Surgical Management of Kienböck Disease: Radial Decompression and Revascularization
Key Takeaway
Kienböck disease, or avascular necrosis of the lunate, presents a complex biomechanical challenge in hand surgery. Joint-leveling procedures like radial decompression aim to reduce lunate strain and stimulate revascularization. This guide details the step-by-step surgical technique for radial metaphyseal decompression, vascularized bone grafting, and salvage options such as lunate excision or prosthetic replacement, providing evidence-based protocols for orthopedic surgeons to optimize patient outcomes and preserve carpal kinematics.
Introduction to Kienböck Disease and Surgical Rationale
Kienböck disease, defined as osteonecrosis (avascular necrosis) of the carpal lunate, presents a profound biomechanical and biological challenge to the orthopedic hand surgeon. The etiology is multifactorial, involving tenuous intraosseous vascular anatomy (often a singular volar or dorsal nutrient vessel lacking robust intraosseous anastomoses), repetitive microtrauma, and biomechanical predispositions such as ulnar negative variance. Left untreated, the ischemic lunate undergoes progressive fragmentation, leading to carpal collapse, rotatory subluxation of the scaphoid, and end-stage radiocarpal arthrosis.
Surgical intervention is dictated by the Lichtman classification, the patient's age, ulnar variance, and functional demands. While joint-leveling procedures (e.g., radial shortening osteotomy) are the gold standard for ulnar-negative patients, radial metaphyseal decompression and lunate revascularization offer critical joint-preserving alternatives, particularly in patients with ulnar neutral or positive variance, or those in the early stages of the disease (Lichtman Stages I, II, and early IIIa).
This masterclass details the operative techniques, biomechanical principles, and postoperative protocols for radial decompression, vascularized bone grafting, and salvage procedures for Kienböck disease.
Radial Decompression for the Treatment of Kienböck Disease
The radial decompression technique, popularized by Illarramendi and De Carli, is a minimally invasive, joint-preserving procedure. Unlike radial shortening osteotomies, it does not alter the gross biomechanical alignment or ulnar variance of the wrist.
Biological and Biomechanical Rationale
The exact mechanism of action for radial decompression remains a subject of academic debate, but it is primarily attributed to two physiological responses:
1. Venous Decompression: Creating a cortical window in the distal radius decreases intraosseous pressure, which may reflexively improve arterial inflow to the carpus via shared capsular vascular networks.
2. Regional Acceleratory Phenomenon (RAP): Surgical trauma to the distal radial metaphysis and extensive periosteal stripping stimulate a profound, localized hyperemic response. This cascade of osteogenic and angiogenic factors promotes revascularization and creeping substitution within the adjacent ischemic lunate.
Preoperative Preparation and Positioning
- Anesthesia: Regional block (axillary or supraclavicular brachial plexus block) or general anesthesia.
- Positioning: The patient is placed in the supine position. The operative extremity is extended onto a radiolucent hand table.
- Tourniquet: A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg (or 100 mm Hg above systolic blood pressure) following exsanguination with an Esmarch bandage.
- Fluoroscopy: A mini C-arm must be available and positioned perpendicular to the hand table to confirm the location of the metaphyseal window and ensure the articular surface is not breached.
Surgical Technique: Step-by-Step (Illarramendi and De Carli)
-
Incision and Approach:
Approach the radius through a 3- to 4-cm longitudinal incision along the radial border of the distal metaphysis. The incision should begin exactly 1 cm proximal to the tip of the radial styloid to avoid the first extensor compartment. -
Neurological Protection:
Identify and meticulously retract the superficial branches of the radial nerve (SBRN) and the lateral antebrachial cutaneous nerve.
Surgical Warning: Neuroma of the SBRN is a debilitating complication. Retraction must be gentle, utilizing blunt instruments or vessel loops. Avoid excessive tension on the skin edges.
