Open Repair of Palmer Class 1C Ulnocarpal Ligament Injuries
Key Takeaway
Palmer Class 1C injuries involve traumatic disruptions of the ulnocarpal ligaments, often presenting with ulnar-sided wrist pain and carpal supination instability. While frequently managed nonoperatively, persistent instability necessitates surgical intervention. This guide details the open repair technique, including foveal bone tunnel preparation, horizontal mattress suture fixation, and precise radioulnar stabilization, ensuring optimal restoration of distal radioulnar joint and ulnocarpal kinematics.
INTRODUCTION TO PALMER CLASS 1C INJURIES
Within the Palmer classification of triangular fibrocartilage complex (TFCC) lesions, Class 1C injuries represent traumatic disruptions of the ulnocarpal ligaments—specifically, the ulnolunate and ulnotriquetral ligaments. These tears may occur within the mid-substance of the ligaments or as avulsions from their distal insertions on the lunate and triquetrum, or proximally from their foveal origins.
Because the ulnocarpal ligaments are integral to the volar stability of the ulnar carpus, their disruption often occurs in tandem with other severe ligamentous trauma, most notably lunotriquetral (LT) interosseous ligament tears and Palmer Class 1B (foveal TFCC) avulsions. While Class 1C injuries can be notoriously difficult to diagnose clinically and radiographically, many heal satisfactorily with conservative immobilization. However, when conservative management fails and significant ulnocarpal instability develops, surgical intervention becomes mandatory to restore wrist kinematics and prevent progressive degenerative arthropathy.
Clinical Pearl: Carpal supination accompanied by a visible or palpable "sagging" of the ulnar side of the carpus is a pathognomonic clinical sign of advanced ulnocarpal instability secondary to a Class 1C lesion.
PATHOANATOMY AND BIOMECHANICS
To master the surgical repair of Class 1C lesions, the orthopaedic surgeon must possess a profound understanding of ulnar-sided wrist biomechanics. The ulnocarpal ligaments originate from the palmar radioulnar ligament and the fovea of the ulnar head, extending distally to insert on the volar aspects of the lunate and triquetrum.
Biomechanical Function
- Prevention of Carpal Supination: The ulnocarpal ligaments act as a critical tether, preventing the proximal carpal row from supinating away from the distal radius and ulna.
- Volar Stability: They provide a volar sling that supports the ulnar carpus. Disruption leads to volar intercalated segment instability (VISI) or a generalized ulnar carpal sag.
- Load Transmission: While the articular disc of the TFCC transmits axial loads, the ulnocarpal ligaments distribute tensile forces during wrist extension and ulnar deviation.
When a Class 1C injury occurs, the loss of this volar tether allows the triquetrum to extend and supinate, leading to incongruency at the lunotriquetral and ulnocarpal joints. If left untreated in a symptomatic patient, this altered kinematic state accelerates chondral wear and leads to ulnocarpal abutment or degenerative arthritis.
CLINICAL EVALUATION AND DIAGNOSIS
Patient Presentation
Patients typically present with a history of a forced hyperextension and pronation injury to the wrist. Chief complaints include deep, poorly localized ulnar-sided wrist pain, weakness in grip strength, and a sensation of "clunking" or instability during forearm rotation.
Physical Examination
- Ulnocarpal Stress Test: Axial loading with ulnar deviation and passive flexion/extension will often reproduce the patient's pain.
- Carpal Sag Sign: Observe the wrist in neutral rotation. A visible volar sagging of the ulnar carpus relative to the distal ulna indicates loss of ulnocarpal ligamentous support.
- DRUJ Ballottement: Assess for concurrent distal radioulnar joint (DRUJ) instability, as Class 1C tears are frequently associated with Class 1B foveal detachments.
Diagnostic Imaging
- Radiographs: Standard posteroanterior (PA), lateral, and oblique views are often normal but may reveal a VISI posture or dynamic ulnar positive variance.
- Magnetic Resonance Imaging (MRI): High-resolution MRI or MR arthrography is the gold standard for non-invasive diagnosis, though mid-substance ulnocarpal ligament tears can still be easily missed due to the complex, striated appearance of the normal ligaments.
- Wrist Arthroscopy: The ultimate diagnostic tool. Arthroscopy allows direct visualization of the ulnocarpal ligaments, the LT interval, and the TFCC foveal attachment. A positive "trampoline test" or a loss of tension in the volar ulnocarpal ligaments confirms the diagnosis.
INDICATIONS FOR SURGICAL INTERVENTION
Class 1C injuries are initially managed nonoperatively with a period of cast or splint immobilization (typically 4 to 6 weeks) followed by targeted rehabilitation. Surgery is indicated when:
1. The patient experiences persistent, debilitating ulnar-sided wrist pain refractory to at least 3 to 6 months of conservative care.
2. There is gross clinical instability, manifested by a symptomatic ulnar carpal sag or dynamic carpal supination.
3. The injury is identified acutely in the setting of a highly unstable DRUJ or concomitant repairable lunotriquetral ligament tear.
