Combination Tenodesis of the Flexor Carpi Ulnaris and Extensor Carpi Ulnaris: A Comprehensive Surgical Guide

Key Takeaway
The combination tenodesis of the flexor carpi ulnaris (FCU) and extensor carpi ulnaris (ECU), modified by Jupiter and Breen, is a robust salvage procedure for distal radioulnar joint instability. By utilizing both tendons, this technique provides dynamic and static stabilization of the distal ulnar stump, effectively preventing radioulnar convergence following distal ulna resection. This guide details the biomechanical rationale, precise surgical approaches, tendon routing, and postoperative rehabilitation protocols.
Introduction to Distal Radioulnar Joint Stabilization
The stability of the distal radioulnar joint (DRUJ) is paramount for the fluid, pain-free pronation and supination of the forearm. When the DRUJ is irreparably damaged—whether through severe rheumatoid arthritis, post-traumatic osteoarthritis, or a previously failed Darrach procedure—resection of the distal ulna is often indicated. However, simple resection can lead to a highly problematic complication: painful radioulnar convergence and instability of the distal ulnar stump.
To combat this, the Combination Tenodesis of the Flexor Carpi Ulnaris (FCU) and the Extensor Carpi Ulnaris (ECU) was developed. Originally conceptualized and later modified by Jupiter and Breen, this sophisticated salvage procedure creates a robust, dynamic, and static soft-tissue sling. By tethering the unstable ulnar stump using slips from both the FCU and ECU, the surgeon can effectively suspend the ulna, preventing it from impinging upon the radius during forceful grip and forearm rotation.
This comprehensive guide provides a masterclass on the Jupiter and Breen modified technique, detailing the biomechanical principles, precise surgical steps, and rigorous postoperative protocols required to achieve optimal outcomes in complex DRUJ reconstructions.
Biomechanical Rationale
Understanding the biomechanics of the forearm is critical when performing a combination tenodesis. The radius rotates around the fixed ulna during pronation and supination. Following a distal ulnar resection, the loss of the triangular fibrocartilage complex (TFCC) and the bony articulation removes the primary stabilizers of the DRUJ.
Without these stabilizers, the pull of the pronator quadratus and the brachioradialis draws the distal ulnar stump radially, causing painful impingement against the radius (radioulnar convergence).
The combination tenodesis addresses this through a dual-vector stabilization approach:
1. Volar Stabilization (FCU): A distally based slip of the FCU is routed from palmar to dorsal through the interosseous space. This counteracts the dorsal subluxation forces acting on the ulnar stump.
2. Dorsal Stabilization (ECU): A slip of the ECU is routed through the medullary canal of the ulna. This provides a dorsal tether, preventing volar migration.
3. Dynamic Sling Effect: Because the tendon slips remain attached to their native insertions (the pisiform for the FCU and the base of the fifth metacarpal for the ECU), muscle contraction during wrist flexion and extension dynamically tightens the sling, actively holding the ulna away from the radius during grip.
Clinical Pearl: The success of this procedure relies heavily on maintaining the native distal attachments of the harvested tendon slips. If the insertions at the pisiform or the fifth metacarpal are compromised, the dynamic stabilizing effect of the tenodesis is lost, leading to recurrent impingement.
Indications and Patient Selection
Careful patient selection is the cornerstone of a successful combination tenodesis. This procedure is technically demanding and should be reserved for specific clinical scenarios.
Primary Indications
- Failed Darrach Procedure: Patients presenting with a painful, unstable ulnar stump and radioulnar convergence following a previous distal ulna resection.
- Severe DRUJ Arthritis: Cases of advanced osteoarthritis or rheumatoid arthritis where joint-preserving procedures (e.g., Suave-Kapandji) are contraindicated, and a primary Darrach procedure is planned but carries a high risk of stump instability.
- Post-Traumatic Reconstruction: Massive bone loss or irreparable comminution of the distal ulna requiring resection and immediate stabilization.
Contraindications
- Active Infection: Any local or systemic infection must be eradicated prior to surgery.
- Inadequate Tendon Integrity: Patients with severe rheumatoid disease who have spontaneous ruptures or severe attenuation of the FCU or ECU tendons are not candidates.
- Proximal Radioulnar Joint (PRUJ) Instability: If the radial head is excised or the PRUJ is unstable, tethering the distal ulna will not restore overall forearm stability.
Preoperative Preparation and Positioning
Meticulous preoperative planning and optimal patient positioning are essential for the seamless execution of the dual-incision approach required for this procedure.
