Scapholunate Ligament Reconstruction: Advanced Surgical Techniques and Biomechanics
Key Takeaway
Scapholunate ligament reconstruction is indicated for chronic dissociation where primary repair is unfeasible. Utilizing tendon grafts like the flexor carpi radialis (FCR) or extensor carpi radialis brevis (ECRB), these technically demanding procedures aim to restore carpal kinematics. Success relies on precise bone tunneling, meticulous graft routing, and rigid temporary Kirschner wire fixation. Patient selection is critical, as pre-existing arthrosis contraindicates these reconstructive weaves.
Introduction to Carpal Ligament Reconstruction
Ligament reconstruction of the wrist, particularly for chronic scapholunate (SL) dissociation, remains one of the most technically demanding challenges in operative orthopaedics. When primary repair is no longer viable due to ligamentous retraction, attenuation, or delayed presentation (typically beyond one month), reconstruction using free tendon grafts or tenodesis becomes necessary. These procedures frequently utilize prolonged slips of the wrist flexors (such as the flexor carpi radialis) or extensors (such as the extensor carpi radialis brevis).
While ligament reconstruction can yield highly satisfactory functional restoration for carefully selected patients, the outcomes can be inherently unpredictable. As Taleisnik astutely pointed out, tendons used as substitute ligaments are subject to viscoelastic creep; they may stretch over time and become lax, leading to recurrent carpal instability. Furthermore, the creation of transosseous tunnels for the passage of tendon slips introduces the risk of iatrogenic fracture and potential avascular changes within the delicate carpal bones.
Clinical Pearl: The fundamental paradox of carpal ligament reconstruction is the balance between stability and mobility. The tightness required to maintain anatomical apposition of the scaphoid and lunate inherently limits eventual wrist motion. All patients must be counseled preoperatively to expect a permanent reduction in their global arc of wrist motion.
Ligament reconstruction is strictly contraindicated in patients with associated degenerative joint disease, such as Scapholunate Advanced Collapse (SLAC). In the presence of arthrosis, salvage procedures—including radial styloidectomy, proximal row carpectomy, partial wrist arthrodesis (e.g., four-corner fusion), or total wrist arthroplasty—must be considered instead.
The Palmer, Dobyns, and Linscheid Technique
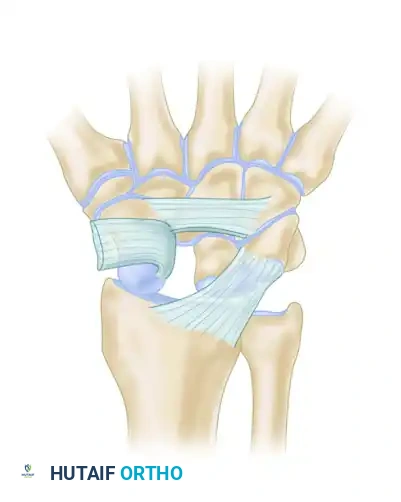
Palmer, Dobyns, and Linscheid pioneered a robust reconstructive technique utilizing a distally attached slip of the flexor carpi radialis (FCR) tendon. This procedure is specifically reserved for patients whose ligament ruptures cannot be maintained with closed reduction and percutaneous pinning, or those whose diagnosis is delayed beyond the acute healing phase.
Preoperative Preparation and Positioning
- Anesthesia and Tourniquet: Administer regional or general anesthesia. Apply a well-padded pneumatic tourniquet to the proximal arm.
- Positioning: Place the patient supine with the operative arm extended on a radiolucent hand table.
- Preparation: Prepare and drape the limb in a standard sterile fashion. Ensure fluoroscopy (C-arm) is readily available from the contralateral side of the table.
Surgical Exposure
Approach the wrist through combined dorsal and palmar incisions to achieve comprehensive exposure of the scapholunate articulations.
Dorsal Approach:
* Perform a longitudinal dorsal incision centered over the Lister tubercle.
* Develop the interval between the wrist extensors (ECRB/ECRL) and the finger extensors (EDC). Retract the tendons radially and ulnarward as needed.
