Mastering the Diagnosis and Management of Wrist Conditions

Key Takeaway
Diagnosing wrist conditions requires a profound understanding of carpal kinematics, precise clinical examination, and a structured imaging algorithm. This guide covers Taleisnik’s columnar theory, Lichtman’s ring concept, and Mayfield’s stages of perilunar instability. It provides orthopaedic surgeons with an evidence-based framework for evaluating wrist trauma, differentiating soft tissue from osseous pathology, and executing appropriate surgical interventions for carpal instability.
INTRODUCTION TO WRIST PATHOLOGY
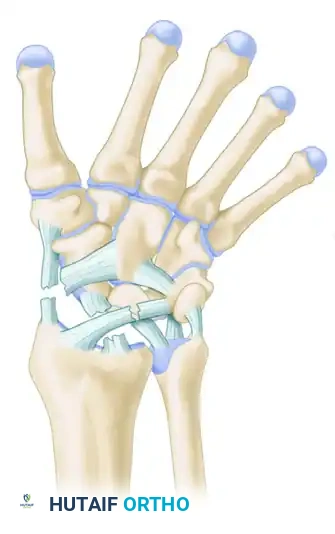
The human wrist is an intricate biomechanical marvel, comprising eight carpal bones, multiple articulating surfaces, and a complex network of intrinsic and extrinsic ligaments. The diagnosis of wrist conditions—whether acute traumatic injuries or chronic degenerative pathologies—demands a meticulous, systematic approach. For the orthopaedic surgeon, mastering the diagnostic algorithm is paramount to preventing long-term sequelae such as carpal collapse, chronic instability, and post-traumatic osteoarthritis (e.g., Scapholunate Advanced Collapse [SLAC] or Scaphoid Nonunion Advanced Collapse [SNAC]).
This comprehensive guide delineates the critical components of clinical evaluation, advanced biomechanical concepts, imaging algorithms, and surgical management strategies for wrist conditions, tailored for the postgraduate orthopaedic practitioner.
COMPREHENSIVE CLINICAL HISTORY
A precise clinical history is the cornerstone of accurate diagnosis. The clinician must document standard demographic data, including age, hand dominance, occupation, and hobbies, as these factors directly influence surgical decision-making and postoperative rehabilitation goals.
Mechanism of Injury
When evaluating traumatic wrist conditions, the exact mechanism of injury is frequently unknown to the patient, yet it dictates the resulting pattern of carpal disruption. Carpal injuries represent a continuous spectrum of tissue failure. The severity and specific pattern of injury depend on four critical variables:
1. Loading in Three Dimensions: The magnitude and vector of the applied force.
2. Duration and Amplitude of Forces: High-energy, rapid-loading events (e.g., motor vehicle accidents) produce different failure patterns than low-energy, sustained loads.
3. Hand Position at Impact: The degree of wrist extension, ulnar or radial deviation, and intercarpal supination at the moment of impact determines which ligamentous structures are tensioned and subsequently fail.
4. Inherent Ligamentous Laxity: Patient-specific collagen composition and baseline hyperlaxity.
Clinical Pearl: Always inquire about modifying factors (e.g., response to NSAIDs, cold, heat, or corticosteroid injections) and previous wrist injuries. Furthermore, documenting current work status and the existence of medicolegal concerns (e.g., workers’ compensation, disability claims, or pending litigation) is essential for assessing the patient's overall psychosocial situation and potential secondary gain.
BIOMECHANICS AND CARPAL KINEMATICS
To accurately diagnose wrist instability, the surgeon must possess a profound understanding of carpal kinematics. Two primary biomechanical models dominate contemporary orthopaedic thought: Taleisnik’s Columnar Concept and Lichtman’s Ring Concept.
Taleisnik’s Columnar Concept
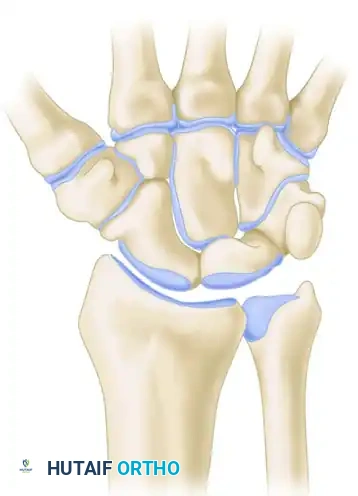
Taleisnik proposed that the wrist functions via three distinct longitudinal columns:
* The Central (Flexion-Extension) Column: Comprises the entire distal carpal row (trapezium, trapezoid, capitate, hamate) and the lunate. This column is primarily responsible for the transmission of flexion and extension forces.
