Masterclass in Wrist Arthroscopy: Indications, Techniques, and Outcomes

Key Takeaway
Wrist arthroscopy has evolved from a purely diagnostic modality into an indispensable therapeutic tool. It is currently the gold standard for evaluating intercarpal ligament injuries, triangular fibrocartilage complex tears, and unexplained wrist pain. This comprehensive guide details the precise indications, biomechanical considerations, step-by-step surgical approaches, and complication management strategies essential for orthopedic surgeons performing advanced arthroscopic interventions of the radiocarpal and midcarpal joints.
INTRODUCTION TO WRIST ARTHROSCOPY
Over the past three decades, wrist arthroscopy has undergone a paradigm shift. Originally conceived as a purely diagnostic modality for unexplained wrist pain, it has rapidly developed into a highly effective, minimally invasive therapeutic tool. Today, it is indispensable for the management of a vast array of radiocarpal and midcarpal disorders, ranging from degenerative arthritis to acute complex carpal fractures.
The advent of high-definition optics, specialized small-joint instrumentation, and refined portal placement techniques has allowed for the creation of new arthroscopic classifications for conditions such as Kienböck disease, triangular fibrocartilage complex (TFCC) injuries, and interosseous ligament tears. These classifications directly guide surgical decision-making and therapeutic intervention.
Currently, arthroscopic assessment of intercarpal ligament injuries and carpal instability is universally considered the "gold standard." It provides unparalleled visualization of articular surfaces and ligamentous integrity, far surpassing the diagnostic capabilities of advanced cross-sectional imaging or traditional open exploration.
PREOPERATIVE EVALUATION AND IMAGING
A meticulous clinical examination must always precede arthroscopic intervention. However, advanced imaging remains a critical component of preoperative planning. Standard posteroanterior (PA), lateral, and specialized radiographic views are mandatory to rule out gross instability, advanced degenerative changes, or occult fractures.
Specialized projections, such as the carpal tunnel view, are essential for identifying specific osseous pathologies, including avulsion fractures of the hamate hook or trapezium, which may present as vague volar wrist pain. Furthermore, occult fractures of the carpal bones require careful radiographic scrutiny.

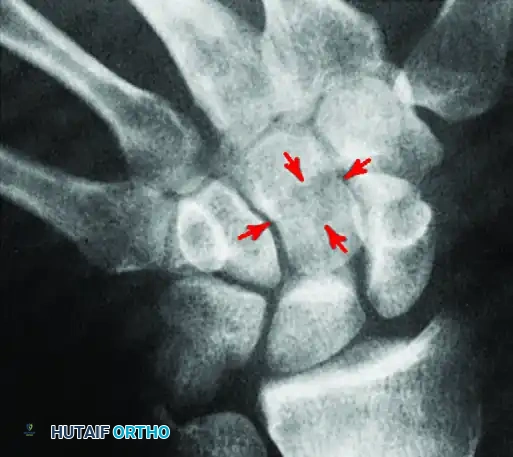
As demonstrated above, a standard PA view of the capitate may show no definite abnormality. However, an angled view can reveal a cystic defect with an associated fracture in the capitate waist. Recognizing these subtle osseous lesions preoperatively allows the surgeon to plan for concurrent arthroscopic debridement or percutaneous fixation.
The Role of Arthrography vs. Arthroscopy
Historically, triple-injection cinearthrography was the primary modality for diagnosing interosseous ligament tears. However, extensive clinical studies have proven that wrist arthroscopy is significantly more accurate than arthrography in identifying the exact location, morphology, and size of TFCC tears, as well as scapholunate (SL) and lunotriquetral (LT) ligament injuries.
Despite the superiority of arthroscopy, arthrography remains a useful adjunct in specific clinical scenarios. The dynamic flow of contrast can highlight abnormal communications between the radiocarpal and midcarpal joints.