-
Soft Tissue Dissection:
Separate the extensor tendons with blunt dissection. The optimal interval is typically between the first extensor compartment (abductor pollicis longus and extensor pollicis brevis) and the second extensor compartment (extensor carpi radialis longus and brevis). -
Periosteal Elevation (The RAP Trigger):
Incise the periosteum longitudinally. Elevate it widely across the distal radial metaphysis. This wide elevation is not merely for exposure; it is a critical step to simulate a reactive healing response (RAP) that drives the regional hyperemia necessary for lunate revascularization. -
Creating the Cortical Window:
Using sharp osteotomes or an oscillating microsaw, create a rectangular cortical window measuring approximately 2.0 × 0.5 cm. The distal extent of this window must begin 2.0 cm proximal to the radial styloid to prevent stress risers that could lead to a distal radius fracture. -
Cancellous Impaction:
Through this cortical window, introduce a curet. Vigorously curet and impact the cancellous bone within the distal metaphysis.
Crucial Technical Point: Do not remove the cancellous bone. The goal is to impact it locally within the metaphysis. You must strictly avoid compromising or breaching the cortex on the opposite (ulnar or volar) side of the radius, and the subchondral bone of the radiocarpal joint must remain pristine. -
Managing the Cortical Flap:
The removed cortical bone from the window can be managed in two ways: - Break the cortex into small 5-mm² fragments and pack them back into the metaphyseal defect.
-
Maintain the cortex as a single piece and leave it impacted (countersunk) into the metaphysis.
-
Closure:
Leave the periosteum open to allow for continued localized hyperemia and decompression. Close the subcutaneous tissue and skin in a routine, layered fashion.
Postoperative Rehabilitation Protocol
- Immobilization: The arm is immobilized in a well-molded, below-elbow volar splint or cast for exactly 2 weeks.
- Early Motion: At the 2-week mark, the cast and sutures are removed. Free active range of motion (AROM) of the wrist and digits is strongly encouraged to prevent capsular contracture.
- Activity Modification: Strenuous activities, heavy lifting, and axial loading of the wrist are strictly avoided for a minimum of 3 months to allow the metaphyseal window to consolidate and the lunate revascularization process to begin.
Lunate Revascularization Procedures
When core decompression is deemed insufficient, or in cases of progressive Lichtman Stage II or IIIa disease without carpal collapse, direct transplantation of an arteriovenous pedicle into the avascular lunate is indicated.
Principles of Vascularized Bone Grafting (VBG)
Transplantation of a vascularized bone graft into necrotic bone introduces live osteocytes, osteoblasts, and an immediate blood supply, bypassing the slow process of creeping substitution. This results in the accelerated formation of new bone and structural reinforcement of the lunate.
Sources of vascularized grafts include:
* Distal Radius (Volar): Based on the pronator quadratus pedicle.
* Pisiform: Transferred as a pedicled graft based on the flexor carpi ulnaris and ulnar artery branches.
* Second Metacarpal: Based on the dorsal metacarpal arteries.
* Distal Radius (Dorsal): The 4th and 5th Extensor Compartment Artery (ECA) graft.
The 4+5 Extensor Compartment Artery (ECA) Graft
The 4+5 ECA graft has become the workhorse for dorsal lunate revascularization due to its reliable anatomy and proximity to the radiocarpal joint.
Surgical Technique (Shin and Bishop):
1. Exposure: A dorsal longitudinal incision is made over the radiocarpal joint. The extensor retinaculum is divided, preserving the compartments.
2. Pedicle Identification: The 4+5 ECA is identified running longitudinally on the dorsal surface of the distal radius, between the 4th and 5th extensor compartments. The anterior interosseous artery is ligated proximal to the 4th and 5th ECA to mobilize the pedicle.
3. Graft Harvest: A corticocancellous block of bone is harvested from the distal radius, keeping the vascular pedicle meticulously attached. Blood flow is verified by observing punctate bleeding from the graft edges upon tourniquet deflation.
