Basic Surgical Techniques and Operating Room Ergonomics in Hand Surgery
Key Takeaway
Mastering basic surgical techniques in hand and upper extremity surgery requires meticulous preoperative planning, optimized operating room ergonomics, and precise tissue handling. This comprehensive guide details essential protocols, from advanced imaging and pharmacologic management to intraoperative positioning and the critical role of the surgical assistant. Adhering to these standardized, evidence-based routines minimizes complications, reduces operative time, and significantly improves functional outcomes for orthopedic patients.
Introduction to Basic Surgical Principles in Hand Surgery
The mastery of hand and upper extremity surgery is predicated upon a profound understanding of intricate anatomy, meticulous preoperative planning, and the disciplined execution of standardized operating room routines. Because surgical outcomes in this highly specialized field depend considerably on the skill, judgment, and precise tissue handling of the surgeon, foundational techniques cannot be overlooked. Disorganization, surgeon fatigue, and uncertainty inevitably diminish the efficiency of the operating team and compromise patient outcomes. This comprehensive guide delineates the critical pathways of preoperative preparation, operating room ergonomics, surgical positioning, and fundamental aftercare required for postgraduate orthopedic practice.
Preoperative Planning and Preparation
It is essential for the orthopedic surgeon to exhaust all necessary diagnostic avenues to formulate an accurate diagnosis and execute the most appropriate surgical intervention. A meticulously obtained clinical history and a detailed, systematic physical examination of the involved extremity are frequently sufficient to determine the primary pathology. However, modern surgical practice demands rigorous preoperative optimization and advanced diagnostic corroboration.
Clinical Evaluation and Advanced Imaging
Routine radiographic evaluation remains the cornerstone of orthopedic diagnostics. Standard anteroposterior (AP), lateral, and oblique radiographic views of the hand and wrist are mandatory. Depending on the suspected pathoanatomy, these must frequently be supplemented with specialized projections:
* Scaphoid Series: Includes ulnar deviation and semi-pronated views to elongate the scaphoid profile and assess for occult fractures.
* Robert’s View (True AP of the Thumb): Essential for evaluating the basilar joint (first carpometacarpal joint) for osteoarthritis or Bennett/Rolando fractures.
* Carpal Tunnel View: Utilized to assess the hook of the hamate and the pisiform.
When plain radiography is insufficient, advanced cross-sectional and functional imaging modalities are employed:
* Magnetic Resonance Imaging (MRI): Provides unparalleled resolution of soft-tissue structures. It is the gold standard for evaluating the triangular fibrocartilage complex (TFCC), intrinsic intercarpal ligaments (e.g., scapholunate, lunotriquetral), flexor/extensor tendon integrity, and early avascular necrosis (e.g., Kienböck disease, Preiser disease).
* Computed Tomography (CT): Essential for defining complex osseous architecture, particularly in intra-articular distal radius fractures, carpal coalition, or non-union evaluation. 3D reconstructions are invaluable for preoperative templating.
* Radionuclide Bone Scanning: Technetium-99m scans may highlight areas of increased osteoblastic activity or altered vascularity before structural changes are visible on plain radiographs, aiding in the diagnosis of occult fractures, osteomyelitis, or Complex Regional Pain Syndrome (CRPS).
Electrodiagnostic Studies
Electrodiagnostic studies, comprising electromyography (EMG) and nerve conduction velocities (NCV), are critical adjuncts in the evaluation of peripheral nerve pathology. They are utilized to:
* Localize precise anatomical zones of nerve compression (e.g., distinguishing cubital tunnel syndrome from Guyon's canal stenosis).
* Quantify the severity of axonal loss or demyelination.
* Differentiate focal entrapment neuropathies from systemic peripheral neuropathies (e.g., diabetic neuropathy) or cervical radiculopathies (double-crush syndrome).