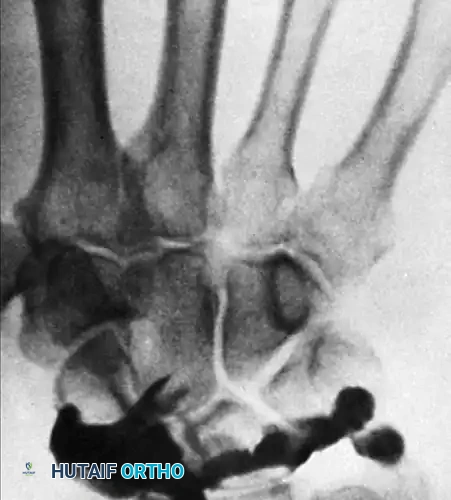
During a standard arthrogram, contrast is injected into the radiocarpal joint. In a normal wrist, the contrast material remains confined to this space.
However, with dynamic maneuvers such as ulnar deviation, abnormal contrast extravasation can be visualized. The passage of contrast into the midcarpal joint between the lunate and triquetrum is a definitive indicator of a lunotriquetral ligament tear.

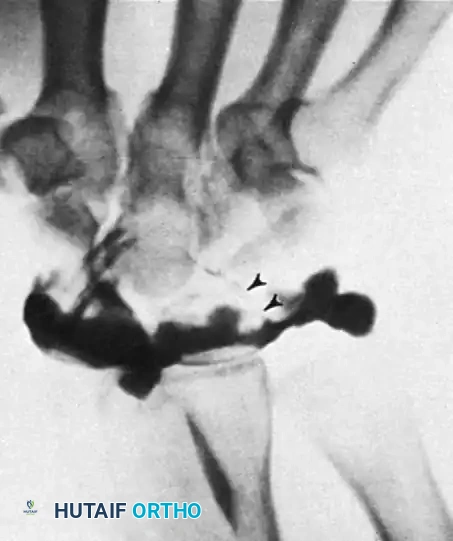
On follow-up overhead views, contrast material may fill the midcarpal joints, including the scapholunate joint from its distal aspect. Careful interpretation is required; a small defect between the contrast material in the scapholunate space and the radiocarpal space indicates an intact scapholunate ligament, despite the presence of contrast in the midcarpal row.
INDICATIONS FOR WRIST ARTHROSCOPY
The indications for wrist arthroscopy have expanded exponentially, encompassing both diagnostic and complex therapeutic procedures.
Diagnostic Indications
- Evaluation of Chronic Wrist Pain: For patients with persistent wrist pain of unknown origin despite exhaustive non-operative management and advanced imaging (MRI/CT).
- Ligamentous Assessment: The gold standard for evaluating the integrity, tension, and functional competence of the scapholunate interosseous ligament (SLIL) and lunotriquetral interosseous ligament (LTIL).
- Articular Surface Examination: Direct visualization of chondral wear patterns, crucial for staging Kienböck disease or SLAC/SNAC wrists.
- Confirmation of Arthrography/MRI: Supplementing equivocal imaging findings, particularly in partial-thickness TFCC tears.
Therapeutic Indications
- TFCC Management: Debridement of central (avascular) tears and arthroscopic-assisted repair of peripheral (vascular) tears.
- Fracture Management: Arthroscopically assisted reduction and internal fixation (ARIF) of intra-articular distal radius fractures, scaphoid fractures, and other carpal fractures. It ensures anatomic restoration of the articular step-off and allows for concurrent treatment of associated soft-tissue injuries.
- Perilunate Injuries: Assessment and assistance in the reduction of perilunate dislocations.
- Synovectomy and Biopsy: Targeted removal of hypertrophic synovium in rheumatoid arthritis or inflammatory arthropathies, and biopsy for diagnostic pathology.
- Loose Body Removal: Extraction of osteochondral fragments.
- Osteochondritis Dissecans (OCD): Debridement and microfracture of osteochondral lesions.
- Ganglion Excision: Resection of the stalk of dorsal wrist ganglions originating from the SL interval.
- Distal Ulnar Resection: Arthroscopic wafer procedure for ulnocarpal impaction syndrome.
Clinical Pearl: When treating intra-articular distal radius fractures, arthroscopy not only confirms articular reduction but also identifies concomitant TFCC tears (present in up to 40% of cases) and SL ligament tears (present in up to 30% of cases), which are frequently missed on standard radiographs.