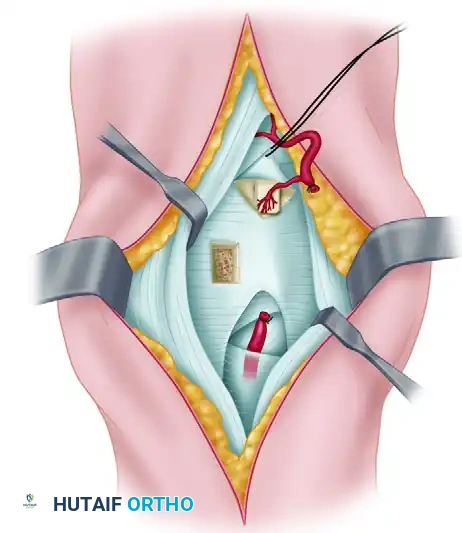
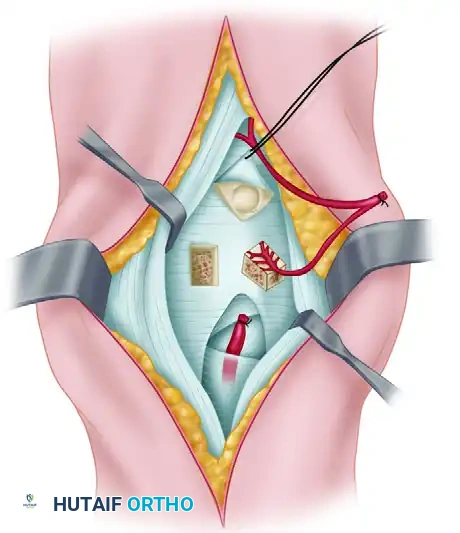
- Lunate Preparation: A dorsal cortical window is created in the lunate. Necrotic, fragmented cancellous bone is carefully debrided using a high-speed burr or curettes until punctate bleeding (if any) or healthy margins are reached.
- Graft Insertion: Cancellous bone graft (autograft from the distal radius) is packed into the lunate defect to restore volume. The vascularized bone graft is then inserted into the dorsal opening.
Orientation: The pedicle must be placed vertically, and the cortical surface of the graft should be oriented in a proximal-distal fashion to avoid kinking the delicate vessels.
Clinical Pearl: The success of a VBG relies entirely on the patency of the microvascular pedicle. Avoid any torsion, tension, or compression of the pedicle during insertion and capsular closure.
Clinical Outcomes and Prognosis
Restoration of lunate architecture and successful revascularization (evidenced by MRI) are reported to occur in 60% to 95% of lunates treated with these techniques. Clinically, these procedures are highly effective, relieving pain and improving grip strength and function in approximately 90% of patients.
However, surgeons must counsel patients regarding long-term expectations. Most longitudinal studies reflect that while early radiographic changes (such as increased radiodensity and halted collapse) are promising, they may not persist indefinitely. In many patients, there is a slow, eventual deterioration in both radiographic parameters and clinical symptoms over a 10- to 15-year horizon, potentially necessitating salvage procedures later in life.
Prosthetic Lunate Replacement and Carpal Kinematics
In cases where the lunate is fragmented but the overall carpal architecture is maintained, prosthetic replacement was historically utilized.
Understanding Carpal Kinematics
To evaluate the success of any lunate procedure, or the degree of carpal collapse in Kienböck disease, specific kinematic indices must be measured on standardized PA radiographs.

Three primary kinematic indices are utilized to assess carpal alignment:
* L1 (Length of the Third Metacarpal): Used as the constant reference denominator to account for variations in patient size and radiographic magnification.
* L2 (Carpal Height): The distance from the base of the third metacarpal to the distal articular surface of the radius.
* Carpal Height Ratio (CHR) = L2 / L1. A normal CHR is approximately 0.54. A decrease indicates carpal collapse.
* L3 (Carpal-Ulnar Distance): The perpendicular distance from the center of rotation of the capitate to the longitudinal axis of the ulna.
* Carpal-to-Ulnar Distance Ratio = L3 / L1. A normal ratio is approximately 0.30. An increase indicates ulnar translation of the carpus.