* The Lateral (Mobile) Column: Consists solely of the scaphoid, which bridges the proximal and distal rows, providing critical stability and mobility.
* The Medial (Rotary) Column: Comprises the triquetrum, functioning as a pivot point for carpal rotation.
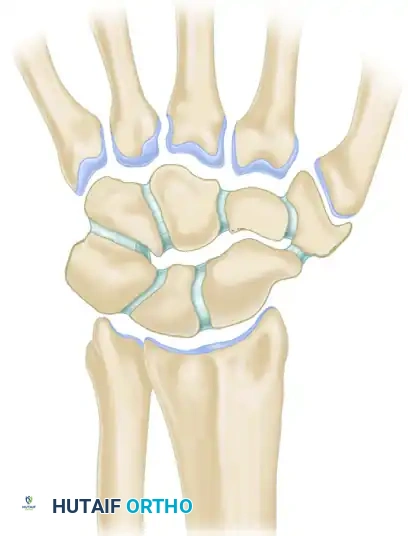
Lichtman’s Ring Concept
Lichtman expanded upon carpal kinematics by describing the carpus as an oval ring. In this model, the proximal and distal carpal rows act as semirigid posts stabilized by robust interosseous ligaments.
* Normal, controlled mobility occurs primarily at the scaphotrapezial and triquetrohamate joints.
* Pathomechanics: Any break in this ring—whether osseous (e.g., scaphoid fracture) or ligamentous (e.g., scapholunate dissociation)—destabilizes the kinematic chain.
Depending on the location of the break, the lunate will fall into an abnormal posture, producing either a Dorsal Intercalated Segmental Instability (DISI) or a Volar Intercalated Segmental Instability (VISI) deformity.
THE SPECTRUM OF PERILUNAR INSTABILITY (MAYFIELD STAGES)
Mayfield, Johnson, and Kilcoyne classically described the progressive stages of perilunar instability resulting from wrist hyperextension, ulnar deviation, and intercarpal supination. This sequential failure occurs in four distinct stages around the lunate.
Stage I: Scapholunate Dissociation
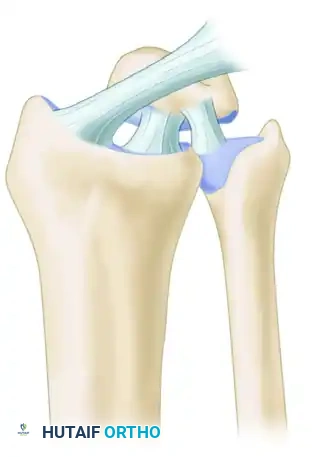
The injury initiates radially with the disruption of the scapholunate (SL) interosseous ligament and the volar radioscaphocapitate ligament. This results in rotatory subluxation of the scaphoid.
Stage II: Capitolunate Disruption
As the force propagates ulnarly, the space of Poirier (a weak area in the volar capsule between the capitate and lunate) is breached. The capitate subluxates dorsally relative to the lunate.
Stage III: Lunotriquetral Disruption (Perilunate Dislocation)
The force continues through the lunotriquetral (LT) interosseous ligament. The entire carpus dislocates dorsally, leaving only the lunate articulated with the distal radius.
Stage IV: Lunate Dislocation
The final stage involves the failure of the dorsal radiocarpal ligament. The capitate is driven proximally, forcing the lunate to rotate and dislocate volarly into the carpal tunnel, often causing acute median nerve compression.
Surgical Warning: A Stage IV lunate dislocation is an orthopaedic emergency. Acute median neuropathy requires immediate closed reduction and subsequent urgent surgical stabilization to prevent irreversible nerve damage and avascular necrosis of the lunate.
PHYSICAL EXAMINATION OF THE WRIST
A careful, detailed examination must be conducted with the forearm and hand fully supported, regardless of whether the evaluation is performed immediately post-injury or for chronic, insidious problems.