- Anesthesia: General anesthesia or a high-quality regional brachial plexus block is recommended to ensure complete muscle relaxation, which is vital for tensioning the tenodesis.
- Positioning: Place the patient in the supine position. The affected upper extremity is extended onto a radiolucent hand table.
- Tourniquet Application: Apply a well-padded pneumatic tourniquet to the proximal arm.
- Preparation and Draping: Prepare the skin with a standard chlorhexidine or iodine-based solution. Arrange sterile drapes to allow full exposure of the limb from the fingertips to the tourniquet, ensuring unrestricted pronation, supination, and elbow flexion during the procedure.
- Exsanguination: Exsanguinate the limb using an Esmarch bandage and inflate the tourniquet to the appropriate pressure (typically 250 mm Hg or 100 mm Hg above systolic blood pressure).
Surgical Technique: Step-by-Step
The modified Jupiter and Breen technique requires two distinct surgical approaches (dorsal and volar) to harvest the tendons and prepare the ulnar stump.
1. Dorsal Approach and Ulnar Preparation
- Incision: Make a 10-cm, dorsal, S-shaped incision. Begin over the carpus, just distal to the wrist extension crease, and extend it proximally over the distal shaft of the ulna.
- Nerve Protection: Carefully dissect through the subcutaneous tissues. It is imperative to identify and protect the dorsal sensory branches of the ulnar nerve (DSUN), which typically cross the operative field from volar to dorsal in this region.
- Retinacular Exposure: Expose the extensor retinaculum. Make a Z-shaped incision in the retinaculum over the sixth dorsal compartment.
- Surgical Tip: Preserve a robust retinacular flap. This will be used later during closure to create a stabilizing sling over the ECU tendon, preventing bowstringing.
- Ulnar Exposure: If the ulnar head is still present (i.e., this is a primary resection rather than a revision of a Darrach), expose the distal ulna using a subperiosteal or extraperiosteal dissection technique. Protect the FCU and ECU muscle bellies with blunt retractors.
- Ulnar Osteotomy: Perform a transverse osteotomy of the ulna at the level of the ulnar neck, or just proximal to the sigmoid notch.
- Depending on the patient's size and anatomy, the length of the distal ulna to be excised is typically 1.5 to 2.0 cm.
- Technique Options: Mark the planned osteotomy site with an osteotome. You may use an oscillating saw with a small blade for a clean cut, or drill a transverse line of holes through the ulnar neck and complete the osteotomy with bone-cutting forceps to minimize thermal necrosis.
2. Extensor Carpi Ulnaris (ECU) Preparation
Once the ulna is prepared, attention is turned to the ECU tendon.
- Tendon Dissection: Dissect the ECU tendon from its musculotendinous junction distally down to, but not into, the sixth dorsal compartment.
- Longitudinal Split: Carefully split the ECU tendon longitudinally. Detach one half from the proximal muscle belly, creating a slip that is 9 to 10 cm long.
- Distal Attachment: It is critical to leave the distal attachment of this slip at the base of the fifth metacarpal completely intact. The sixth dorsal compartment should also remain undisturbed to maintain the tendon's native line of pull.
Surgical Warning: Do not inadvertently detach the ECU from the fifth metacarpal. The entire biomechanical foundation of the dynamic dorsal sling relies on this distal anchor point.
3. Volar Approach and Flexor Carpi Ulnaris (FCU) Preparation
- Positioning Change: Supinate the hand fully to expose the volar-ulnar aspect of the forearm.
- Incision: Beginning at the pisiform, make a 10-cm curved incision extending proximally along the palmar and ulnar side of the forearm.
- Neurovascular Protection: Deepen the incision carefully. Identify and meticulously protect the ulnar neurovascular bundle (ulnar artery and ulnar nerve), which lies immediately radial and deep to the FCU tendon.
- Tendon Harvest: Expose the FCU tendon. Similar to the ECU, create a tendon slip 8 to 10 cm long. Leave this slip distally based and firmly attached to the pisiform.

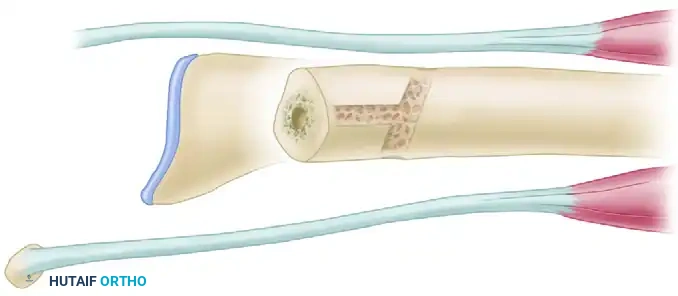
4. Preparation of Ulnar Bone Tunnels
The creation of precise bone tunnels in the distal ulnar stump is required to route the tendon slips and create the tenodesis weave.
