Carpal Ligament Injuries and Instability Patterns: A Comprehensive Surgical Guide
Key Takeaway
Carpal instability represents a complex spectrum of wrist pathology resulting from ligamentous disruption. This comprehensive guide details the biomechanical foundations, advanced radiographic evaluation, and evidence-based surgical management of carpal ligament injuries. From scapholunate dissociation to progressive perilunar instability, mastering these concepts is essential for orthopedic surgeons to restore wrist kinematics, prevent degenerative collapse, and optimize patient outcomes through precise operative intervention and structured postoperative rehabilitation.
CARPAL LIGAMENT INJURIES AND INSTABILITY PATTERNS
The human carpus is a highly complex, intercalated biomechanical linkage system. Posttraumatic loss of alignment of the carpal bones leads to profound kinematic derangements, progressive articular wear, and debilitating functional loss. Describing the posttraumatic loss of alignment of the carpal bones, Linscheid et al. established the foundational framework for understanding these pathologies, grouping carpal instabilities into four primary types:
1. Dorsiflexion instability
2. Palmar-flexion instability
3. Ulnar translocation
4. Dorsal subluxation
Instability in the carpus is further categorized temporally and kinematically. It is considered static if the radiographic intercarpal relationships are persistently abnormal and do not change with motion. Conversely, it is considered dynamic if the resting intercarpal relationships appear normal on standard radiographs but become abnormal under physiologic loads, manipulation, or active motion.
Clinical Pearl: Dynamic instability represents an earlier stage of ligamentous failure. Provocative maneuvers and stress radiography (e.g., clenched-fist views) are mandatory when a patient presents with mechanical wrist pain but normal static radiographs.
Radiographic Evaluation and Wrist Collapse Patterns
Linscheid et al. stressed the critical importance of evaluating the proximal carpal row in the true lateral radiographic projection. In a normal, neutrally positioned wrist, the longitudinal axes of the radius, lunate, capitate, and third metacarpal should be collinear within an approximately 15-degree tolerance.
When the ligamentous constraints fail, the proximal carpal row—acting as an intercalated segment with no direct tendon insertions—collapses into predictable patterns based on the remaining intact ligaments:
* Dorsal Intercalated Segment Instability (DISI): The distal articular surface of the lunate is tilted to face dorsally. This is most commonly associated with scapholunate ligament disruption.
* Volar Intercalated Segment Instability (VISI): The distal articular surface of the lunate faces toward the palm. This is typically associated with lunotriquetral ligament disruption.
INSTABILITY CLASSIFICATION SYSTEMS
Dissociative vs. Nondissociative Instability
Linscheid et al. advocated the vital concept of dissociative and nondissociative instabilities, which dictates the surgical approach:
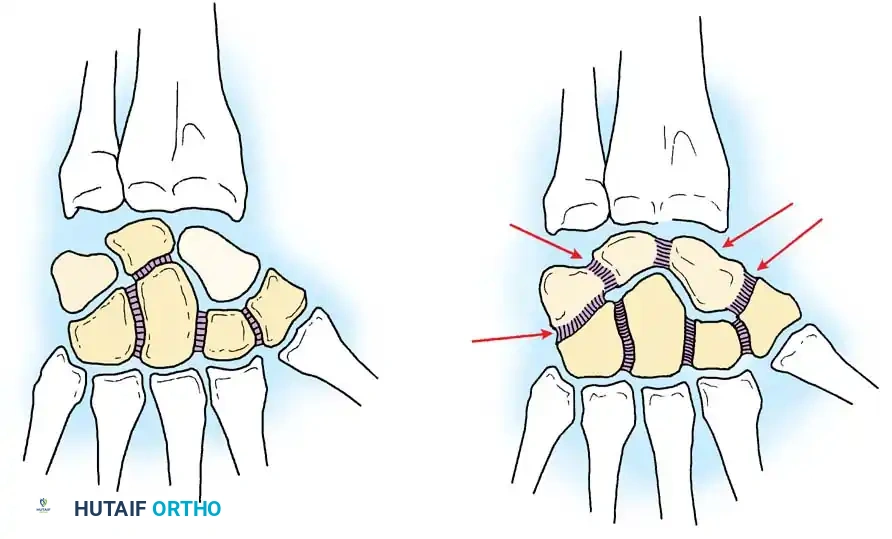
* Dissociative Carpal Instability (CID): Characterized by the disruption of the intrinsic interosseous ligaments between the bones of the proximal carpal row (e.g., scapholunate or lunotriquetral ligaments). The proximal row is "dissociated" from itself.
* Nondissociative Carpal Instability (CIND): Characterized by the disruption of the extrinsic radiocarpal or midcarpal ligaments, while the intrinsic ligaments between the carpal bones remain intact. The entire proximal row moves as a coupled unit but is unstable relative to the radius or the distal carpal row.
The Dobyns and Cooney Classification
Building upon anatomical, mechanical, and kinematic aspects, Dobyns and Cooney developed a comprehensive classification system that remains the gold standard for academic and clinical communication.