Inspection and Palpation
In addition to the standard assessment of motor, sensory, and circulatory integrity, the surgeon must correlate the patient’s subjective complaints with the underlying anatomical structures.
* Document all scars, ecchymosis, swelling, and muscle atrophy.
* Measure active and passive range of motion (ROM) using a goniometer, comparing findings to the contralateral, uninjured side.
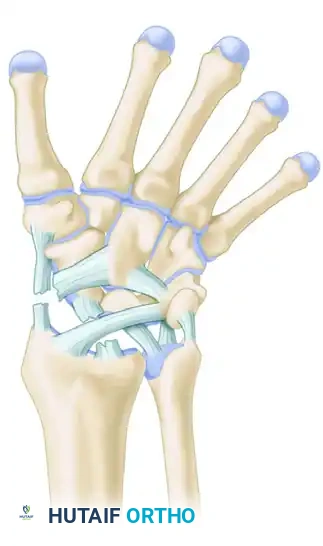
The underlying anatomy must be correlated with easily identified and palpable bony landmarks:
* Radial Styloid & Scaphoid Tuberosity: Tenderness here may indicate scaphoid fractures or scaphotrapezial arthritis.
* Lister’s Tubercle: Acts as a pulley for the Extensor Pollicis Longus (EPL). Tenderness can indicate EPL tenosynovitis or impending rupture following a distal radius fracture.
* Ulnar Styloid & Pisiform: Tenderness may point to Triangular Fibrocartilage Complex (TFCC) tears, extensor carpi ulnaris (ECU) subluxation, or pisotriquetral arthritis.
Differentiating Pathology
It is critical to differentiate overlying superficial tenosynovitis from deep articular or ligamentous pathology.
* First Dorsal Compartment: Pain over the radial styloid exacerbated by Finkelstein's test indicates de Quervain tenosynovitis. This must be distinguished from thumb carpometacarpal (CMC) osteoarthritis (positive grind test) or scaphoid pathology.
* Nerve Compression: Evaluate for carpal tunnel syndrome (median nerve), cubital tunnel or Guyon's canal syndrome (ulnar nerve), and Wartenberg's syndrome (superficial radial nerve) using Tinel's sign and provocative compression tests.
DIAGNOSTIC IMAGING ALGORITHM
The radiographic evaluation of the painful wrist follows a strict, stepwise algorithm to ensure no subtle instability or occult fracture is missed.
1. Routine Radiography
The initial evaluation must always include four standard views:
* Posteroanterior (PA): Assesses carpal arcs (Gilula's lines), ulnar variance, and joint space narrowing.
* Lateral: Evaluates carpal alignment (collinear relationship of the radius, lunate, and capitate) and measures the scapholunate angle (normal 30°-60°) and capitolunate angle (normal <15°).
* Oblique: Excellent for visualizing the scaphotrapezial joint and the dorsal aspect of the triquetrum.
* Scaphoid View: A PA view with the wrist in ulnar deviation and slight extension to elongate the scaphoid and identify occult waist fractures.
2. Advanced and Dynamic Imaging
If routine radiographs are normal but clinical suspicion remains high, the algorithm progresses:
* Instability Series / Fluoroscopy: Patients with suspected ligamentous instability require dynamic imaging (clenched fist views, radial/ulnar deviation views). Abnormal motion, widening of the SL interval (>3mm, "Terry Thomas sign"), or palpable popping must be reproduced and observed fluoroscopically.
* Spot Films: Targeted views of the maximally painful area.
* MRI / CT Scan:
* CT Scan: The gold standard for evaluating osseous anatomy, fracture union, and preoperative planning for intra-articular distal radius fractures.
* MRI: Highly sensitive for occult fractures, avascular necrosis (Kienböck's or Preiser's disease), and intrinsic ligament or TFCC tears.
* Bone Scan: Utilized when MRI is contraindicated or to localize an obscure source of osteoblastic activity.
* Wrist Arthrogram: Historically used for ligamentous tears, though largely supplanted by high-resolution 3T MRI. It remains useful when combined with fluoroscopy or MRI (MR Arthrography) to detect subtle capsular or cartilage defects.
SURGICAL MANAGEMENT AND APPROACHES
When conservative measures fail, or in the presence of acute instability (e.g., perilunate dislocations, acute SL tears), surgical intervention is mandated.