Medical Optimization and Pharmacologic Management
In patients with suspected but undiagnosed systemic illnesses, such as inflammatory arthritides (e.g., Rheumatoid Arthritis, Psoriatic Arthritis), preoperative assessment by a rheumatologist or appropriate medical specialist is mandatory to determine the optimal balance of operative and nonoperative management.
Perioperative medication management requires strict, evidence-based protocols:
* Anticoagulants (Warfarin, DOACs): Must be managed in conjunction with the patient's cardiologist or primary care physician. Bridging therapy with low-molecular-weight heparin (LMWH) may be required depending on the patient's thromboembolic risk profile.
* Immunosuppressive and Biologic Agents: Disease-modifying antirheumatic drugs (DMARDs) and biologic therapies (e.g., TNF-alpha inhibitors) alter wound healing and infection risk. Current American College of Rheumatology (ACR) and American Association of Hip and Knee Surgeons (AAHKS) guidelines should be consulted regarding the timing of withholding and restarting these medications.
* Corticosteroids: Patients on chronic systemic corticosteroids may require perioperative stress-dose steroids to prevent acute adrenal insufficiency.
* Diabetic Medications: Glycemic control is a primary determinant of postoperative infection and wound healing. Hemoglobin A1c should ideally be optimized to < 7.0% prior to elective procedures.
Surgical Warning: Herbal supplements (e.g., Ginkgo biloba, Garlic, Ginseng, St. John’s Wort) can significantly impact hemostasis and anesthetic metabolism. Patients must be explicitly instructed to discontinue these preparations at least two weeks prior to surgery.
Informed Consent and Expectation Management
Before finalizing any operative plan, the surgeon and patient must establish realistic expectations. The informed consent process must be exhaustive and documented meticulously. The patient must fully comprehend:
1. The natural history of the condition with and without surgical intervention.
2. All viable nonoperative alternatives.
3. The potential risks, hazards, and specific complications (e.g., infection, neurovascular injury, stiffness, CRPS).
4. The precise nature of the incisions, including the potential need for secondary incisions for bone, tendon, or nerve graft harvesting.
5. The potential utilization of internal fixation devices (plates, screws, K-wires), surgical drains, or implants (e.g., silicone arthroplasty implants).
6. The rigorous nature of postoperative immobilization (splints, casts) and the understanding that rehabilitation may be prolonged, demanding strict adherence to hand therapy protocols.
Preoperative Skin Preparation and Infection Prophylaxis
Patients are instructed to maintain strict hand hygiene for several days preceding surgery and to avoid any activities that could result in skin abrasions or lacerations.
Clinical Pearl: There are currently limited prospective, randomized studies defining exact infection rates exclusively for elective hand surgery; however, extrapolated data suggests an expected surgical site infection (SSI) rate of slightly more than 1%. If a patient presents on the day of surgery with active cutaneous infections, paronychia, or significant abrasions in the operative field, elective surgery must be delayed.
In the preoperative holding area and operating room, the limb is subjected to rigorous antisepsis. The skin should be scrubbed with an FDA-approved antiseptic solution (chlorhexidine gluconate derivatives or iodophors are highly effective).
* Nail Care: Long or visibly soiled fingernails must be trimmed and meticulously cleaned to eradicate subungual bacterial reservoirs.
* Hair Removal: To avoid creating epidermal micro-lacerations that serve as bacterial niduses, razors must never be used. If excessive hair obscures the surgical field, it should be removed immediately prior to surgery using electric clippers.
Arrangement and Routine in the Operating Room
The operating room (OR) environment directly influences surgical performance. It is paramount for the surgeon to establish a standardized, unwavering routine. This consistency allows the surgical assistants, scrub nurses, and anesthesiologists to anticipate the surgeon's needs, eliminating hesitation, delay, and wasted motion.
Environmental Control and Ergonomics
The operating room must remain a quiet, highly focused, and professional environment. If regional or local anesthesia (e.g., Wide Awake Local Anesthesia No Tourniquet - WALANT) is utilized and the patient is conscious, loud noises, sudden alarms, or inappropriate bursts of conversation can cause severe patient anxiety and must be strictly prohibited.
