyperextension. It results from the rupture or attenuation of the central slip, allowing the lateral bands to subluxate volarly to the axis of PIP joint rotation, converting them into PIP flexors.
- Operative Correction: Extensor tenotomy (Fowler procedure) for mild deformities, or central slip reconstruction with lateral band relocation for moderate, flexible deformities. Fixed deformities necessitate PIP arthrodesis.
Trapeziometacarpal (Basal Joint) Arthroplasty
Osteoarthritis of the thumb basal joint is a ubiquitous cause of debilitating hand pain. The pathophysiology involves attenuation of the deep anterior oblique (beak) ligament, leading to dorsal-radial subluxation of the metacarpal base, altered contact stresses, and progressive cartilage wear.
Indications and Preoperative Planning
Surgical intervention is indicated for patients with Eaton-Littler Stage II-IV disease who have failed conservative management (splinting, NSAIDs, corticosteroid injections).
Surgical Technique: Ligament Reconstruction and Tendon Interposition (LRTI)
The LRTI procedure, popularized by Burton and Pellegrini, remains the gold standard for advanced basal joint arthritis.
- Incision and Exposure: A Wagner or modified dorsal-radial incision is made over the CMC joint. The superficial radial nerve branches are meticulously protected.
- Capsulotomy and Trapeziectomy: A longitudinal capsulotomy exposes the joint. The trapezium is excised piecemeal or en bloc. Surgical Warning: Ensure complete removal of the medial trapezial osteophytes to prevent impingement on the index metacarpal, while protecting the underlying Flexor Carpi Radialis (FCR) tendon.
- Tendon Harvest: The radial half or the entirety of the FCR tendon is harvested proximally through step-ladder incisions, leaving its distal insertion on the base of the second metacarpal intact.
- Ligament Reconstruction: A bone tunnel is drilled through the base of the first metacarpal (from the dorsal-radial cortex to the articular base). The FCR tendon is passed through this tunnel, tensioned to reduce the metacarpal, and sutured to the periosteum and itself.
- Tendon Interposition: The remaining FCR tendon is folded into an "anchovy" (a biologic spacer) and sutured into the trapezial void to prevent proximal metacarpal subsidence.
- Closure and Pinning: The capsule is imbricated. A temporary Kirschner wire (K-wire) may be placed across the CMC joint to maintain distraction and alignment for 4 weeks.
Pitfall: Over-tensioning the FCR graft can lead to a stiff, adducted thumb. The thumb must be pinned in palmar abduction and opposition to ensure a functional first web space.
Metacarpophalangeal (MCP) Joint Arthroplasty
MCP joint destruction in RA is characterized by volar subluxation, ulnar drift, and severe cartilage loss. When joint preservation is no longer viable, implant arthroplasty is the procedure of choice to restore alignment and functional arc of motion.
Implant Selection and Biomechanics
The Swanson silicone elastomer implant remains the most widely utilized prosthesis. It is critical to understand that the silicone implant is not a true joint replacement; it acts as a dynamic spacer that maintains alignment while a fibrous pseudocapsule forms around it.
* Complications: Long-term follow-up studies highlight risks of implant fracture (up to 30% at 10 years) and silicone lymphadenopathy (particulate synovitis). Despite these radiographic findings, clinical satisfaction and functional alignment often remain high. Newer pyrolytic carbon implants offer better wear characteristics but require intact collateral ligaments and precise osseous anatomy, making them less suitable for severe RA deformities.
Step-by-Step Surgical Approach
- Positioning and Incision: The patient is positioned supine with a hand table. A transverse dorsal incision is made over the metacarpal heads, providing access to all four MCP joints simultaneously.
- Extensor Mechanism Management: The extensor hood is incised longitudinally on the radial side of the EDC tendon. The ulnar sagittal band is released to allow radial centralization of the extensor tendon.
- Metacarpal Head Resection: The collateral ligaments are released. An oscillating saw is used to resect the metacarpal head perpendicular to the shaft. Pearl: Resect enough bone to allow for tension-free reduction of the deformity; inadequate resection leads to recurrent subluxation and premature implant failure.