Indications for Surgery
- Acute perilunate dislocations (Mayfield Stages II-IV).
- Acute scapholunate or lunotriquetral ligament ruptures with demonstrable dynamic or static instability.
- Displaced intra-articular fractures of the distal radius or carpus.
- Chronic instability leading to early SLAC/SNAC wrist changes (salvage procedures).
Patient Positioning and Setup
- Position: The patient is placed supine with the operative extremity extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic tourniquet is applied to the proximal arm (typically inflated to 250 mmHg after exsanguination).
- Equipment: Mini-C-arm fluoroscopy must be positioned perpendicular to the hand table to allow for dynamic intraoperative imaging without compromising the sterile field.
The Dorsal Approach to the Wrist
The dorsal approach provides excellent exposure to the proximal carpal row, midcarpal joint, and distal radius.
1. Incision: A longitudinal incision is made centered over Lister’s tubercle, extending from the distal radius to the base of the third metacarpal.
2. Dissection: The extensor retinaculum is exposed. The third extensor compartment is opened, and the EPL tendon is transposed radially.
3. Retinacular Flaps: The second and fourth compartments are elevated subperiosteally to preserve their gliding layers.
4. Capsulotomy: A ligament-sparing capsulotomy (e.g., Berger’s dorsal intercarpal ligament-splitting approach or a tissue-preserving flap) is performed to expose the radiocarpal and midcarpal joints.
5. Intervention: Direct repair of the SL ligament using suture anchors, combined with dorsal capsulodesis if necessary. The carpus is anatomically reduced and stabilized with multiple 0.045-inch or 0.062-inch Kirschner wires (K-wires).
6. Closure: The capsule is meticulously repaired to prevent dorsal intercalated instability. The EPL is left transposed in the subcutaneous tissue to prevent attrition rupture.
The Volar Approach (Extended Carpal Tunnel)
Required for Stage IV lunate dislocations to decompress the median nerve and repair the volar capsular rents (Space of Poirier).
1. Incision: An extended carpal tunnel incision is utilized, crossing the wrist crease obliquely to prevent flexion contractures.
2. Decompression: The transverse carpal ligament is divided, decompressing the median nerve.
3. Reduction: The dislocated lunate is identified, and the volar radiocarpal ligaments are inspected. The lunate is gently reduced dorsally into the lunate fossa using a joystick technique with K-wires.
4. Repair: The robust volar ligaments (radioscaphocapitate and radiolunotriquetral) are repaired using heavy non-absorbable sutures or anchors.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of wrist surgery is heavily dependent on strict adherence to postoperative rehabilitation protocols.
- Phase I (0-2 Weeks): The wrist is immobilized in a bulky plaster splint. Elevation and active range of motion of the digits, elbow, and shoulder are initiated immediately to prevent stiffness and complex regional pain syndrome (CRPS).
- Phase II (2-8 Weeks): Sutures are removed at 10-14 days. The patient is transitioned to a custom-molded thermoplastic short-arm cast or rigid splint. K-wires (if used for carpal stabilization) remain in place for 8 weeks to allow for adequate ligamentous healing.
- Phase III (8-12 Weeks): K-wires are removed in the clinic. The patient begins a formal hand therapy program focusing on active and active-assisted ROM. Passive stretching and aggressive mobilization are strictly avoided to prevent stretching out the newly repaired ligaments.
- Phase IV (12+ Weeks): Progressive strengthening is introduced. Patients are counseled that maximal medical improvement may take up to 12 months, and a mild permanent loss of terminal flexion and extension is expected following major carpal reconstructive surgery.
CONCLUSION
The diagnosis and management of wrist conditions require a masterful synthesis of patient history, advanced biomechanical knowledge, precise physical examination, and targeted imaging. By understanding the kinematic interplay of Taleisnik’s columns and Lichtman’s ring, and by recognizing the progressive stages of Mayfield’s perilunar instability, the orthopaedic surgeon can confidently navigate the complexities of wrist pathology. Prompt, accurate diagnosis followed by meticulous surgical execution and structured rehabilitation ensures the optimal restoration of wrist function and the prevention of debilitating degenerative collapse.
You Might Also Like