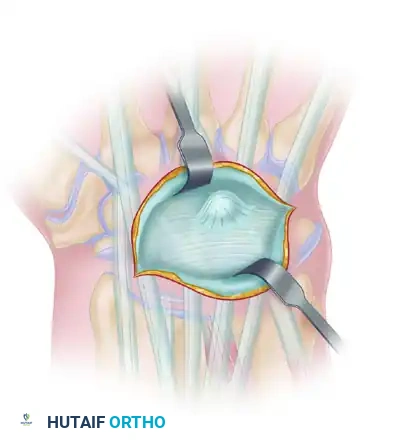
* Elevate a ligament-sparing dorsal capsular flap (e.g., Berger's approach) to expose the proximal carpal row.
Palmar Approach:
* Make a modified Henry approach or an extended carpal tunnel incision.
* Approach the radiovolar wrist capsule through the FCR sheath or slightly to its ulnar side.
* Retract the FCR tendon radially to protect it.
* Enter the capsule precisely at the scapholunate interval. Carefully incise the volar radioscaphocapitate (RSC) and radiolunate (RL) ligaments in a manner that allows for robust repair during capsular closure.
Carpal Reduction and Tunnel Preparation
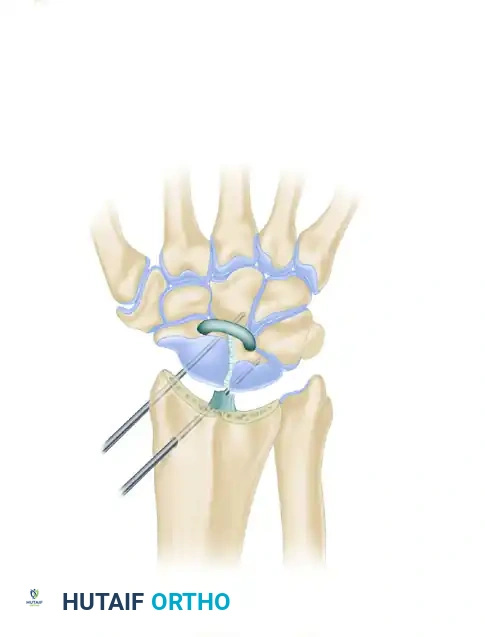
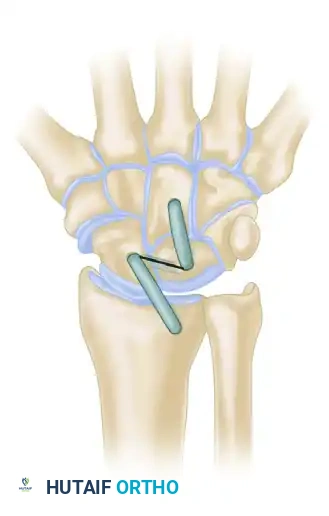
- Provisional Reduction: Debride the SL interval of fibrotic scar tissue. Anatomically reduce the scapholunate interval. Use 0.045-inch or 0.062-inch Kirschner wires as "joysticks" or toggle levers in the scaphoid and lunate to correct the rotary subluxation of the scaphoid and the dorsal intercalated segment instability (DISI) posture of the lunate.
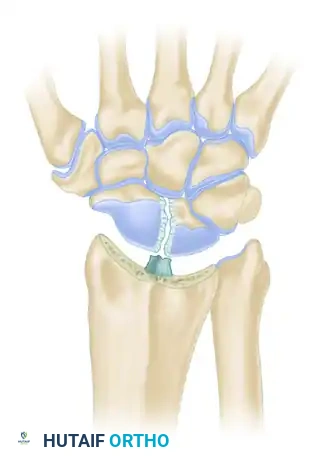
- Drilling Transosseous Tunnels: With the SL interval held in anatomic reduction, carefully drill holes through the scaphoid and lunate for tendon passage.
- Surgical Warning: Avoid fracturing through the delicate cortical surfaces between the scaphoid and lunate. Begin with small drill points (e.g., 1.5 mm) and enlarge the holes gradually using sequentially larger drill bits and hand curets until a 3.0 mm to 3.5 mm tunnel is achieved.