SURGICAL ANATOMY AND PORTAL PLACEMENT
A profound understanding of dorsal wrist anatomy, specifically the extensor compartments, is non-negotiable for safe portal placement. Portals are named according to their relationship with the six dorsal extensor compartments.
Radiocarpal Portals
- 3-4 Portal: The primary viewing portal. Located between the 3rd compartment (Extensor Pollicis Longus - EPL) and the 4th compartment (Extensor Digitorum Communis - EDC), approximately 1 cm distal to Lister's tubercle. It provides an excellent panoramic view of the SL interval, TFCC, and radiocarpal articulation.
- 4-5 Portal: The primary working portal. Located between the 4th compartment (EDC) and the 5th compartment (Extensor Digiti Minimi - EDM).
- 6R Portal: Located immediately radial to the Extensor Carpi Ulnaris (ECU) tendon. Used for viewing the ulnar periphery of the TFCC and the LT interval.
- 6U Portal: Located immediately ulnar to the ECU tendon. Often used for outflow or for instrumentation during TFCC repairs.
- 1-2 Portal: Located between the 1st compartment (APL/EPB) and 2nd compartment (ECRL/ECRB). Useful for viewing the radial styloid and the volar radiocarpal ligaments.
Midcarpal Portals
- Midcarpal Radial (MCR) Portal: Located 1 cm distal to the 3-4 portal, in line with the radial border of the third metacarpal. It provides visualization of the scaphotrapezial-trapezoid (STT) joint and the distal aspect of the SL interval.
- Midcarpal Ulnar (MCU) Portal: Located 1 cm distal to the 4-5 portal, in line with the fourth metacarpal axis. It allows visualization of the capitohamate and triquetrohamate articulations.
Surgical Warning: The dorsal sensory branch of the ulnar nerve (DSBUN) is at high risk during the establishment of the 6U portal. Similarly, the superficial sensory branch of the radial nerve (SBRN) is at risk during 1-2 portal placement. Always use blunt dissection (a "nick and spread" technique) down to the capsule to protect these vital neural structures.
OPERATING ROOM SETUP AND PATIENT POSITIONING
Proper patient positioning is critical for joint distraction and instrument maneuverability.
1. Anesthesia: Regional block (axillary or supraclavicular) or general anesthesia is utilized. A well-padded proximal arm tourniquet is applied.
2. Traction: The arm is placed in a wrist arthroscopy tower. Finger traps are applied to the index and long fingers (and occasionally the ring finger for ulnar-sided pathology).
3. Distraction Force: Approximately 10 to 15 pounds of longitudinal traction is applied to distract the radiocarpal and midcarpal joints. Excessive traction must be avoided to prevent neurapraxia.
4. Equipment: A 2.7-mm or 1.9-mm arthroscope with a 30-degree angle is standard. Small joint shavers, biters, and radiofrequency probes should be readily available.
STEP-BY-STEP SURGICAL TECHNIQUE: THE DIAGNOSTIC SWEEP
A systematic approach ensures no pathology is missed. The standard diagnostic sweep begins in the radiocarpal joint.
- Establish the 3-4 Portal: After identifying Lister's tubercle, a 15-blade scalpel is used to incise only the skin. A mosquito hemostat bluntly dissects the subcutaneous tissue. The trocar is introduced with a volar and slightly proximal trajectory (matching the 11-degree volar tilt of the distal radius).
- Establish the 4-5 Portal: Under direct intra-articular visualization from the 3-4 portal, a spinal needle is inserted at the 4-5 interval to confirm the optimal trajectory for the working portal.
- Volar Ligament Assessment: The arthroscope is directed volarly to inspect the robust volar radiocarpal ligaments (Radioscaphocapitate, Long Radiolunate, Short Radiolunate).
- Scapholunate Interval: The scope is swept radially to evaluate the SLIL. A probe from the 4-5 portal is used to test the tension and integrity of the ligament (Geissler classification).
- Chondral Surfaces: The articular surfaces of the scaphoid, lunate, and radius are inspected for eburnation, chondromalacia, or step-offs.