Surgical Warning: Do not proceed with isolated ulnocarpal ligament repair without thoroughly assessing the DRUJ and the lunotriquetral ligament. Failure to address concurrent Class 1B or LT tears will result in persistent instability and surgical failure.
PREOPERATIVE PREPARATION
- Anesthesia: Regional anesthesia (supraclavicular or axillary brachial plexus block) is preferred, supplemented with intravenous sedation or general anesthesia based on patient preference and surgical duration.
- Positioning: The patient is placed supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg after exsanguination with an Esmarch bandage.
- Equipment: Small joint retractors, a micro-sagittal saw or high-speed burr, 0.045-inch and 0.062-inch Kirschner wires, 2-0 monofilament absorbable sutures, 20-gauge wire loops (or dedicated suture passers), and Steinmann pins for radioulnar transfixation.
SURGICAL TECHNIQUE: OPEN REPAIR OF CLASS 1C LESIONS
The following technique describes the open reattachment of the ulnocarpal complex to the foveal footprint, a procedure utilized when the ligaments are avulsed proximally or when a combined 1B/1C lesion necessitates robust foveal anchoring.
1. Approach and Exposure
- Make a longitudinal or gently curved incision over the dorsoulnar aspect of the wrist, centered over the DRUJ and extending distally toward the triquetrum.
- Dissect through the subcutaneous tissues, taking meticulous care to identify and protect the dorsal sensory branches of the ulnar nerve (DSBUN).
- Incise the extensor retinaculum over the fifth extensor compartment (extensor digiti minimi - EDM). Elevate the retinaculum to expose the dorsal capsule of the DRUJ and the ulnocarpal joint.
- Perform a longitudinal capsulotomy to expose the TFCC, the ulnar head, and the ulnocarpal ligaments.
2. Joint Inspection and Preparation
- Inspect the ulnocarpal ligaments, the lunotriquetral interval, and the foveal attachment of the TFCC.
- Debride any interposed synovitis, degenerative tissue, or loose chondral flaps.
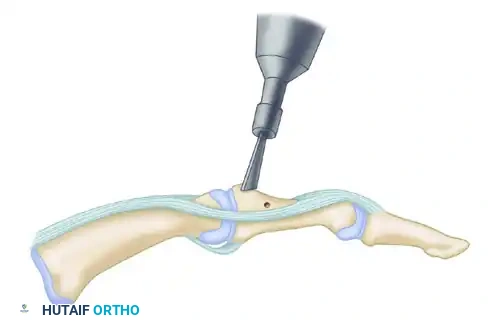
- Identify the avulsed or torn ends of the ulnocarpal ligaments. If the tear is at the foveal origin, prepare the fovea (the depression at the base of the ulnar styloid) using a small curette or a motorized burr to expose bleeding subchondral bone. This decortication is critical for biological healing of the ligamentous footprint.
3. Bone Tunnel Preparation
To achieve secure, isometric fixation of the ulnocarpal complex, transosseous tunnels are created through the ulnar neck.
- Drill a transverse row of small bone tunnels from the dorsomedial aspect of the ulnar neck, directing the drill bits obliquely to exit precisely at the decorticated fovea.
- Typically, three small tunnels are created to accommodate two separate sutures. The center tunnel is designed to share the passage of one limb from each of the two sutures.
- Ensure the bone bridges between the tunnels are sufficiently wide (at least 2-3 mm) to prevent cortical blowout during knot tying.
4. Suture Passage and Ligamentous Repair
- Utilize small, round, noncutting needles armed with 2-0 monofilament, absorbable sutures (e.g., PDS or Maxon).
- Pass the sutures from distal to proximal through the peripheral, foveal attachment area of the TFCC and the proximal stump of the ulnocarpal ligaments.
- Configure the sutures in a horizontal mattress fashion to ensure a broad, secure grasp of the ligamentous tissue without causing ischemic necrosis.
- To retrieve the sutures through the ulnar bone tunnels, use straight needles, 20-gauge wire loops (acting as snares), or a dedicated small joint suture passer.
- Pass the suture limbs from the foveal area out through the dorsomedial ulnar neck tunnels. Remember that the center tunnel will share one end of each of the two sutures.
5. DRUJ Reduction and Suture Tying
- Before tying the sutures, the DRUJ must be anatomically reduced.
- Place the forearm in neutral rotation. Assess the tension on the ulnocarpal ligaments.
- While an assistant maintains the DRUJ reduction and neutral forearm rotation, firmly tie the suture ends over the cortical bone bridge of the ulnar neck.
- Verify the stability of the repair by gently ranging the wrist and forearm. The ulnar carpal sag should be eliminated, and the DRUJ should remain stable.
Pitfall: Tying the sutures with the forearm in extreme pronation or supination can non-isometrically over-constrain the joint, leading to a severe postoperative loss of forearm rotation. Always tie the sutures in neutral rotation unless specific instability patterns dictate otherwise.
6. Capsular Augmentation and Closure
- Close the dorsal joint capsule meticulously.
