Rheumatoid Finger Deformities: Pathomechanics and Surgical Management

Key Takeaway
Rheumatoid arthritis induces complex finger deformities through synovial proliferation, capsular attenuation, and musculotendinous imbalance. This comprehensive guide details the pathomechanics, clinical evaluation, and step-by-step surgical management of intrinsic plus and swan-neck deformities. Key concepts include the Bunnell test for intrinsic tightness, the Nalebuff classification for swan-neck deformities, and evidence-based operative interventions ranging from soft tissue releases and flexor tenodesis to proximal interphalangeal joint arthrodesis and arthroplasty.
FINGER DEFORMITIES CAUSED BY RHEUMATOID ARTHRITIS
The rheumatoid hand represents one of the most complex biomechanical challenges in orthopedic surgery. Finger deformities in rheumatoid arthritis (RA) are rarely the result of a single isolated structural failure; rather, they are caused by the normal physiological forces applied by extrinsic flexors and extensors acting upon joints that have been progressively weakened and destabilized by infiltrative synovitis.
The pathogenesis is multifactorial, involving tightness of the intrinsic muscles, displacement of the lateral bands of the extensor hood, central slip rupture, or the attenuation and rupture of the long extensor or long flexor tendons. Furthermore, flexor tenosynovitis frequently produces a mechanical limitation of interphalangeal joint motion. In these cases, the range of active flexion of the interphalangeal joints is significantly less than passive flexion, a critical clinical distinction that dictates surgical decision-making.
INTRINSIC PLUS DEFORMITY
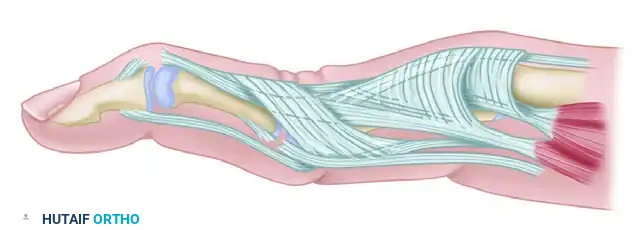
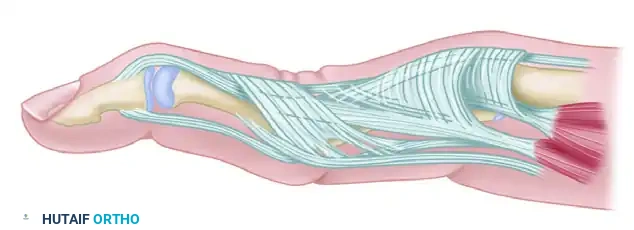
The intrinsic plus deformity is a hallmark of the rheumatoid hand, driven by intrinsic muscle tightness, spasticity, and eventual fibrotic contracture. The intrinsic muscles (lumbricals and interossei) pass volar to the metacarpophalangeal (MCP) joint axis and dorsal to the proximal interphalangeal (PIP) joint axis. When contracted, they force the hand into the "intrinsic plus" posture: MCP joint flexion and PIP joint extension.
In advanced rheumatoid hands with intrinsic plus deformity, the PIP joint cannot be passively flexed while the MCP joint is held in full extension. This deformity frequently develops in tandem with volar subluxation of the MCP joints and ulnar deviation of the digits, creating a complex, multi-planar collapse pattern.
Clinical Evaluation: The Bunnell Test
The Bunnell test (also known as the intrinsic tightness test) is the gold standard for evaluating intrinsic muscle contracture. The test compares the degree of passive PIP joint flexion under two distinct conditions:
1. MCP Joint in Full Extension: This position stretches the intrinsic muscles.
2. MCP Joint in Full Flexion: This position relaxes the intrinsic muscles.
Variable degrees of passive PIP joint flexion loss when the MCP joint is held in extension indicate intrinsic tightness.

Clinical Pearl: Avoiding False Negatives in the Bunnell Test
In the presence of ulnar drift of the fingers, intrinsic tightness may be predominantly or exclusively present on the ulnar side. To test this accurately, strict axial alignment of the finger with the metacarpal must be maintained by the examiner. Any ulnar deviation at the MCP joint during the test will slacken the intrinsic muscles on the ulnar side of the finger, potentially masking the tightness and confusing the clinical findings.
A tight first volar interosseous muscle will pull the extended index finger ulnarward. If the finger is held in strict neutral alignment, the tightness becomes immediately apparent as resistance to PIP flexion.