Graft Harvest and Routing
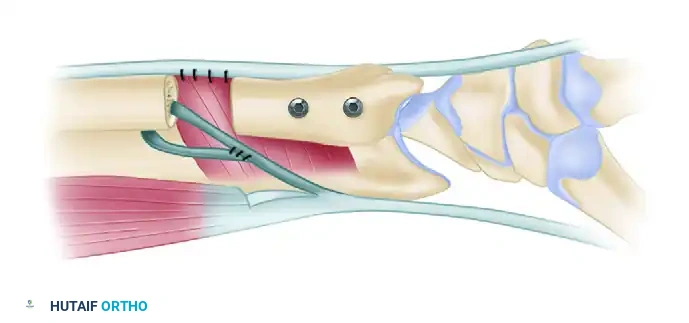
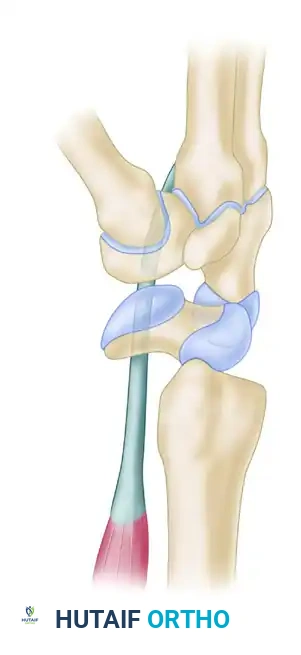
- FCR Preparation: Longitudinally incise the FCR tendon. Split a tendon slip approximately 2 to 4 mm wide, dissecting from the musculotendinous junction proximally down to its distal insertion at the base of the second metacarpal. Leave the distal insertion intact.
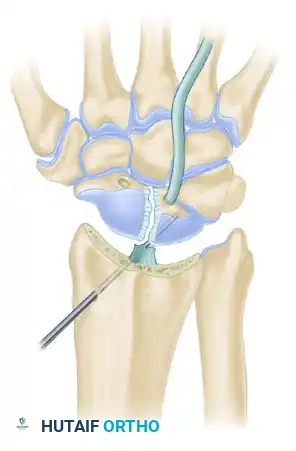
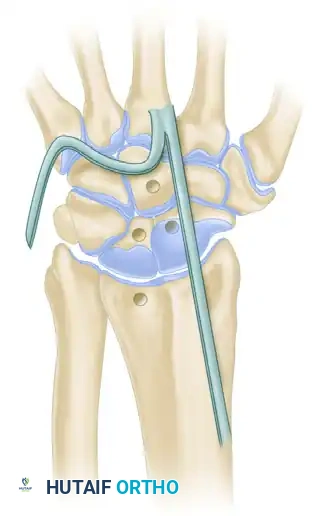
- Lunate Passage: Pass the harvested FCR tendon slip first through the lunate tunnel, routing it from palmar to dorsal.
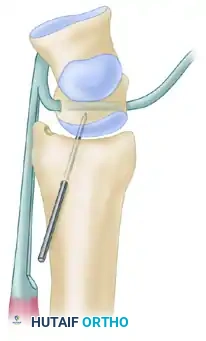
- Lunate Stabilization: With the wrist reduced, stabilize the lunate using a 0.062-inch (1.59-mm) Kirschner wire. Drill this wire from proximal to distal, starting through the radial metaphysis, crossing the radiocarpal joint, and embedding into the lunate. Note: Secure this K-wire stabilization only after the tendon graft has been successfully passed through the lunate.
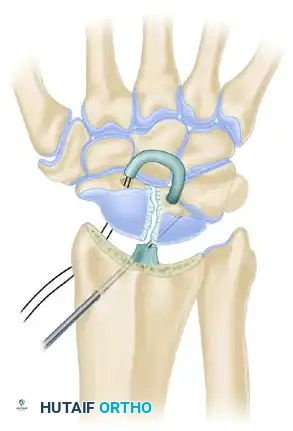
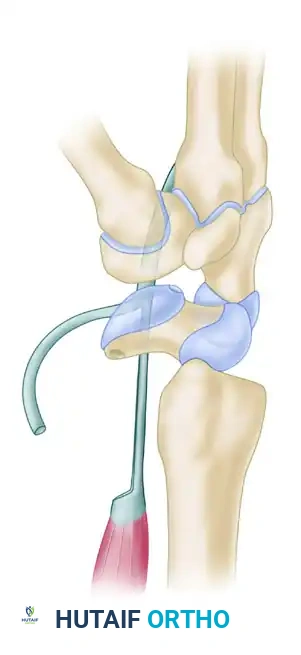
- Scaphoid Passage: Using wire loops or a suture passer, route the tendon slip from dorsal to palmar through the scaphoid drill hole. Apply tension to the graft. Attempt to slightly over-reduce the carpal bones in their alignment with each other and with the articular surface of the radius.