- Soft-Tissue Release: A comprehensive intrinsic release is mandatory. The ulnar intrinsic tendons (abductor digiti minimi, volar interossei) are released or transferred. The volar plate is released from the proximal phalanx to correct volar subluxation.
- Canal Preparation and Trialing: The medullary canals of the metacarpal and proximal phalanx are broached using rectangular rasps. Sizing should allow the implant stems to glide smoothly within the canal (pistoning) to distribute flexion forces and prevent hinge fracture.
- Implantation: The silicone implants are inserted using a no-touch technique to minimize static charge and contamination.
- Capsular Reconstruction: The radial collateral ligament may be reattached or imbricated. The extensor tendon is centralized and reefed radially to prevent recurrent ulnar drift.
Interphalangeal Joint Arthrodesis
Arthrodesis of the PIP and DIP joints provides predictable pain relief, stability, and correction of deformity in both severe OA and RA.
Indications
- Painful, unstable DIP joints (e.g., severe Heberden's nodes, mucous cysts with joint destruction).
- Rigid swan-neck or boutonnière deformities at the PIP joint.
- Thumb MCP or IP joint instability.
Surgical Techniques
1. Tension-Band Wiring:
Highly effective for PIP and thumb MCP arthrodesis.
* Technique: The articular surfaces are prepared using cup-and-cone reamers to maximize cancellous bone contact while allowing angular adjustment. Two parallel longitudinal K-wires are driven across the joint. A transverse hole is drilled distal to the joint, and a 24-gauge stainless steel wire is passed through, crossed in a figure-of-eight over the dorsal aspect of the joint, and tightened around the proximal K-wires. This converts dorsal tensile forces into volar compressive forces during flexion.
2. Headless Compression Screws (Herbert Screw):
The preferred technique for DIP joint arthrodesis due to its low profile and excellent compression.
* Technique: Following articular preparation, a guidewire is driven antegrade from the distal phalanx tip, across the joint, into the middle phalanx. The screw is advanced over the wire until the trailing threads are completely buried within the distal phalanx tuft, preventing nail bed irritation.
Angles of Fusion
Positioning is critical for hand function. The cascade of the fingers must be respected:
* DIP Joints: Fused at 0° to 10° of flexion.
* PIP Joints: Index finger at 25°, Middle at 35°, Ring at 45°, and Small finger at 55° of flexion. This allows the index finger to participate in precision pinch while the ulnar digits facilitate power grip.
* Thumb: MCP joint fused at 15° of flexion; IP joint fused at 0° to 15° of flexion.
Postoperative Rehabilitation Protocols
The success of arthritic hand surgery is inextricably linked to specialized hand therapy.
- Soft-Tissue and Arthroplasty Reconstructions: Following MCP joint arthroplasty, the hand is immobilized in a bulky dressing for 3 to 5 days. A dynamic extension splint is then fabricated, maintaining the MCP joints in extension and slight radial deviation while allowing active flexion. This splint is worn continuously for 6 weeks. The goal is to achieve a functional arc of 0° to 60° at the MCP joints while the pseudocapsule matures.
- Arthrodesis: Joints undergoing fusion are immobilized in a static splint for 4 to 6 weeks until radiographic evidence of trabecular bridging is observed. Early active motion of adjacent, non-operated joints is encouraged immediately to prevent tendon adhesions and complex regional pain syndrome (CRPS).
- Basal Joint Arthroplasty: The thumb is immobilized in a thumb spica cast or orthosis for 4 weeks. Following pin removal (if used), progressive active and active-assisted range of motion is initiated, avoiding forceful pinch or grip until 8 to 12 weeks postoperatively.
Surgical Warning: Patient expectations must be meticulously managed. The primary goals of arthritic hand surgery are pain relief and the restoration of a stable, functional grasp. Normal anatomic range of motion is rarely, if ever, restored, and patients must be counseled on the salvage nature of these complex reconstructions.
You Might Also Like