I. CID (Carpal Instability Dissociative)
* Proximal Carpal Row CID: Includes unstable scaphoid fractures (DISI pattern), scapholunate dissociation (DISI pattern), and lunotriquetral dissociation (VISI pattern).
* Distal Carpal Row CID: Axial radial disruption, axial ulnar disruption, or combined patterns.
II. CIND (Carpal Instability Nondissociative)
* Radiocarpal CIND: Palmar ligament rupture (DISI, ulnar translocation), dorsal ligament rupture (VISI, dorsal translation), or adaptive changes following radial/scaphoid malunion.
* Midcarpal CIND: Ulnar or radial midcarpal instability from palmar ligament damage (VISI), or midcarpal instability from dorsal ligament damage (DISI).
* Combined Radiocarpal-Midcarpal CIND: Capitolunate instability patterns.
III. CIC (Carpal Instability Combined or Complex)
* Involves both dissociative and nondissociative elements, such as perilunate dislocations with radiocarpal instability (DISI and ulnar translocation) or scapholunate dissociation combined with ulnar translation.
IV. Adaptive Carpus
* Malposition of the carpus secondary to extrinsic skeletal deformity, such as distal radial malunion (DISI or dorsal translation), scaphoid nonunion (DISI), or Madelung deformity.
PROGRESSIVE PERILUNAR INSTABILITY
Mayfield, Johnson, and Kilcoyne described the pathomechanics of carpal failure through four sequential stages of progressive disruption of ligament attachments and anatomical relationships to the lunate. This cascade results from forced wrist hyperextension, ulnar deviation, and intercarpal supination.
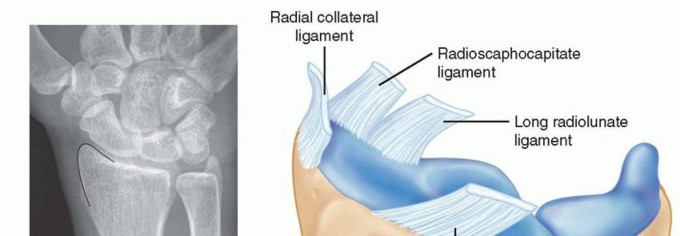
- Stage I (Scapholunate Failure): Disruption of the scapholunate interosseous ligament and volar radioscaphocapitate ligament. This manifests as scapholunate dissociation.
- Stage II (Capitolunate Failure): The force propagates ulnarly through the space of Poirier, disrupting the capitolunate articulation.
- Stage III (Triquetrolunate Failure): Disruption of the lunotriquetral interosseous ligament. The entire carpus separates from the lunate, resulting in a perilunate dislocation.
- Stage IV (Lunate Dislocation): Failure of the dorsal radiocarpal ligament. The capitate is forced proximally, extruding the lunate volarly into the carpal tunnel.
Surgical Warning: A Stage IV lunate dislocation is an orthopedic emergency. The volarly extruded lunate frequently causes acute, severe compression of the median nerve. Delayed reduction can result in permanent median nerve palsy and irreversible ischemic necrosis of the lunate.
SCAPHOLUNATE DISSOCIATION (ROTARY SUBLUXATION OF THE SCAPHOID)
Scapholunate dissociation is the most common and clinically significant form of carpal instability. When the scapholunate interosseous ligament (specifically its robust dorsal subregion) and secondary extrinsic stabilizers fail, the scaphoid flexes volarly and pronates, while the lunate extends dorsally (DISI).
Over time, the capitate migrates proximally into the gap created by the separation of the scaphoid and lunate. This proximal migration is exacerbated when an axial force is exerted on the capitate, such as when making a fist. If left untreated, this altered kinematics inevitably leads to Scapholunate Advanced Collapse (SLAC), characterized by progressive degenerative arthritic changes beginning at the radioscaphoid styloid and progressing to the entire radioscaphoid and capitolunate joints.
Surgical Management of Acute Scapholunate Dissociation
Closed Reduction and Percutaneous Pinning:
In strictly acute settings without gross displacement, closed treatment may be attempted.
1. Attempt reduction by placing the wrist in neutral flexion and a few degrees of ulnar deviation to extend the scaphoid.
2. Under fluoroscopic guidance, percutaneous pinning is performed using 0.045-inch (1.16-mm) Kirschner wires.
3. Place the first K-wire through the scaphoid into the capitate to stabilize the scaphoid's flexion.
4. Place a second K-wire through the scaphoid into the lunate to close the scapholunate interval.
Arthroscopic and Open Reduction:
If closed reduction is unsuccessful or the gap remains >3mm, arthroscopic reduction and percutaneous pin fixation can be attempted. However, open reduction and primary ligament repair remain the gold standard for acute, repairable injuries.
- Approach: A dorsal longitudinal incision is made over the third dorsal compartment. The extensor pollicis longus (EPL) is transposed radially.
- Capsulotomy: A ligament-sparing dorsal capsulotomy (e.g., Berger's dorsal capsular flap) is elevated to expose the proximal carpal row.