- Transverse Tunnel: Starting 1.5 to 2.0 cm proximal to the newly cut end of the ulna, use a 1/4-inch (6 to 7 mm) drill bit to create a transverse tunnel. Drill from the dorsal cortex of the ulna, passing directly through the medullary canal, and exiting out the volar cortex.
- Trajectory: The drill should slant slightly from proximal-dorsal to distal-palmar to facilitate a smooth tendon glide.
- Medullary Tunnel: Next, use a side-cutting power burr or drill to ream the ulnar medullary canal starting directly at the distal cut end of the ulna. Drill proximally up the medullary canal.
- Exit Hole: Create a cortical exit hole for this medullary tunnel approximately 1.5 cm proximal to the end of the ulna, connecting with the medullary reaming.
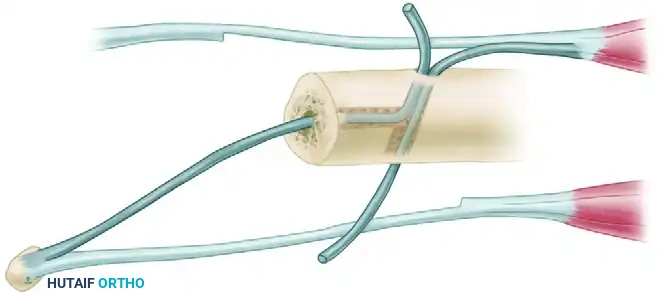
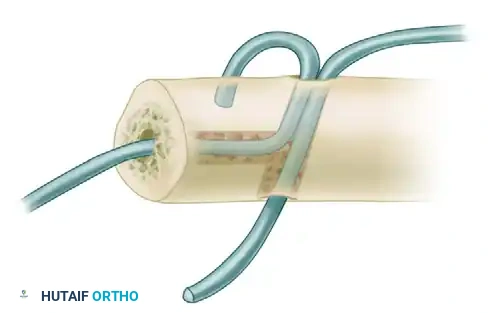
5. Tendon Routing and Tenodesis Weave
This is the most critical phase of the procedure, where the dynamic sling is constructed.
- FCU Routing: Take the distally based FCU slip. Pass it from the palmar compartment, directing it dorsally through the interosseous space, bringing it to the dorsomedial aspect of the ulna.
- ECU Routing: Take the distally based half of the ECU tendon. Pass it directly into the cortical exit hole, routing it distally through the intramedullary canal of the ulna, and out the distal cut end.
- The Weave: Thread the tendons through the prepared transverse and medullary tunnels to initiate the tenodesis weave. The exact routing creates a figure-of-eight or interlocking sling that captures the ulnar stump.
6. Radioulnar Stabilization and Pronator Quadratus Transfer
Before final tensioning of the tendons, the radioulnar relationship must be rigidly stabilized in the correct anatomical position.
- Interosseous Spacing: Insert a lamina spreader between the radius and the ulna. Gently open the spreader to restore and maintain the native interosseous space, ensuring the ulnar stump is not converging on the radius.
- Positioning for Pinning: Flex the patient's elbow to exactly 90 degrees. Position the forearm in neutral rotation, with the fingers pointing directly toward the ceiling.
- Kirschner Wire Fixation: Pass two divergent 0.062-inch Kirschner wires (K-wires) percutaneously through the medial border of the ulna, across the interosseous space, and into the radius.
- Divergence: Placing the wires in divergent directions is crucial to maximize rotational stability and prevent postoperative migration of the radius and ulna.
- Placement: Ensure the K-wires are placed proximal to the proximal margin of the pronator quadratus. This leaves the muscle free for transfer.
- Pronator Quadratus Interposition: Elevate the pronator quadratus. Pass the muscle belly dorsally between the forearm bones (radius and ulna) and anchor it securely to the medial periosteum of the ulna. This soft-tissue interposition acts as a biological buffer, further preventing bony impingement.
7. Final Tensioning and Closure
- Tensioning the Sling: With the K-wires holding the bones in neutral rotation, position the hand and wrist in 10 degrees of ulnar deviation. Pull the routed ECU and FCU tendon slips taut.