- If the capsular tissue is attenuated or if the repair requires additional volar-dorsal support, utilize a strip of the extensor retinaculum to augment the closure. This helps avoid excessive tension on the primary capsular repair.
- Ensure that the retinacular flap is routed deep to the extensor digiti quinti (EDQ) to prevent extensor tendon tethering or bowstringing.
7. Radioulnar Transfixation (Optional but Recommended)
To protect the delicate ulnocarpal and foveal repair—especially in patients with massive instability, poor tissue quality, or uncertain postoperative compliance—temporary radioulnar transfixation is highly recommended.
- Supinate or pronate the forearm slightly based on the primary vector of preoperative instability:
- If the ulna was unstable dorsally, position the forearm in slight supination.
- If the ulna was unstable volarly, position the forearm in slight pronation.
- Crucial Note: Avoid extreme rotation to prevent excessive tension on the newly repaired ligaments.
- Drive a suitably sized Steinmann pin (typically 0.062-inch or 5/64-inch) transversely from the ulna into the radius, positioned just proximal to the sigmoid notch.
- Cut the pin beneath the skin to prevent pin tract infections.
8. Final Closure
- Deflate the tourniquet and achieve meticulous hemostasis.
- Close the subcutaneous tissues with inverted absorbable sutures.
- Close the skin with non-absorbable monofilament sutures or surgical staples.
- Apply sterile dressings and immediately immobilize the extremity in a bivalved long-arm cast or a rigid long-arm posterior splint with the forearm in the previously determined safe position of rotation.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The postoperative rehabilitation following a Class 1C ulnocarpal ligament repair is extensive and requires strict adherence to protect the healing soft tissues while gradually restoring function.
Phase 1: Maximum Protection (Weeks 0 to 2)
- The patient remains in the initial bivalved long-arm cast or splint.
- Strict elevation and digital range of motion (ROM) exercises are encouraged immediately to prevent tendon adhesions and reduce edema.
- At 2 weeks postoperatively, the patient is seen in the clinic. Skin sutures are removed.
- The splint is transitioned to a well-molded, fiberglass long-arm cast.
Phase 2: Continued Immobilization (Weeks 2 to 6)
- The patient remains in the long-arm cast to completely neutralize forearm rotation.
- At 4 weeks postoperatively, the transverse radioulnar Steinmann pin is removed in the clinic under local anesthesia.
- Following pin removal, a new long-arm cast is applied for an additional 2 weeks to protect the repair site as it continues to mature.
- At 6 weeks postoperatively, the long-arm cast is definitively removed.
Phase 3: Intermediate Protection and Early Motion (Weeks 6 to 10)
- At 6 weeks, the patient is transitioned to a short-arm cast for 3 to 4 weeks. This allows for the initiation of gentle, active elbow ROM and very limited, protected forearm rotation, while still supporting the carpus.
- At 9 to 10 weeks postoperatively, the short-arm cast is removed and replaced with a custom-molded, removable short-arm splint (e.g., a Muenster or standard wrist splint, depending on residual DRUJ stability).
- A therapist-supervised rehabilitation program is initiated. Focus is placed on active and active-assisted wrist flexion/extension and gradual forearm pronation/supination.
Phase 4: Strengthening and Return to Activity (Weeks 10 and Beyond)
- The removable splint is worn for an additional 3 to 4 weeks (up to 12-14 weeks postoperatively), primarily during sleep and high-risk activities.
- Passive stretching and joint mobilization techniques are cautiously introduced by the hand therapist.
- Progressive strengthening (isometric progressing to isotonic) begins once painless, functional ROM is achieved.
- Return to Work/Sports: Forceful rotational movements, heavy lifting, and grasping activities must be strictly avoided until the patient is completely comfortable and has achieved satisfactory motion and grip strength (typically 4 to 6 months postoperatively).
COMPLICATIONS AND MANAGEMENT
- Postoperative Stiffness: The most common complication due to the prolonged immobilization required for ligamentous healing. Managed with aggressive, sustained hand therapy. Surgical release is rarely indicated unless stiffness is refractory after 6-12 months of therapy.
- Recurrent Instability: Can occur due to premature return to activity, failure to address concurrent LT or DRUJ pathology, or technical errors during bone tunnel placement. May require revision surgery or salvage procedures (e.g., ulnar shortening osteotomy or partial wrist fusion).
- Hardware Complications: Pin tract infections or pin migration from the radioulnar Steinmann pin. Mitigated by burying the pin beneath the skin and removing it promptly at 4 weeks.
- Nerve Injury: Iatrogenic injury to the dorsal sensory branch of the ulnar nerve (DSBUN) during the surgical approach. Meticulous dissection and the use of blunt retractors are essential to prevent painful neuromas.
By adhering to strict biomechanical principles, executing precise foveal bone tunnel preparation, and enforcing a rigorous postoperative rehabilitation protocol, the orthopaedic surgeon can successfully manage Palmer Class 1C ulnocarpal ligament injuries, restoring stability and function to the complex ulnar-sided wrist.
You Might Also Like