- Reduction: The scapholunate gap is debrided of hematoma and interposed tissue. Joysticks (0.045-inch K-wires) are placed into the scaphoid and lunate. The scaphoid is extended and supinated, while the lunate is flexed, anatomically reducing the joint.
- Fixation: The reduction is held with multiple 0.045-inch K-wires driven from the scaphoid into the lunate and capitate.
- Repair: The dorsal scapholunate ligament is repaired directly using suture anchors placed into the scaphoid or lunate footprint. The dorsal capsule is meticulously repaired to augment stability.
Management of Chronic Scapholunate Dissociation
Management of an old rotary subluxation of the scaphoid (where the primary ligament is irreparable but cartilage is preserved) requires reconstruction of the scapholunate interosseous ligament.
The most widely accepted technique utilizes a segment of the extensor carpi radialis brevis (ECRB) tendon (Modified Brunelli Tenodesis).
1. A strip of the ECRB is harvested, leaving its distal insertion on the base of the third metacarpal intact.
2. The tendon graft is passed volarly to dorsally through a bone tunnel created in the distal pole of the scaphoid.
3. The graft is tensioned to correct scaphoid flexion, passed across the scapholunate interval, and secured to the dorsum of the lunate with a suture anchor.
4. The graft is then looped back and sutured to the dorsal radiotriquetral ligament.
5. The construct is protected with K-wire fixation.
Surgical Pitfall: Insufficient experience with complex ligamentous reconstructions can lead to over-tensioning, resulting in severe wrist stiffness, or under-tensioning, leading to recurrent instability. Meticulous attention to isometric graft placement is paramount.
LUNATE AND PERILUNATE DISLOCATIONS
Perilunate (Stage III) and lunate (Stage IV) dislocations represent high-energy trauma. On the lateral radiographic view, the normal rectangular profile of the lunate becomes triangular (the "spilled teacup" sign) because of its severe volar tilt. On the AP view, the lunate overlaps the capitate, creating the "piece of pie" sign.
Acute Management and Surgical Approach
An anteriorly dislocated lunate can cause acute compression of the median nerve. If the patient’s condition permits, and if swelling is not excessive, the lunate bone should be reduced promptly in the emergency department via longitudinal traction and volar pressure over the lunate.
Because an open release of the transverse carpal ligament may be required to decompress the median nerve, every effort should be made to reduce and control the swelling to permit subsequent wound closure.
Operative Intervention:
When the injury is treated early (within days), manipulative reduction is usually possible, followed by operative stabilization. When treated after 3 weeks, the injury is notoriously difficult to reduce by manipulation due to soft tissue contracture, and open reduction is mandatory.
- Combined Dorsal and Volar Approach: A dual approach is frequently recommended.
- Volar Phase: An extended carpal tunnel incision is made. The transverse carpal ligament is released to decompress the median nerve. The rent in the volar capsule (Space of Poirier) is identified. The lunate is gently manipulated back into the lunate fossa.
- Dorsal Phase: A dorsal approach is utilized to anatomically reduce the carpus around the lunate. The scapholunate and lunotriquetral intervals are reduced using K-wire joysticks and pinned with 0.045-inch K-wires.
- Ligament Repair: The dorsal scapholunate and lunotriquetral ligaments are repaired with suture anchors. The volar capsular rent is repaired if accessible, though dorsal repair is the biomechanical priority.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOLS
The success of carpal ligament surgery relies as much on rigid adherence to postoperative rehabilitation as it does on surgical execution.
Phase I: Immediate Postoperative Period (0-2 Weeks)
* The wrist is immobilized in a bulky, well-padded volar and dorsal splint.
* With the hand strictly elevated to minimize edema, active motion of the fingers, elbow, and shoulder is begun immediately.
* Goal: Prevent complex regional pain syndrome (CRPS) and tendon adhesions.
Phase II: Intermediate Immobilization (2-6 Weeks)
* The initial splint and skin sutures are removed at 2 weeks.
* A custom-molded thermoplastic splint is applied. This must be worn at all times except during supervised bathing and specific, isolated digit exercising.
* Alternative: In a noncompliant patient, a short-arm cast is a more reliable form of immobilization for another month.
* Formal hand therapy is initiated at 2 weeks, focusing on edema control, scar management, and differential tendon gliding.
Phase III: Pin Removal and Mobilization (6-8+ Weeks)
* Protective immobilization and percutaneous K-wires are discontinued when bone union or adequate ligamentous healing is shown radiographically, usually at 6 to 8 weeks.
* Active and active-assisted range of motion (ROM) of the wrist is initiated.
* Passive stretching and aggressive strengthening are strictly avoided until 10 to 12 weeks postoperatively to prevent stretching out the delicate ligamentous repair.
* Patients must be counseled that maximal medical improvement may take up to 12 months, and a mild permanent loss of terminal flexion/extension is an expected outcome of a successful stabilization procedure.
You Might Also Like