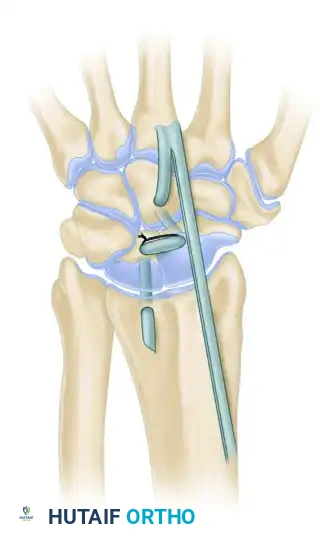
- Scaphoid Stabilization: Stabilize the scaphoid with a second 0.062-inch Kirschner wire, driven from the radial styloid/metaphysis into the scaphoid.
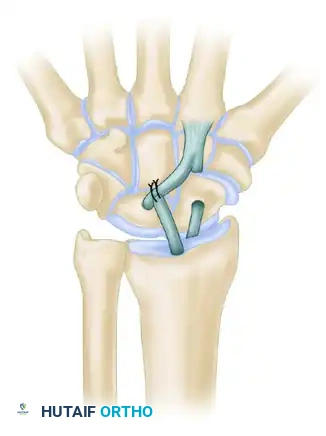
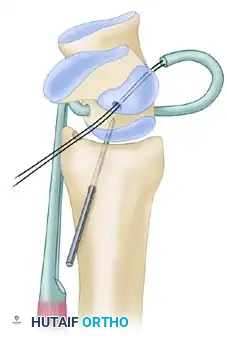
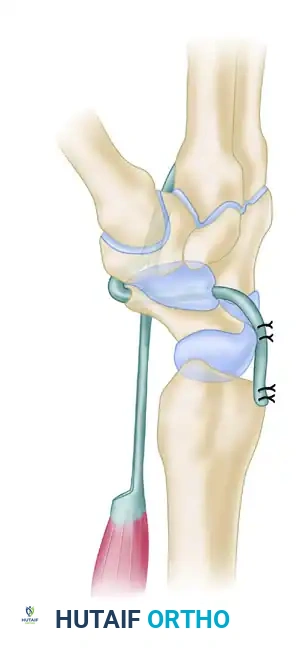
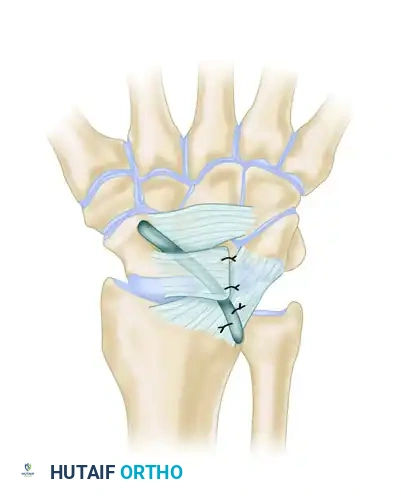
- Radial Passage and Fixation: Drill a final hole in the distal radius at the anatomical footprint of the radioscapholunate ligament. Pass the remaining tendon slip from palmar to dorsal—moving from an intraarticular position on the palmar surface to an extraarticular position on the dorsal surface. Tension the graft firmly and suture the FCR slip back onto itself dorsally using non-absorbable braided sutures.

Alternative Routing Technique: Palmer, Dobyns, and Linscheid also described an alternative sequence: passing the FCR tendon slip dorsally through the scaphoid initially, then palmarward through the lunate (from dorsal to palmar), and finally through the drill hole in the distal radius, suturing the slip to itself near its insertion.
Postoperative Care (Palmer Technique)
- Immediate Post-op: Close the capsule and wounds in layers. Immobilize the limb in a well-molded long-arm thumb spica cast. The wrist should be positioned in mild palmar flexion to offload the dorsal reconstruction, with the forearm in neutral rotation.