- Ulnar Periphery and TFCC: The scope is directed ulnarly. The TFCC is probed for central perforations, peripheral detachments (trampoline test), and degenerative tearing.
- Lunotriquetral Interval: The LTIL is probed for step-offs or instability.
- Midcarpal Examination: The scope is transferred to the MCR portal to evaluate the distal articular surfaces of the scaphoid and lunate, the proximal capitate, and the midcarpal portions of the SL and LT ligaments.
COMPLICATIONS AND RISK MITIGATION
While wrist arthroscopy is minimally invasive, it is not without risk. Complication rates vary in the literature from 1.2% to 5.2%. A recent comprehensive systematic analysis of 895 procedures across 11 studies identified an overall complication rate of 4.7%.
Complications can be systematically divided into four distinct categories:
1. Traction and Positioning Complications
- Peripheral Nerve Injury: Prolonged or excessive traction (>15 lbs) can lead to neurapraxia of the median, ulnar, or radial nerves. Traction time should ideally be limited to under 2 hours.
- Skin Injury: Skin sloughing or blistering can occur at the finger traps if applied incorrectly or if the patient has fragile skin (e.g., chronic corticosteroid use).
- Joint Stiffness: Postoperative stiffness can result from prolonged immobilization or excessive capsular trauma.
2. Portal and Instrument Insertion Complications
- Cutaneous Nerve Injury: The most common complication. The DSBUN is highly vulnerable at the 6U portal, and the SBRN at the 1-2 portal. Strict adherence to the "nick and spread" technique is mandatory.
- Tendon Injury: Iatrogenic laceration of the EPL, EDC, or EDM can occur if the scalpel penetrates beyond the dermis during portal creation.
- Articular Cartilage Scuffing: Forcible entry of the trocar without adequate joint distraction can cause irreversible iatrogenic chondral damage.
3. Procedure-Related Complications
- Compartment Syndrome: A catastrophic complication caused by fluid extravasation into the forearm compartments. This is particularly high-risk during the treatment of acute distal radius fractures where the capsule is breached.
- Mitigation: Avoid high-pressure infusion pumps. Use gravity flow or a syringe system. Frequently palpate the volar forearm during the procedure.
- Hardware Complications: Injury to sensory nerves during the percutaneous insertion of Kirschner wires for fracture or carpal instability fixation.
4. General Arthroscopic Complications
- Infection: Septic arthritis is exceedingly rare (<0.5%) but requires immediate arthroscopic irrigation and debridement if suspected.
- Equipment Failure: Breakage of small joint probes or shaver blades inside the joint necessitates immediate retrieval to prevent third-body wear.
Surgical Warning: If forearm swelling becomes tense during an arthroscopically assisted fracture reduction, immediately halt fluid inflow, remove the arthroscope, and assess compartment pressures. Extravasation through a capsular tear is the leading cause of iatrogenic compartment syndrome in wrist arthroscopy.
POSTOPERATIVE PROTOCOL
Postoperative management is dictated by the specific therapeutic intervention performed.
* Diagnostic Arthroscopy / Simple Debridement: A bulky soft dressing is applied. Immediate active range of motion (ROM) of the fingers is encouraged. The dressing is removed at 3-5 days, and wrist ROM exercises commence.
* TFCC Repair / Ligament Debridement: The wrist is immobilized in a sugar-tong splint or Muenster cast in neutral rotation for 4-6 weeks to protect the repair, followed by a graduated therapy program focusing on proprioception and progressive strengthening.
* Fracture Fixation: Immobilization protocols follow the standard guidelines for the specific fracture pattern, typically requiring 2-6 weeks of rigid support before initiating therapy.
CONCLUSION
Wrist arthroscopy represents a pinnacle of modern orthopedic surgery, offering unparalleled diagnostic accuracy and a robust therapeutic arsenal. A profound mastery of carpal anatomy, meticulous portal placement, and a strict adherence to safety protocols are required to maximize patient outcomes and minimize complications. As technology and techniques continue to evolve, the indications for wrist arthroscopy will undoubtedly continue to expand, further solidifying its role as an essential skill for the contemporary upper extremity surgeon.
You Might Also Like