Preoperative coordination with the OR charge nurse is essential. Arrangements for specialized instrumentation, microsurgical equipment (operating microscope, loupes), specific implants, and intraoperative C-arm fluoroscopy must be confirmed prior to the patient entering the room.
Surgeon Seating and Posture:
Ergonomics in hand surgery cannot be overstated. The surgeon must utilize a stool that is firm, comfortable, and absolutely stable.
* The surgeon should sit with the spine comfortably erect.
* Knees should be positioned almost level with the hips.
* Feet must rest flat and securely on the floor to prevent lower back strain.
* The working surface of the hand operating table must be adjusted precisely to the surgeon's elbow height, providing a stable, fatigue-reducing support for the forearms during microsurgical dissection.
Lighting:
Optimal illumination is critical. For a right-handed surgeon, the primary overhead operating light should be directed from above the surgeon’s left shoulder. This specific trajectory ensures the light shines directly into the operative field, effectively eliminating shadows cast by the surgeon's own hands or instruments.
The Role of the Surgical Assistant
While mechanical hand holders and lead hands are commercially available, none can replicate the dynamic responsiveness of a motivated, well-trained surgical assistant. The assistant's primary duty is to maintain the patient’s hand in a stable, secure, and motionless posture while providing optimal dynamic retraction of the digits to maximize the surgeon’s access to the operative field.

Assistant Positioning:
* The assistant should be seated directly opposite the surgeon.
* To ensure an unobstructed line of sight, the assistant’s stool should be elevated so their head is approximately 8 to 10 cm higher than the surgeon’s head. This prevents the assistant from instinctively leaning forward and obstructing the surgeon’s view or the overhead lighting.
Surgeon Positioning Relative to the Limb:
For the vast majority of procedures, the surgeon should sit on the axillary side of the involved extremity. This standardized positioning ensures that the complex anatomy of either the right or left hand is viewed from the same relative orientation, reinforcing anatomical familiarity.
* Exception: Certain procedures localized strictly to the dorsum of the hand or the dorsal wrist compartments may be executed more ergonomically from the cephalic side (head of the table). If the surgeon elects to change sides, they must consciously recalibrate their anatomical orientation to avoid catastrophic iatrogenic injury.
Instrument Management and the "Drop Technique"
Efficiency at the surgical field is maintained through strict instrument organization. The Mayo stand or basic instrument tray should be positioned on a shelf extending directly from the operating table, perfectly level with the working surface.
Instruments must always be arranged in the exact same order. This spatial consistency allows the experienced surgeon to develop muscle memory, reaching for basic instruments (e.g., Adson forceps, tenotomy scissors, scalpel) without diverting their eyes from the microscopic operative field.
The Drop Technique:
To maximize flow, the "drop technique" is highly recommended.
1. The surgeon utilizes an instrument and, upon completion of that specific task, simply drops or places it in a designated neutral zone on the sterile drape.
2. The scrub nurse immediately retrieves the instrument, cleans it if necessary, and returns it to its exact designated location on the basic tray.
3. Exception: Frequently utilized instruments, such as the primary scalpel, delicate tissue forceps, and dissecting scissors, are retained in the surgeon's hand or immediate vicinity and are not retrieved by the nurse unless explicitly requested.
Specialized instruments (e.g., bone reduction forceps, oscillating saws, micro-vascular clamps) should be organized on a secondary, larger back table. They must be readily available to be passed smoothly to the surgeon upon request. Additional scalpel blades, specialized sutures (e.g., 4-0 to 6-0 Prolene for vessels, 3-0 Supramid for skin), and needles must be immediately accessible to prevent delays during critical phases of the operation, such as vascular anastomosis or nerve coaptation.
Basic Surgical Approaches and Tissue Handling
While the specific approach dictates the success of the procedure, all hand surgery relies on fundamental biomechanical principles of tissue handling.