Surgical Management: Intrinsic Release
When intrinsic tightness limits function and contributes to progressive deformity, surgical release is indicated. The goal is to resect the oblique fibers of the intrinsic wing tendon that extend to the lateral bands, thereby removing the deforming extension force on the PIP joint while preserving the transverse fibers that flex the MCP joint.
Surgical Steps for Intrinsic Release:
1. Incision: A dorsal longitudinal or curvilinear incision is made over the proximal phalanx.
2. Exposure: The extensor hood is exposed. The intrinsic tendon is identified as it fans out into the transverse and oblique fibers.
3. Resection: A triangular segment of the oblique fibers of the intrinsic expansion is excised bilaterally (or unilaterally on the ulnar side if only ulnar intrinsic tightness is present).
4. Verification: The Bunnell test is repeated intraoperatively. Full passive PIP flexion should now be achievable with the MCP joint fully extended.
SWAN-NECK DEFORMITY
The swan-neck deformity is characterized by hyperextension of the PIP joint and flexion of the distal interphalangeal (DIP) joint. In the rheumatoid hand, this deformity can originate from primary pathology at the DIP joint, the PIP joint, or the MCP joint.
Pathomechanics of Swan-Neck Deformity
1. DIP Joint Origin (Terminal Tendon Rupture):
Terminal tendon rupture or attenuation may be associated with infiltrative synovitis of the DIP joint. This leads to a primary mallet deformity (DIP flexion). The loss of terminal extensor tension causes secondary overpull of the central slip at the PIP joint, driving secondary PIP joint hyperextension.
2. PIP Joint Origin (Capsular Disruption and Lateral Band Subluxation):
The deformity frequently begins directly at the PIP joint. Aggressive synovitis causes disruption of the volar plate and capsular structures. This allows the lateral bands and central tendon to tighten and eventually adhere in a fixed, dorsal position. Because they are fixed dorsally, the lateral bands can no longer slide volarly over the condyles during PIP flexion, severely limiting PIP joint flexion. Furthermore, these dorsally and centrally displaced lateral bands become relatively slack distally, rendering them ineffective at extending the DIP joint, which secondarily assumes a mallet posture.
3. Flexor Tenosynovitis and FDS Incompetence:
Flexor tenosynovitis results in ineffective volar support by the flexor digitorum superficialis (FDS) tendon. The loss of FDS tension, combined with the overpull of the central tendon slip and PIP synovitis, stretches the volar restraints, initiating the hyperextended swan-neck position.


The Nalebuff Classification and Treatment Algorithm
Nalebuff, Feldon, and Millender categorized rheumatoid swan-neck deformities into four distinct types based on PIP joint flexibility and radiographic joint preservation. This classification is paramount for guiding surgical intervention.
Type I: Flexible Deformity
- Characteristics: The PIP joint is flexible in all positions of the MCP joint. The deformity is primarily driven by PIP hyperextension with secondary DIP flexion.
- Treatment: The goal is to restrict PIP hyperextension while restoring DIP extension. Options include:
- Dermodesis: Excision of an elliptical wedge of volar skin at the PIP joint to create a dermal flexion contracture.
- Flexor Tenodesis (FDS Tenodesis): Utilizing one slip of the FDS to tether the PIP joint in slight flexion.
- Retinacular Ligament Reconstruction: Reconstructing the oblique retinacular ligament to link PIP extension to DIP extension.
- DIP Joint Fusion: Often performed concomitantly to correct the terminal mallet deformity.
Type II: Intrinsic Tightness Dependent
- Characteristics: PIP joint flexion is limited only when the MCP joint is extended (positive Bunnell test). The deformity is caused by intrinsic muscle tightness.
- Treatment: Requires an intrinsic release to decompress the extensor mechanism, in addition to one or more of the procedures utilized for Type I deformities (e.g., FDS tenodesis) to correct the volar plate laxity.
Type III: Stiff Deformity with Preserved Joint Space
- Characteristics: The PIP joint is stiff and does not allow satisfactory flexion regardless of MCP position. However, radiographs demonstrate a well-preserved PIP joint space without significant cartilaginous destruction.
- Treatment: Soft tissue reconstruction is still viable but requires extensive release.
- Joint Manipulation and Mobilization: Careful closed manipulation.