Silicone Arthroplasty: Historical Context and Complications
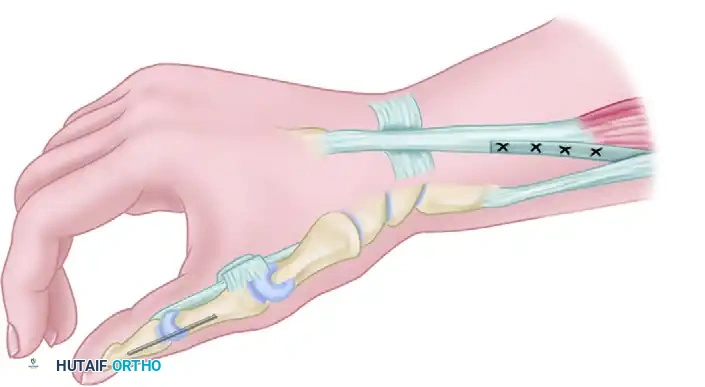
Replacement of the lunate with a hand-carved silicone rubber spacer was previously recommended if there was no significant alteration in the shape of the bone (Lichtman Stage IIIa). A previously molded, lunate-shaped silicone block is inserted into the lunate fossa.
The Critical Role of the Capsule:
If a silicone spacer is used, meticulous repair of the dorsal capsule and the radiocarpal ligaments is paramount. The primary mode of immediate mechanical failure is dorsal subluxation or dislocation of the silicone block due to inadequate ligamentous reconstruction.
The Decline of Silicone Implants:
Troublesome, sight-threatening complications associated with the silicone lunate prosthesis have led to a massive decline in its use. These include:
* Silicone Particulate Synovitis: Micro-abrasion of the implant releases silicone particles, triggering a severe foreign-body macrophage response.
* Foreign Body Cysts: Intraosseous cysts develop in the adjacent scaphoid, capitate, and radius, leading to massive osteolysis.
These complications are exponentially more likely to occur if the implant is oversized, malpositioned, if pre-existing carpal instability is present, or if the patient subjects the wrist to excessive occupational stress. Because of these catastrophic failure modes, the vast majority of modern hand surgeons have abandoned silicone lunate arthroplasty in favor of intercarpal fusions.
Salvage Procedures: Simple Lunate Excision
When joint-preserving procedures fail, or in patients presenting with advanced Lichtman Stage IIIb or IV disease (where carpal collapse and secondary arthrosis have already occurred), salvage procedures are required. Options include Proximal Row Carpectomy (PRC), Scaphoid-Capitate (SC) fusion, Scapho-Trapezio-Trapezoid (STT) fusion, or total wrist arthrodesis.
The Role of Simple Excision
Simple excision of the lunate—without replacement or intercarpal fusion—remains a controversial but viable salvage option for a highly specific subset of patients: the elderly or low-demand individuals.
Biomechanical Consequences:
Following simple excision, the carpus predictably rearranges itself. The capitate and triquetrum migrate proximally into the empty lunate fossa, and the scaphoid assumes a rigidly palmar-flexed posture.
Clinical Outcomes:
Despite this profound kinematic derangement, long-term data demonstrates surprising clinical tolerance. In a cohort of 18 patients followed for an average of 12 years, simple excision produced satisfactory results with continued pain relief. A functional, albeit reduced, range of motion was preserved, and the progression of degenerative radiocarpal changes was significantly less than biomechanical models anticipated.
Surgical Warning: Simple excision is strictly contraindicated in young, active patients or individuals who perform heavy manual labor. In these populations, the resultant carpal instability will rapidly lead to painful, debilitating radiocarpal and midcarpal arthrosis, necessitating a total wrist fusion.
Conclusion
The surgical management of Kienböck disease requires a nuanced understanding of carpal biomechanics, vascular anatomy, and disease staging. Radial decompression offers a low-morbidity, joint-preserving option that leverages the regional acceleratory phenomenon to stimulate healing in early-stage disease. Vascularized bone grafting provides direct biological reconstruction for the ischemic lunate, though long-term durability remains a consideration. When these joint-preserving measures are no longer viable, surgeons must pivot to carefully selected salvage procedures, prioritizing pain relief and functional stability over anatomical restoration.
You Might Also Like