- 10 to 14 Days: Remove the skin sutures. Apply a new long-arm thumb spica cast.
- 6 Weeks: Remove the long-arm cast and transition the patient to a short-arm thumb spica cast for an additional 3 to 4 weeks.
- 8 to 10 Weeks: Remove all stabilizing Kirschner wires in the clinic. Initiate a supervised hand therapy program focusing on active and active-assisted range-of-motion exercises, followed gradually by progressive strengthening.
The Four-Bone Ligament Weave (Almquist et al.)
For patients with chronic, dynamic, or static scapholunate separation, Almquist et al. developed a highly successful four-bone ligament weave reconstruction. In their series, 86% of patients returned to preinjury activities at an average follow-up of 4.8 years.
Indications and Criteria
This specific procedure is indicated when the following criteria are met:
1. Complete scapholunate separation (no intact SLIL remnants).
2. A widely separated, freely movable scapholunate joint (reducible).
3. Absolute absence of radiocarpal or midcarpal arthrosis.
Surgical Execution
Instead of the FCR, this technique utilizes the Extensor Carpi Radialis Brevis (ECRB) tendon.
- Graft Preparation: Harvest exactly half of the ECRB tendon to serve as the new ligamentous complex.
- Tunnel Creation: Drill holes from dorsal to palmar through the nonarticular surfaces of four key structures: the capitate, the lunate, the scaphoid, and the distal radius.
- Weaving and Fixation: Route the split ECRB graft through these four tunnels to recreate the complex multidirectional stabilizing forces of the carpus.
- Internal Fixation: Unlike the Palmer technique which relies heavily on K-wires, the Almquist technique utilizes a 22-gauge wire loop as the sole internal fixation device to hold the scapholunate dissociation reduced while the tendon graft heals.
Stabilization of Rotary Subluxation (Brunelli and Brunelli)
Brunelli and Brunelli introduced a targeted reconstructive technique specifically designed to address the rotary subluxation of the scaphoid, a hallmark of advanced SL instability. This procedure effectively tethers the distal pole of the scaphoid to prevent its abnormal palmar flexion.
Surgical Execution
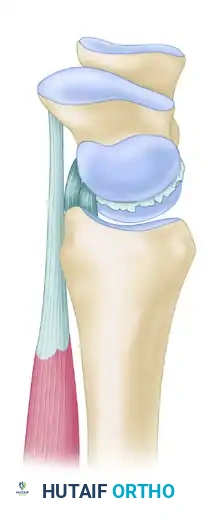
- Graft Harvest: Similar to the Palmer technique, a distally based slip of the flexor carpi radialis (FCR) tendon is harvested.
- Scaphoid Tunnel: A transosseous tunnel is created in the distal pole of the scaphoid. Crucially, this tunnel must be drilled parallel to the distal articular surface of the scaphoid to avoid violating the scaphotrapezial joint.
- Graft Passage and Tensioning: The prepared FCR tendon slip is passed through this distal scaphoid tunnel from palmar to dorsal.
- Reduction: The tendon slip is pulled firmly in a dorsal direction. This vector of pull directly counteracts and reduces the rotary subluxation (palmar flexion) of the scaphoid.
- Final Fixation: Once anatomic reduction is achieved and provisionally pinned, the FCR slip is sutured securely to the robust fibrous elements of the dorsal radiolunate ligament and the dorsal capsule of the distal radius, creating a strong dorsal tether.
Complications and Salvage
Despite meticulous surgical technique, ligament reconstruction of the wrist carries a high complication profile.
* Stiffness: The most common complication is a permanent loss of wrist flexion and extension. Patients must be educated that the primary goal of surgery is pain relief and stability, not the restoration of normal motion.
* Hardware Failure: Kirschner wires may migrate, break, or cause pin-tract infections. They must be monitored radiographically during the 8-to-10-week immobilization period.
* Graft Attenuation: Over years, the tendon graft may stretch, leading to recurrent SL gap formation and eventual SLAC wrist progression.
* Avascular Necrosis: Aggressive drilling of the scaphoid or lunate can disrupt their tenuous intraosseous blood supply, leading to partial or complete avascular necrosis (Preiser's or Kienböck's-like changes).