- Lateral Band Mobilization: Releasing the adherent lateral bands from their fixed dorsal position, allowing them to subluxate volarly during flexion.
- Dorsal Skin Release: Wrinkles and normal laxity of the skin are lost at the PIP joint level after several weeks of fixed hyperextension. A dorsal skin release or local flap may be necessary to permit PIP flexion.
- Dorsoproximal Interphalangeal Capsulotomy: May improve interphalangeal flexion by changing the arc of motion.
Type IV: Stiff Deformity with Joint Destruction
- Characteristics: Fixed PIP joint hyperextension with radiographic evidence of advanced intra-articular destruction, cartilage loss, and erosions.
- Treatment: Soft tissue procedures will fail. Osseous stabilization is required.
- PIP Joint Arthrodesis: The gold standard for the index and middle fingers to provide a stable pinch post.
- PIP Joint Arthroplasty: May be considered in the ring and small fingers (to preserve grip span) only if the MCP joints are well preserved and stable.

OPERATIVE TECHNIQUES FOR SWAN-NECK DEFORMITY
Flexor Sublimis Tenodesis (FDS Tenodesis)
For Type I and Type II deformities where volar plate attenuation is the primary driver of PIP hyperextension, an FDS tenodesis provides a robust volar tether. The Curtis or Beckenbaugh techniques are most commonly employed.
Surgical Steps:
1. Approach: A volar Bruner or mid-lateral incision is made over the PIP joint and proximal phalanx.
2. Tendon Harvest: The flexor sheath is opened (preserving the A2 and A4 pulleys). One slip of the FDS tendon is identified and divided proximally at the level of the A1 pulley, leaving its distal insertion intact.
3. Tenodesis Creation: The harvested FDS slip is routed volarly and anchored into the proximal phalanx.
4. Tensioning: The tendon is tensioned to hold the PIP joint in approximately 20 to 30 degrees of flexion. Fixation can be achieved using a bone anchor, pull-out suture, or intraosseous routing.
Surgical Warning: Over-tensioning the Tenodesis
A primary complication of FDS tenodesis is a progressive flexion contracture of the PIP joint that may exceed 30 degrees. Precise tensioning is critical. Postoperative immobilization of the joint is generally unnecessary; immediate active movement of the joint without protective splinting is encouraged to prevent severe stiffness, relying on the tenodesis to block terminal extension.
Proximal Interphalangeal Joint Arthrodesis
For Type IV deformities, or severe Type III deformities where soft tissue reconstruction is deemed unreliable, PIP arthrodesis provides definitive correction and pain relief. If MCP joint arthroplasty is anticipated in the future, a stable, fused PIP joint is an absolute prerequisite.
Surgical Steps:
1. Approach: A dorsal longitudinal or lazy-S incision is made over the PIP joint.
2. Extensor Mechanism: The central slip is divided, and the collateral ligaments are excised to fully expose the joint surfaces.
3. Joint Preparation: The destroyed articular cartilage and subchondral bone are resected. A cup-and-cone reamer system or flat oscillating saw cuts can be used. The joint is positioned in functional flexion (typically 25° for the index finger, increasing by 5° for each ulnar digit, up to 40° for the small finger).
4. Fixation: Numerous fixation techniques have been described to obtain successful PIP arthrodesis in osteopenic rheumatoid bone. Options include:
* Single or crossed Kirschner wires (K-wires).
* Intraosseous wiring (90-90 wiring technique).
* Tension band wiring.
* Dorsal mini-plates or compression plates.
* Headless compression subchondral screws.
5. Closure: The extensor mechanism is reapproximated over the hardware to provide soft tissue coverage, and the skin is closed.
Postoperative Protocol:
Unlike tenodesis, arthrodesis requires strict immobilization. The digit is placed in a protective splint for 4 to 6 weeks until radiographic evidence of trabecular bridging is observed. Active ROM of the MCP and DIP joints is encouraged immediately to prevent adjacent joint stiffness.
CONCLUSION
The surgical management of rheumatoid finger deformities demands a profound understanding of hand biomechanics and the specific pathological cascade initiated by rheumatoid synovitis. By meticulously evaluating intrinsic tightness via the Bunnell test and accurately classifying swan-neck deformities using the Nalebuff system, the orthopedic surgeon can select the appropriate intervention—ranging from targeted soft tissue releases to definitive arthrodesis—to restore function and alleviate pain in the rheumatoid hand.
You Might Also Like