Incision Principles
Incisions in the hand and digits must be meticulously planned to avoid crossing flexion creases at a 90-degree angle, which inevitably leads to hypertrophic scarring and debilitating flexion contractures.
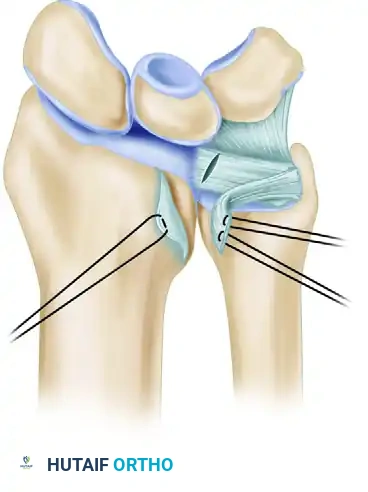
* Midlateral Digital Incisions: Placed along the neutral axis of the digit, connecting the apices of the flexion creases. This approach provides excellent exposure to the flexor tendon sheath and neurovascular bundles while minimizing volar scar contracture. The incision is typically placed dorsal to the neurovascular bundle, utilizing Cleland's ligaments as an anatomical landmark.
* Brunner (Zig-Zag) Incisions: Volar incisions utilizing V-shaped flaps. The apices of the flaps must extend to the midlateral line of the digit, and the angles should be approximately 60 degrees to prevent tip necrosis.
* Z-Plasty: A critical technique used to lengthen a contracted scar or redirect an incision line that inadvertently crosses a tension crease. The standard Z-plasty utilizes 60-degree angles, providing a theoretical 73% increase in length along the central limb.
Hemostasis and Tourniquet Use
A bloodless field is imperative for the identification of delicate neurovascular structures. Pneumatic tourniquets are standardly applied to the proximal arm or forearm.
* Pressure: Typically set at 70-100 mmHg above the patient's systolic blood pressure (usually 200-250 mmHg for the upper arm).
* Time: Ischemia time should generally not exceed 120 minutes. If prolonged surgery is anticipated, the tourniquet should be deflated for 15-20 minutes to allow for ischemic preconditioning and tissue reperfusion before re-inflation.
* Exsanguination is achieved using an Esmarch bandage or limb elevation prior to inflation. Note: Exsanguination is contraindicated in cases of severe infection or malignancy to prevent systemic dissemination.
Postoperative Protocols and Aftercare
The surgical procedure concludes only when the final dressing and splint are applied. Improper postoperative immobilization can ruin a perfectly executed operation.
Splinting and the "Safe Position"
Unless specifically contraindicated by the nature of the repair (e.g., flexor tendon repairs requiring specific dynamic protocols), the hand should be immobilized in the Intrinsic Plus (James) Position, also known as the "Safe Position":
* Wrist: 20 to 30 degrees of extension.
* Metacarpophalangeal (MCP) Joints: 70 to 90 degrees of flexion. This places the collateral ligaments of the MCP joints at maximal stretch, preventing shortening and subsequent extension contractures.
* Interphalangeal (PIP and DIP) Joints: Full extension (0 degrees). This prevents the volar plate from scarring in a shortened position, which would lead to a PIP joint flexion contracture.
* Thumb: Palmar abducted to maintain the first web space.
Elevation and Rehabilitation
Postoperative edema is the primary enemy of hand function. The patient must be instructed to keep the hand strictly elevated above the level of the heart for the first 48 to 72 hours. Active range of motion of all uninvolved joints (shoulder, elbow, and non-immobilized digits) should commence immediately in the recovery room to promote venous and lymphatic return.
Early referral to a certified hand therapist (CHT) is often the differentiating factor between a good and an excellent surgical outcome. Rehabilitation protocols must be tailored precisely to the biomechanical constraints of the surgical repair, balancing the need for early mobilization to prevent adhesions with the necessity of protecting healing tissues.
You Might Also Like