If ligament reconstruction fails or if the patient develops progressive radiocarpal arthrosis, the surgeon must be prepared to transition to salvage procedures. Proximal row carpectomy (PRC) or scaphoid excision with four-corner arthrodesis remain the gold standards for managing the painful, arthritic, and unstable wrist following failed soft-tissue reconstruction.
📚 Medical References
- ligament reconstruction in 6 patients, Acta Orthop Scand 73:663, 2002.
- El-Khoury GY, Terepka RH, Mickelson MR, et al: Fineneedle aspiration biopsy of bone, J Bone Joint Surg 65A:522, 1983.
- Enneking WF: Modifi cation of the system for functional evaluation of surgical management of musculoskeletal tumors in limb salvage of musculoskeletal tumors. In Enneking WF: Limb salvage in musculoskeletal oncology, New York, 1987, Churchill Livingstone. Enneking WF, Dunham WK: Resection and reconstruction for primary neoplasms involving the innominate bone, J Bone Joint Surg 60A:731, 1978.
- Enneking WF, Maale GE: The effect of inadvertent tumor contamination of wounds during the surgical resection of musculoskeletal neoplasms, Cancer 62:1251, 1988.
- Enneking WF, Shirley PD: Resection-arthrodesis for malignant and potentially malignant lesions about the knee using an intramedullary rod and local bone grafts, J Bone Joint Surg 59A:223, 1977.
- Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma, Clin Orthop Relat Res 153:106, 1980.
- Erlemann R, Sciuk J, Bosse A, et al: Response of osteosarcoma and Ewing sarcoma to preoperative chemotherapy: assessment with dynamic and static MR imaging and skeletal scintigraphy, Radiology 175:791, 1990.
- Esther RJ, Bos GD: Management of metastatic disease of other bones, Orthop Clin North Am 31:647, 2000.
- Exner GU, von Hochstetter AR, Augustiny N, et al: Magnetic resonance imaging in malignant bone tumours, Int Orthop 14:49, 1990.
- Fabrizio PL, Stafford SL, Pritchard DJ: Extremity soft-tissue sarcomas selectively treated with surgery alone, Int J Radiat Oncol Biol Phys 48:227, 2000.
- Feigenberg SJ, Marcus RB, Zlotecki RA, et al: Radiation therapy for giant cell tumors of bone, Clin Orthop Relat Res 411:207, 2003.
- Ferracini R, Gino G, Battiston B, et al: Assessment of vascularized fi bular graft one year after reconstruction of the wrist after excision of a giant-cell tumor, J Hand Surg 24B:497, 1999.
- Ferracini R, Masterson EL, Bell RS, et al: Distal ulnar tumours: results of management by en bloc resection in nine patients and review of the literature, J Hand Surg 23B:517, 1998.
- Finn HA, Nicholas RW, Webb JE: Skeletal reconstruction with allograft segments following bone tumor resection, Contemp Orthop 21:455, 1990.
- Finn HA, Simon MA: Staging systems for musculoskeletal neoplasms, Orthopedics 12:1365, 1989.
- Fleming ID, Cooper JS, Henson DE, et al, eds: AJCC cancer staging manual, 5th ed, Philadelphia, 1997, Lippincott-Raven. Forest M, Tomeno B, Vanel D, eds: Orthopedic surgical pathology: diagnosis of tumors and pseudotumoral lesions of bones and joints, Edinburgh, 1998, Churchill Livingstone. Frassica DA, Thurman S, Welsh J: Radiation therapy, Orthop Clin North Am 31:557, 2000.
- Frassica FJ, Frassica DA, McCarthy EF, et al: Metastatic bone disease: evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management, Instr Course Lect 49:453, 2000.
- Frassica FJ, McCarthy EF, Bluemke DA: Soft-tissue masses: when and how to biopsy, Instr Course Lect 49:437, 2000.
- Freiberg AA, Loder RT, Heidelberger KP, et al: Aneurysmal bone cysts in young children, J Pediatr Orthop 14:86, 1994.
- Friedlaender GE, Mankin HJ: Transplantation of osteochondral allografts, Annu Rev Med 35:311, 1984.
- Fuchs B, Davis AM, Wunder JS, et al:
You Might Also Like