- Suturing: While maintaining strict tension to support the radioulnar interosseous space, suture the tendons to themselves, to each other, and to the adjacent periosteum using heavy, non-absorbable braided sutures (e.g., #2-0 or #0 Ethibond).
- Hemostasis and Closure: Deflate the pneumatic tourniquet. Obtain meticulous hemostasis using bipolar electrocautery to prevent postoperative hematoma.
- Retinacular Repair: Repair the Z-lengthened extensor retinaculum, utilizing the preserved flap to create a stabilizing sling over the intact portion of the ECU tendon.
- Skin Closure: Close the subcutaneous tissues and skin of both the dorsal and volar incisions in a standard layered fashion.
- Dressing: Apply a sterile, non-adherent dressing, followed by a bulky soft dressing. Immobilize the extremity immediately in a rigid, well-molded long-arm splint with the forearm in neutral rotation and the elbow at 90 degrees of flexion.
Postoperative Rehabilitation Protocol
The success of the combination tenodesis is highly dependent on strict adherence to a phased postoperative rehabilitation protocol. Premature mobilization can lead to stretching of the tenodesis and recurrent instability, while prolonged immobilization can result in severe joint stiffness.
Phase I: Maximum Protection (Weeks 0 to 2)
- The patient remains in the initial bulky dressing and long-arm splint.
- Strict elevation of the limb is enforced to minimize edema.
- Active range of motion (ROM) of the fingers and thumb is encouraged immediately to prevent tendon adhesions and reduce swelling.
- At 2 weeks postoperative, the patient returns to the clinic. The splint and bulky dressing are removed. Skin sutures are removed.
- A custom-molded fiberglass long-arm cast is applied, maintaining the elbow at 90 degrees of flexion and the forearm in neutral rotation.
Phase II: Continued Immobilization (Weeks 2 to 6)
- The patient wears the long-arm cast continuously for an additional 4 weeks (total of 6 weeks of rigid immobilization).
- Finger and shoulder ROM exercises are continued daily.
- Weight-bearing and lifting with the operative extremity are strictly prohibited.
Phase III: Pin Removal and Early Motion (Week 6 to 8)
- At 6 weeks postoperative, the long-arm cast is removed.
- Radiographs are obtained to confirm maintenance of the radioulnar space.
- The percutaneous 0.062-inch K-wires are removed in the clinic.
- Rehabilitation Initiation: The patient is transitioned to a removable long-arm splint or a Munster-style splint, worn at all times except during therapy.
- Begin active and active-assisted range of motion exercises for the wrist and elbow. Forearm pronation and supination are initiated gently, avoiding forceful terminal rotation.
Phase IV: Strengthening and Weaning (Weeks 8 to 12+)
- Passive range of motion is gradually introduced to address any residual stiffness.
- Splinting is progressively weaned, utilized only as needed for comfort or during high-risk activities.
- Progressive strengthening exercises for grip, wrist, and forearm musculature are initiated.
- Full return to heavy manual labor or high-impact activities may take 4 to 6 months and is dependent on the recovery of satisfactory motion, strength, and the absence of DRUJ pain.
Complications and Pitfalls
While highly effective, the combination tenodesis carries specific risks that the orthopedic surgeon must anticipate and mitigate.
- Nerve Injury: The dorsal sensory branch of the ulnar nerve (DSUN) is at high risk during the dorsal approach. Neuroma formation here is notoriously painful and difficult to treat. The ulnar nerve proper must be protected during the volar FCU harvest.
- Recurrent Instability: Failure to adequately tension the tendon weave, or failure of the patient to comply with the 6-week immobilization protocol, can lead to stretching of the tenodesis and recurrent radioulnar convergence.
- Pin Tract Infection: The percutaneous K-wires are left in place for 6 weeks. Local pin care is essential to prevent superficial infections from tracking into the medullary canal or the interosseous space.
- Loss of Forearm Rotation: Over-tensioning the tenodesis or excessive scarring can lead to a permanent loss of terminal pronation or supination. The use of the lamina spreader and pinning the forearm in strict neutral rotation during surgery is critical to balancing stability with postoperative mobility.
-
Fracture of the Ulnar Stump: Drilling multiple tunnels (transverse and medullary) in a small or osteopenic ulnar stump can create a stress riser. Use appropriately sized drill bits (no larger than 1/4 inch) and ensure adequate bone bridges remain between the tunnels and the cut end of the ulna.
You Might Also Like
